Quality Control for AST -...
37
ROMNEY HUMPHRIES SEPTEMBER 2014 QUALITY CONTROL FOR AST
Transcript of Quality Control for AST -...

R O M N E Y H U M P H R I E S
S E P T E M B E R 2 0 1 4
QUALITY CONTROL FOR AST

ENSURING QUALITY OF AST RESULTS
AST QC
Good media / reagent quality
Equipment properly serviced
Staff are competent
Review patient results

RESPONSIBILITIES FOR AST QC
AST Manufacturer
• Antimicrobial is stable
• Antimicrobial labeled
properly
• Antimicrobial potency
is correct
• Complies with GMP
Laboratory
• Reagents stored
appropriately
• Staff are trained &
competent
• Protocols are followed

STANDARD QC STRAINS

WHICH QC STRAIN DO I TEST?
IF performing CLSI reference testing
(MIC or DD).
IF using a diagnostic manufacturer –
follow their QC recommendations!

M100 S24 APPENDIX C
Use for βlactam/βlactamase inhibitor combinations
Use for all antimicrobials, unless otherwise stated

WHY DO I HAVE TO TEST PSA 27853 VS CARBAPENEMS?
Agent E. coli
ATCC 25922
P. aeruginosa ATCC 27853
Doripenem 0.015–0.06 0.12–0.5
Ertapenem 0.004–0.015 2–8
Imipenem 0.06–0.25 1–4
Meropenem
0.008–0.06 0.25–1
Goal is to get “on scale” endpoints for carbapenems 25922 MICs
are too low (will always test “≤”

OTHER RECENT CHANGES TO “ROUTINE” QC
Table Organism Group Routine QC Change For use ONLY to QC:
2A Enterobacteriaceae Added P. aeruginosa ATCC 27853
carbapenems
2B-1 Pseudomonas
aeruginosa
Deleted E. coli ATCC 25922 NA
2B-2 Acinetobacter spp. E. coli ATCC 25922 tetracyclines trimethoprim-sulfa
2B-3 Burkholderia cepacia E. coli ATCC 25922
chloramphenicol minocycline
trimethoprim-sulfa
2B-4 Stenotrophomonas maltophilia
E. coli ATCC 25922 chloramphenicol minocycline trimethoprim-sulfa
2B-5 Other Non-
Enterobacteriaceae
E. coli ATCC 25922
chloramphenicol
tetracyclines sulfonamides trimethoprim-sulfa

WHAT ARE THOSE “SUPPLEMENTAL” QC STRAINS FOR?
• “Routine” QC Strain
• Test regularly (daily or weekly)
• “Supplemental” QC strain
• May have “S” or “R” characteristic specific for one or more
“special” AST tests
• EXAMPLE: ATCC BAA-977 has includible clindamycin resistance
• Use to assess new test
• Use for training purposes
• Use for competency
• DO NOT need to perform regularly (weekly or daily)

HOW OFTEN SHOULD AST QC BE DONE?
• Daily OR
• On days when patient isolates are
tested OR
• Weekly (after alternate QC plan
implemented)
• 20 – or 30 – day plan
• New, alternative 3 x 5 plan

REMINDER: 20- 30- DAY PLAN
• Perform testing for 20 or 30 consecutive test days,
and document results
• Convert to weekly QC if:
• No more than 1 out of 20 OR
• No more than 3 out of 30 MICs for each antimicrobial
agent/organism combination are outside acceptable MIC
limits
• THEN:
• Perform weekly QC testing AND
• Whenever any reagent component of the test is changed
(new lot / new shipment)

3 X 5 PLAN
• Perform 3 tests / day for 5 days
• 3 separate inocula for each replicate
• If results unacceptable, test another 5 days
• Advantages:
• Possible to identify issues sooner
• Takes less time
• Takes fewer resources
• Statistically comparable to 20-30 dya plan
• Accepted by CAP
• Pending CLIA

Test 3 replicates of each QC strain for 5
days (different inoculum)
0-1 of 15 out of
range? 4 or more of 15 out
of range?
Test another 3 x 5
days
2-3 of 30
out of
range?
PASS. Convert
to weekly QC
2-3 of 15 out of
range?
FAIL.
Continue daily QC
M100-S24.
Yes Yes
Yes No

SOURCES OF IDENTIFIABLE ERROR
QC strain
• Wrong QC strain used
• Improper storage
• Inadequate maintenance
(same F2 for >1 month)
• Contamination
• Nonviable
• Changes (loss of plasmid)
Supplies
• Improper storage
• Contamination
• Damages plates / panels
• expired
Process: not following SOP, transcription error.
Equipment: not functioning properly

WHAT IF MY QC ISN’T DUE TO AN IDENTIFIABLE ERROR?
• QC ranges are established to include >=95% of
results from routine testing
• Some errors are random!
• Perform “corrective Action”:
• Perform QC as soon as possible
• **new** If 5 acceptable QC results are available, no
additional days of QC testing are needed.
• Old: had to do 5 days of QC

