Rapid Appraisal of DHIS
56
-
Upload
saeed-ahmed -
Category
Documents
-
view
65 -
download
0
description
Rapid Appraisal of DHIS
Transcript of Rapid Appraisal of DHIS

Rapid Appraisal of District Health Information System
0

Rapid Appraisal of District Health Information System
1
REPORT DEVELOPERS
This report has been developed by a team headed by Dr. Farooq Azam Jan, DHIS Expert
in close coordination of Mr. Syed Khalid Hussain and Mr. Asad Afzal - HIS Consultants
under the technical supervision of Dr. S.M. Mursalin, Technical Coordinator HIS, WHO.
WHO issued contracts /APWs to following professionals to support this study.
Dr. Farooq Azam Jan
WHO Registration: 2011/173410-0
P.O. 200451300
EMPAK1005227 / 3.1.3 / 57225
Mr. Khalid Hussain Shah
WHO Registration: 2011/185121-0
P.O. 200457286
EMPAK1005227 / 3.1.3 / 57640, 57225
Mr. Asad Afzal Humayoun
WHO Registration: 2011/183433-0
P.O. 200457230
EMPAK1005227 / 3.1.3 / 57640, 57225

Rapid Appraisal of District Health Information System
2
Table of Contents ACKNOWLEDGEMENT 04
ABBREVIATIONS 05
EXECUTIVE SUMMARY 06
1. BACKGROUND 10
1.1 Introduction 10
1.2 Objectives 10
1.3 Districts Selected for Survey 11
1.4 Methodology 11
1.5 Operational Hierarchy 12
2. DATA ANALYSIS AND OBSERVATION 13
2.1. DHIS Functionality at Facility Level 13
2.1(a) DHIS Infrastructure & Functionality 13
i. Respondents by Facilities and Designation 13
ii. Flood Impact on Health Facilities & DHIS Functionality 13
iii. DHIS Trained Staff at the Health Facilities 14
iv. Status of DHIS Trained Staff Compiling Monthly DHIS Data at Facilities 14
v. Availability of DHIS Data Collection Tools and Daily Update 15
2.1(b) DHIS Data Quality Parameters 16
i. Availability of DHIS Procedure Manual & TORs 16
ii. Staff Understanding on DHIS Reporting Tools vs Inconvenience 16
iii. Knowledge and Practice of Monthly Submission of DHIS Reports 17
iv. Reporting Regularity 17
v. Feedback to Facilities vs Type of Feedback 17
vi. Use of DHIS Data for Planning & Management 18
vii. Situaiton of DHIS Tools at the Health Facilities 18
viii. Keeping up Record of the Monthly DHIS Reports 19
2.1(c) DHIS Operational Needs 19
i. Staff Trainings Needs 19
ii. Replenishment of DHIS Tools Supply 20
iii. Need of for Other DHIS Resources 20

Rapid Appraisal of District Health Information System
3
2.2 DHIS Functionality at Managerial Level 20
2.2(a) DHIS Infrastructure & Functionality 20
i. Respondents at Districts by Designation and DHIS Functionality 20
ii. Availability of DHIS Trained Human Resources at Districts 20
iii. Status of Monthly DHIS Reporting Compliance vs Time of reporting 21
iv. Data Accuracy of the Field Units 21
2.2(b) DHIS Quality Parameters 22
i. Usage of Different Quality Factors of the System 22
ii. Validation of DHIS Data Reported in October 2011 23
2.2(c) DHIS Operational Needs 24
i. Initial / Refresher DHIS Training 24
ii. Need of Other Resources 24
3. CONCLUSIONS 25
4. RECOMMENDATIONS 26
ANNEXURES
A. Selected District & Total Number of Health Facilities Visited 28
B. List of Offices/ Facilities Visited 29
C. List of DHIS Data Instruments 31
D. Ensuring Data Quality 32
E Study Supervision and Team 33
F. Timeline of Activities / Work Plan 34
G. Field Data Collection Questionnaire (Managerial Level) 35
H. Field Data Collection Questionnaire (Facility Level) 38
I. Surveyed Data Output Tables 41
J. Monthly DHIS Reporting Form (PHC) 47
K. Monthly DHIS Reporting Form (Secondary Hospitals) 51

Rapid Appraisal of District Health Information System
4
Acknowledgement
In any healthcare system the one most exciting input is the availability of an efficient
Health Management Information System. Though, the national health status of Pakistan
yet to show more achievements compared to many other countries. Federal Ministry of
Health, in early 90s took concrete steps for setting up a coherent and a uniform system of
data collection known as Health Management Information System (HMIS) initially for
public health sector. Several international partners assisted this initiative. Later on to
make this system more comprehensive at the district level it was transformed to District
Health Information System. DHIS gathers information not only from first level care
services but also from District and Tehsil Hospitals. The ultimate objective of all these
efforts is to produce timely information of good quality for decision makers at various
levels of working.
Since the implementation of DHIS at all the districts of Punjab province in 2008, this
performance assessment exercise was unique in its kind. Prime objective of this study
was to realize if the new system is meeting the intended targets and its functionality
adequately as was designed.
I am confident that this report would help Provincial and District Health Managers to
improve evidence based decision making in their respective areas. Here I would like to
thank Dr. Anwar Janjua, former Director Health Services (MIS) Punjab for his kind
support and tremendous cooperation that enabled me and my team to collect the desired
data and other necessary information from the district and health facilities.
Further, I would like to appreciate the overall technical supervision extended by Dr. S.M.
Mursalin, Technical Coordinator, Health Information Management Unit/WHO.
Significant inputs made by Mr. Imran Majeed especially during the study design phase
and development of questionnaire are to be acknowledged. Here I would also thank my
colleagues Mr. Khalid Hussain and Mr. Asad Hamayoun for their hard work and
concerted efforts in completing this assignment and finalizing the End Assignment
Report.
Dr. Farooq Azam Jan January 31, 2012 Team Leader

Rapid Appraisal of District Health Information System
5
Abbreviations
ANC Antenatal Care
BHU Basic Health Unit
CD Civil Dispensary
DHIS District Health Information System
DHQ District Headquarters
DOH District Officer Health
DEO Data Entry Operator
EDO-H Executive District Officer-Health
FLCF First-Level Care Facility
FP Family Planning
GRD Government Rural Dispensary
HMIS Health Management Information System
HR Human Resources
LHS Lady Health Supervisor
LHV Lady Health Visitor
LHW Lady Health Worker
LQAS Lot Quality Assurance Sampling
MCH Maternal and Child Health
MOH Ministry of Health
NGO Non Governmental Organization
OPD Outpatient Department
PHC Primary Healthcare
RHC Rural Health Center
SHC Secondary Healthcare
THQ Tehsil Headquarters Hospital
WHO World Health Organization

Rapid Appraisal of District Health Information System
6
Executive Summary
The provision of timely and effective healthcare services is the key objective of any country’s
health system. To maintain the health system in a good functioning status it is imperative to
regularly monitor it through an efficient Health Information System. This system should be
able to provide timely and qualitative information for evidence based decision making
process. Realizing the impact of this very important factor specially in the public health sector
government initiated a nationally standardized data generation system at all levels called
Health Management Information System (HMIS) in early 90s.
Given the experience both in the development of information systems, the new information
needs and also, the initiation of several new programs this system has been modified to
District Health Information System (DHIS) in 2007. DHIS now have a much wider scope than
the old HMIS. The process led to revision of data collection indicators, tools and software.
The upgraded version of DHIS was completed in 2007 and its implementation at district
levels. But as this implementation was supposed to be carried out by the provincial health
departments thus its timeframe varied from province to province. It was encouraging to note
that Punjab Health Department took the lead to implement this program in all its 36 districts
by end 2007. It was therefore high time to assess if the new system is being implemented as
was primarily envisaged.
This assessment study is based mainly on three focused areas of the system e.g. (i)
Infrastructure & Functionality (ii) Data Quality and (iii) DHIS Operational Needs . Firstly to
analyze and document the existing functionality of DHIS in districts, mainly to get sense of its
functioning and work out immediate needs with regards to availability of Instruments,
equipment and training needs, software issues, data recording and its transmission. Second,
despite regular flow of data from the first level care facility (FLCF) to District HIS Cells and
then to Provincial or National Cells there still exist serious concerns among the provincial and
district managers on data quality and validity. Question is what additional measures are
needed to improve data quality and use. Thirdly to identify the operational needs and areas of
future support for improving the efficiency of information system
To facilitate this process a very simple coded questionnaires was developed both for
managerial and facility information. The theme of the questionnaire was based on three key
assessment areas of the district health information system e.g. (i) DHIS Infrastructure &
Functionality (ii) Data Quality and (iii) DHIS Operational Needs. Both close and open ended
questions were included in the questionnaire. Further the questions were derived from the
DHIS Procedures Manual and the monthly DHIS reporting forms to be used at Primary Health
Care and Secondary Health Care Facilities
Based on the originally approved/agreed plan between DHIS Directorate, Provincial Health
Department and WHO, in total 10 districts were to be selected comprising districts both from
flood and non flood affected districts. Therefore, to keep a balance, five districts were selected
from flood affected areas and other five from non affected areas. The final selection of district
names was made by the Provincial Health Directorate, which was primarily based on resource
availability for the study and to ensure an even geographical coverage.

