ความรู้และทักษะด้านการ Triage...
50
ความรู้และทักษะด้านการ Triage ผู้ป่วยนอก รศ.นพ. ประสิทธิ์ วุฒิสุทธิเมธาวี ภาควิชาเวชศาสตร์ฉุกเฉิน คณะแพทยศาสตร์ มหาวิทยาลัยสงขลานครินทร์
Transcript of ความรู้และทักษะด้านการ Triage...

ความรู้และทักษะด้านการ
Triage ผู้ป่วยนอก
รศ.นพ. ประสิทธ์ิ วุฒิสุทธิเมธาวี
ภาควิชาเวชศาสตร์ฉุกเฉิน คณะแพทยศาสตร์
มหาวิทยาลัยสงขลานครินทร์


การคัดแยกผู้ป่วย • เริ่มต้นสมัยสงคราม นโปเลียน
Ge#ng the right pa-ent to the right resources at the right place and the right -me

Baron Dominique Jean Larrey (1766-1842)
'The worthiest man I have ever met'


Triage
• ESI Triage • Re-triage protocol • Educa-on • Monitoring • Results • Research

มาตรฐานการ Triage
• ผู้ป่วยทุกรายต้องได้รับการประเมินจาก triage nurse
• ต้องมีการคัดแยกผู้ป่วย และให้การรักษาตามลำดับความเร่งด่วน
• ให้การปฐมพยาบาลเบื้องต้น
• Support ผู้ป่วยและญาติ ทั้งทางด้านร่างกายและจิตใจ

Triage
! undertriage
Small SD et al. Acad Emerg Med 1999
3 level VS 5 level

Triage 2 level
emergent
Non-emergent
3 level
emergent
urgent
Non-emergent
4 level
immediate
emergent
urgent
Non-emergent
5 level
immediate
emergent
urgent
Acute non- emergent
Chronic non-emergent
CTAS ESI ATS

Triage
Australian Triage Scale
(1968)
Emergency Severity
Index(ESI)
Canadian Triage Acuity Scale(CTAS)
Cape Triage Scale
Patient Acuity Scale(Singapore)
Taiwan Triage Scale (TTS)
Manchester Triage
Scale(MTS)

CTAS ESI ATS
U.K., and utilizes a presentational flow-chart basedformat (Manchester Triage Group, 1997). Nurses firstidentify the patient's chief complaint, and thenchoose one of 52 flow charts to conduct a structuredinterview and then assign a triage level from 1(immediate care needed) to 5 (care within 4 hours).The system has been endorsed by the Accident andEmergency Nurses Association (Zimmermann, 2001).There is limited research on the Manchester system.In one study of reliability, triage nurse ratings werecompared retrospectively to senior medical staffratings; agreement was only fair to moderate(Goodacre, Gillett, Harris & Houlihan, 1999).
The Canadian Triage and Acuity Scale (CTAS) wasdeveloped by a group of Canadian emergencyphysicians. (Beveridge & Ducharme, 1997; CanadianAssociation for Emergency Physicians [CAEP], 2002).The National Emergency Nurses' Affiliation, Inc.(NENA) and the Canadian Association forEmergency Physicians (CAEP) have endorsed theCTAS as the national standard for ED triage.Canadian hospitals are required to submit data tothe Canadian government, including CTAS ratings,on all ED visits. The Canadian five-level scale hasalso been shown to have good interrater reliabilityin studies in which clinicians rated the acuity ofwritten scenarios taken from actual patient cases
(Beveridge, Ducharme, Janes, Beaulieu & Walter,1999; Manos, Petrie, Beveridge, Walter & Ducharme,2002).
History of the EmergencySeverity Index (ESI)The Emergency Severity Index (ESI) is a five-leveltriage scale developed by ED physicians RichardWuerz and David Eitel in the United States (Gilboyet al., 1999; Wuerz, Milne, Eitel, Travers & Gilboy,2000). The two originators believed that a principalrole for an emergency department triage instrumentis to facilitate the prioritization of patients based onthe urgency of the patients' conditions. The triagenurse determines priority by posing the question,“Who should be seen first?” Drs. Wuerz and Eitelrealized, however, that when more than one top-priority patient is present simultaneously, theoperating question becomes, “How long caneverybody wait?” The ESI was developed around anew conceptual model of ED triage. In addition toasking which patient should be seen first, triagenurses use the ESI to also consider what resourcesare necessary to get the patient through to an EDdisposition. The ESI retains the traditionalfoundation of patient urgency, and then seeks to
Chapter 2.Triage Acuity Systems
9
Patient should be seenSystem Countries Levels by provider within
Australasian Triage Scale (ATS) Australia 1 - Resuscitation Level 1 - 0 minutes(formerly National New Zealand 2 - Emergency Level 2 - 10 minutesTriage Scale of Australia) 3 - Urgent Level 3 - 30 minutes
4 - Semi-urgent Level 4 - 60 minutes5 - Nonurgent Level 5 - 120 minutes
Manchester England 1 - Immediate (red) Level 1 - 0 minutesScotland 2 - Very urgent (orange) Level 2 - 10 minutes
3 - Urgent (yellow) Level 3 - 60 minutes4 - Standard (green) Level 4 - 120 minutes5 - Nonurgent (blue) Level 5 - 240 minutes
Canadian Triage and Acuity Scale Canada 1 - Resuscitation Level 1 - 0 minutes(CTAS) 2 - Emergent Level 2 - 15 minute
3 - Urgent Level 3 - 30 minutes4 - Less urgent Level 4 - 60 minutes5 - Nonurgent Level 5 - 120 minutes
(Australasian College for Emergency Medicine, 2002; Canadian Association of Emergency Physicians, 2002;Manchester Triage Group, 1997)
Table 2-2 Five-level Triage Systems





