Reviewer Practical Exam 2 - Mikey
57
Clinical Pathology Practical 2 Review Special thanks to Pat Siao
-
Upload
remelou-garchitorena-alfelor -
Category
Documents
-
view
242 -
download
1
description
Powerpoint version
Transcript of Reviewer Practical Exam 2 - Mikey
Clinical PathologyPractical 2
Review
Special thanks to Pat Siao
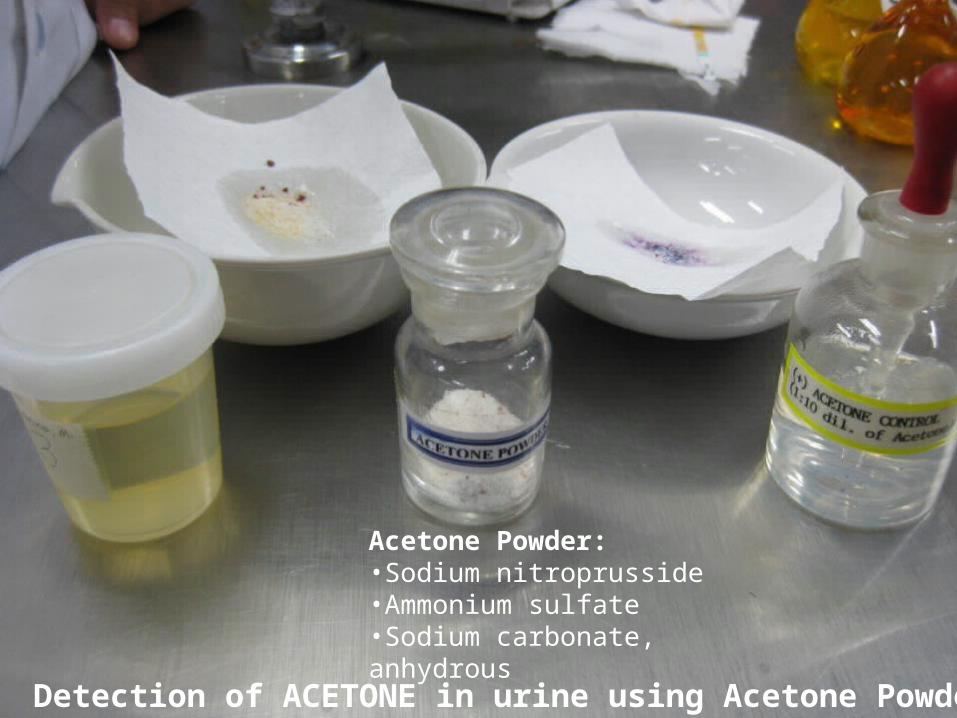
Detection of ACETONE in urine using Acetone Powder
Acetone Powder:•Sodium nitroprusside•Ammonium sulfate•Sodium carbonate, anhydrous
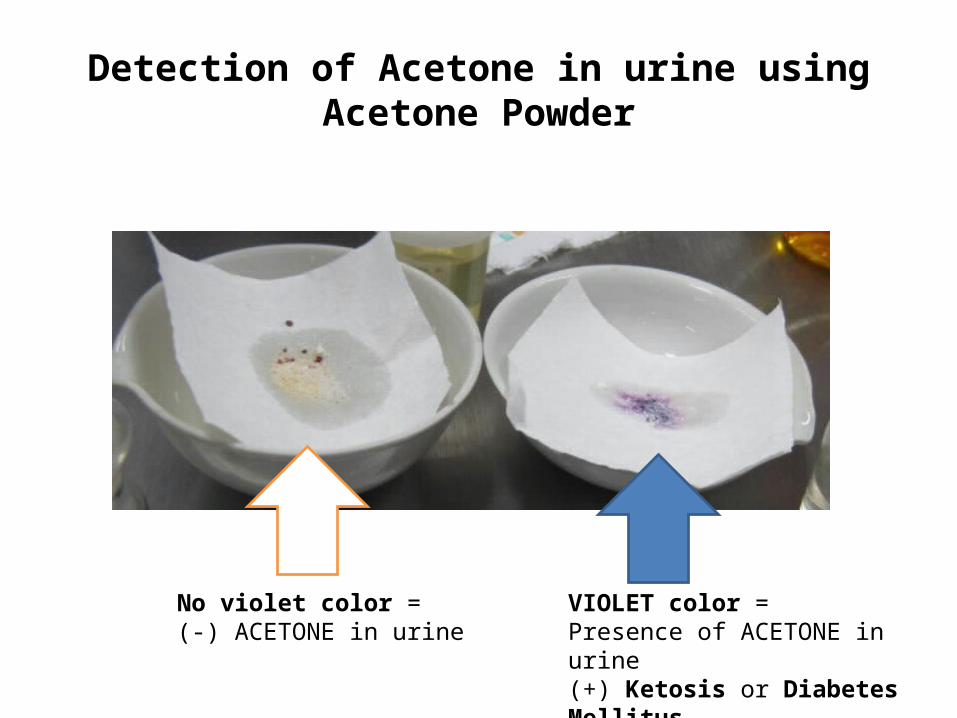
Detection of Acetone in urine using Acetone Powder
VIOLET color =Presence of ACETONE in urine(+) Ketosis or Diabetes Mellitus
No violet color =(-) ACETONE in urine
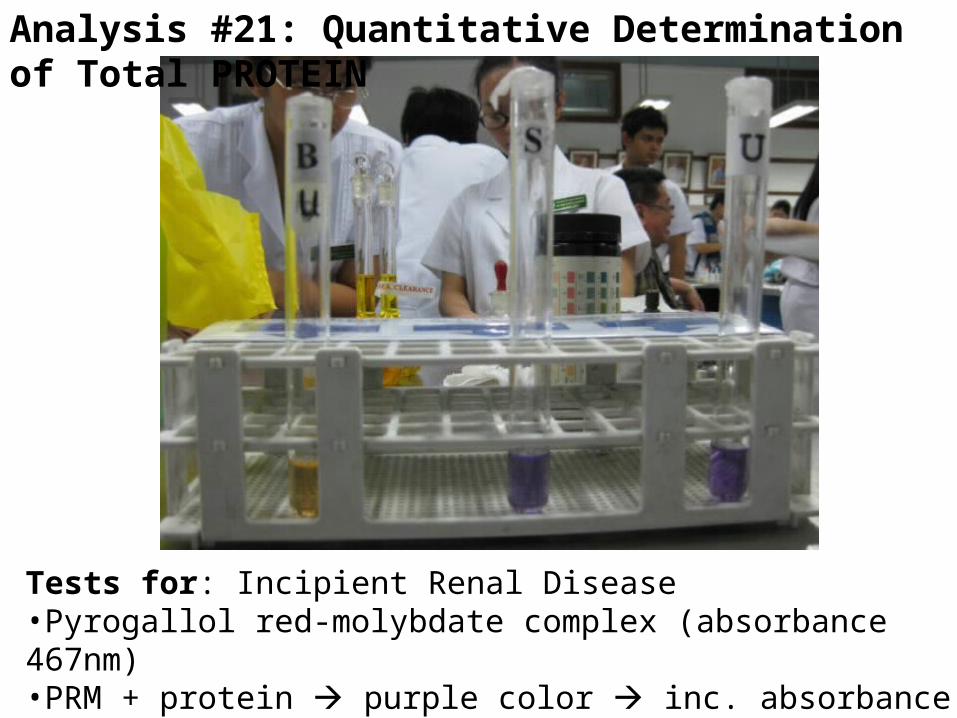
Analysis #21: Quantitative Determination of Total PROTEIN
Tests for: Incipient Renal Disease•Pyrogallol red-molybdate complex (absorbance 467nm)•PRM + protein purple color inc. absorbance (598nm)
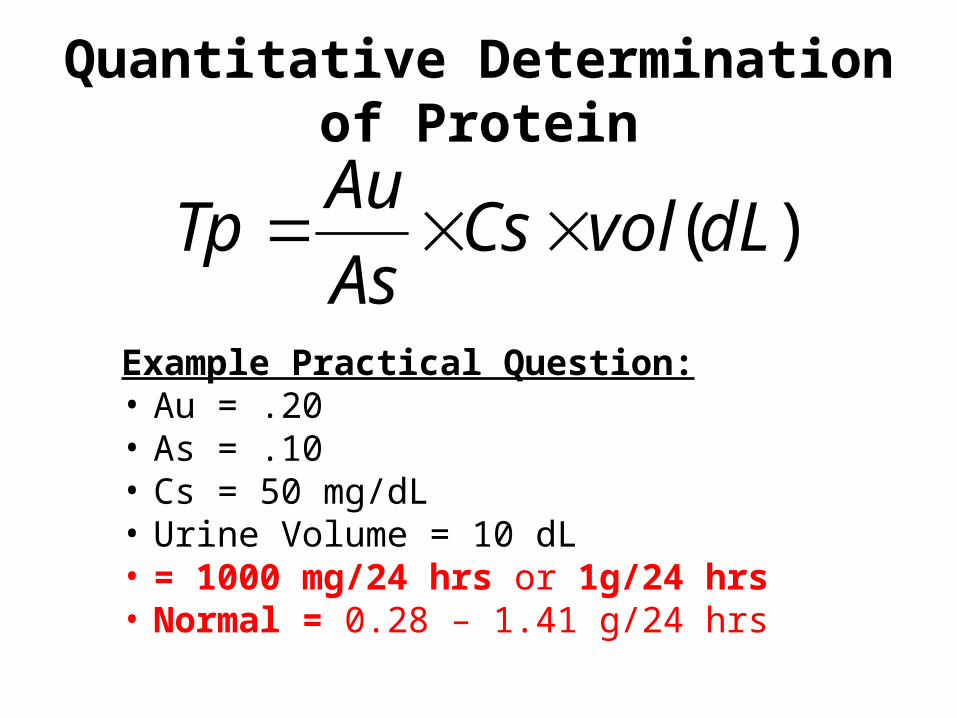
Quantitative Determination of Protein
Example Practical Question:• Au = .20• As = .10• Cs = 50 mg/dL• Urine Volume = 10 dL• = 1000 mg/24 hrs or 1g/24 hrs• Normal = 0.28 – 1.41 g/24 hrs
)(dLvolCsAs
AuTp
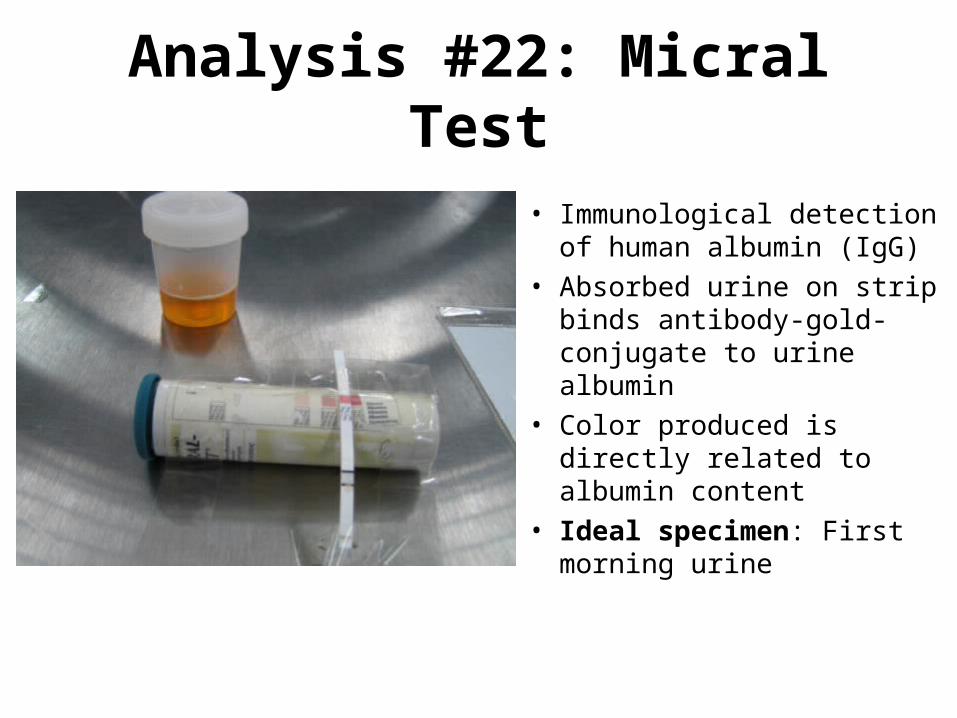
Analysis #22: Micral Test
• Immunological detection of human albumin (IgG)
• Absorbed urine on strip binds antibody-gold-conjugate to urine albumin
• Color produced is directly related to albumin content
• Ideal specimen: First morning urine
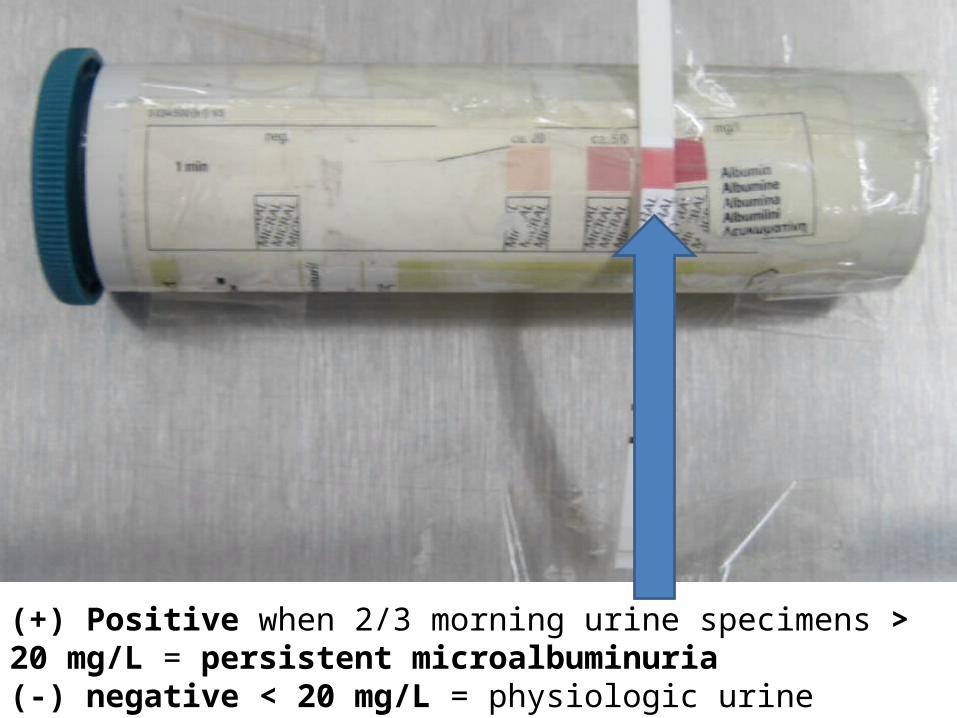
(+) Positive when 2/3 morning urine specimens > 20 mg/L = persistent microalbuminuria(-) negative < 20 mg/L = physiologic urine albumin concentration
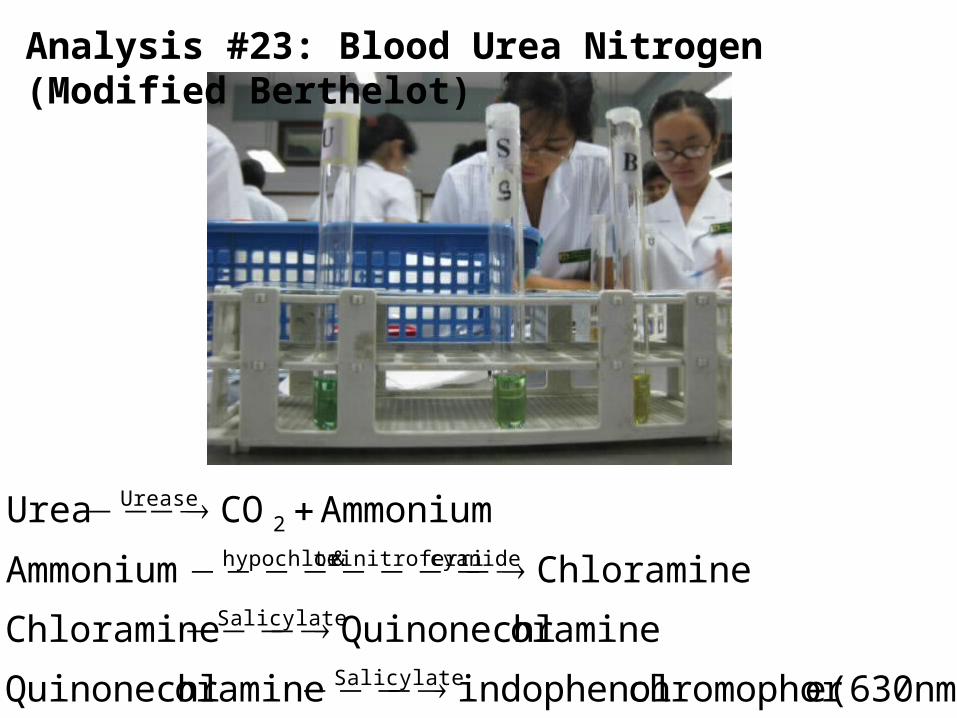
Analysis #23: Blood Urea Nitrogen (Modified Berthelot)
