
Research Article The Role Descriptions of Triage Nurse in...
7
Research Article The Role Descriptions of Triage Nurse in Emergency Department: A Delphi Study Mohsen Ebrahimi, 1 Amir Mirhaghi, 2 Reza Mazlom, 2 Abbas Heydari, 2 Asra Nassehi, 3 and Mojtaba Jafari 4 1 Department of Emergency Medicine, Imam Reza Hospital, Mashhad University of Medical Sciences, Mashhad 9137913316, Iran 2 Evidence-Based Caring Research Center, Department of Medical-Surgical Nursing, School of Nursing and Midwifery, Mashhad University of Medical Sciences, Mashhad 9137913199, Iran 3 Research Center for Health Services Management, Institute for Futures Studies in Health, Kerman University of Medical Sciences, Kerman 7616913555, Iran 4 Department of Medical-Surgical Nursing, Faculty of Nursing and Midwifery, Bam University of Medical Sciences, Khalije Fars Boulevard, Bam, Kerman 7661771967, Iran Correspondence should be addressed to Amir Mirhaghi; [email protected] Received 2 December 2015; Accepted 19 April 2016 Academic Editor: Toomas Timpka Copyright © 2016 Mohsen Ebrahimi et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Background. Triage nurses play a pivotal role in the emergency department. However some researchers have attempted to expand triage nurse’s role; remarkable discrepancies exist among scholarly communities. e aim was to develop a role description of triage nurse relying on the experts. Methods. A modified Delphi study consisting of 3 rounds was performed from March to October 2014. In the first round, an extensive review of the literature was conducted. Expert selection was conducted through a purposeful sample of 38 emergency medicine experts. Results. Response rates for the second and third rounds were 37% and 58%. Average age of panelists was (38.42 ± 5.94) years. irty-nine out of 54 items reached to the final round. Prioritizing had the higher agreement rate and least agreement on triage related interventions. Conclusion. Triage nursing as a relatively new role for nurses needs significant development to be practiced. Comprehensive educational programs and developmental research are required to support diagnostic and therapeutic interventions in triage practice by nurses. 1. Introduction Triage is defined as prioritizing or sorting the patients for the care and treatment that is due to shortage of the necessary resources in the emergency department (ED) [1]. Several studies have focused on the validity and reliability of triage scales [2, 3] and assessed agreement between nurses and physicians [4, 5]. Factors which affect triage practice were also studied [6]. Some studies have explored triage nurse’s daily job activities as well as how they decided to allocate patients to triage categories [7, 8] but researchers rarely try to describe triage nurse job. In response to overcrowding, some studies tried to explain increased efficiency of triage process regarding expanding physician and nurses roles in the triage room [9– 12] in which placing a senior emergency physician with the triage nurse reduced waiting times for nonemergent cases [10] so the concept of team triage has been evolved. Of course, it is clear that it is not possible for most EDs to have a senior emer- gency physician in the triage room. In order to customize patient flow more consciously and despite high satisfaction among staff and patient, initiating X-rays by triage nurses did not reduce transit times for patients with limb injuries in ED [13]. In contrast, some studies have indicated triage nurse ordering seems to be an effective intervention to reduce ED length of stay in patients with injuries [11]. erefore findings revealed that triage nurses’ role is challenging in the ED. Hindawi Publishing Corporation Scientifica Volume 2016, Article ID 5269815, 6 pages http://dx.doi.org/10.1155/2016/5269815
Transcript of Research Article The Role Descriptions of Triage Nurse in...