สงขลานครินทร์เวชสาร ปีที่ 28 ฉบับที่ 4 ก.ค.-ส.ค. 2553 Songkla Med J Vol. 28 No. 4 Jul-Aug 2010Or
igina
l Arti
cle
205
การคัดกรองผู้ป่วยด้วยเกณฑ์คัดแยกและมาตรความเฉียบพลันแคนาดา ในแผนกฉุกเฉินโรงพยาบาลสงขลานครินทร์: การศึกษานำร่อง
ภุมรินทร์ แซล่ิ่มประสิทธิ์ วุฒิสุทธิเมธาวี
Canadian triage and acuity scale in the Emergency Department at Songklanagarind Hospital: preliminary studyPhummarin Saelim, Prasit WuthisuthimethaweeDepartment of Emergency Medicine, Faculty of Medicine, Prince of Songkla University, Hat Yai, Songkhla, 90110, ThailandE-mail: [email protected] Med J 2010;28(4):205-211
บทคัดย่อ:วตัถปุระสงค:์ เพือ่เปรยีบเทยีบความสมัพนัธร์ะหวา่งระดบัการคดักรองดว้ยเกณฑค์ดัแยกและมาตรความเฉยีบพลนัแคนาดา (Canadian Triage and Acuity Scale: CTAS) กบัคา่ใชจ้า่ยของผูป้ว่ยและระยะเวลารอตรวจ ซึง่สามารถบง่ชี้ความแม่นยำของเกณฑ์การคัดแยกผู้ป่วยวสัดแุละวธิกีาร: เกบ็ขอ้มลูไปขา้งหนา้ ตัง้แตว่นัที ่1 เมษายน ถงึ วนัที ่6 กรกฎาคม พ.ศ. 2551 ในผูป้ว่ยทีเ่ขา้รบัการตรวจทีแ่ผนกฉกุเฉนิ และไดร้บัการคดักรองดว้ย CTAS (แบง่เปน็ระดบั I-V ตามความรนุแรง) โดยแพทยใ์ชท้นุและแพทย์ประจำบา้นสาขาเวชศาสตรฉ์กุเฉนิ โดยพจิารณาความสมัพนัธร์ะหวา่งระดบัการคดักรองกบัคา่ใชจ้า่ยในโรงพยาบาล และระยะเวลารอตรวจของผู้ป่วยผลการศกึษา: ผู้ป่วยที่ได้รับการคัดกรองทั้งหมด 789 ราย ค่ามัธยฐานของค่าใช้จ่าย CTAS ระดับ I 2,576 บาท CTAS ระดับ II 745 บาท CTAS ระดับ III 155 บาท CTAS ระดับ IV 124 บาท และ CTAS ระดับ V 80 บาท ค่ามัธยฐานของระยะเวลารอรอตรวจ CTAS ระดับ I 9 นาที CTAS ระดับ II 12 นาที CTAS ระดบั III 18 นาท ีCTAS ระดบั IV 32 นาท ีและ CTAS ระดบั V 42 นาท ี เมือ่วเิคราะหด์ว้ยสถติ ิKruskal-Wallis test !"ว่ามีความแตกต่างกันอย่างมีนัยสำคัญทางสถิติในแต่ละระดับของการคัดกรอง ทั้งในแง่ค่าใช้จ่ายและระยะเวลารอตรวจ
ภาควิชาเวชศาสตร์ฉุกเฉิน คณะแพทยศาสตร์ มหาวิทยาลัยสงขลานครินทร์ อ.หาดใหญ่ จ.สงขลา 90110รับต้นฉบับวันที่ 19 มีนาคม 2553 รับลงตีพิมพ์วันที่ 3 กันยายน 2553
สงขลานครินทร์เวชสาร ปีที่ 28 ฉบับที่ 4 ก.ค.-ส.ค. 2553 Songkla Med J Vol. 28 No. 4 Jul-Aug 2010
Origina
l Article
205
การคัดกรองผู้ป่วยด้วยเกณฑ์คัดแยกและมาตรความเฉียบพลันแคนาดา ในแผนกฉุกเฉินโรงพยาบาลสงขลานครินทร์: การศึกษานำร่อง
ภุมรินทร์ แซ่ลิ่มประสิทธิ์ วุฒิสุทธิเมธาวี
Canadian triage and acuity scale in the Emergency Department at Songklanagarind Hospital: preliminary studyPhummarin Saelim, Prasit WuthisuthimethaweeDepartment of Emergency Medicine, Faculty of Medicine, Prince of Songkla University, Hat Yai, Songkhla, 90110, ThailandE-mail: [email protected] Med J 2010;28(4):205-211
บทคัดย่อ:วตัถปุระสงค:์ เพือ่เปรยีบเทยีบความสมัพนัธร์ะหวา่งระดบัการคดักรองดว้ยเกณฑค์ดัแยกและมาตรความเฉยีบพลนัแคนาดา (Canadian Triage and Acuity Scale: CTAS) กบัคา่ใชจ้า่ยของผูป้ว่ยและระยะเวลารอตรวจ ซึง่สามารถบง่ชี้ความแม่นยำของเกณฑ์การคัดแยกผู้ป่วยวสัดแุละวธิกีาร: เกบ็ขอ้มลูไปขา้งหนา้ ตัง้แตว่นัที ่1 เมษายน ถงึ วนัที ่6 กรกฎาคม พ.ศ. 2551 ในผูป้ว่ยทีเ่ขา้รบัการตรวจทีแ่ผนกฉกุเฉนิ และไดร้บัการคดักรองดว้ย CTAS (แบง่เปน็ระดบั I-V ตามความรนุแรง) โดยแพทยใ์ชท้นุและแพทย์ประจำบา้นสาขาเวชศาสตรฉ์กุเฉนิ โดยพจิารณาความสมัพนัธร์ะหวา่งระดบัการคดักรองกบัคา่ใชจ้า่ยในโรงพยาบาล และระยะเวลารอตรวจของผู้ป่วยผลการศึกษา: ผู้ป่วยที่ได้รับการคัดกรองทั้งหมด 789 ราย ค่ามัธยฐานของค่าใช้จ่าย CTAS ระดับ I 2,576 บาท CTAS ระดับ II 745 บาท CTAS ระดับ III 155 บาท CTAS ระดับ IV 124 บาท และ CTAS ระดับ V 80 บาท ค่ามัธยฐานของระยะเวลารอรอตรวจ CTAS ระดับ I 9 นาที CTAS ระดับ II 12 นาที CTAS ระดบั III 18 นาท ีCTAS ระดบั IV 32 นาท ีและ CTAS ระดบั V 42 นาท ี เมือ่วเิคราะหด์ว้ยสถติ ิKruskal-Wallis test !"ว่ามีความแตกต่างกันอย่างมีนัยสำคัญทางสถิติในแต่ละระดับของการคัดกรอง ทั้งในแง่ค่าใช้จ่ายและระยะเวลารอตรวจ
ภาควิชาเวชศาสตร์ฉุกเฉิน คณะแพทยศาสตร์ มหาวิทยาลัยสงขลานครินทร์ อ.หาดใหญ่ จ.สงขลา 90110รับต้นฉบับวันที่ 19 มีนาคม 2553 รับลงตีพิมพ์วันที่ 3 กันยายน 2553
สงขลานครินทร์เวชสาร ปีที่ 28 ฉบับที่ 4 ก.ค.-ส.ค. 2553206
ภุมรินทร์ แซ่ลิ่ม และคณะ เกณฑ์การคัดกรองในแผนกฉกุเฉิน
สรปุ: การคดักรองผูป้ว่ยดว้ยเกณฑค์ดัแยกและมาตรความเฉยีบพลนัแคนาดามคีวามสมัพนัธอ์ยา่งมนียัสำคญัทางสถติกิบัค่าใช้จ่ายในการรักษาพยาบาลและระยะเวลารอตรวจในการคัดกรองผู้ป่วยฉุกเฉินในโรงพยาบาลสงขลานครินทร์
คำสำคญั: การคัดกรอง, เกณฑ์คัดแยกและมาตรความเฉียบพลันแคนาดา, ค่าใช้จ่าย, แผนกฉุกเฉิน
Abstract:Objectives: To determine the relationship between expense and waiting time with using Canadian Triage and Acuity Scale (CTAS) level, to evaluate the validity of the CTAS triage that was implemented in Emergency Department (ED)Materials and methods: This was a prospective observational study conducted between April 1st and July 6th, 2008. Patients who were triaged by emergency medicine residents at our institution using CTAS (level I-V) were included in the study. The correlations between CTAS levels with waiting times and hospital expense of the patient was calculated.Results: Seven hundred and eighty nine patients were enrolled. The median expenses associated with each CTAS level were CTAS level I 2,576 Baht, CTAS level II 745 Baht, CTAS level III 155 Baht, CTAS level IV 124 Baht and CTAS level V 80 Baht. The median waiting times were CTAS level I 9 minutes, CTAS level II 12 minutes, CTAS level III 18 minutes, CTAS level IV 32 minutes and CTAS level V 42 minutes. For both variables, the differences between groups were statistically significant as determined by the Kruskal-Wallis test in both variables.Conclusion: CTAS is significantly related to the cost of treatment and the waiting time in patients who visited the ED.
Key words: triage, CTAS, cost, Emergency Department
บทนำ โรงพยาบาลสงขลานครินทร์เป็นโรงพยาบาลระดับตติยภูมิ โดยมีผู้มารับบริการที่แผนกฉุกเฉินประมาณ 48,000-60,000 รายต่อปี และมีแนวโน้มเพิ่มขึ้นเรื่อยๆ ในขณะที่ทรัพยากรทางการแพทย์และบุคลากรทางการแพทย์มีจำกัด ทำให้ผู้ป่วยจำนวนหนึ่งไม่ได้รับการบริการในเวลาที่กำหนด ส่งผลให้ประสิทธิภาพทางการรักษาไม่เป็นไปตามที่พึงประสงค์ การคัดกรอง (triage) คือ การประเมินผู้ป่วยอย่างรวดเรว็ใช้เวลาประมาณ 2-5 นาท ีเพือ่แบง่ผูป้ว่ยเปน็กลุม่
ตามความเร่งด่วนและผู้ป่วยสามารถได้รับการบริการในเวลาอันเหมาะสม นอกจากนี้ยังสามารถลดความวิตกกังวล ความเครียดของผู้ป่วยและญาติลงได้1 แต่ในปจัจบุนัยงัไมม่รีะบบการคดักรองผูป้ว่ยทีเ่ปน็มาตรฐานสำหรับทุกโรงพยาบาลในประเทศไทย มีเพียงการศึกษา ข้อมูลผู้มารับบริการ และการจัดทำระบบคัดกรองผู้ป่วยของโรงพยาบาลแต่ละแห่งเท่านั้น เช่น โรงพยาบาลรามาธิบดี มีการคัดกรอง 4 ระดับ2
Canadian Triage and Acuity Scale (CTAS) เปน็ระบบคดักรองผูป้ว่ยทีถ่กูคดิขึน้และพฒันาโดย Beveridge