(630nm) echromophor indophenoloramineQuinonechl
oramineQuinonechlChloramine
ChloramineAmmonium
AmmoniumCOUrea
Salicylate
Salicylate
cyanidenitroferri & tehypochlori
2Urease
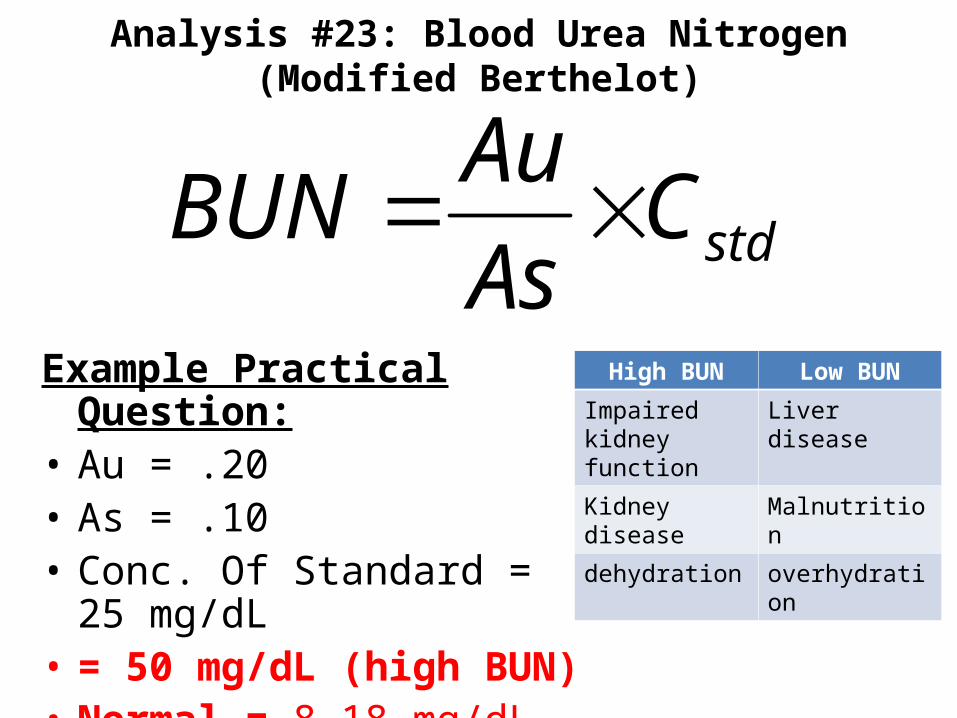
Analysis #23: Blood Urea Nitrogen (Modified Berthelot)
stdCAs
AuBUN
Example Practical Question:• Au = .20• As = .10• Conc. Of Standard = 25 mg/dL• = 50 mg/dL (high BUN)• Normal = 8-18 mg/dL
High BUN Low BUN
Impaired kidney function
Liver disease
Kidney disease Malnutrition
dehydration overhydration
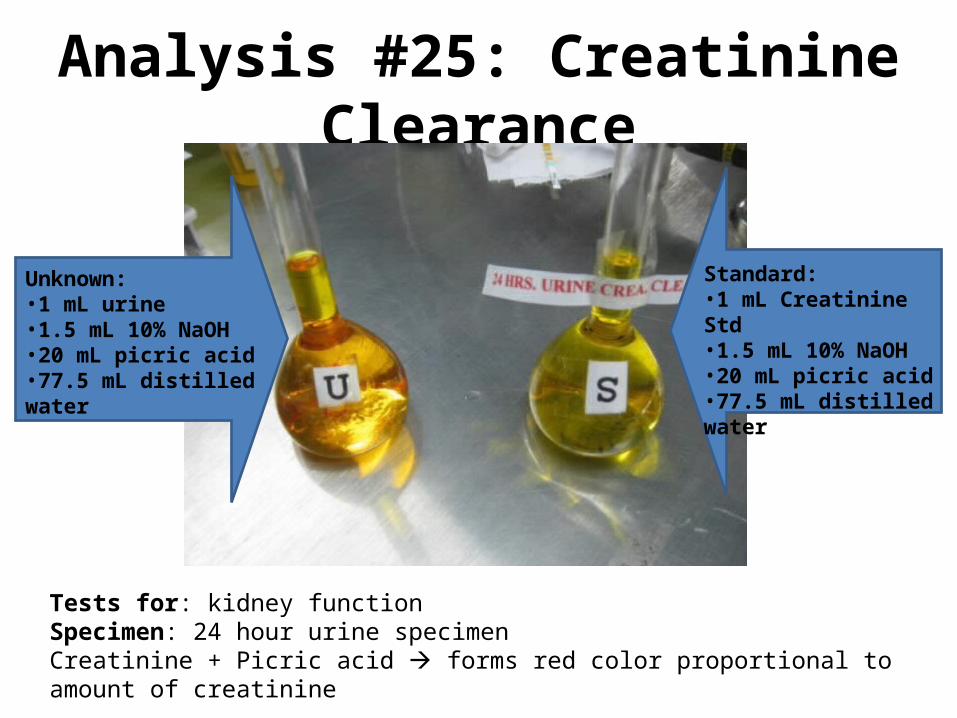
Analysis #25: Creatinine Clearance
Unknown:•1 mL urine•1.5 mL 10% NaOH•20 mL picric acid•77.5 mL distilled water
Standard:•1 mL Creatinine Std•1.5 mL 10% NaOH•20 mL picric acid•77.5 mL distilled water
Tests for: kidney functionSpecimen: 24 hour urine specimenCreatinine + Picric acid forms red color proportional to amount of creatinine
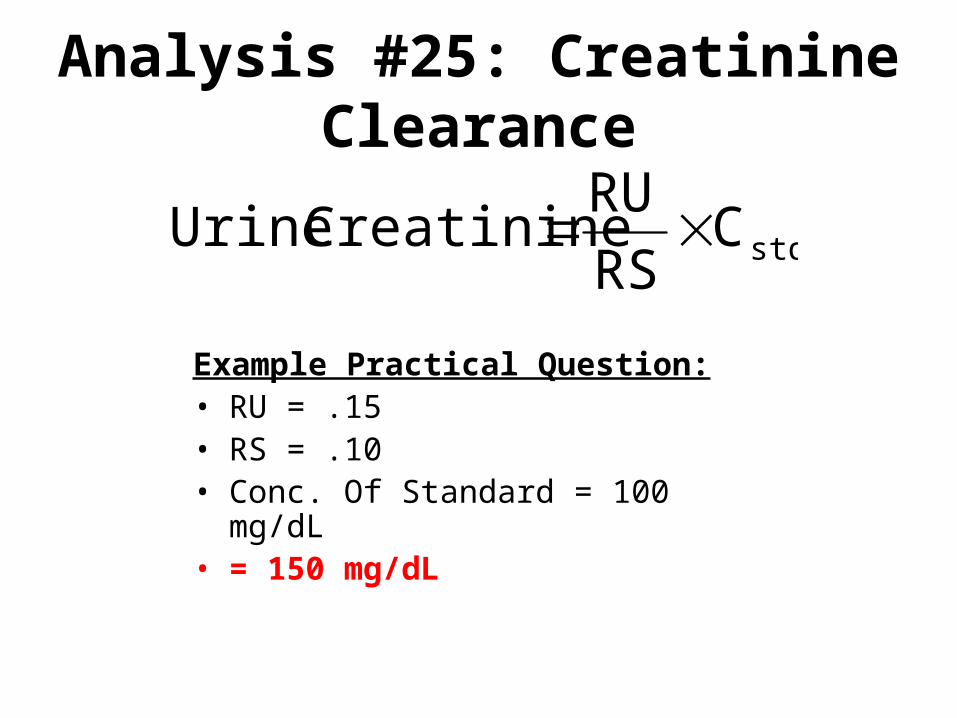
Analysis #25: Creatinine Clearance
stdCRS
RU Creatinine Urine
Example Practical Question:• RU = .15• RS = .10• Conc. Of Standard = 100 mg/dL• = 150 mg/dL
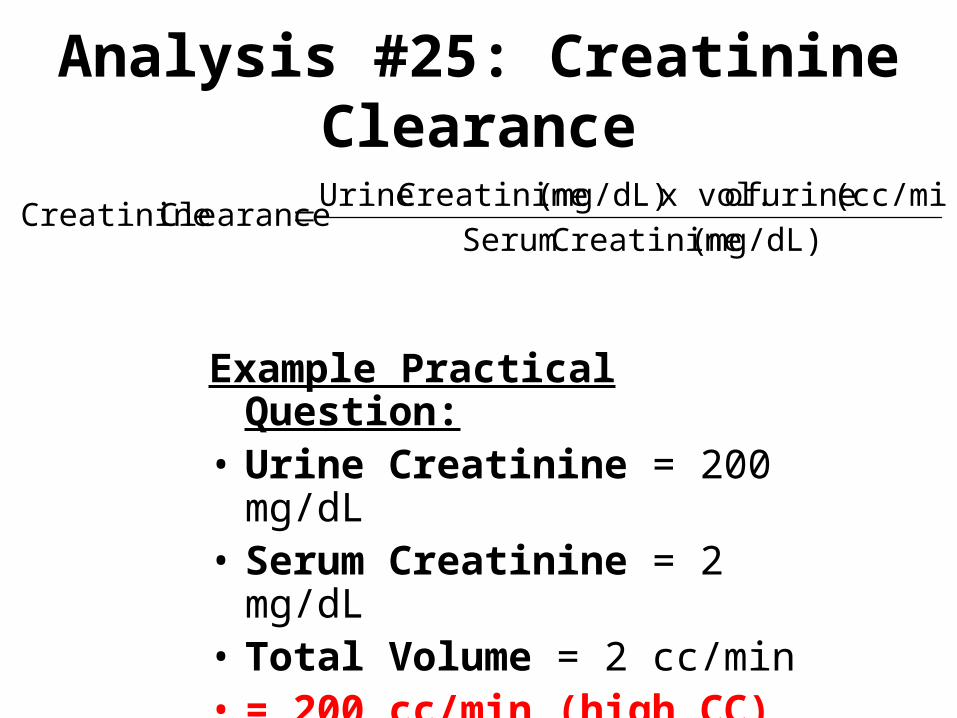
Analysis #25: Creatinine Clearance
(mg/dL) Creatinine Serum
(cc/min) urine of x vol.(mg/dL) Creatinine Urine Clearance Creatinine
Example Practical Question:• Urine Creatinine = 200 mg/dL• Serum Creatinine = 2 mg/dL• Total Volume = 2 cc/min• = 200 cc/min (high CC)• Normal = 55 – 118 cc/min
Microscope Findings in Urine
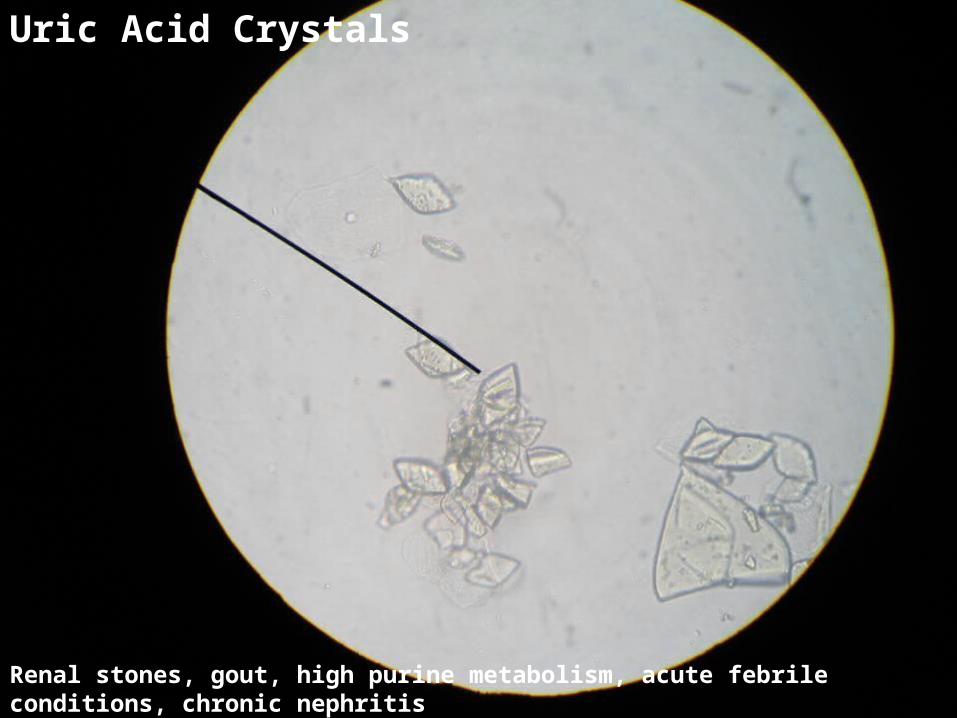
Uric Acid Crystals
Renal stones, gout, high purine metabolism, acute febrile conditions, chronic nephritis
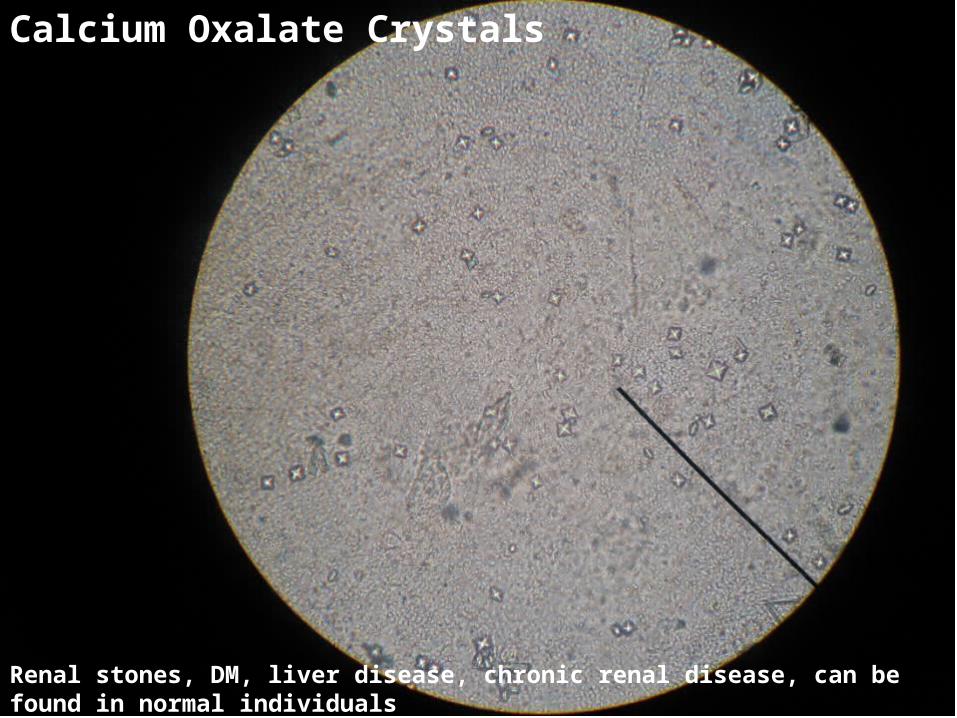
Calcium Oxalate Crystals
Renal stones, DM, liver disease, chronic renal disease, can be found in normal individuals

