Renal System
30
CHAPTER 15: Renal
description
renal system pdf
Transcript of Renal System
-
CHAPTER 15: Renal
-
Urinary System Anatomy Know every diagram on this pp
-
Urinary System Homeostasis
Control of extracellular fluid: interstitial fluid and plasma
Control both ECF volume and composition ECF Composition
Electrolytes (Na+, K+, Cl-) Minerals (PO43-, Mg2+, Ca2+) Acid-base balance (HCO3, H+) Toxic products of metabolism (uremic toxins)
ECF Volume
-
Summary Homeostasis
Digestive and nervous systems indiscriminate Cardiovascular systems only controls blood
pressure The Urinary System (Kidneys) controls composition
of extracellular fluid Homeostasis is the maintenance of the milieu
interieur, based not on what we ingest but what the urinary system keeps
-
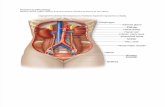
Human Kidney - cut section
25% of cardiac output goes into renal artery at rest
-
Human Kidney - cut section Key structures to know:
cortex, medulla, pelvis, ureter, artery and vein
25% of cardiac output goes into renal artery at rest
-
Nephron 1,000,000/human kidney
500,000/dog kidney
proximal tubule
loop of Henle (descending, then ascending limb)
collecting duct
distal tubule
glomerulus
-
Nephron 1,000,000/human kidney
500,000/dog kidney
Key structures to know: cortex, medulla, pelvis, ureter, artery, vein, nephron and its parts
proximal tubule
loop of Henle (descending, then ascending limb)
collecting duct
distal tubule
glomerulus
-
Proximal tubule
Surrounded by smooth muscle
-
Important vessels: Renal artery and vein (1 of each per kidney) Each nephron has:
Afferent and Efferent arteriole Glomerular capillary bed Peritubular capillary bed (also referred to as Vasa recta capillary bed) Is more attracted to positive molecules because it holds a negative charge,
seen in the filtration of netrans; carbs with charges
Surrounded by smooth muscle
-
3 key renal processes determine what is excreted in urine
Proximal Tubule
Bowmans Space
Filtration
Bowmans or Glomerular
Capsule
1 2 3
-
Glomerular structure (Key: 3 layers of filtration barrier)
Filtration barrier
- Continuous: Limits macromolecular movement across wall to molecules
-
Filtration Glomerular capillaries
Driven by high hydrostatic pressure (Pc; >50 mmHg) in glomerular capillaries
Highly permeable to water and small molecules
Water, electrolytes (such as Na, K, Cl), amino acids, and glucose are freely filtered
Glomerular filtration rate (GFR) = 125 mL/min in normal person; 4 mL/kg/min in other species)
GFR is large (equivalent to plasma volume every 20 mins in all species)
Highly selective (large molecules such as proteins >30,000 Daltons, are kept in plasma)
About 1/3 of plasma entering glomerulus is filtered into Bowmans space (Filtration Fraction = 33%)
2/3 (67%) of water and small molecules and 100% of large proteins enter peritubular capillary
What gets thru: Water, small solutes (freely) Not macromolecules
-
Control of GFR Pressure in the glomerular capillaries causes filtration (GFR)
Think of afferent arteriole as a spigot (opening it will increase GFR by increasing pressure in glomerulr capillaries)
The efferent arteriole is like a pressure relief valve (opening it will lower pressure in the glomerular capillaries and reduce GFR).