ข้อดี
• ถูกต้อง • แม่นยำ • มาตรฐานที่เข้าใจตรงกัน
• ประเมินจากอาการผู้ป่วยเป็นสำคัญ
• ประเมินจาก physiologic parameters

ข้อเสีย
• ยุ่งยาก ซับซ้อน
• หลากหลายตัวแปร • ใช้งานยาก ยกเว้นทำเป็นโปรแกรม computer
• ใช้เวลามาก

Advancing Excellence in Health Care • www.ahrq.gov
Agency for Healthcare Research and Quality
Emergency SeverityIndex, Version 4:ImplementationHandbook
Emergency SeverityIndex, Version 4:ImplementationHandbook


Triage ที่ดี
• ง่าย • รวดเร็ว • ถูกต้อง แม่นยำ

มาตรฐานตรงกัน
• Intrarater reliability
– มาตรฐานในคนเดียวกัน
• Interrater reliability
– มาตรฐานระหว่างบุคคล

Advancing Excellence in Health Care • www.ahrq.gov
Agency for Healthcare Research and Quality
Emergency SeverityIndex, Version 4:ImplementationHandbook
Emergency SeverityIndex, Version 4:ImplementationHandbook

ข้อดี
• ง่าย • รวดเร็ว • ไม่ซับซ้อน

ข้อเสีย
• อาศัยประสบการณ์สูง • ความหมายของทรัพยากรในแต่ละพื้นที่อาจแตกต่างกัน
• Interrater reliability
– พยาบาล VS พยาบาล
– พยาบาล VS หมอ

The Emergency Severity Index (ESI) is a simple touse, five-level triage instrument that categorizesemergency department patients by evaluating bothpatient acuity and resources. Initially the triagenurse assesses only acuity level. If a patient does notmeet high acuity level criteria (ESI level 1 or 2), thetriage nurse then evaluates expected resource needsto help determine a triage level (ESI level 3, 4, or 5).Inclusion of resource needs in the triage rating is aunique feature of the ESI in comparison with othertriage systems. Acuity is determined by the stabilityof vital functions and potential for life, limb, ororgan threat. The triage nurse estimates resourceneeds based on previous experience with patientspresenting with similar injuries or complaints.Resource needs are defined as the number ofresources a patient is expected to consume in orderfor a disposition decision to be reached. Onceappropriately oriented to the algorithm, the triagenurse will be able to rapidly and accurately triagepatients into one of five explicitly defined andmutually exclusive levels. The ESI providesemergency departments with a valid, reliable triagesystem (Eitel, Travers, Rosenau, Gilboy & Wuerz,2003; Travers, Waller, Bowling, Flowers & Tintinalli,2002; Wuerz, Travers, Gilboy, Eitel, Rosenau &Yazhari, 2001; Tanabe, Gimbel, Yarnold, Kyriacou, &Adams, 2004; Tanabe, Gimbel, Yarnold, & Adams,2004).
In this chapter, we present a step-by-step descriptionof how to triage with the ESI algorithm. Subsequentchapters explain key concepts in more detail andprovide numerous examples to clarify the finerpoints of ESI application.
Algorithms are frequently used in emergency care.Most emergency clinicians are familiar with thealgorithms used in courses such as Basic LifeSupport, Advanced Cardiac Life Support, and theTrauma Nursing Core Course. These courses presenta step-by-step approach to clinical decision makingthat the clinician is able to internalize with practice.Each step of the algorithm tells the user whatquestions to ask or what information to gather.Based on the data or answers obtained, a decision ismade and the algorithm directs the user to the nextstep, and ultimately to an outcome.
Triage with the ESI algorithm requires theexperienced ED nurse to start at the top of the
algorithm. A conceptual overview of the ESIalgorithm is presented in Figure 3-1 to illustrate themajor ESI decision points. The actual ESI algorithmis described in detail later in this chapter (Figure 3-1a). The algorithm uses four decision points (A, B,C, and D) to sort patients into one of the five triagelevels (Figure 3-1). With practice, the triage nursewill be able to rapidly move from one ESI decisionpoint to the next.
The four decision points depicted in the conceptualalgorithm (Figure 3-1) are critical to accurate andreliable application of ESI. Figure 3-1 shows the fourdecision points reduced to four key questions:
A. Is this patient dying?
B. Is this a patient who shouldn't wait?
15
Chapter 3. Introduction to the EmergencySeverity Index
patient dying? 1
5 4
3
2
shouldn’t wait?
how many resources?
none one many
vital signs
Figure 3-1. Emergency Severity Index ConceptualAlgorithm, v. 4
yes
yes
no
no
no
consider
©ESI Triage Research Team, 2004. Reproduced withpermission.
A
B
C
D

