![ΠΠΠΠΠΠΠΠΠΠΠΠΠΤΠΠΠCOMPANY PROFILE 2 engKDW Ez [^ WZK&/> , >> E/ h /d/E' ^ X X, ] } Ç d Z } u v Ç Á ( } µ v ] v: µ v î ì í ì v ] ( r P } Á](https://static.fdocuments.us/doc/165x107/5fe010b76605db55a425a508/-company-profile-2-eng-kdw-ez.jpg)
Quel avenir pour la chirurgie thoracique et ... - Siz Nursingchirurgie colo-rectale… • î 30 %...
111
Quel avenir pour la chirurgie thoracique et de la transplanta4on pulmonaire Pr B Rondelet, MD, PhD
Transcript of Quel avenir pour la chirurgie thoracique et ... - Siz Nursingchirurgie colo-rectale… • î 30 %...
Quelavenirpourlachirurgiethoraciqueetdela
transplanta4onpulmonaire
PrBRondelet,MD,PhD
«Laminimalinvasivec’estnouveauetc’estl’avenirdela
chirurgiethoracique… »
VATS:unenouveauté?
DelMedJ.1992Apr;64(4):267-72.Video-assistedthoracicsurgery:ourfirst20cases.DaviesAL,PanasukDB.Video-assistedthoracicsurgeryhasbeenperformedin20pa4entsattheMedicalCenterofDelaware.Opera4onsincludedsevenpulmonarywedgeresec4ons,onemedias4nalprocedure,and12pleuralprocedures.Inallcases,adefini4vediagnosiswasmadeorthelesionwasremoved.Onepostopera4veatypicalpneumoniaoccurred.Onepa4entwhosewedgeresec4onprovedtobesquamouscellcarcinomaonfrozensec4onunderwentaformalthoracotomyandlobectomy.Es4matedsavingsintheeightpa4entswhoformerlywouldhaveundergoneathoracotomyincisionises4matedat$30,000forroomcostalone.Weforeseeamarkedlyexpandedroleforthistechniqueinmajorpulmonaryresec4ons,esophagealprocedures,andcardiacsurgeryinthenearfuture
VATS:unenouveauté?
DelMedJ.1992Apr;64(4):267-72.Video-assistedthoracicsurgery:ourfirst20cases.DaviesAL,PanasukDB.Video-assistedthoracicsurgeryhasbeenperformedin20pa4entsattheMedicalCenterofDelaware.Opera4onsincludedsevenpulmonarywedgeresec4ons,onemedias4nalprocedure,and12pleuralprocedures.Inallcases,adefini4vediagnosiswasmadeorthelesionwasremoved.Onepostopera4veatypicalpneumoniaoccurred.Onepa4entwhosewedgeresec4onprovedtobesquamouscellcarcinomaonfrozensec4onunderwentaformalthoracotomyandlobectomy.Es4matedsavingsintheeightpa4entswhoformerlywouldhaveundergoneathoracotomyincisionises4matedat$30,000forroomcostalone.Weforeseeamarkedlyexpandedroleforthistechniqueinmajorpulmonaryresec4ons,esophagealprocedures,andcardiacsurgeryinthenearfuture

ChestSurgClinNAm.1994Feb;4(1):185-94.Thymoma.Theuseofminimallyinvasiveresec<ontechniques.KaiserLR.Surgeryremainsthecornerstoneoftherapyforthymomawhetherthelesionisencapsulatedorinvasive.Video-assistedthoracicsurgicaltechniquesmaybeapplicableinanumberofpa4entswithencapsulatedthymomafordefini4vetherapy,especiallywhencombinedwithatranscervicalapproachtoachievetotalthymectomy.Ini4alexperiencewithaminimallyinvasiveapproachforresec4onofthymomasisdescribed.Thedevelopmentofnewinstrumenta4onfacilitatestheperformanceoftheseprocedures.
VATS:unenouveauté?
ChestSurgClinNAm.1994Feb;4(1):185-94.Thymoma.Theuseofminimallyinvasiveresec<ontechniques.KaiserLR.Surgeryremainsthecornerstoneoftherapyforthymomawhetherthelesionisencapsulatedorinvasive.Video-assistedthoracicsurgicaltechniquesmaybeapplicableinanumberofpa4entswithencapsulatedthymomafordefini4vetherapy,especiallywhencombinedwithatranscervicalapproachtoachievetotalthymectomy.Ini4alexperiencewithaminimallyinvasiveapproachforresec4onofthymomasisdescribed.Thedevelopmentofnewinstrumenta4onfacilitatestheperformanceoftheseprocedures.
VATS:unenouveauté?
JThoracCardiovascSurg.1992Dec;104(6):1679-85;discussion1685-7.Video-assistedthoracicsurgicalresec<onofmalignantlungtumors.LewisRJ,CaccavaleRJ,SislerGE,MackenzieJW.Fortypa4entswithmalignantpulmonarydiseaseunderwentevalua4on,staging,andabiopsyorresec4onbymeansofvideo-assistedthoracicsurgery.Therewere20menand20womenwhoseagesrangedfrom27to82years.Eightpa4entshadawedgeresec4onformetasta4ccarcinoma,threealobectomyforprimarycarcinoma,sixexplora4onofthethorax,fivebiopsyoftheaortopulmonarywindow,andeighteenasublobarresec4onforprimarycarcinomaofthelung.Therewasnomortality.Threepa4entshadairleaksthatlastedanaverageof8days.Video-assistedthoracicsurgeryseemstobeusefulformoreprecisestagingofcarcinomaofthelung,and,insomepa4ents,resec4onalopera4onscanbeperformed.
VATS:unenouveauté?

JThoracCardiovascSurg.1992Dec;104(6):1679-85;discussion1685-7.Video-assistedthoracicsurgicalresec<onofmalignantlungtumors.LewisRJ,CaccavaleRJ,SislerGE,MackenzieJW.Fortypa4entswithmalignantpulmonarydiseaseunderwentevalua4on,staging,andabiopsyorresec4onbymeansofvideo-assistedthoracicsurgery.Therewere20menand20womenwhoseagesrangedfrom27to82years.Eightpa4entshadawedgeresec4onformetasta4ccarcinoma,threealobectomyforprimarycarcinoma,sixexplora4onofthethorax,fivebiopsyoftheaortopulmonarywindow,andeighteenasublobarresec4onforprimarycarcinomaofthelung.Therewasnomortality.Threepa4entshadairleaksthatlastedanaverageof8days.Video-assistedthoracicsurgeryseemstobeusefulformoreprecisestagingofcarcinomaofthelung,and,insomepa4ents,resec4onalopera4onscanbeperformed.
VATS:unenouveauté?
Thorax.1993Sep;48(9):921-4.Thoracoscopyassistedpulmonarylobectomy.WalkerWS1,CarnochanFM,TinM.Thisreportdescribesapreliminaryexperiencewithsixpa4entsundergoingvideoimagedthoracoscopicpulmonarylobectomy.Threelegupperlobectomies,andoneeachofrightupper,rightlowerandleglowerlobectomywereundertaken.Theresec4onswereperformedasorthodoxdissec4onallobectomyproceduresbutwerecarriedoutundervideothoracoscopicimagingwithinstrumentsintroducedthroughtwostabincisions.Theen4reresectedlobewasdeliveredthrougha7cmsubmammaryintercostalincision.Therewerenoopera4vedeathsorcomplica4onsahributabletothetechnique.Inthreeotherpa4entsconversiontoanopenthoracotomywasrequiredbecauseofbleeding(twocases)orobscureanatomy(onecase).Post-opera4vepaininthoseundergoingthoracoscopicresec4onwaslessthanthatencounteredwithstandardthoracotomyandearlyclinicreviewshowedthepa4entstobepainfreewithexcellentshouldermovement.Majorpulmonaryresec<onaccordingtostandardcancerprac<cesisfeasiblewithvideothoracoscopictechniques.Thisapproachislikelytoofferconsiderablefunc<onalbenefittopa<ents.Specimendeliverythroughthesubmammaryincisionimposesa5cmprimarylesionsizelimita4on.Detailedmedias4nalassessmentisnecessarytoexcludeN2statusbeforeundertakingthoracoscopicsurgery.
VATS:unenouveauté?
Thorax.1993Sep;48(9):921-4.Thoracoscopyassistedpulmonarylobectomy.WalkerWS1,CarnochanFM,TinM.Thisreportdescribesapreliminaryexperiencewithsixpa4entsundergoingvideoimagedthoracoscopicpulmonarylobectomy.Threelegupperlobectomies,andoneeachofrightupper,rightlowerandleglowerlobectomywereundertaken.Theresec4onswereperformedasorthodoxdissec4onallobectomyproceduresbutwerecarriedoutundervideothoracoscopicimagingwithinstrumentsintroducedthroughtwostabincisions.Theen4reresectedlobewasdeliveredthrougha7cmsubmammaryintercostalincision.Therewerenoopera4vedeathsorcomplica4onsahributabletothetechnique.Inthreeotherpa4entsconversiontoanopenthoracotomywasrequiredbecauseofbleeding(twocases)orobscureanatomy(onecase).Post-opera4vepaininthoseundergoingthoracoscopicresec4onwaslessthanthatencounteredwithstandardthoracotomyandearlyclinicreviewshowedthepa4entstobepainfreewithexcellentshouldermovement.Majorpulmonaryresec<onaccordingtostandardcancerprac<cesisfeasiblewithvideothoracoscopictechniques.Thisapproachislikelytoofferconsiderablefunc<onalbenefittopa<ents.Specimendeliverythroughthesubmammaryincisionimposesa5cmprimarylesionsizelimita4on.Detailedmedias4nalassessmentisnecessarytoexcludeN2statusbeforeundertakingthoracoscopicsurgery.
VATS:unenouveauté?
JThoracCardiovascSurg.2003Jul;126(1):292-3.Robot-assistedlobectomy.AshtonRCJr,ConneryCP,SwistelDG,DeRoseJJJr.Video-assistedthoracoscopicsurgery(VATS)forana-tomicpulmonaryresec4onscon4nuestodevelopsinceitsapplica4onintheearly1990s.1-5UsingthedaVinciSurgicalSystem(Intui4veSurgical,Inc.,MountainView,Calif),weperformedananatomicrightlowerlobectomyforstageIanon–smallcelllungcancer.
Robo4clobectomy:unenouveauté?
JThoracCardiovascSurg.2003Jul;126(1):292-3.Robot-assistedlobectomy.AshtonRCJr,ConneryCP,SwistelDG,DeRoseJJJr.Video-assistedthoracoscopicsurgery(VATS)forana-tomicpulmonaryresec4onscon4nuestodevelopsinceitsapplica4onintheearly1990s.1-5UsingthedaVinciSurgicalSystem(Intui4veSurgical,Inc.,MountainView,Calif),weperformedananatomicrightlowerlobectomyforstageIanon–smallcelllungcancer.
Robo4clobectomy:unenouveauté?

Laminimalinvasiven’estpasunedémarchenouvelle…
Ques4ons…
• Y-a-t-ilunintérêtautrequelaperformancemanuelleàfairedelachirurgiemoinsinvasive?
• Quellessontlesrépercussionssurlasociété?
• Commentladémarchepeutelleêtreefficiente?
Fast-TrackChirurgie
• Récupéra:onrapidedespa:entsaprèschirurgie Réhabilita:onprécoce Fast-track-surgery EnhancedrecoveryaBersurgery
• Viselareprised'uneautonomieac4veetcomplètedupa4ent,leplusrapidementpossibleaprèssachirurgie.
• C’estunemédecinefondéesurlesfaits,validéepardespublica4onsscien4fiques.
=
Fast-TrackChirurgie
• Méta-analysed'essaisrandomiséscontrôléspourlachirurgiecolo-rectale…• î30%laduréedeséjour,• î50%lescomplica4onspéri-opératoires.
• Chaqueétape,chaquesoinyestop4miséetorganiséautourdel’opéré.
• Elleaétéini4alementdéveloppéeparlePrHKehletauDanemarken1995pourlachirurgiecolique.
• Larécupéra4onrapideaprèschirurgiesecombineidéalementaveclestechniqueschirurgicalesmini-invasivestellesquelacœlioscopie.
Cafait20ansqu’onfaitça…
• Kehletaeul'intui4onquedenombreusesétapesdelapriseenchargeclassiqueenchirurgiereposaientplussurlepoidsdeshabitudesetsurlestradi4onsquesuruneanalysesystéma4quedesbénéficesapportésauxpa4ents.
• Iladoncanalyséchacunedecesétapesetderechercherquelétaitleniveaudepreuvescien4fiquementpubliéjus4fiantlaprésenceoul'absenced'uneétapedonnéedanslesprotocolesu4lisés.
• Ilapuprouverquedenombreuxactesréalisésétaientnonseulementinu4lesmaisdélétèrespourlaplupartdespa4entsopérésducôlon.

Unpa4entacteur…
• L'autrepilierdelaréflexiondeKehletestl'associa4ondupa4entàsessoins.
• Dansleschémaclassique,lepa4entauneposturepassive.Lesdécisionssontprisesparlespra4ciens;lepa4entestinformé.
• Danslarécupéra4onrapideaprèschirurgie,lepa4entreçoituneinforma4ontrèsapprofondiesurlesdifférentstempsdutraitement.Lapa4entestinscritdansunpartenariat.
• Lepa4entestdoncréellementunmoteurdesapropreréhabilita4onetpeutinfluencerlesdécisionsenfonc4ondesespropressensa4onsetduretourd'informa4onqu'ildonneauxprofessionnelsdesanté.
Touspourunmalade…Unmaladepourtous!
• Pluridisciplinaritédelapriseencharge…• Audelàdubinômehabituelchirurgie-anesthésiste,il
associelepersonnelinfirmier,leskinésithérapeutes,lesdiété4ciens,lesassistantssociaux,lescoordinateursdesoins,etc…
• Chacunvaapportersonexper4sedefaçoncoordonnéepouraheindrelesobjec4fsfixésetcommuniquerpourajusterlapriseenchargesibesoin.
• Cehepluridisciplinaritésetrouveformaliséesousformedeprotocoles/parcourtsdesoinsrigoureuxdontl'exécu4onestrégulièrementévaluée.
Desprincipes…
• Réduirelestressphysiqueetpsychiqueliéàl'interven4on.
• Prévenirlesdysfonc4onsorganiquessecondairesdelachirurgie• Nausées,• Somnolence,• Vomissements,• Dyspepsieetiléusparaly4quepostopératoire,• Douleur...