Weekly QC
Out-of-range (error not identifiable)
Retest (same day)
Result in range?
≥5 recent results for
same lot in range?
Retest result out-of-
range?
Yes, test daily until
5 results available
Any result
out of
range?
PASS. Resume
weekly QC
testing
Result in range?
<5 recent results for
same lot in range?
FAIL.
Corrective Action
M100-S24.
See Q&A section
Yes Yes
No Yes

EXAMPLES
Week Day Result Action
1 1 4
2 1 8
3 1 8
4 1 4
5 1 16 Out of QC, repeat
next day
5 2 8 In range. 5
acceptable QC tests
Week Day Result Action
1 1 4
2 1 8
3 1 16 Out of QC, repeat
next day
3 2 4 In range: 3
acceptable results
(need 2 more)
3 3 8 In range
3 4 8 In range. 5
acceptable QC tests
E. Coli ATCC 25922 and ampicillin
Acceptable Range: 2-8 μg/ml
Lot: 9661
Scenario 1 Scenario 2
M100 S24 (page 216 Q&A)
UH-OH, MORE RESULTS OUT OF QC!
• Probable system error
• Daily QC must be continued until final resolution of
problem!
• Ideas on how to fix this:
• New QC strain
• New lots of materials (incl. new turbidity standards)
• If problem appears to be related to manufacturer, contact them!
• Might need to use another test method

WHAT ABOUT MY PATIENT RESULTS?
• Don’t forget to carefully review each patient result
• Approaches will differ, based on degree and
direction of QC errors
• Things to consider:
• Suppress result for antimicrobial out of QC
• Review individual patient / cumulative data for unusual
patterns (should be doing this anyway)
• Use an alternative method if necessary

EXAMPLE 1: DISK DIFFUSION QC WEEKLY RESULTS
QC Strain Drug Acceptable
Range Result Comment
P. aeruginosa
ATCC 27853
gentamicin 16-21 14 Reason for error; disk not flat on agar surface
tobramycin 19-25 23
E. coli
ATCC 25922
gentamicin 19-26 22
tobramycin 18-26 22
Identifiable error = disk not placed correctly Corrective action: Repeat QC test; OK to report patient results

EXAMPLE 2: DISK DIFFUSION QC
WEEKLY RESULTS
QC Strain Drug Acceptable
Range Result Comment
P. aeruginosa
ATCC 27853
gentamicin 16-21 12 Reason for error not identifiable but used new lot of media (lot A)
tobramycin 19-25 15 Reason for error not identifiable but used new lot of media (lot A)
E. coli
ATCC 25922
gentamicin 19-26 22
tobramycin 18-26 22
Error not Identifiable (possibly media??)
Note: lab should QC new lot of media before using for
patient isolates

SUGGESTED CORRECTIVE ACTION
EXAMPLE 2
• Test new lot of media (lot B) • Suspected problem is lot A media
• Probably contains too high concentration of cations (calcium, magnesium)
• Decreased activity for aminoglycosides with P. aeruginosa
• Elevated cations do not affect aminoglycosides with Enterobacteriaceae
• E. coli ATCC 25922 QC in control

CORRECTIVE ACTION DOCUMENTATION FOR
EXAMPLE 2
P. AERUGINOSA ATCC 27853
GENTAMICIN ZONE = 12 MM
ACCEPTABLE RANGE = 16-21 MM
Date/ Initial
Antimicrobial
Agent Result
Describe problem
Corrective Action taken to resolve
problem
Patient Results affected (yes/no)
Comments
8/8/08
RH
Gentamicin
12 mm
Mueller Hinton agar (lot A) showing small zone with gentamicin and P. aeruginosa; E. coli QC with gentamicin OK.
Obtain new lot of media (Lot B). Repeat QC with Lot A and Lot B. Lot A 12 mm
Lot B 18 mm
No Lot A media probably too high in calcium or magnesium content. Discard Lot A.

Disk Diffusion QC
Troubleshooting
Guide

WHEN DOES 1 VS. 5 VS. NEW AQP REQUIRED?
M100
S24,
Table 5F
CLSI M02-A11.
CLSI M07-A9.
MAINTAINING QUALITY CONTROL STRAINS
• Rehydrate new stock culture or obtain strain from
frozen
• Subculture to appropriate media (F1) store at 2-
8C (as appropriate)
• Subculture to approprirate media (F2) store at 2-
8C (as appropriate)
• Use this for QC on day 1 and to make F3
• Every 7 days, prepare a new F2 from F1
• Every 4 weeks, discard F1 and start again

MAINTAINING QUALITY CONTROL STRAINS (2)
E. coli ATCC 35218; K. pneumoniae ATCC 700603
• Beta-lactamase producers
• Beta-lactamase is plasmid-mediated
• Store at -60C or lower to prevent loss of plasmid; if plasmid is lost, strain would appear susceptible to beta-lactams

DON’T FORGET, TESTING QC
STRAINS IS JUST PART OF QC!
• Reviewing results of patient’s isolates:
• Testing routine QC strains doesn’t ensure every result on a patient’s isolate is accurate
• Patient results may be erroneous due to:
• mixed culture, misidentification
• individual drug/bug problem
• other technical error