Research ArticleThe Role Descriptions of Triage Nurse in EmergencyDepartment: A Delphi Study
Mohsen Ebrahimi,1 Amir Mirhaghi,2 Reza Mazlom,2 Abbas Heydari,2
Asra Nassehi,3 and Mojtaba Jafari4
1Department of Emergency Medicine, Imam Reza Hospital, Mashhad University of Medical Sciences, Mashhad 9137913316, Iran2Evidence-Based Caring Research Center, Department of Medical-Surgical Nursing, School of Nursing and Midwifery,Mashhad University of Medical Sciences, Mashhad 9137913199, Iran3Research Center for Health Services Management, Institute for Futures Studies in Health, Kerman University of Medical Sciences,Kerman 7616913555, Iran4Department of Medical-Surgical Nursing, Faculty of Nursing and Midwifery, Bam University of Medical Sciences,Khalije Fars Boulevard, Bam, Kerman 7661771967, Iran
Correspondence should be addressed to Amir Mirhaghi; [email protected]
Received 2 December 2015; Accepted 19 April 2016
Academic Editor: Toomas Timpka
Copyright © 2016 Mohsen Ebrahimi et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Background. Triage nurses play a pivotal role in the emergency department. However some researchers have attempted to expandtriage nurse’s role; remarkable discrepancies exist among scholarly communities.The aimwas to develop a role description of triagenurse relying on the experts.Methods. Amodified Delphi study consisting of 3 rounds was performed fromMarch to October 2014.In the first round, an extensive review of the literature was conducted. Expert selection was conducted through a purposeful sampleof 38 emergency medicine experts. Results. Response rates for the second and third rounds were 37% and 58%. Average age ofpanelists was (38.42±5.94) years.Thirty-nine out of 54 items reached to the final round. Prioritizing had the higher agreement rateand least agreement on triage related interventions. Conclusion. Triage nursing as a relatively new role for nurses needs significantdevelopment to be practiced. Comprehensive educational programs and developmental research are required to support diagnosticand therapeutic interventions in triage practice by nurses.
1. Introduction
Triage is defined as prioritizing or sorting the patients for thecare and treatment that is due to shortage of the necessaryresources in the emergency department (ED) [1]. Severalstudies have focused on the validity and reliability of triagescales [2, 3] and assessed agreement between nurses andphysicians [4, 5]. Factorswhich affect triage practicewere alsostudied [6]. Some studies have explored triage nurse’s dailyjob activities as well as how they decided to allocate patientsto triage categories [7, 8] but researchers rarely try to describetriage nurse job.
In response to overcrowding, some studies tried toexplain increased efficiency of triage process regarding
expanding physician and nurses roles in the triage room [9–12] in which placing a senior emergency physician with thetriage nurse reducedwaiting times for nonemergent cases [10]so the concept of team triage has been evolved. Of course, it isclear that it is not possible formost EDs to have a senior emer-gency physician in the triage room. In order to customizepatient flow more consciously and despite high satisfactionamong staff and patient, initiating X-rays by triage nursesdid not reduce transit times for patients with limb injuriesin ED [13]. In contrast, some studies have indicated triagenurse ordering seems to be an effective intervention to reduceED length of stay in patients with injuries [11]. Thereforefindings revealed that triage nurses’ role is challenging in theED.
Hindawi Publishing CorporationScientificaVolume 2016, Article ID 5269815, 6 pageshttp://dx.doi.org/10.1155/2016/5269815

2 Scientifica
Role description is designed to guarantee the best possibleperformance by employees. In this way, the emergencyassociations have tried to develop position statement todefine triage nurse role in order to secure patient safetyin triage room. All associations have indicated that triagemust be performed at least by a registered nurse. Despiteremarkable discrepancies among statements, triage nursesare required to perform prioritizing of the patient care, takeeducational programs, and provide a safe environment as wellas interpersonal qualifications needed to fulfill this role [14–17]. However, only the Emergency Nurses Association (ENA)has comprehensively indicated several educational programs(CPR, ALS, ENPC, TNCC, GENE, CEN, and CPEN) in addi-tion to other triage educational programs [14]. Furthermoreinterpersonal qualifications including interpersonal, interdis-ciplinary, critical thinking, and communication skills as wellas accurate decisionmaking have been stated by several emer-gency associations [14–17]. However advanced practice nurs-ing roles have been recommended to improve patient flowthrough the ED [18]; advanced practice nursing roles havebeen rarely addressed by emergency associations. Even theRoyal College of Nursing has indicated triage related inter-ventions such as administrating analgesia [17], so it concludedthat role description of triage nurse suffered from lack of anintegrated approach. There is a strong possibility that it alsoaffects the reliability and validity of decisions among triagenurses in the ED.
