Pulmonic Stenosis, Ventricular Septal Defect, and Right...
8
Pulmonic Stenosis, Ventricular Septal Defect, and Right Ventricular Pressure above Systemic Level By J. I. E. HOFFMAN, M.D., ABRAHAM M. RUDOLPH, MI.D., ALEXANDER S. NADAS, M.D., AND ROBERT E. GROSS, M.D. IT IS USUALLY possible to distinguish pulmonic stenosis with an intact ventric- ular septum (designated as pulmonic stenosis) from pulmonic stenosis with a right-to-left shunt through a ventricular septal defect (te- tralogy of Fallot) by routine clinical, electro- cardiographic, and radiologic examination.1-3 If the diagnosis is still uncertain, it can as a rule be made by phonocardiography and car- diae catheterization,4 particularly if there is very severe pulmonic stenosis with an intact ventricular septum. Characteristically in se- vere pulmonic stenosis the right ventricular systolic pressure is much higher than in the systemic circulation and rises still higher after ectopic beats; the right ventricular pressure tracing is triangular; and right ventricular systole is prolonged so that on phonocardiog- raphy the second heart sound is widely split and the systolic murmur passes beyond aortic valve closure. Unfortunately these commonly accepted criteria may be unreliable. In this paper 10 patients are reported who, although meeting most or all of these criteria for the diagnosis of severe pulmonic stenosis (espe- cially with systolic pressures much higher in the right ventricle than in the systemic ar- teries), nevertheless were proved later to have an associated ventricular septal defect with a right-to-left shunt. An attempt is made to in- dicate how even under these circumstances a correct preoperative diagnosis may be made. From the Sharon Cardiovascular Unit, Children 's Medical Center and the Departnient of Pediatrics, Harvard Medical School, Boston, Mass. Supported in part by a grant (H-2515) from the National Institutes of Health, U. S. Public Health Service, a grant-in-aid from the American Heart Association, and the Massachusetts Heart Associationi. Dr. Rudolph is an Established Investigator of the American Heart Association. Material and Methods These 10 patients were admitted to the Chil- dren's Medical Center for investigation and oper- ation, and all but 1 were seen after June 1957. Cardiac catheterizations as described previously from this laboratory5 were done in all, and phono- cardiogranms were taken with a Sanborn Twin- Beam photographic recorder. Results Clinieally all of these patients had onie or more signs suggestive of valvular pulmonic stenosis with an intact ventricular septunm. There were large "a" waves in the jugular venous pulse in 4; the systolic thrill in 7 anid the stenotic systolic murmur in 8 were maxi- inal at the second or third left intercostal space; the second heart sound was thought to be widely split in 4; and 2 with elinically se- vere pulmonic stenosis had no eyanosis. The electrocardiogram showed P pulmonale in 6 and muarked right ventricular hypertrophy in all 10 the R waves in lead V, were 20 to 30 mm. high in a and over 30 mm. high in 4. On x-ray, 8 had cardiae enlargement (marked in 4) and 4 had what was initerpreted as post- stenotic dilatation of the pulmonary artery. Any of these signls may be found in an other- wise classical tetralogy of Fallot but all of them individually or together favor severe valvular pulmonic stenosis with an intact ven- tricular septum and high right atrial and ventricular pressures. Cardiac catheterization supported the diag- nosis initially when right atrial pressures over 10 mm. Hg were found in 7, and in all 10 the right ventricular systolic pressure was above systemic levels. In 1 the right ventricular sys- tolie pressure of 125 mm. Hg was only 15 mm. Hg above that in the brachial artery, but in all the others it ranged from 150 to 250 mm. Hg, with a systolic gradient between right Circulation, Volume XXII, September 1960 405 by guest on June 27, 2018 http://circ.ahajournals.org/ Downloaded from
Transcript of Pulmonic Stenosis, Ventricular Septal Defect, and Right...

Pulmonic Stenosis, Ventricular Septal Defect,and Right Ventricular Pressure above Systemic Level
By J. I. E. HOFFMAN, M.D., ABRAHAM M. RUDOLPH, MI.D.,ALEXANDER S. NADAS, M.D., AND ROBERT E. GROSS, M.D.
