Renata Smith Pharm.D. HIV and Hepatitis Co-infection June 4 th, 2008.
59
Renata Smith Renata Smith Pharm.D. Pharm.D. HIV and Hepatitis Co- HIV and Hepatitis Co- infection infection June 4 June 4 th th , 2008 , 2008
-
Upload
roland-bishop -
Category
Documents
-
view
217 -
download
0
Transcript of Renata Smith Pharm.D. HIV and Hepatitis Co-infection June 4 th, 2008.

Renata SmithRenata SmithPharm.D.Pharm.D.HIV and Hepatitis Co-HIV and Hepatitis Co-
infectioninfection
June 4June 4thth, 2008, 2008

Objectives:Objectives:
Recognize the modes of transmission for Recognize the modes of transmission for HIV, HCV, and HBVHIV, HCV, and HBV
Recognize the epidemiology of HIV, Recognize the epidemiology of HIV, HCV, and HBVHCV, and HBV
Describe the fundamentals of HIV+HCV Describe the fundamentals of HIV+HCV and HIV+HBV treatmentand HIV+HBV treatment
Identify the common systemic side Identify the common systemic side effects of antiviral/antiretroviral effects of antiviral/antiretroviral therapiestherapies
Identify drug interactions with the Identify drug interactions with the agents used to treat HBV and HCVagents used to treat HBV and HCV

Major Hepatitis VirusesMajor Hepatitis Viruses
VirusVirus Means of transmissionMeans of transmission
Hepatitis AHepatitis A Fecal-oral: Contaminated food or Fecal-oral: Contaminated food or waterwater
Hepatitis BHepatitis B Sexual, mother-to-child, blood Sexual, mother-to-child, blood exposure (transfusion, IDU, exposure (transfusion, IDU, tattoo)tattoo)
In HIV + women MTCT of HBV is In HIV + women MTCT of HBV is much higher much higher
Hepatitis CHepatitis C Blood exposure (transfusion, IDU, Blood exposure (transfusion, IDU, tattoo); sexual, mother-to-child tattoo); sexual, mother-to-child less common. In HIV + women less common. In HIV + women MTCT is 3 fold higher MTCT is 3 fold higher

Prevalence of HCV infection Prevalence of HCV infection in selected subgroups in in selected subgroups in
the U.S.the U.S.
Injection drug users: 52-90%Injection drug users: 52-90% Hemophiliacs: 60-85% Hemophiliacs: 60-85% (if infected prior to (if infected prior to
1987)1987)
HIV infected individuals: 9-40%HIV infected individuals: 9-40% incarcerated HIV+: 50%incarcerated HIV+: 50% MSM: 4-8%MSM: 4-8%

Hepatitis C EpidemiologyHepatitis C Epidemiology
130 million people have HCV worldwide based 130 million people have HCV worldwide based on the 2007 WHO dataon the 2007 WHO data
4 million Americans have chronic hepatitis C 4 million Americans have chronic hepatitis C (HCV RNA+)(HCV RNA+)
2%-20% progress to cirrhosis in 20 years2%-20% progress to cirrhosis in 20 years The rate of progression to cirrhosis increases The rate of progression to cirrhosis increases
by 3 fold if co-infected with HIVby 3 fold if co-infected with HIV This accelerated rate is further magnified in This accelerated rate is further magnified in
patients with low CD4 countpatients with low CD4 count Unclear if HCV adversely affects the rate of Unclear if HCV adversely affects the rate of
HIV progressionHIV progression Unclear if ART improves morbidity/mortality Unclear if ART improves morbidity/mortality
of untreated HCVof untreated HCV

Hepatitis C Virus Disease: Hepatitis C Virus Disease: EpidemiologyEpidemiology
Six genotypesSix genotypes Genotype 1: 75% of HCV infections in United Genotype 1: 75% of HCV infections in United
StatesStates Genotypes 2 and 3: more prevalent in Western Genotypes 2 and 3: more prevalent in Western
EuropeEurope Transmission: percutaneous exposure (most Transmission: percutaneous exposure (most
common), mother-to-child transmission, common), mother-to-child transmission, sexual exposuresexual exposure
High rate of HCV coinfection in HIV-infected High rate of HCV coinfection in HIV-infected injection drug users and hemophiliacs injection drug users and hemophiliacs

