RESPIRATORY REHABILITATION: Broader scope, extended focus€¦ · 1 : score 5 questions: adequate...
65
RESPIRATORY REHABILITATION: Broader scope, extended focus
Transcript of RESPIRATORY REHABILITATION: Broader scope, extended focus€¦ · 1 : score 5 questions: adequate...

RESPIRATORY REHABILITATION: Broader scope, extended focus

1895



1960 1977


‘The physiotherapist will come do exercises on your chest’

1990 1990

LUNGS AND
AIRWAYS
CHEST WALL
AND RESPIRATORY MUSCLES
HEART AND CIRCULATION
LIMB MUSCLES
ANXIETY AND MOTIVATION

Casaburi & ZuWallack NEJM 2009


www.fysionet.nl
www.cebp.nl
www.bvp-sbp.org
Dutch
English
French
Portugese

Retained secretions Lung collaps Weaning
Deconditioning
Inactivity
Emotional functioning

Deconditioning
Inactivity

Herridge et al. N.Engl.J.Med. 2003/2011
%pr
edicte
d
RECOVERY AFTER ARDS
months

‘Our results suggest that the inability to exercise is primarily due
to extrapulmonary disease; our impression is that impaired muscle function had an important effect on
the long-term outcomes in these patients’
Herridge et al. N.Engl.J.Med. 348:683-693, 2003

Helliwell et al. Neuropathology and Appl Neurobiol. 24, 507-517, 1998.
Type I
Type II
~ 3% per day
~ 4% per day
Limb muscle weakness in critically ill patients


Schefold et al. J Cach Sarcop Muscle 2010; 1:147

Gruther et al. J Rehabil Med 2008; 40: 185–189
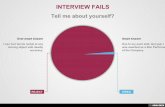
Thigh muscle layer thickness in critically ill ventilated patients
Thigh t
hickne
ss (cm
)
ICU stay (days)

Iwashyna TJ AJRCCM 2012: 186:302

“The physician must always consider
complete bed rest as a highly
unphysiologic and definitely hazardous form of therapy, to be ordered only for
specific indications and discontinued as early as possible”.
The indications for which bed rest should be
prescribed, and for how long, are yet to be defined.
Dock W. The evil sequelae of complete bed rest. JAMA 1944; 125:1083 – 85 .


Rest
Stimulus
Current AND Pre-existent comorbid conditions
Modality Intensity Duration

1 : score 5 questions: adequate response to 5 standardized orders
2 : FAILS = at least 1 risk factor present / 3 : if basic assessment failed, decrease to level 0 4 : safety: each activity should be deferred if severe adverse events (cv., resp. and subject. intolerance) occur during the intervention
Neurological or surgical or trauma condition does not allow transfer to chair
NO-LOW COOPERATION
S5Q1 < 3
MODERATE COOPERATION
S5Q1 ≥ 3
CLOSE TO FULL COOPERATION
S5Q1 ≥ 4/5
FULL COOPERATION
S5Q1 = 5
PHYSIOTHERAPY4
Passive range of motion
Passive bed cycling
NMES
BODY POSITIONING4
2hr turning
Fowler’s position
Splinting
PHYSIOTHERAPY4
Passive/Active range of motion
Resistance training arms and legs
Passive/Active leg and/or cycling in bed or chair
NMES
BODY POSITIONING4
2hr turning
Splinting
Upright sitting position in bed
Passive transfer bed to chair
PASSES BASIC ASSESSMENT3 +
PASSES BASIC ASSESSMENT3 +
PHYSIOTHERAPY4
Passive/Active range of motion
Resistance training arms and legs
Active leg and/or arm cycling in bed or chair
NMES
ADL
BODY POSITIONING4
2hr turning
Passive transfer bed to chair
Sitting out of bed
Standing with assist (2 ≥ pers)
PASSES BASIC ASSESSMENT3 +
PHYSIOTHERAPY4
Passive/Active range of motion
Resistance training arms and legs
Active leg and/or arm cycling in chair or bed
Walking (with assistance/frame)
NMES
ADL
PASSES BASIC ASSESSMENT3 +
LEVEL 0 LEVEL 5
FULL COOPERATION
S5Q1 = 5
PHYSIOTHERAPY4
Passive/Active range of motion
Resistance training arms and legs
Active leg and arm cycling in chair
Walking (with assistance)
NMES
ADL
BODY POSITIONING4
Active transfer bed to chair
Sitting out of bed
Standing
PASSES BASIC ASSESSMENT3 +
LEVEL 1 LEVEL 2 LEVEL 3 LEVEL 4
Obesity or neurological or surgical or trauma condition does not allow active transfer to chair (even if MRCsum ≥ 36)
MRCsum ≥ 36 +
BBS² Sit to stand = 0 +
BBS² Standing = 0 +
BBS² Sitting ≥ 1
MRCsum ≥ 48 +
BBS² Sit to stand ≥ 0 +
BBS² Standing ≥ 0 +
BBS² Sitting ≥ 2
MRCsum ≥ 48 +
BBS² Sit to stand ≥ 1 +
BBS² Standing ≥ 2 +
BBS² Sitting ≥ 3
NO COOPERATION
S5Q1 = 0
FAILS BASIC ASSESSMENT2
PHYSIOTHERAPY:
No treatment
BODY POSITIONING4
2hr turning
BASIC ASSESSMENT =
- Cardiorespiratory unstable:
MAP < 60mmHg or
FiO2 > 60% or
PaO2/FiO2 < 200 or
RR > 30 bpm
- Neurologically unstable
- Acute surgery
-Temp > 40°C
BODY POSITIONING4
Active transfer bed to chair
Sitting out of bed
Standing with assist (≥1 pers)
UZLEUVEN ‘START TO MOVE' ASAP