IT IS USUALLY possible to distinguishpulmonic stenosis with an intact ventric-
ular septum (designated as pulmonic stenosis)from pulmonic stenosis with a right-to-leftshunt through a ventricular septal defect (te-tralogy of Fallot) by routine clinical, electro-cardiographic, and radiologic examination.1-3If the diagnosis is still uncertain, it can as arule be made by phonocardiography and car-diae catheterization,4 particularly if there isvery severe pulmonic stenosis with an intactventricular septum. Characteristically in se-vere pulmonic stenosis the right ventricularsystolic pressure is much higher than in thesystemic circulation and rises still higher afterectopic beats; the right ventricular pressuretracing is triangular; and right ventricularsystole is prolonged so that on phonocardiog-raphy the second heart sound is widely splitand the systolic murmur passes beyond aorticvalve closure. Unfortunately these commonlyaccepted criteria may be unreliable. In thispaper 10 patients are reported who, althoughmeeting most or all of these criteria for thediagnosis of severe pulmonic stenosis (espe-cially with systolic pressures much higher inthe right ventricle than in the systemic ar-teries), nevertheless were proved later to havean associated ventricular septal defect with aright-to-left shunt. An attempt is made to in-dicate how even under these circumstances acorrect preoperative diagnosis may be made.
From the Sharon Cardiovascular Unit, Children 'sMedical Center and the Departnient of Pediatrics,Harvard Medical School, Boston, Mass.
Supported in part by a grant (H-2515) from theNational Institutes of Health, U. S. Public HealthService, a grant-in-aid from the American HeartAssociation, and the Massachusetts Heart Associationi.
Dr. Rudolph is an Established Investigator of theAmerican Heart Association.
Material and MethodsThese 10 patients were admitted to the Chil-
dren's Medical Center for investigation and oper-ation, and all but 1 were seen after June 1957.Cardiac catheterizations as described previouslyfrom this laboratory5 were done in all, and phono-cardiogranms were taken with a Sanborn Twin-Beam photographic recorder.
ResultsClinieally all of these patients had onie or
more signs suggestive of valvular pulmonicstenosis with an intact ventricular septunm.There were large "a" waves in the jugularvenous pulse in 4; the systolic thrill in 7 anidthe stenotic systolic murmur in 8 were maxi-inal at the second or third left intercostalspace; the second heart sound was thought tobe widely split in 4; and 2 with elinically se-vere pulmonic stenosis had no eyanosis. Theelectrocardiogram showed P pulmonale in 6and muarked right ventricular hypertrophy inall 10 the R waves in lead V, were 20 to 30mm. high in a and over 30 mm. high in 4. Onx-ray, 8 had cardiae enlargement (marked in4) and 4 had what was initerpreted as post-stenotic dilatation of the pulmonary artery.Any of these signls may be found in an other-wise classical tetralogy of Fallot but all ofthem individually or together favor severevalvular pulmonic stenosis with an intact ven-tricular septum and high right atrial andventricular pressures.
Cardiac catheterization supported the diag-nosis initially when right atrial pressures over10 mm. Hg were found in 7, and in all 10 theright ventricular systolic pressure was abovesystemic levels. In 1 the right ventricular sys-tolie pressure of 125 mm. Hg was only 15 mm.Hg above that in the brachial artery, but inall the others it ranged from 150 to 250 mm.Hg, with a systolic gradient between right
Circulation, Volume XXII, September 1960 405
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from

4IJOFFMJAN, RDI)()LP,ll NADAS, C'-ROSS
PLMWtC Srum TETRALOGY OF FALLOT
ATYPCAL: TETRALOGY OF FA.OT
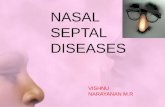
Figure 1Right ventriculaur prnssunrc curtvs 'thi slinul/nacomtt o/i sprf,,,4,surc rlUrrcs (top) avdbr-achial arcfryi pressure cutr i-c (bottom).
venitriele arid systemiciartery of 35 to 120 nim.1ig. An iIntact ventriclular septum was furtlhersuggested wheni in 7 the right ventricular sys-tolic pressure rose 15 to 40 nun. lfg Wabove itsprevious level after a premature leat; in theothier 3 right ventricular prIessiur-es werie niotrecorded during premature beats.The siape of the rihlt ventriCLalrt1 prcss1uri-
cUrVe was rouIgh'ly triaiigular (fig. 1) as foUnldin pulmotnie steniosis but n1ot in tetralogY ofFallot. In 6 the ratio of the curve width 20per cenit above the inidsystolie pressuire to thewidth 20 per cenit below it was smnall anld wellunder 0.70, the lower l:imit of the ranlge estab-lished for tetralogy of Fallot;4 ill the other 4the value of the ratio fell in the zone commnonrto both groups.
