
Strabismus surgery made simple: Dr. Madhu Karna Strabismologist
Quality of life improves after strabismus surgery in 1
patients with Graves’ Orbitopathy 2
3
Hinke Marijke Jellema, MMedSci, CO; Elly Merckel-Timmer, CO; Roel Kloos, MD; 4
Peerooz Saeed, MD, PhD; Maarten P Mourits, MD, PhD 5
Department of Ophthalmology, University of Amsterdam, the Netherlands 6
7
8
Running head: QoL after strabismus surgery in TED. 9
10
11
12
Correspondence and reprint requests to: Hinke Marijke Jellema, Department of 13
Ophthalmology, Academic Medical Centre, Meibergdreef 9, 1105 AZ Amsterdam, the 14
Netherlands. E-mail: [email protected] 15
16
WORD COUNT: 2057 17
KEYWORDS: 18
Quality of life 19
Graves’ Orbitopathy 20
diplopia 21
strabismus 22
GO-QoL 23
field of BSV 24
Page 1 of 19 Accepted Preprint first posted on 3 February 2014 as Manuscript EJE-13-0973
Copyright © 2014 European Society of Endocrinology.
2
ABSTRACT 25
Objective: To evaluate the influence of strabismus surgery on quality of life (QoL) in 26
Graves’ Orbitopathy (GO) patients. 27
Design: Prospective study of case series 28
Methods: Consecutive GO-patients who were scheduled for their first strabismus 29
surgery were included into the study. Patients completed the Graves’ Orbitopathy 30
Quality of Life questionnaire (GO-QoL) within 3 months before surgery and 2-4 31
months after surgery. A complete orthoptic examination, including the field of 32
binocular single vision (BSV), was performed. Clinically relevant response (CRR) of 33
the QoL was also evaluated. 34
Results: Twenty-eight patients were included. GO-QoL score for visual functioning 35
was 46.3±24.2 before surgery and 65.7±30.5 after surgery (p=0.009). The GO-QoL 36
score for appearance changed from 60.6±25.9 to 69.5±24.2 (p=0.005). After surgery, 37
the field of BSV increased from 24.3±34.8 to 68.5±36.0 points (p=0.000). A weak 38
correlation was found between the field of BSV and the visual functioning score after 39
surgery (r=0.417;p=0.034). CRR was found in 20 (71%) of the patients. Those with a 40
CRR showed a larger field of BSV (p=0.002) and better GO-QoL scores (p=0.008). 41
Conclusions: GO-QoL score increases significantly for both visual functioning and 42
appearance after the first strabismus surgery in GO-patients, showing the highest 43
improvement for the visual functioning questions. Both the GO-QoL and field of BSV 44
outcome correlate well with the CRR. 45
46
47
48
49
Page 2 of 19
3
INTRODUCTION 50
At least 40% of patients with Graves’ Orbitopathy suffer from diplopia, which 51
severely interferes with daily life activities like working, driving a car or reading(1-4). 52