HIV/HCV TreatmentHIV/HCV Treatment
Predictors of success in achieving a Predictors of success in achieving a sustained viral response (SVR):sustained viral response (SVR): CD4 count greater than 200CD4 count greater than 200 HIV RNA levels below 10,000 copiesHIV RNA levels below 10,000 copies HCV RNA < 1,000,000HCV RNA < 1,000,000 No alcohol consumptionNo alcohol consumption
HCV Treatment Decisions HCV Treatment Decisions in HIV Coinfected in HIV Coinfected
Treat Hepatitis C if HIV stable and if Treat Hepatitis C if HIV stable and if
CD4 > 200 cells/ml )CD4 > 200 cells/ml ) Treat HIV first if CD4 < 200 cells/mlTreat HIV first if CD4 < 200 cells/ml

Hepatitis C Virus Disease:Hepatitis C Virus Disease:TreatmentTreatment
Pegylated (PEG) interferon (IFN) in combination Pegylated (PEG) interferon (IFN) in combination with ribavirin: higher rates of SVR than standard with ribavirin: higher rates of SVR than standard IFN plus ribavirin or PEG IFN without ribavirin IFN plus ribavirin or PEG IFN without ribavirin
Recommended: 24-48 weeks based on genotypeRecommended: 24-48 weeks based on genotypePEG IFN (Pegasys) alfa-2a 180 mg SQ weekly, or PEG IFN (Pegasys) alfa-2a 180 mg SQ weekly, or
PEG IFN alfa-2b (PEG-Intron) 1.5 mcg/kg SQ PEG IFN alfa-2b (PEG-Intron) 1.5 mcg/kg SQ weeklyweekly
++
Ribavirin (Copegus) 600 mg PO BID if weight >75 kgRibavirin (Copegus) 600 mg PO BID if weight >75 kg(400 mg Q AM, 600 mg Q PM if weight <75 kg)(400 mg Q AM, 600 mg Q PM if weight <75 kg)

PEG-IFN virologic response rates across studies
0
10
20
30
40
50
ACTG APRICOT RIBAVIC
ETRSVR
%
Response
Abstracted from 11th CROI
41
27
49
4037
27
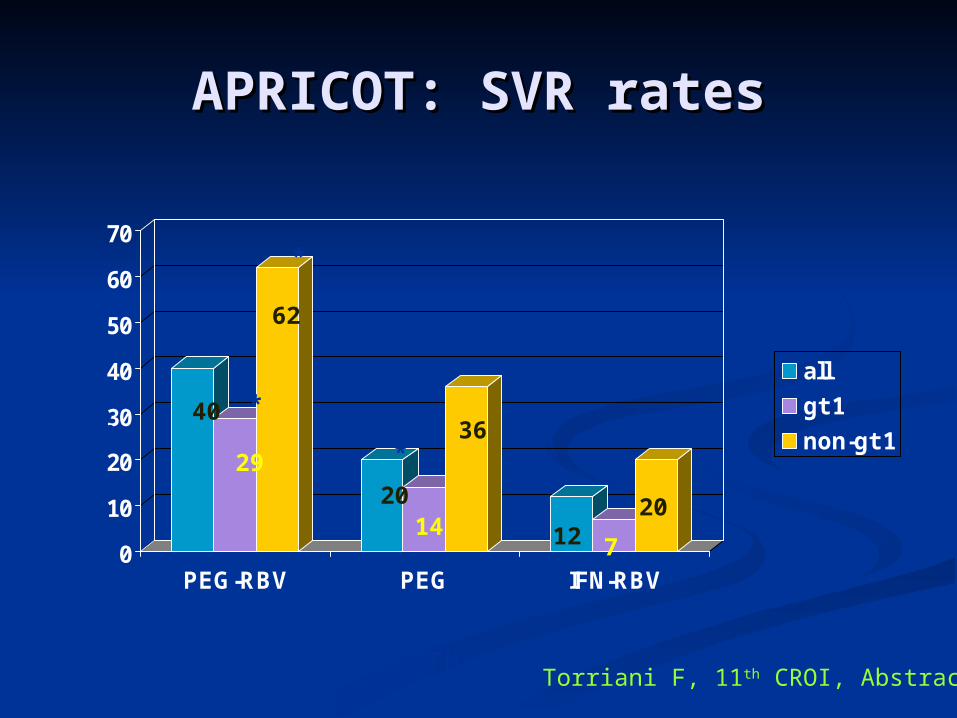
APRICOT: SVR ratesAPRICOT: SVR rates
0
10
20
30
40
50
60
70
PEG-RBV PEG IFN-RBV
all
gt 1
non-gt 1
*
*
*
*
*p<0.05 compared to IFN/RBVTorriani F, 11th CROI, Abstract 112
SVR % 40
29
62
2014
36
12 7
20

