
Report on the Ideal and Current State of Dementia Care ...seniorscarenetwork.ca › wp-content ›...
60
Compiled for Discussion and Planning Purposes Dementia Capacity Planning in the Central East LHIN: Report on the Ideal and Current State of Dementia Care Services November 29 2018 (Revised)
Transcript of Report on the Ideal and Current State of Dementia Care ...seniorscarenetwork.ca › wp-content ›...

Compiled for Discussion and Planning Purposes
Dementia Capacity Planning in the Central East LHIN:
Report on the Ideal and Current State of Dementia Care Services
November 29 2018 (Revised)

November 29, 2018 2
Contents List of Tables ................................................................................................................................................. 3
List of Figures ................................................................................................................................................ 5
Executive Summary ....................................................................................................................................... 7
Introduction .................................................................................................................................................. 8
A Phased Approach to Capacity Planning ..................................................................................................... 9
Phase One: Development of an Ideal State View for Dementia Care .......................................................... 9
Ideal State View – Definition of Components ............................................................................................. 10
The Overarching Principles ......................................................................................................................... 10
Action Areas ................................................................................................................................................ 11
Foundational Elements ............................................................................................................................... 13
Phase Two: Development of the Current State View of Dementia Care ................................................... 14
Heightened Public Awareness .................................................................................................................... 16
Educated Dementia Workforce .................................................................................................................. 18
Appropriate Clinical and Diagnostic Services .............................................................................................. 20
Comprehensive and Responsive Community Supports .............................................................................. 37
Flexible, Proactive and Responsive Care Partner Education, Supports and Respite .................................. 40
Creative and Affordable Housing Models ................................................................................................... 45
Planning for Phase Three ............................................................................................................................ 49
Appendix 1: Dementia Capacity Planning Action Group Members (Phase 1 and 2) and Report
Contributors ................................................................................................................................................ 51
Appendix 2: Stakeholders Consulted .......................................................................................................... 52
Appendix 3: Workforce Training Program Descriptions ............................................................................. 53
Appendix 4: ADP Providers and Sites .......................................................................................................... 54
Appendix 5: Central East LHIN Retirement Homes by LHIN Sub Region .................................................... 55
Appendix 6: LTCH Secure Bed Summary ..................................................................................................... 57
Appendix 7: Decision Matrix………………………………………………………………………………………………………………….60

November 29, 2018 3
List of Tables Table 1: Abbreviations for LHIN Sub Regions Used in this Report ................................................................ 6
Table 2: Overarching Principles - an Ideal State for Dementia Care ........................................................... 11
Table 3: Six Action Areas of Dementia Care ................................................................................................ 12
Table 4: Foundational Elements of a Dementia Care System ..................................................................... 13
Table 5: Current Categories and Examples of Service by Ideal State Action Area ...................................... 15
Table 6: Distribution by Sub-Region of Current Public Awareness Initiatives ............................................ 17
Table 7: Referral from Primary Care Collaborative Memory Services to First Link 2017/18 ...................... 17
Table 8: Central East Dementia Related System Navigation Resources 2017/18 ...................................... 18
Table 9: Regional Workforce Training Delivered by the Central East Behavioural Supports Ontario
Program 2017/18 ........................................................................................................................................ 19
Table 10: Distribution by Sub-Regions of Workforce Dementia Training by Central East Alzheimer
Societies 2017/18 ........................................................................................................................................ 19
Table 11: Public Education Sessions by Alzheimer Society 2017/18 .......................................................... 19
Table 12: Primary Care Geriatric/General Dementia Focused Services in the Central East LHIN 2017/18 20
Table 13: Primary Care Collaborative Memory Services in the Central East LHIN ..................................... 22
Table 14: PCCMS Service Volumes by Team 2017/18 ................................................................................ 23
Table 15: Top 20 CMGs in Inpatients and MRDX in Emergency Room Patients who have Dementia (all
types) 2017/18 ............................................................................................................................................ 24
Table 16: Alternate Level of Care (ALC) Analysis – Central East LHIN Dementia Inpatients, 2017-2018 ... 25
Table 17: Senior Friendly Initiative Summary by Central East LHIN Hospital ............................................. 26
Table 18: Summary of Geriatric Psychiatry and Mental Health Outpatient Services 2017/18 .................. 28
Table 19: Summary of Geriatric Psychiatry and Geriatric Mental Health Inpatient Services 2017/18 ...... 29
Table 20: Referrals, Individuals and Families supported by Community BSO in 2017/18 .......................... 30
Table 21: Number of Available and Actual GAIN Appointments by Sub Region 2017/18 .......................... 31
Table 22: GAIN Visits by FTE 2017/18 ......................................................................................................... 32
Table 23: GAIN Total Caseload by Team and Month 2017/18 ................................................................... 32
Table 24: Location(s), Service hours and Wait List by GAIN Team ............................................................. 33
Table 25: 2017-18 Computed Tomography (CT) Machines Inventory Refresh Central East LHIN ............. 35
Table 26: 2017-18 Magnetic Resonance Imaging (MRI) Machines Inventory Refresh Central East LHIN .. 36
Table 27: Distribution by Sub-Region of Social and Recreational Programming Delivered by Alzheimer
Societies 2017/18 ........................................................................................................................................ 38
Table 28: Central East LHIN Social and Recreational Programs, Sessions and Participants by Alzheimer
Societies 2017/19 ........................................................................................................................................ 39
Table 29: Agencies providing CSS Programs by LHIN Sub-Region .............................................................. 39
Table 30: Percent (%) of Overall Budget Provided by the Central East LHIN by Alzheimer Society 2017/18
.................................................................................................................................................................... 40
Table 31: Caregiver Support Programs and Participants by Alzheimer Society 2017/18 ........................... 41
Table 32: Distribution by Sub-Region of Caregiver Education and Support Groups Delivered by Alzheimer
Societies 2017/18 ........................................................................................................................................ 41
Table 33: Participants in the Central East LHIN's Power for Tools for Caregiver Series 2017/18 .............. 42

November 29, 2018 4
Table 34: Self-Reported estimates of % of Unique Clients with Dementia by ADP .................................... 43
Table 35: In-Home Respite Provided in the Central East LHIN in 2017/18 ................................................. 45
Table 36: Individual Served by ALHRS 2017/18 at Q4 ................................................................................ 46
Table 37: Number of Retirement Homes, Bed Capacity and Specialized Dementia Beds by LHIN Sub
Region 2017/18 ........................................................................................................................................... 46
Table 38: Number of BSO Teams and FTEs by LHIN Sub-Region as of October 2018 ................................. 47
Table 39: LTCH Secure Bed Summary ......................................................................................................... 48
Table 40: Categories of Adaptive Technology in Seniors’ and Dementia Care ........................................... 48
November 29, 2018 5
List of Figures Figure 1: Map of the Central East LHIN ......................................................................................................... 6
Figure 2: Core Concepts of Capacity Planning .............................................................................................. 8
Figure 3: Phases of Dementia Capacity Planning in the Central East LHIN ................................................... 9
Figure 4: Ideal State for Dementia Care in the Central East LHIN .............................................................. 10
Figure 5: Number of GAIN Patients at each Dementia Stage (Past Two Years) .......................................... 34
Figure 6: Infographic - Community and Social Services Utilized in 2017/18 .............................................. 40
Figure 7: Respite Beds by LHIN Sub Region (2018) ..................................................................................... 44
Figure 8: Assistive Robotics at UOIT July 2018 ........................................................................................... 48

November 29, 2018 6
Figure 1: Map of the Central East LHIN
Table 1: Abbreviations for LHIN Sub Regions Used in this Report
Durham North East (DNE) Durham West (DW) Haliburton County and City of Kawartha Lakes (HCCKL) Northumberland County (NC)
Peterborough City and County (PCC) Scarborough North (SN) Scarborough South (SS)

November 29, 2018 7
Executive Summary The purpose of this report is to provide an overview of the consultation and planning approach used in the first two phases of dementia capacity planning in the Central East LHIN. This report also conveys the resulting ideal state recommended for dementia care in the region. Further, this document catalogues all currently available dementia care resources in the Central East LHIN and reports on all available utilization data. It is the first report of its kind and it offers a starting place to enable planning activity relevant to building a local approach to dementia care services. The intention is to use the information gathered thus far, in combination with projection information from the Ministry of Health and Long Term Care about the anticipated rates of dementia among residents of the Central East LHIN, to carry out a gap analysis and inform regional and sub-regional planning.
The development of this report was led the Central East Dementia Capacity Planning Action Group.

November 29, 2018 8
Introduction In 2017/18, the Ministry of Health and Long Term Care (MOHLTC) developed and communicated expectations to the Local Health Integration Networks (LHINs) regarding a standardized process for capacity planning. The MOHLTC articulated dementia care as an initial focus for LHIN capacity planning efforts, to support the implementation of the Ontario Dementia Strategy, approved as part of the 2017 budget. Figure 1 reflects core concepts related to capacity planning.
Figure 2: Core Concepts of Capacity Planning1
The Central East LHIN requested their seniors’ care coordinating entity, Seniors Care Network (the local Regional Geriatric Program) to take the lead to carry out the necessary tasks associated with dementia capacity planning. In turn, Seniors Care Network forged a collaborative partnership with the three local Alzheimer Societies2 and the Central East LHIN to guide the development of the Central East LHIN’s Dementia Capacity Plan. This tri-partite group formed the initial Central East LHIN Dementia Capacity Planning Action Group. Members of the Action Group are indicated in Appendix 1, along with a list of individuals who provided data and/or reviewed drafts of this report.
1 MOHLTC (2017). Capacity planning guide – LHIN planning guide (draft), p. 10
2 Alzheimer Society of Durham Region (ASDR), Alzheimer Society of Peterborough, Kawartha Lakes,
Northumberland & Haliburton (ASPKLNH), Alzheimer Society of Toronto (AST)

November 29, 2018 9
A Phased Approach to Capacity Planning Dementia capacity planning work in the Central East LHIN is occurring in three phases. This report summarizes the results of Phase One and Two.
Figure 3: Phases of Dementia Capacity Planning in the Central East LHIN
Prior to commencing the development of the ideal state view, the Action Group clarified the primary planning questions as:
What ought to be included in the overall system and each of the system parts How will we make judgements about what to include in the system and in system parts? (e.g.
evidence, analysis, consultation, expert opinion) How will the judgements made be vetted? What standards will guide the operation of each of the system parts and how will these be
developed?
The Action Group also considered the desired outcomes of the MOHLTC and local stakeholders and adopted the following outcomes to direct the planning work:
Reduced demand for Long Term Care (LTC) (MOHLTC) Improved health system efficiency (MOHLTC) Increased experience of living well with dementia (Central East LHIN Stakeholders)
Beginning with the end goal in mind, the first phase concluded in July 2018 and produced an ideal state view for dementia care in the Central East LHIN. In the view of the Action Group, this represents the “demand” for services, consistent with the MOHLTC’s capacity planning concepts. The process of developing the ideal state view included the following tasks:
Research and development of an initial ideal state and logic model, drawing on current evidence and the Central East Action Plan for Dementia (2016).
Extensive consultations with 17 groups, and more than 200 participants, including people living with dementia and care partners. (See Appendix 2)
Qualitative analysis of roughly 850 textual statements/lines to extract themes. Double coding and collaborative review of generated themes to inform ideal state development. Development of evidence informed planning assumptions.
Phase One:
Development of an ideal state view for
Dementia Care (Demand)
Phase Two:
Development of the current state view of
Dementia Care (Suppy & Utilization)
Phase Three:
Gap analysis and development of
recommendations (Need)
Phase One: Development of an Ideal State View for Dementia Care
(Demand)

November 29, 2018 10
Refinement of the desired ideal state, which has achieved consensus-based approval from the Planning Committee.
Refinement of current state data components to guide current state data collection.
Ideal State View – Definition of Components The ideal state view for dementia care in the Central East LHIN includes
Two overarching principles (shown in purple and green) Six Action Areas (shown in blue) Four foundational elements (shown in orange)
Figure 4: Ideal State for Dementia Care in the Central East LHIN
The following sections explain each component in greater detail.
The Overarching Principles There are two overarching principles that frame the ideal state for dementia care in the Central East LHIN.

November 29, 2018 11
Table 2: Overarching Principles - an Ideal State for Dementia Care
Principle What does this mean? Why is this included?
People living well with dementia
“Living well with Dementia” refers to the desire of people diagnosed with dementia and their families to enjoy an optimal quality of life and continued participation and engagement in their communities for as long as possible. This also means access to appropriate, dementia informed health and social services when and if needed.
This principle is included because it reflects the focus of various stakeholders in the Central East LHIN who were more inspired by a vision of a good life and retained citizenship, than they were by mere avoidance of Long Term Care and/or improved health system efficiency. Throughout many consultations, stakeholders reflected on the deeply personal impact of dementia on their lives and the lives of their family and friends. This principle assisted in the positioning of all components of the “ideal state” as action areas framed in context with their impact on the lives on people living with dementia.
Equity of dementia related health services for all persons across
various geographies and cultural,
linguistic, underserved and
vulnerable populations
Health Quality Ontario (HQO) defines health equity as that which “allows people to reach their full health potential and receive high-quality care that is fair and appropriate to them and their needs, no matter where they live, what they have or who they are”. Equity is considered a dimension of quality.
The intersection of dementia and equity requires particular focus. Among people living with dementia, Indigenous and Francophone people are also a particular focus in the Central East LHIN, as services specific to these peoples may not yet be readily available. In addition, underserved populations (e.g. few services specific to their needs) may include people with young onset dementia and people with developmental disabilities who also have dementia. Vulnerable populations may include the under-housed or precariously housed and people with dementia that have come into contact with the justice system.
Action Areas
There are six action areas included in the ideal state view. These are defined in the following table.