Desprincipes…
• Combinaisondemesures:jeûnepré-opératoirelimité,u4lisa4ondedrogued’anesthésieàcourteduréed’ac4on,préven4ondel’hypothermie,analgésiemul4modaleauplusprochedelasource,ges4onindividualiséedesapportsliquidiens,u4lisa4onlimitéededrains,u4lisa4onlimitédesondageurinaire,réalimenta4onprécoce,mobilisa4onrapide…
• C’estl’ensembledecesmesuresetlacoordina4ondel’équipedepriseenchargequipermetaupa4entderetrouverplusvitesonautonomie.

Desprincipes…
• Leretouràl'autonomiedupa4entluipermetnonseulementderentrerplusrapidementàlamaison,maisaussidepouvoirmieuxgérerceretouràdomicilehorsducoconprotecteurdel'hôpitaloudelaclinique.
• L'ensembledel'organisa4onestformalisésousformedeprocéduresetprotocolesstandardisés.Ilssuiventlatrajectoiredupa4entetprennentsouventlenomdei4nérairecliniquequicomprendparexemplelesdocumentsd'informa4onquiserontremisaupa4entetlesscoresquipermehentd'évaluersonétatetdedéciderdesasor4e.
Desretombéesimportantes…
• Lespublica4onsscien4fiquesmontrentquelasa4sfac4ondespa4entsestexcellenteetquelestauxdecomplica4onsetréadmissionssontiden4ques(voiremeilleurs)qu’avecunepriseenchargetradi4onnelle.
• Lepa4entretrouveunconfortplusrapidementetladuréed’hospitalisa4onestlimitéeainsilescoûtsdiminuent.
• Danslespaysoùelleestlargementdiffusée,elleréduitlenombredelitsdechirurgienécessairespourfairefaceàlademandedelapopula4ondufaitdelabaissedeladuréemoyennedeséjour,sansquelesdépensessoientreportéessurlamédecinedevilleoulescentresderééduca4on.Lesressourcesainsilibéréespeuventdoncêtreconsacréesàd'autresbesoinssanitaires.
Desretombéesimportantes…
• Ceheapprocheestplébiscitéeaujourd’huiparleNa4onalHealthservice(NHS)etestdevenuelanormeenGrandeBretagne.
• Depuislafin2011,larécupéra4onrapideaprèschirurgiepourlaprothèsetotaledehancheetlaprothèsedugenoubénéficieainsid'unetarifica4onspécialeenGrandeBretagnedanslecadredes"bestprac4cetarifs».
• Unnombrecroissantdecentresadopteégalementlarécupéra4onrapideaprèschirurgieàtraverslemondemaiselleresteconfiden4elleenBelgiquemalgrélespreuvesdesonefficience.
Etlachirurgiethoracique?
Anesthésie&Ges4ondela
douleur
Servicesocial
Nursing
Revalida4on
Soinsintensifs
Chirurgie
Diété4que
Tabacologie

Démarche(s)…
• Toutdoitêtresystéma4quementremisencause…• Etablirunelistedesétapeduprocessuspourchaque
spécialité.• Pourchaqueétape,faireunerevuedelalihérature
exhaus4vepourdégagerlesméthodesquidonnentlemoinsdedysfonc4onsorganiquessecondaires.Abandonnerlestradi4ons,implémenterdesa�tudesbaséessurl’evidencebasedmedicine.
• Etablirdesprotocolespourchaqueen4téimpliquée.• Etablirunparcourtdesoinsquiar4culechaquespécialité
aveclesautres.• Etablirunparcourtde«communica4on»dansl’équipeet
aveclepa4ent.
• Laqualitédelarésec4on:R0,R1…
• Laqualitéducurageganglionnaireetdustaging…
Pourlachirurgie…Lasurvieestcondi4onnéepar…
Stagingmédias4nalpré-op?EUS/EBUScombinésenpremièreinten4onChest.2014Aug;146(2):389-97.Endosonographicmedias<nallymphnodestagingoflungcancer.LibermanM,SampalisJ,DuranceauA,ThiffaultV,HadjeresR,FerraroP.Itisunclearwhetherendoscopicmedias4nallymphnode(LN)stagingtechniquesareequivalenttosurgicalmedias4nalstaging(SMS)techniquesinpa4entswithpoten4allyoperablenon-smallcelllungcancer(NSCLC).Atotalof166pa4entswithconfirmedorsuspectedNSCLCwhorequiredSMSbasedoncurrentguidelineswereenrolledinthisprospec4vecontrolledtrialcomparingendosonographicmedias4nalLNstagingwithSMS.Eachpa4entservedashisorherowncontrol.Allpa4entsunderwentendobronchialultrasound(EBUS),endoscopicultrasound(EUS),andSMSduringasingleprocedure.ResultsofEBUS,EUS,andcombinedEBUS/EUSwerecomparedwithSMS(goldstandard)andinpa4entswithnega4veLNstagingresults,withLNsamplingatpulmonaryresec4on.
ThecombinedEBUS/EUSprocedurecanreplacesurgicalmedias<nalstaginginpa<entswithpoten<allyresectableNSCLC.Addi<onally,endosonographyleadstoimprovedstagingcomparedwithSMSbecauseitallowsthebiopsyofLNsandmetastasesunaPainablewithSMStechniques.

Stagingmédias4nalpré-op?Uneplacepourlamédias4noscopie?
InteractCardiovascThoracSurg.2013Nov;17(5):823-8.Medias<nalstagingindailyprac<ce:endosonography,followedbycervicalmedias<noscopy.Dowereallyneedboth?VerhagenAF,SchuurbiersOC,Looijen-SalamonMG,vanderHeideSM,vanSwietenHA,vanderHeijdenEH.Inpa4entswithlungcancer,endosonographyhasemergedasaminimallyinvasivemethodtoobtaincytologicalproofofmedias4nallymphnodes,suspiciousformetastasesonimaging.Incaseofanega4veresult,itiscurrentlyrecommendedthatacervicalmedias4noscopybeperformedaddi4onally.However,indailyprac4ce,asecondprocedureisogenregardedsuperfluous.Thegoalofourstudywastoassesstheaddi4onalvalueofacervicalmedias4noscopy,ageranega4veresultofendosonography,inrou4neclinicalprac4ce.Inaretrospec4vecohortstudy,therecordsof147consecu4vepa4entswithanindica4onformedias4nallymphnodestagingandanega4veresultofendosonographywereanalysed.Asasubsequentprocedure,124pa4entsunderwentacervicalmedias4noscopyand23pa4entswerescheduledforanintendedcura4veresec4ondirectly.Thenega4vepredic4vevalue(NPV)forbothdiagnos4cprocedureswasdetermined,aswellasthenumberofpa4entswhoneededtoundergoamedias4noscopytofindonefalse-nega4veresultofendosonography(numberneededtotreat(NNT)).Clinicaldataofpa4entswithafalse-nega4veendosonographywereanalysed.
Inpa<entswithahighprobabilityofmedias<nalmetastases,basedonimaging,andnega<veendosonography,cervicalmedias<noscopyshouldnotbeomiPed,notevenwhentheaspirateseemsrepresenta4ve.
Stagingmédias4nalpré-op?Quelletechniquedemédias4noscopie?
JThoracCardiovascSurg.2013Oct;146(4):774-80.Video-assistedmedias<noscopiclymphadenectomyisassociatedwithbePersurvivalthanmedias<noscopyinpa<entswithresectednon-smallcelllungcancer.TurnaA,DemirkayaA,OzkulS,OzB,GursesA,KaynakK.Weaimedtoanalyzetheaccuracyofvideo-assistedmedias4noscopiclymphadenectomy(VAMLA)asatoolforpreopera4vestagingandtheimpactofthetechniqueonsurvivalinpa4entswithnon-smallcelllungcancer(NSCLC)undergoingpulmonaryresec4on.BetweenMay2006andDecember2010,433pa4entsunderwentpulmonaryresec4onforNSCLC,89(21%)hadVAMLAbeforeresec4onand344(79%)hadstandardmedias4noscopy.Thepa4entswhohadnega4veVAMLA/medias4noscopyresultsunderwentanatomicpulmonaryresec4onandsystema4clymphnodedissec4on.Themedianandmeannumbersofresectedlymphnodesta4onswere5and4.9intheVAMLAgroupand4
Video-assistedmedias<noscopiclymphadenectomywasassociatedwithbePersurvival(oddsra<o,1.34;95%VAMLAwasassociatedwithimprovedsurvivalinNSCLCpa<entswhohadresec<onalsurgery.
Stagingmédias4nalpré-op?Quelle(s)technique(s)?Quand?Comment?
EurJCardiothoracSurg.2014May;45(5):787-98.RevisedESTSguidelinesforpreopera<vemedias<nallymphnodestagingfornon-small-celllungcancer.DeLeynP,DoomsC,KuzdzalJ,LardinoisD,PasslickB,Rami-PortaR,TurnaA,VanSchilP,VenutaF,WallerD,WederW,ZielinskiM.1.Incaseofcomputedtomography(CT)-enlargedorpositronemissiontomography(PET)-posi4vemedias4nallymphnodes,4ssueconfirma4onisindicated.
a.Endosonography[endobronchialultrasonography(EBUS)/esophagealultrasonography(EUS)]withfine-needleaspira4on(FNA)isthefirstchoice(whenavailable),sinceitisminimallyinvasiveandhasahighsensi4vitytoruleinmedias4nalnodaldisease.b.Ifnega4ve,surgicalstagingwithnodaldissec4onorbiopsyisindicated.Video-assistedmedias4noscopyispreferredtomedias4noscopy.Thecombineduseofendoscopicstagingandsurgicalstagingresultsinthehighestaccuracy.
2.WhentherearenoenlargedlymphnodesonCTandwhenthereisnouptakeinlymphnodesonPETorPET-CT,directsurgicalresec4onwithsystema4cnodaldissec4onisindicatedfortumours≤3cmlocatedintheouterthirdofthelung.3.IncentraltumoursorN1nodes,preopera4vemedias4nalstagingisindicated.ThechoicebetweenendoscopicstagingwithEBUS/EUSandFNAorvideo-assistedmedias4noscopydependsonlocalexper4setoadheretominimalrequirementsforstaging.4.Fortumours>3cm,preopera4vemedias4nalstagingisadvised,mainlyinadenocarcinomawithhighstandardizeduptakevalue.5.Forrestaging,invasivetechniquesprovidinghistologicalinforma4onareadvisable.Bothendoscopictechniquesandsurgicalproceduresareavailable,buttheirnega4vepredic4vevalueislowercomparedwiththeresultsobtainedinbaselinestaging.Anintegratedstrategyusingendoscopicstagingtechniquestoprovemedias4nalnodaldiseaseandmedias4noscopytoassessnodalresponseagerinduc4ontherapyneedsfurtherstudy.
Résec4onpulmonaireVATSlobectomy:Techniquesûreetefficace?
ZhonghuaYiXueZaZhi.2013Oct8;93(37):2972-5.[Acompara<vestudyofcompletevideo-assistedthoracoscopiclobectomyandvideo-assistedmini-thoracotomyintreatmentoflungcancer].ZhangY,LiYB,LiuBD,ChenDH,WangRT,LiuL,QianK,ZhiXY.Toexploretheclinicalapplica4onvalueofcompletevideo-assistedthoracoscopic(cVATS)lobectomyinthemini-invasivetreatmentoflungcancer.90pa4entswithnon-smallcelllungcancer(NSCLC)whohadundergonelobectomywerereviewed.Accordingtosurgicalapproach,completevideo-assistedthoracoscopiclobectomygroup(cVATS,n=47)andvideo-assistedmini-thoracotomygroup(VAMT,n=43)werestudied.Numbersofdissectedlymphnodes,opera4ondura4on,volumesofintraopera4vebleeding,dura4onofpostopera4vecatheterdrainage,lengthofpostopera4vehospitalstay,incidenceratesofpostopera4vecomplica4ons,postopera4vepainscoresofpa4entswerecomparedbetweenthetwogroupsretrospec4vely.
Completevideo-assistedthoracoscopiclobectomyissafeandeffec<vesurgicalstrategyforlungcancerpa<entswithadvantageofrapidrecovery.
Résec4onpulmonaireRobo4clobectomy:Techniquesûreetefficace?
AnnSurg.2017Feb;265(2):431-437.Long-termSurvivalBasedontheSurgicalApproachtoLobectomyForClinicalStageINonsmallCellLungCancer:ComparisonofRobo<c,Video-assistedThoracicSurgery,andThoracotomyLobectomy.YangHX1,WooKM,SimaCS,BainsMS,AdusumilliPS,HuangJ,FinleyDJ,RizkNP,RuschVW,JonesDR,ParkBJ.Tocomparethelong-termoutcomesamongrobo4c,video-assistedthoracicsurgery(VATS),andopenlobectomyinstageInonsmallcelllungcancer(NSCLC).Survivalcomparisonsbetweenrobo4c,VATS,andopenlobectomyinNSCLChavenotyetbeenreported.SomestudieshavesuggestedthatsurvivalagerVATSissuperior,forunclearreasons.Threecohorts(robo4c,VATS,andopen)ofclinicalstageINSCLCpa4entswerematchedbypropensityscoreandcomparedtoassessoverallsurvival(OS)anddisease-freesurvival(DFS).Univariateandmul4variateanalyseswereperformedtoiden4fyfactorsassociatedwiththeoutcomes.
MinimallyinvasiveapproachestolobectomyforclinicalstageINSCLCresultinsimilarlong-termsurvivalasthoracotomy.UseofVATSandrobo<csisassociatedwithshorterlengthofstay,andtherobo4capproachresultedingreaterlymphnodeassessment.
Résec4onpulmonaireVATS,Est-ceefficaced’unpointdevueoncologique?
AnnThoracSurg.2014Jul;98(1):197-202.Thoracoscopicapproachtolobectomyforlungcancerdoesnotcompromiseoncologicefficacy.BerryMF,D'AmicoTA,Onai4sMW,KelseyCR.Wecomparedsurvivalbetweenvideo-assistedthoracoscopicsurgery(VATS)andthoracotomyapproachestolobectomyfornon-smallcelllungcancer.Overallsurvivalofpa4entswhohadlobectomyforanystagenon-smallcelllungcancerwithoutpreviouschemotherapyorradia4onfrom1996to2008wasevaluatedusingtheKaplan-Meiermethodandmul4variateCoxanalysis.Propensityscoringwasusedtoassesstheimpactofselec4onbias.
Thethoracoscopicapproachtolobectomyfornon-smallcelllungcancerdoesnotresultinworselong-termsurvivalcomparedwiththoracotomy.
Résec4onpulmonaireYa-t-ilunealterna4veefficaceauVATSsiconversion?
EurJCardiothoracSurg.2014Oct;46(4):614-9.doi:10.1093/ejcts/ezu050.Epub2014Feb26.Thecomparisonofcomplica<on,pain,qualityoflifeandperformancea`erlungresec<onswiththoracoscopyandaxillarythoracotomy.ErusS,TanjuS,KapdağlıM,ÖzkanB,DilegeŞ,TokerA.Theaimofthisprospec4vestudywastocomparetheeffectsofaxillarythoracotomy(AT)andvideo-assistedthoracoscopicsurgery(VATS)onacute-phaseresponses,performancestatusandqualityoflifeinpa4entsundergoingpulmonaryresec4on.Figy-fivepa4entswithperipherallylocatedlunglesionswereenrolledintothisstudy.SurgerywasdonebyVATSorAT.Forcedexpiratoryvolume,smokinghabits,complica4ons,Charlsoncomorbidityindex,sex,age,lengthofincision,lengthofopera4on,lengthofhospitalstay,lengthofdrainage,lengthofairleakage,preopera4veandpostopera4veC-reac4veprotein(CRP)values,visualanaloguescale,qualityoflifeandperformancestatusofthepa4entsweremeasuredandcompared.
AxillarythoracotomyisatechniqueequivalenttoVATSintermsofearlycomplica<ons,,performancestatusandqualityoflife;VATSprovidedashorterpostopera<vestay.