Rapid Appraisal of District Health Information System
7
The districts included in this survey were; Rawalpindi, Jhelum, Sheikhupura, Okara,
Faisalabad, Bhakkar, Layyah, Muzaffargarh, Dera Ghazi Khan and Rajanpur. In total 15
health facilities were planned to be visited per district with the aimed at to consider a mixtures
of various types of health facilities from each district. Therefore a total of 150 facilities were
visited. From these 10 Forms (annex-A) and 150 Forms (annex-B) were finally collected.
The collected data was finally entered into the computer software SPSS (V-16) and analyzed
both in graphical and tabulation form. Following are some major findings of this rapid
appraisal;
(a) DHIS Status at Facility Level
i. DHIS Infrastructure & Functionality
All health facilities affected by the flood of 2010-2011 were found re-habilitated.
DHIS functioning observed to be an integral part of the public sector healthcare
delivery system, as each and every health facility either it is primary or secondary
healthcare, are regularly generating the health information of their respective areas.
The 80% of the facilities’ incharges (e.g. 133 out of 150) got DHIS training, whereas
the remaining 20% were observed as either untrained or self-trained.
Among the staff deputed for preparation of monthly DHIS reports at the facilities it
was observed that 92% (138 out of 150) were properly trained for this task.
The availability of different data recording tools/registers was seen at 82% and 75%
facilities do daily updation of these registers.
ii. DHIS Quality
Better understanding of the staff about DHIS forms was reported at 91%, whereas the
remaining staff reported to face difficulty in understanding the Section-II, III and
Section-VIII of the forms. Besides the junior rank officials, some Senior Medical
Officer, Medical Officers and Female Medical Officers were also included in this
category.
DHIS procedure manual was found at 71% facilities (i.e. 107 out of 150). Similarly
DHIS relevant TORs of the staff seen at 51% facilities.
Almost all the staff had correct knowledge and practice regarding submission of
monthly DHIS reports to their respective EDO-Health.
During the last 12-months, 100% reporting regularity was observed at the facilities,
however only three (03) facilities missed their five reports due to floods.
It was encouraging to note that the 72% of the visited facilities (108 out of 150)
confirmed that they regularly receive feedback from their respective EDOs-Health.
However majority of the feedback 44% (66 facilities) was through discussion on
monthly targets of the facilities and their performance.
Almost half of the surveyed facilities (54%) used DHIS data for their routine planning.

Rapid Appraisal of District Health Information System
8
A considerable number of facilities faced shortage of DHIS tools, as during 2011; 18%
(27 out of 150) of the surveyed facilities faced this problem.
Almost all the targeted facilities kept copies of their monthly sent reports for record.
iii. DHIS Operational Needs
There was a dire need for the supply of DHIS Tools / instruments in most of the
facilities/ Districts.
DHIS tools replenishment needed by 67% of the facilities and majority of them need
one year supply in advance.
The need of trained staff was reported by 43% (64) of the facilities. Whereas, 41% (61)
facilities needed DHIS tools supply and some 23% (35) expressed for other kind of
needs (e.g. Computer supplies/software). Other important expressed need was for
online DHIS Data Entry System.
(b) DHIS Situation at Managerial Level
i. DHIS Infrastructure & Functionality.
Comparing districts, the managerial level questionnaires was responded by the
Statistical Officers/DHIS Coordinators (80%), whereas only 20% EDOs-Health
participated in this survey.
All desired hardware and the corresponding DHIS software was found available at all
ten districts. Further the DHIS activities are being handled by an independent DHIS
Cell, which is very encouraging.
All the District DHIS Coordinators received DHIS training, but only six Data Entry
Operators reported to have a regular training whereas the rest four did not have.
The monthly reporting compliance by the districts was observed to be excellent.
The data accuracy or consistency among facilities and districts HMIS units was
observed to be excellent (81% - 100%).

Rapid Appraisal of District Health Information System
9
ii. Data Quality.
Almost all districts surveyed were found using DHIS data for LQAS techniques, (Lot
Quality Assurance sampling), for both-way feedback, their service monitoring and
district health planning. In the context of planning, it was observed that EDO-H didn’t
use data for strategic planning, but they did use this for day to day managerial issues.
A negligible difference of reported figures collected from the health facilities and with
the one with respective EDOs Health was observed.
iii. DHIS Operational Needs.
It was observed that District DHIS Office staff at the districts already reported to be
trained on DHIS functionality, however they asked for further training.
Regarding the need of resources out of those ten interviewed, nine district level
respondents asked for refresher training, eight requested for system maintenance, six
demanded computer hardware and four asked for updated DHIS software. Half of the
districts asked for computer operators.

Rapid Appraisal of District Health Information System
10
1. Background
1.1 Introduction
National HMIS Cell, being is functioning since 1998 and has the mandate to assist Health
Sector in development and launch of a nationally standardized Health Information System.
National Health Information System is a mechanism of data collection, transmission,
analysis and information feedback for all health related information. Over the years National
Health Information System has become one of the major data source for the health sector in
the country.
Based on long implementation experience and demand from end users the existing system is
now being transformed to a more efficient District Health Information System (DHIS). The
reformed system, unlike the previous system, would gather and collate information from
secondary hospitals (i.e. DHQ, THQ Hospitals) and some other important health care levels,
as well. Currently out of 134 districts, staff from 96 districts have been successfully trained
and shifted on District Health information System (DHIS). From these, nearly 65 districts
have started regular reporting since last six months. This HIS Unit sponsored by WHO is
responsible for data collection and analysis for the health data.
Many partners including, WHO have been providing institutional support for development
and the improvement of National Health Information System at the Federal, Provincial and
District levels. Punjab Implemented the new system’ DHIS in all districts (36). Health
Department of Punjab has requested WHO to conduct this appraisal for improvement and
strengthening the system.
1.2 Objectives.
Since 2009 DHIS is fully implemented and reporting at each District of Punjab province,
thus there is a need for a quick rapid appraisal of District Health Information System mainly
for improving the efficiency of DHIS.
Following were the more specific objectives;
To realize the current situation of Infrastructure & Functionality
To assess the available Data Quality and
To assess the DHIS Operational Needs
Rapid Appraisal of District Health Information System
11
1.3 Districts Selected for Survey
The selection of the districts was made from two basis i.e. one where the devastating flood of
2010-2011 damaged the public health settings and the second non flood affected areas. The list
of selected districts can be seen from the table below.
Non-Flood Affected Districts Flood Affected Districts
1. Rawalpindi 1. Layyah
2. Jhelum 2. Bhakkar
3. Sheikhupura 3. Muzaffargarh
4. Okara 4. Dera Ghazi Khan
5. Faisalabad 5. Rajanpur
1.4 Methodology
a) Sampling Protocol:
Based on the originally approved/agreed plan between DHIS Directorate, Provincial Health
Department and WHO, in total 10 districts were to be selected comprising districts both from
flood and non flood affected districts. Therefore, to keep a balance, five districts were selected
from flood affected areas and other five from non affected areas. The final selection of district
names was made by the Provincial Health Directorate, which was primarily to ensure an even
geographical coverage in non flood affected districts.
Regarding the total number of health facilities to be surveyed per district, a convenient random
sampling technique was adopted. This aimed at to consider a mixtures of various types of
health facilities from a district. In total 15 health facilities were planned to be visited per
district. Therefore a total of 150 facilities were visited. From these 150 Forms (annex-B) were
finally collected. Provincial Health Departments are adopting same procedure for monitoring
and data quality in their respective districts, called Lot Quality Assurance Sampling
Technique. (LQAS)
The type/ list of these 15 health facilities/district is as follows;
(i) Managerial Office = 1 (EDO-H office)
(ii) Health Facilities;
- DHQ = 1
- THQ = 1
- MCH Centre = 3
- Dispensary/CD/GRD = 3
- RHC = 3
- BHU = 4
Total = 16

Rapid Appraisal of District Health Information System
12
b) Data Collection Tool/Questionnaire
A very simple and easy to understand questionnaire was developed both for managerial and
facility information. The theme of the questionnaire was based on three key areas of the
district health information system e.g. (i) DHIS Infrastructure & Functions (ii) Data Quality
and (iii) DHIS Supply/Other Needs. Both close and open ended questions were included in the
questionnaire. Further the questions were derived from the DHIS Procedures Manual and the
monthly DHIS reporting forms to be used at Primary Health Care and Secondary Health Care
Facilities.
Moreover, to check the respondent’s knowledge and practice regarding monthly DHIS
reporting activities, relevant questions were included in questionnaire. LQAS being an
authenticated way of observing data quality, figures pertaining to five basic monthly reported
indicators were also surveyed (see questionnaires at annexure).
c) Data Collection Approach
For the field visits, ten Data Collectors/Enumerators were engaged (i.e. one per district),
where the District Focal Person (DHIS Coordinator of the respective district) joined them
from respective districts. They also helped them for selection of facilities and preparation of
field visit routing plan. Enumerators were given one day training at Islamabad on data
collection strategy and on the understanding of data collection tools (questionnaires).
d) Data Analysis Tool
The collected data was entered and analyzed in computer software SPSS (V-16) and the
analytical views and observations are given both in graphical as well as tabulated form.
1.5 Study Operational Hierarchy