C. How many resources will this patient need?
D. What are the patient's vital signs?
The answers to the questions guide the user to thecorrect triage level.
Decision Point A: Is the PatientDying?Simply stated, at decision point A (Figure 3-2) thetriage nurse asks if this patient is dying. If theanswer is “yes,” the triage process is complete andthe patient is automatically triaged as ESI level 1. A“no” answer moves the user to the next step in thealgorithm, decision point B.
The following question is used to determinewhether the patient is dying (conceptual algorithm):Does the patient require immediate life-savingintervention? The following questions are helpful indetermining whether the patient meets level-1criteria:
Chapter 3. Introduction to the Emergency Severity Index
16
high risk situation?or
confused/lethargic/disoriented?or
severe pain/distress?
danger zonevitals?
<3 m >180 >50
3 m-3y >160 >40
3-8 y >140 >30
>8y >100 >20
how many different resources are needed?
none one many
1
2
5 4
3
A
B
C
D
requires immediate life-saving intervention?
yes
no
no
yes
consider
RRHR
SaO
2<92
%
A
Figure 3-1a. ESI Triage Algorithm
©ESI Triage Research Team, 2004. Reproduced with permission.
A. Immediate life-saving intervention required: airway, emergency medications, orother hemodynamic interventions (IV, supplemental O2, monitor, ECG or labs DONOT count); and/or any of the following clinical conditions: intubated, apneic,pulseless, severe respiratory distress, SPO2<90, acute mental status changes, orunresponsive.
Unresponsiveness is defined as a patient that is either:(1) nonverbal and not following commands (acutely); or (2) requires noxious stimulus (P or U on AVPU) scale.
B. High risk situation is a patient you would put in your last open bed.
Severe pain/distress is determined by clinical observation and/or patient rating ofgreater than or equal to 7 on 0-10 pain scale.
C. Resources: Count the number of different types of resources, not the individual tests or x-rays (examples: CBC, electrolytes and coags equals one resource; CBCplus chest x-ray equals two resources).
Resources
• Labs (blood, urine)• ECG, X-rays• CT-MRI-ultrasound-angiography
• IV fluids (hydration)
• IV or IM or nebulized medications
• Specialty consultation
• Simple procedure =1(lac repair, foley cath)
• Complex procedure =2(conscious sedation)
Not Resources
• History & physical (including pelvic)• Point-of-care testing
• Saline or heplock
• PO medications• Tetanus immunization• Prescription refills
• Phone call to PCP
• Simple wound care (dressings, recheck)
• Crutches, splints, slings
D. Danger Zone Vital SignsConsider uptriage to ESI 2 if any vital sign criterion is exceeded.
Pediatric Fever Considerations1 to 28 days of age: assign at least ESI 2 if temp >38.0 C (100.4F)
1-3 months of age: consider assigning ESI 2 if temp >38.0 C (100.4F)
3 months to 3 yrs of age: consider assigning ESI 3 if: temp >39.0 C (102.2 F), or incomplete immunizations, or no obvious source of fever
© ESI Triage Research Team, 2004 – (Refer to teaching materials for further clarification)
Figure 3-2. Decision Point A: Is the Patient Dying?
1A
requires immediate life-saving intervention?
yes
no
A

C. How many resources will this patient need?
D. What are the patient's vital signs?
The answers to the questions guide the user to thecorrect triage level.
Decision Point A: Is the PatientDying?Simply stated, at decision point A (Figure 3-2) thetriage nurse asks if this patient is dying. If theanswer is “yes,” the triage process is complete andthe patient is automatically triaged as ESI level 1. A“no” answer moves the user to the next step in thealgorithm, decision point B.
The following question is used to determinewhether the patient is dying (conceptual algorithm):Does the patient require immediate life-savingintervention? The following questions are helpful indetermining whether the patient meets level-1criteria:
Chapter 3. Introduction to the Emergency Severity Index
16
high risk situation?or
confused/lethargic/disoriented?or
severe pain/distress?
danger zonevitals?
<3 m >180 >50
3 m-3y >160 >40
3-8 y >140 >30
>8y >100 >20
how many different resources are needed?
none one many
1
2
5 4
3
A
B
C
D
requires immediate life-saving intervention?
yes
no
no
yes
consider
RRHR
SaO
2<92
%
A
Figure 3-1a. ESI Triage Algorithm
©ESI Triage Research Team, 2004. Reproduced with permission.
A. Immediate life-saving intervention required: airway, emergency medications, orother hemodynamic interventions (IV, supplemental O2, monitor, ECG or labs DONOT count); and/or any of the following clinical conditions: intubated, apneic,pulseless, severe respiratory distress, SPO2<90, acute mental status changes, orunresponsive.
Unresponsiveness is defined as a patient that is either:(1) nonverbal and not following commands (acutely); or (2) requires noxious stimulus (P or U on AVPU) scale.
B. High risk situation is a patient you would put in your last open bed.
Severe pain/distress is determined by clinical observation and/or patient rating ofgreater than or equal to 7 on 0-10 pain scale.
C. Resources: Count the number of different types of resources, not the individual tests or x-rays (examples: CBC, electrolytes and coags equals one resource; CBCplus chest x-ray equals two resources).
Resources
• Labs (blood, urine)• ECG, X-rays• CT-MRI-ultrasound-angiography
• IV fluids (hydration)
• IV or IM or nebulized medications
• Specialty consultation
• Simple procedure =1(lac repair, foley cath)
• Complex procedure =2(conscious sedation)
Not Resources
• History & physical (including pelvic)• Point-of-care testing
• Saline or heplock
• PO medications• Tetanus immunization• Prescription refills
• Phone call to PCP
• Simple wound care (dressings, recheck)
• Crutches, splints, slings
D. Danger Zone Vital SignsConsider uptriage to ESI 2 if any vital sign criterion is exceeded.
Pediatric Fever Considerations1 to 28 days of age: assign at least ESI 2 if temp >38.0 C (100.4F)
1-3 months of age: consider assigning ESI 2 if temp >38.0 C (100.4F)
3 months to 3 yrs of age: consider assigning ESI 3 if: temp >39.0 C (102.2 F), or incomplete immunizations, or no obvious source of fever
© ESI Triage Research Team, 2004 – (Refer to teaching materials for further clarification)
Figure 3-2. Decision Point A: Is the Patient Dying?
1A
requires immediate life-saving intervention?
yes
no
A

Chapter 3. Introduction to the Emergency Severity Index
17
Life-saving Not life-saving
Airway/breathing • BVM ventilation Oxygen administration• Intubation • nasal cannula • Surgical airway • non-rebreather• Emergent CPAP• Emergent BiPAP
Electrical Therapy • Defibrillation Cardiac Monitor• Emergent cardioversion • External pacing
Procedures • Chest needle decompression Diagnostic Tests• Pericardiocentesis • ECG• Open thoracotomy • Labs• Intraoseous access • Ultrasound
• FAST (Focused abdominal scan for trauma)
Hemodynamics • Significant IV fluid resuscitation • IV access• Blood administration • Saline lock for medications• Control of major bleeding
Medications • Naloxone • ASA• D50 • IV nitroglycerin• Dopamine • Antibiotics • Atropine • Heparin• Adenocard • Pain medications
• Respiratory treatments with beta agonists
Table 3-1. Immediate Life-saving Interventions
• Does the patient require an immediate airway,medication, or other hemodynamicintervention?
• Does the patient meet any of the followingcriteria: already intubated, apneic, pulseless,severe respiratory distress, SpO2 < 90 percent,acute mental status changes, or unresponsive?
Research has demonstrated that the triage nurse isable to accurately predict the need for immediateinterventions (Tanabe et al., in press). Table 3-1 listsinterventions that are considered life saving andthose that are not, for the purposes of ESI triage.
Interventions not considered life saving includesome interventions that are diagnostic ortherapeutic, but none that would “save a life.” Life-saving interventions are aimed at securing anairway, maintaining breathing, or supportingcirculation. Listed below are additional questions
that may be helpful in determining whether thepatient requires a life-saving intervention.
• Does this patient have a patent airway?
• Is the patient breathing?
• Does the patient have a pulse?
• Is the nurse concerned about the pulse rate,rhythm, and quality?
• Was this patient intubated pre-hospital becauseof concerns about the patient's ability tomaintain a patent airway, spontaneously breathe,or maintain oxygen saturation?
• Is the nurse concerned about this patient's abilityto deliver adequate oxygen to the tissues?
The ESI level-1 patient always presents to theemergency department with an unstable condition.Because the patient could die without immediate