To quantify the impact of the disease on functioning and appearance, the GO-QoL 53
questionnaire was developed into Dutch and English, validated and translated in six 54
other languages (www.eugogo.eu)(1-5). For both functioning and appearance, a total 55
of 100 points can be scored. Terwee et al (2001) studied the effect of different 56
surgical treatments on GO-QoL outcome and concluded that for strabismus surgery a 57
minimum of 6 points of change has to be considered as minimal important change. 58
However, to our knowledge, this minimum clinically important difference was not 59
confirmed by other studies. 60
The importance of QoL in evaluating the outcome of treatment has been 61
stretched by the EUGOGO group and the Amsterdam declaration (6-8). In line with 62
this, the goal of the present study is to quantify the QoL before and after strabismus 63
surgery in GO-patients. Approximately 170 new GO-patients are referred to our 64
hospital each year and about 50 (29%) patients require strabismus surgery. This 65
percentage is almost comparable to the numbers assessed in a previous study and a 66
comparable setting1. Improvement of QoL for the functional part can be established 67
by creating the largest possible field of binocular single vision (BSV)2. In the 68
literature, this measurement is scarcely used as outcome criteria (10-14). However, 69
in the clinical setting, this instrument is the best available equipment for quantifying 70
binocular single vision in other directions than primary position. The purpose of this 71
study is to evaluate the effect of strabismus surgery on the GO-QoL and to 72
investigate the correlation between the GO-QoL and the field of BSV. 73
74
Page 3 of 19
4
SUBJECTS AND METHODS 75
The study was conducted according to the principles of the Declaration of 76
Helsinki (seventh edition, October 2008, Seoul) and in accordance with the Medical 77
Research Involving Human Subjects Act (WMO).This research did not receive any 78
specific grant from any funding agency in the public, commercial or not-for-profit 79
sector. Our local ethical committee reviewed the research protocol. No approval was 80
needed, because all interventions are normally carried out within the daily routine. 81
Between December 2011 and September 2012, all consecutive GO-patients 82
(clinically and biochemically euthyroid) in our tertiary referral center who needed a 83
first strabismus surgery for diplopia were asked to participate into the study. Patients 84
with pre-existent strabismus, suppression and/or vision < 0.2 in one or both eyes 85