Triple Phosphate
Renal Canaliculi, Chronic Pyelitis, Enlarged prostate, UTI

Hyaline Cast
Severe renal disease with increased numbers, healthy individuals after heavy exercise

Granular Cast
Nonpathologic – strenuous exercise/stress; Pathologic – Glomerulonephritis, Pyelonephritis

Bacteria
With increased WBC UTI
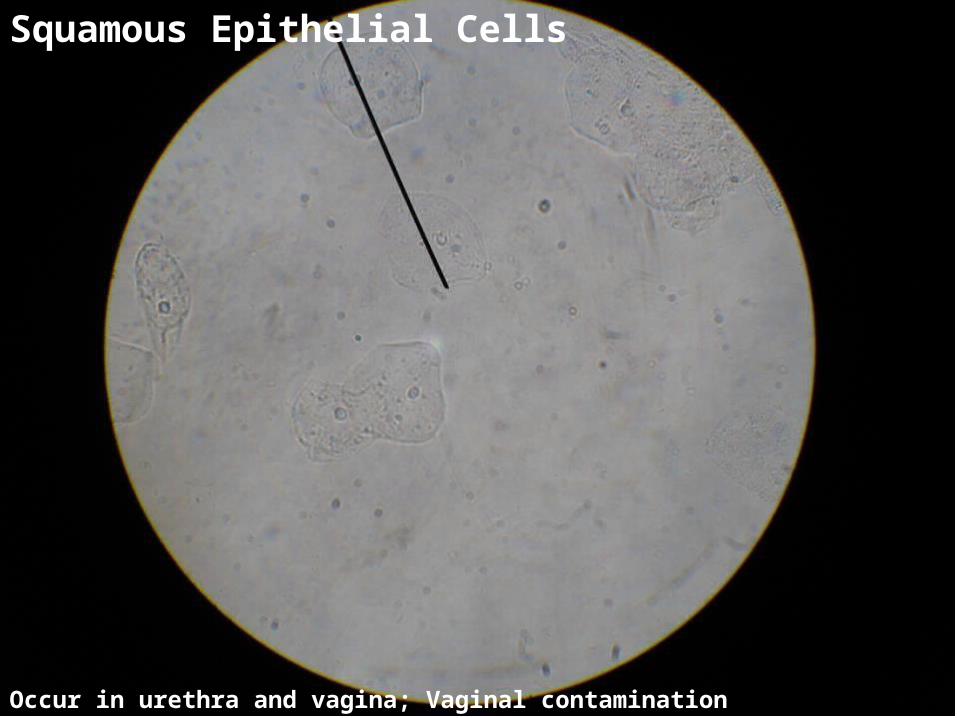
Squamous Epithelial Cells
Occur in urethra and vagina; Vaginal contamination