and dizzy patient with a heart rate of 30 or 200.Although this change may not affect a large numberof patients, it will result in the accuratecategorization of the most acutely ill patients. Priorto v. 4, triage nurses were frequently confrontedwith two distinct levels of ESI level-2 patients;patients who required immediate evaluation andpatients who could wait a brief time (10 minutes orso) without clinical deterioration. This dilemma ledto a large, multi-center, prospective study that wasconducted to identify characteristics of ESI level-2patients who actually received immediateinterventions (Tanabe et al., in press). Results fromthat multicenter study were the impetus formodifying the ESI system. This updated edition ofthe ESI handbook presents the changes anddescribes ESI v. 4.
An ESI level-1 patient is not always brought to theemergency department by ambulance. The patientwith a drug overdose or acute alcohol intoxicationmay be dropped at the front door. Children may bebrought by car and carried into the emergencydepartment. The experienced triage nurse is able toinstantly identify this critical patient. With a brief,across-the-room assessment the triage nurserecognizes the patient that is in extremis. Thispatient is taken immediately to the treatment areaand resuscitation efforts are initiated.
Patients assessed as an ESI level 1 constituteapproximately 1 percent to 3 percent of all EDpatients (Eitel et al., 2003; Wuerz, Milne, Eitel,Travers & Gilboy, 2000; Wuerz et al., 2001). Uponarrival, the patient's condition requires immediateresuscitation from either the emergency physicianand nurse or the trauma or code team. From ESIresearch we know that most ESI level-1 patients areadmitted to intensive care units, while some die inthe emergency department (Eitel et al., 2003; Wuerz,2001). A few ESI level-1 patients are discharged fromthe ED, if they have a reversible change in level ofconsciousness or vital functions such ashypoglycemia, seizures, alcohol intoxication, oranaphylaxis.
Examples of ESI level 1:
• Cardiac arrest.• Respiratory arrest.• Severe respiratory distress.• SpO2 < 90.• Critically injured trauma patient who presents
unresponsive.• Overdose with a respiratory rate of 6.
• Severe respiratory distress with agonal or gasping-type respirations.
• Severe bradycardia or tachycardia with signs ofhypoperfusion.
• Hypotension with signs of hypoperfusion.• Trauma patient who requires immediate
crystalloid and colloid resuscitation. • Chest pain, pale, diaphoretic, blood pressure
70/palp.• Weak and dizzy, heart rate = 30.• Anaphylactic reaction.• Baby that is flaccid. • Unresponsive with strong odor of ETOH.• Hypoglycemia with a change in mental status.
Decision Point B: Should thePatient Wait?Once the triage nurse has determined that thepatient does not meet the criteria for ESI level 1, thetriage nurse moves to decision point B (see Figure 3-3). At decision point B the nurse needs to decidewhether this patient should wait to be seen. If thepatient should not wait, the patient is triaged as ESIlevel 2. If the patient can wait, then the user movesto the next step in the algorithm.
Three broad questions are used to determinewhether the patient meets level-2 criteria.
1. Is this a high-risk situation?
2. Is the patient confused, lethargic or disoriented?
3. Is the patient in severe pain or distress?
The triage nurse obtains pertinent subjective andobjective information to quickly answer thesequestions. A brief introduction to ESI level-2 criteriais presented here, while a more detailed explanationof patients who meet ESI level-2 criteria will bepresented in Chapter 4.
Chapter 3. Introduction to the Emergency Severity Index
19
Figure 3-3. Decision Point B: Should the PatientWait?
high risk situation?or
confused/lethargic/disoriented?or
severe pain/distress?
2
B
yes

to the ED with a chief complaint, signs andsymptoms, or history suggestive of a problem orcondition that is serious and, unless dealt withpromptly, can deteriorate rapidly. Often patient age,past medical history, and current medicationsinfluence the perceived severity of the chiefcomplaint. For example, a frail elderly patient withsevere abdominal pain is at a much higher risk ofmorbidity and mortality than a 20-year-old. Theelderly patient with abdominal pain should beclassified as ESI level 2, while the 20-year-old with
stable vital signs will usually be classified as ESI level3. It is common for the triage nurse to identify ahigh-risk situation which may then be confirmed byfinding abnormal vital signs. For example, a patientwho complains of a fever and productive cough maybe found to have a respiratory rate of 32 and anoxygen saturation of 90 percent. The experiencedtriage nurse uses knowledge and expertise torecognize that this patient probably has pneumonia,is at risk for desaturating and is therefore high risk.Inexperienced ED nurses are not likely to have the
Chapter 4. ESI Level 2
28
System Examples/diagnosis Signs/symptoms
Abdomen Abdominal pain in the elderly Severe pain, stable vital signsGastrointestinal bleeding Tachycardia, vomiting blood or bright
red blood per rectum
Cardiac Chest pain Constant or intermittent, stable vital signsAcute arterial occlusion Absence of distal pulseHistory of angioplasty with chest pain Stable vital signsPericardial effusion Chest pain and shortness of breathInfective endocardititis History of drug abuse
General Immunocompromised patients May or may not have feverOncology patientsTransplant (post or on waiting list)
Genitourinary Testicular torsion Sudden onset of testicular painAcute renal failure Unable to be dialyzed
Gynecological Ectopic pregnancy + pregnant, severe lower quadrant painSpontaneous abortion Bleeding and tachycardia with stable
blood pressure
Mental Health Combative, hostile, hystericalSuicidal attempt/complaintETOH with traumaSexual assault - any
Neurologic Rule out meningitis Headache, fever, lethargy
History of multiple cerebrovascular Motor or speech deficitsaccidents
Acute ischemic stroke Motor or speech deficits
Pediatric Vomiting, diarrhea, unable to eat Sunken fontanel, poor skin turgor, lethargyAsthma attack Nasal flaring or use of intercostals
Respiratory Acute epiglottitis DroolingSevere asthma Severe shortness of breathPleural effusions Severe shortness of breathSpontaneous pneumothorax Sudden onset of shortness of breath
Trauma Motor vehicle crash with transient loss History of head traumaof consciousness
Stab wound to the groin Bleeding controlled, obvious stab wound
Table 4-1. Examples of High-risk Situations

