EMERGING INFECTIOUS DISEASE -...
47
IS YOUR LABORATORY READY EMERGING INFECTIOUS DISEASE
Transcript of EMERGING INFECTIOUS DISEASE -...

IS YOUR LABORATORY READY
EMERGING INFECTIOUS DISEASE

46 yo anesthetist assistant from Johannesburg
Fever day 1, Headache day 4, Works until day 5
Admitted to hospital Day 5 for suspected encephalitis
CSF workup normal, fever 103.5°
No recent history of travel or insect bites
Patient dies on Day 23 of il lness
CASE 1: SOUTH AFRICA
1996
41 yo Dutch woman referred by GP to hospital
Patient presented to GP with fever on July 5
Recent travel to Uganda June 5 -28
Travel group 7 Dutch tourists and 2 guides
Placed in hospital ward with 3 other patients
Malaria ruled out x 3-given antimicrobials
July 7, rapid deterioration with liver failure
Patient dies on July 11
CASE 2: NETHERLANDS
2008
January 4, 44 yo female with HA, fever, diarrhea N&V
Previous travel to Uganda, return on January 1
Self treated with ciprofloxacin x 2, developed rash
January 6-7 seen as outpatient treated with anti -emetics
Return to PCP January 8 with worsening symptoms
Admission to hospital with diagnosis of hepatitis ↑LFT’s
Negative leptospirosis, malaria, hepatitis, arbovirus, rickettsia
Workup for Ebola and Marburg VHF negative
Cholecystectomy for acalculous cholecystitis
Discharged on January 19
Patient read of death of Dutch patient 7/2008
CASE 2+: UNITED STATES
2008
10/2 --38 yo male returns from Dubai very il l
Patient was moderately il l on the Emirates flight
Travels home by private transport with friend
Admitted to hospital 3 hours later
Recent travel to Afghanistan to brother’s wedding
10/6 patient dies
CASE 3: GLASGOW, SCOTLAND
2012

May 18, 55 yo male fever, sore throat, fatigue
Travel history —no travel to West Africa
Patient sent home after non-diagnostic workup
May 21, patient returns to hospital, worsening symptoms
Patient transferred to second hospital, ?VHF
May 25, patient dies
CASE 4:NEW JERSEY
2015
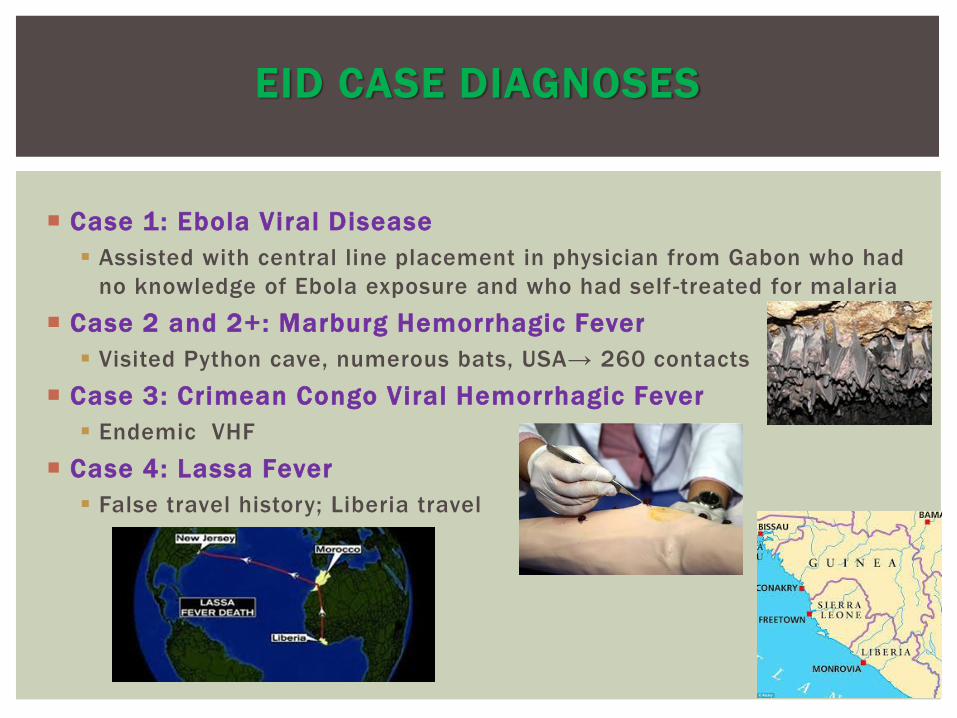
Case 1: Ebola Viral Disease
Assisted with central line placement in physician from Gabon who had
no knowledge of Ebola exposure and who had self -treated for malaria
Case 2 and 2+: Marburg Hemorrhagic Fever
Visited Python cave, numerous bats, USA→ 260 contacts
Case 3: Crimean Congo Viral Hemorrhagic Fever
Endemic VHF
Case 4: Lassa Fever
False travel history; Liberia travel
EID CASE DIAGNOSES