Despite this cumulative evidence of severe
p)U1linoitiC stenosis atll 10 patienits had venttric-lar septal defects witlh right-to-left shunts.
This was provedi preo)peratively itn 2 by pass-iiug the, catheteri fromi righit v (litriele to aortathroulgh tle defeect. T4i thlese 2 as well as iii.) other patienits, inlicator-dilution curvessshoweTd a righIA-to-left shulint at the ventricularlevel; ini 2 of these ttie shun-ft was shown byinijeetions made iinto the bod3 of time right vei-triele but nlot into the infundibuluni. TIdica-tor-dilutioii curves were also donie irn 2 of theremainingg 3 patients aiilI sliowedl a riglht-to-left slhunt at the atrial buit not at the veuitric-ular le-vel. The magnitude of these right-to-leftshunts varied widlely, so that systemic arterialoxyge.n saturation raniged froimi 47 to 93 percent; in 6 of the 1.0 it was betwveen 80 and 89ter cenit.
Circulation, Volume XXII, September 960
46
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from

I IjAINICTSTEN SS 407
RV mnt RV body LV
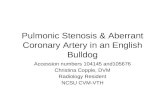
rigure 2Elect 10(0 rtio'7,rams(t(o)p), ext{ernal phonocarclworams (eenter), and pressure curees(b4tt-oiti) to show that thc notch1 in the (tsr nth limb 0! the rigiht uentricular bodyprA'r.sSaTu Carfer Ociafccr (t thU be',ld rt' the sq/t4oli(,hpr ss.a in tie right rentricalar inflan-dtibnld or thU 1(- ft rtaftrich XVotr' als,O thc eaulgJ dia(mond-slhaped mai'mar.
T[here was a notchl or aibrup)t chiange in di-rectioi of the, ase.ndling limib of thie right VenI-tricular pi1essure cur-ve mn l; thlis inotct alwvaysoeccurred about the, level of the. svstemiiie svs-tolie pressure, aIndl wvas also near tite systoliePressure ill thie infundfibular chamnber in. 3(figt. 2).
At; cardiae eatliet erizat ilol the site of thesteniosis wvas ktdgeId to be (lefinitely valvulara8ll(;ifliiitliluular in. 3, valvular and(I possiblyinfundibular in 3, anI( i ifundibilar alone ill2' itn. 2 the pulinoii,ay arter.1-y was ntlt entertledtl)lt einealnni'ooram in I siowed atn iiiftndlibu-Jar ehamtber. Four shiowed a zone of negativepressiure as thie eathieter ti) passed fr1omii thepulniinay ar.tery to atid(i through the stenotiea'rea (BernlOntil Iielet) an(d I of these was a
?atielit wN"ithL pureI'0 inIfuuibiilaclr StenToSiS.Plhonoeardiograims were t-aken in all these
)atients (fig. 3) Thie first- hleart so80111( w-asnormn-ally1 split in all calld was eitlher normal orrXeduleced in intensity. Five biadl a swstolie eliekP.US to 0.14 secund after the beginn1-in:fg of tlefirst lheart sound; in 3 this eliek vas otloder.-int expirationi itt I it incr-eased (iulling intsJ)irat-tion atd in 1 dlid no-t chlan}ge in intensity withlr-espiration. Four hadsof(Jt thiird lhea-rt soundsCirculation, Volume AXX', Sept(cnbcr 1960
anld 8 bad fourth he,-art soulnds of sliglht tomarked inrteniisity.