Side Effects of Side Effects of InterferonInterferon
Flu-like symptomsFlu-like symptoms HeadacheHeadache Fatigue or astheniaFatigue or asthenia Myalgia, arthralgiaMyalgia, arthralgia Fever, chillsFever, chills
Neuropsychiatric Neuropsychiatric disordersdisorders
DepressionDepression Mood labilityMood lability AnxietyAnxiety
Lab alterationsLab alterations NeutropeniaNeutropenia AnemiaAnemia ThrombocytopeniaThrombocytopenia
AlopeciaAlopecia Asthma like symptoms Asthma like symptoms
( ( 20%-30% of patients)20%-30% of patients)
NauseaNausea DiarrheaDiarrhea Weight lossWeight loss Injection-site reactionInjection-site reaction

Side Effects of Side Effects of RibavirinRibavirin
Hemolytic anemia-dose Hemolytic anemia-dose dependentdependent
TeratogenicityTeratogenicity Cough, dyspnea, sinus congestionCough, dyspnea, sinus congestion Rash and pruritusRash and pruritus InsomniaInsomnia AnorexiaAnorexia
COPEGUSCOPEGUS®® (ribavirin, USP) (ribavirin, USP) [package insert]. Nutley, NJ: Hoffmann-La Roche; 2002.[package insert]. Nutley, NJ: Hoffmann-La Roche; 2002.

Rare side effects of HCV Rare side effects of HCV treatmenttreatment
Acute congestive heart failureAcute congestive heart failure Renal failureRenal failure SeizuresSeizures Hearing lossHearing loss Retinopathy resulting in vision lossRetinopathy resulting in vision loss Pulmonary fibrosis or pneumonitis, and Pulmonary fibrosis or pneumonitis, and
sepsissepsis Severe depression with suicidal ideationsSevere depression with suicidal ideations Deaths have been reported from acute Deaths have been reported from acute
myocardial infarction, stroke, suicide, and myocardial infarction, stroke, suicide, and sepsis.sepsis.

Treatment of Side EffectsTreatment of Side Effects
NeupogenNeupogen®® for Neutropenia for Neutropenia ProcritProcrit®® for anemia for anemia Appetite stimulantsAppetite stimulants AntidepressantsAntidepressants Ibuprofen for flu like symptoms and Ibuprofen for flu like symptoms and
bone painbone pain Antihistamines for itchingAntihistamines for itching

Drug interactions in Drug interactions in HIV/HCVHIV/HCV
CoinfectionCoinfection
Didanosine and Stavudine plus Didanosine and Stavudine plus Ribavirin appear to cause Ribavirin appear to cause mitochondrial toxicity resulting in mitochondrial toxicity resulting in lactic acidosis, peripheral neuropathylactic acidosis, peripheral neuropathy
Retrovir and Ribavirin may result in Retrovir and Ribavirin may result in increase risk of anemiaincrease risk of anemia
Avoid using these drugs together Avoid using these drugs together

Ribavirin and Adverse Ribavirin and Adverse EventsEvents
Ribavirin (continued):Ribavirin (continued): Teratogenic; women with potential for Teratogenic; women with potential for
pregnancy and men receiving ribavirin pregnancy and men receiving ribavirin must use contraception consistently must use contraception consistently during ribavirin therapy and for 6 during ribavirin therapy and for 6 months after completion of therapymonths after completion of therapy

Hepatitis CHepatitis CINTERFERON AND INTERFERON AND
RIBAVIRINRIBAVIRIN Serious, less common side effectsSerious, less common side effects
Bacterial infectionsBacterial infections Thyroid diseaseThyroid disease Severe depression, suicideSevere depression, suicide SeizuresSeizures Vision or hearing lossVision or hearing loss Kidney or heart failureKidney or heart failure Fetal abnormalities/fetal lossFetal abnormalities/fetal loss