were excluded. An informed consent form was signed by patients who could be 86
included. Data regarding, gender, date of first diagnosis of GO, prior treatment for 87
their thyroid and eye disease and diplopia complaints before the strabismus 88
operation were recorded. A full orthoptic exam was performed within 3 months before 89
and 2-4 months after surgery. This examination included: prism covertest at near (30 90
cm) and distance (5 m), cyclodeviation on 2 ½ m with help of the Maddoxscreen and 91
the cycloforometer of Francheshetti3, measurement of ductions by a motilitymeter4, 92
eye position measured in 9 directions of gaze with the Maddoxglass and 93
Maddoxcross (Amsterdam motility scheme) and the field of BSV at 2 ½ m with help 94
of the Maddoxscreen5. A stable orthoptic examination during the last 3 months was 95
part of the inclusion criteria. The choice of surgery procedure was based on the full 96
orthoptic exam5. There were no restrictions about the type of surgical procedure. 97
Patients were operated by three orbital surgeons (RK, PS and MM). 98
Page 4 of 19
5
Patients completed both subscales within the GO-QoL; the visual functioning 99
and the appearance questions6. Questionnaires were self-administered, without 100
supervision, following verbal and written instructions. 101
All GO-QoL questions were scored as `severely limited' (one point), `a little 102
limited' (two points), or `not limited at all' (three points). The questions 1 - 8 and 103
questions 9 - 16 were added up to two raw scores from 8 to 24 points, and then 104
transformed to two total scores from 0 to 100 by the following formula: total score = 105
((raw score - 8)/16 x 100). For both total scores holds that higher scores indicate 106
better QoL. For questions 1 and 2, the answers `no drivers' license' or `never learned 107
to ride a bike' were scored as a missing value. When there were missing values for 108
some items, total scores were calculated for the remaining completed items. The 109
transformation was then adjusted to: total score = ((raw score - *)/ (2 x *) x 100) 110
where * is the number of completed items7. 111
The outcome of the field of BSV was scored with help of a modified score 112
system for diplopia by Holmes et al (2005)8 (Table 1). The original system is a 113
subjective score system containing the questions about double vision during 114
“reading” (4 points) and in “any position” (1 point). Also, the question if a person can 115
get rid of the double vision (-1 point) is part of the score list. Those three questions 116
were deleted and gaze position up 5º, right 20º and left 20º were added. Score points 117