pain of 8/10 is a good example of an ESI level-4patient. It is not necessary to rate this patient as alevel 2 based on pain alone.
In some patients, pain can be assessed by clinicalobservation: distressed facial expression, diaphoresis,body posture, and changes in vital signs. The triagenurse observes physical responses to acute pain thatsupport the patient's rating. For example, the patientwith abdominal pain who is diaphoretic,tachycardic, and has an elevated blood pressure; orthe patient with severe flank pain, vomiting, paleskin, and a history of renal colic are both goodexamples of patients that meet ESI level-2 criteria.Chapter 4 provides additional information on ESIlevel 2 and pain.
Severe distress can be physiological or psychological.Examples of distress include the sexual assaultvictim, the combative patient, or the bipolar patientwho is currently manic.
ESI level-2 patients constitute a relatively lowvolume, high-risk group that comprise 20 percent to30 percent of emergency department patients(Travers et al., 2002; Wuerz et al., 2001, Tanabe,Gimbel et al., 2004). Once an ESI level-2 patient isidentified, the triage nurse needs to ensure that thepatient is cared for in a timely manner. Registrationcan be completed by a family member or at thebedside. ESI level-2 patients need vital signs and acomprehensive nursing assessment but notnecessarily at triage. Placement should not bedelayed to finish obtaining vital signs. ESI researchhas shown that 50 to 60 percent of ESI level-2patients are admitted from the ED (Wuerz et al.,2001).
Decision Point C: ResourceNeedsIf the answers to the questions at the first twodecision points are “no,” then the triage nursemoves to decision point C (see Figure 3-4). Thetriage nurse should ask, “How many differentresources do you think this patient is going toconsume in order for the physician to reach adisposition decision?” The disposition decisioncould be to send the patient home, admit to theobservation unit, admit to the hospital, or even totransfer to another institution. This decision pointagain requires the triage nurse to draw from past
experiences in caring for similar emergencydepartment patients. ED nurses need to clearlyunderstand that the estimate of resources has to dowith standards of care and is independent of type ofhospital (i.e., teaching or non-teaching) andlocation. A patient presenting to any emergencydepartment should consume the same generalresources in order for a disposition to be reached.Considering the patient's brief subjective andobjective assessment, past medical history, allergies,medications, age, and gender, how many differentresources will be used in order for the physician toreach a disposition? In other words, what is typicallydone for the patient who presents to the emergencydepartment with this common complaint? Thetriage nurse is asked to do this based on his or herassessment of the patient and should not considerindividual practice patterns, but rather the routinepractice in the particular ED.
To identify resource needs the triage nurse must befamiliar with emergency department standards ofcare. The triage nurse must be knowledgeable aboutthe concept of “prudent and customary.” One easyway to think about this concept is to ask thequestion “Given this patient's chief complaint orinjury, what resources is the emergency physicianlikely to utilize?” Resources can be hospital services,tests, procedures, consults or interventions that areabove and beyond the physician history andphysical, or very simple emergency departmentinterventions such as applying a bandage. Furtherexplanations and examples are provided in Chapter 5.
A list of what is and what is not considered aresource for purposes of ESI triage classification canbe found in Table 3-3. ESI level-3 patients arepredicted to require two or more resources; ESI level-4 patients are predicted to require one resource; andESI level-5 patients are predicted to require noresources (Table 3-4).
Chapter 3. Introduction to the Emergency Severity Index
21
Figure 3-4. Resource Prediction
how many different resources are needed?
none one many
C

Research has shown that ESI level-3 patients makeup 30 percent to 40 percent of patients seen in theemergency department (Eitel et al., 2003; Wuerz etal., 2001). They often require a more in-depthevaluation but are felt to be stable in the short term,and certainly may have a longer length of stay inthe ED. ESI level 4 and ESI level 5 make up between20 percent and 35 percent of ED volume, perhapseven more in a community with poor primary careaccess. Appropriately trained mid-level providerswith the right skills mix could care for these patientsin a fast-track or express care setting, recognizingthat a high proportion of these patients have atrauma-related presenting complaint. Since theirphysical condition is stable, these patients couldsafely wait several hours to be seen.
Chapter 3. Introduction to the Emergency Severity Index
22
Resources Not resources
Labs (blood, urine) History & physical (including pelvic)
ECG, X-rays Point-of-care testingCT-MRI-ultrasoundangiography
IV fluids (hydration) Saline or heplock
IV, IM or nebulized PO medicationsmedications Tetanus immunization
Prescription refills
Specialty consultation Phone call to PCP
Simple procedure = 1 Simple wound care(lac repair, Foley cath) (dressings, recheck)Complex procedure = 2 Crutches, splints, (conscious sedation) slings
Table 3-3. ESI Resources
ESI Level Patient Presentation Interventions Resources
5 Healthy 10-year-old child with poison ivy Needs an exam and prescription None
5 Healthy 52-year-old male ran out of blood Needs an exam and prescription Nonepressure medication yesterday; BP 150/92
4 Healthy 19-year-old with sore throat Needs an exam, throat culture, Lab (throatand fever prescriptions culture)*
4 Healthy 29-year-old female with a urinary Needs an exam, urine, and urine Lab (urine,tract infection, denies vaginal discharge culture, maybe urine hCG, and urine C&S,
prescriptions urine hCG)**
3 A 22-year-old male with right lower Needs an exam, lab studies, 2 or morequadrant abdominal pain since early IV fluid, abdominal CT, and this morning + nausea, no appetite perhaps surgical consult
3 A 45-year-old obese female with left lower Needs exam, lab, lower extremity 2 or moreleg pain and swelling, started 2 days non-invasive vascular studiesago after driving in a car for 12 hours
* In some regions throat cultures are not routinely performed; instead, the patient is treated based onhistory and physical exam. If that is the case the patient would be an ESI level 5.
** All 3 tests count as one resource (Lab).
Table 3-4. Predicting Resources

Decision Point D:The Patient'sVital SignsBefore assigning a patient to ESI level 3, the nurseneeds to look at the patient's vital signs and decidewhether they are outside the accepted parametersfor age and are felt by the nurse to be meaningful. Ifthe vital signs are outside accepted parameters, thetriage nurse should consider upgrading the triagelevel to ESI level 2. However, it is the triage nurse’sdecision as to whether or not the patient should beupgraded to an ESI level 2 based on vital signabnormalities. This is decision point D.
Vital sign parameters are outlined by age (see Figure3-5). The vital signs used are pulse, respiratory rate,and oxygen saturation and, for any child under agethree, body temperature. Using the vital sign criteria,the triage nurse can upgrade an adult patient whopresents with a heart rate of 104, or this patient canremain ESI level 3. A 6-month-old baby with a coldand a respiratory rate of 48 could be triaged ESI level2 or 3. Based on the patient's history and physicalassessment, the nurse must ask if the vital signs areenough of a concern to say that the patient is highrisk and cannot wait to be seen. Chapter 6 explainsvital signs in detail and gives examples.
Temperature is only included with children underage three. Significant fever may exclude youngchildren from categories 4 and 5. This will helpidentify potentially bacteremic children and avoidsending them to a fast track setting or waiting aprolonged time. Pediatric fever guidelines will bedescribed in detail in Chapter 6.
Does Time to Treatment InfluenceESI Triage Categories?An estimate of how long the patient can wait to beseen by a physician is an important component ofmost triage systems. The Australasian and CanadianTriage Systems require patients to be seen by aphysician within a specific time period, based ontheir triage category. ESI does not mandate specifictime standards in which patients must be evaluatedby a physician. However, patients who meet criteriafor ESI level 2 should be seen as soon as possible; itis up to the individual institution to determine apolicy. Frequently, there may be confusion betweeninstitutional policy and “flow or process of patientcare” and ESI triage level.
We will describe four patient scenarios in whichflow and triage category may seem to conflict. Oftentrauma patients present to the triage nurse aftersustaining a significant mechanism of injury, such asan unrestrained passenger in a high-speed motorvehicle crash. The patient may have left the crashscene in some way other than by ambulance, andthen presents to triage with localized right upperquadrant pain with stable vital signs. This patient isphysiologically stable, walked into the ED and doesnot meet ESI level-1 criteria. However, the patient isat high risk for a liver laceration and othersignificant trauma, so should be triaged as ESI level2. Frequently, EDs have trauma policies and traumaresponse level categorization that will require rapidinitiation of care. Triage and trauma response levelare both important and should be recorded as twodifferent scores. While the triage nurse recognizesthis is a physiologically stable trauma patient andcorrectly assigns ESI level 2, she should facilitatepatient placement and trauma care as outlined bythe trauma policy. The patient is probably stable foranother 10 minutes and does not require immediatelife-saving interventions. If the same patientpresented with a blood pressure of 80 palpable, theywould be triaged as ESI level 1 and requireimmediate hemodynamic, life-saving interventions.
Chapter 3. Introduction to the Emergency Severity Index
23
Figure 3-5. Danger Zone Vital Signs
danger zonevitals?
<3 m >180 >50
3 m-3y >160 >40
3-8 y >140 >30
>8y >100 >20
3
D
no
consider
RRHR
SaO
2<92
%