Résec4onpulmonaireVATSvsMini-thoracotomied’unpointdevuedouleur….
EurJEurJCardiothoracSurg.2014Nov;46(5):907-12.doi:10.1093/ejcts/ezu092.Epub2014Mar18.Postopera<vepaincontrol:videothoracoscopicversusconserva<vemini-thoracotomicapproach.Andree�C,MennaC,IbrahimM,CicconeAM,D'AndrilliA,VenutaF,RendinaEA.Themanagementofpostopera4vepaininthoracicsurgeryisanopenissue.Theaimofthisstudywastocomparepostopera4vepainageravideothoracoscopiclobectomyversusamini-thoracotomyapproach.BetweenApril2011andJanuary2013weenrolledinaprospec4ve,non-randomizedstudy145pa4entsundergoingpulmonarylobectomywithlymphadenectomyforStageIlungcancer.In75cases(GroupA),surgerywasperformedthroughavideothoracoscopicapproach.In70cases(GroupB),surgerywasundertakenthroughaconserva4vemini-thoracotomy.Painwasassessedbyvisualanaloguescaleandlungfunc4onbyspirometryandsix-minutewalkingtest(6MWT)beforesurgery,at48hand1monthagersurgery.
ThevideothoracoscopicapproachinthetreatmentofStageIlungcancerreducespostopera<vepain,whichseemstoallowarapidfunc<onalrecoveryofpa<ents.
Résec4onpulmonaireVATSvsthoracotomie:Résultats…
PLoSOne.2013Dec31;8(12):e82366.ThoracoscopiclobectomyversusopenlobectomyinstageInon-smallcelllungcancer:ameta-analysis.CaiYX,FuXN,XuQZ,SunW,ZhangN.Theobjec4veofthepresentmeta-analysiswastoevaluatethesurvival,recurrencerate,andcomplica4onsinpa4entswithstageInon-smallcelllungcancer(NSCLC)whoreceivedvideo-assistedthoracoscopicsurgery(VATS)oropenlobectomy.
Pa<entswithstageINSCLCundergoingVATSlobectomyhadlongersurvivalandfewercomplica<onsthanthosewhoreceivedopenlobectomy.

Résec4onpulmonaireVATSvsthoracotomie:Coûts…
AnnThoracSurg.2014Jul;98(1):191-6.Ninety-daycostsofvideo-assistedthoracicsurgeryversusopenlobectomyforlungcancer.FarjahF,BackhusLM,VargheseTK,MulliganMS,ChengAM,Alfonso-CristanchoR,FlumDR,WoodDE.Complica4onsagerpulmonaryresec4onleadtohighercostsofcare.Video-assistedthoracoscopicsurgery(VATS)forlobectomyisassociatedwithfewercomplica4ons,butlowerinpa4entcostsforVATShavenotbeenuniformlydemonstrated.Becausesomecomplica4onsoccuragerdischarge,wecompared90-daycostsofVATSlobectomyversusopenlobectomyandexploredwhetherdifferen4alhealthcareuseagerdischargemightaccountforanyobserveddifferencesincosts.Acohortstudy(2007-2011)ofpa4entswithlungcancerwhohadundergoneresec4onwasconductedusing
VATSlobectomyisassociatedwithlower90-daycosts--arela4onshipthatappearstobemediatedbylowerratesofPLOS.AlthoughVATSmayleadtolowerratesofPLOSamongpa4entsundergoinglobectomy,observa4onalstudiescannotverifythisasser4on.StrategiesthatreducePLOSwilllikelyresultincost-savingsthatcanincreasethevalueofthoracicsurgicalcare.

Résec4onpulmonaireVATS/Robo4c:L’épargnepulmonaire,camarche?
JThoracOncol.2017Jan20ComparisonofSegmentectomyandLobectomyinStageIAAdenocarcinomas.ZhaoZR1,SituDR2,LauRW1,MokTS3,ChenGG1,UnderwoodMJ1,NgCS4Recentstudieshavesuggestedthatsegmentectomymaybeanacceptablealterna4vetreatmenttolobectomyforsurgicalmanagementofsmallerlungadenocarcinomas.Theobjec4veofthisstudywastocomparesurvivalagerlobectomyandsegmentectomyamongpa4entswithpathologicalstageIAadenocarcinomacategorizedasstageT1b(>0to≤20mm)accordingtotheneweighthedi4onoftheTNMsystem.
Pa<entswhounderwentsegmentectomymayhavesurvivaloutcomesnodifferentthanthoseofsomepa<entswhoreceivedlobectomyforpathologicalstageIAadenocarcinomasatleast10butnolargerthan20mminsize.Theseresultsshouldbefurtherconfirmedthroughprospec4verandomizedtrials.
Résec4onpulmonaireVATS/Robo4c:L’épargnepulmonaire,camarche?
EurJCardiothoracSurg.2017Apr11.StageInon-small-celllungcancer:long-termresultsoflobectomyversussublobarresec<onfromthePolishNa<onalLungCancerRegistry†.DziedzicR1,ZurekW1,MarjanskiT1,RudzinskiP2,OrlowskiTM2,SawickaW3,MarczykM4,PolanskaJ4,RzymanW1.Anatomicallobarresec4onandmedias4nallymphadenectomyremainthestandardforthetreatmentofearlystagenon-small-celllungcancer(NSCLC)andarepreferredoverproceduressuchassegmentectomyorwedgeresec4on.However,thereisanongoingdebateconcerningtheinfluenceoftheextentoftheresec4ononoverallsurvival.Theaimofthisar4clewastoassesstheoverallsurvivalfordifferenttypesofresec4onforStageINSCLC.Weperformedaretrospec4veanalysisoftheresultsofthesurgicaltreatmentofStageINSCLC.Between1January2007and31December2013,thedatafrom6905pa4entswhounderwentStageINSCLCopera4onswerecollectedinthePolishNa4onalLungCancerRegistry(PNLCR)andoverallsurvivalwasassessed.Apropensityscore-matchedanalysiswasusedtocompare3groupsofpa4ents,eachconsis4ngof231pa4ents
Wedgeresec<onwasassociatedwithsignificantlylower3-yearand5-yearsurvivalratescomparedtotheothermethodsofresec<on.Therewasnosignificantdifferencein3-yearor5-yearsurvivalratesbetweenlobectomyandsegmentectomy.Segmentectomy,butnotwedgeresec<on,couldbeconsideredanalterna<vetolobectomyinthetreatmentofpa<entswithStageINSCLC.

Résec4onpulmonaireVATSvsrobo4c:Coûts…Effetduvolumeopératoire.
Chest.2017Feb;151(2):329-339.HospitalVolumeandOutcomesofRobot-AssistedLobectomies.TchoutaLN1,ParkHS2,BoffaDJ1,BlasbergJD1,DeherbeckFC1,KimAW3..Theposi4veimpactofhospitalopera4vevolumeonoutcomesfollowingvideo-assistedthoracoscopicsurgeryhasbeenestablished.Thegoalofthisstudywastodeterminewhetherornotthisvolume/outcomerela4onshiptranslatestorobot-assistedthoracoscopicsurgery(RobATS)lobectomy.Pa4entswhounderwentRobATSlobectomywereiden4fiedbetween2008and2013intheHealthcareCostandU4liza4onProjectNa4onalInpa4entSampledatabase.Hospitalvolume,aswellasdemographic,clinical,andhealth-caresystem-relatedfactorswereselectedaspoten4alpredictorsofoutcomes.Outcomevariablesincludedlengthofstay(LOS),inpa4entmortality,andcomplica4ons.Hospitalsweredesignatedbyquar4lesaccordingtoannualcasevolume,withverylow-volumedefinedasthefirstquar4leandhigh-volumedefinedasthefourthquar4le.Regressionanalyseswereusedtoiden4fyindependentpredictorsoftheoutcomesofinterest.
Undergoinglobectomyathigh-volumeRobATScentersconfersfavorablemortalityandLOSoutcomescomparedwithverylow-volumecenters.However,thebeneficialeffectofvolumeonmortalitysuggestsaneedforthecarefuladop<onofthispromisingtechnology.
Stagingper-opVATSvsthoracotomie:Curageganglionnaire…
JThoracDis.2014Jan;6(1):45-51.Compara<vestudyofsystema<cthoracoscopiclymphadenectomyandconven<onalthoracotomyinresectablenon-smallcelllungcancer.WangW,YinW,ShaoW,JiangG,WangQ,LiuL,LiuD,WangZ,ZhuZ,ChenH,HeJ.Toassessthefeasibilityandsafetyofthevideo-assistedthoracoscopysurgery(VATS)systema4clymphnodedissec4oninresectablenon-smallcelllungcancer(NSCLC).Theclinicaldataofpa4entswithNSCLCwhounderwentVATSorthoracotomycombinedwithlobectomyandsystema4clymphadenectomyfromJanuary2001toJanuary2008wereretrospec4velyanalyzedtoiden4fytheirdemographicparameters,numberofdissectedlymphnodesandpostopera4vecomplica4ons.Forpa<entswithresectableNSCLC,VATSsystema<clymphnodedissec<onissafeandeffec<vewithfewerpostopera<vecomplica<ons,andsignificantlyfasterpostopera<verecoverycomparedwithtradi<onalopenchestsurgery.

