Radiological Errors- What? Why? How? When?Audit Aims •Provide a robust, sustainable and useful...
67
Radiological Errors- What? Why? How? When? Pamela Parker Lead Sonographer
Transcript of Radiological Errors- What? Why? How? When?Audit Aims •Provide a robust, sustainable and useful...
-
Radiological Errors-
What? Why? How? When?
Pamela Parker
Lead Sonographer
-
The greatest of
faults, I should
say, is to be
conscious of
none
Thomas Carlyle philosopher,
satirical writer, essayist, historian
and teacher.
Born: 4 December 1795,
Died: 5 February 1881
-
Clinical Govenance
"Clinical governance is a system through
which NHS organisations are accountable
for continuously improving the quality of
their services and safeguarding high
standards of care by creating an
environment in which excellence in clinical
care will flourish."
(Scally and Donaldson 1998, p.61)
-
Main Components of Clinical
Governance
• Identifying what can and does go wrong
during care
• Understanding the factors that influence
this
• Learning lessons from any adverse events
• Ensuring action is taken to prevent
recurrence
• Putting systems in place to reduce risks
-
Main Components of Clinical
Governance • Clinical audit
• Education, training and continuing
professional development
• Evidence-based care and effectiveness
• Patient and carer experience and
involvement
• Staffing and staff management
-
Patient and carer experience and
involvement
• Complaint, incident and compliment
analysis
• Patient satisfaction surveys
– Staff
– Service
• Patient Information Leaflet Review
-
And why do you
look at the
speck in your
brother's eye,
but do not
consider the
plank in your
own eye?
Matthew 7:3
-
Incident Review
-
What’s gone wrong?
Apr-13 May-13 Jun-13 Jul-13 Aug-13 Sep-13 Oct-13 Nov-13
DATIX
NT Data 2 4 4 1 1 2
Reports 2 2
Patient Incidents
(Falls etc) 1 1
Staff Incidents (Falls
etc) 1
Referral Issues 1
Needle Stick 1
-
Understanding the influencing
factors
-
Understanding the influencing
factors
-
Patient Complaints
-
What’s gone wrong? PALS Apr-13 May-13 Jun-13 Jul-13 Aug-13 Sep-13 Oct-13
Rushed scan. (Obs) 1 2
Sonog attitude (Obs) 2 2 1 1
Waiting list (MSK) 1 1
Sonog attitude (MSK) 1 2
Sonog attitude (A&E) 1
Pt perception MSK
Pt perception TRUS
Sonog attitude (Gen) 1
PALS Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15
Rushed scan, poor
communication 1
Unhappy with Souvenir
Scans 2 1
Sonographer attitude 1
Pt wanted cons scan 1
Pt scanned as IP an
OP not required. Pt
states was not
informed 1
Post surgical FB
reported - surgeon
disagrees 1
-
Staff focus
• Patient Satisfaction surveys
– How good was your sonographer today at
each of the following?
Listening to you
Explaining the
procedure
Explaining how to
get your results
Explaining when to
get your results
Being Polite
Making you feel at
ease
-
What’s gone right?
-
What’s gone right?
Very professional, felt really relaxed
The sonographer is great, She put me at ease
Please add any other comment you want to make about this sonographer.
Brilliant, helpful and happy people
Procedure quick, polite and efficient
Sonographer was very polite, thank you
Very polite and easy to understand.
Made me feel so at ease. Relaxing voice and was very efficient and professional.
Very relaxed experience
The sonographer was exceptionally clean and tidy and very polite. She explained
everything that was going on.
top marks 10/10
I initially felt shy but put at ease with such caring staff
I liked her she was nice, thank you lovely lady
there were 3 people in the room everyone was very kind and polite
don't want to lose that
The Sonographer deserves pay rise because she knows her job well and society
-
Staff focus and multi-disciplinary
working
• Sonographer Multisource Feedback
– The purpose of this survey is to provide
sonographers with information about their
work through the eyes of those they work with
– It is intended to help inform their further
development
-
Sonographer Multisource Feedback
-
Sonographer Multisource Feedback
-
Happiness Scores!