were reformatted and the score system was objectively used. 118
Two orthoptists (HMJ and EMT) independently defined the clinical relevant 119
response (CRR) in each patient. Patients who showed clinical sufficient improvement 120
on the Amsterdam motility scheme were called responders. 121
Statistical analyses were done with help of SPPS 19.0 (Statistical Package for the 122
Social Sciences, Version 19.0, Chicago, Illinois, USA). Each variable was verified for 123
Page 5 of 19
6
normal distribution with help of the Kolmogorov-Smirnov test. If the data met the 124
requirements for normal distribution, parametric tests were applied. If not, non-125
parametric tests were used. To uncover the main and interaction effects of 126
categorical independent variables on an interval dependent variable ANOVA was 127
used. 128
129
RESULTS 130
28 patients were included into the study. Twenty-one patients were excluded. 131
13 patients because they needed a reoperation, 2 patients because of suppression 132
and thus no diplopia complaints, in 6 patients the data were incomplete. Of the 133
included patients, 8 were male (29%) and 20 were female (71%). Mean age was 134
54.5±11.2 year. All general data can be found in table 2. The type of surgery is listed 135
in Table 3. 136
The field of BSV changed from 24± 35 points to 68± 37 points (p=0.000) 137
(Figure 1). The GO-QoL for visual functioning before surgery was 46±26 points and 138
increased to 66±31 points after surgery (p=0.009). The questions about appearance 139
scored 61±26 points before and 71±22 after surgery (p=0.005)(Figure 2). A prior 140
performed decompression did not influence outcome (p=0.224). 141
Between the diplopia groups (eg intermittent, gaze dependent, constant or 142
abnormal head posture), no different outcome in score of the preoperative field of 143
BSV (ANOVA p=0.111) or the score of the GO-QoL for visual functioning (p=0.430) 144
was found. 145
A weak correlation was found between the field of BSV and the GO-QoL for 146
the visual functioning score after surgery (r=0.417;p=0.034)(Figure 3), but not for 147
appearance (r=0.180;p=0.374). 148
Page 6 of 19
7
CRR was found in 20 (71%) patients. The responders showed significant 149
larger fields of BSV (p=0.002) after surgery and better outcome on GO-QoL for visual 150
functioning (p=0.008) compared to the non-responders. 151
152
153
DISCUSSION 154
The present study is, to the best of our knowledge and inspired by the 155
Amsterdam declaration, the first prospective study focusing on the QoL after 156
strabismus surgery in GO-patients. After this strabismus surgery, a significant 157