Rapid Appraisal of District Health Information System
13
2. Data Analysis and Observation
Study team was much satisfied with the collection of desired data as a total of ten filled-in
forms were received from the managerial offices/levels (EDOs-Health) and 150 from the
targeted facilities. The collected data was entered into the computer software SPSS (V-16),
aiming at to get appropriate data analysis. The point-wise data analysis & discussions based on
the data collection questionnaire for both facility and managerial levels are as follows;
2.1 DHIS Functionality at Facility Level 2.1(a) DHIS Infrastructure & Functionality i. Respondents by Facilities and Designation
The field survey at the targeted health facilities revealed that in total nine District
Headquarters Hospitals were interviewed against the planned ten. Reasoning of this
when confirmed was that DHQ Hospital, Rawalpindi doesn’t report the monthly DHIS
data to their EDO-Health. However, to cover the sampling size in number, an additional
Tehsil Headquarters Hospital of Rawalpindi district i.e. total 11 THQ Hospitals instead
of planned 10 were included. The other facilities e.g. MCHCs, GRDs, RHCs and BHUs
were covered according to approved plan (see table # annexure-H).
Out of the selected 150 health facilities majority of the respondents (88) were
professionals and qualified officials, which significantly compliment the credibility of
our data. The graph below shows the number and type of respondents in this study.
ii. Flood Impact on Health Facilities & DHIS Functionality It is observed that out of the total 75 health facilities, selected from the five flood
affected districts (i.e. Layyah, Bhakkar, Muzaffargarh, DG Khan & Rajanpur), only five
(05) facilities were reported to be seriously affected by floods. All were later re-
habilitated by the health departments.
43
2624 24
1412
41 1 1
0
5
10
15
20
25
30
35
40
45
50
Medical Officer
Dispenser LHV Sr. Medical Officer
Medical Supdtt.
Medical Technician
Woman Medical Officer
DOH Pharmasist Statistical Officer
Num
be
rs
Status of Respondents by Designation

Rapid Appraisal of District Health Information System
14
An encouraging point was that the monthly DHIS data reporting is now being
considered as an integral part by all the District Health Offices. Resultantly, almost all
the health facilities either primary or secondary type is regularly generating the health
information for District Health Offices.
iii. DHIS Trained Staff at the Health Facilities A timely, accurate and reliable data generation is well desired from this District Health
Information System. It is observed that this is more or less and this is absolutely
dependent upon the incharge of the health facilities. Therefore, their training on the
DHIS Data Collection and Reporting tools becomes critical. It was found during the
survey that out of 150 incharges of the facilities, 133 (80%) got DHIS training, whereas
for remaining 17 health facilities, no staff was formally trained in DHIS. So the DHIS is
being maintained either by untrained or a self-trained person.
In this context the situation by districts revealed that almost all the (100%) incharge of
the visited facilities at districts of Bhakkar, D.G. Khan, Jhelum, Muzaffargarh and
Okara got DHIS training. This was followed by Rawalpindi, Rajanpur, Sheikhupura
and Layyah with 80% - 87% interviewed staff trained Somehow, comparatively less
number of DHIS trained staff/ incharges (53% ) were found trained in District
Faisalabad. This needs to be further explored.
iv. Status of DHIS Trained Staff Compiling Monthly DHIS Data at Facilities DHIS reports are to be submitted on monthly basis from the health facilities to districts.
Therefore the training of health facility staff, preparing such reports becomes mandatory
for some good information. (i.e. DHIS-21 & DHIS-22).
100 100 100 100 100
87 8780 80
53
0102030405060708090
100
(Per
cen
t)
Status of DHIS Trained Staff by District

Rapid Appraisal of District Health Information System
15
Dispenser LHVMedical Officer
Medical Technician
NurseStatistical Assistant
Staff Deputed 87 23 20 13 2 5
Trained Staff 81 22 16 13 2 4
0
20
40
60
80
100
Nu
mb
ers
Status of Trained vs Untrained Staff Deputed for Monthly DHIS Reporting
97
86 84 83 83 82 8277
73 71
0102030405060708090
100
Perc
enta
ge
Status of Availability of Different Data Tools andTheir Daily Update by District
Tools Availability (%age)Daily Updation (%age)
Fortunately, the received data analysis showed some good results. As out of the 150
staff interviewed, 138 (92%) had DHIS Training on Data Collection Tools. While
analyzing for the type of staff trained, it was found that higher number of dispensers got
this training that was 81/87 (i.e. 93%). Other staff interviewed included LHVs. Where
all l22 were trained, Out of 20 Medical Officers interviewed 16 were trained. For
Medical Technicians out of 13 interviewed all were trained), nurses (total 2
interviewed) both were trained. Out of five (5) Statistical Assistants, four (4) were
found trained.
v. Availability of DHIS Data Collection Tools and Daily Up-date Availability of different data recording tools/registers (list annexed) and their daily
update was also observed during the survey. The overall analysis of the ten surveyed
districts showed that data collection tools were available in 82% of the facilities
surveyed. However, the daily updation was being done at 75% of the health facilities.

Rapid Appraisal of District Health Information System
16
0
3
6
9
12
15
# Fa
cilit
ies
Vis
ited
Status of Availability of DHIS Procedures Manual & TORs
Availability of Manual
Availability of TORs
The graph above shows that most of the health facilities of district Muzaffargah,
Bhakkar, Faisalabad, Layyah and Okara update their activity registers on daily basis,
which is very encouraging. On the other hand, some of the health facilities belonging to
districts of DG Khan, Sheikhupura, Rawalpindi, Rajanpur and Jhelum do not update
their record on daily basis.
2.1 (b) DHIS Data Quality Parameters i. Availability of DHIS Procedure Manual & TORs
One of the basic parameter for having good quality of data is to have ‘DHIS Procedural
manual’ for ready reference. So that in case of some ambiguity this manual could be
consulted. . The study revealed that out of 150 health facilities DHIS procedure manual
was available only at 107 facilities. On the other hand roles and responsibilities (TORs)
with respect to DHIS were found available at only 77 selected facilities. .
Among districts, considerable disparity in availability of procedure manual was
observed in the districts of Muzaffargarh, DG Khan, Jhelum, Okara and Rajanpur.
However, better availability of TORs was observed at districts of Muzaffargarh,
Layyah, Bhakkar and Faisalabad. However, comparatively lesser availability of DHIS
Manual was observed at Sheikhupura, Rawalpindi and Layyah.
ii. Staff Understanding on DHIS Reporting Tools vs Inconvenience Better understanding of the staff deputed at the health facilities (136 out of 150) on the
chapters and indicators of monthly DHIS form (DHIS-21) was observed in the Districts
of Bhakkar, DG Khan, Jhelum and Layyah. However, lesser understanding (14 out of
150) was noted in the districts Rajanpur, Rawalpindi, Sheikhupura and Faisalabad. Here
majority of the staff faced difficulty mainly to understand the Sections-II, III and VIII.
It is pertinent to mention here that Section-II of the form related to ‘monthly
performance’ of the health facility with reference to set their monthly targets. Section-
III gives data of OPD by gender and the age group and whereas Section-VIII relates to
‘maternal and child health’ activities.

Rapid Appraisal of District Health Information System
17
Receive Feedback
(72%)
No Feedback (28%)
Status of Health Facilities Received Feedback From EDO-Health on DHIS
Reports
It was noted that both junior levels staff (Medical Technician & LHVs) and the senior
rank officers i.e. Senior Medical Officer, Medical Officers and Woman Medical
Officers, also face difficulty in understanding DHIS forms and thus need necessary
refresher training in some of the districts.
iii. Knowledge and Practice of Monthly Submission of DHIS Reports
A question about the exact dates of submission of monthly report was asked. It was
observed that almost all the incharges of the health facilities had knowledge and
practice regarding the timing of submission of monthly DHIS reports to their respective
EDOs-Health. However, some variation between the knowledge and practice was
observed at Bhakkar, Faisalabad and Layyah district and this may be due to certain
follow up delays.
iv. Reporting Regularity In principle each health facility has to submit monthly report. It was seen that almost
all the health facilities compiles its monthly DHIS report and send regularly to their
respective EDO-Health office.
In this context, as per facilities record, it was noted that only three (03) health facilities
out of 150 surveyed missed their only five reports due to floods. Otherwise all of these
sent their monthly reports. These facilities included; Civil Dispensary, Gajanthal/ DG
Khan (missed one report), BHU Kotla Nasir / Rajanpur (one report) and THQ hospital,
Jampur / Rajanpur (three reports).
Regarding the data quality, it was noted that standardized monthly DHIS reporting form
is being used at all type of health facilities. In principle the routine healthcare activities
varies from each type of health facility. The review team observed that monthly data
forms being reported by a CD/GRD contained incomplete figures compared to the
information obtained from RHC or BHU level facility.
v. Feedback to Facilities vs Type of Feedback A proper and timely feedback mechanism plays key role not only to cover the short
falls of the missing data to be reported from the health facilities, but also, to positively
improve the healthcare services delivery at each level. Therefore, when inquired, out of
the 150 selected facilities, 108 (72%) informed said that these are regularly receiving
feedback from their respective EDO-Health. Remaining 42 (28%) facilities informed
that these didn’t receive such
feedback from higher formations.
Among districts, relatively better
response was obtained from the
districts of Okara, DG Khan,
Jhelum, Sheikhupura and
Rawalpindi. However, EDO-Health
Faisalabad, DG Khan and Rajanpur
need to enhance feedback to their
health facilities. .