November 29, 2018 12
Table 3: Six Action Areas of Dementia Care
Action Area What does this mean? Why is this included?
Heightened Public
Awareness
Every citizen will know more about dementia and how to interact and support people living with dementia. People living with dementia will know where to turn for help and will be supported to live well.
Awareness is considered the entry point for people experiencing memory problems to reach out for help, and for people living in general society to develop compassion and understanding for neighbours, friends and relatives who may be impacted by dementia.
Educated Dementia Workforce
The people paid to work in helping professions (e.g. regulated and unregulated health care workers) will have the necessary skills to support and care for people living with dementia and their families.
Consistent with Ontario’s Chronic Disease Management framework, prepared, proactive teams are a cornerstone of excellent health care services for people who live with complex health conditions like dementia. A well-trained workforce can help individuals living with dementia and their caregivers to optimize their independence, function and quality of life
Appropriate clinical and diagnostic
services
Expert interprofessional clinical services, positioned across the continuum (e.g. primary care, specialty care, home care, acute care, long term care) that can assess, diagnose, plan, intervene, rehabilitate, palliate and evaluate clinical outcomes.
Although health care services are only one part of living with dementia, appropriate care and services and effective care plans can make a difference in the quality of life of people living with dementia and their families.
Comprehensive and responsive community
supports
A range of community-based social, recreational and transportation supports for people living with dementia that can be tailored to the needs of individuals at different stages of disease.
All too often, through our consultations, people with dementia described being excluded from community activities as their disease progressed. This includes the identification of a diagnosis of dementia as an exclusion criteria for some services (e.g. transportation)
Flexible, proactive and responsive care partner education,
supports and respite
A range of education, supports (e.g. services and strategies) and respite options that are tailored to personal preferences and schedules, actively offered and available a) at a variety of price points, b) through difference delivery mechanisms (e.g. in home, external, virtual), c) at various times of day (or days of the week) and, d) in various locations (e.g. each LHIN sub-region or neighbourhood).
Care partners reinforced the need for flexibility, affordability, availability, and proximity and for active offers of assistance as they sometimes struggled to identify what they need.
Creative and Housing models that go beyond People living with dementia expressed

November 29, 2018 13
affordable housing models and adaptations
independent living and assisted/supported living or long term care, which are viewed as unavailable or expensive. Adaptations may include: congregate living or shared accommodation options and technology assisted living.
that when individual dwellings become too difficult to manage, there are few available options for people to continue to live safely and affordably in the community in non-institutional settings.
Foundational Elements Several themes emerged through the consultation process that are best described as foundational elements that should under pin all action areas. These are defined as follows
Table 4: Foundational Elements of a Dementia Care System
Foundational Element
What does this mean? Why is it included?
Coordination, care planning and
system navigation sustained
throughout the entire dementia
journey
The activities of coordination, care planning and system navigation refer to functions that may be performed by a variety of service personnel that help people living with dementia and their families find their way to the right services for their needs.
This has been included as a foundational element because care partners have identified “finding their way” to resources very difficult. They have also found the plethora of “coordinators/navigators” adds to their difficulties, as they must repeat their stories every time. Sustained, rather than episodic navigation supports are essential so that navigators can make personalized connections with people living with dementia, understand their specific needs and link them to the services and resources that suit them best.
Quality standards for dementia care
There are new standards for dementia care, published by HQO that are applicable across multiple action areas. There are also services that would benefit from the development of quality standards specific to the needs of people with dementia (e.g. Adult Day Programs, clinical pathways)
This has been included to reinforce the need to examine taken-for-granted processes (e.g. clinical pathways for diabetes or orthopedic surgery, service eligibility and allocations) to ensure their applicability to people living with dementia in a community setting.
Performance measuring and
quality monitoring
This includes quality and outcome measures that tell the story of the impact of identified action areas on the lives of people with dementia.
There is a need to develop performance measures appropriate for a people living with dementia that reflect their aspiration to live well. Such measure might include length of stay in the community following diagnosis, quality of life for people living with
November 29, 2018 14
dementia and their care partners, goal attainment and death in location of choice.
Enabling technologies
This refers to digital solutions such as electronic medical records, or supportive technologies such as automated detection sensors, home automation, assistive robotics that can facilitate care as well as social inclusion and activities of daily living.
There is significant development in the area of assistive technology and artificial intelligence that has the potential to support residents of the Central East LHIN who may be living with dementia.
The MOHLTC identified the following core elements that ought to be included in the existing (current state) and planned capacity for dementia care in the LHINs:
Dementia community programs (adult day programs, overnight respite) Behavioural supports in the community Care partner education and counselling programs Diagnostic services Program components, implementation, target population, expected/known outcomes Spaces, waitlists, staffing hours Program uptake and completion rates Costs
The Central East Action Group further identified the following core elements for collection (where applicable):
Capacity (supply) – e.g. Seats/places, appointments, individuals, beds Utilization: used/available places per year (uptake) Average Length of Stay Staff to client ratios by program Service hours Location(s) Waitlist (number of people, average length of wait if available) Funding Source - % LHIN funding and % other funding (by base and one time) Average cost
All available program data has been included in this report. It should be noted that not all programs were able to supply data across each requested element.
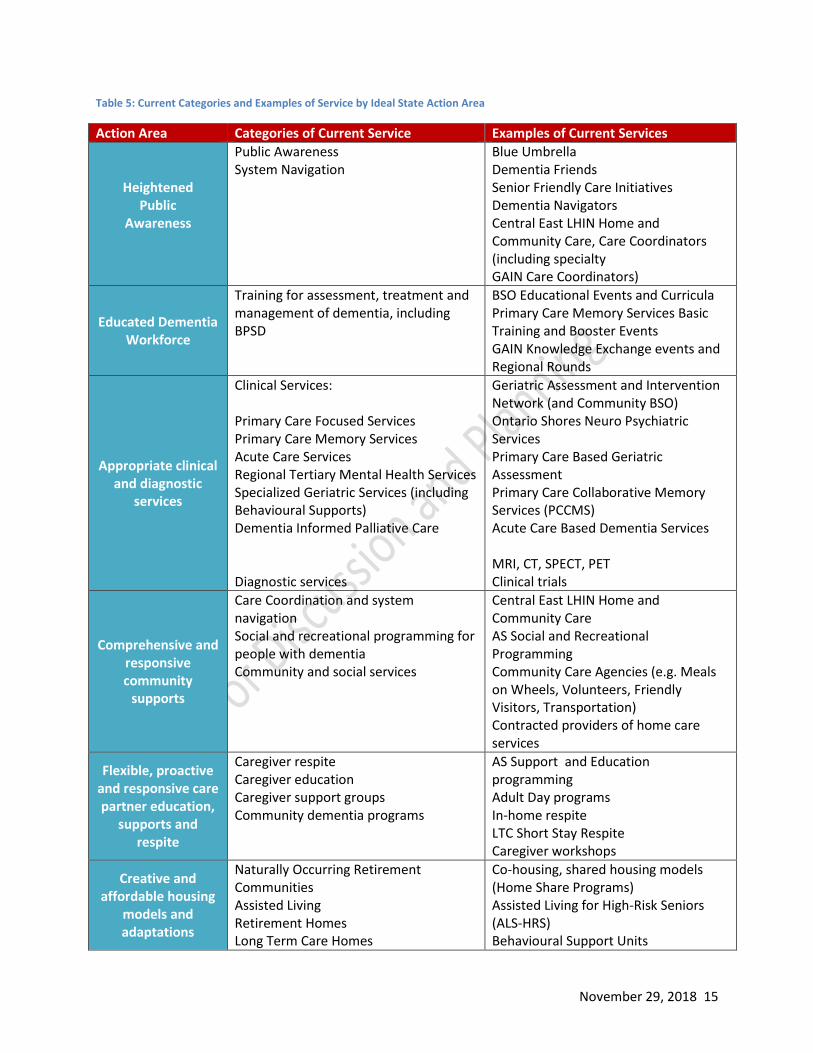
Across each of the action areas, several categories of services were identified, around which current state information was collected. The following table summarizes these services:
Phase Two: Development of the Current State View of Dementia Care (Supply & Utilization)
November 29, 2018 15
Table 5: Current Categories and Examples of Service by Ideal State Action Area
Action Area Categories of Current Service Examples of Current Services
Heightened Public
Awareness
Public Awareness System Navigation
Blue Umbrella Dementia Friends Senior Friendly Care Initiatives Dementia Navigators Central East LHIN Home and Community Care, Care Coordinators (including specialty GAIN Care Coordinators)
Educated Dementia Workforce
Training for assessment, treatment and management of dementia, including BPSD
BSO Educational Events and Curricula Primary Care Memory Services Basic Training and Booster Events GAIN Knowledge Exchange events and Regional Rounds
Appropriate clinical and diagnostic
services
Clinical Services: Primary Care Focused Services Primary Care Memory Services Acute Care Services Regional Tertiary Mental Health Services Specialized Geriatric Services (including Behavioural Supports) Dementia Informed Palliative Care Diagnostic services
Geriatric Assessment and Intervention Network (and Community BSO) Ontario Shores Neuro Psychiatric Services Primary Care Based Geriatric Assessment Primary Care Collaborative Memory Services (PCCMS) Acute Care Based Dementia Services MRI, CT, SPECT, PET Clinical trials
Comprehensive and responsive community
supports
Care Coordination and system navigation Social and recreational programming for people with dementia Community and social services
Central East LHIN Home and Community Care AS Social and Recreational Programming Community Care Agencies (e.g. Meals on Wheels, Volunteers, Friendly Visitors, Transportation) Contracted providers of home care services
Flexible, proactive and responsive care partner education,
supports and respite
Caregiver respite Caregiver education Caregiver support groups Community dementia programs
AS Support and Education programming Adult Day programs In-home respite LTC Short Stay Respite Caregiver workshops
Creative and affordable housing
models and adaptations
Naturally Occurring Retirement Communities Assisted Living Retirement Homes Long Term Care Homes
Co-housing, shared housing models (Home Share Programs) Assisted Living for High-Risk Seniors (ALS-HRS) Behavioural Support Units

November 29, 2018 16
Adaptive technology LTCHs with embedded BSO staff LTCH with secure units Retirement Homes (with Dementia Care Units) Emerging Technologies
The following sections include available service information about each category and program.
Heightened Public Awareness
Public Awareness Initiatives
The Alzheimer Societies are the lead agencies providing public information about dementia. There are currently five initiatives that support this effort.
Dementia Friendly Communities – Blue Umbrella Program: Training and recognition programs that support the development of a Dementia Friendly Community as a place where people living with dementia are understood, respected and supported; an environment where people living with dementia will be confident that they can contribute to community life.
Dementia Friends (AS Canada): A web-based national awareness campaign that is helping Canadians to learn a little about dementia, and then turn that understanding into simple actions that can improve the lives of people living with dementia.
Awareness Month Activities (January): Using media, public events and education, local Alzheimer Societies across Canada highlight educational and awareness building activities throughout the month of January.
Health and Wellness Fairs: Alzheimer Societies participate in many community health & wellness fairs to provide promote public awareness and provide education materials to those wishing to learn more about dementia.
Social Media: information and awareness is sent out via a variety of social media mediums to inform the public of dementia related activities, supports and services.
The following table illustrates the distribution of these activities LHIN-wide.

November 29, 2018 17
Table 6: Distribution by Sub-Region of Current Public Awareness Initiatives3
Central East LHIN Sub Region
Dementia Public Awareness Initiatives (Lead: Alzheimer Societies)
SN SS DW DNE NH PCC HCCKL
Dementia Friendly Communities – Blue Umbrella Program
Dementia Friends (AS Canada)
Awareness Month Activities (January)
Health and Wellness Fairs
Social Media
Red = While the AS receives LHIN funding for this functional centre it is not fully funded and the FTE is supplemented by grants, foundations and donors.
System Navigation
There are four initiatives focused on providing navigation to people living with dementia and/or frailty.
First Link is a program that gives persons with dementia, their care partners and family a direct connection to a wide variety of services and supports offered through the Alzheimer Society and within the community. In 2017, the Alzheimer Societies collectively received 452 referrals from Primary Care Collaborative Memory Services (see section “Primary Care Collaborative Memory Services for more information).
Table 7: Referral from Primary Care Collaborative Memory Services to First Link 2017/184
Measure ASDR ASPKL AST TOTAL
Primary Care Collaborative Memory Service referrals to First Link 330 111 11 452
The First Link Care Navigator coordinates and integrates supports and services around the person living with dementia and their care partner. In this direct client service role, they are the key “go-to” person for families after a dementia diagnosis, with responsibility for identifying needs, supporting self-management goals, and strengthening the communication and care planning linkages between providers and across sectors along the continuum of care.
Central East LHIN Home and Community Care (HCC) Care Coordinators are regulated health professionals who provide ongoing system navigation, support and case management expertise to roughly 44,000 patients per day, and their families, who are receiving care in the community. Care Coordinators complete regular comprehensive assessments to develop responsive care plans based on the needs and goals of patients and caregivers. This includes determining and evaluating eligibility for service; arranging and monitoring service delivery (including clinical, professional and/or personal support services); referrals to Community Support Services, Adult Day Programs and other allied community organizations (such as the Alzheimer Society);
3 Source: Alzheimer Societies Program Data
4 Source: Alzheimer Societies Program Data

November 29, 2018 18
placement counselling and admissions into Long-Term Care; facilitating caregiver respite services; and regular communication with Primary Care Providers.
GAIN Nurse Care Coordinators carry out similar functions above but hold additional specialty knowledge and expertise in geriatric assessment, to allow for greater contributions to team-based comprehensive geriatric assessment and care planning activities.
Table 8: Central East Dementia Related System Navigation Resources 2017/185
Central East LHIN Sub Region (FTEs)
Dementia Related Navigation Initiative SN SS DW DNE NH PCC HCCKL
First Link (Lead: Alzheimer Societies) 0.5 0.5 1 1 0.7 0.7 0.7
First Link Navigator Role (System Navigation) (Lead: Alzheimer Societies)
0 0 0.5 0.5 0.33 0.33 0.33
HCC Care Coordinators (Lead: Central East LHIN)6 89 0 72 0 11 21 15
GAIN Nurse Care Coordinators (Lead: Seniors Care Network/Central East LHIN)
4 2(+2) 2 1(+1) 3 3(+1) 3
TOTAL FTE by Sub-Region 93.5 2.5 75.5 2.5 15.03 24 19.03
(Unfilled Positions)
Educated Dementia Workforce
Training For Assessment, Treatment and Management of Dementia, Including Behavioural and Psychological Symptoms of Dementia (BPSD)
This section focuses on established, recurring training mechanisms (e.g. courses, programs) and does not included less formal workforce training provided through Clinical Rounds presentations or local conferences.
In the Central East LHIN, training related to the assessment, treatment and management of dementia and behavioural and psychological symptoms of dementia is regularly provided by the Central East Behavioural Supports Ontario Program and the Alzheimer Societies. There are four core programs considered part of the standard behavioural support curriculum including P.I.E.C.E.S, Gentle Persuasive Approaches (GPA), U-First and Montessori Methods. There is also additional workforce training provided by the Alzheimer Societies. Available descriptions of programs are included at Appendix 3. The volume and nature of this training is summarized in the tables below.
5 Source: Alzheimer Societies Program Data, GAIN Program Data
6 Source: Central East LHIN, HCC; note data used represents total number of Long-Stay Caseloads, as equivalent 1
Caseload = 1.0 FTE. Scarborough (SN and SS) and Durham (DW and DNE) sub-regions are combined as caseloads may cross sub-region boundaries. Excludes palliative caseloads.