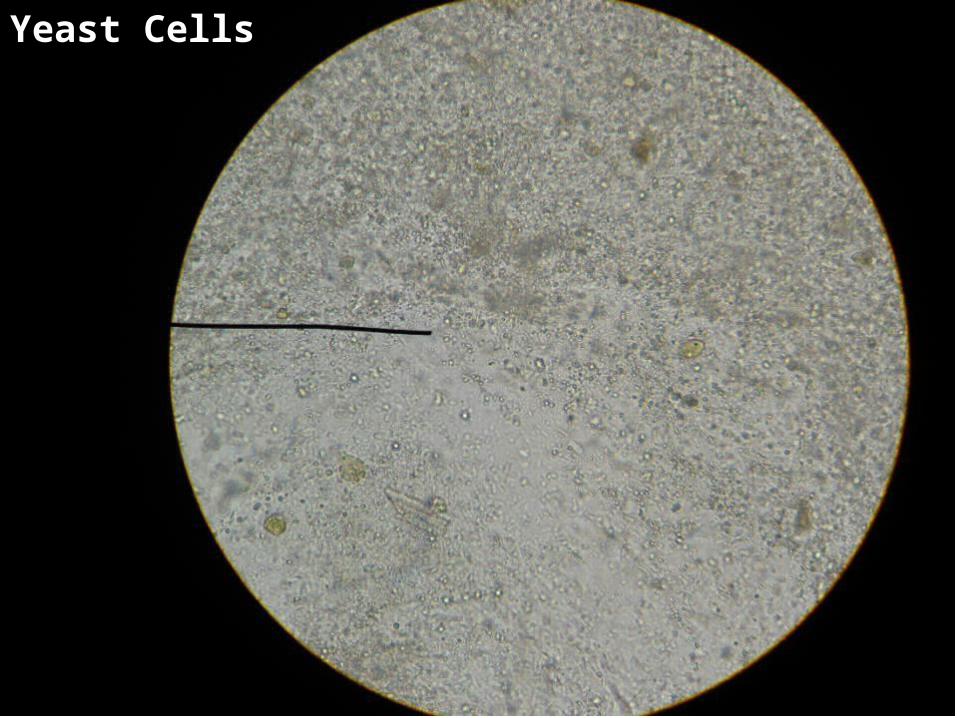
Yeast Cells (Budding Yeast)
UTI especially from diabetic parents, immunosuppressed patients, skin or vaginal inefections