Rapid Appraisal of District Health Information System
18
Yes(54%)
No(46%)
Health Facilities used DHIS Data for Planning
To a question on type of feedback the health facilities received. It was observed that
majority of the facilities 66 (44%) told by their respective EDO-Health to visit EDO’s
office and discuss the monthly targets and their performance etc. Some 26 (17%)
facilities responded that, their high ups called them to discuss the administrative and
managerial issues. At the 15 (10%) facilities correction of the monthly DHIS data was
asked. However, only one facility found to be received feedback on their stock and
supplies.
vi. Use of DHIS Data for Planning and Management Adequate and appropriate health data is desired not only for day to day operational use
but also for planning and management of the health services. During the survey, the
facility’s incharges were asked; either they use DHIS data for any kind of planning or
for any other management functions. It was realized that nearly half of the targeted
facilities (54%) use this data for their routine planning, whereas the remaining half
(46%) didn’t use it for any
purpose rather sent to their
EDOs-H.
Among districts, comparatively
good responses were received
from the districts of Jhelum,
Muzaffargah, Sheikhupura and
Bhakkar. On the other hand
facilities of D G Khan didn’t use
DHIS data for any kind of
planning. Similar response was
also reported from the Districts
of Rajanpur and Faisalabad.
It was asked as to what kind planning is done .It was found that they use data for
multiple reasons like for managing the medicine stock, setting of monthly OPD targets,
follow-up of disease pattern, field/seasonal planning, provision of maternal & child
healthcare and family planning services, EPI services planning, performance evaluation
of the staff and organization of community meetings.
vii. Situation of DHIS Tools at the Health Facilities To keep up the daily records of the different healthcare activities at any health facility,
sufficient stock of registers is essential. It was noted that during 2011 a considerable
number of health facilities e.g. 18% (27 out of 150) reported to have faced DHIS tools
shortage.
Among districts, better stock position was observed at district DG Khan and
Rawalpindi. It was followed by Faisalabad, Layyah, Okara, Bhakkar and Muzaffargah.
However, comparatively high stock-out of DHIS tools was observed at Sheikhupura,
Jhelum and Rajanpur.

Rapid Appraisal of District Health Information System
19
Facilities Didn't Faced
Shortage(82%)
1-Month Shortage
(15%)
3-Month shortage
(3%)
Facilities Faced
Shortage(18%)
Status of Facilities Faced Shortage of DHIS Tools
Trainings Not Needed
(15%)
Forms Filling(9%)
LQAS Technique
(11%)
Indicators' Analysis
(65%)
Staff Need Training
(85%)
Status of Staff Needs DHIS Trainings
To identify the duration
of this shortage, it was
noticed that 15% (20)
health facilities faced
such shortage for three
months or more, which
could be a matter of
concern for the district
health managers. On the
other hand, 3% (7)
facilities told that DHIS
tools shortage is there
for one month only.
viii. Keeping up Record of the Monthly DHIS Reports Since no computerized data management is being done currently at the health facilities,
therefore, pervious months records of monthly report is desired to be kept at the
facilities. This past record is essential for making comparison regarding OPD burden,
disease patterns and other healthcare activities. It was noticed that almost all the
targeted health facilities were found be kept such record. Only four facilities of district
Faisalabad reported not keeping up such record.
2.1(c) DHIS Operational Needs Needs i. Staff Training Needs.
It was realized that there is a significant need for training on DHIS tools and
mechanism. About 85% (128 out of 150) of the health facilities incharges recommended
for having refresher training in DHIS. Though, there were some extensive training
organized in DHIS but still
a need was felt for
improvement of their skill.
This survey revealed that
out of the total 150
interviewed staff, 65% (97)
asked for training in DHIS
‘indicators analysis, which
is a healthy sign. Some
11% (18) staff needs
training on LQAS
technique and 9% (13)
officials informed that they
need training on DHIS forms filling.

Rapid Appraisal of District Health Information System
20
0
2
4
6
8
10
EDO-Health Distt. Coordinator
# o
f D
istr
icts
Respondents Status by Designation
ii. Replenishment of DHIS Tools Supply To overcome the shortage of DHIS tools, it was enquired as to what kind of supply or
replenishment of DHIS tools is desired by the health facilities. The data analysis pointed
out that 67% (100 out of 150) of the facilities needed replenishment of tools. Further
investigation revealed that 27% (41 out of 100) need six months advance supply.
However, 39% (59 out of 100) of the health facilities desired to have whole year supply
of DHIS tools (see table # 14 at annexure-H).
iii. Need for other DHIS Resources
To a question on what kind of DHIS relevant resources they needed, multiple answers
were given by the respondents e.g. 160 responses were recorded from the 150 targeted
interviewees. Further data investigation concluded that 43% (64) wanted to have
additional human resources for DHIS. This was followed by 41% (61 responses) for
DHIS Tools and some 23% (35 responses) for various miscellaneous things.
2.2 DHIS Functionality at Managerial Level
2.2(a) DHIS Infrastructure & Functionality i. Respondents at Districts Level by Designation and DHIS Functionality
Comparing across districts, it was observed that majority of the managerial level
questionnaires 80% (8 out of 10) were responded by the Statistical Officers, who are also
performing at the districts as DHIS Coordinators. However, 20% (2 out of 10) were the
responded by EDO-Health.
Further the data analysis
revealed that at all 10 selected
districts DHIS was implemented
in letter and spirit. And all the
financial and technical support
for this program was extended
by the provincial health
department.
It was also noted that all desired
hardware and the corresponding DHIS software was provided to all the 10 targeted
districts. Moreover, the DHIS activities are being managed by an independent District
level DHIS Cell, which was an encouraging sign.
ii. Availability of DHIS Trained Human Resources by District Regarding the availability of type of staff trained in DHIS (e.g. EDO-Health, Distt.
Coordinator & Data Entry Operator), it was observed that all the District Coordinators
got DHIS training. On the other hand, 60% (six out of ten) EDO-Health were trained.
Another potential factor involved in this system is data entry operators. It was found that
70% of the data entry operators are exposed to DHIS Training.

Rapid Appraisal of District Health Information System
21
As per schedule, 1
5th of month(70%)
Not as per schedule
(30%)
Status of Timing for Sending Monthly DHIS Reports to Provincial DHIS Cell
iii. Status of Monthly DHIS Reporting Compliance vs Time of Reporting In almost all the districts visited it was observed the monthly DHIS reporting
compliance was in perfect condition. All the surveyed districts were found to be
sending their monthly reports to Provincial DHIS Cell regularly.
Regarding the timing of
sending monthly DHIS
reports by the EDO-Health
office to their provincial
DHIS Cell, it was
observed that out of the ten
surveyed districts, seven
districts (70%) were
observing stipulated time
schedule i.e. 15th
of next
month.
However, other three
(30%) though send their
reports regularly, but with some extra delay, which might be due to some
administrative reasons. These three districts were Districts of Rawalpindi, DG Khan and
Rajanpur.
iv. Data Accuracy of the Field Units The quality of data at district level depends upon what is being received from the health
facilities. . When asked from District Health Office about data accuracy it was informed
by the interviewed officials that 40% of their field units achieved the level of (80 -
100%) data accuracy. The other 30% achieved just level-2 (i.e. 71% - 80%) and level-3
(i.e. 51% - 70%).
100
7060
0
20
40
60
80
100
120
Dist. Coordinator DHIS Computer Operator EDO Health
Pe
rce
nta
ge
District Level Health Staff Trained in DHIS by Type.

Rapid Appraisal of District Health Information System
22
80% - 100%(40%)
71% - 80%(30%)
51% - 70%(30%)
Data Accuracy of Field Units
Among districts, better result
was reported from Jhelum,
Muzaffargah, Bhakkar and
Rajanpur. However,
comparatively low data
accuracy was observed at
Districts of Sheikhupura,
Faisalabad and Layyah.
Based on the analysis, it is
suggested that this area of
data quality needs to be
addressed in a benefitting
manner.
2.2(b) DHIS Data Quality Parameters
i. Usage of innovative Lot Quality Assurance Sampling Method An Innovative system was designed as part of DHIS development process to assess and
improve the quality of data being produced by DHIS. This technique was labeled as
LQAS (Annex-D). The findings of the survey revealed that all the surveyed districts
were using LQAS techniques for checking data quality and observing both-way
feedback and service monitoring. In the context of planning, this review highlighted
that at the district level, DHIS is not being used for strategic planning, but to sort of
District Health Plans.
100 100 10090 90
0
10
20
30
40
50
60
70
80
90
100
Use LQAS Technique Sent Feedback to Facilities
Receive Feedback from Provincial DHIS
Cell
Use Data for Services Monitoring
Use Data for Health Planning
Per
cen
t
Status of Different DHIS Quality Data UsageUse of Different Data Quality Assessment Methods

Rapid Appraisal of District Health Information System
23
ii. Validation of DHIS Data Reported in October 2011 In order to validate the monthly reported data, survey team collected the figures for some basic
indicators for the month of October 2011, both from the health facilities and respective EDO’s
office. The comparison of the figures for both the levels showed that there is a very slight
difference of figures. Though this difference is minor however it could challenge the
credibility of both the institutions..
Validation of Data for 5-Indicators of DHIS Reports (Oct'2011)
District Figures Reported by Total # of
OPD
Total # of suspected
Malaria
Total # Family
Plg. visits
Total # of 1st ANC visits
Total # of community
meetings
Bhakkar Health Facilities 56811 539 365 1660 36
EDO Office 56811 539 365 1660 36
D G Khan Health Facilities 65894 1147 1163 2619 36
EDO Office 65894 1147 1163 2619 36
Faisalabad Health Facilities 128771 277 1618 2767 35
EDO Office 128774 277 1617 2749 34
Jhelum Health Facilities 48863 622 593 1480 133
EDO Office 48846 307 593 1479 132
Layyah Health Facilities 52552 842 506 1212 17
EDO Office 52552 842 506 1212 17
Muzaffargarh Health Facilities 109869 3977 1048 1802 37
EDO Office 109869 3977 1048 1802 37
Okara Health Facilities 14701 169 715 957 14
EDO Office 13689 155 686 907 14
Rajanpur Health Facilities 40721 2223 761 1592 64
EDO Office 51125 2223 777 1592 64
Rawalpindi Health Facilities 45397 680 916 1316 61
EDO Office 49414 690 894 1350 101
Sheikhupura Health Facilities 71180 328 747 3137 174
EDO Office 70725 328 747 3137 174
Overall 10-Districts
150-Health Facilities 634759 10790 8432 18542 607
10-EDO Offices 647699 10485 8396 18507 645