Adherence MattersAdherence Matters
Pegasys + Ribavirin Study at AASLDA Pegasys + Ribavirin Study at AASLDA
45% genotype 1 had SVR45% genotype 1 had SVR 67% had SVR if >80% adherent67% had SVR if >80% adherent 40% had SRV if < 80% adherent40% had SRV if < 80% adherent 76% genotype 2 had SVR76% genotype 2 had SVR 86% had SVR if > 80% adherent86% had SVR if > 80% adherent
Pegasys/RBV 1000/1200 mg 48 week Pegasys/RBV 1000/1200 mg 48 week NV15942 studyNV15942 study
76% SVR with 80% adherence76% SVR with 80% adherence

Case study HIV/HCVCase study HIV/HCV 42F diagnosed with HIV/HCV 15 years 42F diagnosed with HIV/HCV 15 years
ago on HAART. HIV RNA < 50, CD4 ago on HAART. HIV RNA < 50, CD4 count 765 cells/ml.count 765 cells/ml.
HCV RNA 2 million IU HCV RNA 2 million IU HCV genotype 1AHCV genotype 1A LFTs elevated, AFP elevated, moderate LFTs elevated, AFP elevated, moderate
fibrosis, liver biopsy shows no cirrhosisfibrosis, liver biopsy shows no cirrhosis No other preexisting conditionsNo other preexisting conditions No other medications No other medications No psychiatric illness No psychiatric illness NKDANKDA

Would you treat this patient Would you treat this patient for HCV?for HCV?

YES!!!!!YES!!!!!

What would you use???What would you use???
Peg-IFN 180 mcg SQ weekly Peg-IFN 180 mcg SQ weekly
++Ribavirin 600 mg bid if > 75Kg or Ribavirin 600 mg bid if > 75Kg or
Ribavirin 400 mg am, 600 mg pm if < Ribavirin 400 mg am, 600 mg pm if < 75 Kg75 Kg

Duration of Therapy???Duration of Therapy???

48 weeks48 weeks

Counseling parametersCounseling parameters
Flu like symptomsFlu like symptoms Bone pain/muscle pain/hair Bone pain/muscle pain/hair
loss/lethargyloss/lethargy Bone marrow suppressionBone marrow suppression Teratogenesity of RibavirinTeratogenesity of Ribavirin Psychiatric adverse effectsPsychiatric adverse effects ART drug interactions with RibavirinART drug interactions with Ribavirin
Monitoring parametersMonitoring parameters
HCV viral loadHCV viral load Early viral response (EVR)Early viral response (EVR)>> 2 log 2 log22 decrease at 12 decrease at 12
weeksweeks Rapid viral response (RVR)= undetectable at 4 weeksRapid viral response (RVR)= undetectable at 4 weeks Sustained viral response (SVR)= undetectable 24 Sustained viral response (SVR)= undetectable 24
weeks after end of therapyweeks after end of therapy Slow responders= 2 log reduction in HCV RNA but Slow responders= 2 log reduction in HCV RNA but
did not suppress viral load very quicklydid not suppress viral load very quickly
CBC CBC (anemia/neutropenia/thrombocytopenia)(anemia/neutropenia/thrombocytopenia)
Pregnancy testPregnancy test



HIV and HBV coinfectionHIV and HBV coinfection

HIV HIV
40 million 40 million worldwideworldwide
1 million in the US1 million in the US Target: CD4 cellsTarget: CD4 cells Reverse Reverse
TranscriptaseTranscriptase Nucleos(t)ide Nucleos(t)ide
Analogues and Analogues and other ARVother ARV
Mutations=ResistaMutations=Resistancence
HBVHBV
400 million 400 million worldwideworldwide
1.25 million in the 1.25 million in the USUS
Target: hepatocytesTarget: hepatocytes Reverse Reverse
TranscriptaseTranscriptase Nucleos(t)ide Nucleos(t)ide
Analogues and Analogues and immunomodulatorsimmunomodulators
Mutations=ResistancMutations=Resistancee