-
Clinical Audit
• Quality Assurance vs Clinical Audit
• Clinical Examination vs Technical Issues
• Staff quality Vs Equipment Quality
-
Background
• Sonographers now undertake and report
medical ultrasound examinations in most
UK hospitals
• RCR view this as a delegated task
• Quality assurance is important
– to ensure that delegation is appropriate
– to guarantee safe and effective practices to
service users
-
Implementing Audit
• Ultrasound is renowned for its operator
dependence
• A ‘real-time’ imaging modality
• Immediate interpretation of the moving
ultrasound image
• An audit programme should be a process
of review, learning and improvement for
both the service and individuals
-
Audit Aims
• Provide a robust, sustainable and useful
audit and case review process that
identifies needs for service improvement
that will ultimately lead to better patient
care.
• Provide a process of review and learning
that contributes positively to sonographers’
continuing professional development.
-
Clinical Audit
• A robust, sustainable audit programme for
diagnostic ultrasound is hard to implement
• Time and resources are required
• Relevant to clinical practice
• No one accepted method of performing a
review of practice
– BMUS Recommended Audit Tool
-
British Medical Ultrasound Society
• The BMUS recommended peer review
audit tool
• Reproducible mechanism with which
quality factors can be measured reliably
and repeatedly.
– Image Quality
– Report Quality
– Clinical Quality
-
Recommendations for Use
• Audit is undertaken in conjunction with a
discrepancy meeting.
• A tolerance level of acceptable quality is
agreed
• Cases falling below this tolerance level
should be discussed openly within a
discrepancy meeting
• Learning points and further action agreed
-
Points to Consider
• Randomised audit sample
• Anonymity
• Reviewers
• Quality Benchmarks
• Feedback
• Learning from discrepancies
-
Score Criteria
IMAGE QUALITY (I)
3 Good Image Quality
2 Acceptable Diagnostic Quality
1 Poor Image Quality
REPORT QUALITY (R)
3 Report Content and Structure
Optimal
2 Report of Acceptable Quality
1 Poor Report Quality
CLINICAL QUALITY (C)
Yes = 1 point, No = 0 points
Clinical Referral Appropriate
Clinical Question Answered
Appropriate advice or conclusion
-
Clinical Audit – Is anything
wrong?
-
Discrepancy Reflection
Type of Discrepancy
A Observation
B Interpretation
C Poor imaging technique
D Poor Wording
Grade of discrepancy
0 No Discrepancy
1 Discrepancy with report –
no action required
2 Discrepancy with report –
report amended
3 Significant discrepancy with
report – action required
-
What’s gone wrong?
-
Education, Training and CPD
• Literature reviewed and presented at CPD
meeting : Guidelines updated
• GB imaging presentation given to support
practice
• Discussed with sonographer. Need to be
mindful of terminology used in reports
• Equipment issues identified resulted in
equipment being transferred from main
service
-
Summary – So Far
• Identifying what can and does go wrong
during care
• Understanding the factors that influence
this
• Learning lessons from any adverse events
• Ensuring action is taken to prevent
recurrence
• Putting systems in place to reduce risks
-
Learning lessons from any
adverse events • Discrepancy Meetings
• PDR’s
– Team objectives
– Team results
• Operational Group Meetings
• Staff meetings
• Incident reporting
• Incident recording
-
Gallstones – US features
Gallstones?
Gallstones?
-
Gallstones ?
YES √ No x – Gas filled duodenum
-
Duty of Candour
-
Background
• 27th November 2014 marked an historic
moment for NHS in England
• Statutory duty of candour comes into force
following two decades of campaign
• Regulation 20: Duty of Candour. Care
Quality Commission
• March 2015
-
Definition
• A legal duty to be open and honest with
patients or their families when things go
wrong that can cause harm
• Duty of Candour aims to help patients
receive accurate, truthful information from
health providers
-
Definition
• ‘Any patient harmed by the provision of a
healthcare service is informed of the fact
and an appropriate remedy offered,
regardless of whether a complaint has
been made or a question asked about it’
www.professionalstandards.org.uk
-
Why?