All patients presented to a community hospital without a
biocontainment unit
The diagnosis at presentation was unknown
All patients had non-specific symptoms at presentation,
predominantly fever and malaise
Several patients were less than truthful with travel history
All patients had multiple contacts while sick
COMMONALITY IN EID CASES

All of the patients will have laboratory tests
Most will not be in isolation initially
Standard PPE will not be consistently employed
Blood will be transferred by ungloved hands and possibly by
pneumatic tube
Geography of travel and or exposures will determine infectious
disease differential diagnosis—truthfulness is paramount
SCENARIOS YOU CAN PREDICT WITH THE EID
PATIENTS

EMERGING INFECTIOUS DISEASE (EID)
GLOBAL AVIATION ROUTES
32 yo female with fever and headache
Recently returned from Australia
30 day adventure travel trip
Exposures?
Horses, camels, kangaroos, Tasmanian devil
Hiking and camping in the forest
Insect bites
EID CASE PRESENTS TO YOUR ED

Arthropod borne disease?
Hendra virus
Lyssa virus
Nipah virus
Japanese encephalitis
AUSTRALIAN TRAVELER
WHAT ARE THE POSSIBILITIES?
Picture: Locations of previous Henipavirus outbreaks (red stars –
Hendra virus; blue stars – Nipah virus) and distribution of
Henipavirus flying fox reservoirs (red shading – Hendra virus; blue
shading – Nipah virus)

OPPORTUNITIES FOR OUTBREAKS OF EID
Increases in travel, trade, and tourism
Zoonotic disease and human interaction in tourism
Animal pathogen spillover
Environmental changes resulting in new endemic regions
Refugee crises and population displacement
I l legal animal trade
Market for exotic animal products
Urbanization
Natural disasters in populated areas