CURRENT TREATMENT CURRENT TREATMENT OPTIONS FOR HBV/HIV OPTIONS FOR HBV/HIV
CoinfectedCoinfected Peg-Inf &2a (PegasysPeg-Inf &2a (Pegasys®®) x 6 months) x 6 months LamivudineLamivudine (LM/Epivir (LM/Epivir®®) 300 mg daily) 300 mg daily Adefovir (ADV/HepseraAdefovir (ADV/Hepsera®®) 10 mg daily) 10 mg daily Entecavir (ETV/BaracludeEntecavir (ETV/Baraclude®®) 0.5-1 mg daily) 0.5-1 mg daily Telbivudine (L-dt/TyzekaTelbivudine (L-dt/Tyzeka®®)) TenofivirTenofivir (TDF/Viread (TDF/Viread®®) 300 mg daily) 300 mg daily EmtricitabineEmtricitabine (FTC/Emtriva (FTC/Emtriva®®) 200 mg daily ) 200 mg daily TruvadaTruvada® ® (300/200 mg) 1 tab daily(300/200 mg) 1 tab daily




DHHS DHHS Recommendations ForRecommendations ForTreatment of HBV/HIV Treatment of HBV/HIV
CoinfectionCoinfection11
Need to Need to TreatTreat
RecommendationRecommendation
HIV and not HIV and not HBVHBV
TDF/FTC or TDF + 3TC considered first choice TDF/FTC or TDF + 3TC considered first choice NRTI backbonesNRTI backbones
HIV and HBVHIV and HBV TDF/FTC or TDF + 3TC considered first-choice TDF/FTC or TDF + 3TC considered first-choice NRTI backbones (activity against both viruses) NRTI backbones (activity against both viruses) OROR
ETV with 1 NRTI aboveETV with 1 NRTI aboveCaveat: Use of 3TC, FTC, or TDF as the only Caveat: Use of 3TC, FTC, or TDF as the only active anti-HBV agent should be avoided active anti-HBV agent should be avoided because of the risk of HBV resistancebecause of the risk of HBV resistance
HBV and not HBV and not HIVHIV
Peg-IFN-Peg-IFN-αα (does not lead to development of drug- (does not lead to development of drug-resistant HIV or HBV mutants) or ADV (risk of resistant HIV or HBV mutants) or ADV (risk of HIV mutants)HIV mutants)
Avoid FTC, 3TC, and TDF w/o full HAART regimen Avoid FTC, 3TC, and TDF w/o full HAART regimen to prevent rapid development of drug-resistant to prevent rapid development of drug-resistant HIV mutationsHIV mutations
1. DHHS. Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents - October 10, 2006. http://AIDSinfor.nih.gov; 2. Supplement to Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents, April 30, 2007
For HBV/HIV co-infected patients, ETV should not be used for treatment of HBV infection w/o concomitant treatment for HIV2

AASLD GUIDELINES for Treatment AASLD GUIDELINES for Treatment of HBV/HIV Coinfectionof HBV/HIV Coinfection11
Treat patients meeting criteria for chronic hepatitis B Treat patients meeting criteria for chronic hepatitis B (CHB)(CHB)
Patients not on HAART and not anticipated to require Patients not on HAART and not anticipated to require HAART in the near future should be treated with therapy HAART in the near future should be treated with therapy that does not target HIV such as Peg-IFN-that does not target HIV such as Peg-IFN-αα
Telbivudine should not be used in this circumstance Telbivudine should not be used in this circumstance because of the risk of selection of the major LAM because of the risk of selection of the major LAM resistance mutation M204I in the YMDD motifresistance mutation M204I in the YMDD motif
Patients should receive therapies effective against both Patients should receive therapies effective against both viruses: LAM + TDF or FTC + TDF are preferredviruses: LAM + TDF or FTC + TDF are preferred
Patients on effective HAART that does not include a drug Patients on effective HAART that does not include a drug active against HBV may be treated with Peg-IFN-active against HBV may be treated with Peg-IFN-αα, ADV, , ADV, or ETVor ETV
Add ADV or TDF in patients with LAM resistanceAdd ADV or TDF in patients with LAM resistance

To Construct an Antiretroviral Regimen, Select 1 Component from Column A + 1
from Column B
Column AColumn A
Preferred Preferred ComponeComponentsnts
NNRTI OR PI Efavirenz atazanavir + ritonavir fosamprenavir + ritonavir 2x/day) lopinavir/ritonavir2 (2x/day)
AlternativAlternative to e to Preferred Preferred ComponeComponentsnts
NNRTI OR PI nevirapine atazanavir fosamprenavir fosamprenavir + ritonavir 1x/day) lopinavir/ritonavir (1x/day) saquinavir + ritonavir
Column BColumn B
Dual – NRTI OptionsDual – NRTI Options
Preferred Preferred ComponentsComponents(alphabetical (alphabetical order)order)
abacavir/lamivudine (for patients who test negative for HLA B5701)
ORtenofovir/emtricitabine
Alternative Alternative to Preferred to Preferred ComponentsComponents(order of (order of preference)preference)
zidovudine/lamivudinezidovudine/lamivudine
OROR
didanosine +(emtricitabine or didanosine +(emtricitabine or lamivudine)lamivudine)