Rapid Appraisal of District Health Information System
24
90
80
60
0
10
20
30
40
50
60
70
80
90
100
Data Entry Operator EDO-Health Distt. Coordinator
Per
cen
tage
Training Need Assessment for DHIS Functioning at Districts
2.2 (c) DHIS Operational Needs i. Initial / Refresher DHIS Training
Though, DHIS relevant staff at the districts already reported to be trained on DHIS
functionality, however they need further training.
The training demands by cadre it was observed that 90% of the surveyed Data Entry
Operators need such training. Further eight EDOs were also found to be trained in DHIS.
In 60% of the surveyed District DHIS Coordinators also requested for the training.
ii. Need of Other Resources The respondents were given six options to answer their requirement related to DHIS
improvement. Since multiple responses were recorded, therefore the data analysis
concluded that 90% (9 out of 10) respondents asked for refresher training. It was
followed by system maintenance (80%), hardware and tools demanded by 60%. Half of
the districts asked for computer operators and 40% respondents requested for updated
DHIS software.
90
80
60 60
50
40
0
10
20
30
40
50
60
70
80
90
100
Refresher TrainingSystem Maintenance Hardware DHIS Instruments / ToolsComputer operatorSoftware
Per
cen
t
Status DHIS Resources Needed by Districts

Rapid Appraisal of District Health Information System
25
3. Conclusions
The District Health Information System (DHIS) has been designed for collecting and reporting
information so that the Managers of health institutions can manage, plan, monitor and evaluate
the operations and performance of the health facilities and disease patterns in their respective
districts.
This study has demonstrated various encouraging findings. The findings suggest that efforts
made by the Provincial and District HIS stakeholders have now bore fruit and DHIS have
become truly functional in selected districts, which is a much commendable effort. However
certain deficiencies have become evident from this survey this included lack of capacity of the
data relating health personnel and non use of information for evidence based decision making
especially for planning and management of health services.
Results show that there is still a need for refresher training. Staff are facing difficulties in
filling various sections of the monthly reporting forms especially section-II which is of prime
importance in assessing the performance indicators of the respective health facilities.
Therefore thus a need for the enhancement of the capacity of healthcare providers especially
related to data collection, its entry and particularly as the data analysis. In this regard a
refresher training of all the healthcare providers including incharge of the facilities becomes
imperative.
It was encouraging to note that the reporting regularity of most of the health facilities was in
optimal state Data accuracy remained with acceptable limits.
This study suggested specific training for the healthcare providers with emphasis on use of
information and evidence based decision making. Prime aim of DHIS is not the gain of data or
information but to improve health conditions based on data.
The current situation of DHIS as evident from the results of this study demands that the
decision makers has to take initiative for further collaborations among various vertical health
programmes. For this an integrated approach be adopted which will not only save the
resources but also improve the efficiency of the District Health Information System in totality.
There is need to enhance the use of information at the facility level by improving capacity of
the Health Managers and health providers.
On the basis of the results of this report signify that training and system strengthening
strategies for improving performance are continuous processes and need regular attention of
health care managers.

Rapid Appraisal of District Health Information System
26
4. Recommendations
To improve the quality of Services and optimizing utilization of resources, the District
Health Managers, Medical Officers / In-charge of the Health Facilities need to be
encouraged to use information generated through DHIS. For this purpose quarterly
meetings / Supervisory visits and discussions among information generators and users
are mandatory.
To realize the real use of information special efforts are required to establish a regular
feedback mechanism between health facilities and District DHIS Cell.
Basic training to the new staff, not previously exposed to the DHIS or refresher
training is to be ensured training.
There is a need for building capacity of DHIS Focal persons and Statistical Officers in
data analysis and use of information.
There is continuous need for improvement of DHIS Software specially for making this
user friendly.
Need for regular estimate/ forecasting and availability of DHIS Printed supplies at
district and facility levels.
Need for reasonable budgetary allocation to maintain the system in working
conditions.
Filling of the vacant posts of technical staff by posting / recruitment in the district is
required on priority basis.
Establishment of online DHIS reporting system at Health facility level needs to be
implemented in future for rapid data transmission.
A need was that such assessment study should become a regular feature of DHIS
implementation in districts in order to improve efficiency of health information system.

Rapid Appraisal of District Health Information System
27
Annexures

Rapid Appraisal of District Health Information System
28
Selected Districts
Number of Total Health Facilities Visited
Annexure-A
District DHQ THQ RHC BHU MCH GD/CD Total
Bhakkar 1 1 3 5 2 3 15
D G Khan 1 1 3 4 3 3 15
Faisalabad 1 1 3 4 3 3 15
Jhelum 1 1 3 4 3 3 15
Layyah 1 1 3 5 2 3 15
Muzaffargarh 1 1 3 4 3 3 15
Okara 1 1 3 4 3 3 15
Rajanpur 1 1 3 8 1 1 15
Rawalpindi 0 2 3 4 3 3 15
Sheikhupura 1 1 3 4 3 3 15
Total 9 11 30 46 26 28 150

Rapid Appraisal of District Health Information System
29
List of Offices/Facilities Visited District Sr # Name of Office/Facility District Sr # Name of Office/Facility
Raw
alp
ind
i 1. EDO-Health, Rawalpindi
Jh
elu
m
1. EDO-Health, Jhelum
2. THQ Hospital Gujjar KHan 2. DHQ Hospital Jhelum
3. THQ Hospital Taxila 3. THQ Hospital Jhelum
4. MCH 1 Gujjar Khan 4. MCH Kehwra
5. MCH Dhab Ali Asbar 5. MCH Kala Gujran
6. MCH S. Town 6. MCH Shandar Chowk
7. GRD Walayatabad 7. GRD Rathian
8. GRD Shakrial 8. GRD Khurd
9. GRD Sorasi 9. GRD Lahri
10. RHC Khayabane Sir Syed 10. RHC Domaili
11. RHC Mandra 11. RHC Dina
12. RHC Kotli Satiyan 12. RHC Jalalpur Sharif
13. BHU Devi 13. BHU Dherila Jalip
14. BHU Jatli 14. BHU Sohan
15. BHU Salargah 15. BHU Banth
16. BHU Bijincal 16. BHU Kala Gujran
Sh
eik
hu
pu
ra
1. EDO-Health, Sheikhupura
Fais
ala
bad
1. EDO-Health, Faisalabad
2. DHQ Hospital Sheikhupura 2. DHQ HJospital Faisalabad
3. THQ Hospital Mureedke 3. THQ Hospital Samundary
4. MCH Centre 1 4. MCH Ravi Mohallah
5. MCH Fish Form 5. MCH Khalidabad
6. MCH Khokhar Town 6. MCH 224/RB
7. GRD Khanpur 7. CD 76/GB
8. GRD Burj Attari 8. CD 72/GB
9. GRD Ferozwala 9. CD 248/RB
10. RHC Kharianwala 10. RHC Satyana
11. RHC Jandial Sher Khan 11. RHC 65/GB
12. RHC Sharqpur Sharif 12. RHC 229/GB
13. BHU Ranikey 13. BHU 267/RB
14. BHU Chapka Minara 14. BHU 468/GB
15. BHU Bhiki 15. BHU 474/GB
16. BHU Nabi pur 16. BHU 198/GB
Ok
ara
1. EDO-Health, Okara
Layyah
1. EDO-Health, Layyah
2. DHQ Hospital Okara 2. DHQ Hospital Layyah
3. THQ Hospital Depalpur 3. THQ Hospital Karor
4. MCH Mucipal 4. MCH Layyah
5. MCH Okara 5. MCH Choubara
6. MCH ShairghaR 6. BHU 366
7. GRD 18 7. GRD 150
8. GRD 34 8. GRD 98 ml
9. GRD-39/3R 9. GRD Sumra thal
10. RHC Wasawala 10. RHC Fateh pur
11. RHC Shah Bor 11. RHC Jaman
12. RHC Renala Khurd 12. RHC Azam Chowk
13. BHU Fazal Shah 13. BHU 157 TDa
14. BHU Bhoman Shah 14. BHU 151- TDA
15. BHU 4/42 15. BHU Sammarpur
16. BHU 23/2L 16. BHU 306 TDA
Annexure-B