• 24% The percentage of NHS trusts that
regularly inform patients of safety
incidents.
• 1 Million : The estimated number of patient
safety incidents in English hospitals every
year
• 50% The percentage of patient safety
incidents that are avoidable
-
Why?
• £9 -10 billion :The potential liability of the
NHS; (based on reporting from NHS trusts
about medical accidents, deemed to be
negligence risks).
-
Development
• “Robbie’s Law”
-
Robbie’s Law
• In December 1989, Robbie Powell aged
10, of Ystradgynlais in Wales is
hospitalised for four days.
• He loses 25% of his body weight and is
critically dehydrated.
• The hospital suspects Addison’s disease
• Doctors there order an ACTH test for the
condition, but this isn’t followed through.
-
Robbie’s Law
• The test recommendation isn’t
communicated to the Powells, but is
communicated to his GPs. Instead the
Powells are told by the hospital that
Robbie suffers from gastroenteritis caused
by a throat infection
-
Robbie’s Law
• Four months later, in April 1990, Robbie
again suffers from vomiting, weight loss
and acute stomach pains.
• He is seen seven times by five doctors
over 15 days.
• None of them perform the basics: check
symptoms, do a blood test or refer to the
hospital.
-
Robbie’s Law
• Only one doctor checks the medical
records, containing the crucial warning
from the hospital.
• He dies from critical dehydration as a
result of Addison’s disease.
-
Robbie’s Law
• His death could have
been avoided, but
due to a combination
of mismanagement,
dishonesty and
deliberate cover-up,
none of the doctors
are prosecuted
http://www.robbieslawtrust.co.uk/summary/
-
Outcome
• Robbie’s Law and the Duty of Candour is
born from a seriously dire need for
openness and honesty in healthcare.
• Robbie’s Law means that healthcare staff
must tell patients and their next of kin the
truth, when a patient safety incident occurs
-
Openness
• Letter sent to the patient with apologies
given about what had happened.
• The patient came to see the treating GP
shortly after receiving the letter.
• He had been giving thought to speaking to
a solicitor about the delay in diagnosis
• On reflection he had been struck by the
openness, the apologies and the care and
support of the GP
-
Learning
• The patient felt that the most important
thing to happen was for the doctors to
learn from the incident
-
Being Open When Errors Are
Made • Open discussions between the patient and
the healthcare provider when things go
wrong.
• Acceptance by healthcare staff that open
conversations will take place at an early
stage.
• Reduction in overly defensive approaches
to information sharing about incidents in
relation to the patient in question.
-
Triggers
• The death of a patient when due to
treatment received or not received (not
just their underlying condition).
• Severe harm - in essence permanent
serious injury as a result of care provided.
• Moderate harm - in essence non
permanent serious injury or prolonged
psychological harm.
-
Moderate harm - US
• Misdiagnosis leading to unnecessary
surgery
• Misdiagnosis leading to delays in
treatment
• Therapeutic treatment delivered incorrectly
-
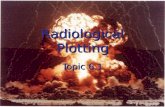
How do we deal with this?
Duty of Candour
Radiology Report Discrepancy Flowchart
-
Radiology Report Discrepancy Flowchart
Radiology review meeting held & discrepancy
identified
Level of radiological discrepancy determined at
review
Grade 0 or Grade 1
Grade 2 and 3 (no clinical
significance)
Grade 2 and 3 with reasonable likelihood of clinical significance
Decision by referrer/clinician following discussions between Radiology and the clinical team. Should the patent be informed?