Case 1 HIV/HBVCase 1 HIV/HBV 22 yo MSM infected with HIV/HBV x 12 22 yo MSM infected with HIV/HBV x 12
yearsyears HIV RNA 180, 000, CD4 275 cells/ml,HIV RNA 180, 000, CD4 275 cells/ml, HBV DNA 1,000,000 copies/mlHBV DNA 1,000,000 copies/ml HBeAg(+)HBeAg(+) LFTs elevatedLFTs elevated AFP normalAFP normal Liver biopsy-no cirrhosisLiver biopsy-no cirrhosis Does this patient therapy for HIV and Does this patient therapy for HIV and
HBV?HBV?

Table 5. Indications for Initiating Antiretroviral Therapy for the Chronically HIV-1 Infected Patient
Clinical Condition and/or CD4 CountRecommendations
• History of AIDS-defining illness• CD4 count <200 cells/mm3 (AIDS diagnosis)• CD4 count 200-350 cells/mm3• Pregnant women*• Persons with HIV-associated nephropathy• Persons coinfected with hepatitis B virus (HBV), when HBV treatment is
indicated (Treatment with fully suppressive antiviral drugs active against both HIV
and HBV isrecommended.)
Antiretroviral therapy should be initiated.• Patients with CD4 count >350 cells/mm3 who do not meet any of the
specific conditions listed above. The optimal time to initiate therapy in asymptomatic patients with CD4 count >350 cells/mm3 is not well defined. Patient scenarios and comorbidities should be taken into consideration.
December 1st, 2007Updated HIV Treatment
Guidelines


What would you start What would you start therapy with?therapy with?
ABAC/3TC/EFVABAC/3TC/EFV AZT/3TC/LPV/rtvAZT/3TC/LPV/rtv TDF/FTC/EFVTDF/FTC/EFV TDF/FTC/NVPTDF/FTC/NVP Peg-INFPeg-INF

To Construct an Antiretroviral Regimen, Select 1 Component from Column A + 1
from Column B
Column AColumn A
Preferred Preferred ComponeComponentsnts
NNRTI OR PI Efavirenz atazanavir + ritonavir fosamprenavir + ritonavir 2x/day) lopinavir/ritonavir2 (2x/day)
AlternativAlternative to e to Preferred Preferred ComponeComponentsnts
NNRTI OR PI nevirapine atazanavir fosamprenavir fosamprenavir + ritonavir 1x/day) lopinavir/ritonavir (1x/day) saquinavir + ritonavir
Column BColumn B
Dual – NRTI OptionsDual – NRTI Options
Preferred Preferred ComponentsComponents(alphabetical (alphabetical order)order)
abacavir/lamivudine (for patients who test negative for HLA B5701)
ORtenofovir/emtricitabine
Alternative Alternative to Preferred to Preferred ComponentsComponents(order of (order of preference)preference)
zidovudine/lamivudinezidovudine/lamivudine
OROR
didanosine +(emtricitabine or didanosine +(emtricitabine or lamivudine)lamivudine)

What would you start What would you start therapy with?therapy with?
ABAC/3TC/EFVABAC/3TC/EFV AZT/3TC/LPV/rtvAZT/3TC/LPV/rtv TDF/FTC/EFVTDF/FTC/EFV TDF/FTC/NVPTDF/FTC/NVP Peg-INFPeg-INF

Case 2 HIV/HBVCase 2 HIV/HBV
36F HIV/HBV infected on HAART 36F HIV/HBV infected on HAART with AZT/3TC/fosAPV/rtv x 2 yearswith AZT/3TC/fosAPV/rtv x 2 years
HBVeAg(-) seroconverted HBVeAg(-) seroconverted HBV DNA undetectable (< 60 HBV DNA undetectable (< 60
copies/ml)copies/ml) LFTs normalLFTs normal Would you change anything Would you change anything
in this patient’s regimen???in this patient’s regimen???