Amorphous Urates

Pus Cells
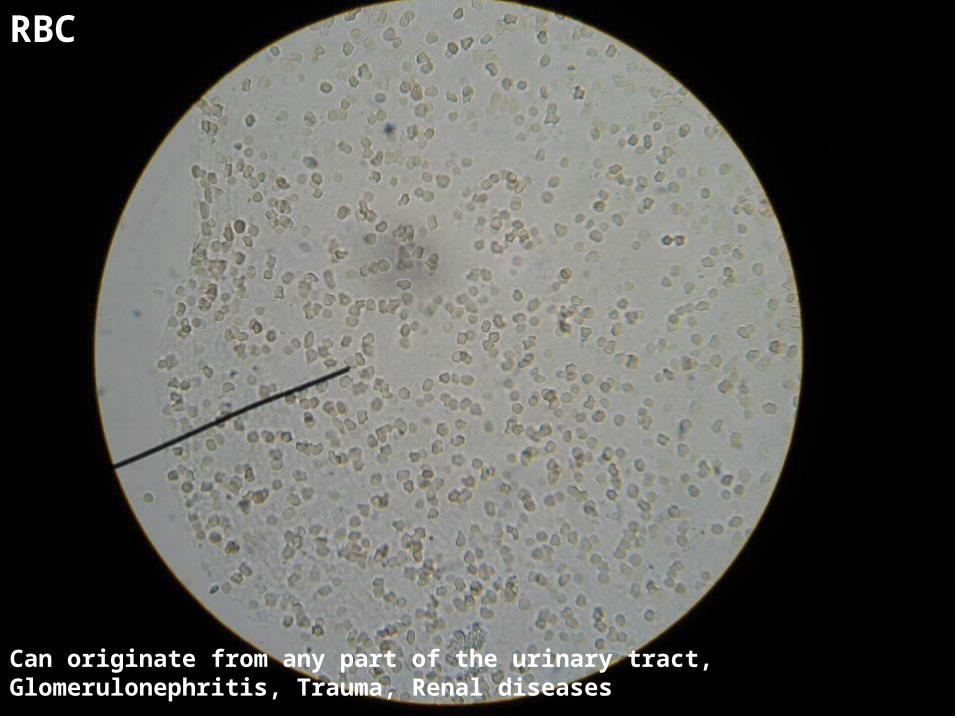
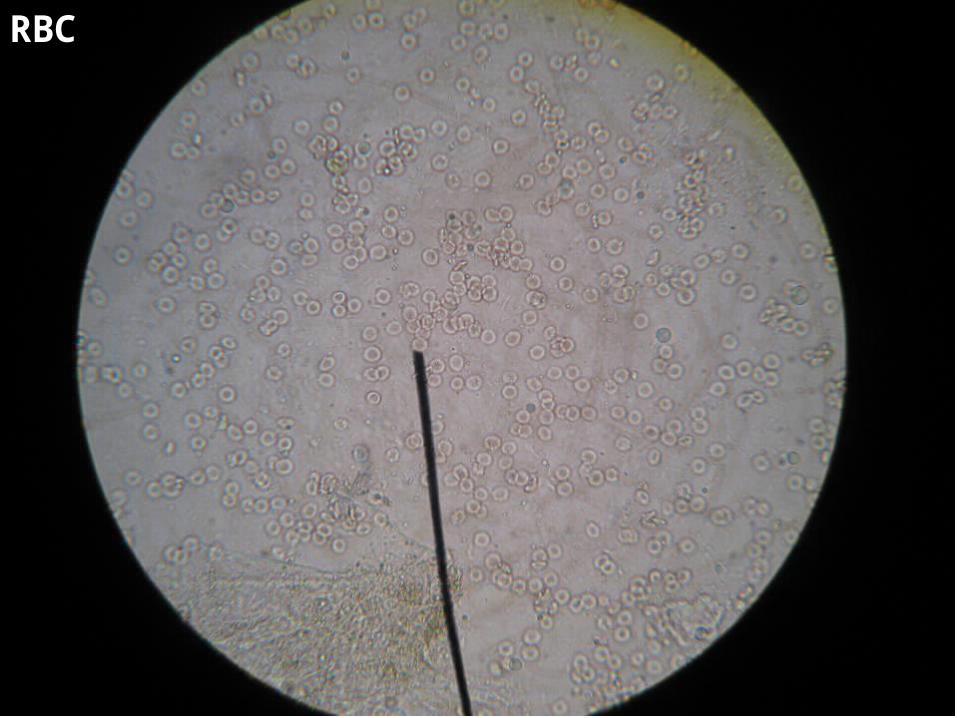
RBC
Can originate from any part of the urinary tract, Glomerulonephritis, Trauma, Renal diseases
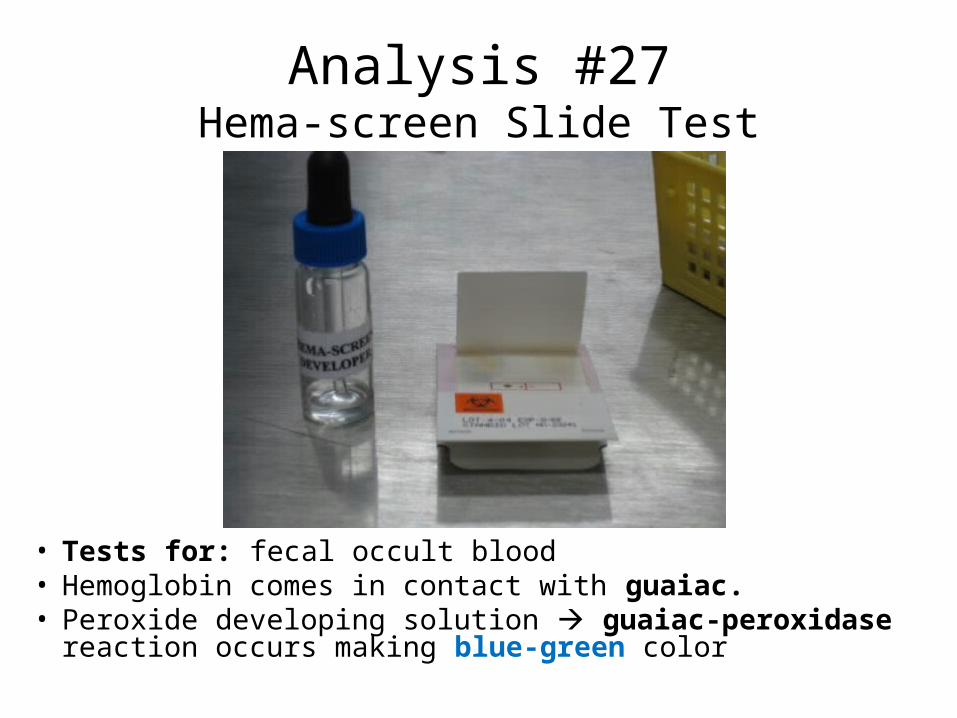
Analysis #27Hema-screen Slide Test
• Tests for: fecal occult blood• Hemoglobin comes in contact with guaiac.• Peroxide developing solution guaiac-peroxidase reaction
occurs making blue-green color
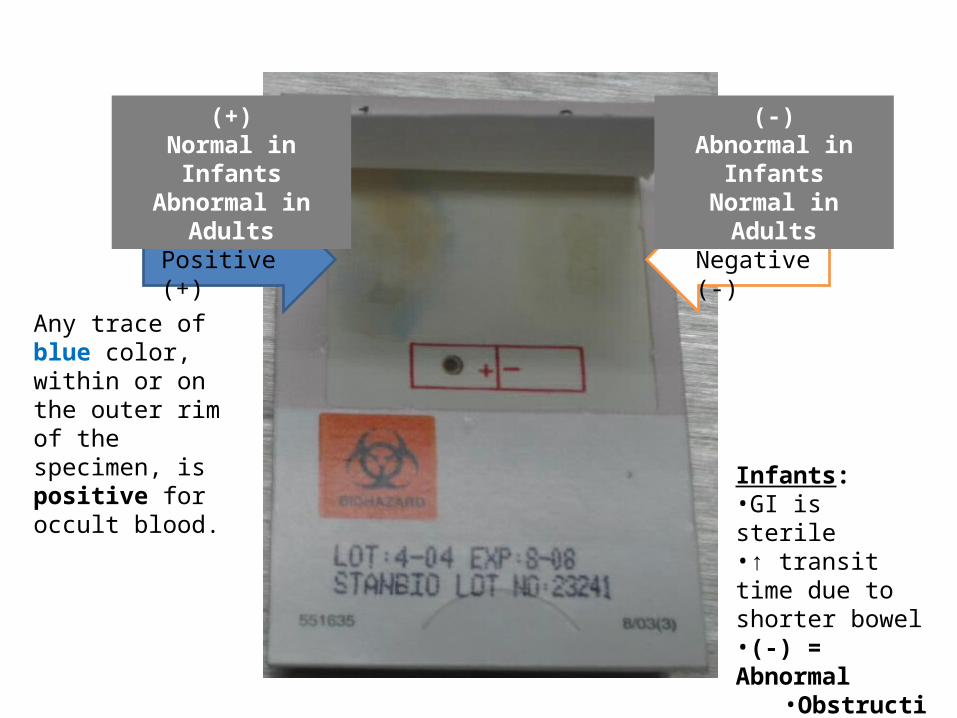
Positive (+) Negative (-)
Any trace of blue color, within or on the outer rim of the specimen, is positive for occult blood.
(+)Normal in Infants
Abnormal in Adults
(-)Abnormal in Infants
Normal in Adults
Infants:•GI is sterile•↑ transit time due to shorter bowel•(-) = Abnormal
•Obstruction•Cystic Fibrosis
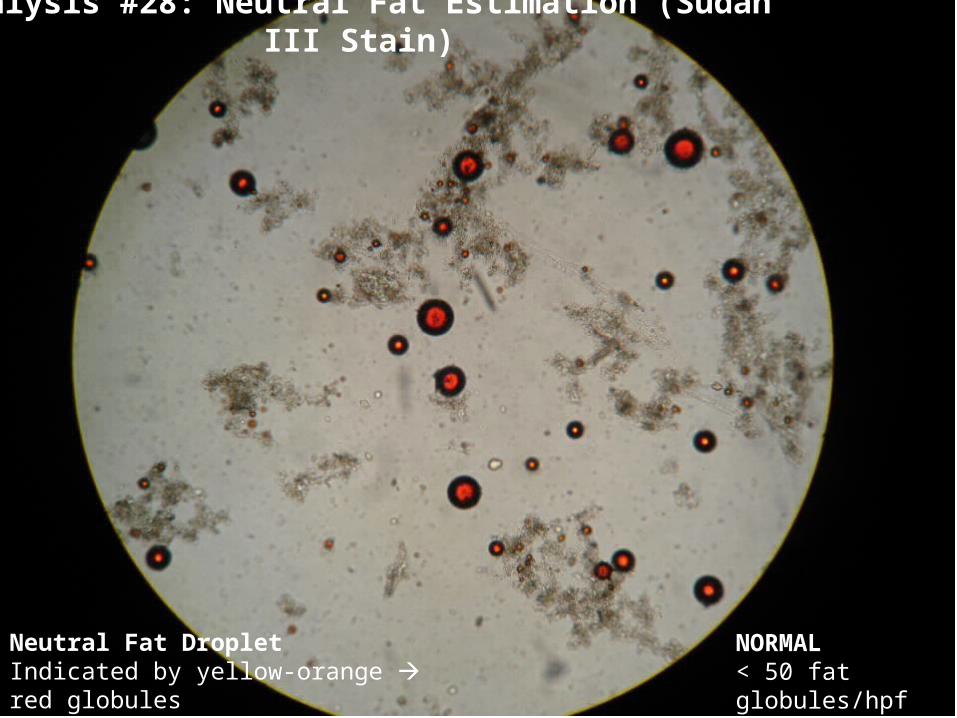
Analysis #28: Neutral Fat Estimation (Sudan III Stain)
Neutral Fat DropletIndicated by yellow-orange red globules
NORMAL< 50 fat globules/hpf
Positive (+)Normal
Negative (-)Abnormal
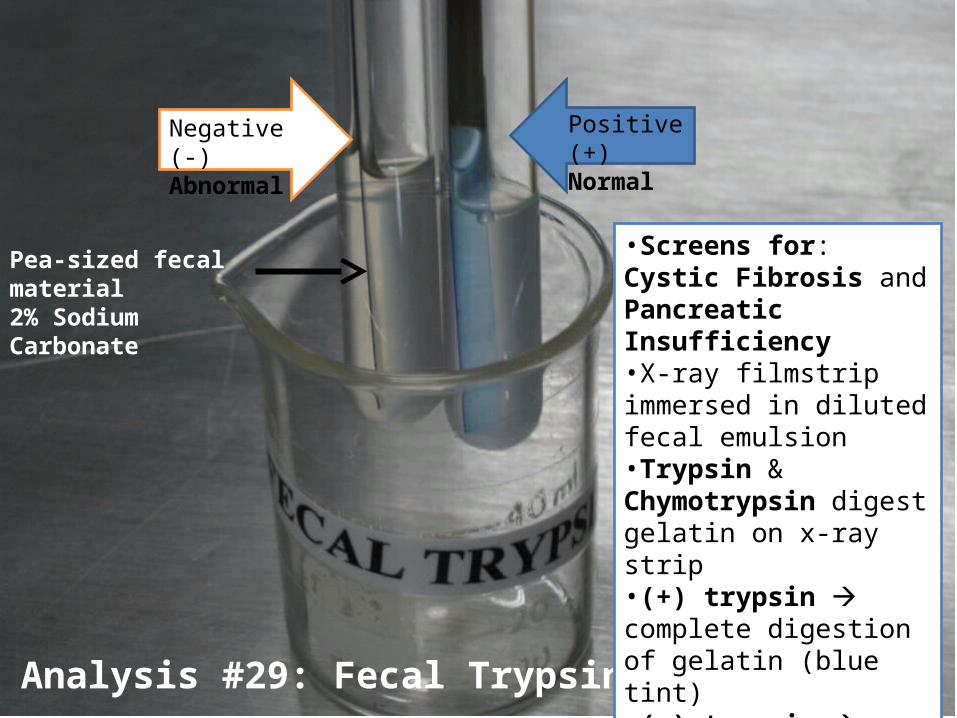
Analysis #29: Fecal Trypsin Determination
•Screens for: Cystic Fibrosis and Pancreatic Insufficiency•X-ray filmstrip immersed in diluted fecal emulsion•Trypsin & Chymotrypsin digest gelatin on x-ray strip•(+) trypsin complete digestion of gelatin (blue tint)•(-) trypsin gelatin remains intact