Ident-fleat ion of the 2 components of theseeonid lheart somnd may be diffieult if pul-miioinie closuilrc is -very soft antd is obscured bythe systolic murntur passing beyond the aortic(losingr soulld and-( if the absen'ce, of a suiitableexternal refere-nice makces it difficult to be sure
thlat a smial. lvbtion dloes inideed representl)ulmooiie closure. Iln 6 the seeond heart souindwas regarde(ld as, sintle or narrowly split (upto 0.03 seconitl) 111id in 4 it was probably wide-ly split (0.06 to 0.10 seconid).
rElie systolic( niniuriiiiii was dliamond-shiaiedin 9 anld decrescenlo in 1I but hadl many varia-tionis in conifiguratilon. tIn all it began imme-diately or shortly after the first heart sound,which was alway-s distinct, and it begran beforetile svstolie elick ini tile 5 whio had it. Iin theml-ost severelv affected patient there was a softlecereseneado systolit imurmur enrlitig at or be-fore tile single seconid heart sounid (fig. 3C).In 3 thie systoli c mnurmur inervaset';l ralpidly toa mnatxinrnu ini thle fitst quarter of systole, e-mauited at thiis intensity for a sihort timtie, anidtfll-n (ecreased(1 to eltd at or beyond the secoindIlert souutdtl (fig. 3-)-F). Four othfers (fig. 3(-0
i
47
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from

4I1I/'FMAN. RIDOLPIlI, NAI)AM, (Il)RSS
I
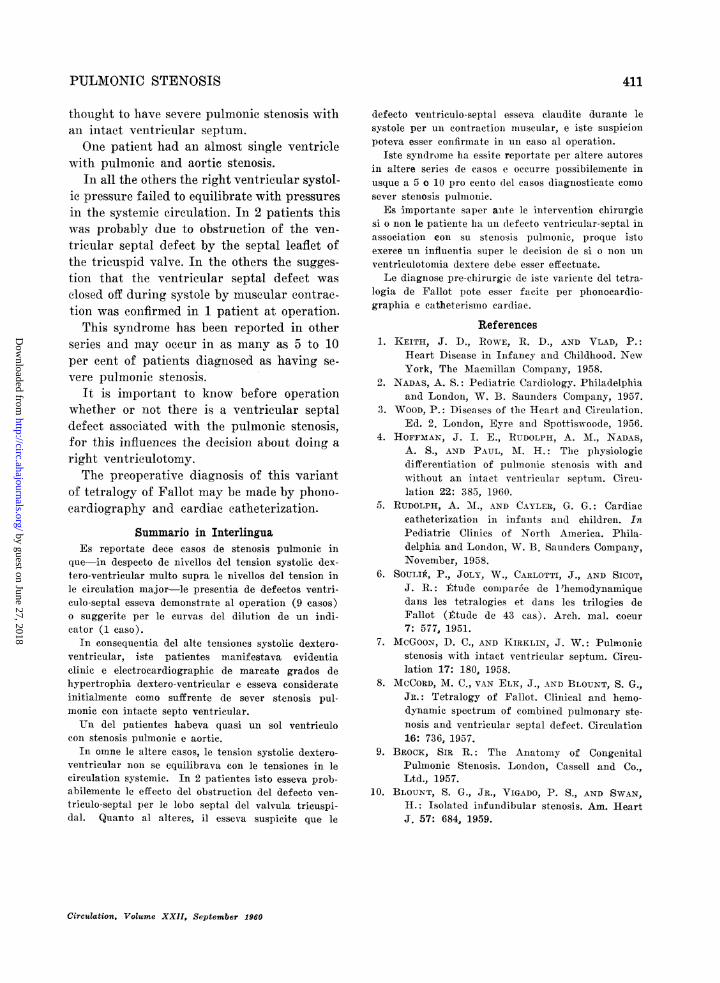
Figure 3I1ho oe,oardiot;rt /s. A:. '1 /])pictt pu1 10//it StI 1/05/s.
1B. h'1 it ftt/el f icy/ of Fu/lot. (2 Pa/titit/s 11/
ti/is st /iis. ,21 IS, secondti left i//it/S2 1 ost l)f ptac ;tI1S, fourth it f i/te /cstasil sp)t (5'; Sj, first heart
SO/f1 /l; S s eo/ /ti bc/irt so/f/lti; S /of /rth heartfso/lnf/t; Sil,M //slfttoliti C1//f//o; S(, sytolic cHitck.