Delphi method as an iterative process is to exploreimplicit information leading to differing judgments andsearch information which may generate a consensus onbehalf of the respondent group [19]. It has been employedby many nurse researchers in a wide variety of studies [20].So Delphi method was used to develop a role description oftriage nurse relying on the emergency medicine experts.
2. Materials and Methods
A modified Delphi study consisting of 3 rounds was per-formed from March to October 2014. Anonymity, iterationwith controlled feedback, and statistical consensus wereincluded in the Delphi method [20].
The study was approved by the Research Ethics Commit-tee at the Mashhad University of Medical Sciences. Confi-dentiality and anonymity of the experts’ participation weresecured. It was clearly defined that there is no obligation forthem to reply to the questionnaire.
In the first round, an extensive review of the literaturewas conducted [21]. Main question of the study was, what arethe attributes of the triage nurse role? Electronic databaseswere searched from inception to February 2014. Medline(Pubmed) and Scopus were searched without any additionalfilter. The keywords searched alone and in combination were“triage”, “nurse”, “role”, “Job”, “analysis”, “position”, and“statement”. Titles and abstracts were reviewed to identifythe relevant studies in the primary review. In the secondaryreview, articles were included only if the study defined role ofthe triage nurse. Studies were excluded if they have not beenapproved by emergency associations or colleges. Extendedreview was conducted to retrieve additional studies using
search engines. Data were extracted from relevant articlesbased on researchers’ agreement to identify attributes ofthe triage nurse contributing to the generation of itemspool to compose the primary questionnaire. Researcherscontinued to collect data until they reach a point of datasaturation. In the first round, selecting items for primaryquestionnaire were based on the three researchers’ consensus.Each researcher rated relevancy of items using Likert-typescale items (5: completely, 4: mostly, 3: moderately, 2: slightly,and 1: not at all). Average of rated responses was reported foreach item (Figure 1).
Expert selection was conducted through a purposefulsample of 38 emergency medicine experts and emergencynursing scholars. They were involved in emergency medicineand emergency nursing, so they were invited to take part.Experts were ED directors and physicians or nurses whohave known interest in triage practice and research. Potentialcontributors were retrieved from triage committees andassociations, authors of triage publications, and publishedarticles. All contributors were individually communicated byemail.
In the second round, an initial task list of triage nurserole was sent to the expert panelists in May 2014. Fifty-fouritems were included in the questionnaire. Items were relatedto the domains including basics, ethics, triage assessment,decision making, informing, competencies, environment,and documentation. Expert opinions on proposed tasks wereobtained by responses on a 5-point Likert scale (1: stronglydisagree, 2: disagree, 3: undecided, 4: agree, and 5: stronglyagree). Participants were asked to comment on any itemsas needed. Completed questionnaires were analyzed andagreement on each item was reported.
In the third round, a modified questionnaire was sent tothe expert panelists in July 2014. Participants were informedabout the opinion of other colleagues as well as theirs. Bothsecond- and third-round questionnaires were sent to all theindividuals regardless of their contributions in the secondround. Two reminders sent to the participants who did notreply. Reminders were sent at two-week interval.
Proportions and percentages were calculated for ordinaldata of Likert-type response scale. The data of each iterativeround was analyzed using MS Excel (2007). Only stronglyagree and agree responses to items were assumed as approveditems [22]. Each approved item which obtained a consensuslevel of 80% was identified for the next phase. The feedbackfor each round contained statistical result from the formerround, which included the consensus level reached for eachitem.
3. Results
Six expert panelists of 38were female. Average age of panelistswas (38.42± 5.94). Most participants had a medical degree inemergency medicine. All participants had an affiliation witha university hospital.