Angiotensin would increase filtration rate of GFR
-
Control of GFR An increase in systemic arterial blood
pressure might be expected to increase renal blood flow and GFR
However, if blood pressure increases, there is an automatic constriction of the afferent arteriole
Renal blood flow and GFR do not change Renal autoregulation. Regardless of what
happens to blood pressure, renal blood pressure remains the same
Blood pressure
-
Reabsorption: Overview Not filtered solutes
Albumin and other large proteins (>30,000 Daltons) Filtered solutes
Tubular Reabsorption and Secretion Subtypes:
Conserved solutes: important for kidney to save (goal = 100% reabsorption) examples: glucose and amino acids
Balanced solutes: kidney balances input with urinary excretion (goal = balance) examples: Na+, K+, H+
Excreted solutes: important to eliminate in urine (goal = excretion) urea, medications (antibiotics)
Water Regulated by Urine Concentrating Mechanism
-
Conserved Solute Reabsorption
Glucose as an example Sodium-Glucose Linked Transporter (SGLT) in
brush border membrane Secondary active transport SGLT2 early in proximal tubule SGLT1 late in proximal tubule
GLUcose Transporter (GLUT) in basolateral membrane
Facilitated diffusion Normally, >99% of glucose reabsorbed before end
of proximal tubule Amino Acid reabsorption is identical except that
there are different carriers >99% in proximal tubule
Drug Industry: Developing SGLT inhibitors for treatment of metabolic syndrome
Metabolic Syndrome (people and cats): Issue: Obesity, Hyperglycemia (insulin resistance) Develop: Heart and Kidney Disease
-
Balanced solutes (sodium) Renal handling General Scheme
65% reabsorption in proximal tubule Without regard to body need
Rest of reabsorption is more distal in nephron Most is with regard to body need
Typically, about 99% of filtered load is reabsorbed but it varies according to body needs
Hormonal influence on sodium reabsorption Aldosterone enhances distal tubule reabsorption
Location Na+ H2O
Proximal tubule 65% 66%
Loop of Henle 25% 15%
Distal tubule 8% 4%
Total 98% 85%
-
Overall scheme for Renal Na Handling
Cortical nephrons Juxtamedullary nephrons Short loop of Henle Long loop of Henle Thin descending limb Thin descending limb Thick ascending limb Thin ascending limb
Thus, the juxtamedullary would be able to filter a larger amount of urine
-
Overall scheme for Renal Na Handling
Freely filtered Proximal reabsorption
multiple carriers 65% - no regard to body need
Thick Ascending Limb Distal tubule Collecting Duct
Note: There is an accumulation of NaCl and Urea in the interstitial fluid in the medulla of the kidney
Urea is a byproduct of protein metabolism produced by liver and some is mainteined in medulla but most is excreted in the urine
-
Na+ Factoids
Active Transport Proximal Distal Thick segment of ascending limb
Passive Diffusion Loop of Henle: the Na enters the cells, which then
expel it because of the Na/K pump (think SGLT-1/2 transporters)
-
Distal tubule and collecting duct
Na reabsorption (and K/H secretion) Adjusted in accordance with body needs Hormone-sensitive:
Aldosterone from adrenal cortex increases Na reabsorption (and K/H secretion)
-
Secretion
Secretion is often used for what we called Excreted Solutes Increases amount of substance that is excreted in urine Examples:
Urea (waste product of protein metabolism) Medications, such as antibiotics
-
pH of extracellular fluid (ECF) is tightly regulated
Enzyme systems function optimally within small pH ranges ECF pH normally 7.3 7.5 Diet and associated metabolic processes alter H+ production
Meat proteins: increase H+ generation Plant proteins: herbivores (horses, cows) and vegetarians; less H+
Defense of acid-base homeostasis is achieved by 3 systems that act in concert (Immediate):
Buffers act as sponge to bind free H+ in ECF which minimize effects of H+ on pH (only free H+ contribute to pH)
Kidneys control bicarbonate, while respiratory controls carbon dioxide (Short-term = minutes):
Ventilation (respiratory system removes or retains CO2) (Long-term = hours to days):
Renal handling (reabsorption, excretion) of HCO3- and H+
-
Renal Contribution to Acid-Base Balance
Proximal tubule Bicarbonate reabsorption Carbonic anhydrase
enzyme present in cytosol and on brush border surface of tubular cells
Distal Tubule Proton secretion NH3 and Phosphate in
tubular fluid serve as buffers to absorb the H+
Proximal Distal Tubular Cell Tubular Cell
Tubular fluid Tubular fluid
-
Regardless of hydration, 2/3 of water will be reabsorbed at proximal tubule Little Xs are NaK2Cl Osmolarity of the fluid in interstitial fluid is 600 mo/L Urea is added as well, which increases osmolarity Waters move through aquaporins and channels
-
Kidney is responsible for: Conversion of Vitamin D to its active form Release of erythropoietin (stimulation of red blood cell production) Regulates blood pressure Regulates electrolyte levels Regulates acid-base balance