) iamove typilc-al diaimi(i1-shiape( systolic
mnI rnulIs that iievertlmeIls(I s were: mnaximiialearlv in svstole, so thalt t hex resembled a kit eIying onri its side wvithI its tail poil/.thing towardthe 2 of tfi/sc Iurimlri/rs enlded at, and
2 enledl afterr thlie semolld hteart so/ntid. Finlallvy2 hadl sylni/eti ial (liamond-shiaped systolic
1iiirs withl their maxima iii. miidsvstole,I/lIt 1 elded well before the seeond heart soliudali dtfeatolcr at or inst 1/cyomd it (figr. 3K and(lL); in ea/li, sf/I/I ot)mi)le\es di liave early
dliInlolth-shapl)cd miunurirs.
A.natoimi(c details were not (-.td at open-heart
(oper,ation in 9. All had inifumalibular stenosis,NvIhie wvas suggrested 'b> the low intravalvullar
positioll of thie thrill aHid in at least 8 y at
indenltation in the right -venitricular outflowtrliact somyie dlistaeiee below thie pilltlhoIia >valve; in addition there}were 4 w-ithi valvuilarlsteniosis an(d thrilis in the pulitiloiarv artery.One patienit had a correeted transpositionnwiththe right ventriele aiteriorly anid oii the ( pa-tient s ) left atndl the pulilonar>r artery ellnerg-wii'g to the right of an(] poster ior- to the ;aortai.'I'lis patient hladi whait was alinost a sing-leventriteile wt the lower tliree quailters of thIeventricula141<r sep)tIumn1 m1is.sig11(1a wdwithl -martke(l1i111i(iselar1 Ihvpertrophy b)el()0Xow the pIllnon1ar>vaan.d aortie. valves. Alt th.e othiers iad(1 higlInelni/ira nou,s venit etio lar stl;eptal defteet s; one otthlese was reeor:ded as being '`qiqite small,' 8
1l.lj(: t\ (f 0.;-) to 1 .( (,1l 11.2 l4 1le 1ha ra of05tI 10tn- and 4 hadi areasof 1.' to 29.0 (,III.2
DiscussionIn 1951 Sol ie, Joly, (a1arlotti, andS>olt
tdeserib)ed rigidvetvelltri-icla i systol ie j)pissutresabove systemni(e- 'levels in 3 of 22 patientsxwitltetralogxv of Fallot. MeGoon ami -(1 Kirklin IIIrepor,ting 32 patients with ''an essen-tiaillt y in-taet vxen.trieillar septum,n,'' mnentioned 1 patieiitwith a ventri-icul:ar sept:al defect and an ahnor-niallv higlh righlit vontrienilar pressure. In ourseries 9! of 10 patient;s were seen in. a periodwlhen tahoit 235) patients with pihilmonie stenosisal'li about 35 with tetralogy of Fallot werecatheterized. In the same period soine withtetralogy of Fallot and a fewr writh puflmoniestenosis were operated on withouit cardiaccatheterization and many others in bothgroups were seen hult niot. operated on. Theremia- be still rmore patients with this syndromewhio have been diagiiosed as piilmoniie stenosisand(] inxwhoin the error has not yet been this-covered, but even witlhouit themn this varianitof fetralogy of- Fallol seemns to he relativelyto/lu/mon.