3.1. Round One. Twenty-three studies were chosen among353 articles which have been retrieved through search-ing databases and 7 were included in the final analysis.

Scientifica 3
330 obvious irrelevantarticles excluded in
primary review
20 articles excluded insecondary review13 irrelevant to triage practice5 irrelevant to role analysis2 with abstracts unavailable
7 articles used in thestudy
4 articles included inextended review
23 articles selected forsecondary review
353 articles identified (“triage”,“nurse”, “role”, “Job”, “analysis”,
“position”, and “statement”)
Figure 1: Study selection process.
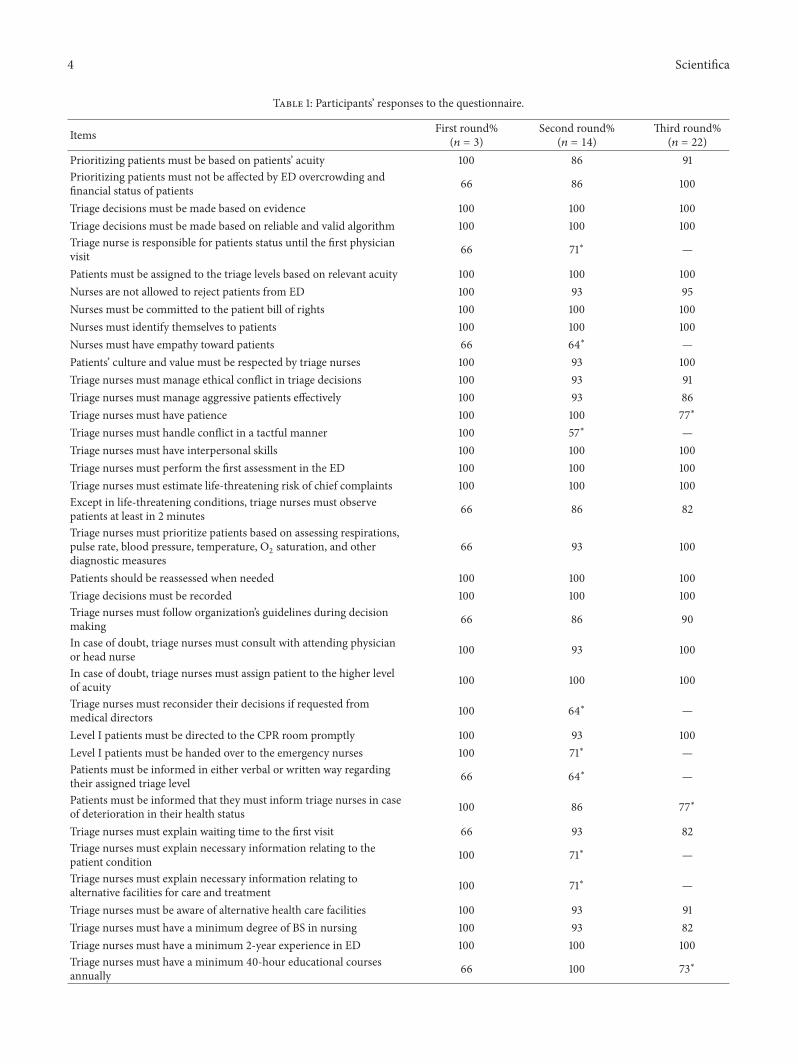
Sixty-two items were primarily extracted from the final stud-ies and redundant items were merged together, remaining 54items in the list (Table 1).
3.2. Round Two. Response rate for the second round was 31%(14/38). The number of items which remained in the end ofthe round was 43 (80%). Forty-one percent (22/54) of itemsachieved a complete consensus. 11 items were excluded sincethey did not reach a consensus level of 80%. Excluded itemsincluded legal issues (triage nurse responsibility for patientstatus and handing over level I patients to the emergencynurses and reconsidering their decisions); informing issues(informing patients about assigned triage level, their con-dition, outcomes, and potential care and treatment); ethicalissues (empathy and tactfulness characteristics); and otherissues (mandatory research participation and responsibilityfor triage room facilities and condition). Four new items wereproposed including diagnostic and therapeutic interventionsand added to the next round questionnaire (49 items). Four(7%) items were suggested to be edited lightly by participants(Table 1).