November 29, 2018 19
Table 9: Regional Workforce Training Delivered by the Central East Behavioural Supports Ontario Program 2017/187
Courses8 Sessions Participants
P.I.E.C.E.S. Sessions 4 107
GPA Sessions 56 685
U-FIRST Sessions 11 148
Central East Capacity Building Sessions (Community of Practice, Mental Health First Aid For Seniors, Education Committee Events)
17 763
Total 88 1703
Table 10: Distribution by Sub-Regions of Workforce Dementia Training by Central East Alzheimer Societies 2017/18
9
Central East LHIN Sub Region
Workforce Training by Type/Course SN SS DW DNE NH PCC HCCKL
U- First*
GPA*
Other Capacity Building Training including; PSW, staff and volunteer
Anti-stigma Education - Blue Umbrella
Virtual Dementia Tour
Dementia Workforce Training Consultation and Education
Red = Not LHIN Funded
*The Alzheimer Societies deliver GPA/UFirst to the non-regulated, retirement home and CSS sector while BSO delivers this
training to the LTC and regulated sector. The Alzheimer Society does not deliver PIECES.
Table 11: Public Education Sessions by Alzheimer Society 2017/1810
Measure ASDR ASPKL AST TOTAL
# of Public Education Sessions 175 226 58 459
# of Individuals Served through Public Education (registered & NUI) 2583 2490 1597 6670
Primary Care Memory Clinic Training and Booster Training
In addition to the training identified above, 80 health professionals from the Central East LHIN, including primary care physicians, nurses, nurse practitioners, occupational therapists, social workers and others attended initial Primary Care Collaborative Memory Clinic Training in February 2016. This training program was developed by Dr. Linda Lee and includes a 15 hour didactic component, an eight hour
7 Source: Central East LHIN, Behavioural Supports Ontario Program (July 27, 2018)
8 http://brainxchange.ca/Public/Files/BSO-Resources/BETSI-Part-D-Program-Inventory-Updated-191212.aspx
9 Source: Alzheimer Societies Program Data
10 Source: Alzheimer Society Program Data
November 29, 2018 20
clinical observation and several mentored patient visits. Upon completion, trainees began to deliver or support the delivery of primary care based memory services locally.
Dr. Linda Lee and team at the Centre for Family Medicine (Kitchener) Memory Clinic follow up on initial training with an annual Booster education event, intended to reinforce concepts and bring forward emerging practices. In 2017/18, 54 health professional attended a Booster session held in Keene Ontario. An estimated 32 additional individuals have undertaken the initial Primary Care Memory Clinic Training as part of an existing team already delivering this service or new teams establishing new memory clinic sites.
Appropriate Clinical and Diagnostic Services
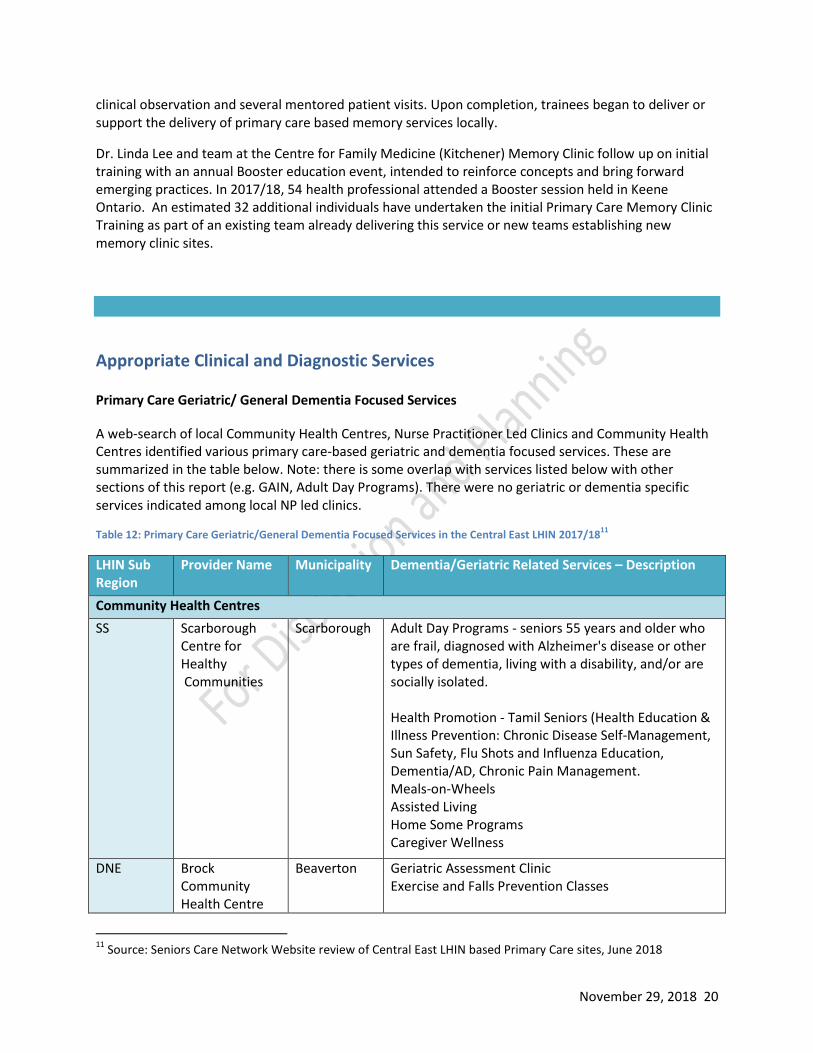
Primary Care Geriatric/ General Dementia Focused Services
A web-search of local Community Health Centres, Nurse Practitioner Led Clinics and Community Health Centres identified various primary care-based geriatric and dementia focused services. These are summarized in the table below. Note: there is some overlap with services listed below with other sections of this report (e.g. GAIN, Adult Day Programs). There were no geriatric or dementia specific services indicated among local NP led clinics.
Table 12: Primary Care Geriatric/General Dementia Focused Services in the Central East LHIN 2017/1811
LHIN Sub Region
Provider Name Municipality Dementia/Geriatric Related Services – Description
Community Health Centres
SS Scarborough Centre for Healthy Communities
Scarborough Adult Day Programs - seniors 55 years and older who are frail, diagnosed with Alzheimer's disease or other types of dementia, living with a disability, and/or are socially isolated. Health Promotion - Tamil Seniors (Health Education & Illness Prevention: Chronic Disease Self-Management, Sun Safety, Flu Shots and Influenza Education, Dementia/AD, Chronic Pain Management. Meals-on-Wheels Assisted Living Home Some Programs Caregiver Wellness
DNE Brock Community Health Centre
Beaverton Geriatric Assessment Clinic Exercise and Falls Prevention Classes
11
Source: Seniors Care Network Website review of Central East LHIN based Primary Care sites, June 2018

November 29, 2018 21
DNE Carea Community Health Centre
Oshawa GAIN Community Team
NC Port Hope Northumberland Community Health Centre
Port Hope GAIN Community Team Primary Care Memory Clinic Community Health Worker (Some of the classes for adults and seniors include Active Fit and Fun for those 55+, Nordic Pole Walking, Yoga and Pilates)
HCCKL Community Care City of Kawartha Lakes
Lindsay Adult Day Programs Care for Caregivers (In-Home Respite, Meals-on-Wheels) Caregiver Support Groups Elder Abuse Awareness & Education Exercise for Seniors - SAGES Exercise for Seniors - Closing the Gap GAIN Community Team
Family Health Teams
SN East GTA FHT Scarborough General Intake/Assessment: Full assessment by OT or RN, referral for groups, home assessment, or individual follow up with OT, Pharmacist, Dietitian, or Social Worker as needed. Falls Prevention Workshop Older Adult Exercise Program Memory and Aging Group Mild Cognitive Impairment Memory Group Mental Health & Aging Workshop Nutrition & Aging Workshop Caregiver Support Group
NC Northumberland Hills FHT
Cobourg Exercise Classes & Falls Prevention Program Seniors Assessment Clinic Program
NC Trent Hills FHT Campbellford PATH Program - a health care clinic for older people designed to help patients and families cope with the challenges of chronic illness.
HCCKL City of Kawartha Lakes FHT
Kawartha Lakes
Memory Clinic (Also see section “Primary Care Memory Services”)
HCCKL Haliburton Highlands FHT
Haliburton RN led programming providing education, consultation, referral and memory assessments.
Primary Care Collaborative Memory Clinics/Services
The Primary Care Collaborative Memory Clinics (PCCMS) or Services (PCCMS) are interprofessional (IP) teams consisting of social workers, nurses (some with behavioural supports experience) and occupational therapists, working collaboratively with primary care physicians in various clinic locations across the Central East LHIN. Physicians and teams offering this service receive training and carve out

November 29, 2018 22
time from usual primary care to offer dedicated clinical days specific to memory assessment and dementia care. Teams may also include pharmacists in some locations. The IP team and the physicians work together to provide assessment, early diagnosis, treatment and support of daily challenges associated with memory loss.
There are eight Primary Care Collaborative Memory Services/Clinics operating in the Central East LHIN.
Table 13: Primary Care Collaborative Memory Services in the Central East LHIN
LHIN Sub Region
Practice Name LHIN Supported (Y/N) Serving Home visits
Physician Lead
SS East GTA Family
Health Organization/ Carefirst FHT
Yes - IP Team funded by LHIN and hosted
through ASDR
Broader Community
Y Dr. Seung-Jun Lee/
Dr. Kinsey Lam
DNE Clarington Family
Health Organization
Yes - IP Team funded by LHIN and hosted
through ASDR
Broader community
Y Dr. Vincent Ho
DNE Oshawa Clinic Family Health Organization
Yes - IP Team funded by LHIN and hosted
through ASDR
FHO Patients only
Y Dr. Sina Sajed
NC Trent Hills FHT No – IP Team drawn
from existing FHT staff FHT Patients
only N Dr. Jamie Read
NC Northumberland
Family Health Team
Yes - IP Team funded by LHIN and hosted
through ASPKLNH and PHCHC
FHT Patients only
Y Dr. Wang Xi
NC Port Hope
Community Health Centre
Yes - IP Team funded by LHIN and hosted
through ASPKLNH and PHCHC
Broader Community
Y Vacant (coverage by Mary Ann Hicks, NP)
HCCKL Haliburton Highlands Family Health Team
Yes - IP Team funded by LHIN and hosted
through ASPKLNH and HHHS
FHT Patients only
Y Dr. Tina Stephenson
HCCKL City of Kawartha
Lakes Family Health Team
No –IP Team drawn from existing FHT staff
FHT Patients only
Dr. Eric Reddy
The following table reflects service volumes for PCCMS in 2017/18 (to March 31, 2018). Programs marked with (*) were newly operational in2017/18.

November 29, 2018 23
Table 14: PCCMS Service Volumes by Team 2017/1812
LHIN Sub Region
Practice Name
# Appts. Avail. per year
# Referrals
# New Patients Seen
# Follow-up Patients Seen
Utilization (Total patients seen/appts.)
Referral Rate to specialist (patients referred/total patients seen)
SS East GTA FHO/ Carefirst FHT
204 113 108 69 87% 12%
DNE Clarington FHO 288 116 109 120 80% 10%
DNE Oshawa Clinic
FHO 378 209 144 169 83% 5%
NC Trent Hills FHT* 7 7 7 0 100% 2%
NC Northumberland FHT*
42 51 33 4 88% 3%
NC Port Hope CHC* 36 38 32 8 111% 10%
HCCKL Haliburton Highlands FHT*
57 48 46 9 96% 13%
HCCKL City of Kawartha Lakes FHT
96 128 90 57 153% 4%
Total 1108 710 569 436 91% Range 2-13%
PCCMS team may offer between one and four clinical days per month. Most teams are booking new appointments several months into the future, indicative of growing wait times.
Acute Care Services
The Action Group noted difficulty in identifying the population living with dementia from other populations who use acute care services. This is because patients with dementia often present at the hospital with other acute conditions. In 2017/18, in the Central East LHIN, there were 3912 patients with a dementia diagnosis as any ‘type13’ in the coded hospital data. Of these patients, 60614 had a Case Mix Group (CMG) of dementia. CMG15 is a means of classifying patients in the acute care sector who have similar characteristics. The remaining patients were grouped into a different CMG.
12
Source: Program Data 13
Type may include: Main Problem Diagnosis (MRDX); Pre-Admit Co-morbidity (Type 1): Post-Admit Co-morbidity (Type 2); Secondary Diagnosis (Type 3) 14
Inpatient Data: CIHI DAD database via Intellihealth. Inclusions: Fiscal Year 2017-2018; LHIN of Patient = Central East. Treating facility may be located in another LHIN; Any diagnosis ICD-10 codes in F01^ (Vascular Dementia), F02^ (Dementia in Other Specified Neurological Conditions), F03^ (Unspecified Dementia), G30^ (Alzheimer's Disease). Codes provided by CCO. 15 Source: https://www.cihi.ca/en/submit-data-and-view-standards/methodologies-and-decision-support-
tools/case-mix

November 29, 2018 24
In 2017/18, in the Central East LHIN there were 3318 emergency department patients seen with a dementia diagnosis recorded at any location in the record. Of these patients, 71916 of these had a Main Problem Diagnosis (MPDx) of dementia. The remaining patients presented with a different MPDx
The top 20 CMGs and MPDx for these patients are listed in Table 15.
Table 15: Top 20 CMGs in Inpatients and MPDX in Emergency Room Patients who have Dementia (all types) 2017/1817
CMG - Inpatients Patient Volume MPDx – Emergency Department
Patient Volume
(810) Palliative Care 279 (N390) Urinary Tract Infection, Site Not Specified 115 (135) Aspiration Pneumonia 173 (J189) Pneumonia, Unspecified 65 (487) Lower Urinary Tract Infection 167 (A419) Sepsis, Unspecified 58 (138) Viral/Unspecified Pneumonia 160 (J690) Pneumonitis Due To Food And Vomit 49 (196) Heart Failure Without Coronary Angiogram 158 (R410) Disorientation, Unspecified 48 (671) Organic Mental Disorder 138 (R53) Malaise And Fatigue 43 (139) Chronic Obstructive Pulmonary Disease 119 (F059) Delirium, Unspecified 41 (811) General Symptom/Sign 108 (R296) Tendency To Fall, Not Elsewhere Classified 38 (727) Fixation/Repair Hip/Femur 107 (E860) Dehydration 37 (654) Other/Unspecified Sepsis 105 (R509) Fever, Unspecified 36 (026) Ischemic Event Of Central Nervous System 99 (I500) Congestive Heart Failure 34 (477) Renal Failure 79 (R64) Cachexia 32 (726) Hip Replacement With Trauma/Complication Of Treatment 67
(Z043) Examination And Observation Following Other Accident 31
(254) Gastrointestinal Hemorrhage 59 (R55) Syncope And Collapse 27 (194) Myocardial Infarction/Shock/Arrest Without Coronary Angiogram 52 (K922) Gastrointestinal Haemorrhage, Unspecified 24 (136) Bacterial Pneumonia 51 (S099) Unspecified Injury Of Head 23 (202) Arrhythmia Without Coronary Angiogram 50
(I64) Stroke, Not Specified As Haemorrhage Or Infarction 20
(040) Seizure Disorder, Except Status Epilepticus 44 (S72100) Intertrochanteric Fracture, Closed 19 (765) Single Intracranial Injury 43 (R5688) Other And Unspecified Convulsions 18 (809) Awaiting Placement 37 (N179) Acute Renal Failure, Unspecified 17
16
Emergency Department Data: CIHI NACRS Database via Intellihealth. Inclusions: Fiscal Year 2017-2018; LHIN of Patient = Central East. Treating facility may be located in a different LHIN; Any Problem ICD-10 codes in F01^ (Vascular Dementia), F02^ (Dementia in Other Specified Neurological Conditions), F03^ (Unspecified Dementia), G30^ (Alzheimer's Disease). Codes provided by CCO. 17
Source: Central East LHIN, Decision Support (October 26, 2018)