WHAT’S A LAB TO DO?
Risk assessment— what can your lab do safely
PPE training and skills development
Lab Drills with debriefing and alteration of lab SOP’s
Befriend your Public Health Department Colleagues
Insert the Lab Medical Director centrally in the communication
Presentation of Emerging Infectious Disease cases in
community hospital Emergency Departments is not preventable
BUT
Mitigation of risk of disease transmission in the laboratory can be
implemented, and treating the patient is crucial.
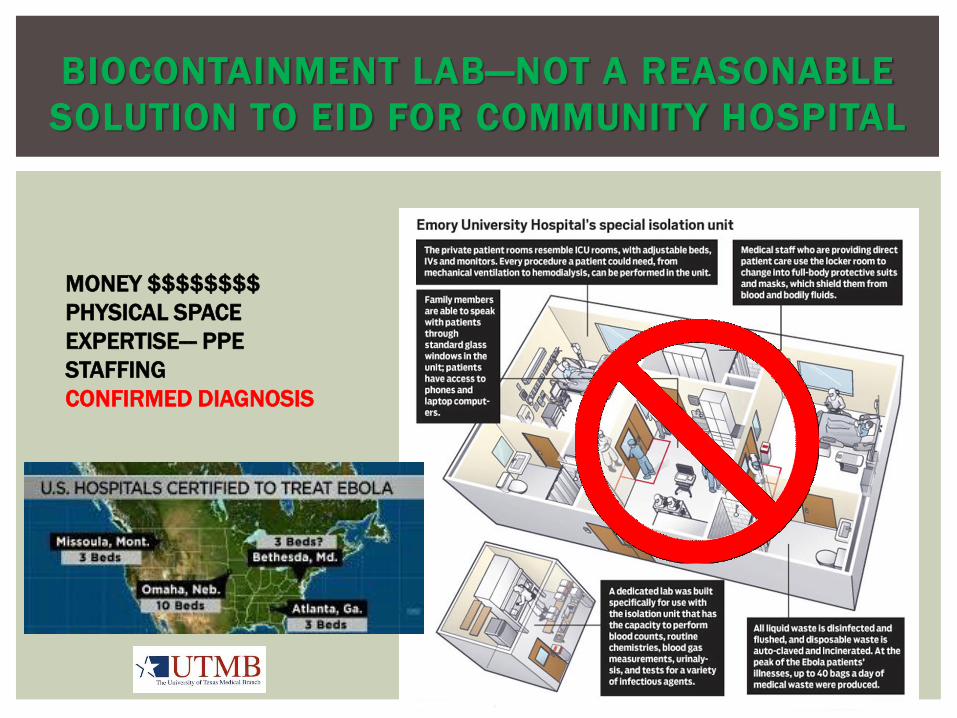
BIOCONTAINMENT LAB—NOT A REASONABLE
SOLUTION TO EID FOR COMMUNITY HOSPITAL
MONEY $$$$$$$$
PHYSICAL SPACE
EXPERTISE--- PPE
STAFFING
CONFIRMED DIAGNOSIS

Provide technical assistance
Ebola testing validated at Dallas LRN 10/2014
Provide personnel to assist with state and local public health
responses
Laboratorian from CDC
Epidemiologists for contact tracing
Public relations personnel
CDC LABORATORY RESPONSE NETWORK
MISSION: Maintain integrated national and international network of laboratories
that are fully equipped to respond quickly to acts of chemical or biological
threats, emerging diseases and other public health threats and emergencies.

Duty of an acute care facility
assess, rule out, and refer
Timeline to referral and disposition of PUI?
“Just in case” estimate— plan for 96 hours
SENTINEL LABORATORY
“The physician must be able to tell the
antecedents, know the present, and foretell
the future - must mediate these things, and
have two special objects in view with regard
to disease, namely, to do good or to do no
harm. “
Hippocrates

MMWR DECEMBER 12, 2014 / 63(49) ; 1175-117
CLINICAL INQUIRIES REGARDING EBOLA VIRUS DISEASE RECEIVED
BY CDC — UNITED STATES, JULY 9 –NOVEMBER 15, 20149
Among 33 recent travelers who tested negative for Ebola, alternative diagnoses
were available for 13, the most common being malaria (n = 5) and viral illnesses
(n = 4), including influenza. At least two persons who tested negative for Ebola
died from other causes. Based on reports from health departments and health
care providers, in several instances efforts to establish alternative diagnoses
were reported to have been hampered or delayed because of infection control
concerns. For example, laboratory tests to guide diagnosis or management (e.g.,
complete blood counts, liver function tests, serum chemistries, and malaria
tests) were reportedly deferred in some cases until there were assurances of a
negative Ebola virus test result. In other instances, radiologic studies, such as
computed tomography and ultrasound scans, or evaluation for noninfectious
conditions, such as severe hypertension and tachycardia, were reportedly
delayed while a diagnosis of Ebola was under consideration.