Stagingper-opVATSvsthoracotomievsrobo4c:Curageganglionnaire…?
AnnSurg.2017Feb;265(2):431-437.Long-termSurvivalBasedontheSurgicalApproachtoLobectomyForClinicalStageINonsmallCellLungCancer:ComparisonofRobo<c,Video-assistedThoracicSurgery,andThoracotomyLobectomy.YangHX1,WooKM,SimaCS,BainsMS,AdusumilliPS,HuangJ,FinleyDJ,RizkNP,RuschVW,JonesDR,ParkBJ.Tocomparethelong-termoutcomesamongrobo4c,video-assistedthoracicsurgery(VATS),andopenlobectomyinstageInonsmallcelllungcancer(NSCLC).Survivalcomparisonsbetweenrobo4c,VATS,andopenlobectomyinNSCLChavenotyetbeenreported.SomestudieshavesuggestedthatsurvivalagerVATSissuperior,forunclearreasons.Threecohorts(robo4c,VATS,andopen)ofclinicalstageINSCLCpa4entswerematchedbypropensityscoreandcomparedtoassessoverallsurvival(OS)anddisease-freesurvival(DFS).Univariateandmul4variateanalyseswereperformedtoiden4fyfactorsassociatedwiththeoutcomes.
MinimallyinvasiveapproachestolobectomyforclinicalstageINSCLCresultinsimilarlong-termsurvivalasthoracotomy.UseofVATSandrobo4csisassociatedwithshorterlengthofstay,andtherobo4capproachresultedingreaterlymphnodeassessment.
Stagingper-opPeutonencoreêtremoinsinvasif?
JThoracCardiovascSurg.2017Feb10Anoveltechniquefortumorlocaliza<onandtargetedlympha<cmappinginearly-stagelungcancer.HacheyKJ1,DigesuCS1,ArmstrongKW1,GilmoreDM2,KhullarOV3,WhangB1,TsukadaH1,ColsonYL4.Toinves4gatesafetyandfeasibilityofnaviga4onalbronchoscopy(NB)-guidednear-infrared(NIR)localiza4onofsmall,ill-definedlunglesionsandsen4nellymphnodes(SLN)foraccuratestaginginpa4entswithnon-smallcelllungcancer(NSCLC).Pa4entswithknownorsuspectedstageINSCLCwereenrolledinaprospec4vepilottrialforlesionlocaliza4onandSLNmappingviaNB-guidedNIRmarking.Successfullocaliza4on,SLNdetec4onrates,histopathologicstatusofSLNversusoverallnodes,andconcordancetoini4alclinicalstageweremeasured.Exvivoconfirma4onofNIR+SLNsandadverseeventswererecorded.
NB-guidedNIRlesionlocaliza<onandSLNiden<fica<onwassafeandfeasible.Thisminimallyinvasiveimage-guidedtechniquemaypermittheaccuratelocaliza<onandnodalstagingofearlystagelungcancers.
Therefore, 2 separate groups used the strategy of combin-ing both blue dye and radioisotopes to aid in the detection ofthe SLN in patients with lung cancer. Schmidt and col-leagues18 used intraoperative injection of both blue dyeand technetium-99m to identify the mediastinal lymph no-des. However, again, the rate of SLN identification wasonly 81%.18 The second group, Tiffet and colleagues,19
studied intraoperative injection of both markers, identifyingSLN in only 13 (54%) of 24 patients, with some patients ex-hibiting only blue dye or technetium-99mmigration and notboth markers.19 These previous approaches have demon-strated the technical difficulty of visualizing blue dyewithinthe anthracotic nodes and the differences in anatomy thatmake use of Geiger counters to identify radioisotopes diffi-cult. In addition, the use of radioactivity poses a biologicrisk to the surgeon, operating room personnel, patient, andpathologist and is limited by the ‘‘shine through’’ to nearbystructures. As a standard approach to the thousands of pa-tients with lung cancer, this is not an ideal solution. Thepoor reliability negates the clinical utility of these ap-proaches and new innovations are needed.
NIR IMAGINGRecent success with ICG in lymph node mapping in pre-
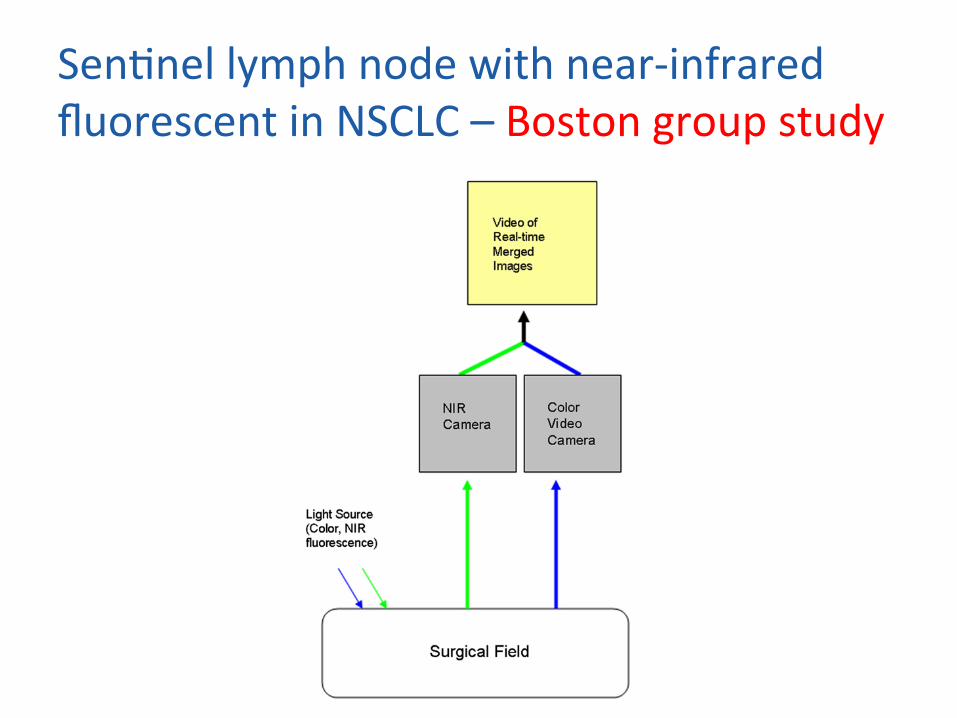
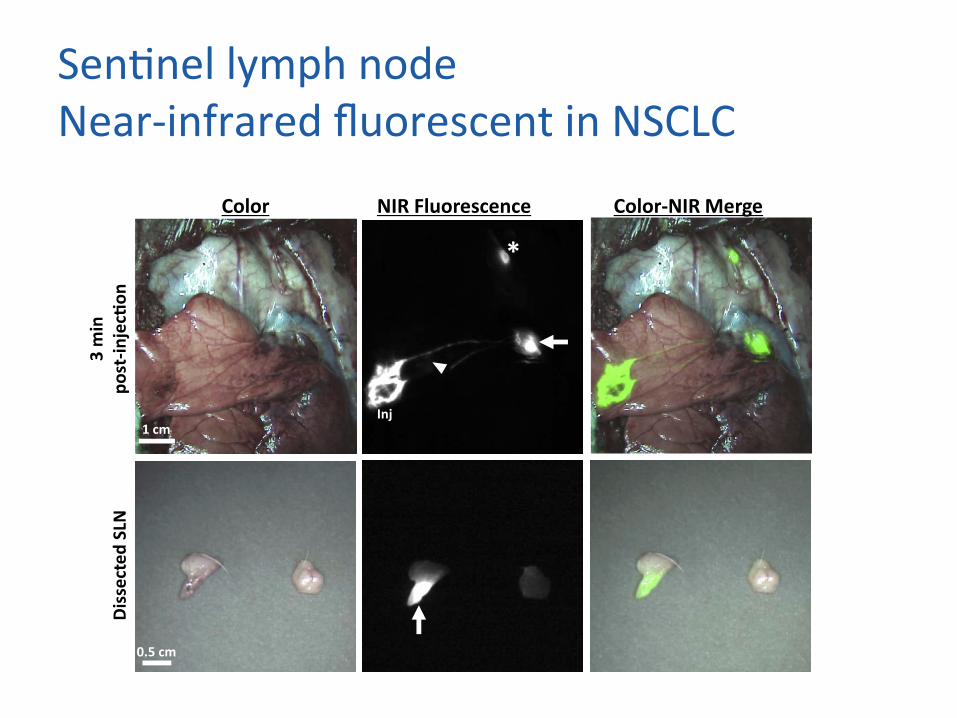
clinical trials involving animal models and clinical trials ofbreast cancer have renewed the interest in SLN biopsy inNSCLC.20,21 NIR fluorescence uses safe NIR excitation toprovide simultaneous intraoperative imaging of visiblereflected light and the NIR fluorescence emitted from ICG(Figure 1). ICG can quickly and reliably migrate to draininglymph node basins, permitting rapid and accurate SLN iden-tification in a real-time intraoperative setting. Invisible NIRlight penetrates into tissue, detecting fluorescent objects ata depth of 1 cm in solid tissue. By maintaining separationof the visible and NIR fluorescent light, it is possible to si-multaneously acquire color and NIR fluorescence imagesand to overlay the 2 images. Thus, a single, intraoperativeprocedure is available to visualize SLNs, in which the surgi-cal field remains unaltered, without additional radiation riskto the patient or operating staff. To date, NIR-guided SLNdetection in nonthoracic systems has been characterizedby the identification of the SLN using NIR technology and
concurrent real-time videoscopic images of the necessaryanatomic landmarks required for safe and accurate surgicaldissection, low background signal from biologic tissue,a nearly 100% sensitivity owing to the high signal/noise ra-tio in the node, and successful identification of a single SLNstation in more than 90% of cases.
TECHNIQUEIn our phase I clinical trial, we assessed the safety and
feasibility of NIR imaging using ICG for SLN identificationin NSCLC in 29 patients. From the results of large animalstudies, our initial technique consisted of peritumoral sub-pleural injection of low-dose ICG (3.8 mg) coupled withfresh frozen plasma under direct visualization using theopen-platform fluorescence-assisted resection and explora-tion camera. After injection, the surgeon proceeded with theplanned operation, avoiding excision of the tumor or manip-ulation of the lymphatic drainage system while the ICG wasmigrating within the lymphatic channels to the SLN for atleast 5 minutes and for up to 20 minutes. Inconsistent visu-alization of migration and/or SLN identification led to thefollowing alterations of our initial technique.
Imaging PlatformAt the onset of our trial, most lung resections were per-
formed through a thoracotomy, making the open FLARE
TABLE 1. Initial sentinel lymph node biopsy mapping studies in
non–small cell lung cancer
Group Year Technique Success rate (%)
Little et al14 1999 Blue dye 47
Liptay et al15 2000 Radioisotope 81
Liptay et al16 2009 Radioisotope 51
Noromi et al17 2007 Preoperative radioisotope 81
Schmidt et al18 2002 Intraoperative blue
dye/radioisotope
81
Tiffet et al19 2005 Intraoperative blue
dye/radioisotope
54
FIGURE 1. Near-infrared imaging. The light source of normal white light
and near-infrared fluorescence is reflected off the surgical field and col-
lected by the camera, producing a real-time merged image.
Session VIII: Innovation and the Future Gilmore et al
S82 The Journal of Thoracic and Cardiovascular Surgery c September 2012
Sen4nellymphnodewithnear-infraredfluorescentinNSCLC–Bostongroupstudy
Sen4nellymphnodeNear-infraredfluorescentinNSCLC
lower lobe in the residual three injections and from theleft lower lobe in 2 animals (Table 3). This highlights thevariability of lymphatic mapping in the lung, with asignificant number of SLN being located within the N2mediastinal stations and skipping traditional N1 nodes“nearest” the tumor.
Comment
In this preclinical study, we demonstrate feasibility ofNIR fluorescence-guided SLN mapping using the clin-ically available fluorophore ICG. Previously, we haveshown the utility of NIR quantum dots for intraopera-tive SLN mapping of the lung and pleura in swine [21,22]. Unfortunately, quantum dot fluorophores are cur-rently not approved for human use and, given the
concern of heavy metal content, will not be approvedin the near future. Direct identification of SLN withICG alone requires a large dose of ICG that carries arisk of anaphylaxis and may lead to diffuse greenstaining and distortion of the surgical field [19, 20]. Lowdoses of ICG bound to plasma proteins enhance fluo-rescence intensity of ICG, and allow NIR detectionwith light-emitting diode– based excitation light in asafe environment without the use of lasers, withoutradiation risk, and without distortion of the surgicalfield. Using a large-animal model, the current studydemonstrates that NIR fluorescence imaging with ICGis an effective, simple, and rapid method for SLNmapping in the lung. Furthermore, a dramatic en-hancement of ICG fluorescence is seen when boundwith plasma proteins, resulting in protein concentra-
Color NIR Fluorescence Color-NIR Merge
3 m
in
post
-inje
c!on
D
isse
cted
SLN
1 cm Inj
*
0.5 cm
Fig 4. In vivo and ex vivo identification of the sentinel lymph node (SLN) using 250 !M indocyanine green (ICG):porcine plasma (PL). Thetop row demonstrates in vivo near-infrared (NIR) imaging of the injection site, lymphatic migration, and SLN identification. After resection ofthe SLN, bottom row, ex vivo NIR fluorescence imaging confirms uptake of ICG within the lymph nodes. Arrow indicates primary SLN; ar-rowhead indicates bronchus, and asterisk (*) indicates secondary lymph node.
Fig 5. Dose-dependent increase in signal-to-background (SBR) and signal-to-bronchus ra-tio (SBrR): After in vivo injection of 200 !L of125 !M or 250 !M bound to porcine plasma,the SBR and SBrR were calculated. There is adose-dependent increase in both (A) SBR and(B) SBrR when compared with the 10 !Mdose.
316 KHULLAR ET AL Ann Thorac SurgSENTINEL LYMPH NODE MAPPING IN PORCINE LUNG 2013;95:312–8
GEN
ERA
LT
HO
RA
CIC
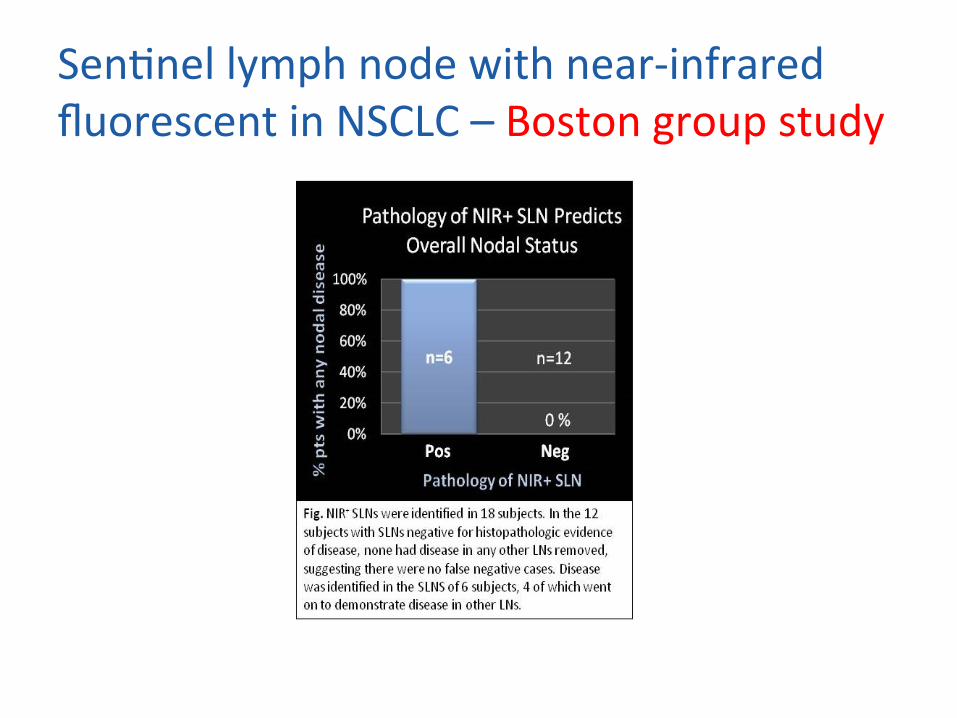
Sen4nellymphnodewithnear-infraredfluorescentinNSCLC–Bostongroupstudy
DrainagepleuralCombiendedrain?…1
TohokuJExpMed.2014;232(1):55-61.Postopera<vedrainagewithonechesttubeisappropriateforpulmonarylobectomy:arandomizedtrial.TanakaM,SagawaM,UsudaK,MachidaY,UenoM,MotonoN,SakumaT.Toexpandpostopera4veresiduallungsagerpulmonarylobectomy,thoracicdrainagewithtwochesttubeshasbeenrecommended.Severalstudiesrecentlydemonstratedthatpostopera4vedrainagewithonechesttube(PD1)wasassafeasthatwithtwochesttubes(PD2).However,mostofthepa4entsinthosestudiesunderwentlobectomybystandardthoracotomy.Althoughthenumberofpulmonarylobectomiesbyvideo-assistedthoracicsurgery(VATS)hasbeenincreasinginrecentyears,therehavebeennoreportsthatcomparedPD1withPD2agerpulmonarylobectomy,includingthatbyVATS.Toelucidatewhetherpostopera4vemanagementwithPD1isassafeasthatwithPD2,weconductedarandomizedcontrolledtrial.
Inconclusion,sincePD1hasadvantagesinsavingcostand<meandinlowriskoftranscutaneousinfec<on,PD1isappropriatea`erpulmonarylobectomybyVATSandbyopenthoracotomy.
DrainagepleuralOnl’enlèvequand?EurJCardiothoracSurg.2014Feb;45(2):241-6.Earlychesttuberemovala`ervideo-assistedthoracicsurgerylobectomywithserousfluidproduc<onupto500ml/day.BjerregaardLS,JensenK,PetersenRH,HansenHJ.Infast-trackpulmonaryresec4ons,weremovedchesttubesagervideo-assistedthoracicsurgery(VATS)lobectomywithserousfluidproduc4onupto500ml/day.Subsequently,weevaluatedthefrequencyofrecurrentpleuraleffusionsrequiringreinterven4on.Datafrom622consecu4vepa4entsundergoingVATSlobectomyfromJanuary2009toDecember2011wereregisteredprospec4velyinanins4tu4onaldatabase.Dataincludedage,gender,lobe(s)resected,bleedinganddura4onofsurgery.Follow-upwas30daysfromdischarge.Allcomplica4onsrequiringpleurocentesisorreinser4onofachesttube,andallreadmissionswereregistered.Twenty-threepa4entswereexcludedduetomissingdata,in-hospitalmortalityandlosstofollow-up,leaving599forfinalanalysis.Ourprimaryoutcomewasthenumberofpa4entsrequiringreinterven4onduetorecurrentpleuraleffusion.Secondaryoutcomesincluded4meofchesttuberemovaland4metodischarge.Theincidenceofrecurrentpleuraleffusionsrequiringreinterven4onwascomparedbetweenthreegroupsaccordingtothepostopera4veday(POD)ofchesttuberemoval(Day0-1,2-3and≥4,respec4vely)usingFisher'sexacttest.
Ourfindingssuggestthatchesttuberemovala`erVATSlobectomyissafedespitevolumesofserousfluidproduc<onupto500ml/day.Thepropor4onofpa4entswhodevelopedpleuraleffusionnecessita4ngreinterven4onwaslow(2.8%),andacomplica4onofthereinterven4onwasseeninonly1pa4ent.
DrainagepleuralCombiendedrain?…ZERO
EurJCardiothoracSurg.2013Aug;44(2):225-9;discussion229.Omiingchesttubedrainagea`erthoracoscopicmajorlungresec<on.UedaK,HayashiM,TanakaT,HamanoK.Absorbablemeshandfibringlueappliedtopreventalveolarairleakagecontributetoreducingthelengthofchesttubedrainage,lengthofhospitaliza4onandtherateofpulmonarycomplica4ons.Thisstudyinves4gatedthefeasibilityofomi�ngchesttubedrainageinselectedpa4entsundergoingthoracoscopicmajorlungresec4on.Intraopera4veairleakagesweresealedwithfibringlueandabsorbablemeshinpa4entsundergoingthoracoscopicmajorlungresec4on.Thechesttubewasremovedjustagertrachealextuba4onifnoairleakagesweredetectedinasuc4on-inducedairleakagetest,whichisanoriginaltechniquetoconfirmpneumostasis.Pa4entswithbleedingtendencyorextensivethoracicadhesionswereexcluded.
Therefinedstrategyforpneumostasisallowedtheomissionofchesttubedrainageinthemajorityofpa<entsundergoingthoracoscopicmajorlungresec<onwithoutincreasingtheriskofadverseevents,whichmaycontributetoafast-tracksurgery.
AnesthésiePériduraleoublocparavertébral,c’estu4le?
JCardiothoracVascAnesth.2012Feb;26(1):78-82.Thoracicepiduralorparavertebralcatheterforanalgesiaa`erlungresec<on:istheoutcomedifferent?ElsayedH,McKevithJ,McShaneJ,ScawnN.Theaimofthisstudywastodeterminewhetherthoracicepiduralanalgesia(TEA)oraparavertebralcatheterblock(PVB)withmorphinepa4ent-controlledanalgesiainfluencedoutcomeinpa4entsundergoingthoracotomyforlungresec4on.Thestudypopula4onconsistedof1,592pa4entswhohadundergonethoracotomyforlungresec4onbetweenMay2000andApril2008.
Paravertebralcatheteranalgesiawithmorphinepa<ent-controlledanalgesiaseemsaseffec<veasthoracicepiduralforreducingtheriskofpostopera<vecomplica<ons.Theauthorsaddi<onallyfoundthatparavertebralcatheteruseisassociatedwithashorterhospitalstayandmaybeabePerformofanalgesiaforfast-trackthoracicsurgery.
FasttrackinthoracicsurgeryRapportd’expérience…EurJCardiothoracSurg.2009Aug;36(2):383-91;discussion391-2.Fast-trackrehabilita<onforlungcancerlobectomy:afive-yearexperience.Das-Neves-PereiraJC,BaganP,Coimbra-IsraelAP,Grimaillof-JuniorA,Cesar-LopezG,Milanez-de-CamposJR,RiquetM,Biscegli-JateneF.Fast-trackrehabilita4onisagroupofsimplemeasuresthatreducesmorbidity,postopera4vecomplica4onandacceleratespostopera4verehabilita4onreducinghospitalstay.Itcanbeappliedtolungcancerlobectomy.Fast-trackrehabilita4oncornerstonesare:minimallyinvasivesurgicaltechniquesusingvideo-assistedandmusclesparringincisions,normovolemia,normothermia,goodoxygena4on,euglicemia,nounnecessaryan4bio4cs,epiduralpa4ent-controlledanalgesia,systemicopiods-freeanalgesia,earlyambula4onandoralfeeding.Ourobjec4veistodescribeafive-yearexperiencewithfast-trackrehabilita4onAretrospec4venon-controlledstudyincluding109consecu4vepa4entssubmihedtofast-trackrehabilita4oninthepostopera4vecareoflungcancerlobectomywasperformed.Onlycollabora4vepa4entswhocouldreceivedouble-lumenintuba4on,epiduralcatheterswithpa4ent-controlledanalgesia,whohadKarnofskyindexof100,previousnormalfeedingandambula4on,absenceofmorbidobesity,diabetesorasthma,wereeligible.Postopera4veoralfeedingandaggressiveambula4onstartedassoonaspossible.
Fast-trackrehabilita<onforlungcancerlobectomiescanbesafelyperformedinaselectedgroupofpa<entsifamo<vatedmul<disciplinarygroupofprofessionalsisavailableandseemstoreducepostopera<vecomplica<onandhospitalstay.