EXAMPLE
• S. agalactiae isolated from blood and wound
cultures from an 82 year old woman with diabetes
and right ankle pain / swelling
Penicillin 0.06 S
Cefotaxime 0.12 S
Clindamycin >32 R
Erythromycin >32 R
Vancomycin 4 NS
What should we review?
Do ID and AST results correlate?
Were appropriate drugs reported?
Are results from similar drugs (class) OK?
Were appropriate comments added?
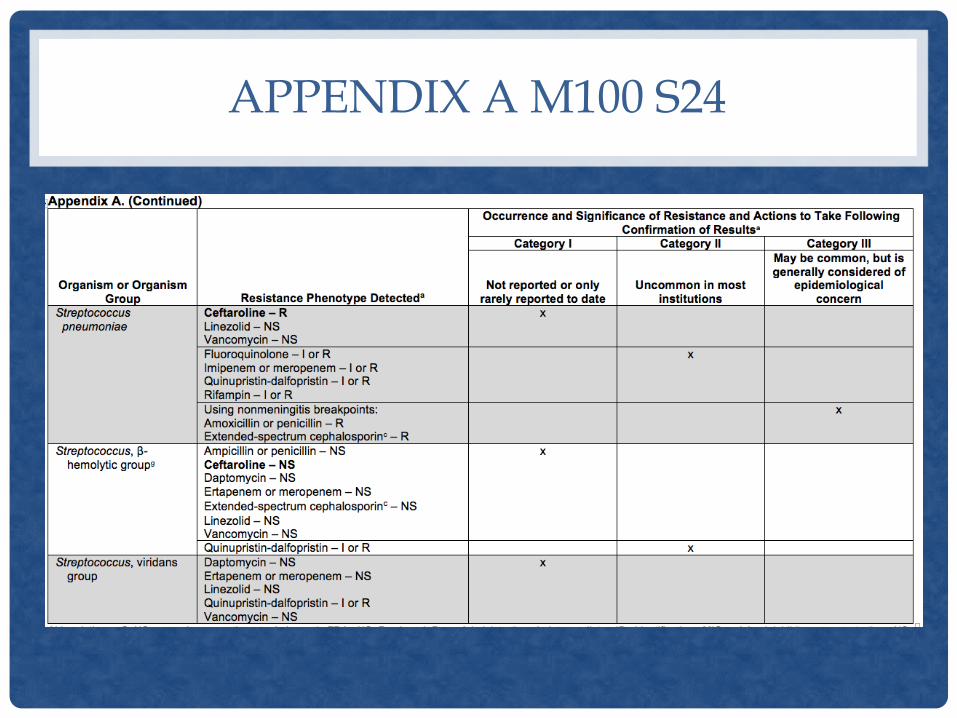
APPENDIX A M100 S24

SUGGESTED STEPS TO CONFIRM
ID AND AST RESULTS:
1.Check for transcription errors, contamination, or defective panel, plate, or card.
2.Check previous reports on the patient to determine if the isolate was encountered and confirmed earlier.
3.Repeat organism ID and AST with initial method to ensure they reproduce.
4.Confirm organism ID with second method performed in-house or at a referral laboratory.
5.Confirm AST results with second method (eg, in-house or referral laboratory). The second method might be:
A CLSI reference method (eg, broth microdilution, agar dilution, or disk diffusion) or
An FDA-cleared commercial test.

EXAMPLE: CONFIRM VANCOMYCIN- RESISTANT S. AGALACTIAE
ID AST Results
Initial tests Automated method
Automated method
Vancomycin 4 µg/ml
ID: Streptococcus agalactiae
Repeat tests Automated method
Etest
w or w/o
Automated method
Etest:
Vancomycin 4 µg/ml
Automated:
Vancomycin 4 µg/ml
ID: Streptococcus agalactiae
Repeat tests Conventional biochemicals and/or 16S sequencing
None S. agalactiae
Forward to local or state public health laboratory CDC


ADDITIONAL RESOURCES…

SHOULD WE EDIT ANY “S” OR “I” TO “R” BASED ON INTRINSIC RESISTANCE PROFILE FOR AN ISOLATE?
Any editing rule is based on ID and AST results being accurate!!! So, we must consider….
• Competency of personnel doing testing
• Testing pure cultures – use purity plates for broth MIC tests
• Reliability of organism ID
• Reliability of AST results
• Impact to patient care
• Situations where it would be wise to confirm results

CLSI “S” TO “R” EDITING RULES
Organisms Criteria Edit any “S” to
”R”
Staphylococcus
spp.
Oxacillin “R” All ß-lactams
except ceftaroline
Staphylococcus
spp.
Beta streptococci
Inducible
clindamycin
resistance
Clindamycin

UCLA ADDITIONAL “S” TO “R”
EDITING RULES (BASED ON INTRINSIC R)
Organisms Edit “S” to ”R”
Citrobacter braakii/ freundii
Enterobacter aerogenes
Enterobacter cloacae
Hafnia alvei
Morganella morganii
Proteus vulgaris
Providencia rettgeri / stuartii
Serratia marcescens
ampicillin
ampicillin-sulbactam
cefazolin
Klebsiella oxytoca
Klebsiella pneumoniae
ampicillin