Rashes in pediatrics Shilpa R Singh MD. Measles RNA virus, Paramyxoviridae Family Humans are the...
61
Rashes in pediatrics Shilpa R Singh MD
-
Upload
kaitlynn-seal -
Category
Documents
-
view
215 -
download
1
Transcript of Rashes in pediatrics Shilpa R Singh MD. Measles RNA virus, Paramyxoviridae Family Humans are the...

Rashes in pediatricsShilpa R Singh MD

Measles
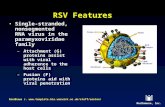
RNA virus , Paramyxoviridae Family
Humans are the only host
Incidence declined in 1963 after vaccine
Current rate < 1case /1,000,000 population
Infection imported from abroad, outbreaks occur in community with low vaccination

Transmission
• Respiratory tract or conjunctivae through droplet carrying virus
• Infectious from 3 days before up to 4-6 days after the onset of rash

Pathology
• Necrosis of respiratory tract epithelium and lymphocytic infiltrate
• Small vessel vasculitis on skin and oral mucosa
• Fusion of infected cell result in multinucleated giant cells Warthin – Finkeldey Giant cell , Pathognomonic

Clinical Manifestation
Prodromal symptoms - fever, malaise, dry (occasional croupy) cough, coryza, conjunctivitis with clear d/c, marked photophobia
1 to 4 days prior to rash - Koplik spots on the buccal mucosa
Koplik spots ( 50 – 70 %) - tiny, bluish-white dots surrounded by red halos on buccal mucosa opposite lower molars

rubeola (nine-day or red measles)
Day 3 or 4 - blotchy, erythematous, blanching, maculopapular exanthem appears
Rash begins at the hairline and spreads cephalocaudally and involves palms and soles
Rash typically lasts 5 - 6 days
Can see desquimation in severe cases


rubeola (nine-day or red measles)
Patients can be systemically ill
Incubation period 9-10 days
Patients contagious from 4 days prior to the rash until 4 days after the resolution of the rash
Highly contagious - 90% for susceptible people

rubeola (nine-day or red measles)
High morbidity and mortality common in children in underdeveloped countries
Peak season is late winter to early spring
Potential complications - OM, PNA, obstructive laryngotracheitis, acute encephalitis
Vaccination is highly effective in preventing disease

rubeola (nine-day or red measles)


Diagnosis and Complications
• Clinical Diagnosis
• Labs – Decreased White count ( Lymphocytes more than neutrophils )
• Serum IgM ( Appears 1 -2 days after onset of rash , till 1 month )
• Most common cause of death – Pneumonia
• Most common complication – Acute Otitis media
• Others – Tracheitis , bronchiolitis , febrile seizure , encephalitis , hemorrhagic measles ,keratitis , myocarditis

Treatment and Prevention
• Supportive
• No prophylactic antibiotics
• Vitamin A ( 6 months – 2 yrs , hospilatized , malnutrition other complications )
• Vaccination 2 dosages , 1st dose 12- 15 months , 2nd dose 4 -6 yrs of age
• MMR – live vaccine , do not give to pregnant or immunosuppressed

Rubella (german measles)
Rubella virus (Togaviridae )
Little or no prodrome in children
In adolescents - 1-5 days of low-grade fever, malaise, headache, adenopathy, sore throat, coryza
Exanthem - discrete, pinkish red, fine maculopapular eruption - begins on the face and spreads cephalocaudally
Rash becomes generalized in 24 hours and clears by 72 hours


rubella (german measles)
Suboccipital , post auricular and anterior cervical lymph nodes common
Forchheimer spots - small reddish spots on the soft palate - can sometimes be seen on day 1 of the rash
Arthritis and arthralgias - frequent in adolescents and young women - beginning on day 2 or 3 lasting 5-10 days
Up to 25% of patients are asymptomatic - serology testing may be necessary to establish the diagnosis

Forchheimer spot

rubella (german Measles)
Important in establishing the diagnosis if the patient is pregnant or has been in contact c a pregnant woman
Peaks in late winter to early spring
Contagious from a few days before the rash to a few days after the rash
Incubation period 14-21 days
Complications - rare in childhood - arthritis, purpura thrombocytopenia, mild encephalitis

rubella (german Measles)

Congenital Rubella Syndrome
• Deafness
• Ocular - Cataract , Retinopathy
• Heart – PDA , Pulmonary artery stenosis , Pulmonary valve stenosis
• Low birth weight
• Neonatal Purpura