Physiologic Mechanism
Tn tetralogv of Fallot ther-e is us-uially rapidlpl ressu,e e quiTlibrium across the ventricularseptal defect so that systolic pressures ini theright aiid left ventricles anid aorta are similaranid rise slightly or not at all after ectopiebecats, rixght anid le]ft ventricular pressure
Circulation, Volunme XXIi, Scptvmber 196(/
408S
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from

1IL N I C STrENOS-4(S
tt-iriit(gs liave similar shapes vith almost par-allel sides and flit or romute(l tops, amid( vel-trienlar ejeetimn etitis at alIGot the samhfe tieill two ventl'ieldes. Conseqenpetly the secon(dlheailrt soit is single oi- itarrol x Split allnd thesvystolie minr mi. d(oes tot imass beyond aortieaT.lVe clo(sujre.4 Byvcotrast, all 10 patietitsreporXted herel̂ aet:\eil as if thle velitrietilat1<4 sep-tintwEere itttaet, int that the tight Ve1tlielecoll(1 gleIletrate a-I sy-stolie press-ure hig-her- tha.-ittliat; ill the svstetoie eil-au!lsItiott attd(ottld fill-ttfiter elevtte tlhis aftet- eetop)i beats. lit a o-oupof patientits with tetr-aloyrv of Fa0lot stuIdlied inltlis laboratory, 30 m.m. 1g wvas about theittaxoitto-ll.l (differ,ettec founi.d betwN-een right veti-trielalm-r atdtsvstlenie aruterial svstolie piesslilels Whenl sVstolie p-ressures ill the r-igTht veIn-triele andl aiorta wer,e alm.ost identicall, so that(lifferett(ees grn.eater than this probably. ilndicatesome. failtre of pressre equilibraitioll h)et7e,et(tthe twio ventr-icles. In the onie patienit wjTi tt asystolie radlient of onily 15 niiin. ITg betweetnrigholit ventriele atid systemie artery evideneeof ani intalct septiui was inferred fronti a 25"mino. JTi rise in right ventricular systolie Pres'sore after ectopie beats and fromii the (lenioii-stratiott of a widlely split second heart souttdwvitlh the, systolic inurntuir eniding after aortievaIlve closure. Tli this patient, too, as well asitt 5 others, tlte shape of the riglht vetitrienairMPreSSutre curveswas typical of pulinonic ste
ttosis.Tltis failure of ral)id pressure equilib)rationi
aeros-Ss tlte veittrieular septal defet suiggeststhat thie vetiticlar selittm mav be futlctioll-allyv initatt dliruing ialt- or all of sy-stole anl.dthl(e following J)ossihle reasons based ott oilrexperi cie witlth these 1T patients mayv be ad-
need1. The defeet tayv be occludled by the septal
IWa/flet of the tricuspid valve. In one patienitat autopsy this leaflet had ain anomalotis 1ri-gint frioi thte i-imarginl of the ventricular septal(lefeet (fi(g. 4) aid couldl eoneeivalyfir hfazerve ob-strtitetl it (lutiiit systole. Inl anlother patientat opteratioi the tricuspid val.vAe leaIfflet mwasfolnldl to he 1p)artly adherent to the rimn of thedefeet.
RVSD
i.RV
Figure 4kigh l tea/toitle sholviny.NIittJ tUa//nt//li/'js(i / o1/
ttiettri)uip 1711,ftell t /tfrt/ the vt/l/Qit/ aJ thete't/ict?/11/1 se.T}t/ deftect. 1A', riyht atrium; I/,Vriuhit rottic/e; 1VSD-I, retric u/ar septti d/otft.
2. 1If thte ieifet is ver> sttttllt1lttt pllt¾ess-iiteqitililbration011 ass it eoitld he dIelaved. Souiattd htis lolleagtles" ii iroke(d tltis exlattatiotill pattieiits Nh itll tlissvtltdrolltte whto tad ittilltiotal right1t-o-left Shtittts attld 2leCord, vatlElk, attd l lointt fonitt(d a. d e tect ittitli. iII di-tIteterittl thtell patiellt . 4 ltI 2 pal ieltts IliMITt1- se11ries had small defects, thottgllt 1 ot(d I1tshad att arterial oxygen s,attiratioti l 8 1(If2 I'
3. If thIte lefe(et is siftl atedl itt 1t t it i1tt 'lililitr e1alltaber, it illtav become isolafed fromtttlte lhodv of the irigylht vent,ricle dnrittg. systo!caIJtd thits maIy itIot he attIc to deeon press it.TIhltis may have oe(eiirredl in 1 patient CretPotedsl,<Aitj(j(})l 81(t J\;-jllsli7 J)Ut IVf1S 11(t- 'vllby AlcGloon an b Irkit u a tt ot
itt o01r series.4. It is possiile that the vettrttietlat selptal
defec t eould be ocel toted by ilt- raltioln oftlte ]In perftrojpieid mtttsele of ttle septlni amltItite eristca snr {ttritlaris so thafit toxxardl
Circuelation, Volumac XXII, September 11960
409t
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from

HOFFMAN, RUDOLPH, NADAS, GROSS
the end of systole the ventricular septumwould be effectively closed. Recently, proof ofthis hypothesis was obtained in one of thesepatients at operation. The right ventricle wasopened while the circulation was maintainedby the pump oxygenator; the heart was notstopped. With each contraction the ventricu-lar septal defect was squeezed closed by thehypertrophied muscle around it and the in-fundibular chamber was cut off from the bodvof the right ventricle.One or both of these events might have
caused the notch in the aseending limit of theright ventricular pressure tracing in this pa-tient and 6 others. A similar notch was notedonly once in pulmonic stenosis in a patientwith marked infundibular stenosis.