November 29, 2018 25
Alternate Level of Care (ALC)
The patient population living with dementia has a very high percentage of ALC days. Among inpatients
with CMG 670 (Dementia), by sub-region, Peterborough City and County (83.92%) and Northumberland
County (80.76%) had the highest rates of ALC, while Scarborough North (54.94%) and Haliburton County
and City of Kawartha Lakes (60.67%) had the lowest % ALC in this time period (2017/18).
Table 16: Alternate Level of Care (ALC) Analysis – Central East LHIN Dementia Inpatients, 2017-201818
Inpatients with CMG 670
(Dementia) Inpatients with
Dementia Comorbidity* All Inpatients**
Total Length of Stay (LOS) 25445 days 62017 days 750685 days
Alternate Level of Care (ALC) LOS 18259 days 31846 days 133782 days
% ALC Days 71.76% 51.35% 17.82%
Acute care service providers (e.g. hospitals) do not operate discrete dementia programming. However, across the Central East LHIN, all hospital provide a number of Senior Friendly Care Initiatives, and many of these initiatives also serve the needs of people living with dementia who are hospitalized. Table 17 provides a summary of Senior Friendly Care Initiatives by hospital.
In effort to reduce ALC burden, the Home and Community Care (HCC) division of the Central East LHIN provides on-site Care Coordination support for the majority of hospitals within the region, and remote support for any remaining acute care facilities. These hospital-based Care Coordinators actively collaborate with patients, families and hospital partners to provide discharge, in-home and/or Long-Term Care counselling, arrange services and facilitate transfers to the appropriate discharge destination.
18
Source: Central East LHIN, Decision Support (October 26, 2018)

November 29, 2018 26
Table 17: Senior Friendly Initiative Summary by Central East LHIN Hospital19
19
Source: Seniors Care Network Senior Friendly Care Committee
CMH HHHS LH NHH OS PRHC RMH SRH Total
Organizational Support
1 X X X X X X X X 82 X X X X X X X X 83 X X X X X X X 74 X X X X X X X 75 X X X X X X X 7
Processes of Care
6Delirium X X X X X X X X 8Functional Decline X X X X X X 6
7 GAIN X X X X X X X X 88 GEM X X X X X 5
9 Acute Care for Elders (ACE) unit X 110 GERI Unit X X 211 Integrated Care of the Elderly Unit X X 212 Geriatric Assessment and Behavioural Unit (GABU) X X 213 Interim LTC program/CCC and Functional Enhancement Unit X X 214 Assess & Restore X X X 3
15 Geriatric Activation Programme (GAP) X X 216 Geri Acute X X 217 Alternate Level of Care (ALC) Programme X X X X X 518 Mobilization Programs (e.g., MOVE ON, Move and Walk) X X X X X X X 719 Recreation Program X X X X X X X X 8
20 Designing programs to meet the needs of Seniors (e.g., restorative care and inpatient rehabilitation, Transitional Restorative Care program)
X X X X X X X 7
21 X X X X X X X X 8
22 Falls X X X X X X X X 823 Least Restraint X X X X X X X X 824 Wound care (e.g., Save our Skin Team) X X X X X X X 725 Polypharmacy review for older adults X X X X X X X 726 Purposeful rounding for older adults X X X X X X 627 Delirium, Dementia and/or Depression X X X X X X 628 X X X X 429 Internal Psychogeriatric Programmes (Memory Clinic) X X X X X 530 X X X X X 531 Memory Clinic X X 232 Geriatric Consultation X X X X 433 Geriatric Neuropsychiatry Program - Outpatient Service X X X X X X X 734 X X X X X X 635 X X X X X X 636 FHT Collaboration re: Seniors Care X X X X X 537 X X 2Emotional and Behavioural Environment
38 X X X X X X X 7
39 Elder Abuse Initiatives X X X X X X X 7Ethics in Clinical Care and Research
40 SF focus in research and ethics where appropriate X X X X X X 641 Research Chair in Community Dementia X 1Physical Environment
42 Environmental Modification X X X X X X X 743 Signage X X X X X X X 744 Elder Friendly Equipment (e.g., pocket talkers, magnifiers) X X X X X X X X 8
Volunteer Programs (e.g., Call Ahead for Volunteer Assistance (CAVA), Hospital Elder Life Program (HELP), Mealtime Assistance Program)
Central East Senior Friendly Care Initiatives - Summary - August 2017
Provincial Initiatives
IP Programs
Continence (e.g., Catheter-Associated Urinary Tract Infection, Catheter Out Program, Acquired UTI Protocol )
Community Referral for Assess and Restore
BSO Initiatives (e.g., Montessori Method, GPA, PIECES training)
Certified/Designted Specialized Geriatric Programs (e.g., NICHE, PATH, BPSO)
Transitions (e.g., HINT, PATH-NHH)
External Psychogeriatric Programs (e.g., PASE, Ontario Shores, GAIN, Memory Clinic)
Specialized Geriatrics Units
Elder/SFH Care Steering Committee or SFH focus on various committeesSFH Clinical Manager/LeadEducation to build gerontological expertise/practiceInventory of SFH initiativesHealth promotion materials focused on seniors

November 29, 2018 27
Regional Tertiary Geriatric Mental Health Services
In 2017/18, Ontario Shores Centre for Mental Health Sciences, the Peterborough Regional Health Centre and the Scarborough and Rouge Hospital provided clinical services to people with dementia through in-patient and out-patient services. These services are summarized in the following sections.
Outpatient Services
Ontario Shores Centre for Mental Health Sciences (OSCMHS) Durham Region Psychogeriatric Resource Consultation (DRPRC) Program is a Ministry of Health funded outreach program designed to meet the educational needs of health care staff working in Long- term care facilities, community service agencies, and homecare organizations. The Geriatric Long Term Care Outreach Team (GLTCOT) is for residents of long-term-care facilities who have a psychiatric concern that is either treatment resistant or complex in nature presenting with one or more of the following: cognitive changes, behavioural changes, mood changes, anxiety or psychotic symptoms.
The Specialized Neurocognitive Disorders Clinic (SNDC), formally called the Memory Clinic, is a diagnostic clinic for older adults with suspected dementia or with new onset of cognitive impairment where the diagnosis is unclear, presentations are unusual or cognitive difficulties may co-exist with a psychiatric disorder, complex medical problems or drug interactions.
Peterborough Regional Health Centre (PRHC)
Psychiatric Assessment Services for the Elderly (PASE) is an outreach program that offers geriatric mental health assessment, consultation and education services, for people 65 and older. PASE clinicians and psychiatrists provide direct assessment and consultation for clients in long-term care facilities, retirement homes, and in community settings with a primary care referral. The program is separately mandated to offer Psychogeriatric Resource Consultant (PRC) services for the HKPR district.
Scarborough and Rough Hospital (SRH)
The Psychogeriatric Outreach Program (POP) and Geriatric Mental Health Outreach Team (GMHOT) conduct assessments and provides reports with recommendations for nursing home staff to help them manage patients who are presenting with concerning behaviours, including agitation, aggression, depression, resistance to care, psychotic symptoms or other indications of mental illness. The service is available to address the needs of patients and staff in the early stages of managing difficult behaviour in an attempt to avoid hospitalization.
Scarborough Psychogeriatric Resource Consultants (PRC) hosted at Providence Care and the Scarborough and Rouge Hospital as part of the Regional Geriatric Program (RGP) of Toronto is a Ministry of Health funded outreach program designed to meet the educational needs of health care staff working in Long- term care facilities, community service agencies, and homecare organizations.

November 29, 2018 28
Table 18: Summary of Geriatric Psychiatry and Mental Health Outpatient Services 2017/1820
Provider Service # of appointment available/yr.
# of unique patients served
# visits
% Actual Utilization
# people on waitlist
Average length of wait (days) (Visits/appts.
)
OSCMHS DRPRC Workload is not captured in visits.
OSCMHS GLTCOT 1200 1316 110% 28 25
OSCMHS SNDC 940 809 86% 47 171
PRHC PASE 440021 848 4568 104% 0 25.37
SRH POP n/a 190 2884 -- 6 3
SRH GMHOT n/a 380 2010 -- 0 3
Inpatient Services
Ontario Shore Centre for Mental Health Sciences
The Geriatric Dementia Unit (GDU) is a 23-bed inpatient unit at Ontario Shores Centre for Mental Health Sciences (Ontario Shores) that provides specialized services to meet the mental health needs of patients, usually over the age of 65, with dementia and challenging behaviours.
The Geriatric Transitional Unit (GTU) is a 20-bed inpatient; 59-day length of stay, unit at Ontario Shores Centre for Mental Health Sciences (Ontario Shores) that provides specialized services to meet the mental health needs of individuals, usually over the age of 65, with dementia and presenting with challenging behaviour or severe psychiatric symptomatology. This includes psychogeriatric resources to address the assessment, management and transitional care needs of the client with the goal of reintegration to community or long term care.
The Geriatric Psychiatry Unit (GPU) is a 25-bed inpatient unit at Ontario Shores Centre for Mental Health Sciences (Ontario Shores) that provides specialized services to meet the complex mental health needs of seniors, usually over the age of 65, with serious mental illness including individuals who are resistant to treatment.
20
Source: Program Data 21
PASE utilizes a unique measure of Service Provider Interactions (SPIs). SPIs are related to, but different from, visits and the program reports both “SPIs” as well as “visits” to the LHIN. SPIs are all of the total patient encounters (face-to-face and non-face-to-face) that staff and physicians engage in. This enables data capture of intensity of service, recording the important distinction between one health professional seeing a patient in a day or three health professionals seeing a patient in the day. The program has identified this as a more accurate measure of the patient-care activity in a program, and is potentially a more accurate estimate of workload per FTE. In contrast, “visits” is data that has had duplicate encounters deleted. Thus, if a case manager and a psychiatrist see a patient together only one visit is counted, where two SPIs would be counted. Measures of service intensity are valuable in the care of older adults with complex health concerns. The difference in utilization rates (104% vs 91%) between SPI and visits suggests that a visit metric may not accurately reflect the nature of complex frail seniors/dementia care.
November 29, 2018 29
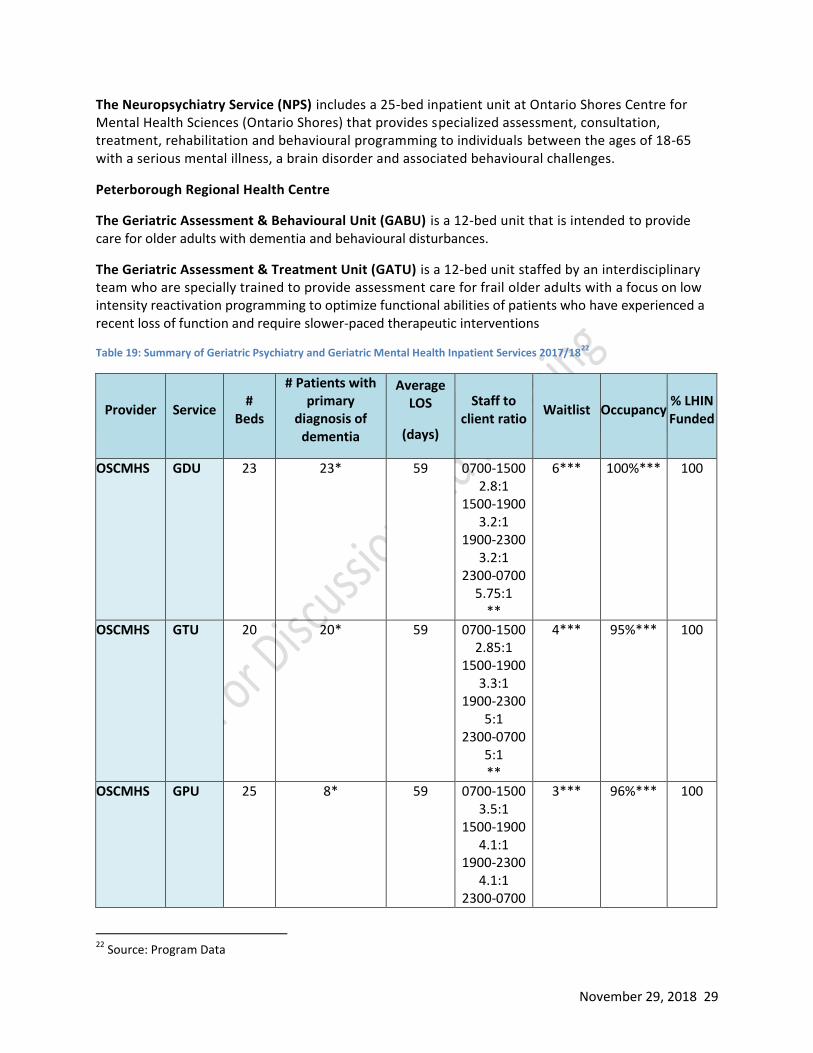
The Neuropsychiatry Service (NPS) includes a 25-bed inpatient unit at Ontario Shores Centre for Mental Health Sciences (Ontario Shores) that provides specialized assessment, consultation, treatment, rehabilitation and behavioural programming to individuals between the ages of 18-65 with a serious mental illness, a brain disorder and associated behavioural challenges.
Peterborough Regional Health Centre
The Geriatric Assessment & Behavioural Unit (GABU) is a 12-bed unit that is intended to provide care for older adults with dementia and behavioural disturbances.
The Geriatric Assessment & Treatment Unit (GATU) is a 12-bed unit staffed by an interdisciplinary team who are specially trained to provide assessment care for frail older adults with a focus on low intensity reactivation programming to optimize functional abilities of patients who have experienced a recent loss of function and require slower-paced therapeutic interventions
Table 19: Summary of Geriatric Psychiatry and Geriatric Mental Health Inpatient Services 2017/1822
Provider Service #
Beds
# Patients with primary
diagnosis of dementia
Average LOS
(days)
Staff to client ratio
Waitlist Occupancy % LHIN Funded
OSCMHS GDU 23 23* 59 0700-1500 2.8:1
1500-1900 3.2:1
1900-2300 3.2:1
2300-0700 5.75:1
**
6*** 100%*** 100
OSCMHS GTU 20 20* 59 0700-1500 2.85:1
1500-1900 3.3:1
1900-2300 5:1
2300-0700 5:1 **
4*** 95%*** 100
OSCMHS GPU 25 8* 59 0700-1500 3.5:1
1500-1900 4.1:1
1900-2300 4.1:1
2300-0700
3*** 96%*** 100
22
Source: Program Data