improvement of the GO-QoL score for both visual functioning and appearance 158
occurs. Both the field of BSV and GO-QoL score after surgery are significantly higher 159
in the responders group. 160
In contrast to a previous study, we found a significant higher GO-QoL score for 161
the visual functioning after surgery (mean improvement 19.4±34.5 in the present 162
study compared to mean 2.8±25.4 in the study of Terwee et al (2001))7. The 163
improvement is also higher as the mentioned 6 points of minimal clinically important 164
difference(MCID)7. The hospital setting, duration of the GO, the mean age, sex 165
distribution and number of participating patients (n=31 versus present study n=28) is 166
comparable in both studies. The improvement of the subjective score we found in this 167
study is more in line with what clinicians would expect. Terwee et al. could not clearly 168
explain why the improvement of the subjective score in het study was rather modest7. 169
Explanations for the differences of results between her and our studies are the 170
following: 1. Terwee et al. sent questionnaires 3 months after the operation per mail, 171
while our questionnaires were embedded in the treatment protocol; 2. Because the 172
questionnaire was embedded in the protocol, the response rate was 100% compared 173
Page 7 of 19
8
to 80% in Terwee’s study. Maybe the 20% of non-responders were the ones who 174
were asymptomatic, which influence the total score negatively; 3. For the last five 175
years strabismus surgery in GO-patients has been a focus of research in our 176
institute, which might have improved the outcome of strabismus surgery and thus the 177
outcome of the subjective evaluation. To ratify this, the CCR of Terwee et al. was 178
50% as we found 71% of patients responding to the strabismus surgery; 4. In the 179
present study only primary strabismus surgeries were included, in the study of 180
Terwee et al. this item is not specified. This could also clarify the difference between 181
the visual functioning score before surgery which is lower at baseline in the present 182
study. 183
Terwee et al. (2001) suggested that the surgery is part of a larger surgery plan 184
and that this minor invasive strabismus surgery does not change the outcome 185
significantly. However, in our study group 16 patients underwent decompression 186
surgery which counts as a major invasive surgery. GO-QoL was not different 187
between the group with or without prior decompression surgery (p=0.224). 188
In general, one should take into account that changes of the GO-QoL score 189