I4néraireUnpa4entdansunmouvementdèslepremiercontact…
CMOinterven4onchirurgicale
Bilanpréopératoire
Interven4onchirurgicale
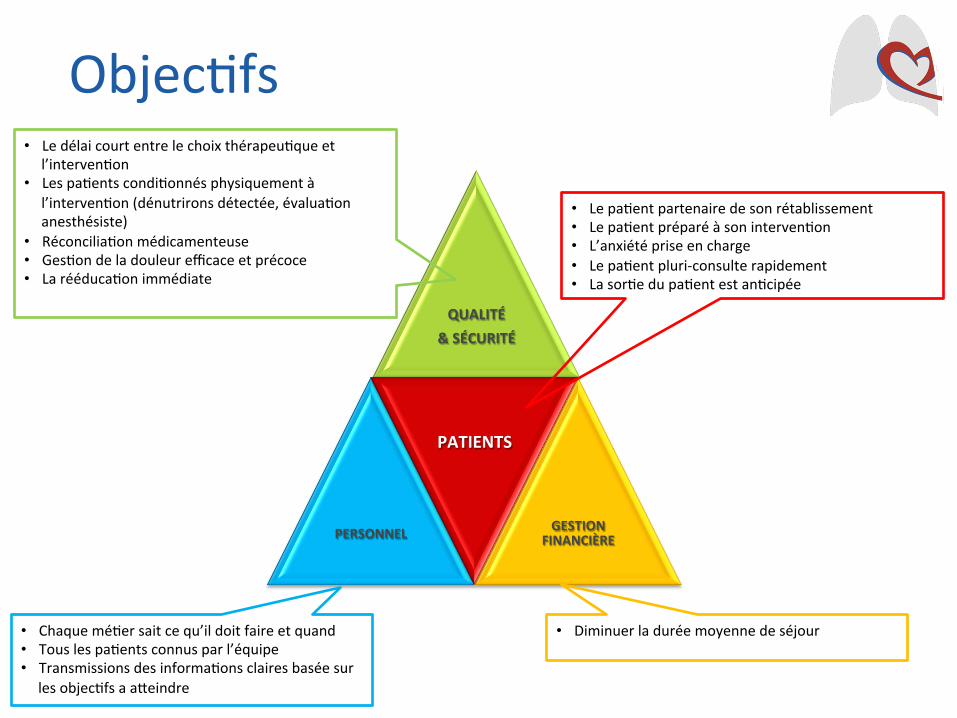
Objec4fs
QUALITÉ&SÉCURITÉ
PERSONNEL
PATIENTS
GESTIONFINANCIÈRE
• Lepa4entpartenairedesonrétablissement• Lepa4entpréparéàsoninterven4on• L’anxiétépriseencharge• Lepa4entpluri-consulterapidement• Lasor4edupa4entestan4cipée
• Ledélaicourtentrelechoixthérapeu4queetl’interven4on
• Lespa4entscondi4onnésphysiquementàl’interven4on(dénutrironsdétectée,évalua4onanesthésiste)
• Réconcilia4onmédicamenteuse• Ges4ondeladouleurefficaceetprécoce• Larééduca4onimmédiate
• Chaquemé4ersaitcequ’ildoitfaireetquand• Touslespa4entsconnusparl’équipe• Transmissionsdesinforma4onsclairesbaséesur
lesobjec4fsaaheindre
• Diminuerladuréemoyennedeséjour
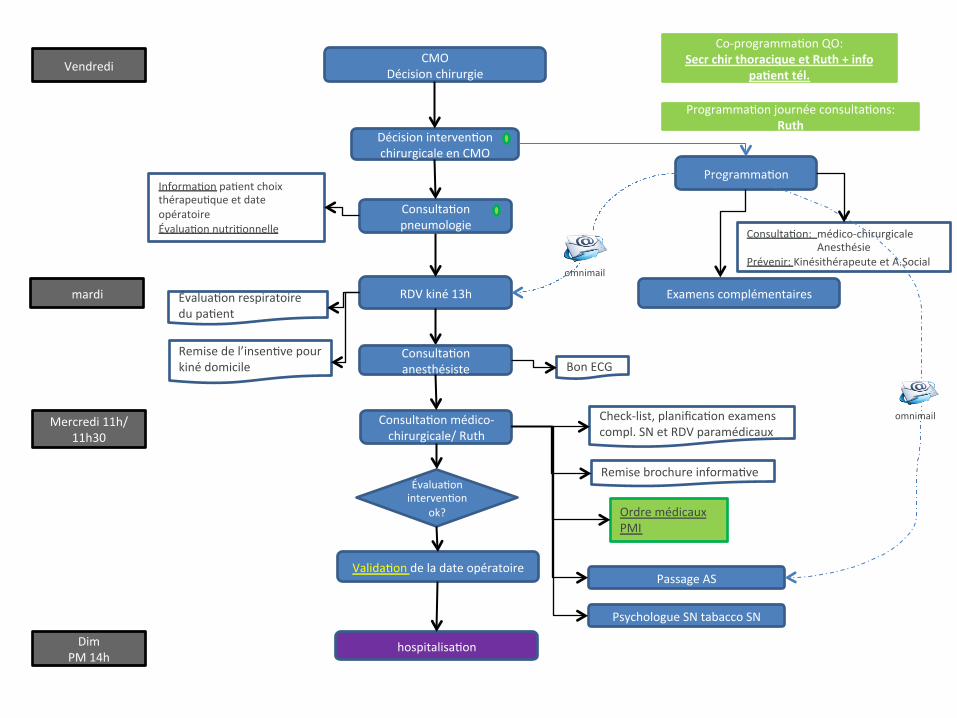
Consulta4onmédico-chirurgicale/Ruth
Check-list,planifica4onexamenscompl.SNetRDVparamédicaux
Décisioninterven4onchirurgicaleenCMO
Vendredi
Programma4on
ExamenscomplémentairesRDVkiné13hÉvalua4onrespiratoiredupa4ent
Remisedel’insen4vepourkinédomicile
Valida4ondeladateopératoire
DimPM14h
hospitalisa4on
Consulta4on:médico-chirurgicaleAnesthésiePrévenir:KinésithérapeuteetA.Social
Remisebrochureinforma4ve
CMODécisionchirurgie
Programma4onjournéeconsulta4ons:Ruth
Co-programma4onQO:SecrchirthoraciqueetRuth+info
pa<enttél.
Consulta4onanesthésiste
PsychologueSNtabaccoSN
mardi
Mercredi11h/11h30
PassageAS
BonECG
Consulta4onpneumologie
Informa4onpa4entchoixthérapeu4queetdateopératoireÉvalua4onnutri4onnelle
omnimail
OrdremédicauxPMI
Évalua4oninterven4on
ok?
omnimail
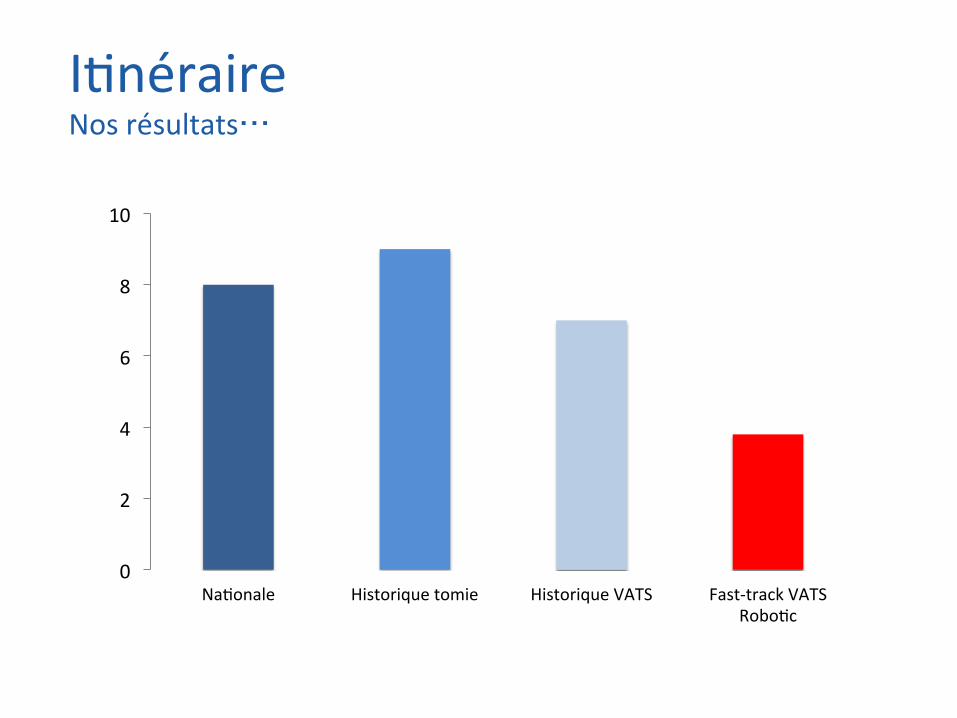
0
2
4
6
8
10
Na4onale Historiquetomie HistoriqueVATS Fast-trackVATSRobo4c
I4néraireNosrésultats…

Conclusions
• Lefastrackestunesurlacons4tu4ondeparcourtdesoinsbaséssurl’evidencebasemedicinequiréduitlestressphysiqueetpsychiqueliéàl'interven4on.
• C’estunevisionintégréeetinterdisciplinairedelapriseenchargedupa4ent.
• Cehedémarchediminueladuréeduséjourhospitalier,lescoûtsgénérauxetpourraitraisonnablementavoirunimpactsurlamorbi-mortalité(cfchirurgiediges4veetcardiaque).