3.3. Round Three. Response rate for third round was 58%(22/38). The number of items which reached to the end ofthe round was 43 (88%). Fifty-five percent (27/49) of itemsachieved a complete consensus. Seven items were excludedsince they did not reach a consensus level of 80%. Excludeditems included ethical issues (having patience); competencyissues (continuing education); and other issues (diagnosticand therapeutic intervention and physician participations).
No item was proposed for the next round questionnaire (39items) (Table 1).
4. Discussion
Triage related interventions still need extensive developmentto be reliable enough to practice by triage nurses. Our resultsdid not reveal substantial agreement on triage nurse ordering(Table 1) which is consistent with most position statementson triage nurse role [14–17]. However some studies supporteddiagnostic interventions by triage nurse as well as advancedpractice nursing roles [11, 18, 23]; scientific evidence is limitedto ensure significant impact on patient flow in the emergencydepartment and efficiency [24]. Despite this inconsistency,expanding the role of triage nurse caused significant increasesin nurses’ satisfaction [12]. Further studies are needed todevelop more clarification of the contextual factors relatedto the interventions and investigate the impact of them onthe ED measures as the next generation of triage studies.Educational preparation and organized teamwork are essen-tially required for advanced practice role to be successfullyimplemented [25]. So prioritizing care and introducing fasttrack for patients were known as the fundamental role fortriage nurse which is unique to the emergency departmentand associated with desirable outcomes [24].
There is broad consensus that nurses are accountable forensuring safe triage practices [14–17]. Our results did notindicate a broad consensus among clinicians that physiciansroutinely perform triage in ED (Table 1). Several studiesdemonstrated that intelligent use of physicians in triagecauses substantial improvement in ED patient flow and
4 Scientifica
Table 1: Participants’ responses to the questionnaire.
Items First round%(𝑛 = 3)
Second round%(𝑛 = 14)
Third round%(𝑛 = 22)
Prioritizing patients must be based on patients’ acuity 100 86 91Prioritizing patients must not be affected by ED overcrowding andfinancial status of patients 66 86 100
Triage decisions must be made based on evidence 100 100 100Triage decisions must be made based on reliable and valid algorithm 100 100 100Triage nurse is responsible for patients status until the first physicianvisit 66 71∗ —
Patients must be assigned to the triage levels based on relevant acuity 100 100 100Nurses are not allowed to reject patients from ED 100 93 95Nurses must be committed to the patient bill of rights 100 100 100Nurses must identify themselves to patients 100 100 100Nurses must have empathy toward patients 66 64∗ —Patients’ culture and value must be respected by triage nurses 100 93 100Triage nurses must manage ethical conflict in triage decisions 100 93 91Triage nurses must manage aggressive patients effectively 100 93 86Triage nurses must have patience 100 100 77∗
Triage nurses must handle conflict in a tactful manner 100 57∗ —Triage nurses must have interpersonal skills 100 100 100Triage nurses must perform the first assessment in the ED 100 100 100Triage nurses must estimate life-threatening risk of chief complaints 100 100 100Except in life-threatening conditions, triage nurses must observepatients at least in 2 minutes 66 86 82
Triage nurses must prioritize patients based on assessing respirations,pulse rate, blood pressure, temperature, O
2saturation, and other
diagnostic measures66 93 100
Patients should be reassessed when needed 100 100 100Triage decisions must be recorded 100 100 100Triage nurses must follow organization’s guidelines during decisionmaking 66 86 90
In case of doubt, triage nurses must consult with attending physicianor head nurse 100 93 100
In case of doubt, triage nurses must assign patient to the higher levelof acuity 100 100 100
Triage nurses must reconsider their decisions if requested frommedical directors 100 64∗ —
Level I patients must be directed to the CPR room promptly 100 93 100Level I patients must be handed over to the emergency nurses 100 71∗ —Patients must be informed in either verbal or written way regardingtheir assigned triage level 66 64∗ —
Patients must be informed that they must inform triage nurses in caseof deterioration in their health status 100 86 77∗
Triage nurses must explain waiting time to the first visit 66 93 82Triage nurses must explain necessary information relating to thepatient condition 100 71∗ —
Triage nurses must explain necessary information relating toalternative facilities for care and treatment 100 71∗ —
Triage nurses must be aware of alternative health care facilities 100 93 91Triage nurses must have a minimum degree of BS in nursing 100 93 82Triage nurses must have a minimum 2-year experience in ED 100 100 100Triage nurses must have a minimum 40-hour educational coursesannually 66 100 73∗

Scientifica 5
Table 1: Continued.