Varicella (chickenpox)
Caused by varicella-zoster virus
Highly contagious
Brief prodrome of low-grade fever, URI symptoms, and mild malaise may occur
Rapid appearance of puritic exanthem

varicella (chickenpox)
Lesions appear in crops - typically have 3 crops
Crops begin in trunk and scalp, then spread peripherally
Lesions begin as tiny erythematous papules, then become vesicles surrounded by red halos
Lesions began to dry - umbilicated appearance, then surrounding erythema fades and a scab forms

varicella (chickenpox)
Hallmark - lesions in all stages of evolution
All scabs slough off 10-14 days
Scarring not typical unless superinfected
Cluster in areas of previous skin irritation
Puritic lesions on the skin
Painful lesions along the oral, rectal, and vaginal mucosa, external auditory canal, tympanic membrane

Varicella Lesions

varicella (chickenpox)
Occurs year-round, peaks in late autumn and late winter through early spring
Incubation period ranges from 10-20 days
Contagious 1-2 days prior to rash until all lesions are crusted over
Complications - secondary bacterial skin infections (GAS), pneumonia, hepatitis, encephalitis, Reye syndrome

varicella (chickenpox)
Severe in the immunocompromised host - can be fatal
Can have severe CNS, pulmonary, generalized visceral involvement (often hemorrhagic)
Need to get varicella-zoster immunogloblin 96 hours post-exposure to possible varicella

varicella (chickenpox)

Adenovirus
30 distinct types
Variety of infections including conjunctivitis, URIs, pharyngitis, croup, bronchitis, bronchiolitis, pneumonia (occ fulminant), gastroenteritis, myocarditis, cystitis, encephalitis
Can be accompanied by a rash - variable in nature
Typically can see - conjunctivitis, rhinitis, pharyngitis c or s exudate, discrete, blanching, maculopapular rash

adenovirus
Can see anterior cervical and preauricular LAD, low-grade fever, malaise
Peak season is late winter through early summer
Contagious during first few days
Incubation period 6-9 days

Coxsackie hand-foot-and-mouth disease
Brief prodome - low-grade fever, malaise, sore mouth, anorexia
1-2 days later, rash appears
Oral lesions - shallow, yellow ulcers surrounded by red halos
Cutaneous lesions - begin as erythematous macules then evolve to small, thick-walled, grey vesicles on an erythematous base

Coxsackie hand-foot-and-mouth disease
Highly contagious
Incubation period 2-6 days
Lasts 2-7 days
Peak season summer through early fall
If no cutaneous lesions - herpangina
less painful and less intense than herpes gingivostomatitis



erythema infectiosum (fifth disease)
Caused by Parvovirus B19
Affects preschool and young school aged children
Peak incidence in late winter and early spring, but it is seen year round
Characterized by rash - large, bright red, erythematous patches over both cheeks - warm, but non-tender

erythema infectiosum (fifth disease)
Facial rash fades, then see a symmetrical, macular, lacy, erythematous rash on the extremities
Resolution occurs within 3-7 days of onset
Transmitted by respiratory secretions, replicates in the RBC precursors in the bone marrow
Can cause aplastic crisis in patients with sickle cell disease, other hemogloblinopathies, and other forms in hemolytic anemia

erythema infectiosum (fifth disease)

Question 10 month old infent is seen in clinic with history of fever up to 39.44 C (103 F ) for
past 3 days . The child is playful and physical exam is unremarkable except for
fever . No sick contacts at home . She does not attend day care .Of the folowing most
likely virus causing this childs fever 1.Parvo virus
2. Herpes Simplex Virus 3. HHV-6
4. Epstein Barr virus (EBV ) 5. Cytomegalovirus

roseola infantum (exanthem subitum)
Febrile illness affecting children 6-36 months
Human herpesvirus 6 is causative agent
Symptoms include:
fever, usually >39
anorexia
irritability
these symptoms subside in 72 hours

roseola infantum (exanthem subitum)
As fever defervenscences, usually an erythematous, maculopapular rash that appear on the trunk and then spread to the extremities, face, scalp, and neck
Occurs year-round
More common in late fall and early spring
Incubation period thought to be 10-15 days

roseola infantum (exanthem subitum)

Infectious mononucleosis
Acute self-limiting illness of children and young adults
Caused by EBV
Transmission by oral contact, sharing eating utensils, transfusion, or transplantation
Incubation period 30-50 days (shorter, 14-20 days, in transfusion-acquired infection)
Don’t usually see “classic mono” in young children

Infectious mononucleosis
Prodrome - fatigue, malaise, anorexia, HA, sweats, chills lasting 3-5 days
Symptoms
fever - can have wide daily fluctuations
pharyngitis c tonsillar and adenoidal enlargement c or s exudate, halitosis, palatal petechiae
LAD - anterior cervical and posterior cervical - in classic cases, generalized LAD toward end of wk 1