Pea-sized fecal material2% Sodium Carbonate
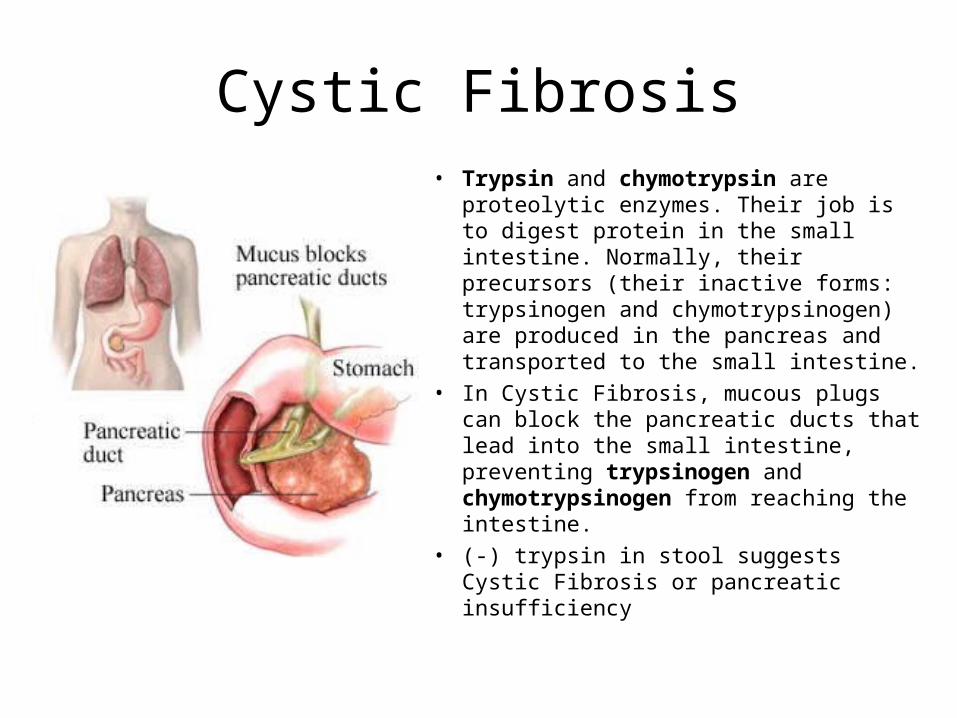
Cystic Fibrosis• Trypsin and chymotrypsin are proteolytic
enzymes. Their job is to digest protein in the small intestine. Normally, their precursors (their inactive forms: trypsinogen and chymotrypsinogen) are produced in the pancreas and transported to the small intestine.
• In Cystic Fibrosis, mucous plugs can block the pancreatic ducts that lead into the small intestine, preventing trypsinogen and chymotrypsinogen from reaching the intestine.
• (-) trypsin in stool suggests Cystic Fibrosis or pancreatic insufficiency
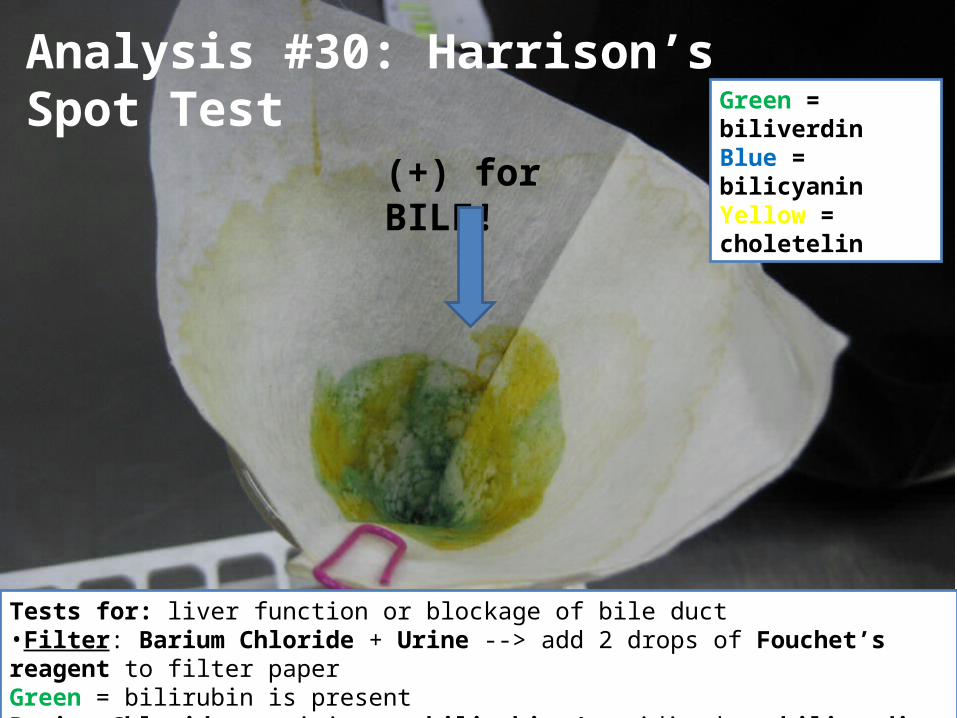
(+) for BILE!
Analysis #30: Harrison’s Spot TestGreen = biliverdinBlue = bilicyaninYellow = choletelin
Tests for: liver function or blockage of bile duct•Filter: Barium Chloride + Urine --> add 2 drops of Fouchet’s reagent to filter paperGreen = bilirubin is presentBarium Chloride precipitates bilirubin oxidized to biliverdin by ferric chloride
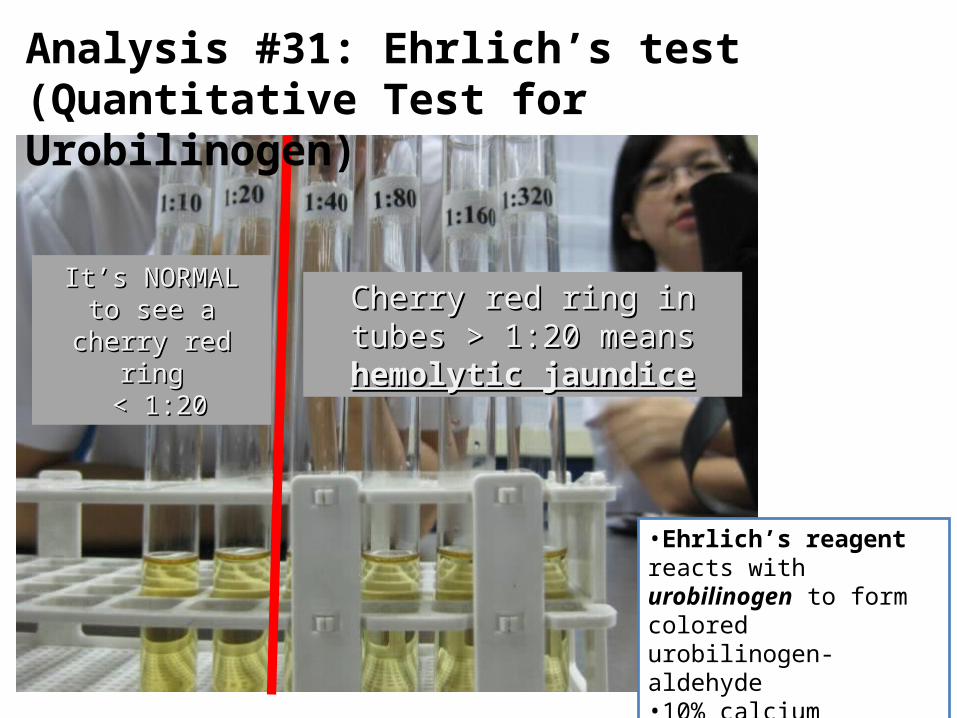
It’s NORMAL to see It’s NORMAL to see a cherry red ringa cherry red ring
< 1:20< 1:20Cherry red ring in tubes > 1:20 Cherry red ring in tubes > 1:20