can be influenced by the side-effects, costs and possible available alternative 190
treatments like prism therapy. Also, total score changes in the lower end of the score 191
scale may be less important than changes to the higher end of the score7. However, 192
in contrast to the results of Terwee et al (2001) we had a lower baseline GO-QoL 193
score (due to stricter inclusion criteria) and despite of that still a higher treatment 194
effect. The side effect aspect may explain the weak correlation found between the 195
GO-QoL for visual functioning and the field of BSV after surgery. The field of BSV is 196
a clinical measurement in a setting wherein the head of the patients is being moved 197
Page 8 of 19
9
slowly which is different from movements in daily life (question 4 of the visual 198
functioning questionnaire 199
Another aspect which can influence the outcome of the GO-QoL is the regression to 200
the mean phenomenon9. However, by merely asking the patients to fill in the GO-QoL 201
one time before and one time after the surgery, we cannot distinguish between the 202
influence of the surgery and that of the regression of the mean. 203
It would be interesting to see if the GO-QoL outcome also applies to the 204
results 6 – 12 months after surgery for orthoptic stability, as was found in our 205
previous results. 10 Hatt et al (2012) found no changes in the health related quality of 206
life questionnaire one year after surgery (HR-QoL) in both the diplopic and non-207
diplopic patients following successful strabismus surgery11. A future study may reveal 208
if this is also applicable for the GO-patient group. 209
We are aware of the fact that we evaluated the GO-QoL and BSV scores after 210
one strabismus surgery and that for many patients multiple strabismus surgeries are 211
needed12-14, and therefore undervalue the final outcome12. For that reason, a future 212
study will focus on the effect after 2 surgeries. 213
In conclusion, the GO-QoL and the field of BSV outcome both add in their own 214
way to the information for the clinician regarding CRR in GO-patients who undergo 215
strabismus surgery. 216
217
DECLARATION OF INTEREST 218
All authors state that there is no conflict of interest that could be perceived as 219
prejudicing the impartiality of the research reported. 220
221
222
Page 9 of 19
10
FUNDING 223
This research did not receive any specific grant from any funding agency in 224
the public, commercial or not-for-profit sector. 225
226
227
ACKNOLEDGEMENTS 228
The authors thank Yvette Braaksma-Besselink, Yolande Everhard-Halm, and 229