Items First round%(𝑛 = 3)
Second round%(𝑛 = 14)
Third round%(𝑛 = 22)
Nurses must be knowledgeable about clinical semiology 100 100 100Nurses must be knowledgeable about advanced and basic adult lifesupport 100 86 82
Nurses must be knowledgeable about emergencies 100 100 100Nurses must be knowledgeable about gynecological, maternal,neonatal, children, and geriatrics emergencies 100 100 100
Nurses must be knowledgeable about outcome of disease 100 71∗ —Nurses must participate in at least one emergency research 100 50∗ —Triage roommust be somewhere between emergency department andsecurity room 100 100 100
Triage room must be easily recognizable for patients 100 100 100Triage room must have an appropriate view on entrance of ED 100 100 100Triage room must be accessible for ambulances, stretchers, andwheelchairs 100 100 100
Triage room must be at least 12 square meters 100 79∗ —Triage room must be equipped for professionals standard infectioncontrol precautions 100 93 82
Triage room must have alarm, telephone, and closed-circuit television 100 100 100Triage nurses are responsible for facilities of triage room 100 79∗ —Triage nurses are not permitted to leave the triage room, except forhanding over level I patients 100 86 77∗
Triage nurses must document triage assignments 100 93 100Triage nurses must report daily and monthly statistics of triage 100 93 100Triage nurses must consider hospital facilities when assigningpatients to triage level — Proposed 82
Diagnostic related interventions must be performed by triage nurses — Proposed 41∗
Therapeutic related interventions must be performed by triage nurses — Proposed 55∗
Physician must participate in prioritizing of patients in triage room — Proposed 77∗∗Less than consensus level of 80%.
results in shorter length of stay especially in overcrowdedconditions in the ED [24, 26]. Some studies suggested thatemergency nurse practitioners as an optimal choice havegreater impact on quality measures and financial indicesin ED [12, 27]. Comparison between the nurse practitionerand general practitioners demonstrated that the nurse prac-titioner can deal with patients effectively [12, 28] and they canbe assumed as superb candidates for expanded and extendedrole [29].
A limitation of the study is that the modified Delphimethod was used. Several modifications of the originalDelphi method have been described in the literature [30] andstandardized definitions of these modifications are not avail-able. Besides, panelists did not generally mention rationale incase of disagreement.
5. Conclusions
Triage nursing as a relatively new role for nurses is a challeng-ing role in a dynamic environment which needs significant
development to be practiced. Prioritizing is defined as thepivotal role for triage nurse. Comprehensive educational pro-grams and developmental research are required to supportdiagnostic and therapeutic interventions in triage practice bynurses.
Appendix
Search Strategies
Primary Search. Primary search included the following:(“triage” [MeSH Terms] OR “triage” [All Fields]) AND(“nurse’s role” [MeSHTerms] OR (“nurse’s” [All Fields] AND“role” [All Fields]) OR “nurse’s role” [All Fields] OR (“nurse”[All Fields] AND “role” [All Fields]) OR “nurse role” [AllFields]).
Competing Interests
The authors declare that there are no competing interests.