Exercise training
Mobilisation – Body positioning
Active muscle (resistance) training Transcutaneous electrical muscle stimulation
Passive stretching and range
of motion exercise
MODALTIES FOR PHYSICAL TRAINING
UNSTABLE-BED RIDDEN-UNCOOPERATIVE
STABLE-COOPERATIVE

Daily Mobility Team Interventions (n=165)
‘Usual’ care: Physical Therapy on physician order (n=166)
Critically ill patient < 48 hours MV
Morris et al. Crit. Care Med. 2008: 36: 2238

Morris et al. Crit. Care Med. 2008: 36: 2238

0
5
10
15
20
First Out Bed Ventilator ICU LOS Hospital LOS
Usual Care Mobility Team
* #
*
Morris et al. Crit. Care Med. 2008;36: 2238
Days
(median)

Daily Physical and/or Occupational Therapy
‘Usual’ care: Physical and/or Occupational Therapy on physician order
Critically ill patient • < 72 hours MV and forecast of at least another 24hour on MV • Barthel Index > 70 (max 100) in 2 weeks before admission

Schweikert et al. Lancet 2009; 373:1874-1882

Contraindication to Rehabilitation Intervention
(43% of ICU days)
Sedation Shock Renal support
Out of ICU Acute Respiratory Distress Extubation
Cognitive alteration
Bourdin et al. Respir. Care 2010: 55:400

1 : score 5 questions: adequate response to 5 standardized orders
2 : FAILS = at least 1 risk factor present / 3 : if basic assessment failed, decrease to level 0 4 : safety: each activity should be deferred if severe adverse events (cv., resp. and subject. intolerance) occur during the intervention
Neurological or surgical or trauma condition does not allow transfer to chair
NO-LOW COOPERATION
S5Q1 < 3
MODERATE COOPERATION
S5Q1 ≥ 3
CLOSE TO FULL COOPERATION
S5Q1 ≥ 4/5
FULL COOPERATION
S5Q1 = 5
PHYSIOTHERAPY4
Passive range of motion
Passive bed cycling
NMES
BODY POSITIONING4
2hr turning
Fowler’s position
Splinting
PHYSIOTHERAPY4
Passive/Active range of motion
Resistance training arms and legs
Passive/Active leg and/or cycling in bed or chair
NMES
BODY POSITIONING4
2hr turning
Splinting
Upright sitting position in bed
Passive transfer bed to chair
PASSES BASIC ASSESSMENT3 +
PASSES BASIC ASSESSMENT3 +
PHYSIOTHERAPY4
Passive/Active range of motion
Resistance training arms and legs
Active leg and/or arm cycling in bed or chair
NMES
ADL
BODY POSITIONING4
2hr turning
Passive transfer bed to chair
Sitting out of bed
Standing with assist (2 ≥ pers)
PASSES BASIC ASSESSMENT3 +
PHYSIOTHERAPY4
Passive/Active range of motion
Resistance training arms and legs
Active leg and/or arm cycling in chair or bed
Walking (with assistance/frame)
NMES
ADL
PASSES BASIC ASSESSMENT3 +
LEVEL 0 LEVEL 5
FULL COOPERATION
S5Q1 = 5
PHYSIOTHERAPY4
Passive/Active range of motion
Resistance training arms and legs
Active leg and arm cycling in chair
Walking (with assistance)
NMES
ADL
BODY POSITIONING4
Active transfer bed to chair
Sitting out of bed
Standing
PASSES BASIC ASSESSMENT3 +
LEVEL 1 LEVEL 2 LEVEL 3 LEVEL 4
Obesity or neurological or surgical or trauma condition does not allow active transfer to chair (even if MRCsum ≥ 36)
MRCsum ≥ 36 +
BBS² Sit to stand = 0 +
BBS² Standing = 0 +
BBS² Sitting ≥ 1
MRCsum ≥ 48 +
BBS² Sit to stand ≥ 0 +
BBS² Standing ≥ 0 +
BBS² Sitting ≥ 2
MRCsum ≥ 48 +
BBS² Sit to stand ≥ 1 +
BBS² Standing ≥ 2 +
BBS² Sitting ≥ 3
NO COOPERATION
S5Q1 = 0
FAILS BASIC ASSESSMENT2
PHYSIOTHERAPY:
No treatment
BODY POSITIONING4
2hr turning
BASIC ASSESSMENT =
- Cardiorespiratory unstable:
MAP < 60mmHg or
FiO2 > 60% or
PaO2/FiO2 < 200 or
RR > 30 bpm
- Neurologically unstable
- Acute surgery
-Temp > 40°C
BODY POSITIONING4
Active transfer bed to chair
Sitting out of bed
Standing with assist (≥1 pers)
UZLEUVEN ‘START TO MOVE' ASAP