Chance favors the
prepared mind.
Louis Pasteur

BIOPREPAREDNESS --AMP MODEL
GETTING STARTED
Biorisk
Management
Assessment
→
←Performance
Mitigation
↑
Laboratory Biorisk Management,
2015 CRC Press
Encompasses specific risks during outbreaks as well as day-to-day operations
First considerations for working with a potentially
harmful microbe.
Precautions must be taken in the laboratory to
mitigate risk of transmission in daily operations.
•What physical spaces in the lab can be utilized?
negative air pressure room
closed centrifuge system
biosafety hood
•What protective equipment is available.
PPE- standard or high level
closed automated instrument systems
autoclave for waste disposal
•How would you contain the microbe to limit
contamination or accidental infection?
KNOW YOUR BUG!
Know your Lab Biosafety Level http://ABSA.org





LABORATORY BIOSAFETY LEVEL CRITERIA BIOSAFETY IN MICROBIOLOGICAL AND BIOMEDICAL LABORATORIES

Bacterial microorganisms
and safety classification
Although in the past
all risk assessment
was based on a rigid
risk and biosafety level
format, the new
biorisk protocols
incorporate the
traditional classes of
pathogen risk and BSL
information however,
do not rely solely on
these predetermined
risk classifications.

Route of transmission
Human-to-human or vector borne
Contact, droplet, airborne
Localization of infectious agent in the body
Which body fluids or tissues are infectious
Infectivity
High consequence pathogen?
Is prophylaxis, vaccine, or treatment available
What laboratory testing might be necessary
RISK ASSESSMENT
FIRST IDENTIFY RISK GROUP OF PATHOGEN
THEN
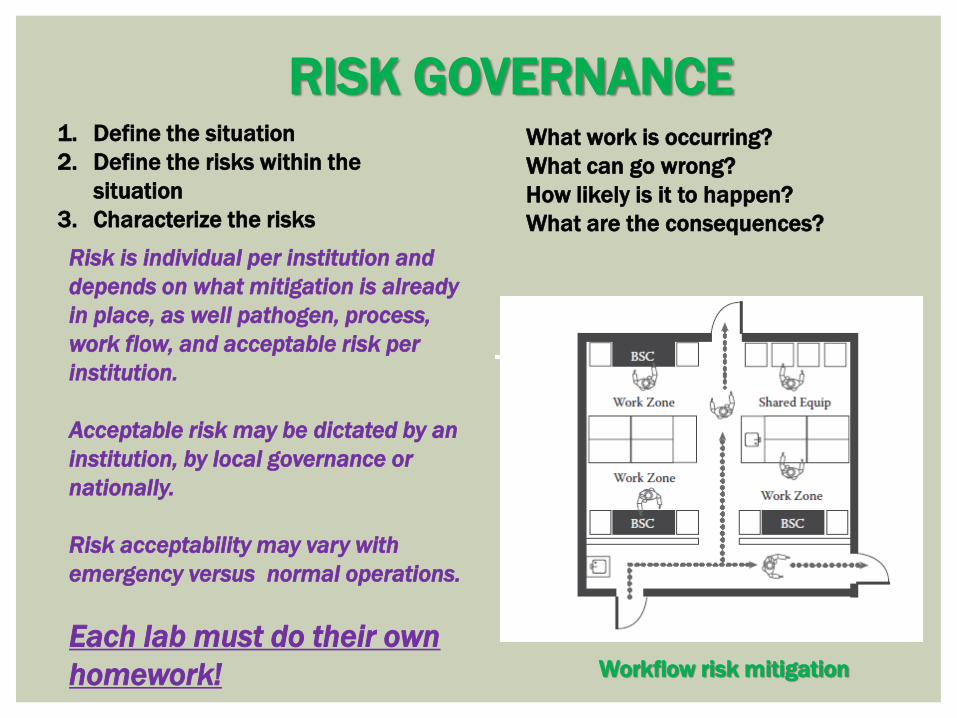
1. Define the situation
2. Define the risks within the
situation
3. Characterize the risks
What work is occurring?
What can go wrong?
How likely is it to happen?
What are the consequences?
RISK GOVERNANCE
Risk is individual per institution and
depends on what mitigation is already
in place, as well pathogen, process,
work flow, and acceptable risk per
institution.
Acceptable risk may be dictated by an
institution, by local governance or
nationally.
Risk acceptability may vary with
emergency versus normal operations.
Each lab must do their own
homework! Workflow risk mitigation
RISK MITIGATION STRATEGY
Mitigation Controls Include: Elimination
Removal of biorisk—ie: no testing performed in core lab
Substitution
Options— ie: POC in patient room only
Engineering controls- primary and secondary
Equipment—BSC’s, closed automation, alarms, badge swipes, sensors
Intentional removal of hazardous material from the laboratory
Administrative controls
Who will conduct work
Training
Acceptable behaviors
Practices and Procedures
Policies, SOP’s
Personal protective equipment
What level of protection is necessary for each task
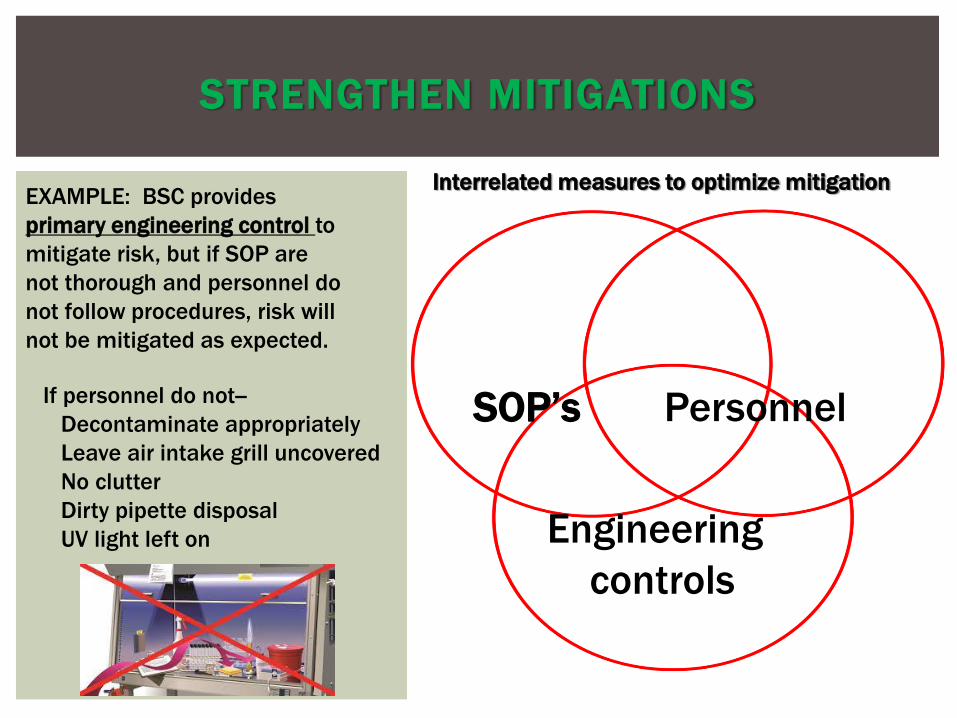
STRENGTHEN MITIGATIONS
SOP’s Personnel
Engineering
controls
If personnel do not--
Decontaminate appropriately
Leave air intake grill uncovered
No clutter
Dirty pipette disposal
UV light left on
Interrelated measures to optimize mitigation EXAMPLE: BSC provides
primary engineering control to
mitigate risk, but if SOP are
not thorough and personnel do
not follow procedures, risk will
not be mitigated as expected.