November 29, 2018 30
6.25:1 **
OSCMHS NPS 25 8* 59-120 (depending
on diagnosis)
0700-1500 3.1:1
1500-1900 3.5:1
1900-2300 4.1:1
2300-0700 5:1 **
0*** 100*** 100
PRHC GATU 12 (flex up to 28)
46 Days 5:1 Night 9:1
1-2 weeks 99% 100
PRHC GABU 12 59 6:1 1-2 weeks 99% 100 * Provided by OSCMHS as a snapshot from August 20, 2018 ** Includes registered and non-registered staff *** Provided by OSCMHS as a snapshot from September 10, 2018
Community Focused Specialized Geriatric Services
Behavioural Supports Ontario (Community)
Behavioural Supports Ontario (BSO) refers to a program that relies on trained health professionals and programming to help older people with challenging behaviours resulting from complex mental health, addictions, dementia and other neurodegenerative issues. In the Central East LHIN, BSO provides staff and training in the community, in collaboration with GAIN and the PCCMS, and in Long Term Care (LTC). Table 18 highlights the referrals received across all programs and the number of individuals living with responsive behaviours and their families supported in the community by the program. Table 20: Referrals, Individuals and Families supported by Community BSO in 2017/18
23
Community (GAIN BSO RPNs & PCCMS BSO Clinicians)*
Q1 Q2 Q3 Q4 Average per
Quarter
Total # of accepted referrals 168 116 134 163 145
Total # of individuals supported 411 388 397 441 409
Total # of individual family members/ informal care partners supported
519 459 455 508 485
*Data for one GAIN site not included for Q1, Q2 & Q4.
23
Source: Program Data

November 29, 2018 31
The Geriatric Assessment and Intervention Network (GAIN)
GAIN is a network of 12 hospital and community-based interprofessional teams providing comprehensive assessments and creating care plans with patients to optimize function and independence and keep older people living at home.
GAIN focuses on the: (1) reduction of distress to the person and the family; (2) improvement and/or maintenance of function; (3) optimization of the individual’s capacity for autonomous living; and (4) maximization and maintenance of the highest possible level of independence.
GAIN teams provides both clinic and home-based (in private homes or retirement homes) clinical services to older adults with frailty issues and who are living with multiple, complex medical problems including one or more geriatric syndromes (e.g., cognitive impairment, decreased function, falls or risk of falls, impaired mobility, incontinence, and/or multiple medications).
GAIN teams provide service to older adults who are experiencing changes in their support needs, who have safety concerns, or psychosocial and mental health concerns or who are frequent health service users.
The overall program goal is to assist older adults to remain in their homes for as long as possible.
Capacity and Utilization
GAIN teams collectively make approximately 28000 appointments available to patients each year. Each team may make available between 1550 and 4300 appointments annually. This variation reflects:
The number of Full Time Equivalents (FTEs) on the team The stage of development of the team (e.g. experienced vs novice team members) and staff
turnover Degree of implementation of standardized processes Availability of geriatrician support, which ranges from daily support to two days per month.
Table 21 compares the number of appointments GAIN teams collectively make available against actual visits carried out by teams in each sub-region. Table 21: Number of Available and Actual GAIN Appointments by Sub Region 2017/18
24
LHIN Sub Region
# of Available Appointments/Year
2017/18 Visits25 (Actual)
% Actual Utilization
SN 7100 6973 98%
SS 4450 4741 107%
DW 1900 2505 132%
24
Source: Program Data 25
As of July 1, 2017, GAIN teams counted more than one visit per day per patient as follows: One visit is counted for each encounter regardless of the number of GAIN clinicians/team members present, the number of family members/caregivers present or the length of time of the encounter. For example, if 2 BSO clinicians see a patient together, only one BSO clinician records the visit. It is assumed that a Comprehensive Geriatric Assessment (CGA) will include 2-3 clinicians. A CGA may take 1-2 visits. Each visit to complete the CGA is counted as 1 visit, regardless of how many clinicians participate. Subsequent to the CGA, all additional visits are counted. For example, if a patient comes into a clinic in the morning and a clinician goes to the home in the afternoon this is counted as two visits.

November 29, 2018 32
DNE 2250 2495 111%
NC 4400 5767 131%
PCC 4187 4043 97%
HCCKL 3750 3997 107%
Total 28037 3052126 109%
Table 22 reflects available appointments and actual visits (e.g. completed appointments) in relation available staffing. Table 22: GAIN Visits by FTE 2017/18
27
LHIN Sub Region
# of Available Appointments/Year
2017/18 Visits
(Actual)
# Teams
# FTEs Ratio of
Appoint./FTEs (Budget)
Ratio of Visits/FTE (Actual)
% Difference
SN 7100 6973 2 16 444 436 -2%
SS 4450 4741 2 18 247 263 7%
DW 1900 2505 1 7.4 257 339 32%
DNE 2250 2495 1 10 225 250 11%
NC 4400 5767 2 14 314 412 31%
PCC 4187 4043 2 14 299 289 -3%
HCCKL 3750 3997 2 15 250 266 7%
Total 28037 30521 12 94.4 319 323 1%
Caseload Beginning in September 2017, GAIN commenced the collection of a total caseload metric. This metric reflects the ongoing nature of the care provided to patients and the role of team-based intensive case management as a support to older patients living with frailty in the community. The GAIN Caseload uses the following definition “a patient is deemed to be on the GAIN caseload if he/she has had a visit within the previous 12 (rolling) month period”28. This metric is a rolling value, calculated monthly by identifying and counting the unique patient identifiers occurring in the last 12 months. Note, while not all patients receiving intensive case management have a diagnosis of dementia, it is estimated that the majority do. Table 23: GAIN Total Caseload by Team and Month 2017/18
29
LHIN Sub Region
Team Sept Oct Nov Dec Jan Feb March
SN Carefirst 140 139 148 140 141 159 178 SN SPLC 411 428 444 450 457 456 454
26
This represents an increase of 6% from 2016/17 27
Source: Program Data 28
GAIN Data Dictionary 2018-19 (April 24, 2018) 29
Source: Program Data

November 29, 2018 33
SS SRH-Centenary 812 815 800 900 1042 1164 1271 SS SRH-General 1025 1004 992 1110 1260 1424 1608
DW Carea 305 347 368 384 473 460 470 DNE Lakeridge Health 821 776 812 815 801 803 771 NC Trent Hills 127 131 143 166 178 187 235 NC Port Hope CHC 353 353 341 337 324 331 328
PCC PRHC hospital and
community teams (2) 1033 1020 1012 995 995 986 975
HCCKL CCCKL 351 388 424 449 463 479 498 HCCKL HHHS 188 191 192 195 197 198 199
Total GAIN Caseload 5566 5592 5676 5941 6331 6647 6987
Currently, length of stay cannot be routinely collected in GAIN. Evaluation data collected in GAIN in 2017 showed wide variation in length of stay among patients receiving intensive case management, ranging from 20 to 580 days.
Table 24: Location(s), Service hours and Wait List by GAIN Team
30
LHIN Sub Region Locations Service Hours 90th % Wait time31
(days) (as of March 2018)
SN Carefirst M-F 8-4 79
SN SPLC M-F 830-5 44
SS SRH-Centenary M-F 8-4 118
SS SRH-General M-F 8-4 72
DW Carea M-F 8-6 132
DNE Lakeridge Health M-F 8-4 181
NC Trent Hills M-F 8-4 123
NC Port Hope CHC M-F 8-4 87
PCC PRHC hospital and community
teams (2) M-F 8-6 172
HCCKL CCCKL M-F 8-4 64
HCCKL HHHS M-F 8-4 93
For patients seen in GAIN and diagnosed or identified with dementia, GAIN tracks the dementia stage, as determined upon the completion of the comprehensive geriatric assessment (CGA). Figure 5 illustrates the trends in dementia stage, as evaluated using the Global Deterioration Scale32 seen across the program in the past two years.
30
Source: Program Data 31
90% Wait Time = The maximum wait time in days that 90% of patients wait for a first appointment 32 Source: Reisberg B (1988). Functional assessment staging (FAST). Psychopharmacology bulletin: 24: 653-659.

November 29, 2018 34
Figure 5: Number of GAIN Patients at each Dementia Stage (Past Two Years)33
The GAIN program is 100% funded by the Central East LHIN. In 2017/18 the GAIN program was
supported by the LHIN with $11,103,529.00 in total operational funds.
Based on the 2017/18 funding and actual volume data, an estimated cost for each patient on the GAIN caseload (using the final 2017/18 caseload value of 6987) is $1589.17. The average per visit cost is $363.80. Many teams are currently operating below these averages.
33
Source: Program Data
0
50
100
150
200
250
Q116/17
Q216/17
Q316/17
Q416/17
Q117/18
Q217/18
Q317/18
Q417/18
Nu
mb
er
Stage 1 Stage 2 Stage 3 Stage 4
Stage 5 Stage 6 Stage 7
Global Deterioration Scale13 (Stages) 1. Normal Cognition, Function intact 2. Subjective complaints only 3. Mild Cognitive Impairment (e.g. difficulty with high
level tasks, such as planning a dinner party) 4. Mild dementia (e.g. difficulty remembering current
events or recent events. IADLs impaired) 5. Moderate dementia (e.g. difficulty remembering
Prime Minister/US President, Re-wears clothes - wearing the same clothes day after day)
6. Severe dementia (e.g. difficulty remembering names of first degree relatives (children, spouse), BADLs impaired
7. Very severe dementia (e.g. non-verbal, non-ambulatory)

November 29, 2018 35
Diagnostic Services
The Fourth Canadian Consensus Conference on the Diagnosis and Treatment of Dementia34 recommended:
Although neuroimaging is not required in all persons with cognitive impairment, consistent with previous recommendations, it is indicated in many patients presenting to [Family Physicians] FPs. Of relevance to FPs is the additional indication for structural neuroimaging: a computed tomography scan or magnetic resonance imaging is indicated in the assessment of a person with cognitive impairment if the presence of unsuspected cerebrovascular disease would change clinical management. Positron emission tomography metabolic amyloid imaging (using fludeoxyglucose F 18), functional magnetic resonance imaging, and magnetic resonance spectroscopy are intended only for specialized clinical and research settings. (p. 436).
Since CT and MRI are utilized routinely for diagnosis in dementia care, information about these services is included in the tables below.
Table 25: 2017-18 Computed Tomography (CT) Machines Inventory Refresh Central East LHIN35
Sub-Region
Hospital CT Machine Detail
Number of Machines
Base CT Operating Hours
Number of CT Procedures Completed
Weekdays (DAYS / EVENINGS) Hours of Operation
Weekends (DAYS / EVENINGS) Hours of Operation
Scarborough and Rouge 10,996 63,457
SN Birchmount Site 1 X X
SN Centenary Site 1 X X
SS General Site 2 X X
Lakeridge Health 10,918 54,094
DW Ajax Site 1 X X
DNE Oshawa site 1 X X
DNE Bowmanville site 1 X X
NC Northumberland Hills 1 3,935 10,761 X X
PCC Peterborough Regional Health Centre
1 6,015 24,793 X X
HCCKL Campbellford Memorial 1 1890 3385 X X
HCCKL Ross Memorial 1 2,242 10,563 X X
Total 11 35,996 167,053
34
Moore et al. (2014). Fourth Canadian consensus conference on the diagnosis and treatment of dementia. Canadian Family Physician, 60, 433-438. Retrieved from http://www.cfp.ca/content/cfp/60/5/433.full.pdf 35
Source: Central East LHIN, Finance and Risk Management Unit (September 5, 2018)

November 29, 2018 36
Table 26: 2017-18 Magnetic Resonance Imaging (MRI) Machines Inventory Refresh Central East LHIN36
Sub-Region
Hospital MRI Machine Detail
Number of Machines
Base MRI Operating Hours
Number of MRI Procedures Completed
Weekdays (DAYS / EVENINGS, and may offer nights) Hours of Operation
Weekends (DAYS / EVENINGS) Hours of Operation
The Scarborough and Rouge 12,868 24,667 X X
SN Birchmount Site 1 X X
SN Centenary Site 1
SS General Site 1 X X
Lakeridge Health37 11,911 23,338 X X
DW Ajax Site 1 X X
DNE Oshawa site #1 1
DNE Oshawa site #2 1 X X
NC Northumberland Hills 1 3,536 7,495 X X
PCC Peterborough Regional Health Centre
1 5,028 8,666 X X
HCCKL Ross Memorial 1 3,290 6,172 X X
Total 9 36,633 70,338
The Central East LHIN does not currently offer Positron Emission Tomography (PET). This service is offered in other LHINs (e.g. Champlain, HNHB, NW, SW, and TC). Single Photon Emission Computed Tomography (SPECT) is not in common use for dementia care in the Central East LHIN.
Clinical Trials
During the dementia capacity planning consultations, it was identified that there is limited access in the Central East LHIN to clinical trials for dementia-related pharmacological or other treatments. This was seen as a barrier to innovative quality care. There is also no agreement among dementia providers about mechanisms to provide access to clinical trials region-wide. Currently, the Kawartha Centre is the only clinical trial site for phase 2 and 3 pharmaceutical research in dementia in the Central East LHIN. The Kawartha Centre is part of the C5R Consortium of Canadian Centres involved in Clinical Cognitive Research, a consortium of 20 sites across Canada conducting pharmaceutical trials, concurrent international research, small (phase 2) and large (phase 3) cohort trials including double blind placebo controlled studies, in the area of dementia and Alzheimer disease38.
36
Source: Central East LHIN, Finance and Risk Management Unit (September 5, 2018) 37
Lakeridge Health as one MRI at their Ajax Pickering site, and two MRIs at their Oshawa site. 38
Source: The Kawartha Centre

November 29, 2018 37
Comprehensive and Responsive Community Supports
Home and Community Care
The Home and Community Care (HCC) division of the Central East LHIN provides a broad range of community-based health and social support programs to members of the community. In addition to a number of specialty programs targeted toward specific patient groups or populations, a large component of HCC are frontline Care Coordinators who provide ongoing system navigation, support and case management expertise for patients and their caregivers in the community.
While Care Coordinators do not exclusively serve patients with Dementia, patients are grouped into caseloads according to level of impairment, stability and predictability of health conditions, and risk for deterioration. While patients with dementia are represented on all caseloads, patients with more significant health or social care needs, frailty or who are living with moderate-advanced Dementia are managed on smaller Complex (CO) caseloads wherein they receive more intensive case management, more frequent reassessments and are eligible for higher levels of service. It is estimated that the majority of patients on Complex caseloads have a diagnosis of dementia and/ or frailty. Patients with dementia represented on the remaining Community Independence (CI) and Chronic (CR) caseloads would typically be in early-moderate stages of the disease progression, and would receive counselling, referrals and services in accordance with the identified needs at that time. Care Coordinators of patients on CI or CR caseloads have the unique opportunity to support early intervention for patients with early or more stable dementia progression.
Table 27: Total Number of Patients Active on the Central East LHIN HCC Long-Stay Caseloads, by Population Type and Sub-region (as of November 26, 2018)
39
SN & SC DW & DNE
NC PCC HCCKL Sub-region
to be determined
LHIN Total
Complex Patient
Population 1754 1450 133 286 180 23 3826
Community Independent and Chronic
Patient Populations
8,145 6,399 1,115 2,244 1,498 124 19,525
39
Source: Central East LHIN Home and Community Care Division, at-a-glance data as of November 26, 2018. Please note, data from Scarborough and Durham Sub-regions are combined as caseloads may cross boundaries.