Conclusions
• L’avenirdelaChirurgieThoraciqueestdoncl’intégra4ondesdifférentsmé4ersdansdesmissionscommunesdéfiniesautouretaveclepa4entpourchaquepathologie.
• L’organisa4ondeshôpitauxdoitêtrerevuefondamentalementetorganiséeen“trajetsdesoins”plutôtqu’enservicesmédicauxetparamédicaux.

Entransplanta4onpulmonaire,onpeutencoreavancer?

Theshortageofdonorlungs
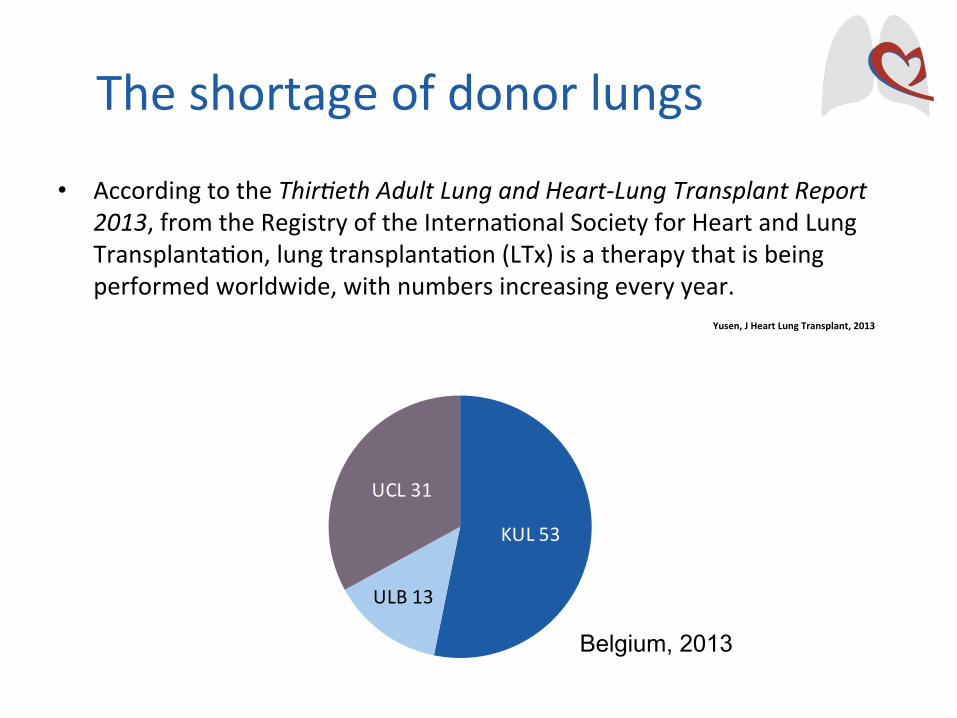
• AccordingtotheThir:ethAdultLungandHeart-LungTransplantReport2013,fromtheRegistryoftheInterna4onalSocietyforHeartandLungTransplanta4on,lungtransplanta4on(LTx)isatherapythatisbeingperformedworldwide,withnumbersincreasingeveryyear.
5 7 38 89204
450
758970
11601289
1412 13891510 1547 1559
1700 17841974 2012
2218
2569
27942920 2981
3278
3519
0
500
1000
1500
2000
2500
3000
3500
4000
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
Num
ber o
f Tra
nspl
ants
Bilateral/DoubleLung
SingleLung
Yusen,JHeartLungTransplant,2013
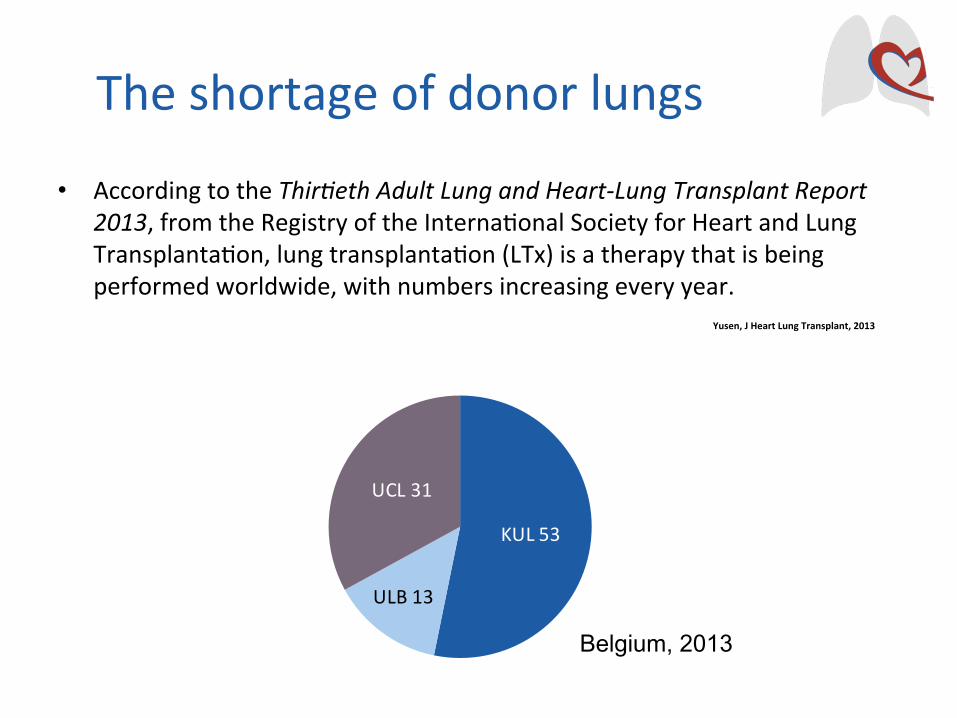
KUL53
ULB13
UCL31
Theshortageofdonorlungs
Belgium, 2013
• AccordingtotheThir:ethAdultLungandHeart-LungTransplantReport2013,fromtheRegistryoftheInterna4onalSocietyforHeartandLungTransplanta4on,lungtransplanta4on(LTx)isatherapythatisbeingperformedworldwide,withnumbersincreasingeveryyear.
Yusen,JHeartLungTransplant,2013
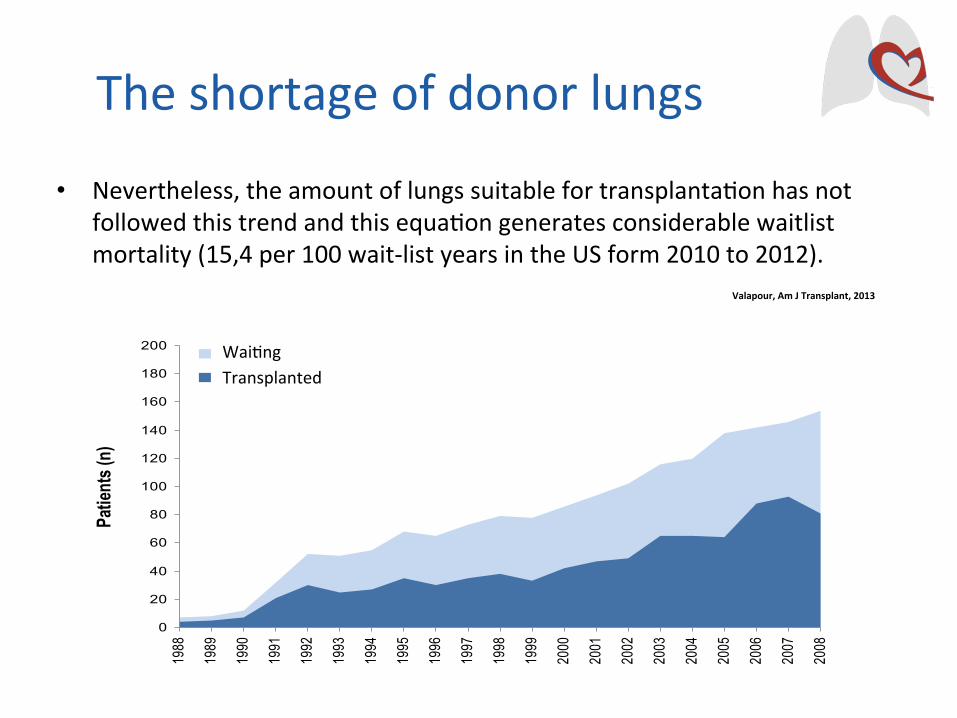
• Nevertheless,theamountoflungssuitablefortransplanta4onhasnotfollowedthistrendandthisequa4ongeneratesconsiderablewaitlistmortality(15,4per100wait-listyearsintheUSform2010to2012).
Theshortageofdonorlungs
0
20
40
60
80
100
120
140
160
180
200
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
Patie
nts (
n)
En attente(n)Transplantés (n)
Wai4ngTransplanted
Valapour,AmJTransplant,2013
0%
20%
40%
60%
80%
100%
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
0
10
20
30
40
50
0-11 12-17 18-34 35-49 50-59 60+ Donor mean age
% o
f tra
nspl
ants
Med
ian
dono
r ag
e (y
ears
)
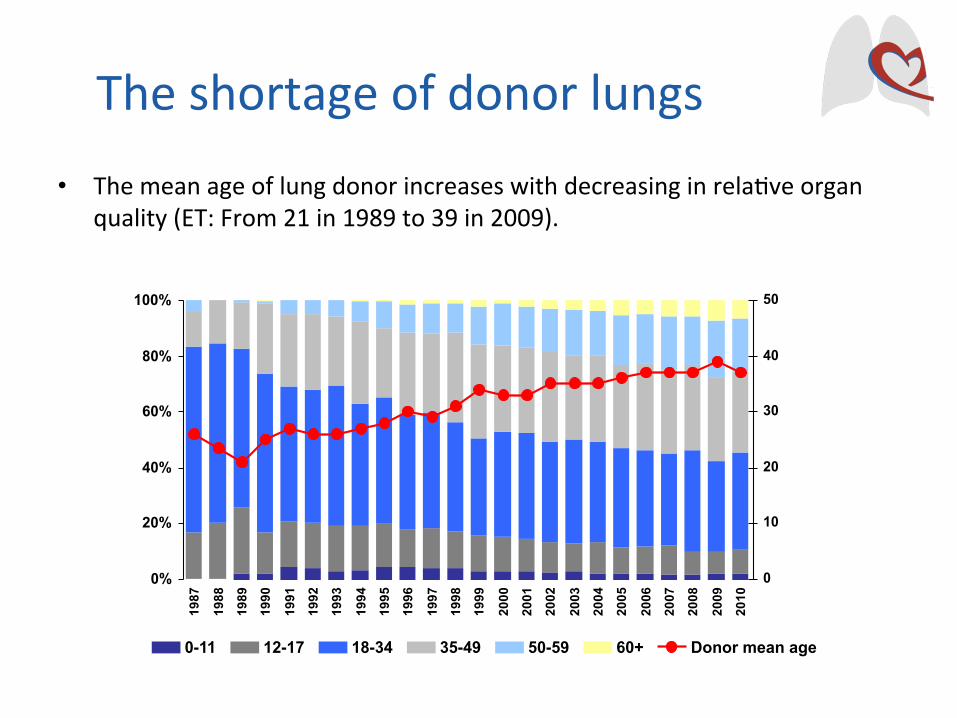
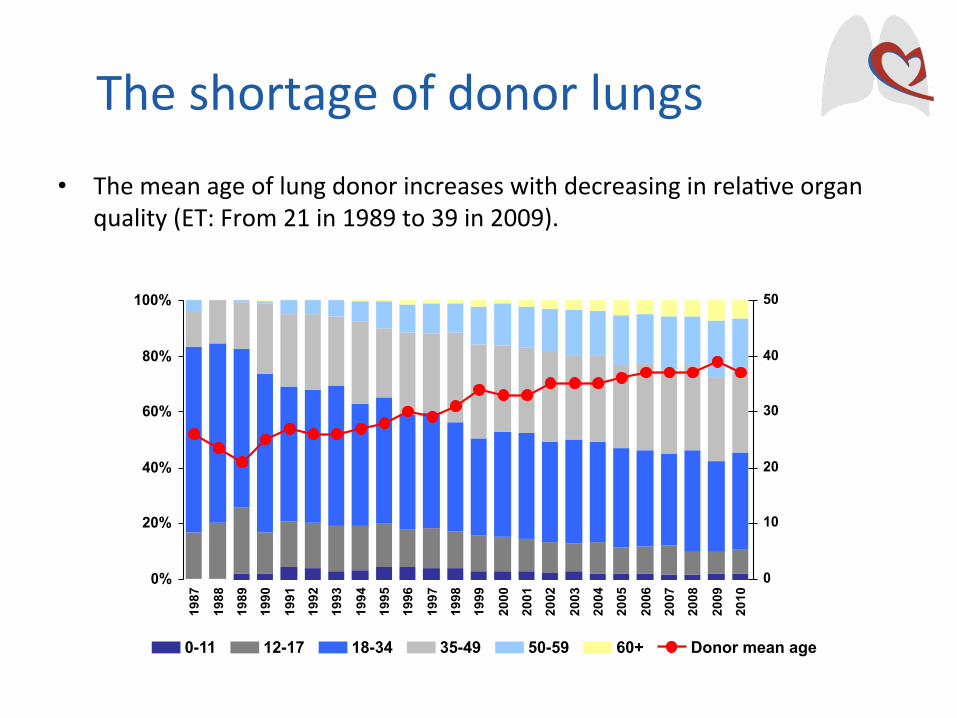
• Themeanageoflungdonorincreaseswithdecreasinginrela4veorganquality(ET:From21in1989to39in2009).
Theshortageofdonorlungs
• Donor lungs are subjected to several injurious mechanisms during the brain death/organ donation process (such as ventilator-acquired pneumonia, neurogenic and hydrostatic pulmonary edema, barotrauma). Thus, it is not surprising that the majority of donor lungs are not utilized for transplantation (39% ET 2012, 22% in the US 2012).
Theshortageofdonorlungs
StrategiesforlungdonorpoolexpansionIdealdonor
• Idealdonor:• <55year-old,• <20pack-yearsmokinghistory,• nochesttrauma,• clearchestX-ray,• centralP/F>300,• absenceofpurulentsecre4onsandorganismsongramstainofrespiratory
samples.
• Thisscenarioisknowntocorrespondtolessthanhalfofthedonorsu4lizedfortransplanta4on.
Pierre,JThoracCardiovascSurg,2002
StrategiesforlungdonorpoolexpansionExtendedcriteriadonor
• Severalstudiesaddressingtheuseofextendedcriteriadonors• Areviewstudysummarizedthefindingsof10studiesrangingfrom1993
to2010,bringingthebestevidenceuptodate.• Althoughnocleardifferencesinmidorlong-termsurvivalwereobserved,4of
thesestudiesrevealedworseearlyoutcomes(suchas30-and90-daymortality,ICUandhospitalstayandgasexchangeatICUarrival).
• Recently,theHannovergrouphasshownaninteres4ngalgorithmproposingalloca4onofextendedcriteriadonorlungstolower-riskrecipients.Resultswereencouraginganddeservefurtheranalysis.
Schiavon,InteractCardiovascThoracSurg,2012
Sommer,JHeartLungTransplant,2013
StrategiesforlungdonorpoolexpansionControlledDCDdonor
• The first successful LTx was performed from DCD (Hardy - 1963) • the concept of using controlled DCD lungs has been clinically
revisited by D’Alessandro in 1995.
• Series of studies have followed, reporting an increasing international experience and highlighting the potential of DCD to partially address the shortage of donor lungs… But…
• Nevertheless, caution is still observed in the transplant community as there are a series of specific injuries that the DCD lung is prone to, specially during the interval from withdrawal of life sustaining therapies to pulmonary artery flush.
D’Alessandro,Transplanta<on,1995
Cypel,JHeartLungTransplant,2009Erasmus,Transplanta<on,2010LoveRB,AmJTransplant,2012Mason,AnnThoracSurg2012
DeOliveira,JThoracCardiovascSurg,2010Levvey,AmJTransplant,2012
Puri,AnnThoracSurg,2009
StrategiesforlungdonorpoolexpansionUncontrolledDCDdonor
• Anotherpoten4alsourceoflungscomesfromtheuseofuncontrolledDCDs(MaastrichtcategoriesIandII).
• ThegroupofMadridhasexploredthispeculiarpool,repor4ngtheexperiencewith29cases.Ninety-dayand1-yearmortalitywere22%and32%respec4vely,withhigherratesofprimarygragdysfunc4on(PGD)2-3thanexpected.
deAntonio,JHeartLungTransplant,2007