6 Scientifica
Acknowledgments
Many thanks are due to Dr. Mojtaba Jafari for his help. Alsothe authors gratefully acknowledge all participants for theircooperation.
References
[1] A. Mirhaghi, H. Kooshiar, H. Esmaeili, andM. Ebrahimi, “Out-comes for emergency severity index triage implementation inthe emergency department,” Journal of Clinical and DiagnosticResearch, vol. 9, no. 4, pp. OC04–OC07, 2015.
[2] N. Farrohknia, M. Castren, A. Ehrenberg et al., “Emergencydepartment triage scales and their components: a systematicreview of the scientific evidence,” Scandinavian Journal ofTrauma, Resuscitation and Emergency Medicine, vol. 19, article42, 2011.
[3] A. Mirhaghi, A. Heydari, R. Mazlom, and M. Ebrahimi, “Thereliability of the canadian triage and acuity scale:meta-analysis,”North American Journal of Medical Sciences, vol. 7, no. 7, pp.299–305, 2015.
[4] A. R. Allen, M. J. Spittal, C. Nicolas, E. Oakley, and G. L. Freed,“Accuracy and interrater reliability of paediatric emergencydepartment triage,” EmergencyMedicine Australasia, vol. 27, no.5, pp. 447–452, 2015.
[5] M. Ebrahimi, A. Heydari, R. Mazlom, and A. Mirhaghi, “Reli-ability of the Australasian triage scale: meta-analysis,” WorldJournal of Emergency Medicine, vol. 6, no. 2, pp. 94–99, 2015.
[6] A.-K. Andersson, M. Omberg, and M. Svedlund, “Triage in theemergency department—aqualitative study of the factorswhichnurses consider when making decisions,” Nursing in CriticalCare, vol. 11, no. 3, pp. 136–145, 2006.
[7] M. F. Gerdtz and T. K. Bucknall, “Triage nurses’ clinical decisionmaking. An observational study of urgency assessment,” Journalof Advanced Nursing, vol. 35, no. 4, pp. 550–561, 2001.
[8] M. Fry and G. Burr, “Current triage practice and influencesaffecting clinical decision-making in emergency departments inNSW, Australia,” Accident and Emergency Nursing, vol. 9, no. 4,pp. 227–234, 2001.
[9] B. R. Holroyd, M. J. Bullard, K. Latoszek et al., “Impact of atriage liaison physician on emergency department overcrowd-ing and throughput: a randomized controlled trial,” AcademicEmergency Medicine, vol. 14, no. 8, pp. 702–708, 2007.
[10] J. P. Travers and F. C. Y. Lee, “Avoiding prolonged waiting timeduring busy periods in the emergency department: is there arole for the senior emergency physician in triage?” EuropeanJournal of EmergencyMedicine, vol. 13, no. 6, pp. 342–348, 2006.
[11] B. H. Rowe, C. Villa-Roel, X. Guo et al., “The role of triage nurseordering on mitigating overcrowding in emergency depart-ments: a systematic review,”Academic EmergencyMedicine, vol.18, no. 12, pp. 1349–1357, 2011.
[12] S. Reveley, “The role of the triage nurse practitioner in generalmedical practice: an analysis of the role,” Journal of AdvancedNursing, vol. 28, no. 3, pp. 584–591, 1998.
[13] W. Parris, S. McCarthy, A.-M. Kelly, and S. Richardson, “Dotriage nurse-initiated X-rays for limb injuries reduce patienttransit time?” Accident and Emergency Nursing, vol. 5, no. 1, pp.14–15, 1997.
[14] The Emergncy Nurses Association, Triage Qualifications: Posi-tion Statement, ENA, Des Plaines, Ill, USA, 2011.
[15] The College of Emergency Nursing Australasia, Triage Nurse:Position Statement, CENA, Surrey Hills, Australia, 2009.
[16] The National Emergency Nurses Affiliation, Role of the TriageRegistered Nurse, ON NENA, Pembroke Pines, Fla, USA, 2011.