H i g h e n e r g y p r o c e d u r e s g e n e r a t e s m a l l e r d i a m e t e r a e r o s o l s Blending, mix ing with p ipet te, dropping samples, sonicat ion
1.0 -7.5 micrometer
L o w e r e n e r g y p r o c e d u r e s g e n e r a t e l a r g e r d r o p l e t s Centr i fuging, vor texing, sp i l l ing , shaking, p ipet t ing, pour ing, opening
>50 micrometer
Large droplets fa l l out of the a i r qu ickly contaminat ing work sur faces and equipment
Large droplets contaminate worker ’s hands, f ingers, and wr is ts
O n c e h a n d c o n t a m i n a t i o n h a s o c c u r r e d , p a t h o g e n s a r e e a s i l y t r a n s m i t t e d f r o m h a n d s t o m u c o u s m e m b r a n e s o n n o s e , e y e s a n d m o u t h . H a n d - t o - f a c e c o n t a c t ( H F C ) r o u t e o f e x p o s u r e i s p a r t i c u l a r l y i m p o r ta n t .
M i c r o b i a l a g e n t s h a n d l e d i n B S L - 2 a r e t r a n s m i t t e d b y i n g e s t i o n , p e r c u t a n e o u s i n j e c t i o n , o r d i r e c t c o n t a c t w i t h m u c o u s m e m b r a n e s r a t h e r t h a n b y i n h a l a t i o n i n m o s t c a s e s .
S t u d y o f 9 3 w o r k e r s f r o m 2 1 B S L - 2 l a b s , 5 6 % m a l e s , p r o f e s s o r s , p o s t do c s , r e s e a r c h f e l l o w s a n d a s s o c i a t e s , M D ’ s , g r a d u a t e s t u d e n t s .
S i t e s t o u c h e d → n o s e 4 4 % > f o r e h e a d 3 6 % > c h i n / c h e e k 1 2 . 5 % > m o u t h 4 % > e y e 1 . 7 %
7 2 % t o u c h e d t h e i r f a c e a t l e a s t o n c e , w i t h r a n g e o f 0 . 2 - 1 6 H F C / h r
LABORATORY GENERATED AEROSOLS
BIOSAFETY RISK
Eye and face protection should be mandatory for
pathogens with low infectious doses or agents with high
likelihood of direct contact transmission.
J Occupational and Environmental
Hygiene. Sept, 2014 625.-632.