Preoperative Diagnosis
Accurate preoperative diagnosis of this le-sion is essential in indicating the need for sur-gical repair with extracorporeal circulationrather than with hypothermia and in makingright ventriculotomy mandatory. Phonocar-diography was of great help in suggestingthat these patients did not have pulmonic ste-nosis with an intact ventricular septum inas-much as (a) the systolic murmur was maximalearly in systole, whether or not it passed be-yond aortic valve closure or (b) the systolicmurmur ended before a single or closelv splitsecond heart souiid, whether or not the mur-mur was maximal early in systole. It is truethat in mild pulmonic stenosis right ventricu-lar ejection may not be prolonged so that thesystolic murmur may be maximal in midsys-tole and end at the aortic component of anormally split second heart sound, but thesepatients will not show the features of markedright ventricular hypertrophy.
These phonocardiographic criteria may nothold if there is puluonic stenosis and ventric-ular inversion (corrected transposition).Three patients with this syndrome have beenseen with phonocardiograms typieal of tetral-ogy of Fallot but with no evidence of an asso-eiated ventricular septal defect on cardiaccatheterization. The diagnosis has not yet beenproved at operation. anid until then phono-
cardiograms in this syndrome should be inter-preted with caution.
If after clinical, radiologic, and phonocar-diographic examination cardiac catheteriza-tion is required, it is obvious that in patientswith pulmonic stenosis complete reliailce toexclude an associated ventricular septal defectcannot be placed on a high right ventricularsystolic pressure that rises further after ec-topic beats and on a triangular right ventric-ular pressure curve. The only direct preopera-tive demonstration of this defect is thepassage of the catheter through it from theright ventricle to the aorta; failing this, indi-cator-dilution studies or angiocardiographyshould always be done. The site of injection ofthe indicator or radiopaque dye is important,for if it is injected into the infundibulum orinto a stream that does not pass through thedefect, the right-to-left ventricular shunt maynot be revealed. This happened in 2 of ourpatients with arterial oxygen saturations of89 and 93 per cent, in both of whom rightatrial injection showed a right-to-left shunt.Failure to demonstrate a right-to-left ventric-ular shunt by these technics, especially whenthe arterial oxygen saturation is near normal,is thus not unequivocal evidence of its ab-sence. Another possible source of error occurswith marked tricuspid regurgitation and aright-to-left atrial shunt, for then indicatorinjected into the body of the right ventriclemight be swept back into the right atrium andthen across to the left side; a good angio-cardiogram should help to avoid this error andhas the additional advantage of demonstratingthe anatomy of the outflow tract of the rightventricle.
SummaryTen patients with pulmonic stenosis are re-
ported who, despite having right ventricularsystolic pressures much above systemic levels,had ventricular septal defects proved at opera-tion in 9 and suggested by indicator-dilutioncurves in the other.
Because of the high right veentricular sys-tolic pressures these patienits had clinical andelectrocardiographic evidence of marked rightvenitricular hypertrophy and were initially
Circulation, Volume XXII, September 1960
410
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from
PULMONIC STENOSIS
thought to have severe pulmonic stenosis withan intact ventricular septum.One patient had an almost single ventricle
with pulmoinic and aortic stenosis.In all the others the right ventricular systol-
ic pressure failed to equilibrate with pressuresin the system-ic circulation. In 2 patients thiswas probably due to obstruction of the ven-tricular septal defect by the septal leaflet ofthe tricuspid valve. In the others the sugges-tion that the ventricular septal defect wasclosed off during systole by muscular contrac-tion was confirmed in 1 patient at operation.
This syndrome has been reported in otherseries and may occur in as many as 5 to 10per cent of patients diagnosed as having se-vere pulmonic stenosis.
It is important to know before operationwhether or not there is a ventricular septaldefect associated with the pulmonic stenosis,for this influences the decision about doing aright ventriculotomy.The preoperative diagnosis of this variant
of tetralogy of Fallot may be made by phono-cardiography and cardiac catheterization.