StrategiesforlungdonorpoolexpansionExvivolungperfusion
• ClinicalEVLPwasshowntosafelyincreasethedonorpoolbypreservinghigh-riskdonorlungswithsimilaroutcomestostandardcriteriadonorlungs.
CypelM,NEnglJMed,2011
EVLP

EVLP – Philosophies…
• Evaluation – Extending donor pool • Improving quality – Reconditionning • Prolong perfusion and/or transport time • Research
EVLP – Philosophies…
• Evaluation – Extending donor pool • Improving quality – Reconditionning • Prolong perfusion and/or transport time • Research
EVLP Evaluation – Extending donor pool
• Evaluation of poor prognostic donor… • DCD donor • Circulatory death • Extending criteria donor • Hanging victim • Infected or suspicion of infection
• Evaluation of in vivo inevaluable donor… • Maastricht 2 • High-pressure pneumoplegia • ECMO
• Evaluation for prognosing… • Perfusate protein expression during EVLP can differentiate lungs with good
outcome from lungs PGD3 after transplantation.
Elgharably,ThoracSurgClin,2015
Bozso,CanRespirJ,2014
Machuca,AnnSurg.2014
Bozso,TransplInt,2014
BenneP,AnnThoracSurg,2014
Suzuki,AmJTransplant,2014
Boffini,TransplInt,2014
Pa<l,JThoracCardiovascSurg,2014
GarcíaSáez,EurJCardiothoracSurg,2014
EVLP Evaluation – Extending donor pool
Transplant Proc. 2013 Sep;45(7):2624-6.
Ex vivo lung perfusion increases the pool of lung grafts: analysis of its potential and real impact on a lung transplant program. Boffini, Ricci, Barbero, Bonato, Ribezzo, Mancuso, Attisani, Simonato, Magistroni, Mansouri, Solidoro, Baldi, Pasero, Amoroso, Rinaldi.
BACKGROUND: Among the strategies to increase the number of lung transplants, ex vivo lung perfusion (EVLP) represents a novel technique to expand the donor pool. METHODS: Data from donors referred to our center were retrospectively analyzed to identify grafts that could potentially be potentially reconditioned by EVLP and for comparison with those obtained by clinical application of EVLP program in our center. RESULTS: Among 75 rejected lungs, 23 organs have been identified as potentially treatable with EVLP with a hypothetic increase of lung transplant activity of 53%. After the introduction of the EVLP program in our center, lung transplantation with reconditioned grafts was performed in 7 (23%) patients with a 30% increase in transplant procedures. CONCLUSION: Although less than expected, EVLP increased the number of lungs suitable for transplantation.

EVLP – Philosophies…
• Evaluation – Extending donor pool • Improving quality – Reconditionning • Prolong perfusion and/or transport time • Research

EVLP Improving quality – Reconditioning
• Improve function… • EVLP alone • Plasmin administration • Hydrogen preconditioning
• Treating… • Aspiration with intrabronchial surfactant instillation • Acute pulmonary embolism with urokinase • Reducing microbial load by high-dose empirical AB • Inflammation by mechanical removal of dendritic cell-generating non-classical monocytes
• Surgical act… • LVRS - Lobectomy
Cypel,ThoracSurgClin,2015
Motoyama,JHeartLungTransplant,2014
Noda,Transplanta<on,2014
Inci,JSurgRes,2013
Inci,AnnThoracSurg,2014
Andreasson,JHeartLungTransplant,2014
Stone,JHeartLungTransplant,2014
Nosoi,TransplantProc,2014

WorldwideexperiencewithclinicalEVLPResults
• Toronto conducted a nonrandomized clinical trial to assess the feasibility of EVLP selecting high-risk donor lungs for this modality of preservation.
• 23 donor lungs were submitted to EVLP, • 20 being ultimately transplanted (15 bilateral/5 unilateral), • PGD grade 2 or 3 at 72 hours: 15% of the EVLP group and 30% of the
contemporary no EVLP controls (116 cases), with no significant difference, • Time on mechanical ventilation, ECLS requirement, ICU stay, hospital stay and
30-day mortality were not different.
• This experience was recently updated… • with a total of 50 lung transplants from 58 EVLPs (86% yield), • PGD 3 at 72 hours was recorded in 2% EVLP vs. 8.5% control (P=0.14), • Again, time on mechanical ventilation, ECLS requirement, ICU stay, hospital stay
and 30-day mortality were not different, • 1-year survivals: 87% for EVLP group vs. 86% for the standard group.
CypelM,NEnglJMed,2011
Cypel,JThoracCardiovascSurg,2012
WorldwideexperiencewithclinicalEVLPResults
• Vienna reported their experience… • 13 clinical EVLPs which rendered 9 double-lung transplants (69% yield), • Early outcomes - days on mechanical ventilation, ICU stay, hospital stay and 30-
day mortality were comparable to 119 contemporary conventional preservation transplants,
• Interestingly, all the four declined cases developed massive pulmonary edema and were recovered from donors with trauma history.
• The groups from Toronto, Vienna and Paris presented their clinical EVLP experience at the 2013 ISHLT meeting.
• A total of 125 clinical EVLPs were performed with an 82.5% yield, • Incidence of PGD3 at 72 hours was 5% and the 12-month mortality was 12%.
Aigner,AmJTransplant,2012
Cypel,JournalofHeartandLungTransplanta<on2013
WorldwideexperiencewithclinicalEVLPResults
• TheNOVELLungtrialisanFDAmandatedmul4centerclinicaltrial(NOVELLungTrial)studyingEVLPformarginaldonors.
• Theini4alreportincluded31pa4entsthatreceivedEVLPlungs.EarlyoutcomessuchasPGD,lengthonmechanicalven4la4on,ICUstay,hospitalstayand30-daymortalityweresimilarto31non-EVLPcontrols.
• Atthe2014ISHLTmee4ng,thetrialresultswereupdatedto76EVLPsrendering42lungtransplants(55%conversionrate).Incomparisonwith42contemporarycontrols,earlyoutcomesand1-yearsurvivalwerenotdifferent.
Sanchez,JHeartLungTransplant,2014
Sanchez,JHeartLungTransplant,2013

EVLP – Philosophies…
• Evaluation – Extending donor pool • Improving quality – Reconditionning • Prolong perfusion and/or transport time • Research

EVLPProlongperfusionand/ortransport4me
Am J Transplant. 2014 Oct;14(10):2412-6.
Combined liver and lung transplantation with extended normothermic lung preservation in a patient with end-stage emphysema complicated by drug-induced acute liver failure. Ceulemans, Monbaliu, Verslype, van der Merwe , Laleman , Vos , Neyrinck, Van Veer, De Leyn , Nevens , Pirenne , Verleden , Van Raemdonck . Isolated lung transplantation (LuTx) and liver transplantation are established treatments for irreversible lung and liver failure. Combined liver and lung transplantation (cLiLuTx) is a less common, but approved therapy of combined organ failure, mostly applied in patients suffering from progressive cystic fibrosis and advanced liver disease. We report a patient who was listed for LuTx due to end-stage chronic obstructive pulmonary disease and who developed drug-induced acute hepatic failure. The only therapeutic option was hyper-urgent cLiLuTx. To correct the poor coagulation in order to reduce the per-operative risk of bleeding, the liver was transplanted first. In anticipation of the longer lung preservation time, cold flushed lungs were preserved on a portable lung perfusion device for ex vivo normothermic perfusion for 11 h 15 min, transplanted sequentially off-pump, and reperfused after a total ex vivo time of 13 h 32 min and 16 h for the first and second lung, respectively. Ten months later, the patient is doing well and no rejection occurred. Normothermic ex vivo lung perfusion may help to prolong preservation time, facilitating long-distance transport and combined organ transplantation..

EVLPProlongperfusionand/ortransport4me
Eur J Cardiothorac Surg. 2014 Mar;45(3):e54-60.
Successful prolonged ex vivo lung perfusion for graft preservation in rats. Noda, Shigemura, Tanaka, Bhama, D'Cunha, Luketich, Bermudez.
Ex vivo lung perfusion (EVLP) strategies represent a new frontier in lung transplantation technology, and there have been many clinical studies of EVLP in lung transplantation. The establishment of a reliable EVLP model in small animals is crucial to facilitating translational research using an EVLP strategy. The main objective of this study was to develop a reproducible rat EVLP (R-EVLP) model that enables prolonged evaluation of the explanted lung during EVLP and successful transplantation after EVLP. The donor heart-lung blocks were procured with cold low-potassium dextran solution and immersed in the solution for 1 h at 4 °C. And then, the heart-lung blocks were flushed retrogradely and warmed up to 37 °C in a circuit perfused antegradely with acellular perfusate. The perfusate was deoxygenated with a gas mixture (6% O2, 8% CO2, 86% N2). The perfusion flow was maintained at 20% of the entire cardiac output. At 37 °C, the lungs were mechanically ventilated and perfusion continued for 4 h. Every hour, the perfused lung was evaluated for gas exchange, dynamic lung compliance (Cdyn) and pulmonary vascular resistance (PVR). R-EVLP was performed for 4 h. Pulmonary oxygenation ability (pO2/pCO2) was stable for 4 h during EVLP. It was noted that Cdyn and PVR were also stable. After 4 h of EVLP,

EVLP – Philosophies…
• Evaluation – Extending donor pool • Improving quality – Reconditionning • Prolong perfusion and/or transport time • Research
EVLPResearch
World J Exp Med. 2014 May 20;4(2):7-15.
Animal models of ex vivo lung perfusion as a platform for transplantation research. Nelson, Bobba, Ghadiali, Hayes, Black, Whitson. Ex vivo lung perfusion (EVLP) is a powerful experimental model for isolated lung research. EVLP allows for the lungs to be manipulated and characterized in an external environment so that the effect of specific ventilation/perfusion variables can be studied independent of other confounding physiologic contributions. At the same time, EVLP allows for normal organ level function and real-time monitoring of pulmonary physiology and mechanics. As a result, this technique provides unique advantages over in vivo and in vitro models. Small and large animal models of EVLP have been developed and each of these models has their strengths and weaknesses. In this manuscript, we provide insight into the relative strengths of each model and describe how the development of advanced EVLP protocols is leading to a novel experimental platform that can be used to answer critical questions in pulmonary physiology and transplant medicine.
• The use of EVLP… • allows an objective assessment of high-risk donor lungs. • autorize treatment, reconditionning of suposed non-transplantable
lungs. • permits when these lungs are transplanted, acceptable rates of primary
graft dysfunction, with an early and mid-term outcomes similar to those with conventionally selected and transplanted lungs.
• permits to explore new source of donors (DCD donor, circulatory death, extending criteria donor, hanging victim, infected organs, ECMO…).
• help to prolong preservation time, facilitating long-distance transport and combined organ transplantation.
• leads to experimental platform that can be used to answer questions in pulmonary physiology and transplant medicine.
Conclusions

Theshortageofdonorlungs
• AccordingtotheThir:ethAdultLungandHeart-LungTransplantReport2013,fromtheRegistryoftheInterna4onalSocietyforHeartandLungTransplanta4on,lungtransplanta4on(LTx)isatherapythatisbeingperformedworldwide,withnumbersincreasingeveryyear.
5 7 38 89204
450
758970
11601289
1412 13891510 1547 1559
1700 17841974 2012
2218
2569
27942920 2981
3278
3519
0
500
1000
1500
2000
2500
3000
3500
4000
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
Num
ber o
f Tra
nspl
ants
Bilateral/DoubleLung
SingleLung
Yusen,JHeartLungTransplant,2013
KUL53
ULB13
UCL31
Theshortageofdonorlungs
Belgium, 2013
• AccordingtotheThir:ethAdultLungandHeart-LungTransplantReport2013,fromtheRegistryoftheInterna4onalSocietyforHeartandLungTransplanta4on,lungtransplanta4on(LTx)isatherapythatisbeingperformedworldwide,withnumbersincreasingeveryyear.
Yusen,JHeartLungTransplant,2013

• Nevertheless,theamountoflungssuitablefortransplanta4onhasnotfollowedthistrendandthisequa4ongeneratesconsiderablewaitlistmortality(15,4per100wait-listyearsintheUSform2010to2012).
Theshortageofdonorlungs
0
20
40
60
80
100
120
140
160
180
200
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
Patie
nts (
n)
En attente(n)Transplantés (n)
Wai4ngTransplanted
Valapour,AmJTransplant,2013
0%
20%
40%
60%
80%
100%
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
0
10
20
30
40
50
0-11 12-17 18-34 35-49 50-59 60+ Donor mean age
% o
f tra
nspl
ants
Med
ian
dono
r ag
e (y
ears
)
• Themeanageoflungdonorincreaseswithdecreasinginrela4veorganquality(ET:From21in1989to39in2009).
Theshortageofdonorlungs
• Donor lungs are subjected to several injurious mechanisms during the brain death/organ donation process (such as ventilator-acquired pneumonia, neurogenic and hydrostatic pulmonary edema, barotrauma). Thus, it is not surprising that the majority of donor lungs are not utilized for transplantation (39% ET 2012, 22% in the US 2012).
Theshortageofdonorlungs