Culture of biorisk management
Understand the science of implemented controls
Understand the consequences of failure to practice controls
Will not willingly circumvent engineering controls
Will not feel threatened by administrative controls
Institutional management must choose reliable employees
Physical competence
Trustworthiness
Mental competence
Emotional stability
Ability to uphold obligations for safety and integrity
STRENGTHEN MITIGATIONS
Personnel Behavior
Test orders: l imit testing/ timed/batch testing
Specimen collection: limit exposures
Specimen transport: no pneumatic tube
Processing of specimen(s): aerosolization?
Shipping of specimen(s): category A, who is trained?
Reporting: who and how? Logs
Medical staff communication: timely, who?
Waste and decontamination: city, county, state laws
STANDARD SOP’S FOR EID
STAFF AND ENVIRONMENTAL
RISK MITIGATION

Minimize test menu—disease dependent
Control test timing- Nursing colleagues
Control number of lab staff exposed
Provide written specimen collection guidance
Medical director should be involved with clinicians to guide
lab test utilization
This requires a medical director to interact with the clinical
team to determine necessity with a view towards acceptable
risk for lab staff.
TEST MENU CONTROLS
RISK MITIGATION
Ebola Test Menu recommendations:
CBC Malaria ABO Rh
Basic Metabolic panel Respiratory Panel Blood gas
PT/INR Blood cultures Urinalysis
LFT’s including bilirubin Rapid Strep Mg, Phos,
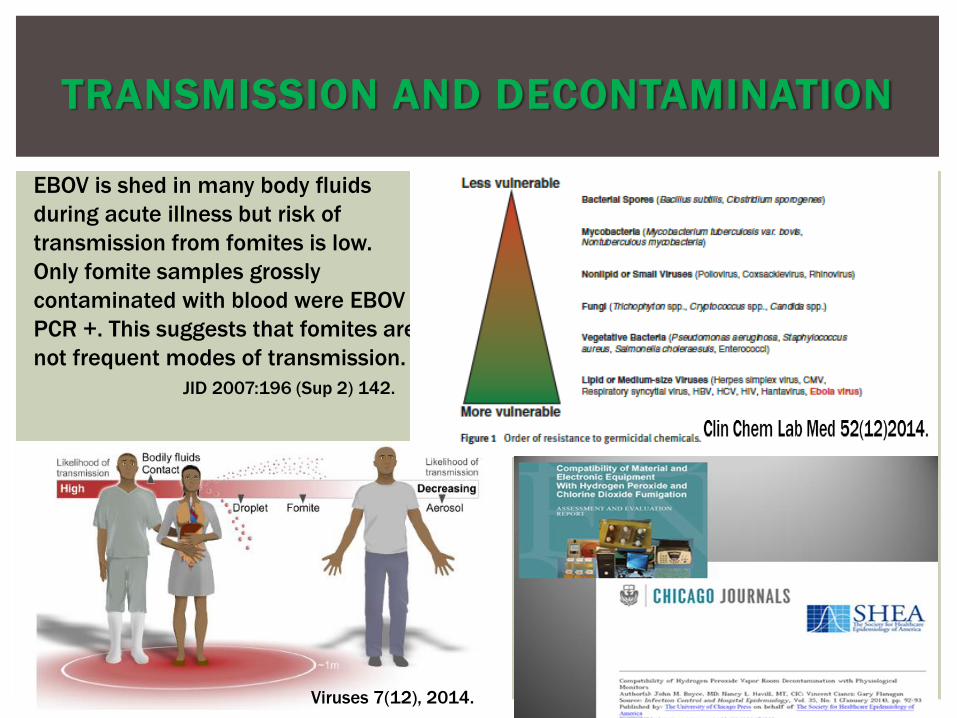
TRANSMISSION AND DECONTAMINATION
Viruses 7(12), 2014.
EBOV is shed in many body fluids
during acute illness but risk of
transmission from fomites is low.
Only fomite samples grossly
contaminated with blood were EBOV
PCR +. This suggests that fomites are
not frequent modes of transmission.
JID 2007:196 (Sup 2) 142.