Case 2 HIV/HBVCase 2 HIV/HBV
Continue this successful Continue this successful antiretroviral regimen and monitor antiretroviral regimen and monitor for HBV resistance.for HBV resistance.
Substitute TDF for AZT or Substitute TDF for AZT or change COMB to Truvada.change COMB to Truvada.
Change the PI to EFV to reduce the Change the PI to EFV to reduce the risk of hepatotoxicity.risk of hepatotoxicity.
Case 3 HIV/HBVCase 3 HIV/HBV
26M infected with HIV/HBV26M infected with HIV/HBV HBeAg(+)HBeAg(+) HBV DNA 800,000 copies/mlHBV DNA 800,000 copies/ml ALT elevatedALT elevated HIV RNA 10,000 copies/mlHIV RNA 10,000 copies/ml CD4 652 cells/mlCD4 652 cells/ml WHAT would you do?WHAT would you do?

Case 3 HIV/HBVCase 3 HIV/HBV
Treat with antiretroviral regimen Treat with antiretroviral regimen that contains TDF and FTC or 3TCthat contains TDF and FTC or 3TC
Treat with Peg-INFTreat with Peg-INF Treat with Entecavir aloneTreat with Entecavir alone Treat with Telbivudine aloneTreat with Telbivudine alone Treat with Adefovir aloneTreat with Adefovir alone


DHHS DHHS Recommendations ForRecommendations ForTreatment of HBV/HIV Treatment of HBV/HIV
CoinfectionCoinfection11
Need to Need to TreatTreat
RecommendationRecommendation
HIV and not HIV and not HBVHBV
TDF/FTC or TDF + 3TC considered first choice TDF/FTC or TDF + 3TC considered first choice NRTI backbonesNRTI backbones
HIV and HBVHIV and HBV TDF/FTC or TDF + 3TC considered first-choice TDF/FTC or TDF + 3TC considered first-choice NRTI backbones (activity against both viruses) NRTI backbones (activity against both viruses) OROR
ETV with 1 NRTI aboveETV with 1 NRTI aboveCaveat: Use of 3TC, FTC, or TDF as the only Caveat: Use of 3TC, FTC, or TDF as the only active anti-HBV agent should be avoided active anti-HBV agent should be avoided because of the risk of HBV resistancebecause of the risk of HBV resistance
HBV and not HBV and not HIVHIV
Peg-IFN-Peg-IFN-αα (does not lead to development of drug- (does not lead to development of drug-resistant HIV or HBV mutants) or ADV (risk of resistant HIV or HBV mutants) or ADV (risk of HIV mutants)HIV mutants)
Avoid FTC, 3TC, and TDF w/o full HAART regimen Avoid FTC, 3TC, and TDF w/o full HAART regimen to prevent rapid development of drug-resistant to prevent rapid development of drug-resistant HIV mutationsHIV mutations
1. DHHS. Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents - October 10, 2006. http://AIDSinfor.nih.gov; 2. Supplement to Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents, April 30, 2007
For HBV/HIV co-infected patients, ETV should not be used for treatment of HBV infection w/o concomitant treatment for HIV2
Case 3 HIV/HBVCase 3 HIV/HBV
Treat with antiretroviral Treat with antiretroviral regimen that contains TDF regimen that contains TDF and FTC or 3TCand FTC or 3TC
Treat with Peg-INFTreat with Peg-INF Treat with Entecavir aloneTreat with Entecavir alone Treat with Telbivudine aloneTreat with Telbivudine alone Treat with Adefovir aloneTreat with Adefovir alone

An Approach to An Approach to Management of HIV/HBV Management of HIV/HBV
CoinfectionCoinfection HAART experienced on LAM, active HBVHAART experienced on LAM, active HBV
Add TDFAdd TDF HAART-naïve, replicative HBV, need therapy HAART-naïve, replicative HBV, need therapy
for both:for both: TDF/FTC or 3TC containing ARTTDF/FTC or 3TC containing ART
HAART-naïve, need to treat HIV but not HBV:HAART-naïve, need to treat HIV but not HBV: Same as aboveSame as above
Avoid monotherapy for HBV, Avoid monotherapy for HBV, use 2 agents with non-overlapping resistance use 2 agents with non-overlapping resistance
profilesprofiles
•http://aidsinfo.nih.gov/guidelines
•http://clinicalcareoptions.com
•http://medscape.com
•https://https://aasldaasld.org.org

QUESTIONS?????