StrategiesforlungdonorpoolexpansionIdealdonor
• Idealdonor:• <55year-old,• <20pack-yearsmokinghistory,• nochesttrauma,• clearchestX-ray,• centralP/F>300,• absenceofpurulentsecre4onsandorganismsongramstainofrespiratory
samples.
• Thisscenarioisknowntocorrespondtolessthanhalfofthedonorsu4lizedfortransplanta4on.
Pierre,JThoracCardiovascSurg,2002

StrategiesforlungdonorpoolexpansionExtendedcriteriadonor
• Severalstudiesaddressingtheuseofextendedcriteriadonors• Areviewstudysummarizedthefindingsof10studiesrangingfrom1993
to2010,bringingthebestevidenceuptodate.• Althoughnocleardifferencesinmidorlong-termsurvivalwereobserved,4of
thesestudiesrevealedworseearlyoutcomes(suchas30-and90-daymortality,ICUandhospitalstayandgasexchangeatICUarrival).
• Recently,theHannovergrouphasshownaninteres4ngalgorithmproposingalloca4onofextendedcriteriadonorlungstolower-riskrecipients.Resultswereencouraginganddeservefurtheranalysis.
Schiavon,InteractCardiovascThoracSurg,2012
Sommer,JHeartLungTransplant,2013
StrategiesforlungdonorpoolexpansionControlledDCDdonor
• The first successful LTx was performed from DCD (Hardy - 1963) • the concept of using controlled DCD lungs has been clinically
revisited by D’Alessandro in 1995.
• Series of studies have followed, reporting an increasing international experience and highlighting the potential of DCD to partially address the shortage of donor lungs… But…
• Nevertheless, caution is still observed in the transplant community as there are a series of specific injuries that the DCD lung is prone to, specially during the interval from withdrawal of life sustaining therapies to pulmonary artery flush.
D’Alessandro,Transplanta<on,1995
Cypel,JHeartLungTransplant,2009Erasmus,Transplanta<on,2010LoveRB,AmJTransplant,2012Mason,AnnThoracSurg2012
DeOliveira,JThoracCardiovascSurg,2010Levvey,AmJTransplant,2012
Puri,AnnThoracSurg,2009

StrategiesforlungdonorpoolexpansionUncontrolledDCDdonor
• Anotherpoten4alsourceoflungscomesfromtheuseofuncontrolledDCDs(MaastrichtcategoriesIandII).
• ThegroupofMadridhasexploredthispeculiarpool,repor4ngtheexperiencewith29cases.Ninety-dayand1-yearmortalitywere22%and32%respec4vely,withhigherratesofprimarygragdysfunc4on(PGD)2-3thanexpected.
deAntonio,JHeartLungTransplant,2007
StrategiesforlungdonorpoolexpansionExvivolungperfusion
• ClinicalEVLPwasshowntosafelyincreasethedonorpoolbypreservinghigh-riskdonorlungswithsimilaroutcomestostandardcriteriadonorlungs.
CypelM,NEnglJMed,2011

EVLP
EVLP – Philosophies…
• Evaluation – Extending donor pool • Improving quality – Reconditionning • Prolong perfusion and/or transport time • Research

EVLP – Philosophies…
• Evaluation – Extending donor pool • Improving quality – Reconditionning • Prolong perfusion and/or transport time • Research

EVLP Evaluation – Extending donor pool
• Evaluation of poor prognostic donor… • DCD donor • Circulatory death • Extending criteria donor • Hanging victim • Infected or suspicion of infection
• Evaluation of in vivo inevaluable donor… • Maastricht 2 • High-pressure pneumoplegia • ECMO
• Evaluation for prognosing… • Perfusate protein expression during EVLP can differentiate lungs with good
outcome from lungs PGD3 after transplantation.
Elgharably,ThoracSurgClin,2015
Bozso,CanRespirJ,2014
Machuca,AnnSurg.2014
Bozso,TransplInt,2014
BenneP,AnnThoracSurg,2014
Suzuki,AmJTransplant,2014
Boffini,TransplInt,2014
Pa<l,JThoracCardiovascSurg,2014
GarcíaSáez,EurJCardiothoracSurg,2014
EVLP Evaluation – Extending donor pool
Transplant Proc. 2013 Sep;45(7):2624-6.
Ex vivo lung perfusion increases the pool of lung grafts: analysis of its potential and real impact on a lung transplant program. Boffini, Ricci, Barbero, Bonato, Ribezzo, Mancuso, Attisani, Simonato, Magistroni, Mansouri, Solidoro, Baldi, Pasero, Amoroso, Rinaldi.
BACKGROUND: Among the strategies to increase the number of lung transplants, ex vivo lung perfusion (EVLP) represents a novel technique to expand the donor pool. METHODS: Data from donors referred to our center were retrospectively analyzed to identify grafts that could potentially be potentially reconditioned by EVLP and for comparison with those obtained by clinical application of EVLP program in our center. RESULTS: Among 75 rejected lungs, 23 organs have been identified as potentially treatable with EVLP with a hypothetic increase of lung transplant activity of 53%. After the introduction of the EVLP program in our center, lung transplantation with reconditioned grafts was performed in 7 (23%) patients with a 30% increase in transplant procedures. CONCLUSION: Although less than expected, EVLP increased the number of lungs suitable for transplantation.

EVLP – Philosophies…
• Evaluation – Extending donor pool • Improving quality – Reconditionning • Prolong perfusion and/or transport time • Research
EVLP Improving quality – Reconditioning
• Improve function… • EVLP alone • Plasmin administration • Hydrogen preconditioning
• Treating… • Aspiration with intrabronchial surfactant instillation • Acute pulmonary embolism with urokinase • Reducing microbial load by high-dose empirical AB • Inflammation by mechanical removal of dendritic cell-generating non-classical monocytes
• Surgical act… • LVRS - Lobectomy
Cypel,ThoracSurgClin,2015
Motoyama,JHeartLungTransplant,2014
Noda,Transplanta<on,2014
Inci,JSurgRes,2013
Inci,AnnThoracSurg,2014
Andreasson,JHeartLungTransplant,2014
Stone,JHeartLungTransplant,2014
Nosoi,TransplantProc,2014
WorldwideexperiencewithclinicalEVLPResults
• Toronto conducted a nonrandomized clinical trial to assess the feasibility of EVLP selecting high-risk donor lungs for this modality of preservation.
• 23 donor lungs were submitted to EVLP, • 20 being ultimately transplanted (15 bilateral/5 unilateral), • PGD grade 2 or 3 at 72 hours: 15% of the EVLP group and 30% of the
contemporary no EVLP controls (116 cases), with no significant difference, • Time on mechanical ventilation, ECLS requirement, ICU stay, hospital stay and
30-day mortality were not different.
• This experience was recently updated… • with a total of 50 lung transplants from 58 EVLPs (86% yield), • PGD 3 at 72 hours was recorded in 2% EVLP vs. 8.5% control (P=0.14), • Again, time on mechanical ventilation, ECLS requirement, ICU stay, hospital stay
and 30-day mortality were not different, • 1-year survivals: 87% for EVLP group vs. 86% for the standard group.
CypelM,NEnglJMed,2011
Cypel,JThoracCardiovascSurg,2012
WorldwideexperiencewithclinicalEVLPResults
• Vienna reported their experience… • 13 clinical EVLPs which rendered 9 double-lung transplants (69% yield), • Early outcomes - days on mechanical ventilation, ICU stay, hospital stay and 30-
day mortality were comparable to 119 contemporary conventional preservation transplants,
• Interestingly, all the four declined cases developed massive pulmonary edema and were recovered from donors with trauma history.
• The groups from Toronto, Vienna and Paris presented their clinical EVLP experience at the 2013 ISHLT meeting.
• A total of 125 clinical EVLPs were performed with an 82.5% yield, • Incidence of PGD3 at 72 hours was 5% and the 12-month mortality was 12%.
Aigner,AmJTransplant,2012
Cypel,JournalofHeartandLungTransplanta<on2013

WorldwideexperiencewithclinicalEVLPResults
• TheNOVELLungtrialisanFDAmandatedmul4centerclinicaltrial(NOVELLungTrial)studyingEVLPformarginaldonors.
• Theini4alreportincluded31pa4entsthatreceivedEVLPlungs.EarlyoutcomessuchasPGD,lengthonmechanicalven4la4on,ICUstay,hospitalstayand30-daymortalityweresimilarto31non-EVLPcontrols.
• Atthe2014ISHLTmee4ng,thetrialresultswereupdatedto76EVLPsrendering42lungtransplants(55%conversionrate).Incomparisonwith42contemporarycontrols,earlyoutcomesand1-yearsurvivalwerenotdifferent.
Sanchez,JHeartLungTransplant,2014
Sanchez,JHeartLungTransplant,2013

EVLP – Philosophies…
• Evaluation – Extending donor pool • Improving quality – Reconditionning • Prolong perfusion and/or transport time • Research

EVLPProlongperfusionand/ortransport4me
Am J Transplant. 2014 Oct;14(10):2412-6.
Combined liver and lung transplantation with extended normothermic lung preservation in a patient with end-stage emphysema complicated by drug-induced acute liver failure. Ceulemans, Monbaliu, Verslype, van der Merwe , Laleman , Vos , Neyrinck, Van Veer, De Leyn , Nevens , Pirenne , Verleden , Van Raemdonck . Isolated lung transplantation (LuTx) and liver transplantation are established treatments for irreversible lung and liver failure. Combined liver and lung transplantation (cLiLuTx) is a less common, but approved therapy of combined organ failure, mostly applied in patients suffering from progressive cystic fibrosis and advanced liver disease. We report a patient who was listed for LuTx due to end-stage chronic obstructive pulmonary disease and who developed drug-induced acute hepatic failure. The only therapeutic option was hyper-urgent cLiLuTx. To correct the poor coagulation in order to reduce the per-operative risk of bleeding, the liver was transplanted first. In anticipation of the longer lung preservation time, cold flushed lungs were preserved on a portable lung perfusion device for ex vivo normothermic perfusion for 11 h 15 min, transplanted sequentially off-pump, and reperfused after a total ex vivo time of 13 h 32 min and 16 h for the first and second lung, respectively. Ten months later, the patient is doing well and no rejection occurred. Normothermic ex vivo lung perfusion may help to prolong preservation time, facilitating long-distance transport and combined organ transplantation..

EVLPProlongperfusionand/ortransport4me
Eur J Cardiothorac Surg. 2014 Mar;45(3):e54-60.
Successful prolonged ex vivo lung perfusion for graft preservation in rats. Noda, Shigemura, Tanaka, Bhama, D'Cunha, Luketich, Bermudez.
Ex vivo lung perfusion (EVLP) strategies represent a new frontier in lung transplantation technology, and there have been many clinical studies of EVLP in lung transplantation. The establishment of a reliable EVLP model in small animals is crucial to facilitating translational research using an EVLP strategy. The main objective of this study was to develop a reproducible rat EVLP (R-EVLP) model that enables prolonged evaluation of the explanted lung during EVLP and successful transplantation after EVLP. The donor heart-lung blocks were procured with cold low-potassium dextran solution and immersed in the solution for 1 h at 4 °C. And then, the heart-lung blocks were flushed retrogradely and warmed up to 37 °C in a circuit perfused antegradely with acellular perfusate. The perfusate was deoxygenated with a gas mixture (6% O2, 8% CO2, 86% N2). The perfusion flow was maintained at 20% of the entire cardiac output. At 37 °C, the lungs were mechanically ventilated and perfusion continued for 4 h. Every hour, the perfused lung was evaluated for gas exchange, dynamic lung compliance (Cdyn) and pulmonary vascular resistance (PVR). R-EVLP was performed for 4 h. Pulmonary oxygenation ability (pO2/pCO2) was stable for 4 h during EVLP. It was noted that Cdyn and PVR were also stable. After 4 h of EVLP,

EVLP – Philosophies…
• Evaluation – Extending donor pool • Improving quality – Reconditionning • Prolong perfusion and/or transport time • Research
EVLPResearch
World J Exp Med. 2014 May 20;4(2):7-15.
Animal models of ex vivo lung perfusion as a platform for transplantation research. Nelson, Bobba, Ghadiali, Hayes, Black, Whitson. Ex vivo lung perfusion (EVLP) is a powerful experimental model for isolated lung research. EVLP allows for the lungs to be manipulated and characterized in an external environment so that the effect of specific ventilation/perfusion variables can be studied independent of other confounding physiologic contributions. At the same time, EVLP allows for normal organ level function and real-time monitoring of pulmonary physiology and mechanics. As a result, this technique provides unique advantages over in vivo and in vitro models. Small and large animal models of EVLP have been developed and each of these models has their strengths and weaknesses. In this manuscript, we provide insight into the relative strengths of each model and describe how the development of advanced EVLP protocols is leading to a novel experimental platform that can be used to answer critical questions in pulmonary physiology and transplant medicine.
• The use of EVLP… • allows an objective assessment of high-risk donor lungs. • autorize treatment, reconditionning of suposed non-transplantable
lungs. • permits when these lungs are transplanted, acceptable rates of primary
graft dysfunction, with an early and mid-term outcomes similar to those with conventionally selected and transplanted lungs.
• permits to explore new source of donors (DCD donor, circulatory death, extending criteria donor, hanging victim, infected organs, ECMO…).
• help to prolong preservation time, facilitating long-distance transport and combined organ transplantation.
• leads to experimental platform that can be used to answer questions in pulmonary physiology and transplant medicine.
Conclusions




![E } ] ( } í Ç µ v î ì î í r î ì î î](https://static.fdocuments.us/doc/165x107/61d22598186b7f513908dfef/e-v-r-.jpg)



![v v o µ ] W o v î ì î ì r î í l î ì î î r î ... · / v v o µ ] W o v î ì î ì r î í l î ì î î r î ï ( / v v o µ ] W o v î ì î ì r î í l î ì î î](https://static.fdocuments.us/doc/165x107/600570084499ff768d735382/v-v-o-w-o-v-r-l-r-v-v-o-w-o-v-.jpg)





![î ì î í r î ì î î Z P ] } v / ^ ] v v v P ] v ] v P ...](https://static.fdocuments.us/doc/165x107/62da430cd2eb350bb64a434b/-r-z-p-v-.jpg)