Linda Groenveld, all orthoptists, for their clinical contribution to the article. Also, we 230
would like to acknowledge the effort of prof. dr. Wilmar Wiersinga with regard to the 231
discussion section. 232
233
Reference List 234
235
1. Sasim IV, Berenschot TTJM, Isterdael van C, Mourits MP. Planning health care for 236
patients with Graves' orbitopathy. Graefes Arch Clin Exp Ophthalmol 2008;246:1315-237
21. 238
2. Schotthoefer EO, Wallace DK. Strabismus associated with thyroid eye disease. Curr 239
Opin Ophthalmol 2007;18:361-5. 240
3. Klainguti G, Strickler J, Chamero J. Comparison of five methods for subjective 241
assessment of ocular cyclodeviation. Klin Monatsbl Augenheilkd 1992;200:409-13. 242
4. Mourits MP, Prummel MF, Wiersinga WM, Koornneef L. Measuring eye movements in 243
Graves' ophthalmopathy. Ophthalmology 1994;101:1341-6. 244
Page 10 of 19
11
5. Gutter M, van Petegem - Hellemans J, van Wijnen - Segeren I, Jellema HM. Orthopics: 245
Handbook of Practical Skills. 1th ed. Ridderkerk: Luiten Publishing; 2010. 246
6. Terwee CB, Gerding MN, Dekker FW, et al. Development of a disease specific quality 247
of life questionnaire for patients with Graves'ophthalmopathy: the GO-QOL. Br J 248
Ophthalmol 1998;82:772-9. 249
7. Terwee CB, Dekker FW, Mourits MP, et al. Interpretation and validity of changes in 250
scores on the Graves' Ophthalmopathy quality of life questionnaire (GO-QOL) after 251
different treatments. Clinical Endocrinology 2001;54:391-8. 252
8. Holmes JM, Leske DA, Kupersmith MJ. New methods for quantifying diplopia. 253
Ophthalmology 2005;112:2035-9. 254
9. Barnett AG, van der Pols J.C., Dobson AJ. Regression to the mean:what is it and how to 255
deal with it. International Journal of Epidemiology 2005;34:215-20. 256
10. Gutter M, van Petegem - Hellemans J, van Wijnen - Segeren I, Jellema HM. 257
Handleiding praktische vaardigheden orthoptie. 3 ed. Barendrecht: Uitgeverij Luiten; 258
2008. 259
11. Hatt SR, Leske DA, Liebermann L, Holmes JM. Changes in Health-Related Quality of 260
Life 1 year following strabismus surgery. Am J Ophthalmol 2012;153:614-9. 261
12. Jellema HM, Saeed P, Everhard-Halm YS, et al. Bilateral inferior rectus recession in 262
patients with Graves orbitopath: is it effective? Ophthalmic Plastic and Reconstructive 263
Surgery 2012;28:268-72. 264
13. Lyons CJ, Rootman J. Strabismus in Graves' Orbitopathy. Pediatric Endocrinology 265
Reviews 2010;7:227-9. 266
Page 11 of 19
12
14. Dickinson AJ, Perros P. Thyroid-Associated_Orbitopathy; who and how to treat? 267
Endocrinol Metab Clin N Am 2009;38:373-88. 268
269
270
FIGURE LEGENDS 271
272