November 29, 2018 38
Placement services
As defined in the Long-Term Care Homes Act, 2007, Central East LHIN Care Coordinators are the designated placement coordinators responsible for the accurate counselling and management of applications to Long-Term Care (LTC). As of October 2018, there were 11,233 unique patients waiting for Placement in a Central East LTC home, and in 2017/18, Care Coordinators managed over 17,000 Placement referrals. These activities include the provision of regular and ongoing placement counselling, the completion and sharing of assessments and updates to Long-Term Care Homes, and modification of patient files as necessary. Table 28 below provides a breakdown of total placement referrals (of all types: Long Stay, Short Stay Respite, Convalescent Care, and Short Stay Interim) by sub-region, but would not include patients for whom counselling was completed but the patient was not made eligible for any reason (patient/Substitute Decision Maker choice, ineligibility, etc.). Table 28: Total Number of LTC Placement Referrals Managed by Central East LHIN, by Sub-Region 2017/18
40
SN & SC DW & DNE NC PCC HCCKL LHIN Total
Total Placement Referrals (all types)
8243 5234 597 2575 499 17,148
Social and Recreational Programming for People with Dementia
The Alzheimer Societies provide a wide variety of social and recreational programs for people with dementia, summarized below. Many of these programs are not funded by the Central East LHIN.
Table 29: Distribution by Sub-Region of Social and Recreational Programming Delivered by Alzheimer Societies 2017/1841
Central East LHIN Sub Region
Social Recreational Programs 2017/18 SN SS DW DNE NH PCC HCCKL
Art’s Based Programs (Art, Choir, Writing)
Minds in Motion®
Music & Memory® (IPod Project)
Physical Programs (Walking)
Social Programs (Activity club, knitting, Brainwaves café, Gardening,
Cooking)
Red = Note: Social Programs are not funded by the CE LHIN but rely on Grants, Foundations and Donor Funding. As a result, program availability is dependent on funding and varies from year to year.
40
Total number includes all Placement referral types: Long Stay, Short Stay Respite, Convalescent Care, Short Stay Interim 41
Source: Alzheimer Societies Program Data

November 29, 2018 39
Table 30: Central East LHIN Social and Recreational Programs, Sessions and Participants by Alzheimer Societies 2017/1942
Measure TOTAL
Number of Unique Social and Recreational Programs 19
Number of Social/Recreation Program Sessions 316
Number of Individuals participating in social & recreational programs 928 Red= Not LHIN Funded
Community and Social Services (CSS)
There are 43 agencies providing CSS in the Central East LHIN. These agencies represent a broad spectrum of services such as meal delivery, transportation, adult day programs, crisis intervention and support, respite, home making and home maintenance, and other programs that assist individuals and caregivers. Below is the number of CSS agencies by LHIN Sub Region.
Table 31: Agencies providing CSS Programs by LHIN Sub-Region43
LHIN Sub Region # Agencies
SN 6
SS 6
DW 4
DNE 7
NC 5
PCC 12
HCCKL 3
LHIN Total 43
The table above includes agencies that provide other services as well as CSS (i.e. CMHA, CHC, Hospitals etc.).
Data specific to the use of CSS services by people living with dementia is not available. It is, however, likely that people living with dementia make use of many CSS services and for this reason, supply and utilization data has been included and is summarized below.
42
Source: Alzheimer Societies Program Data 43
Source: Central East LHIN, Contract Management, Performance and Accountability Unit (August 24, 2018)

November 29, 2018 40
Figure 6: Infographic - Community and Social Services Utilized in 2017/1844
Flexible, Proactive and Responsive Care Partner Education, Supports and Respite
Caregiver Education and Caregiver Support Groups
Alzheimer Societies
Local Alzheimer Societies provide the majority of caregiver education and support specific to dementia through programming that may be offered to caregivers or caregivers and people living with dementia together. It is important to note that there is variation in the level of support provide by the Central East LHIN for Alzheimer Society programming.
Table 32: Percent (%) of Overall Budget Provided by the Central East LHIN by Alzheimer Society 2017/18
ASDR1 ASPKL2 AST3
57% 68% 1.76%
44
Source: Central East LHIN, Contract Management, Performance and Accountability Unit (August 24, 2018)
521,217 Visits
227,767 Meals
Delivered
161,086 Hours
139,797 Attendance
Days
23,008 Individuals
Served
5,944 Visits
40,881 Hours
1,119 Hours
Trips
Meals on Wheels
Respite
Adult Day Program
Congregate Dining
Footcare
Home Making
Home Maintenance

November 29, 2018 41
Table 33: Caregiver Support Programs and Participants by Alzheimer Society 2017/18
Measure ASDR1 ASPKL2 AST3 TOTAL
Number of Individuals Served through Caregiver/Family Support 1383 2400 516 4299
Number of Visits 3385 3005 739 7129
Number of Support Groups 15 24 3 42
Number of Support Group Participants 1193 1936 262 3391
Total Uniquely Identified Individuals Served by Agency (funded programs) 4164 2203 483 6850
Total Uniquely Identified Individuals Served by Agency (non-funded programs) 665 116 0 781
Table 34: Distribution by Sub-Region of Caregiver Education and Support Groups Delivered by Alzheimer Societies 2017/1845
Central East LHIN Sub Region
Caregiver/Person Living with Dementia Support SN SS DW DNE NH PCC HCCKL
Caregiver Respite during Support Groups
Peer Support Groups (both CG/PLWD)
Friendly Visiting
Early Stage Support Groups
One on One Support; Home/Office or Phone Visits (both CG/PLWD)
Recreational Programming (Lawn bowling/gardening etc. one off groups)
Enhance Care - TEACH program
Enhance Care - CARERS program
Caregiver/Person Living with Dementia Education
Taking Control of Our Lives - A Self Mgmt. program for CG/PLWD
First Link Learning Series - First Steps (both CG/PLWD) Workshops
First Link Learning Series - First Steps (both CG/PLWD) Lectures
First Link Learning Series - Next Steps for CG
Support for Living Well
First Link Learning Series - Options for Care for CG
First Link Learning Series - Care in the Later Stages for CG
Finding Your Way - Safety Education
Specialized Workshops - Aphasia/Resilient Care Giver workshop
Public Lectures
Powerful Tools for Caregivers
Public Education French Language Services
Red= Not LHIN Funded
45
Source: Alzheimer Societies Program Data

November 29, 2018 42
Other Caregiver Education
In 2017/2018, the Central East LHIN, Home and Community Care Division’s Self-Management Team held 14 Caregiver Education Workshops, titled “Powerful Tools for Caregivers”. Data specific to caregivers of persons living with dementia is not available. The program is 100% funded by the Central East LHIN.
Table 35: Participants in the Central East LHIN's Power for Tools for Caregiver Series 2017/1846
Total Number of Participants Attending 1 or More Sessions 145
Total Number of Participants Attending 4 or More Sessions 116
Graduation Rate 80.00%
Respite Care
Home and Community Care, Caregiver Respite Program
The Central East LHIN has dedicated funding available for the provision of in-home respite hours for caregivers of qualifying patients in the community. Respite hours are provided in the form of Personal Support Service in the patient’s home and eligibility is determined following thorough assessment by HCC Care Coordinators. Service hours are allocated with consideration of patient complexity, care needs and assessment of caregiver distress. While the service does not exclusively support Caregivers of persons with dementia, those with more complex care needs and advanced cognitive impairment are eligible for greater weekly service hours. By the end of Quarter 2 (FY 2018/19), the Central East LHIN had provided caregiver respite, through contracted agencies, to 5,473 unique caregivers, amounting to 84,067 hours of service47. To ensure responsiveness to the needs of caregivers, scheduling for respite hours is based on the needs of caregivers with hours available in shorter segments, blocks or overnight if needed.
Adult Day Programs
Adult Day Programs (ADPs) in the Central East LHIN provide supports to older people, people with acquired brain injury and their respective caregivers. Most ADPs provide a range of participant-driven social and recreational programming, meals, exercise (including falls prevention classes), cognitive stimulation/rehabilitation and supervision. Caregivers accessing ADPs are provided with respite for up to 8 hours, depending on the site, and among a few ADPs, extended hours, weekend hours and overnight options. CareFirst Seniors, located in Scarborough North LHIN Sub-region, provides extended hours, weekend hours and overnight stays and Victorian Order of Nurses (VON), which operates in multiple locations, provides overnight/weekend hours at their Peterborough City and County LHIN Sub-region site.
The Central East LHIN currently provides partial to total operating funding to fourteen (14) Adult Day Program (ADP) providers who operate forty (40) ADP programs in thirty nine (39) sites across the Central East LHIN. In 2017/18, at Q4, the LHIN’s share of ADP funding ranged from a high of 100% at the Brain Injury Association of Durham and Four Counties Brain Injury Association, to a low of
46
Source: Central East LHIN, Home and Community Care Division (July 27, 2018) 47
Source: Central East LHIN, Home and Community Care Division (November 25, 2018)

November 29, 2018 43
42.10% at the Oshawa Seniors Centre. The median LHIN funding share for ADPs is 76.05%. Participant costs to attend ADPs also vary across sites.
The operating cost by functional centre per attendance day in 2017/18 varied across all ADP providers, ranging from $39.29 (Brain Injury Association of Durham Region) to $114.78 (Regional Municipality of Durham). Other variations between ADP providers have been noted and include staffing, where the ratio of FTEs to attendance days ranged in 2017/18 from 1.0 FTE to 465 attendance days (Haliburton Highlands Health Services) to 1.0 FTE to 3660 attendance days (Brain Injury Association of Durham).
In 2017/18, ADPs provided 139,797 of 136,822 budgeted attendance days (e.g. one space, per one individual, on one day), or 102% of planned attendance days, and served 2973 of 2909 individuals targeted for services (102%). In this same year, all providers met or exceeded 70% of their target for individuals served, with six providers over-subscribed (e.g. greater than 100% of target). The following table illustrates the estimated population living with dementia served by each ADP.
Table 36: Self-Reported estimates of % of Unique Clients with Dementia by ADP48
Organization Estimate % of Unique Clients with Dementia (Self-Reported)
Brain Injury Association of Durham Region Not reported
Carefirst Seniors & Community Services Association
32%
Centres D’Accueil Heritage Not reported
Community Care City of Kawartha Lakes 36%
Community Care Durham 87%
Four Counties Brain Injury Association Not reported
Haliburton Highlands Health Services 95%
Oshawa Senior Citizens Centres 90-100%
(one specialized dementia site)
Regional Municipality of Durham 95-100% (one specialize dementia program)
Scarborough Centre for Health Communities 71%
Senior Persons Living Connected 70%
TransCare Community Support Services 46%
Victorian Order of Nurses 85%
48
Source: Seniors Care Network & Central East LHIN. (2018, June). Central East Adult Day Program Environmental Scan.