Rapid Appraisal of District Health Information System
30
Bh
ak
ka
r
1. EDO-Health, Bhakkar
Mu
zaff
arg
arh
1. EDO-Health, Muzaffargarh
2. DHQ Hospital Bhakkar 2. DHQ Hospital Muzaffargarh
3. THQ Hospital Kalarkot 3. THQ Hospital Kot Addu
4. MCH Kalorkot 4. MCH Kot Addu
5. MCH Bhakkar 5. MCH Muzaffargarh
6. BHU Saeed wala 6. MCH Ali Pur
7. GRD 7. CD TMA
8. GD 42 TDA 8. CD Darbar Muhammad Musa
9. GRD City 9. CD Binda Ishaq
10. RHC Behal 10. RHC Sinwan
11. RHC Jandawala 11. RHC Khan Garh
12. RHC Dewala 12. RHC Shabir Sultan
13. BHU Dagger 13. BHU Khanpur
14. BHU 67 ml 14. BHU Jadaywala
15. BHU Kohawar Kalam 15. BHU Mariain
16. BHU Kotta Jam 16. BHU Dani
Der
a G
ha
zi K
ha
n
1. EDO-Health, Dera Ghazi Khan
Raja
np
ur
1. EDO-Health, Rajanpur
2. DHQ Hospital D G Khan 2. DHQ Hospital Rajanpur
3. THQ Hospital Taunsa 3. THQ Hospital Jam Pur
4. RHC Tibbi Qaisrani 4. MCH Jam Pur
5. RHC Shah Sadar Dir 5. BHU Jahan Pur
6. RHC Chotti Zarin 6. BHU Kota Subzal
7. CD Gagan Thal 7. BHU Kot Lafasan
8. CD Jinnah Colony 8. BHU Murghat
9. GRD Drehama 9. CD Khal Chas
10. MCH 3 10. RHC Mithan Kot
11. MCH Taunsa 11. RHC Fazal Pur
12. MCH 1 12. RHC Muhammad Pur
13. BHU Haghi Ghazi 13. BHU Wang
14. BHU Nutkani 14. BHU Kotla Nasir
15. BHU Ghausabad 15. BHU Noor Pur
16. BHU Hairo Sharqi 16. BHU Tabbi Londan

Rapid Appraisal of District Health Information System
31
List of DHIS Data Instruments
DHIS – 01 (R) Central Registration Point Register
DHIS – 02 (F) OPD Ticket
DHIS – 02-A (F) Medicine Requisition Slip
DHIS – 03 (R) Outpatient Department Register
DHIS – 04 (F) OPD Abstract Form
DHIS – 05 (R) Laboratory Register
DHIS – 06 (R) Radiology/Ultrasonography/CT Scan/ECG Register
DHIS – 07 (R) Indoor Patient Register
DHIS – 08 (F) Indoor Abstract Form
DHIS – 09 (R) Daily Bed Statement Register
DHIS – 10 (R) Operation Theater (OT) Register
DHIS – 11 (R) Family Planning Register
DHIS – 12 (C) Family Planning Card
DHIS – 13 (R) Maternal Health Register
DHIS – 14 (C) Antenatal Card
DHIS – 15 (R) Obstetric Register
DHIS – 16 (R) Daily Medicine Expense Register
DHIS – 17 (R) Stock Register (Medicine/Supplies)
DHIS – 18 (R) Stock Register (Equipment/Furniture/Linen)
DHIS – 19 (R) Community Meeting Register
DHIS – 20 (R) Facility Staff Meeting Register
DHIS – 21 (MR) PHC Facility Monthly Report Form
DHIS – 22 (MR) Secondary Facility Report Form
DHIS – 23 (MR) Tertiary Hospital Monthly Report Form
DHIS – 24 (YR) Catchment Area Population Chart
DHIS – 25 (YR) Health Institute Database (HID) Report Form
DHIS – 26 (M) Training Manual for Trainers for DHIS
DHIS – 27 (M) Participants Manual for DHIS
DHIS – 28 (M) Procedures Manual for DHIS
DHIS – 29 (M) DHIS Software User’s Manual
Annexure-C
Rapid Appraisal of District Health Information System
32
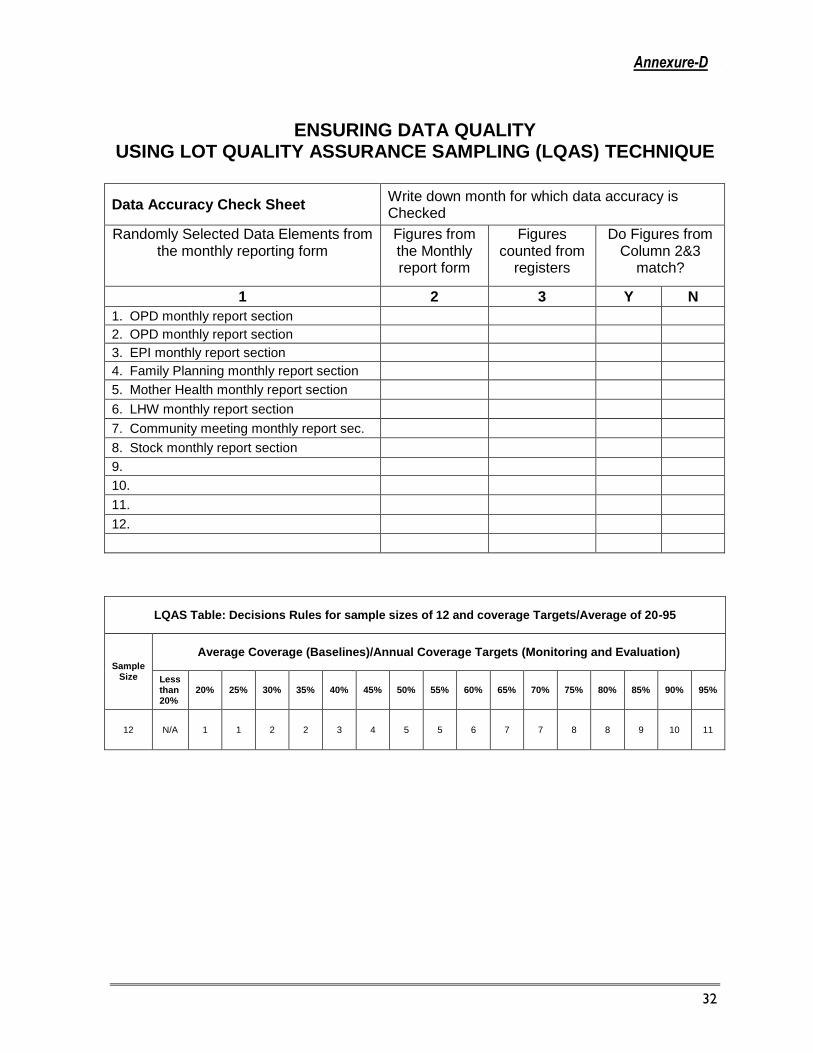
ENSURING DATA QUALITY USING LOT QUALITY ASSURANCE SAMPLING (LQAS) TECHNIQUE
Data Accuracy Check Sheet Write down month for which data accuracy is Checked
Randomly Selected Data Elements from the monthly reporting form
Figures from the Monthly report form
Figures counted from
registers
Do Figures from Column 2&3
match?
1 2 3 Y N
1. OPD monthly report section
2. OPD monthly report section
3. EPI monthly report section
4. Family Planning monthly report section
5. Mother Health monthly report section
6. LHW monthly report section
7. Community meeting monthly report sec.
8. Stock monthly report section
9.
10.
11.
12.
LQAS Table: Decisions Rules for sample sizes of 12 and coverage Targets/Average of 20-95
Sample Size
Average Coverage (Baselines)/Annual Coverage Targets (Monitoring and Evaluation)
Less than 20%
20% 25% 30% 35% 40% 45% 50% 55% 60% 65% 70% 75% 80% 85% 90% 95%
12 N/A 1 1 2 2 3 4 5 5 6 7 7 8 8 9 10 11
Annexure-D

Rapid Appraisal of District Health Information System
33
Study Supervision and Team
Study Team
Dr. Farooq Azam Jan, Team Leader/ DHIS Review Study
Mr. Khalid Hussain Shah, HIS Consultant/Member Review Team
Mr. Asad Afzal Hamayoun, HIS Consultant/Member Review Team
WHO Technical Supervision
Ms. Fatma Giha, Information Management Coordinator
Dr. S.M. Mursalin, Technical Officer, HIS
Mr. Imran Majeed Malik, Data Management Supervisor, / Study Design
Mr. Zeeshan Abbas, Data Analysis support
Punjab Health Department
Dr. Muhammad Anwar Janjua, Director MIS
Mr. Farooq Ahmed, Data Management Officer, MIS Cell
District Health Office
Ch. Ali Ahsan, District Focal Person, Rawalpindi
Dr. Roadab Irfan, District Focal Person, Jhelum
Miss Noor Fatima, District Focal Person, Sheikhupura
Ms. Sajida Tufail, District Focal Person, Okara
Mr. Ijaz Hussain, District Focal Person, Faisalabad
Mr. Muzamil Mubeen, District Focal Person, Layyah
Mr. Javed Aziz, District Focal Person, Bhakkar
Mr. Saleemullah, District Focal Person, Dera Ghazi Khan
Ms. Tahira Saleem, District Focal Person, Muzaffargarh
Mr. Tahir Mehmood, District Focal Person, Rajanpur
Annexure-E

Rapid Appraisal of District Health Information System
34
TIMELINE OF ACTIVITIES / WORKPLAN (October – January, 2011)
Activities October November December January
Wk-1
Wk-2
Wk-3
Wk-4
Wk-5
Wk-6
Wk-7
Wk-8
Wk-9
Wk-10
Wk-11
Wk-12
Wk-13
Wk-14
Wk-15
Wk-16
Technical Coordination
Team Formation
Development of working paper / technical material
Consultative Meeting for Questionnaire (development & finalization)
Logistic Arrangements
Preparatory & Coordination Meeting
Field Activity
Data Collection, Synchronization, and Entry
Analysis and report development
Report Review
Finalization of Report & Dissemination
Dissemination of Results
Annexure-F