Exercise training
Mobilisation – Body positioning
Active muscle (resistance) training
Transcutaneous electrical muscle stimulation
Passive stretching and range of
of motion exercise
MODALTIES FOR PHYSICAL TRAINING
ACUTE-INSTABLE-UNCOOPERATIVE
CHRONIC-STABLE-COOPERATIVE

Effect of passive stretching on the wasting of muscle in the
critically ill
Griffiths et al. Nutrition 1995; 11:428-432

Protocol
1 leg 3 hours passive motion, 3 times per day, mainly ankle motion (25% passive stretch Ant.Tibialis)
1 leg flat position
twice daily passive
motion (5 min) both legs

140%
120%
100%
80%
60%
40%
20%
0%
1
2
3
4
5
% c
hang
e f
iber
are
a
Con1 Con2 CPM1 CPM2
Griffiths et al. Nutrition 1995; 11:428-432
less severe
p< 0.02 (more severe)


Passive stretching 10 h per day in addition to ‘Usual’ care
‘Usual’ care: respiratory physiotherapy mobilisation
7 critically ill patient • 0-3 days ICU and forecast of at least 10 days at the ICU
Study design
Llano-Diez et al. Crit Care 2012; 16:2499-2505

Llano-Diez et al. Crit Care 2012; 16:2499-2505


Cycle programme (passive/active) 20’ per day in addition to ‘Usual’ care
‘Usual’ care: respiratory physiotherapy mobilisation
Critically ill patient • ’5 days ICU and forecast of another 7 days at the ICU
Study design
Burtin et al. Crit Care Med 2009; 37:2499-2505

ICU and Hospital stay
0
5
10
15
20
25
30
35
40
45
ICU stay Hospital stay
Control
Treatment
Days

Burtin et al. Crit Care Med 2009
TR CO
0
100
200
300
400
500
600
p < 0.056M
WD
(m
)
143 [37-226] m 196 [126-329] m
43 m
TR CO
10
15
20
25
30 p < 0.05
SF
-36
PF
sco
re (
10-3
0)
15 [14-23] points 21 [18-23]
TR CO TR CO1.0
1.5
2.0
2.5
3.0
ICU discharge hospital discharge
QF
(N
/kg
)
p < 0.01
p < 0.05

Exercise training
Mobilisation – Body positioning
Active muscle (resistance) training
Transcutaneous electrical muscle stimulation
Passive range of motion exercise
MODALTIES FOR PHYSICAL TRAINING
ACUTE-INSTABLE-UNCOOPERATIVE
CHRONIC-STABLE-COOPERATIVE


100% 75- 99% 50- 75% 1- 50% 0% Segers et al. under review
DOES NMES ACHIEVE SUCCESSFULLY MUSCLE CONTRACTIONS IN ICU PATIENTS?

Responders Non-responders P-value
Gender (M/F) 14/8 8/14 .07
Age, yrs (mean +/-
SD )
56 (12) 63 (10) .07
APACHE II 25 (9) 27 (6) 0,523
Glasgow Coma
Scale
7 (3) 9 (3) 0,063
Intensity (mA) 64 (8) 68 (13) 0,297
BMI, kg/m² (mean
+/-SD)
25,4 (4,3) 25,6 (5,4) .916
Edema (n) n= 8 n= 16 0,015
Diagnosed with
sepsis
7 13 .037
Segers et al. under review

Mortality and ARDS

Iwashyna TJ AJRCCM 2012: 186:302

Unroe et al. Ann Intern Med 2010: 153:167
Health outcome at 3 months
Good
Fair
Poor





Ries et al. Ann.Intern Med. 1995; 122: 823

CONCLUSIONS I

CONCLUSIONS II

REACHING OUT BEYOND THE BORDERS:
THE CHALLENGE OF ADJUSTING THE SAILS


PULMONARY REHABILITATION TEAM


Acknowledgements ICU PHYSICAL THERAPY TEAM


CARDIOVASCULAR AND RESPIRATORY RESEARCH GROUP