November 29, 2018 44
Organization Estimate % of Unique Clients with Dementia (Self-Reported)
Yee Hong 25-100% (one specialized dementia site)
Long Term Care (LTC) Respite Beds
The Central East LHIN has 49 respite beds available in LTC. The following chart illustrates the breakdown of available LTC respite beds by sub-region.
Figure 7: Respite Beds by LHIN Sub Region (2018)49
During consultations related to Dementia Capacity Planning, participants reported difficulty accessing respite beds in LTC and participants perceived a decline in the availability of respite beds in some LHIN sub regions. This was attributed to the optional nature of respite beds (e.g. LTCH are not required to offer respite beds) and the reported administrative burden associated with intake into short stay respite beds in LTC. Since 2016, three Short Stay Respite (SSR) beds have closed (two of which were in one LTCH), leaving 49 beds remaining in Central East. Demand for each SSR bed varies by LTCH and is often dependent on factors such as the geographic location or other features of the home, characteristics of the room itself, and the presence of shared accommodation.
Central East LHIN staff noted that while the SSR service is widely appreciated and utilized, there are challenges and opportunities to improve the availability of this resource to support patients and caregivers in the community. It is acknowledged that the SSR service is difficult to arrange for patients and caregivers on short notice and there are often multiple patients and caregivers competing for beds during peak times. SSR beds are scarce for patients who require secure accommodation or have responsive behaviours. While caregivers of patients with responsive behaviours may find significant benefit with SSR, LTCHs may have difficulty with initiating successful strategies to support responsive behaviours during time-limited stays.
49
Source: Central East LHIN, Contract Management, Performance and Accountability Unit (June 19, 2018)
1 3
4 4 5
6
26
0
5
10
15
20
25
30
DW HC NC SN DNE PC SS
Respite Beds By Sub-Region (2018)
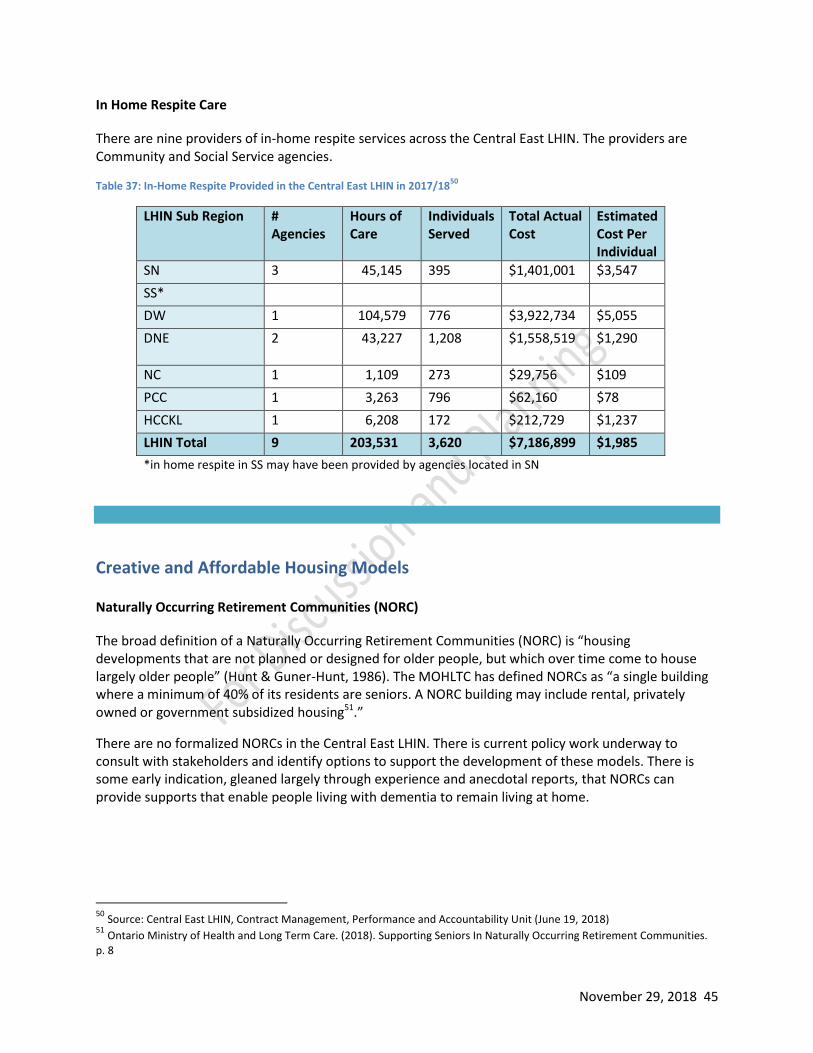
November 29, 2018 45
In Home Respite Care
There are nine providers of in-home respite services across the Central East LHIN. The providers are Community and Social Service agencies.
Table 37: In-Home Respite Provided in the Central East LHIN in 2017/1850
LHIN Sub Region # Agencies
Hours of Care
Individuals Served
Total Actual Cost
Estimated Cost Per Individual
SN 3 45,145 395 $1,401,001 $3,547
SS*
DW 1 104,579 776 $3,922,734 $5,055
DNE 2 43,227 1,208 $1,558,519 $1,290
NC 1 1,109 273 $29,756 $109
PCC 1 3,263 796 $62,160 $78
HCCKL 1 6,208 172 $212,729 $1,237
LHIN Total 9 203,531 3,620 $7,186,899 $1,985
*in home respite in SS may have been provided by agencies located in SN
Creative and Affordable Housing Models
Naturally Occurring Retirement Communities (NORC)
The broad definition of a Naturally Occurring Retirement Communities (NORC) is “housing developments that are not planned or designed for older people, but which over time come to house largely older people” (Hunt & Guner-Hunt, 1986). The MOHLTC has defined NORCs as “a single building where a minimum of 40% of its residents are seniors. A NORC building may include rental, privately owned or government subsidized housing51.”
There are no formalized NORCs in the Central East LHIN. There is current policy work underway to consult with stakeholders and identify options to support the development of these models. There is some early indication, gleaned largely through experience and anecdotal reports, that NORCs can provide supports that enable people living with dementia to remain living at home.
50
Source: Central East LHIN, Contract Management, Performance and Accountability Unit (June 19, 2018) 51
Ontario Ministry of Health and Long Term Care. (2018). Supporting Seniors In Naturally Occurring Retirement Communities. p. 8

November 29, 2018 46
Assisted Living for High-Risk Seniors
In 2017/18 the Central East LHIN served 1765 individuals through its Assisted Living for High Risk Seniors
program. Data is not available regarding the number of participants who are living with a diagnosis of
dementia.
Table 38: Individual Served by ALHRS 2017/18 at Q452
Sub-region
Health Service Provider Individuals Served
Q4 2017/18 Corridor Individuals Served Q4 2017/18 Actual
SN/SS
Carefirst Seniors & Community Services Association
266-398 331
TransCare Community Support Services 154-230 190
Yee Hong Centre for Geriatric Care 127-191 164
DNE/DW Community Care Durham (Oshawa and Courtice)
251-377 435
HCCKL Community Care City of Kawartha Lakes 98-148 139
Haliburton Highlands Health Services 54-80 79
Across Sub-regions
Victorian Order of Nurses for Canada 322-484 427
Total
1,765
Retirement Homes
There are 63 retirement homes listed on the Central East LHIN’s Health Line that collectively offer 5875 beds. Of these, six providers indicate they operate specialized dementia care beds, for a total of 118 such beds LHIN-wide. The breakdown of retirement homes by sub region is provided in Table 17.
Table 39: Number of Retirement Homes, Bed Capacity and Specialized Dementia Beds by LHIN Sub Region 2017/1853
LHIN Sub region
Number of Homes
Total Bed Capacity
Specialized Dementia Beds
SN 5 477 10
SS 6 679 52
DW 11 1209 0
DNE 16 1455 33
NC 10 656 23
PCC 9 940 0
HCCKL 6 459 0
Totals 63 5875 118
52
Source: Central East LHIN, Contract Management, Performance and Accountability Unit (August 17, 2018) 53
Source: Review of Central East LHIN Health Line (August 15, 2018). Missing data validated directly by Homes.

November 29, 2018 47
A detailed list of retirement homes is provided at Appendix 5. There are no published standards describing the services or care model of retirement home-based dementia care units. Participants in the dementia capacity planning consultation process have reported varying experiences with dementia or memory care offered in a retirement home setting.
Long Term Care Homes
There are 68 Long Term Care Homes (LTCHs) in the Central East LHIN. As of October 2018, 61 LTCHs had been funded with permanent behavioural support staff.
Table 40: Number of BSO Teams and FTEs by LHIN Sub-Region as of October 201854
LHIN Sub region
Total # of LTC Homes
Total Bed Capacity55
# BSO Teams Funded
# FTEs
SN 5 1071 5 20
SS 17 3161 14 23.7
DW 7 1021 6 7
DNE 12 1770 10 12
NC 8 667 7 6
PCC 8 1111 8 15.5
HCCKL 11 892 11 12
Totals 68 9693 61 86.2
Behavioural Support Units in LTC
Behavioural Support Transition Units (BSTU) wrap higher intensity care around residents with complex responsive behaviours. The Central East LHIN does not have any LTC-based BSTUs. Bendale Acres, a Central East LHIN based LTCH in Scarborough, has two behavioural units that were self-initiated in 2004/2005, and which are therefore not designated as BSTUs under the Ministry of Health and Long Term Care designated BSTU model. These units include: a 17-bed Cognitive Support Unit, supporting individuals with Alzheimer Disease and other dementias who may be frail and demonstrate exit seeking behaviours; and a 15-bed Behavioural Support Unit that typically serves less frail residents, exhibiting more aggressive behaviours (e.g. those with Frontal Lobe and/or Parkinsonian Dementias).
Secure Units in LTC
A number of LTCH provide secure housing and systems. This includes homes considered secure homes with Wanderguard Systems, coded exits or home-wide security. There are 38 homes with some or all of these interventions, providing a total of 1049 secure spaces. The breakdown of interventions by clusters is shown in the following table.
54
Source: Central East LHIN, Behavioural Supports Ontario Program Office - 2017/18 Q4 Report (May 22, 2018) 55
Source: Central East LHIN, Contract Management, Performance and Accountability Unit (June 19, 2018)

November 29, 2018 48
Table 41: LTCH Secure Bed Summary56
Cluster #
LTCH Secure Unit/# beds
Wanderguard System
Coded Exits
Secure home/facility
Scarborough 14 509 2
Durham 11 342
Northeast 13 198 4 5
Total 38 1049 4 5 2
Adaptive Technology
There is currently no systematic implementation of adaptive technology for dementia care underway in the Central East LHIN. There are pockets of technology implementation such as the Music and Memory program (IPod) of the Alzheimer Societies and the use of robotic pets in LTC. The following table summarizes emerging categories of technology with applications to seniors and dementia care.
Table 42: Categories of Adaptive Technology in Seniors’ and Dementia Care57
Category Examples
Automated detection Stove sensors, falls, cardiac arrest, implantable devices
Home automation Doors that lock when a person lays in bed Lights that turn on when a person walks into a room
Home and personal monitoring Bed sensors that turn on lights when a person rises in the night Scales that detect and report rapid weight change
Motivation Text messaging, reminders, robotics
Social inclusion Video chat, Social media
The University of Ontario Institute of Technology has several researchers focused in the area of assistive robotics and has developed collaborative partnerships with industry in an effort to bring prototypes to market. There is also work underway at Ontario Shores to study the integration of technology into dementia care. This work is still in the early stages.
Figure 8: Assistive Robotics at UOIT July 201858
56
Source: Central East LHIN, Behavioural Supports Ontario Program Office, from Long-Term Care Homes lists, by branch, Home and Community Care, Placement Intranet page. 57
Bucholtz et al., 2013; Hanson, Takahashi & Pecina, 2013; Ludwig et al., 2012; Renda, 2012; 58
Photo Credit: Dr. Patrick Hung, University of Ontario Institute of Technology (August 3, 2018)

November 29, 2018 49
Planning for Phase Three While this report is not intended to provide analysis, the data presented raise several important questions. These have been documented as considerations to inform analysis planned for Phase 3.
Considerations:
There is significant variation in the nature of data available across various programs. This may limit the ability to draw system-level conclusions.
This report describes what is currently occurring, but does not attempt to evaluate the sufficiency of current services. Where available, utilization rates and wait time information has been included that may be suggestive of demand for service in various programs or locations.
Trends showing service shifts (e.g. services moving from one provider type to another) require further analysis. Evaluation of drivers of these shifts and alignment with Senior Friendly Care principles and best practice approaches in these areas is critical. Examples include:
o The decrease in overnight respite offered in LTC and the move to increase the amount of overnight respite provided by ADPs
o The increase in “dementia care” beds offered in retirement homes
In addition, the Action Group identified a number of planning assumptions to inform the future gap analysis. These include:
Based on current evidence, ten year survival from diagnosis will be assumed. These means that service planning should include the provision of increasing levels of support to persons living with dementia for a minimum of 10 years from diagnosis.
If the proportion of persons without a diagnosis could be as high as 30%59, and current estimates may be low, planning for numbers greater than projected is prudent.
If nearly 80% of community-dwelling persons with a diagnosis of dementia in the Central East LHIN also have six or more comorbid conditions60—such as diabetes, osteoporosis and cardiovascular disease, linkages to specialized geriatrics and other clinical services are critical.
If the Central East LHIN has greater proportions of community-dwelling persons with a diagnosis of dementia in the lower income quintiles and smaller proportions of people in the higher income quintiles61, fees for services must be minimized.
If in 2013, 9.4% of community-dwelling Central East LHIN residents with a diagnosis of dementia, (more than 1,100 individuals) were aged 40 to 6462 there is a need to offer services tailored to younger people.
59
Alzheimer Society of Ontario. (2016) Ontario Dementia Profile Series Bulletin #1: Highlights by LHIN / Central East. Author. p. 3. 60
Ibid. p. 4. 61
Ibid. p. 4. 62
Ibid. p. 3.

November 29, 2018 50
Due to the diversity in the evidence about the rate of conversion to dementia63, it is recommended to include a defined focus on Mild Cognitive Impairment in capacity planning that includes educational supports
The Canadian Geriatrics Society suggests that for each person diagnosed with dementia there are, on average, 2.5 caregivers involved
Dementia care providers need to demonstrate cultural competency and be able to provide culturally appropriate support
A strategy for providing dementia care in First Nations, Métis and Inuit populations should be developed specifically with members of these communities.
Additionally, the Action Group identified the following highlights from the Dementia Care in Canada Report64 (CIHI, 2018) as worthy of note:
From 2002 to 2013, dementia prevalence grew from 5.7% to 7.3% (across Canada), while incidence remained steady at about 1.5% for women and 1.4% for men. This suggests that factors other than new diagnosis are responsible for increases in prevalence, likely the fact that Canadians with dementia now live longer.
61% of seniors with dementia live at home, and 25% of seniors with dementia who receive care at home exhibit responsive behaviours.
Seniors living with dementia who receive their initial assessment to determine eligibility for long-term care in a hospital are 6 times more likely to enter residential care than those assessed elsewhere.
Compared with seniors without a dementia diagnosis — seniors with dementia are less likely to be referred to palliative care teams, are prescribed fewer palliative care medications, and are infrequently referred to or are denied access to hospice care.
The third phase of the Dementia Capacity Planning work will be led by the Central East LHIN and commence following the LHIN’s analysis of the MOHLTC’s Regional Profile Tool (Fall 2018). This tool is expected to provide projection data to inform demand and need scenarios that may enable a robust gap analysis and the development of recommendations for action. To facilitate gap analysis work in the third phase, the Action Group developed a decision matrix that combines elements of the Provincial Senior Friendly Care Framework and the Alzheimer Society of Canada PEARLS framework. This decision matrix, found at Appendix 7, draws from the best available evidence in design for older people and people living with dementia and may assist in the task of deciding and prioritizing among options for future action.
Recommendations for action are expected to draw upon the current state and ideal state, and include strategies to build and enhance the foundations of a high quality dementia care system for the Central East LHIN.
63
Langa, K. M. (2014). The diagnosis and management of mild cognitive impairment: A clinical review. Journal of the American Medical Association (JAMA), 312(23), 2551-2561. 64
https://www.cihi.ca/en/dementia-in-canada

November 29, 2018 51
Appendix 1: Dementia Capacity Planning Action Group Members (Phase 1 and 2)
and Report Contributors
Seniors Care Network Alzheimer Societies Central East LHIN Kelly Kay Rhonda Schwartz Stacey Hawkins
Denyse Newton (ASDR) Kari Quinn-Humphrey (AST) Leslie Parham (ASPKLNH)
Karen Lee Boulton Lauren Chitra Marilee Suter Parisha Mehrfar Consulted Jai Mills Lisa Mizzi Lori Brady Michelle Nurse Stewart Sutley Tunde Igli
Report Contributors
Seniors Care Network & Specialized Geriatric Services
Alzheimer Societies Central East LHIN Primary Care Memory Services
Andra Duff-Woskosky Brandi Flowers Cheryl Troicuk Erin Ainstey Kelly Kay (Editor) Melinda Wall Rhonda Schwartz Stacey Hawkins
Denyse Newton (ASDR) Kari Quinn-Humphrey (AST) Leslie Parham (ASPKLNH)
Cindy Massy Strauss George Jacob Irem Ali Karen Lee Boulton Lauren Chitra Lisa Mizzi Marilee Suter Melissa Reid Parisha Mehrfar Pauline Rahaman Sue Wojdylo Suzanne Way
Adrienne Bell-Smith Debbie McLeod Janet Bottom Jo-Elle Nelson Linda Stirling

November 29, 2018 52
Appendix 2: Stakeholders Consulted
We completed 29 consultations between February 12 and July 10, 2018 to validate the draft ideal state.
Groups/individuals consulted include:
• Patients and Caregivers • All LHIN Sub-region Planning Tables • Two Primary Care Provider Groups • Three Specialized Geriatrics Committees • ASDR Client Advisory Group • Alzheimer Society PKLNH Board • CE LHIN Metis, Inuit and Indigenous Peoples' Health Advisory Circle • Durham Region Francophone Table • BSO Design Team • Senior Friendly Care Committee • Peterborough Council on Aging • One to one consultations with representatives from the Metis Nation and Lovesick Lake
Native Women’s Association • Durham Region Council on Aging • Central East LHIN PFAC • Physician Lead for MH&A and Ontario Shores • Curve Lake First Nations Community • HCC Care Coordinators • HCC Contracted Service Providers

November 29, 2018 53
Appendix 3: Workforce Training Program Descriptions
P.I.E.C.E.S is a 16 -hr program that provides an approach to understanding and enhancing care for individuals with complex physical cognitive/mental health needs and behavior changes.
Gentle Persuasive Approaches - the overall goal of this program is to provide front -line staff with the knowledge and skills to effectively and respectfully manage episodes of responsive behaviours that are catastrophic and aggressive in nature. The program is aimed at enhancing the confidence and self -efficacy of front -line staff when managing responsive behaviours of a physically/verbally aggressive nature.
U-First - the goal of the U -First! Program is to offer training to care providers in how to improve the quality of the interaction between the formal care provider and the person living with Alzheimer’s disease and other dementias. Through dialogue and a case -based approach, learners gain confidence in working with people with responsive behaviours.
DementiAbility Methods: The Montessori Way™ - a two-day program teaching innovative approaches to working with older adults living with cognitive and/or physical impairments based on the educational philosophies of childhood educator Dr. Maria Montessori. Participants in this workshop learn about the basic principles of Montessori Programming, along with practical “hands-on” opportunities to apply the techniques and consider how this philosophy of care can be adopted for their clients and programs.