Rapid Appraisal of District Health Information System
35
REVIEW OF DISTRICT HEALTH INFORMATION SYSTEM
(In selected districts of Punjab)
(District Managerial Level Questionnaire)
District: ________________________ Date of Visit ___________________ Respondent Name: ________________________ Designation. (1) EDO, (2) Dist. Coord.
PART-I DHIS INFRASTRUCTURE & FUNCTIONING
1. Is DHIS implemented at your district? Yes No
1.1 If YES, then tell since when (Year) it was implemented.
1.2 Does DHIS Cell exists in EDO Office (Please observe) Yes No
1.3 Is your DHIS Cell affected by flood (2010-2011) Yes No
1.4 If YES, does it re-habilitated after flood. Yes No
2. What is your monthly (Oct’11) DHIS reporting compliance to your Prov. DHIS Cell? 1: (81% - 100%), 2: 71% -80%), 3: 51%-70%), 4: (50% or Less than 50%)
1 2 3 4
3. Are DHIS Instruments (Registers) available (As per Requirement)? Yes No
3.1 If YES, for how much Period
4. What is the Funding Source of DHIS Functioning?
5. Is a separate Hardware Computer available for DHIS? Yes No
6. Corresponding Functioning of DHIS Software Available Yes No
7. Are the Human Resources Trained on DHIS functioning?
7.1 EDO Yes No
7.2 Dist Coordinator (DHIS) Yes No
7.3 DHIS Computer Operator Yes No
8. Is there a defined DHIS specific Terms of Reference / Roles & Responsibility of each level (EDO, Distt. Coord. Health Facility Staff).
Yes No
8.1 If YES, Please provide a copy. (Please get copy, if possible) Available Not Available
9. What is the data accuracy of your field units? 1: (81% - 100%), 2: 71% -80%), 3: 51%-70%), 4: (50% or Less than 50%)
1 2 3 4
10. When did you sent your past-month (Oct’11) DHIS data (electronically) to the Provincial DHIS Cell? (1) As Per Schedule - 15
th of the Month, (2) Not as per schedule
1 2
10.1 Verify from system (email etc) when the last report (Oct’11) was sent. As per schedule Not as per schedule
Annexure-G

Rapid Appraisal of District Health Information System
36
-2-
PART-II DHIS DATA QUALITY
1. Do you have DHIS Procedural Manual in your office? Yes No
2. Is your DHIS data entry operator fully understands the DHIS reporting Forms?
Yes No
3. Do you check the data quality of your field units through LQAS? Yes No
4. Do you send the data feedback to your health facilities? Yes No
5. Do you receive regular feedback from your Prov. DHIS Cell? Yes No
6. Do you analyze the monthly DHIS data for service monitoring? Yes No
7. Do you use the DHIS data for your district health planning? Yes No
7.1 If YES, Please explain.
8. Please get data of following indicators by Health Facilities (For Oct’2011) from respective DHIS Cell of the district.
Name of Health Facilities (only selected for survey) Total # of OPD
Total # of suspected
Malaria
Total # Family
Planning visits
Total # of 1st ANC visits
Total # of community
meetings
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
PS. Cross check with concerned facility monthly report of the same month (as per Facility Level Questionnaire).

Rapid Appraisal of District Health Information System
37
-3-
PART-III DHIS SUPPLY/OTHER NEEDS
1. Is your Human Resource need any DHIS training?
1.1 EDO Yes No
1.2 Dist Coordinator (DHIS) Yes No
1.3 DHIS Computer Operator Yes No
2. Is the supply of DHIS Data Collection Tools (Registers) needs to be replenished? (Normally supply of Tools issued for 2-months)
Yes No
2.1 If YES, then tell what kind of replenishment. (1-In advance 6 month, 2-Whole year stock)
1 2
3. Do you need relevant resources (if not available) to run DHIS?
3.1 DHIS Computer Operator Yes No
3.2 Hardware Yes No
3.3 Software Yes No
3.4 System Maintenance Yes No
3.5 DHIS Instruments / Tools Yes No
3.6 DHIS Refresher Trainings Yes No
Name of Data Collector: _________________________________

Rapid Appraisal of District Health Information System
38
REVIEW OF DISTRICT HEALTH INFORMATION SYSTEM (In selected districts of Punjab)
(Facility Level Questionnaire)
Name of Facility ______________________________ Facility’s ID ___________________Type: ______________________
Union Council _________________________ Tehsil __________________________ District __________________________
R/Name (Preferably Facility In-Charge) ________________________________ Designation: __________________
Health Facility Affected by Flood 2010-11 (Yes / No), if YES Does it Re-habilitated (Yes / No)
PART-I DHIS FUNCTIONING
1. What is your length of service in the Health Department? (1) Less than 1 year (2) 1-5 Year (3) 6-10 Year (4) More than 10 Year
1 2 3 4
2. Since how long you are working at this Facility? (1) Less than 1 year (2) 1-5 Year (3) 6-10 Year (4) More than 10 Year
1 2 3 4
3. Since how long you have been assigned DHIS Functioning/Reporting? (1) Less than 1-Year (2) 1-3 Year (3) More than 3-Year
1 2 3
4. Are you trained on DHIS Data Collection Instruments (Registers)? Y N
4.1 If YES, then tell the source (Agency) from where you got the training?
5. Who fill the DHIS Monthly Reporting Form (Designation)?
5.1 Is above staff/person trained for this task? Y N
6. Are the following data resources (Tools) available for monthly DHIS recording & reporting?
6.1 1. Monthly DHIS Reporting Forms Y N
2. OPD tickets Y N
3. Abstract register Y N
4. Laboratory register Y N
5. Mother Health Y N
6. Child Health Y N
7. Catchment Area Population chart Y N
8. Stock register Y N
9. Family Planning Register Y N
10. Meeting & Yearly attendances register. Y N
6.2 Are the Registers updated on daily basis? (see any one of the register for validation) Y N
Annexure-H

Rapid Appraisal of District Health Information System
39
PART-II DHIS DATA QUALITY
1. Do you have DHIS Procedural Manual at your facility? Y N
2. Do you have defined DHIS related Roles & Responsibility of each staff? Y N
3. Do you fully understand the DHIS reporting Forms? Y N
3.1 If NO, then which section you feel difficult to understand. (write Form Sec. #)
4. Do you know when the monthly DHIS reporting Form should be sent to EDO office? (1) Within 7-Days (2) Within 15-Days (3) Within 30-Days
1 2 3
5. From where you get the data to fill DHIS reporting Forms?
6. Do you submit monthly DHIS Forms to your EDO-H regularly? Y N
6.1 If NO, State the reason
7. When did you submit your monthly DHIS report to your EDO-H? (1) 5th of each month (2) 15th of each month (3) After 30-days.
1 2 3
8. Do you remember how many monthly reports were not submitted by your facility to EDO-H during last 12-Months? (State in numbers)
8.1 If YES, State the reason
9. Do you receive any feedback of your monthly report? Y N
9.1 If YES, then state the kind of feedback.
10. Which section of the DHIS reporting form you often analyze (I - XVII)?
11. Is your facility using the DHIS data for planning? Y N
11.1 If YES, what kind of planning you usually do?
12. Have you faced any shortage of DHIS Tools (Registers) at your facility during 2011?
Y N
12.1 If YES, then state the shortage in months.
(1) 1-Month (2) 2-Months (3) 3-Months or more 1 2 3
13. Do you keep the copy of monthly DHIS reported forms for your record? Y N
13.1 If YES, then check the final figures of past-month (Oct-11) of following indicators from their copy. (If NOT then see their Registers).
1. Total # of OPD
2. Total # of Suspected Malaria
3. Total # Family Planning visits
4. Total # of 1st ANC visits 5. Total # of community meetings

Rapid Appraisal of District Health Information System
40
PART-III DHIS SUPPLY/OTHER NEEDS
1. Do you need any training of DHIS on reporting mechanism? Y N
1.1. If YES, then tell kind of training.
(1) Form filling (2) LQAS check (3) Indicators’ analysis etc. 1 2 3
2. Is the supply of DHIS Tools (Registers) needs to be replenished? Y N
2.1 If YES, then tell what kind of replenishment.
(1) In advance 6 month (2) Whole year stock 1 2
3. Do you need relevant resources (if not available) for DHIS functioning? Y N
3.1
If YES, state the kind of resource (Could be Multiple Responses)
i) HR Y N
ii) Tools Y N
iii) Others (Elaborate others, if YES for data entry purpose e.g. write below the response in your own words)
Y N

Rapid Appraisal of District Health Information System
41
Table # 1: Respondents by Type of Facility
Designation DHQ THQ MCH GRD RHC BHU Total
DOH 0 0 1 0 0 0 1
Dispenser 1 0 1 18 1 5 26
LHV 0 0 23 1 0 0 24
Medical Officer 0 2 1 8 5 27 43
Medical Supdtt. 5 9 0 0 0 0 14
Medical Technician 1 0 4 2 0 5 12
Pharmacist 1 0 0 0 0 0 1
Sr. Medical Officer 0 0 0 0 23 1 24
Statistical Officer 1 0 0 0 0 0 1
Woman Medical Officer 0 0 0 1 1 2 4
Total 10-Districts 9 11 30 30 30 40 150
Table # 3: Status of Tools Availability &Their Daily Update at selected Facilities.
District Tools Availability (%age) Daily Update (%age)
Muzaffargarh 97 97
Jhelum 86 80
Bhakkar 84 84
D G Khan 83 50
Rajanpur 83 72
Faisalabad 82 82
Layyah 82 82
Okara 77 77
Rawalpindi 73 68
Sheikhupura 71 62
Overall 10-Districts 82 75
Table # 2: Status of Facility Incharges Trained on DHIS
District Trained Not Trained Total Facility
Visited # of Facility % # of Facility %
Bhakkar 15 100 0 0 15
D G Khan 15 100 0 0 15
Faisalabad 8 53 7 47 15
Jhelum 15 100 0 0 15
Layyah 13 87 2 13 15
Muzaffargarh 15 100 0 0 15
Okara 15 100 0 0 15
Rajanpur 12 80 3 20 15
Rawalpindi 12 80 3 20 15
Sheikhupura 13 87 2 13 15
Overall 10-Districts 133 89 17 11 150
Annexure-I