Moderate (2) Major (3)
Date apology provided recorded on DATIX by member of staff who gave the apology
Written apology offered to the patient/family
Actions taken to provide patient with explanation and apology recorded on DATIX by service or specialty lead
Letter sent to [email protected] for
inclusion on DATIX
10 days
Moderate (2) Major (3)
Serious Incident / Never Event investigation
Yes or No
Error recorded in discrepancy meeting
notes DATIX closed if Grade
2 or 3
Investigation concluded
Summary of discrepancy meeting notes discussed at RMT on a quarterly basis and included in Imaging
DIG report
Letter including outcomes and learning
approved by Health Group triumvirate prior
to sending to the patient/family
Letter offering to share final report and an offer to meet with the panel to discuss
the report sent to patient/family
Letter sent to [email protected] for inclusion on DATIX
10 days
The incident investigation must be shared with the patient/family. This includes action plans, details of investigations and means actual written
reports and if necessary, plain English explanations of their contents.
Radiology Lead for the discrepancy meeting discusses with referring clinical team and informs referrer via letter of error and any remedial actions
taken (such as arranged further scans)
Written apology is provided to the patient/family
Radiology records incident on DATIX
Ultrasound to discuss discrepancy with
Radiologist before notifying referrer.
No
Yes
Not significant Significant
-
Radiology Report Discrepancy Flowchart
Radiology review meeting held & discrepancy
identified
Level of radiological discrepancy determined at
review
Grade 0 or Grade 1
Grade 2 and 3 (no clinical
significance)
Grade 2 and 3 with reasonable likelihood of clinical significance
Decision by referrer/clinician following discussions between Radiology and the clinical team. Should the patent be informed?
Moderate (2) Major (3)
Date apology provided recorded on DATIX by member of staff who gave the apology
Written apology offered to the patient/family
Actions taken to provide patient with explanation and apology recorded on DATIX by service or specialty lead
Letter sent to [email protected] for
inclusion on DATIX
10 days
Moderate (2) Major (3)
Serious Incident / Never Event investigation
Yes or No
Error recorded in discrepancy meeting
notes DATIX closed if Grade
2 or 3
Investigation concluded
Summary of discrepancy meeting notes discussed at RMT on a quarterly basis and included in Imaging
DIG report
Letter including outcomes and learning
approved by Health Group triumvirate prior
to sending to the patient/family
Letter offering to share final report and an offer to meet with the panel to discuss
the report sent to patient/family
Letter sent to [email protected] for inclusion on DATIX
10 days
The incident investigation must be shared with the patient/family. This includes action plans, details of investigations and means actual written
reports and if necessary, plain English explanations of their contents.
Radiology Lead for the discrepancy meeting discusses with referring clinical team and informs referrer via letter of error and any remedial actions
taken (such as arranged further scans)
Written apology is provided to the patient/family
Radiology records incident on DATIX
Ultrasound to discuss discrepancy with
Radiologist before notifying referrer.
No
Yes
Not significant Significant
-
Duty of Candour - In Practice
• Errors discussed and graded at
discrepancy meeting
• Where deemed to be a moderate
disagreement in the report an apology is
given via the referring clinician
• Actions recorded
-
How do we deal with this?
We acknowledge our mistakes and say sorry
-
What is an apology?
• Clinical staff may
worry that being open
with patients may
compromise the
ability to deal with a
claim if one is
subsequently made
by the patient
• In reality candour is
all about sharing
accurate information
with patients
• The facts are the
facts and staff should
be supported to help
patients understand
what has happened to
them.
-
What is an apology?
• Where staff should be
more cautious is
where the facts are
not yet know or where
they are being asked
to speculate beyond
what is known.
• It can be more
damaging to a
relationship with the
patient to speculate
inaccurately than to
investigate and find
the facts and then
provide the extra
information.
-
Apology or Admission of Liability
• Saying sorry is not an admission of
liability; it is the right thing to do
• NHS LA does not withhold cover if an
apology or explanation has been given
www.nhsla.com
http://www.nhsla.com/
-
Clinical Governance - Summary
• What? – Clinical
– Staff
– Patient Focus
• Why? – Basis for quality care
• How? – Audit
– Surveys
• When? – Continuously