November 29, 2018 54
Appendix 4: ADP Providers and Sites
Organization Location of Sites # of Programs
Brain Injury Association of Durham Region Oshawa 1
Carefirst Seniors & Community Services Association
2 sites in Scarborough 2
Centres D’Accueil Heritage Oshawa 1
Community Care City of Kawartha Lakes Lindsay (2 sites), Bobcaygeon, Fenelon Falls, Little Britain, Omemee
6
Community Care Durham Clarington,Pickering,Uxbridge, Whitby
4
Four Counties Brain Injury Association Peterborough, Lindsay 2
Haliburton Highlands Health Services Haliburton, Minden 2
Oshawa Senior Citizens Centres 4 sites in Oshawa 4
Regional Municipality of Durham Oshawa, Beaverton, Port Perry 3
Scarborough Centre for Health Communities Scarborough 1
Senior Persons Living Connected Scarborough 1
TransCare Community Support Services Scarborough 1
Victorian Order of Nurses
Campbellford, Cobourg, Curve Lake, Havelock, Lakefield, Peterborough Square, Port Hope, Woodland
8
Yee Hong 3 sites in Scarborough (4 programs)
4
TOTAL 39 40

November 29, 2018 55
Appendix 5: Central East LHIN Retirement Homes by LHIN Sub Region
LHIN Sub-Region
Home Name Total Bed Capacity
Specialized Dementia Care Beds
DNE Bowmanville Creek Retirement Community 143
DNE Butternut Manor - Uxbridge 63
DNE Carriage House Retirement Residence (The) 94
DNE Cedarcroft Place by Revera - Oshawa 77
DNE Centennial Retirement Residence 77
DNE Chartwell Bon Air Residence - Retirement Centre 9
DNE Chartwell Wynfield Retirement Residence 107
DNE Douglas Crossing Retirement Community 103 19
DNE Dre's Lodge Retirement Residence 29
DNE Harmony Estate Seniors Residence 10
DNE Harmony Hill Retirement Community Residence - Durham Region
205
DNE Port Perry Place - Port Perry Villa 100
DNE Seasons Clarington - Retirement Community 112 14
DNE Traditions of Durham Retirement Residence 141
DNE West Shore Village 71
DNE White Cliffe Terrace Retirement Residence 114
DW Abbeylawn Manor Retirement Home 56
DW Amica at Whitby 139
DW Chartwell Colonial Retirement Residence 96
DW Chartwell Harwood Retirement Residences 130
DW Chartwell Parkway Retirement Residence 76
DW Chartwell Pickering City Centre 117
DW Court at Pringle Creek (The) 120
DW Lynde Creek Manor Retirement Residence 94
DW Orchard Villa Long Term Care - Pickering - Orchard Villa Retirement Community
61
DW Village of Taunton Mills (The) - Retirement Home 184
DW Viva Retirement Communities - Pickering 136
HCCKL Adelaide Place Retirement Community 125
HCCKL Caressant Care Lindsay - Retirement Home 93
HCCKL Country Estates Retirement Home 38
HCCKL Kawartha Lakes Retirement Residence 93
HCCKL Lakeland Village Assisted Living 38
HCCKL William Place Retirement Residence 72
NC Cobourg Retirement Residence 47

November 29, 2018 56
NC Empire Crossing Retirement Community 63
NC Extendicare - Cobourg - The Landmark Assisted Living 38 23
NC Hillside Haven Retirement Residence 25
NC Island Park Retirement Residence - Sienna Senior Living 85
NC Palisade Gardens 175
NC Regency Manor Nursing Home - Regency Retirement Community
41
NC Roseglen Village for Seniors 94
NC Tower of Port Hope Retirement Residence 43
NC Victoria Retirement Living 45
PCC Applewood Retirement Residence 131
PCC Canterbury Gardens Retirement Residence 134
PCC Empress Gardens Retirement Residence 87
PCC Jackson Creek Retirement Residence 70
PCC Mapleview Retirement Residence 60
PCC Peterborough Retirement Residence 104
PCC Princess Gardens Retirement Residence 126
PCC Royal Gardens Retirement Residence 127
PCC Rubidge Retirement Residence 101
SN Alexis Lodge Retirement Residence 32 10
SN Carefirst Transitional Care Centre 30
SN McNicoll Manor/Moll Berczy Haus 115
SN Shepherd Village - Shepherd Terrace - Retirement Residence
150
SN Sts Peter and Paul Residence 150
SS Cedarbrook Lodge Retirement Residence 208 25
SS Ehatare Retirement Home 100
SS McCowan Retirement Residence 142 27
SS Retirement Suites by the Lake 92
SS Scarborough Retirement Residence 127
SS Villa Karuna 10
Total 5875 118 Source: Health Line Retirement Residences - Central East LHIN http://www.centraleasthealthline.ca/listServices.aspx?id=10158

November 29, 2018 57
Appendix 6: LTCH Secure Bed Summary65
Cluster LTCH Secure Unit/# beds
Wanderguard System
Coded Exits
Secure home/facility
Northeast
1. Centennial Place 32
2. Extendicare Cobourg 23
3. Extendicare Haliburton X
4. Extendicare Lakefield X
5. Extendicare Peterborough X
6. Fairhaven 31 X X
7. Fenelon Court X
8. Golden Plough 20
9. Pleasant Meadow Manor X
10. Riverview Manor X
11. Springdale Country Manor X
12. St. Joseph’s at Fleming 51
13. Victoria Manor 41
Northeast Totals
13 198 4 5
Durham
14. Bay Ridges 30
15. Fairview Lodge 26
16. Hillsdale Estates 50
17. Hillsdale Terraces 25
18. Lakeview Manor 29
19. Orchard Villa 32
20. Port Perry Place 16
21. The Village of Taunton Mills 60
22. The Wynfield 26
23. Thornton View 25
24. Winbourne Park 23
Durham Totals
11 342
Scarborough
25. Bendale Acres 17 X
26. Craiglee
27. Extendicare Rouge Valley 32
28. Fieldstone Commons 32
29. Hellenic 26
65
Data gathered from Central East LHIN Long-Term Care Homes lists, by branch, Home and Community Care, Intranet Placement page

November 29, 2018 58
30. Ina Grafton Gage 32
31. Midland Gardens 57
32. Mon Sheong 23
33. Seven Oaks 34
34. Shepherd Lodge 84
35. Trilogy 60
36. Wexford Residence 30 X
37. Yee Hong Finch 50
38. Yee Hong McNicoll 32
Scarborough Totals
14 509 2
LHIN Total 38 1049 4 5 2

Appendix 7: Decision Framework – Dementia Service Planning
Decision Criteria
Examples from Existing Frameworks (E.g. LHIN Decision making framework, Senior Friendly (sF) Care Framework, Alignment
1 System/ strategic alignment
• Consistent with the provincial and local priorities(leadership) (LHIN) • Person-centred care can only happen with strong leaders who are champions of person-centred care, ingrain it is their organizational philosophy values,
and model the actions expected of staff in their own interactions with residents, families and staff. (PEARLS) • Leadership is committed to deliver an optimal experience for frail seniors as an organizational priority. This commitment empowers the development of
human resources, policies and procedures, caregiving processes, and physical spaces that are sensitive to the needs of frail patients. (sfCare)
LHIN, PEARLS, sfCare
2 Evidence-informed
• Extent to which the initiative allows evidence based information to inform system change (LHIN) • Care is designed based on evidence and best practices that are mindful of the physiology, pathology, and social science of aging and frailty. Care and
service across the organization are delivered in a way that is integrated with the health care system and supports transitions to the community (sfCare) • I receive the right treatment for my condition, and it contributes to improving my health. (HQO patient) • The care I provide is based on best evidence and produces the desired outcome. (HQO provider) • Allows evidence based information to inform system change (LHIN)
HQO, LHIN, sfCare
3 Effective • I receive the right treatment for my condition, and it contributes to improving my health. (HQO patient) • Each resident is engaged in stimulating and meaningful activities with recreational plans tailored to the person’s interests, preferences and abilities.
Continuous assessment, review and revision of these plans is done as the person’s abilities and interests change. (PEARLS)
HQO, LHIN, PEARLS, sfCare
4 Safe • I will not be harmed by the health system – physically, emotionally or otherwise (HQO patient) • The care my patient receives does not cause the patient to be harmed. (HQO provider) • Extent to which initiative mitigates safety issues (LHIN) • Safety and security (sfCare Principle)
HQO, LHIN, sfCare
5 Efficient • The care I receive from all practitioners is well coordinated and efforts are not duplicated. (HQO patient) • The value of my time is respected. I deliver care to my patients using available human, physical, and financial resources efficiently, with no waste to the
system. (HQO provider) • Extent to which the initiative contributes to effective utilization of health services, financial, and human resources capacity to optimize health and other
benefits within the system (LHIN) • Program/initiative demonstrates value for money for required investments including maximum efficiency & effectiveness.(LHIN) • Care and service across the organization are delivered in a way that is integrated with the health care system and supports transitions to the community
(sfCare)
HQO, LHIN, sfCare
6 Individual-focused
• My goals and preferences are respected. My family and I are treated with respect and dignity. (HQO patient) • Decisions about my patient’s care reflect the goals and preferences of the patient and his or her family or caregivers. HQO) • Putting the patient voice at the centre of health care planning and the degree to which patients/clients have a say in the type and delivery of care, in
alignment with Patients First Act. (LHIN) • Extent to which the initiative impacts needs of defined population (LHIN) • Families and friends are involved, supported and engaged in the life of the person with dementia (PEARLS) • Person-centred care principles are embedded into the strategic plan and operational processes to begin and sustain culture change. (PEARLS) • Care and service are provided in a way that is free of ageism and respects the unique needs of patients and caregivers. This maximizes quality and
satisfaction with the experience. (sfCare) • Older adults are partners with the care team. (sfCare) • Care is flexible and aligned with an individual's preferences. (sfCare)
HQO, LHIN, PEARLS, sfCare

November 29, 2018 60
Decision Criteria
Examples from Existing Frameworks (E.g. LHIN Decision making framework, Senior Friendly (sF) Care Framework, Alignment
7 Timeliness/ Accessible
• I know how long I have to wait to see a doctor or for tests or treatments I need and why. I am confident this wait time is safe and appropriate. (HQO patient)
• My patient can receive care within an acceptable time after the need is identified. (HQO provider) • Extent to which the initiative improves access for defined population (LHIN) • An older adult will not be denied access to care or the opportunity to participate in research based solely on their age (sfCare)
HQO, LHIN, sfCare
8 Equitable • No matter who I am or where I live, I can access services that benefit me. I am fairly treated by the health care system. (HQO patient) • Every individual receives high quality care that is fair and appropriate to them, no matter where they live, what they have, or who they are. (HQO
provider) • Extent to which the initiative improves health status or access to care for underserved populations (LHIN) • An older adult will not be denied access to care or the opportunity to participate in research based solely on their age (sfCare)
HQO, LHIN, sfCare
9 Sustainability • Extent to which the initiative can be sustained by resources over time (LHIN) • Spread - The extent to which the results of a practice have been replicated outside of its original setting.
LHIN
10 Environment • Working within current regulations and legislation a physical and social environment is promoted to support the resident’s abilities, strengths and personal interests and enhance the daily life of people with dementia (PEARLS)
• The structures, spaces, equipment, and furnishings provide an environment that minimizes the vulnerabilities of frail patients, promoting safety, comfort, independence, and functional well-being. (sfCare)
PEARLS, sfCare
11 Individual experience
• Extent to which individual experience improves (LHIN) • Care and service are provided in a way that is free of ageism and respects the unique needs of patients and caregivers. This maximizes quality and
satisfaction with the experience. (sfCare)
LHIN, sfCare
12 Ethical Considerations
• Care is provided and research is designed in a way that protects the autonomy, choice and diversity of the most vulnerable of patients. (sfCare) sfCare
13 Partnerships/ collaboration
• Extent to which initiatives involve collaboration across the system (LHIN) • Degree to which appropriate levels of partnership and/or appropriateness of partnerships, both LHIN funded and non-LHIN funded, will be achieved in
order to ensure service quality enhancement, improved comprehensiveness, optimal resource use, minimal duplication, and/or increased coordination in alignment with Patients First Act.
• The organization collaborates with system partners to meet the needs of older adults (sfCare)
LHIN, sfCare
14 Innovation • Answers the question “What is likely to be different” HQO








![FEASIBILITY ASSESSMENT REPORT - Haliburton Solar and Wind · 2018. 1. 10. · FEASIBILITY ASSESSMENT REPORT . 8/15/2013 HSWXII0037 [Haliburton Hatchery] . This report represents the](https://static.fdocuments.us/doc/165x107/60a9eccdd6bce525843e02b8/feasibility-assessment-report-haliburton-solar-and-wind-2018-1-10-feasibility.jpg)