Summario in InterlinguaEs reportate dece casos de stenosis pulmonic in
que in despecto de nivellos del tension systolic dex-tero-ventricular multo supra le nivellos del tension inle circulation major-le presentia de defectos ventri-culo-septal esseva demonstrate al operation (9 casos)o suggerite per le curvas del dilution de un indi-cator (1 caso).In consequentia del alte tensiones systolic dextero-
ventricular, iste patientes manifestava evidentiaelinic e electrocardiographic de marcate grados dehypertrophia dextero-ventricular e esseva considerateinitialmente como sufffrente de sever stenosis pul-monic con intacte septo ventricular.Un del patientes habeva quasi un sol ventriculo
coin stenosis pulmonic e aortic.In omne le altere casos, le tension systolic dextero-
ventricular non se equilibrava con le tensiones in lecirculation systenmie. In 2 patientes isto esseva prob-abilemente le effecto del obstruction del defecto yen-triculo-septal per le lobo septal del valvula tricuspi-dal. Quanto al alteres, il esseva suspicite que le
defecto venitriculo-septal esseva claudite durante lesystole per uni contractioni muscular, e iste suspicionlpoteva esser confirmate in uIi caso al operation.
Iste synidrome ha essite reportate per altere autoresin altere series de casos e occurre possibilemente inusque a 5 o 10 pro cento dcel easos diagnosticate comosever stenosis pulmonie.Es importante saper ante le intervention chirurgic
si o non le patienite ha uin defecto ventricular-septal inassociation con su stenosis pulmonic, proque istoexerce un influentia super le decision de si o noin univentriculotomia dextere debe esser effectuate.Le diagnose pre-chirurgic dce iste variente del tetra-
logia de Fallot pote esser facite per phonocardio-graphia e catheterisiiio cardiac.
References1. KEITH, J. D., ROWE, R. D., AND VLAD, P.:
Heart Disease in Infaney and Childhood. NewYork, The Macmillan Coampany, 1958.
2. NADAS, A. S.: Pediatric Cardiology. Philadelphiaand London, W. B. Saunders Company, 1957.
3. WOOD, P.: Diseases of the Heart and Circulation.Ed. 2. London, Eyre and Spottiswoode, 1956.
4. HOFFMAN, J. I. E., RUDOLPH, A. M., NADAS,A. S., AND PAUL, M. H.: The physiologicdifferentiation of pulmonlic stenosis with andwithout an initact ventricular septum. Circu-lation 22: 385, 1960.
5. RUDOLPH, A. 3I., AND CAYLER, G. G.: Cardiaccatheterizationi in infaants and children. InPediatric Clinics of North America. Phila-delphia and London, W. B. Saunders Company,November, 1958.
6. SOULIE, P., JOLY, W., CARLOTTI, J., AND SICOT,J. R.: Rtude compar6e de 1 'hemodynainiquedans les tetralogies et dans les trilogies deFallot (Etude de 43 cas). Arch. mal. coeur7: 577, 1951.
7. McGooN, D. C., AND KIRKLIN, J. W.: Pulmonicstenosis with intact ventricular septum. Cireu-lation 17: 180, 1958.
8. MCCORD, M. C., VAN ELK, J., AND BLOUNT, S. G.,JR.: Tetralogy of Fallot. Clinical and hemo-dynamic spectrum of conmbined pulmonary ste-nosis and ventricular septal defect. Circulation16: 736, 1957.
9. BROCK, SiR R.: The Anatomy of CongenitalPulmonic Stenosis. London, Cassell and Co.,Ltd., 1957.
10. BLOUNT, S. G., JR., VIGADO, P. S., AND SWAN,H.: Isolated infundibular stenosis. Am. HeartJ. 57: 684, 1959.
Circulation, Volume XXII, September 1960
411
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from

ROBERT E. GROSSJ. I. E. HOFFMAN, ABRAHAM M. RUDOLPH, ALEXANDER S. NADAS and
above Systemic LevelPulmonic Stenosis, Ventricular Septal Defect, and Right Ventricular Pressure
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1960 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.22.3.405
1960;22:405-411Circulation.
http://circ.ahajournals.org/content/22/3/405located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle column ofClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from