Infectious mononucleosis
Symptoms cont:
splenomegaly - develops in 50% of patients in 2nd-3rd wk
hepatomegaly in 10% of patients
exanthem - erythematous, maculopapular, rubelliform rash in 5-10% of patients

Infectious mononucleosis
Complications:
pneumonia
hemolytic anemia and thrombocytopenia
icteric hepatitis
acute cerebellar ataxia, encephalitis, aseptic meningitis, myletis, Guillain-Barre
rarely myocarditis and pericarditis

Infectious mononucleosis
Complications cont:
upper airway obstruction from tonsillar and adenoidal enlargement
seen more often in younger patients
children < 5 yrs of age c obstruction are more likely to have secondary OM, recurrent bouts of OM, tonsillitis, and sinusitis
splenic rupture

Infectious mononucleosis
Diagnosis:
classic finding - lymphocytosis (50% or more) c 10% atypical lymphocytes
80% or more of patients c elevated liver enzymes
Monospot - detects heterophil antibodies - specific, not as sensitive - 85% of adolescents + and fewer younger patients
specific EBV antibody titers and PCR

Infectious mononucleosis
DDx
If fever and exudative tonsillitis predominate
GAS, diphtheria, viral pharyngitis
If LAD and splenomegaly predominate
CMV, toxo, malignancy, drug-induced mono
If severe hepatic involvement
viral hepatitis, leptospirosis

herpes simplex infections
Primarily involve the skin and mucous surfaces
Can be disseminated in neonates and immunocompromised hosts
Produces primary infection - enters a latent or dormant stage, residing in the sensory ganglia - can be reactivated at any time

herpes simplex infections
HSV-1
• >90% of primary infections caused by HSV-1 are subclinical
• more common
• HSV-2
• usually the genital pathogen
• usual pathogen of neonatal herpes

herpes simplex infection
• Diagnosis
• usually made clinically
• can scrap base of vesicle and a special stain - Giemsa-stained (Tzanck)
• ballooned epithelial cells c intranuclear inclusions and multinucleated giant
• viral cultures take 24-72 hours

Primary herpes simplex infections
• Herpetic gingivostomatitis
• high fever, irritability, anorexia, mouth pain, drooling in infants and toddlers
• gingivae becomes intensely erythematous, edematous, friable and tends to bleed
• small yellow ulcerations c red halos seen on buccal and labial mucosa, tongue, gingivae, palate, tonsils

primary herpes simplex infections
• Herpetic gingivostomatitis
• yellowish white debris builds on the mucosal surfaces causing halitosis
• vesiculopustular lesions on perioral surfaces
• anterior cervical and tonsillar LAD
• symptoms last 5-14 days, but virus can be shed for weeks following resolution


primary herpes simplex infections
• Skin infections
• fever, malaise, localized lesions, regional LAD
• direct inoculation (usually cold sores)
• lesions are deep, thick-walled, painful vesicles on an erythematous base - usually grouped, but may be single
• lesions evolve over several days - pustular, coalesce, ulcerate, then crust over

primary herpes simplex infections
• Skin infections
• most common sites are lips and fingers or thumbs (herpes whitlow)
• eyelids and periorbital tissue infection can lead to keratoconjunctivitis - dx by dendritic ulcerations on slit lamp exam
• can lead to visual impairment - consult ophtho

Recurrent herpes simplex infection
• Triggers include fever, sunlight, local trauma, menses, emotional stress
• Seen most commonly as cold sores
• Prodrome of localized burning, itching or stinging before eruption of grouped vesicles

recurrent herpes simplex infection
• Vesicles contain yellow, serous fluid and are often smaller and less thick-walled than the primary lesions
• Vesicular fluid becomes cloudy after 2-3 days, then crusts over
• Regional, tender LAD

herpes zoster (shingles)
• Caused by varicella-zoster virus
• After primary infection, virus lies dormant in genome of sensory nerve root cell
• Postulated triggers include mechanical and thermal trauma, infection, debilitation as well as immunosuppression
• Lesions are grouped, thin-walled vesicles on an erythematous base distributed along the course of a spinal or cranial nerve root (dermatome)

herpes zoster (shingles)
• Lesions evolve from macule to papule to vesicle then crusted over a few days
• May have associated nerve root pain - not common in pediatrics - usually short-lived unless it involves a cranial nerve root dermatome
• +/- fever or constitutional symptoms
• Regional LAD common

herpes zoster (shingles)
• Thoracic, cervical, trigeminal, lumbar, facial nerve dermatomes (order of frequency)
• If cranial nerve involvement - prodrome of severe HA, facial pain, or auricular pain prior to the eruption
• Affected patients can transmit varicella, but less of a problem b/c lesions are often covered by clothing and the o/p is not involved in most cases

herpes zoster (shingles)