Rapid Appraisal of District Health Information System
42
Table # 4: Status of Availability of DHIS Manual and TORs of Staff
District Manual Available
(# of Facility) %
TORs Available (# of Facility)
%
Bhakkar 11 73 14 93
D G Khan 14 93 2 13
Faisalabad 11 73 10 67
Jhelum 13 87 2 13
Layyah 9 60 15 100
Muzaffargarh 15 100 15 100
Okara 11 73 0 0
Rajanpur 10 67 8 53
Rawalpindi 9 60 7 47
Sheikhupura 4 27 4 27
Overall 10-Districts 107 71 77 51
Table # 5: Respondents Understanding of DHIS Forms vs Sections Difficult to Understand
District Understand
(# Respondents) Not Understand (# Respondents)
Forms Section Difficult to Understand
Section-II Section-III Section-VIII
Bhakkar 15 0 - - -
D G Khan 15 0 - - -
Faisalabad 14 1 - - 1
Jhelum 15 0 - - -
Layyah 15 0 - - -
Muzaffargarh 15 0 - - -
Okara 15 0 - - -
Rajanpur 8 7 7 - -
Rawalpindi 11 4 3 1 -
Sheikhupura 13 2 1 1 -
Overall 10-Districts 136 14 11 2 1
Table # 6: Status of Knowledge and Practice regarding Monthly DHIS Report Submission
District
Knowledge Practice Within 7-days
Within 15-days
Within 30-days Total
5th of Month
15th of Month
After 30 Days Total
N N N N N N
Bhakkar 15 0 0 15 14 1 0 15
D G Khan 14 1 0 15 15 0 0 15
Faisalabad 15 0 0 15 14 1 0 15
Jhelum 15 0 0 15 15 0 0 15
Layyah 15 0 0 15 14 1 0 15
Muzaffargarh 14 0 1 15 15 0 0 15
Okara 15 0 0 15 15 0 0 15
Rajanpur 15 0 0 15 15 0 0 15
Rawalpindi 11 0 4 15 12 0 3 15
Sheikhupura 14 1 0 15 14 1 0 15
Overall 10-Districts 143 2 5 150 143 4 3 150

Rapid Appraisal of District Health Information System
43
Table # 7: Status of Health Facilities Received Feedback from their EDO-Health
District Yes No
Total N % N %
Bhakkar 10 67 5 33 15
D G Khan 15 100 0 0 15
Faisalabad 4 27 11 73 15
Jhelum 14 93 1 7 15
Layyah 11 73 4 27 15
Muzaffargarh 9 60 6 40 15
Okara 15 100 0 0 15
Rajanpur 5 33 10 67 15
Rawalpindi 12 80 3 20 15
Sheikhupura 13 87 2 13 15
Overall 10-Districts 108 72 42 28 150
Table # 8: Status of Issues and Type of Feedback Received from their EDO-Health
District To discuss
target/ performance
Admin & Managerial
Issue
Ask for correction in
the forms
Stock & Medicine
Total
Bhakkar 7 2 1 0 10
D G Khan 9 6 0 0 15
Faisalabad 3 0 1 0 4
Jhelum 8 6 0 0 14
Layyah 6 3 2 0 11
Muzaffargarh 6 3 0 0 9
Okara 5 0 10 0 15
Rajanpur 3 0 1 1 5
Rawalpindi 8 4 0 0 12
Sheikhupura 11 2 0 0 13
Overall 10-Districts 66 26 15 1 108
Table # 9: Is your facility using the DHIS Data for Planning
District Yes No
Total N % N %
Bhakkar 10 67 5 33 15
D G Khan 0 0 15 100 15
Faisalabad 5 33 10 67 15
Jhelum 15 100 0 0 15
Layyah 9 60 6 40 15
Muzaffargarh 15 100 0 0 15
Okara 7 47 8 53 15
Rajanpur 2 13 13 87 15
Rawalpindi 7 47 8 53 15
Sheikhupura 12 80 3 20 15
Overall 10-Districts 82 55 68 45 150

Rapid Appraisal of District Health Information System
44
Table # 10: Status of Shortage of DHIS Tools at Health Facilities
District
Yes No
Total N % N %
Bhakkar 2 13 13 87 15
D G Khan 0 0 15 100 15
Faisalabad 1 7 14 93 15
Jhelum 6 40 9 60 15
Layyah 1 7 14 93 15
Muzaffargarh 3 20 12 80 15
Okara 2 13 13 87 15
Rajanpur 5 33 10 67 15
Rawalpindi 0 0 15 100 15
Sheikhupura 7 47 8 53 15
Overall 10-Districts 27 18 123 82 150
Table # 11: Status of Shortage of DHIS Tools at Facilities
District Facilities Surveyed
Facilities Facing Shortage of Tools
Shortage in Months
N % 1-Month % 3-Month %
Bhakkar 15 2 13 1 7 1 7
D G Khan 15 0 0 0 0
Faisalabad 15 1 7 1 7 0 0
Jhelum 15 6 40 4 27 2 13
Layyah 15 1 7 0 0 1 7
Muzaffargarh 15 3 20 0 0 3 20
Okara 15 2 13 0 0 2 13
Rajanpur 15 5 33 1 7 4 27
Rawalpindi 15 0 0 0 0
Sheikhupura 15 7 47 0 0 7 47
Overall 10-Districts 150 27 18 7 5 20 13

Rapid Appraisal of District Health Information System
45
Table # 12: Facilities Keep Record of the Monthly DHIS Reports
District Yes No
Total N % N
%
Bhakkar 15 100 0 0 15
D G Khan 15 100 0 0 15
Faisalabad 11 73 4 27 15
Jhelum 15 100 0 0 15
Layyah 15 100 0 0 15
Muzaffargarh 15 100 0 0 15
Okara 15 100 0 0 15
Rajanpur 15 100 0 0 15
Rawalpindi 15 100 0 0 15
Sheikhupura 15 100 0 0 15
Overall 10-Districts 146 97 4 3 150
Table # 13: Facility's Incharges Need Trainings vs Kinds of Trainings they Needed
District Total
Facilities Visited
Facility's Incharges Need Training
Kinds of Training Needed
N % Forms Filling
% LQAS Check
% Indicators'
Analysis %
Bhakkar 15 14 93 3 20 2 13 9 60
D G Khan 15 15 100 0 0 0 0 15 100
Faisalabad 15 14 93 6 40 2 13 6 40
Jhelum 15 11 73 2 13 1 7 8 53
Layyah 15 15 100 1 7 0 0 14 93
Muzaffargarh 15 15 100 0 0 0 0 15 100
Okara 15 8 53 1 7 5 33 2 13
Rajanpur 15 15 100 0 0 2 13 13 87
Rawalpindi 15 9 60 0 0 4 27 5 33
Sheikhupura 15 12 80 0 0 2 13 10 67 Overall 10-
Districts 150 128 85 13 9 18 12 97 65

Rapid Appraisal of District Health Information System
46
Table # 14: Status of DHIS Tools Supply Replenishment
District Total
Facilities Visited
Facilities Need Replenishment
Kinds of Replenishment
N % 6-Months Advance Supply
% Whole Year
Supply %
Bhakkar 15 7 47 1 7 6 6
D G Khan 15 15 100 0 0 15 15
Faisalabad 15 1 7 0 0 1 1
Jhelum 15 4 27 3 20 1 1
Layyah 15 11 73 10 67 1 1
Muzaffargarh 15 14 93 2 13 12 12
Okara 15 15 100 3 20 12 12
Rajanpur 15 14 93 13 87 1 1
Rawalpindi 15 4 27 2 13 2 1
Sheikhupura 15 15 100 7 47 8 8
Total 150 100 67 41 27 59 39
Table # 15: Status of DHIS Relevant Resources Facilities Needed
District # of Facilities
Visited
# Facilities Needed Resources
Kinds of Resources Needed
HR Tools Other
N % N % N % N %
Bhakkar 15 7 47 5 33 5 33 1 7
D G Khan 15 15 100 5 33 15 100 0 0
Faisalabad 15 7 47 7 47 2 13 2 13
Jhelum 15 8 53 7 47 2 13 8 53
Layyah 15 5 33 4 27 3 20 0 0
Muzaffargarh 15 15 100 12 80 15 100 0 0
Okara 15 2 13 2 13 2 13 0 0
Rajanpur 15 11 73 10 67 9 60 8 53
Rawalpindi 15 9 60 8 53 1 7 6 40
Sheikhupura 15 9 60 4 27 7 47 10 67
Total 150 88 59 64 43 61 41 35 23

Rapid Appraisal of District Health Information System
47
Annexure-J

Rapid Appraisal of District Health Information System
48

Rapid Appraisal of District Health Information System
49

Rapid Appraisal of District Health Information System
50

Rapid Appraisal of District Health Information System
51
Annexure-K

Rapid Appraisal of District Health Information System
52

Rapid Appraisal of District Health Information System
53

Rapid Appraisal of District Health Information System
54

Rapid Appraisal of District Health Information System
55