EBOLA VIRAL DISEASE TRANSMISSION
Viruses, 7(12)2014

Initial PPE Recommendations Direct Care
Metamorphosis – Is More Better?

Exceeding PPE recommendations may actually increase the
rate of exposure.
Unfamiliar doffing techniques = self contamination
Extra gear can increase anxiety
Awkward movement, curtails activities
Train frequently, actual donning and doffing performance
Train only those who are willing volunteers for high level PPE
Always have a PPE buddy
PPE CONTROVERSY
MORE IS BETTER---NOT ALWAYS!
Ann Intern Med. 2014;161(10):751-752.

PPE
Overkill?
High risk?
The Dallas Ebola event demonstrated how a laboratory facility
without a biocontainment lab could implement risk mitigation
measures to ensure the safety of the laboratory staff and lab
environment while providing excellent diagnostic care for the
Ebola stricken patients.
Flexibility and adaptability are paramount in daily operations
Use of elimination and substitution controls were used as well
as primary engineering controls, administrative measures,
new and revised procedures and PPE training.
Personnel were volunteers, carefully chosen
OPTIMIZE BIORISK MITIGATION
Heroic phase— action heroes and ADRENALINE
Honeymoon phase—people pull together united
Fatigue/Conflict– every man for himself, blame
PTSD/Recovery– lessons learned, anxiety situations
MAKE SURE TO
1. Set boundaries, send people home
2. Emphasize teamwork
3. Provide guidance and emotional support
EMOTIONAL RESPONSES TO CRISIS
•Create opportunities to express concern
•Inspire personal safety
•Provide resources for response
•Address loss of revenue/liability
•Control speed of information flow
•Anticipatory guidance
•Answer queries :family’s safety
HEALTHY LAB ENVIRONMENT
IN CRISIS
Listen to staff concerns
Address the science--factual, candid, uncertainty
Update, be visible, be transparent
Frequent updates build trust and manage expectations
Open communications dispel rumors
Rumors in your own lab and in the community
Social support—personal stories
Psychosocial consequences can be extremely stressful
Thank your staff—
Laboratorians, the unrecognized heroes
CRISIS COMMUNICATION
EARLY AND OFTEN
As laboratory scientists, healthcare workers, and
humanitarians we have a moral duty to aid the sick and dying,
albeit with minimal risk to ourselves.
This can be accomplished by careful consideration of the risks,
with implementation of biosafety controls and protection.
Globalization has introduced many new as yet undiscovered
diseases as well as environmental and anthropogenic changes
that allow ancient or well known diseases to become endemic in
new global regions.
We cannot remove ourselves as laboratory scientists from the
risk of encountering an emerging infectious disease, thus we
must be prepared to encounter them but kept safe.
Bev Dickson, 2014 USA Ebola Event Participant