Figure 1: The score of the field of binocular single vision before surgery (left boxplot) 273
and after surgery (right boxplot)(p=0.000). 274
275
Figure 2: GO-QoL questionnaire score for visual functioning (left two bars) and 276
appearance (right two bars) before and after surgery. 277
278
Figure 3: Correlation between the score of the field of BSV and the score for visual 279
functioning of the GO-QoL after surgery (r=0.417;p=0.034). 280
281
Page 12 of 19
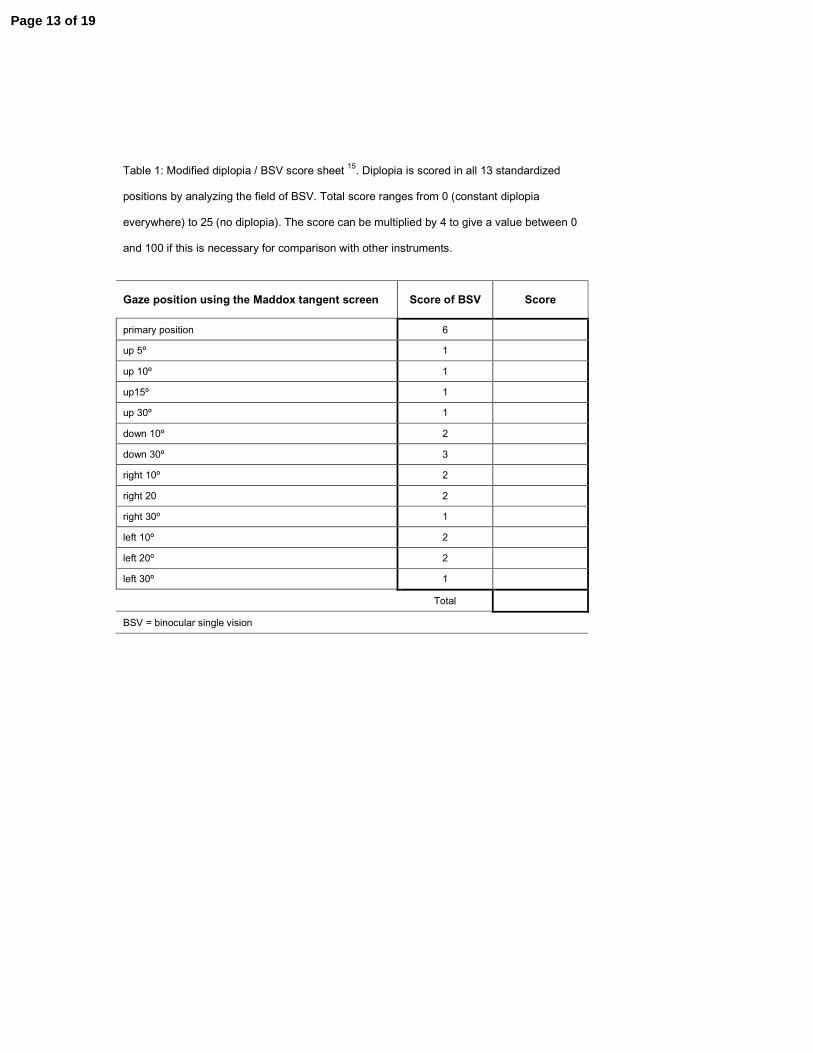
Table 1: Modified diplopia / BSV score sheet
15. Diplopia is scored in all 13 standardized
positions by analyzing the field of BSV. Total score ranges from 0 (constant diplopia
everywhere) to 25 (no diplopia). The score can be multiplied by 4 to give a value between 0
and 100 if this is necessary for comparison with other instruments.
Gaze position using the Maddox tangent screen Score of BSV Score
primary position 6
up 5º 1
up 10º 1
up15º 1
up 30º 1
down 10º 2
down 30º 3
right 10º 2
right 20 2
right 30º 1
left 10º 2
left 20º 2
left 30º 1
Total
BSV = binocular single vision
Page 13 of 19

Page 14 of 19
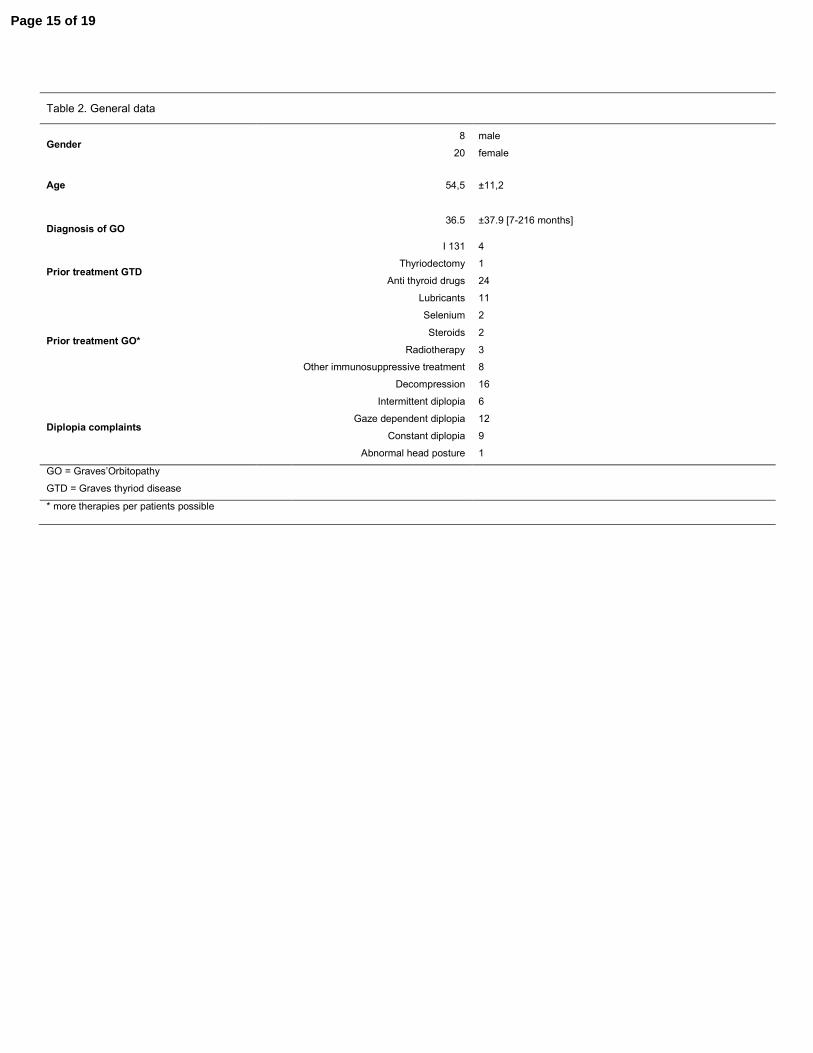
Table 2. General data
Gender 8
20
male
female
Age 54,5 ±11,2
Diagnosis of GO 36.5 ±37.9 [7-216 months]
Prior treatment GTD
I 131
Thyriodectomy
Anti thyroid drugs
4
1
24
Prior treatment GO*
Lubricants
Selenium
Steroids
Radiotherapy
Other immunosuppressive treatment
Decompression
11
2
2
3
8
16
Diplopia complaints
Intermittent diplopia
Gaze dependent diplopia
Constant diplopia
Abnormal head posture
6
12
9
1
GO = Graves’Orbitopathy
GTD = Graves thyriod disease
* more therapies per patients possible
Page 15 of 19
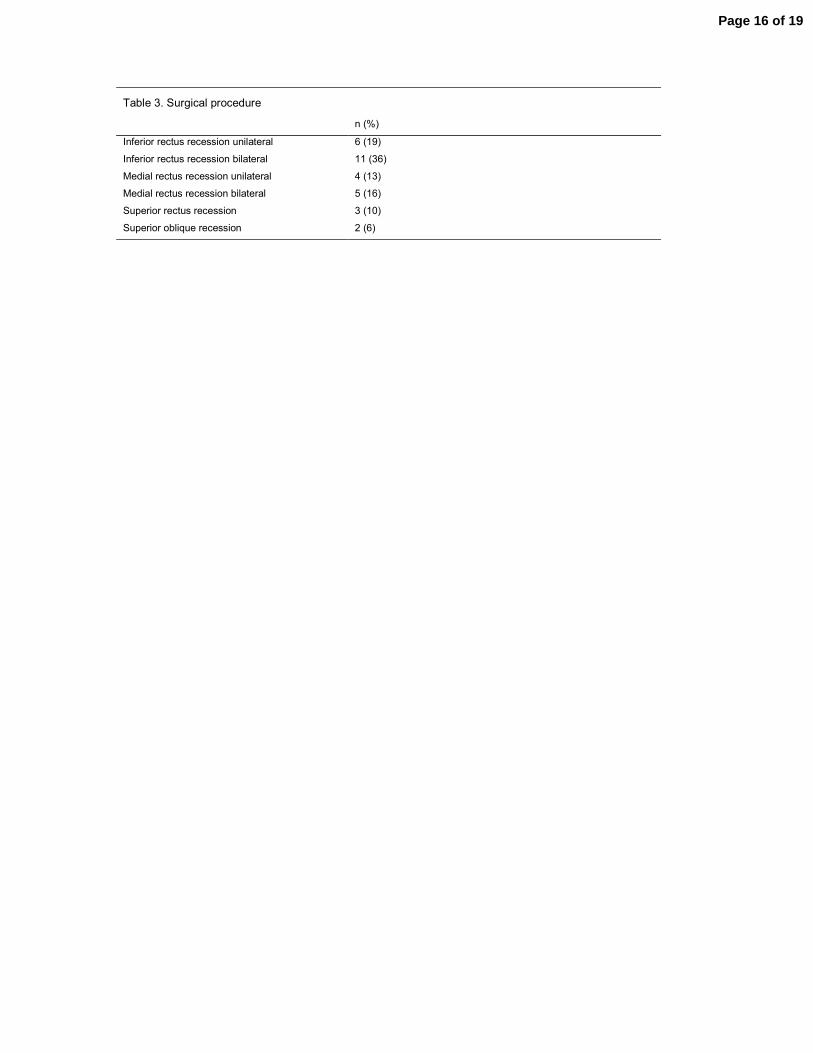
Table 3. Surgical procedure
n (%)
Inferior rectus recession unilateral
Inferior rectus recession bilateral
Medial rectus recession unilateral
Medial rectus recession bilateral
Superior rectus recession
Superior oblique recession
6 (19)
11 (36)
4 (13)
5 (16)
3 (10)
2 (6)
Page 16 of 19
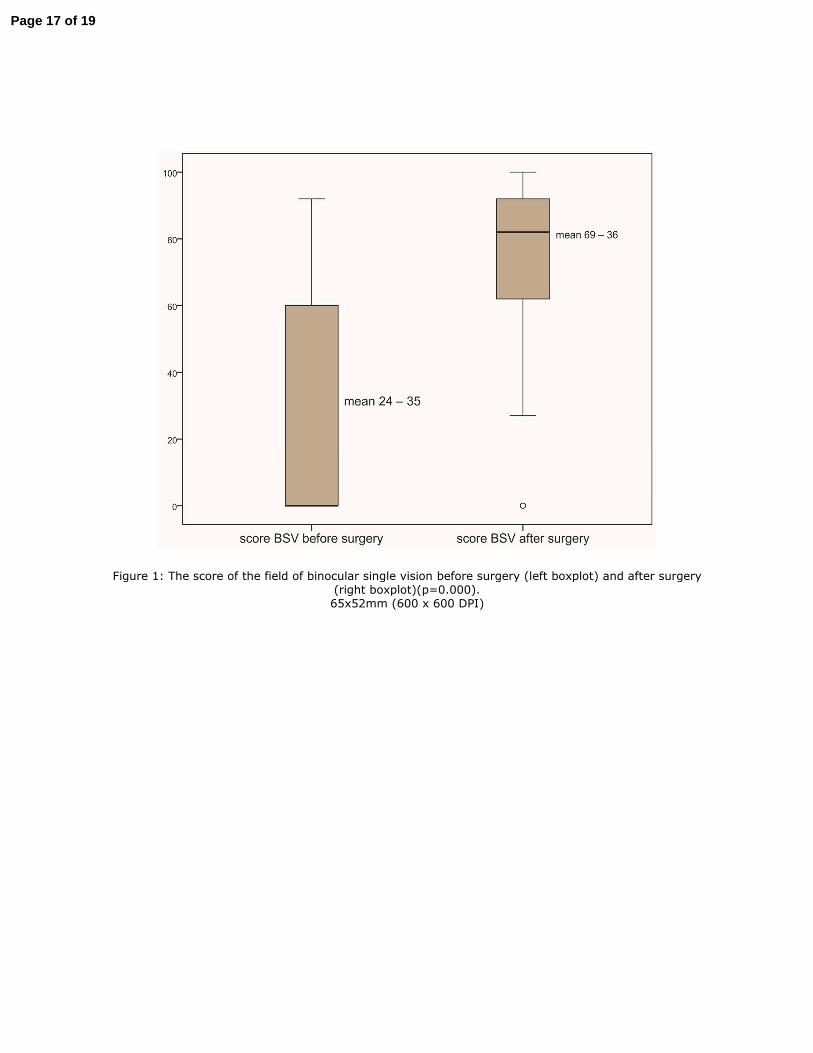
Figure 1: The score of the field of binocular single vision before surgery (left boxplot) and after surgery (right boxplot)(p=0.000). 65x52mm (600 x 600 DPI)
Page 17 of 19
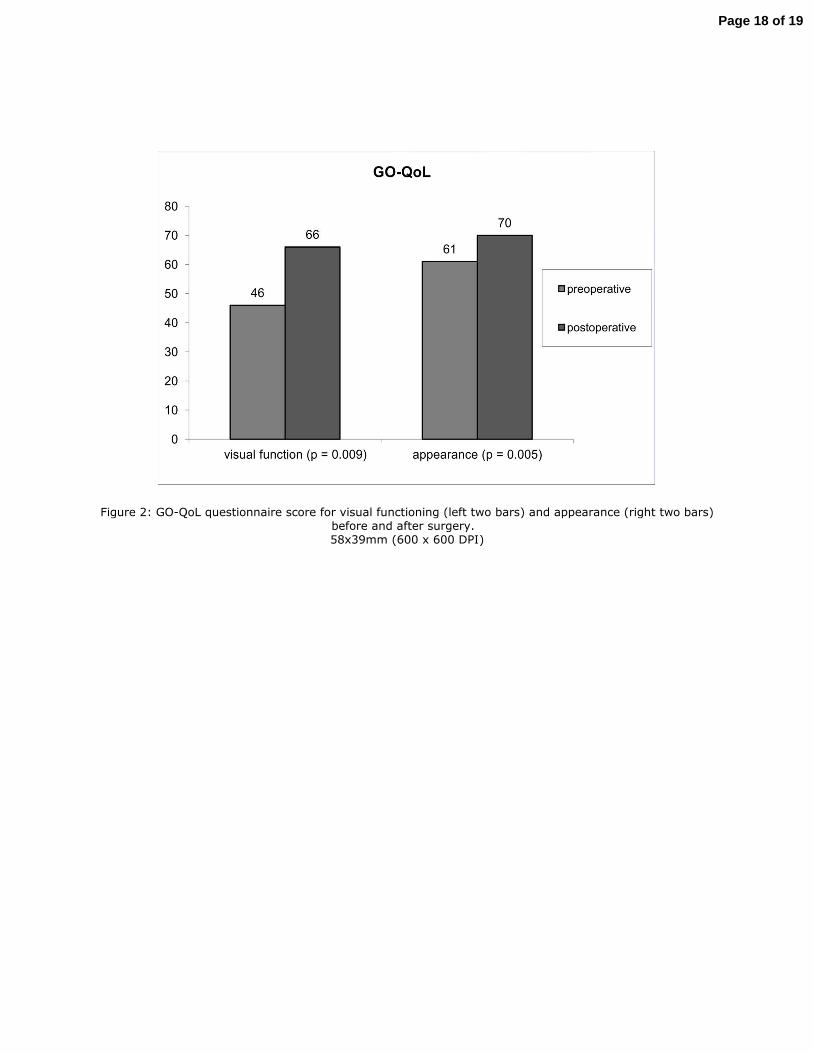
Figure 2: GO-QoL questionnaire score for visual functioning (left two bars) and appearance (right two bars) before and after surgery. 58x39mm (600 x 600 DPI)
Page 18 of 19
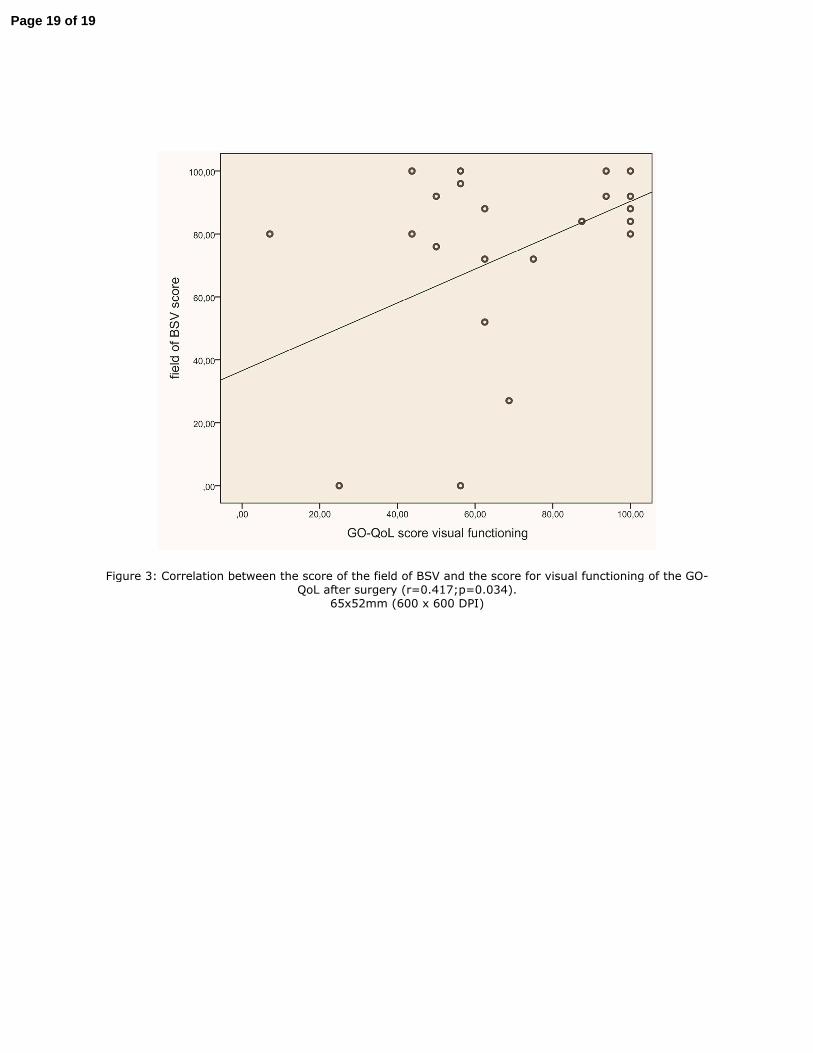
Figure 3: Correlation between the score of the field of BSV and the score for visual functioning of the GO-QoL after surgery (r=0.417;p=0.034).
65x52mm (600 x 600 DPI)
Page 19 of 19


