[17] The College of Emergency Medicine Clinical EffectivenessCommittee, Emergency Nurse Consultant Association, Facultyof Emergency Nursing, Royal College of Nursing EmergencyCareAssociation,Triage Position Statement, CEM, London,UK,2011.
[18] E. Elder, A. N. B. Johnston, and J. Crilly, “Review article:systematic review of three key strategies designed to improvepatient flow through the emergency department,” EmergencyMedicine Australasia, vol. 27, no. 5, pp. 394–404, 2015.
[19] F. Hasson, S. Keeney, andH.McKenna, “Research guidelines forthe Delphi survey technique,” Journal of Advanced Nursing, vol.32, no. 4, pp. 1008–1015, 2000.
[20] S. Keeney, F. Hasson, and H. P. McKenna, “A critical review ofthe Delphi technique as a research methodology for nursing,”International Journal of Nursing Studies, vol. 38, no. 2, pp. 195–200, 2001.
[21] J. Stewart, C. O’Halloran, P. Harrigan, J. A. Spencer, J. R.Barton, and S. J. Singleton, “Identifying appropriate tasks for thepreregistration year: modified Delphi technique,” British Medi-cal Journal, vol. 319, no. 7204, pp. 224–229, 1999.
[22] D. F. Polit, C. T. Beck, and S. V. Owen, “Focus on researchmethods: Is the CVI an acceptable indicator of content validity?Appraisal and recommendations,” Research in Nursing andHealth, vol. 30, no. 4, pp. 459–467, 2007.
[23] D. Pringle, “Expanding nurses’ scope of practice,” Nursingleadership, vol. 22, no. 2, pp. 1–4, 2009.
[24] S. Oredsson, H. Jonsson, J. Rognes et al., “A systematic review oftriage-related interventions to improve patient flow in emer-gency departments,” Scandinavian Journal of Trauma, Resusci-tation and Emergency Medicine, vol. 19, article 43, 2011.
[25] J. Considine, E. Lucas, R. Payne, M. Kropman, H. E. Stergiou,and H. Chiu, “Analysis of three advanced practice roles inemergency nursing,” Australasian Emergency Nursing Journal,vol. 15, no. 4, pp. 219–228, 2012.
[26] L. Burstrom, M. Nordberg, G. Ornung et al., “Physician-ledteam triage based on lean principles may be superior for effi-ciency and quality? A comparison of three emergency depart-ments with different triage models,” Scandinavian Journal ofTrauma, Resuscitation and Emergency Medicine, vol. 20, article57, 2012.
[27] D. Bahena and C. Andreoni, “Provider in triage: is this a placefor nurse practitioners?” Advanced Emergency Nursing Journal,vol. 35, no. 4, pp. 332–343, 2013.
[28] B. L. Lim, Z. R. Eunice Tay, A. Vasu, and W. J. KennethHeng, “Comparing triage evaluation of adult dyspneic patientsbetween emergency nurses and doctors using simulated scenar-ios,” International Emergency Nursing, vol. 21, no. 2, pp. 103–112,2013.
[29] M. Griffin and V. Melby, “Developing an advanced nursepractitioner service in emergency care: attitudes of nurses anddoctors,” Journal of Advanced Nursing, vol. 56, no. 3, pp. 292–301, 2006.
[30] R. Boulkedid, H. Abdoul, M. Loustau, O. Sibony, and C.Alberti, “Using and reporting the Delphi method for selectinghealthcare quality indicators: a systematic review,” PLoS ONE,vol. 6, no. 6, Article ID e20476, 2011.
Submit your manuscripts athttp://www.hindawi.com
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Breast CancerInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
HematologyAdvances in
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
ScientificaHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PediatricsInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Advances in
Urology
HepatologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
InflammationInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Surgery Research and Practice
Current Gerontology& Geriatrics Research
Hindawi Publishing Corporationhttp://www.hindawi.com
Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
NursingResearch and Practice
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com
HypertensionInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Prostate CancerHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Surgical OncologyInternational Journal of


