means means hemolytic jaundicehemolytic jaundice
Analysis #31: Ehrlich’s test(Quantitative Test for Urobilinogen)
•Ehrlich’s reagent reacts with urobilinogen to form colored urobilinogen-aldehyde•10% calcium chloride – removes bilirubin
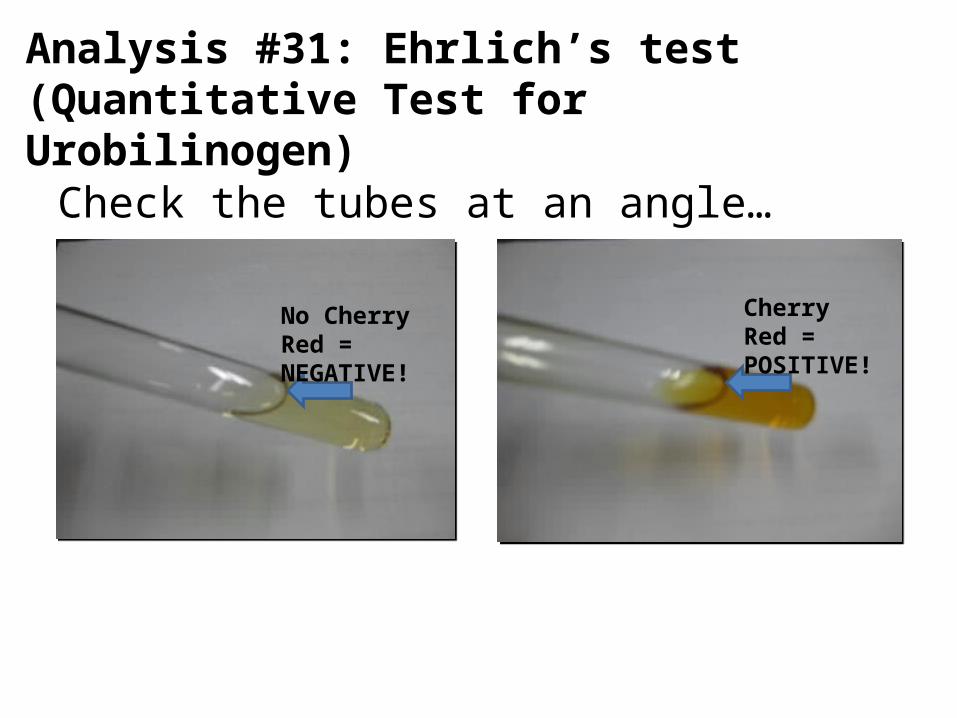
Check the tubes at an angle…
Cherry Red = POSITIVE!
No Cherry Red = NEGATIVE!
Analysis #31: Ehrlich’s test(Quantitative Test for Urobilinogen)
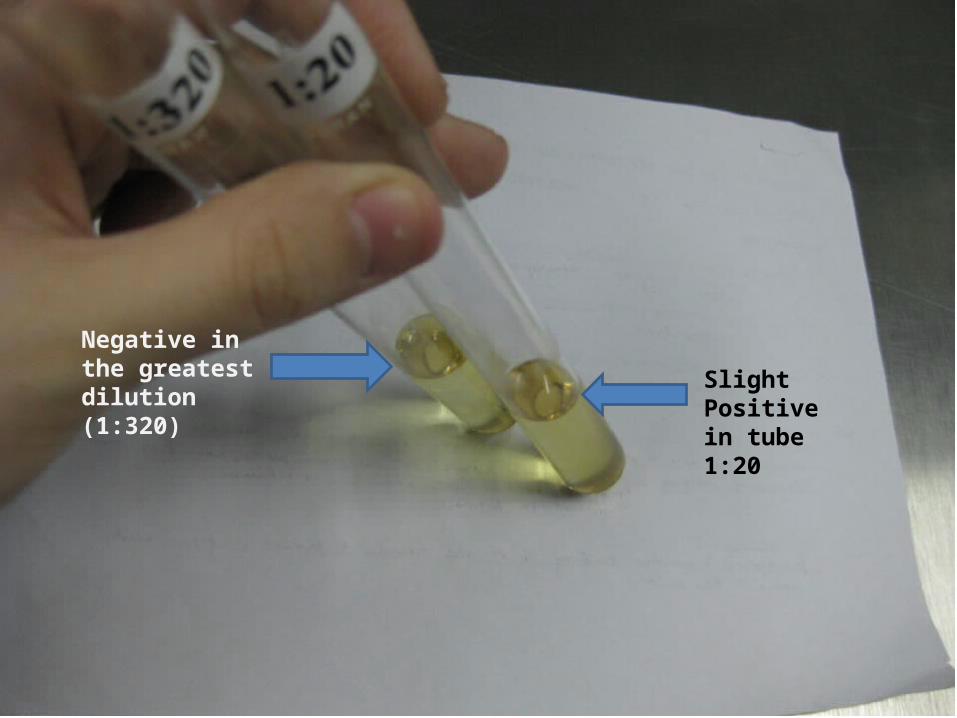
Slight Positive in tube 1:20
Negative in the greatest dilution (1:320)
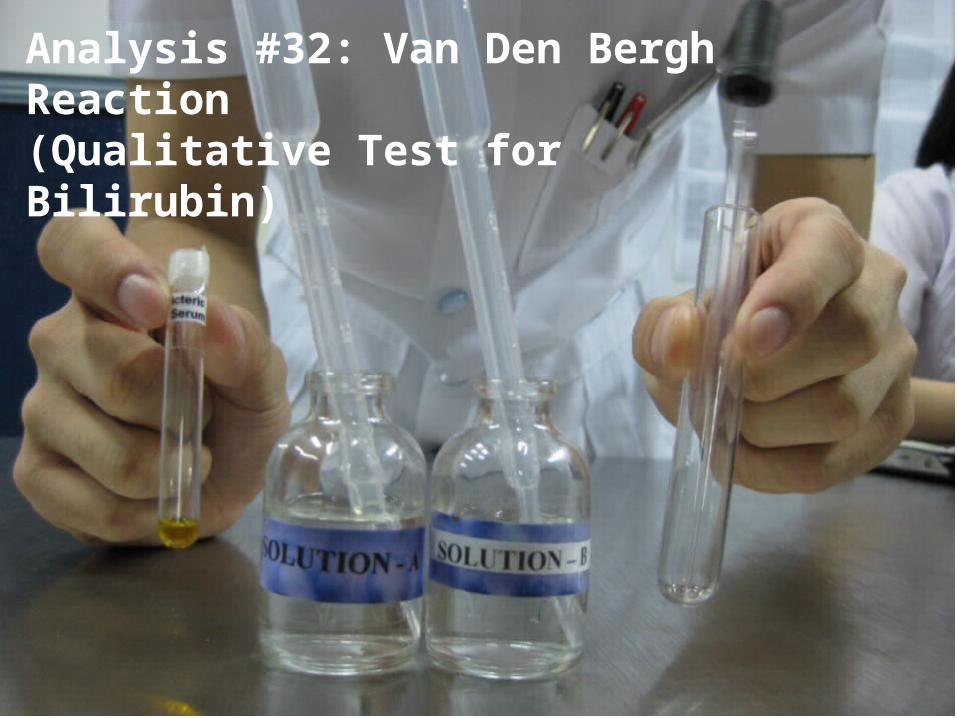
Analysis #32: Van Den Bergh Reaction(Qualitative Test for Bilirubin)
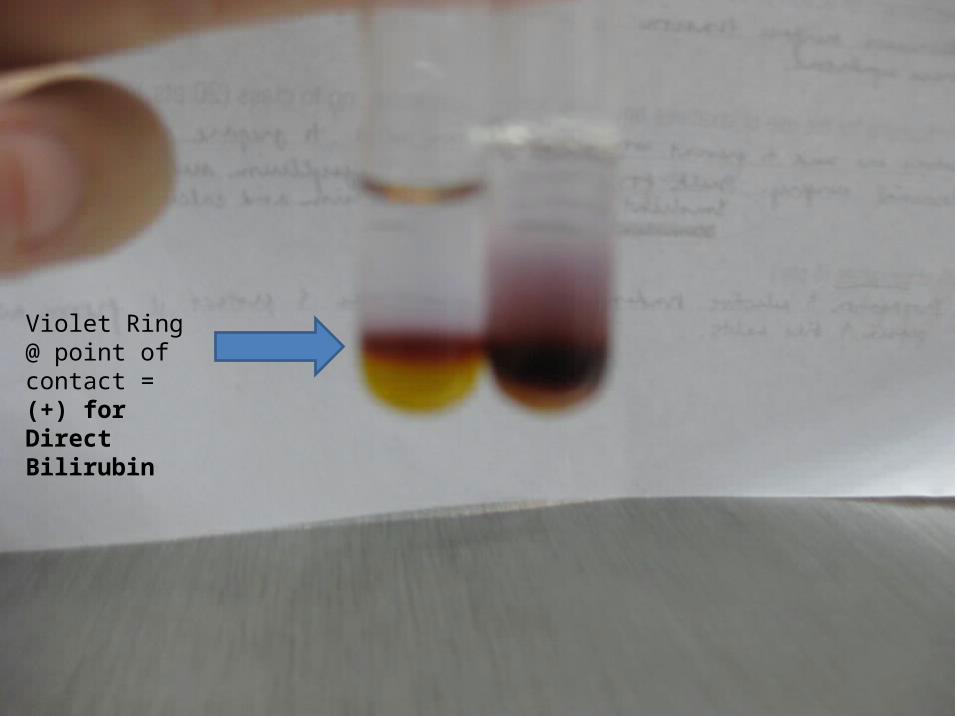
Violet Ring @ point of contact =(+) for Direct Bilirubin
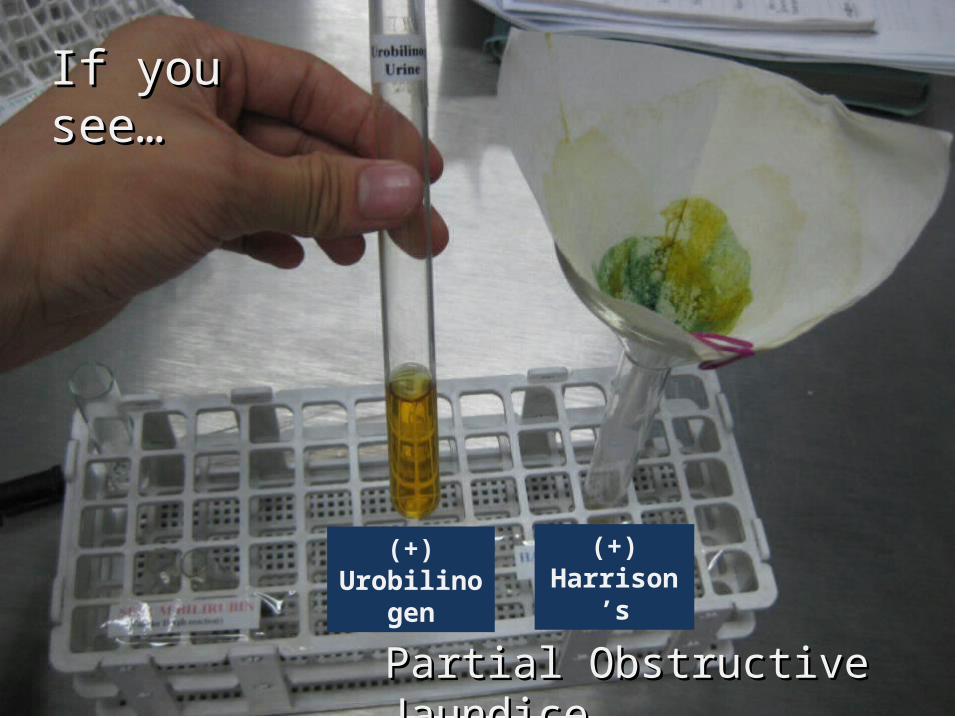
If you see…If you see…
(+)Urobilinogen
(+)Harrison’s
Partial Obstructive JaundicePartial Obstructive Jaundice
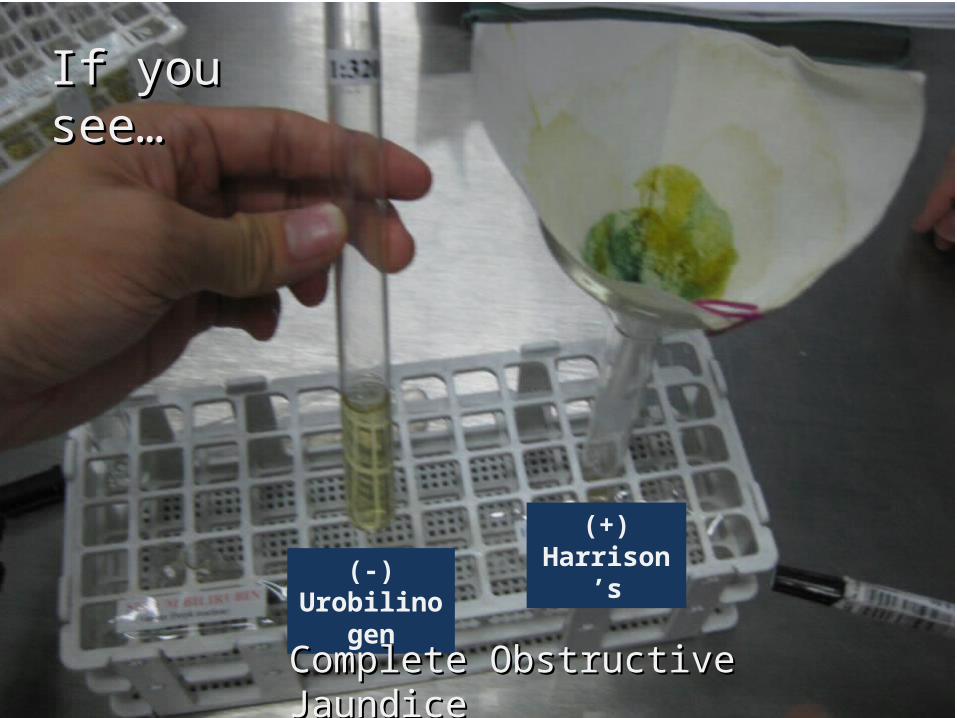
If you see…If you see…
(-)Urobilinogen
(+)Harrison’s
Complete Obstructive JaundiceComplete Obstructive Jaundice
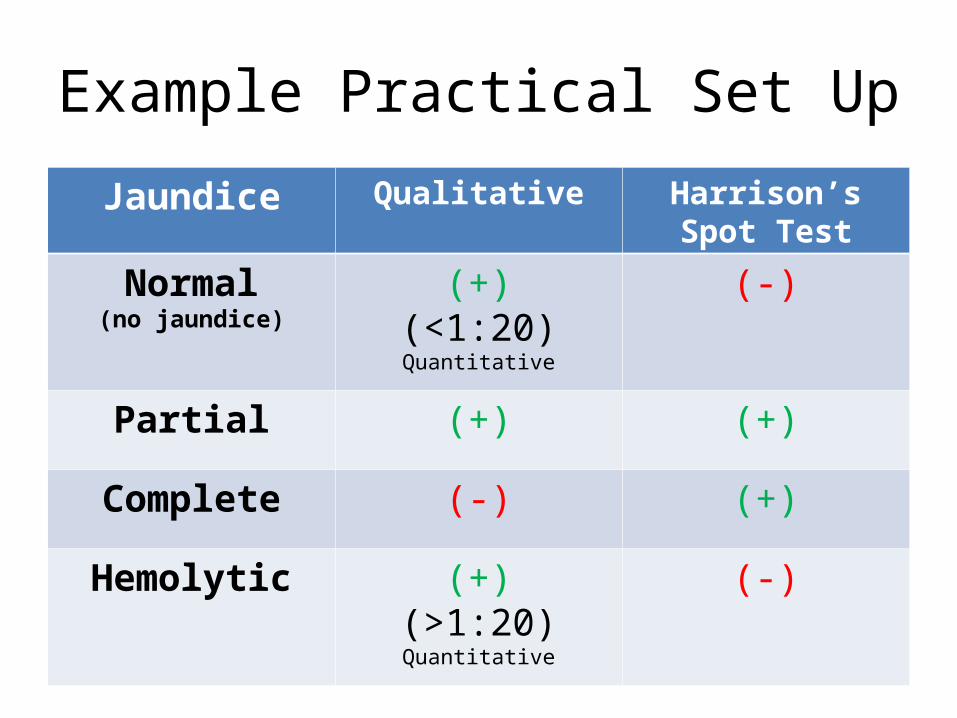
Example Practical Set Up
Jaundice Qualitative Harrison’s Spot Test
Normal(no jaundice)
(+)(<1:20)Quantitative
(-)
Partial (+) (+)
Complete (-) (+)
Hemolytic (+)(>1:20)Quantitative
(-)