When using ESI as a triage system, vital signsassessment is not necessary in the triage area forpatients who are immediately categorized as level 1or 2. If the patient appears unstable or presents witha chief complaint that necessitates immediatetreatment, then transport of the patient directly tothe treatment area should be expedited. For thesepatients, the resuscitation team is responsible forobtaining and monitoring vital signs at the bedside.This would include patients that have clinicalappearances that indicate high risk or need forimmediate cardiovascular or respiratoryintervention. These patients may appear pale,diaphoretic, or cyanotic. However, the triage nursehas the option to perform vitals in the triage area, ifan open bed is not immediately available or if he orshe feels that the vital signs may assist in confirmingthe triage acuity level. Some patients may notinitially be identified as ESI level 1 until vital signsare taken. For example, an awake, alert elderlypatient who complains of dizziness might be foundto have a life-threatening condition when a heartrate of 32 or 180 is discovered during vital signmeasurement.
As shown in the ESI algorithm in Chapter 3, ifpatients do not meet ESI level-1 or 2 criteria, thetriage nurse comes to decision point C. The nursethen determines how many resources the patient isexpected to need in the ED. If the patient isexpected to need one or no resources, he or she canbe assigned an ESI level of 4 or 5 and no vital signassessment is necessary. But if the patient is expectedto need two or more resources, then the nursecomes to decision point D and vital signs should beassessed. Vital signs can play a more important rolein the evaluation of some patients at triage,especially those triaged as ESI level 3. The range ofvital signs may provide supporting data for potentialindicators of serious illness. If any of the dangerzone vital signs are exceeded, it is recommended
that the triage nurse consider up-triaging the patientfrom level 3 to level 2.
Vital signs that are explicitly included in ESI triageare heart rate, respiratory rate, and oxygensaturation (for patients with potential respiratorycompromise). Temperature is specifically used in ESItriage for children under age 3 (see below). It isimportant to note that when considering abnormalvital signs, blood pressure is not included in the ESIalgorithm. This does not mean that the triage nurseshould not take a blood pressure or a temperatureon older children or adults but that these vital signsare not necessarily used to assist in selecting theappropriate triage acuity level.
Vital Signs and Pediatric FeverIn this version of the ESI Handbook, version 4 (v.4)of the ESI algorithm has been updated to includemore current pediatric fever criteria. As shown inFigure 6-2, note D of the ESI algorithm addressespediatric fever considerations for ESI triage. Thissection incorporates recommendations from theAmerican College of Emergency Physicians' ClinicalPolicy for Children Younger Than Three YearsPresenting to the Emergency Department With Fever(ACEP, 2003).
The ESI Triage Research Team recommends that vitalsigns in patients under age 3 be assessed at triage. Inparticular, temperature measurement is importantduring triage of all children from newborn through36 months of age, and vital sign evaluation isessential to the overall assessment of a known febrileinfant under age 36 months (Baraff, 2000). Thishelps to differentiate ESI level-2 and 3 patients andminimize the risk that potentially bacteremicchildren will be sent to an express care area orotherwise experience an inappropriate wait.Remember, if a patient is in immediate danger or
Chapter 6.The Role of Vital Signs in ESI Triage
44
Figure 6-2. Danger Zone Vital Signs
D. Danger Zone Vital SignsConsider uptriage to ESI 2 if any vital sign criterion is exceeded.
Pediatric Fever Considerations1 to 28 days of age: assign at least ESI 2 if temp >38.0 C (100.4F)
1-3 months of age: consider assigning ESI 2 if temp >38.0 C (100.4F)
3 months to 3 yrs of age: consider assigning ESI 3 if: temp >39.0 C (102.2 F), or incomplete immunizations, or no obvious source of fever

Appendix B. ESI Triage Algorithm, v. 4
B–2
Notes:
A. Immediate life-saving intervention required: airway, emergency medications, orother hemodynamic interventions (IV, supplemental O2, monitor, ECG or labs DONOT count); and/or any of the following clinical conditions: intubated, apneic,pulseless, severe respiratory distress, SPO2<90, acute mental status changes, orunresponsive.
Unresponsiveness is defined as a patient that is either:(1) nonverbal and not following commands (acutely); or (2) requires noxious stimulus (P or U on AVPU) scale.
B. High risk situation is a patient you would put in your last open bed.
Severe pain/distress is determined by clinical observation and/or patient rating ofgreater than or equal to 7 on 0-10 pain scale.
C. Resources: Count the number of different types of resources, not the individual tests or x-rays (examples: CBC, electrolytes and coags equals one resource; CBCplus chest x-ray equals two resources).
Resources
• Labs (blood, urine)• ECG, X-rays• CT-MRI-ultrasound-angiography
• IV fluids (hydration)
• IV or IM or nebulized medications
• Specialty consultation
• Simple procedure =1(lac repair, foley cath)
• Complex procedure =2(conscious sedation)
Not Resources
• History & physical (including pelvic)• Point-of-care testing
• Saline or heplock
• PO medications• Tetanus immunization• Prescription refills
• Phone call to PCP
• Simple wound care (dressings, recheck)
• Crutches, splints, slings
D. Danger Zone Vital SignsConsider uptriage to ESI 2 if any vital sign criterion is exceeded.
Pediatric Fever Considerations1 to 28 days of age: assign at least ESI 2 if temp >38.0 C (100.4F)
1-3 months of age: consider assigning ESI 2 if temp >38.0 C (100.4F)
3 months to 3 yrs of age: consider assigning ESI 3 if: temp >39.0 C (102.2 F), or incomplete immunizations, or no obvious source of fever
© ESI Triage Research Team, 2004 – (Refer to teaching materials for further clarification)

Triage nurse
Immediate/emergent
ER urgent
ESI 1,2
ESI 3
wai-ng ESI 4,5
Re-triage
Re-triage
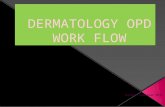
OPD






Undertriage VS overtriage

มาตรการ
• อบรมพยาบาล
• พัฒนาระบบคัดแยกผู้ป่วย ESI 5 level
• งานวิจัยพยาบาล การคัดแยก
• งานวิจัยแพทย์ ดูผลกระทบ MM
• ตรวจสอบ reliability ของการคัดแยก " inter-rater
• อบรมซ้ำบ่อยๆ

Kohn LT et al. To Err is Human: Building a Safer Health System, 1999
Error in healthcare
Process > Individual