Microscope Findings in Feces

Vegetable Cells

Vegetable Cells

Vegetable Cells

Vegetable Fibers
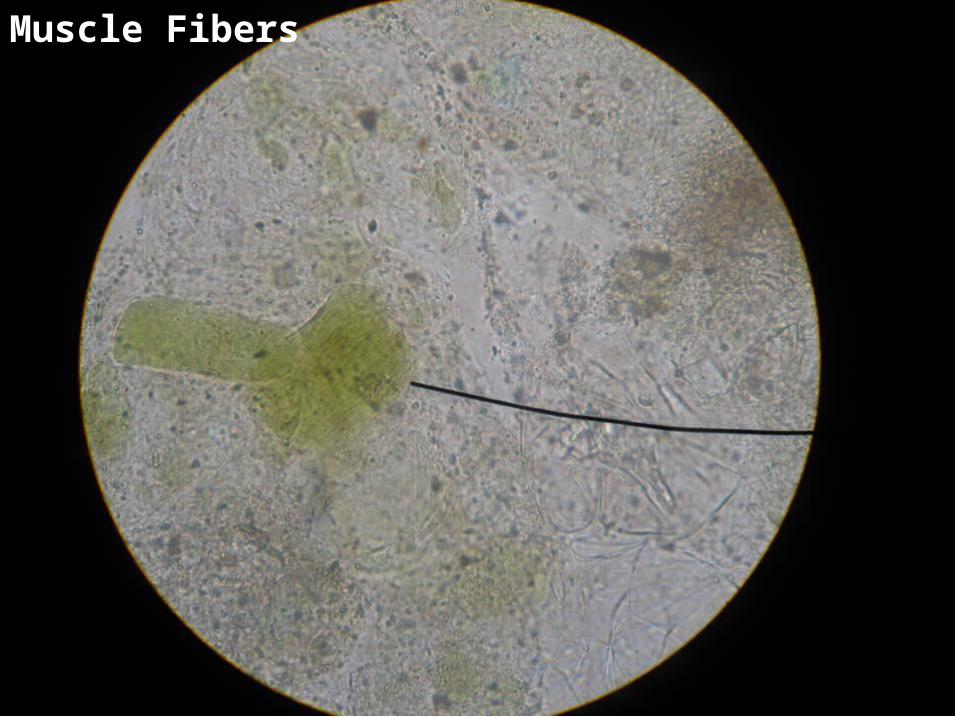
Muscle Fibers

Muscle Fibers

Muscle Threads
Yeast Cells
RBC

Pus Cells
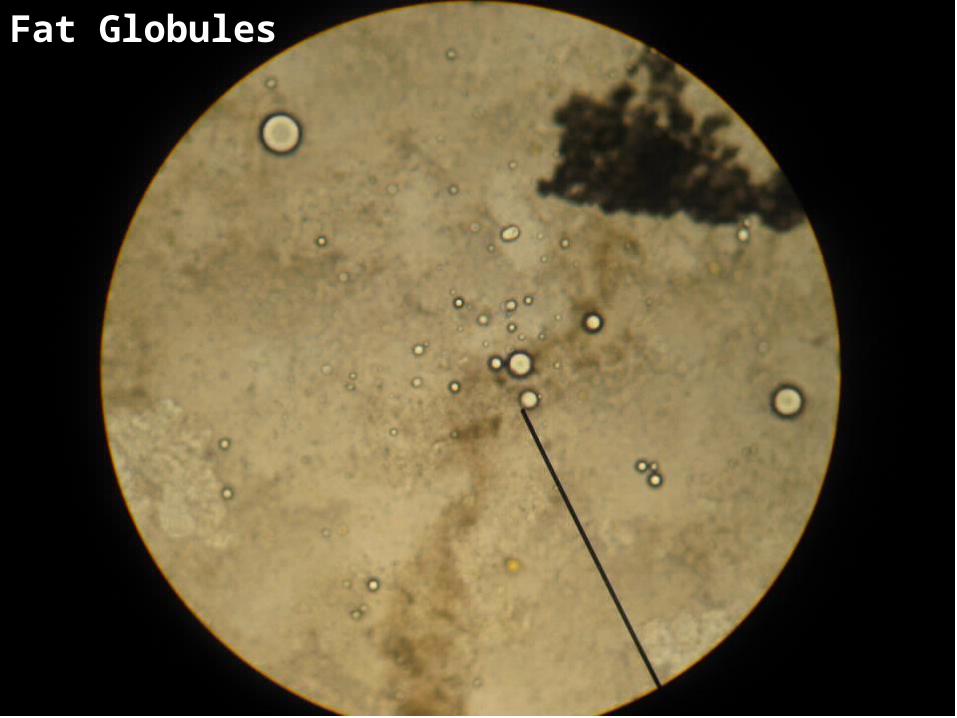
Fat Globules
Analysis #33: Blood Grouping
• Forward typing determines antigens on patient's or donor's cells– Cells are tested with the
antisera reagents anti-A, anti-B
• Reverse typing determines antibodies in patient's or donor's serum or plasma
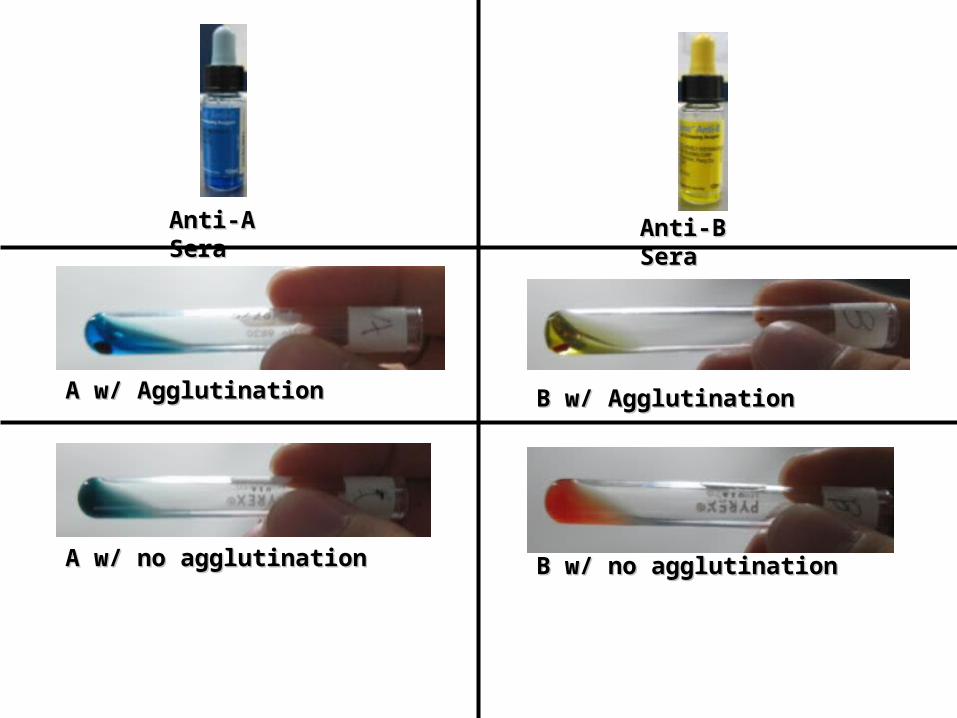
Anti-A SeraAnti-A Sera
A w/ AgglutinationA w/ Agglutination
A w/ no agglutinationA w/ no agglutination
Anti-B SeraAnti-B Sera
B w/ AgglutinationB w/ Agglutination
B w/ no agglutinationB w/ no agglutination

Forward Typing Table
Anti-A Anti-B
Blood Type
(-)(-) (-)(-) OO(+)(+) (+)(+) ABAB(+)(+) (-)(-) AA(-)(-) (+)(+) BB
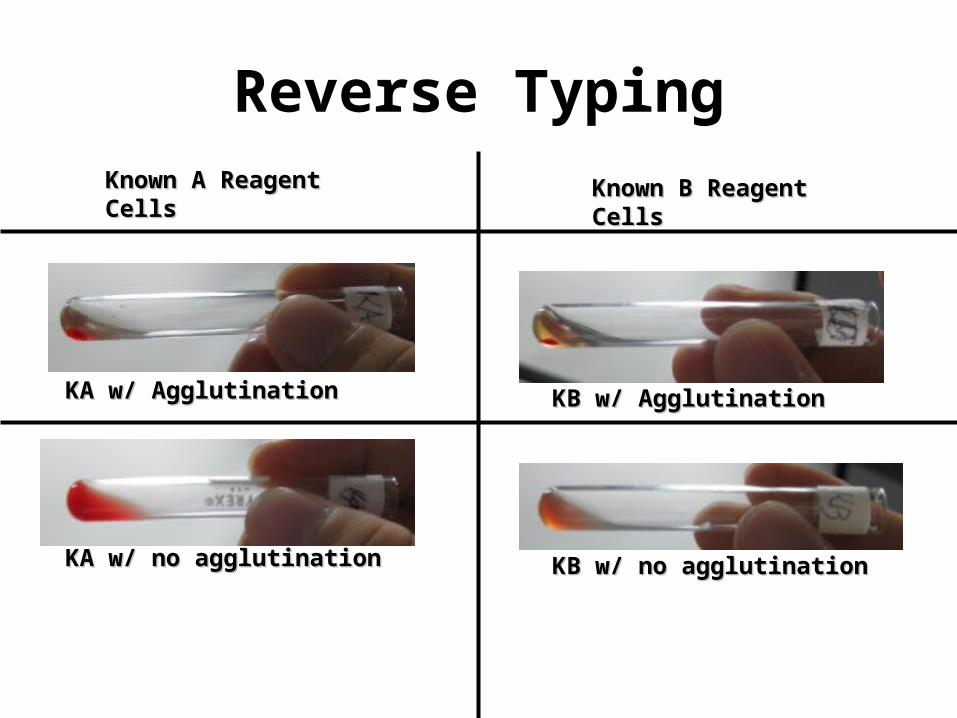
Reverse TypingKnown A Reagent CellsKnown A Reagent Cells
KA w/ AgglutinationKA w/ Agglutination
KA w/ no agglutinationKA w/ no agglutination
Known B Reagent CellsKnown B Reagent Cells
KB w/ AgglutinationKB w/ Agglutination
KB w/ no agglutinationKB w/ no agglutination
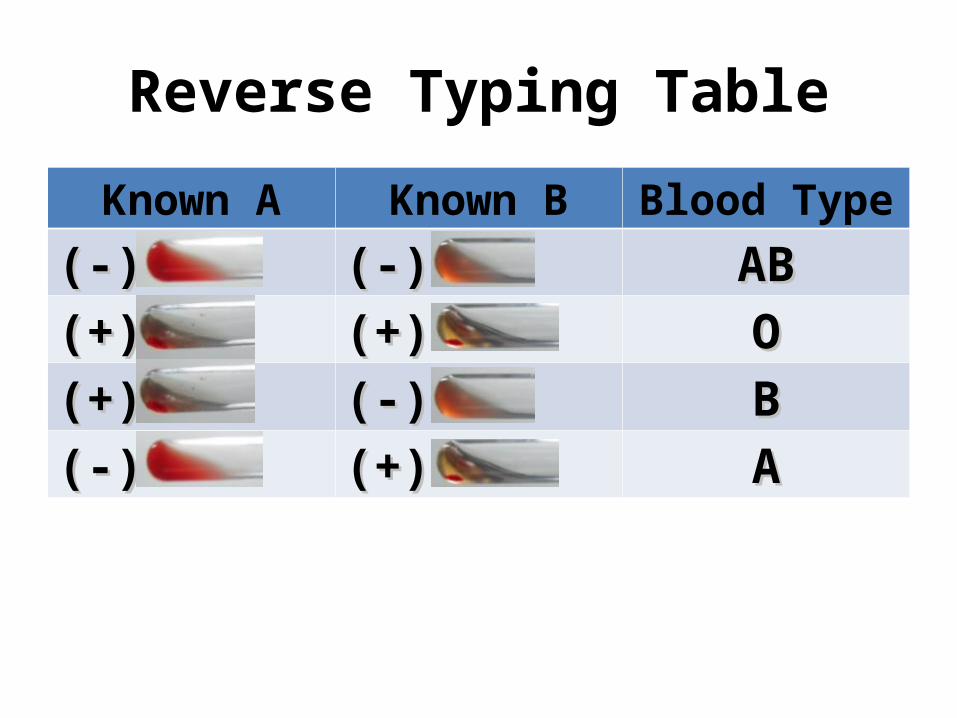
Reverse Typing Table
Known A Known B Blood Type
(-)(-) (-)(-) ABAB(+)(+) (+)(+) OO(+)(+) (-)(-) BB(-)(-) (+)(+) AA
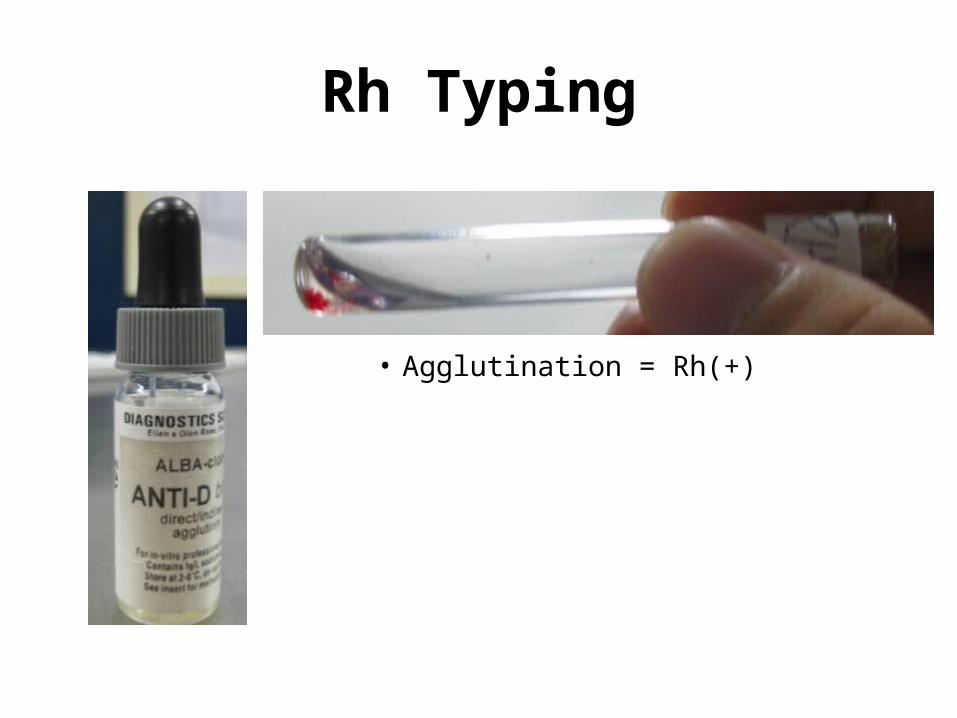
Rh Typing
• Agglutination = Rh(+)