สรุป
• คัดแยกเพื่อค้นหาผู้ป่วยที่มีภาวะคุกคามต่อชีวิต
• กลไกที่ต่อเนื่อง • มี high index of suspicion อยู่ตลอดเวลา
• Physiologic parameters

Decision Point D:The Patient'sVital SignsBefore assigning a patient to ESI level 3, the nurseneeds to look at the patient's vital signs and decidewhether they are outside the accepted parametersfor age and are felt by the nurse to be meaningful. Ifthe vital signs are outside accepted parameters, thetriage nurse should consider upgrading the triagelevel to ESI level 2. However, it is the triage nurse’sdecision as to whether or not the patient should beupgraded to an ESI level 2 based on vital signabnormalities. This is decision point D.
Vital sign parameters are outlined by age (see Figure3-5). The vital signs used are pulse, respiratory rate,and oxygen saturation and, for any child under agethree, body temperature. Using the vital sign criteria,the triage nurse can upgrade an adult patient whopresents with a heart rate of 104, or this patient canremain ESI level 3. A 6-month-old baby with a coldand a respiratory rate of 48 could be triaged ESI level2 or 3. Based on the patient's history and physicalassessment, the nurse must ask if the vital signs areenough of a concern to say that the patient is highrisk and cannot wait to be seen. Chapter 6 explainsvital signs in detail and gives examples.
Temperature is only included with children underage three. Significant fever may exclude youngchildren from categories 4 and 5. This will helpidentify potentially bacteremic children and avoidsending them to a fast track setting or waiting aprolonged time. Pediatric fever guidelines will bedescribed in detail in Chapter 6.
Does Time to Treatment InfluenceESI Triage Categories?An estimate of how long the patient can wait to beseen by a physician is an important component ofmost triage systems. The Australasian and CanadianTriage Systems require patients to be seen by aphysician within a specific time period, based ontheir triage category. ESI does not mandate specifictime standards in which patients must be evaluatedby a physician. However, patients who meet criteriafor ESI level 2 should be seen as soon as possible; itis up to the individual institution to determine apolicy. Frequently, there may be confusion betweeninstitutional policy and “flow or process of patientcare” and ESI triage level.
We will describe four patient scenarios in whichflow and triage category may seem to conflict. Oftentrauma patients present to the triage nurse aftersustaining a significant mechanism of injury, such asan unrestrained passenger in a high-speed motorvehicle crash. The patient may have left the crashscene in some way other than by ambulance, andthen presents to triage with localized right upperquadrant pain with stable vital signs. This patient isphysiologically stable, walked into the ED and doesnot meet ESI level-1 criteria. However, the patient isat high risk for a liver laceration and othersignificant trauma, so should be triaged as ESI level2. Frequently, EDs have trauma policies and traumaresponse level categorization that will require rapidinitiation of care. Triage and trauma response levelare both important and should be recorded as twodifferent scores. While the triage nurse recognizesthis is a physiologically stable trauma patient andcorrectly assigns ESI level 2, she should facilitatepatient placement and trauma care as outlined bythe trauma policy. The patient is probably stable foranother 10 minutes and does not require immediatelife-saving interventions. If the same patientpresented with a blood pressure of 80 palpable, theywould be triaged as ESI level 1 and requireimmediate hemodynamic, life-saving interventions.
Chapter 3. Introduction to the Emergency Severity Index
23
Figure 3-5. Danger Zone Vital Signs
danger zonevitals?
<3 m >180 >50
3 m-3y >160 >40
3-8 y >140 >30
>8y >100 >20
3
D
no
consider
RRHR
SaO
2<92
%

When using ESI as a triage system, vital signsassessment is not necessary in the triage area forpatients who are immediately categorized as level 1or 2. If the patient appears unstable or presents witha chief complaint that necessitates immediatetreatment, then transport of the patient directly tothe treatment area should be expedited. For thesepatients, the resuscitation team is responsible forobtaining and monitoring vital signs at the bedside.This would include patients that have clinicalappearances that indicate high risk or need forimmediate cardiovascular or respiratoryintervention. These patients may appear pale,diaphoretic, or cyanotic. However, the triage nursehas the option to perform vitals in the triage area, ifan open bed is not immediately available or if he orshe feels that the vital signs may assist in confirmingthe triage acuity level. Some patients may notinitially be identified as ESI level 1 until vital signsare taken. For example, an awake, alert elderlypatient who complains of dizziness might be foundto have a life-threatening condition when a heartrate of 32 or 180 is discovered during vital signmeasurement.
As shown in the ESI algorithm in Chapter 3, ifpatients do not meet ESI level-1 or 2 criteria, thetriage nurse comes to decision point C. The nursethen determines how many resources the patient isexpected to need in the ED. If the patient isexpected to need one or no resources, he or she canbe assigned an ESI level of 4 or 5 and no vital signassessment is necessary. But if the patient is expectedto need two or more resources, then the nursecomes to decision point D and vital signs should beassessed. Vital signs can play a more important rolein the evaluation of some patients at triage,especially those triaged as ESI level 3. The range ofvital signs may provide supporting data for potentialindicators of serious illness. If any of the dangerzone vital signs are exceeded, it is recommended
that the triage nurse consider up-triaging the patientfrom level 3 to level 2.
Vital signs that are explicitly included in ESI triageare heart rate, respiratory rate, and oxygensaturation (for patients with potential respiratorycompromise). Temperature is specifically used in ESItriage for children under age 3 (see below). It isimportant to note that when considering abnormalvital signs, blood pressure is not included in the ESIalgorithm. This does not mean that the triage nurseshould not take a blood pressure or a temperatureon older children or adults but that these vital signsare not necessarily used to assist in selecting theappropriate triage acuity level.
Vital Signs and Pediatric FeverIn this version of the ESI Handbook, version 4 (v.4)of the ESI algorithm has been updated to includemore current pediatric fever criteria. As shown inFigure 6-2, note D of the ESI algorithm addressespediatric fever considerations for ESI triage. Thissection incorporates recommendations from theAmerican College of Emergency Physicians' ClinicalPolicy for Children Younger Than Three YearsPresenting to the Emergency Department With Fever(ACEP, 2003).
The ESI Triage Research Team recommends that vitalsigns in patients under age 3 be assessed at triage. Inparticular, temperature measurement is importantduring triage of all children from newborn through36 months of age, and vital sign evaluation isessential to the overall assessment of a known febrileinfant under age 36 months (Baraff, 2000). Thishelps to differentiate ESI level-2 and 3 patients andminimize the risk that potentially bacteremicchildren will be sent to an express care area orotherwise experience an inappropriate wait.Remember, if a patient is in immediate danger or
Chapter 6.The Role of Vital Signs in ESI Triage
44
Figure 6-2. Danger Zone Vital Signs
D. Danger Zone Vital SignsConsider uptriage to ESI 2 if any vital sign criterion is exceeded.
Pediatric Fever Considerations1 to 28 days of age: assign at least ESI 2 if temp >38.0 C (100.4F)
1-3 months of age: consider assigning ESI 2 if temp >38.0 C (100.4F)
3 months to 3 yrs of age: consider assigning ESI 3 if: temp >39.0 C (102.2 F), or incomplete immunizations, or no obvious source of fever

Triage nurse
Immediate/emergent
ER urgent
ESI 1,2
ESI 3
wai-ng ESI 4,5
Re-triage
Re-triage
OPD

ขอบคุณครับ