Pulmonary-Allergy Drugs Advisory Committee September 6, 2002 Pulmonary-Allergy Drugs Advisory...
64
Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002 September 6, 2002 Pulmonary-Allergy Drugs Pulmonary-Allergy Drugs Advisory Committee Advisory Committee NDA 21-395 Spiriva ® (tiotropium bromide) Inhalation Powder Eugene J. Sullivan, MD FCCP Medical Officer Division of Pulmonary and Allergy Drug Products
-
Upload
roland-goodman -
Category
Documents
-
view
227 -
download
4
Transcript of Pulmonary-Allergy Drugs Advisory Committee September 6, 2002 Pulmonary-Allergy Drugs Advisory...

Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Pulmonary-Allergy Drugs Pulmonary-Allergy Drugs Advisory CommitteeAdvisory Committee
Pulmonary-Allergy Drugs Pulmonary-Allergy Drugs Advisory CommitteeAdvisory Committee
NDA 21-395Spiriva® (tiotropium bromide)
Inhalation Powder
Eugene J. Sullivan, MD FCCPMedical Officer
Division of Pulmonary and Allergy Drug Products
NDA 21-395Spiriva® (tiotropium bromide)
Inhalation Powder
Eugene J. Sullivan, MD FCCPMedical Officer
Division of Pulmonary and Allergy Drug Products

2Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
OutlineOutlineOutlineOutline
• Background• PK/PD characteristics• Overview of P3 clinical program• Safety findings• Efficacy findings
– Bronchodilator efficacy– Dyspnea efficacy– Other efficacy findings
• Summary
• Background• PK/PD characteristics• Overview of P3 clinical program• Safety findings• Efficacy findings
– Bronchodilator efficacy– Dyspnea efficacy– Other efficacy findings
• Summary

3Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Background: COPD IndicationBackground: COPD IndicationBackground: COPD IndicationBackground: COPD Indication
• Proposed Indication for tiotropium: “treatment of bronchospasm
and dyspnea associated with COPD” • No drugs approved in the US carry an Indication
for the treatment of specific symptoms of COPD, or for the “treatment of COPD”
• Proposed Indication for tiotropium: “treatment of bronchospasm
and dyspnea associated with COPD” • No drugs approved in the US carry an Indication
for the treatment of specific symptoms of COPD, or for the “treatment of COPD”

4Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Background: COPD IndicationBackground: COPD IndicationBackground: COPD IndicationBackground: COPD Indication• Currently approved drugs:
– “treatment of bronchospasm associated with COPD”
• Distinction: treatment of bronchospasm vs. treatment of the disease
• FEV1
– direct measure of bronchospasm– “surrogate” measure of the disease itself (a
constellation of physical signs and symptoms, physiologic processes, and histopathologic features)
• Currently approved drugs: – “treatment of bronchospasm associated with
COPD”• Distinction: treatment of bronchospasm
vs. treatment of the disease• FEV1
– direct measure of bronchospasm– “surrogate” measure of the disease itself (a
constellation of physical signs and symptoms, physiologic processes, and histopathologic features)

5Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Background: COPD IndicationBackground: COPD IndicationBackground: COPD IndicationBackground: COPD Indication
• Presumed clinical benefit of bronchodilators– approved based on spirometry, but clinically
detectable benefit is presumed– “as-needed” use of the bronchodilator
albuterol reflects bronchodilator-mediated symptom benefit
• Presumed clinical benefit of bronchodilators– approved based on spirometry, but clinically
detectable benefit is presumed– “as-needed” use of the bronchodilator
albuterol reflects bronchodilator-mediated symptom benefit
6Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Background: COPD Efficacy VariablesBackground: COPD Efficacy VariablesBackground: COPD Efficacy VariablesBackground: COPD Efficacy Variables
• Primary: Measure of bronchodilation– Usually FEV1
• After chronic use (for maintenance drugs)• Peak FEV1, FEV1-Time Curve AUC
• Secondary (supportive)– Other spirometry variables– “Rescue” albuterol use– Peak flow– Six-minute walk test – Exacerbations, Patient-Reported Outcomes,
etc.
• Primary: Measure of bronchodilation– Usually FEV1
• After chronic use (for maintenance drugs)• Peak FEV1, FEV1-Time Curve AUC
• Secondary (supportive)– Other spirometry variables– “Rescue” albuterol use– Peak flow– Six-minute walk test – Exacerbations, Patient-Reported Outcomes,
etc.

7Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Background: Tiotropium Background: Tiotropium P3 Primary Efficacy VariablesP3 Primary Efficacy Variables
Background: Tiotropium Background: Tiotropium P3 Primary Efficacy VariablesP3 Primary Efficacy Variables
• All studies: – Change from baseline in “trough” (pre-dose)
FEV1
• Two studies: – Change from baseline in “trough” (pre-dose)
FEV1
and– Transitional Dyspnea Index (TDI)
• All studies: – Change from baseline in “trough” (pre-dose)
FEV1
• Two studies: – Change from baseline in “trough” (pre-dose)
FEV1
and– Transitional Dyspnea Index (TDI)

8Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
OutlineOutlineOutlineOutline
• Background• PK/PD characteristics• Overview of P3 clinical program• Safety findings• Efficacy findings
– Bronchodilator efficacy– Dyspnea efficacy– Other efficacy findings
• Summary
• Background• PK/PD characteristics• Overview of P3 clinical program• Safety findings• Efficacy findings
– Bronchodilator efficacy– Dyspnea efficacy– Other efficacy findings
• Summary
9Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
PK/PD CharacteristicsPK/PD CharacteristicsPK/PD CharacteristicsPK/PD Characteristics
• Bioavailability of tiotropium– Oral ingestion 2-3%– Oral inhalation 19.5%
• Single dose PK (oral inhalation): – Cmax= 5 minutes– Detectable in blood for 2-4 hours– Prolonged urinary excretion
• detectable in urine for 25 days after a dose of 108mcg
• Volume of distribution: 32 liters/kg
• Bioavailability of tiotropium– Oral ingestion 2-3%– Oral inhalation 19.5%
• Single dose PK (oral inhalation): – Cmax= 5 minutes– Detectable in blood for 2-4 hours– Prolonged urinary excretion
• detectable in urine for 25 days after a dose of 108mcg
• Volume of distribution: 32 liters/kg
10Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
PK/PD CharacteristicsPK/PD CharacteristicsPK/PD CharacteristicsPK/PD Characteristics
• Elimination:– 74% eliminated in urine as parent compound
• 44% by 4 hours, 54% by 24 hours, 61% by 96 hours
• active renal secretion (renal clearance > creatinine clearance)
– Fate of remaining 26% not well established• non-enzymatic hydrolysis• hepatic metabolism (CYP2D6 and CYP 3A4)
• Elimination:– 74% eliminated in urine as parent compound
• 44% by 4 hours, 54% by 24 hours, 61% by 96 hours
• active renal secretion (renal clearance > creatinine clearance)
– Fate of remaining 26% not well established• non-enzymatic hydrolysis• hepatic metabolism (CYP2D6 and CYP 3A4)

11Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
PK/PD CharacteristicsPK/PD CharacteristicsPK/PD CharacteristicsPK/PD Characteristics
• Terminal elimination half-life = 5-6 days• Multiple-dose accumulation: 2-3 fold
– suggests effective T1/2= 24-36 hours• PK characteristics are indicative of
extensive tissue binding, with slow release back into circulation– large volume of distribution and long terminal
elimination half-life
• Terminal elimination half-life = 5-6 days• Multiple-dose accumulation: 2-3 fold
– suggests effective T1/2= 24-36 hours• PK characteristics are indicative of
extensive tissue binding, with slow release back into circulation– large volume of distribution and long terminal
elimination half-life

12Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
PK/PD CharacteristicsPK/PD CharacteristicsPK/PD CharacteristicsPK/PD Characteristics• Pharmacodynamic effect increases with
multiple daily dosing– Spirometry data from Phase 3 studies – Separate “sub-study” of one of the Phase 3
studies (122A, ipratropium-controlled)• N= 28• six-hour, serial spirometry on Days 1, 2, 3,
8, and 50– Maximum (“steady state”) effect is achieved by
Day 8
• Pharmacodynamic effect increases with multiple daily dosing– Spirometry data from Phase 3 studies – Separate “sub-study” of one of the Phase 3
studies (122A, ipratropium-controlled)• N= 28• six-hour, serial spirometry on Days 1, 2, 3,
8, and 50– Maximum (“steady state”) effect is achieved by
Day 8

13Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
PD Effect Increases with Multiple DosingPD Effect Increases with Multiple DosingPD Effect Increases with Multiple DosingPD Effect Increases with Multiple DosingPhase 3, one-year, placebo-controlled studies:Phase 3, one-year, placebo-controlled studies:Mean FEV1 Average and Peak Response (Liters)[Studies 114 and 115, ITT Data Set]
Tiotropium PlaceboResponse Test Day114 115 114 115
Average(3-hour)
18
5092176260344
0.160.220.200.200.190.190.19
0.170.230.240.210.210.200.20
0.020.020.01-0.02-0.02-0.01-0.03
0.020.020.020.01-0.020.00-0.01
Peak 18
5092176260344
0.240.280.270.260.260.250.26
0.240.310.310.280.280.260.26
0.080.080.080.050.040.060.04
0.080.090.080.070.040.060.05
14Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
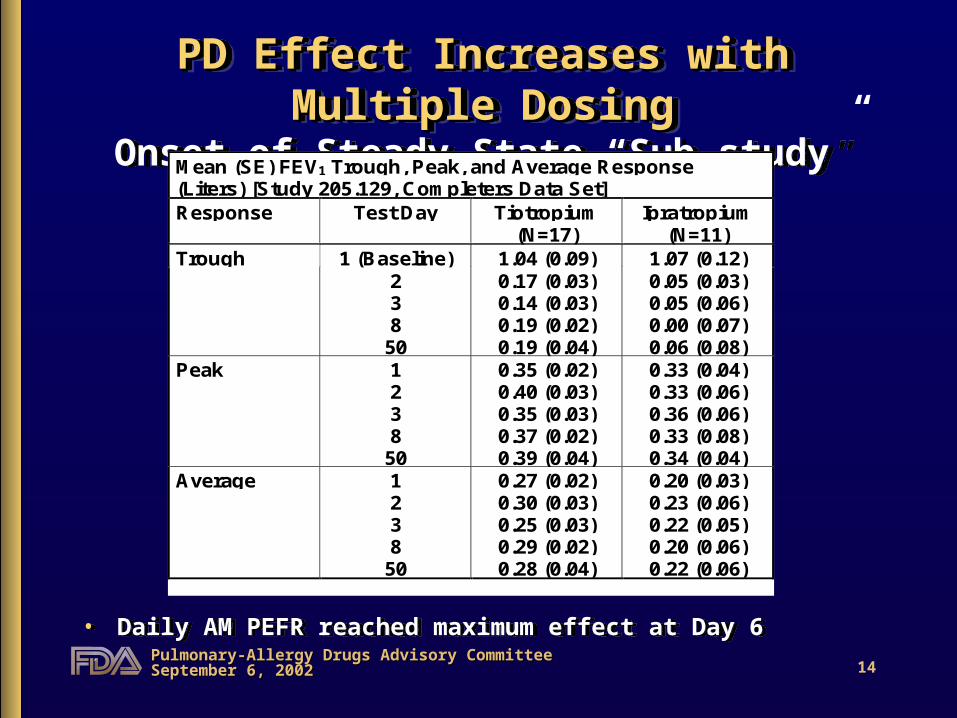
PD Effect Increases with Multiple DosingPD Effect Increases with Multiple DosingOnset of Steady State “Sub-study”
PD Effect Increases with Multiple DosingPD Effect Increases with Multiple DosingOnset of Steady State “Sub-study”
• Daily AM PEFR reached maximum effect at Day 6• Daily AM PEFR reached maximum effect at Day 6
Mean (SE) FEV1 Trough, Peak, and Average Response(Liters) [Study 205.129, Completers Data Set]Response Test Day Tiotropium
(N=17)Ipratropium
(N=11)1 (Baseline) 1.04 (0.09) 1.07 (0.12)Trough
238
50
0.17 (0.03)0.14 (0.03)0.19 (0.02)0.19 (0.04)
0.05 (0.03)0.05 (0.06)0.00 (0.07)0.06 (0.08)
Peak 1238
50
0.35 (0.02)0.40 (0.03)0.35 (0.03)0.37 (0.02)0.39 (0.04)
0.33 (0.04)0.33 (0.06)0.36 (0.06)0.33 (0.08)0.34 (0.04)
Average 1238
50
0.27 (0.02)0.30 (0.03)0.25 (0.03)0.29 (0.02)0.28 (0.04)
0.20 (0.03)0.23 (0.06)0.22 (0.05)0.20 (0.06)0.22 (0.06)

15Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
OutlineOutlineOutlineOutline
• Background• PK/PD characteristics• Overview of P3 clinical program• Safety findings• Efficacy findings
– Bronchodilator efficacy– Dyspnea efficacy– Other efficacy findings
• Summary
• Background• PK/PD characteristics• Overview of P3 clinical program• Safety findings• Efficacy findings
– Bronchodilator efficacy– Dyspnea efficacy– Other efficacy findings
• Summary

16Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Phase 3 Clinical ProgramPhase 3 Clinical ProgramPhase 3 Clinical ProgramPhase 3 Clinical ProgramStudy
(# subjects)Treatments Location Duration Primary
Endpoint
114(n=470)
115(n=451)
Tiotropium QDvs.Placebo(3:2 randomization)
US 1 year TroughFEV1
response(13 weeks)
122A(n=288)
122B(n=247)
Tiotropium QDvs.Ipratropium MDI QID(2:1 randomization)
Netherlandsand Belgium
1 year TroughFEV1
response(13 weeks)
130(n=623)
137(n=584)
Tiotropium QDvs.Salmeterol BIDvs.Placebo(1:1:1 randomization)
Multinational 6months
TroughFEV1
responseand TDI focal score(6 months)
Study(# subjects)
Treatments Location Duration PrimaryEndpoint
114(n=470)
115(n=451)
Tiotropium QDvs.Placebo(3:2 randomization)
US 1 year TroughFEV1
response(13 weeks)
122A(n=288)
122B(n=247)
Tiotropium QDvs.Ipratropium MDI QID(2:1 randomization)
Netherlandsand Belgium
1 year TroughFEV1
response(13 weeks)
130(n=623)
137(n=584)
Tiotropium QDvs.Salmeterol BIDvs.Placebo(1:1:1 randomization)
Multinational 6months
TroughFEV1
responseand TDI focal score(6 months)

17Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Phase 3: Patients StudiedPhase 3: Patients StudiedPhase 3: Patients StudiedPhase 3: Patients Studied• Inclusion Criteria:
– age 40 years– smoking history > 10 pack-years– FEV1 60% or 65% predicted– FEV1 70% of FVC
• Exclusion Criteria:– h/o asthma, allergic rhinitis, or atopy– elevated blood eosinophil count– significant disease other than COPD– symptomatic prostatic hypertrophy or bladder outlet
obstruction– narrow angle glaucoma– MI (1 year), cardiac arrhythmia requiring drug treatment,
or hospitalization for heart failure (3 years)
• Inclusion Criteria: – age 40 years– smoking history > 10 pack-years– FEV1 60% or 65% predicted– FEV1 70% of FVC
• Exclusion Criteria:– h/o asthma, allergic rhinitis, or atopy– elevated blood eosinophil count– significant disease other than COPD– symptomatic prostatic hypertrophy or bladder outlet
obstruction– narrow angle glaucoma– MI (1 year), cardiac arrhythmia requiring drug treatment,
or hospitalization for heart failure (3 years)
18Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
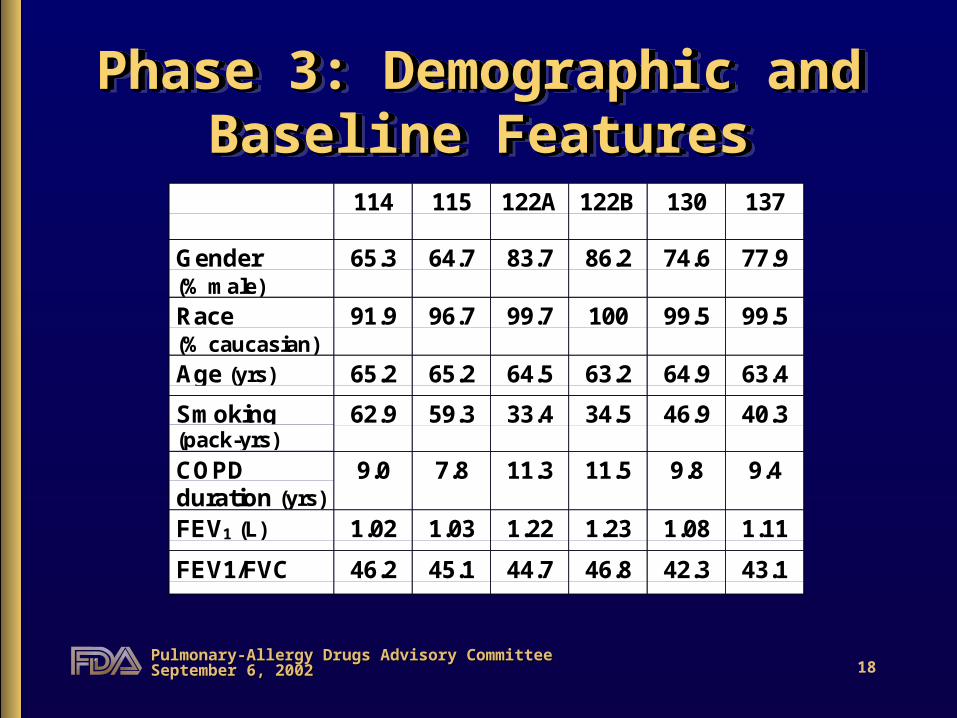
Phase 3: Demographic and Phase 3: Demographic and Baseline FeaturesBaseline Features
Phase 3: Demographic and Phase 3: Demographic and Baseline FeaturesBaseline Features
114 115 122A 122B 130 137
Gender(% male)
65.3 64.7 83.7 86.2 74.6 77.9
Race(% caucasian)
91.9 96.7 99.7 100 99.5 99.5
Age (yrs) 65.2 65.2 64.5 63.2 64.9 63.4
Smoking(pack-yrs)
62.9 59.3 33.4 34.5 46.9 40.3
COPDduration (yrs)
9.0 7.8 11.3 11.5 9.8 9.4
FEV1 (L) 1.02 1.03 1.22 1.23 1.08 1.11
FEV1/FVC 46.2 45.1 44.7 46.8 42.3 43.1FEV1/FVC

19Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
OutlineOutlineOutlineOutline
• Background• PK/PD characteristics• Overview of P3 clinical program• Safety findings• Efficacy findings
– Bronchodilator efficacy– Dyspnea efficacy– Other efficacy findings
• Summary
• Background• PK/PD characteristics• Overview of P3 clinical program• Safety findings• Efficacy findings
– Bronchodilator efficacy– Dyspnea efficacy– Other efficacy findings
• Summary

20Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Safety DatabaseSafety DatabaseSafety DatabaseSafety Database
• 1308 patients exposed in P3• Phase 3 Safety Evaluations:
– adverse events– vital signs– physical examination– clinical labs– ECGs (timing not specified)
• 1308 patients exposed in P3• Phase 3 Safety Evaluations:
– adverse events– vital signs– physical examination– clinical labs– ECGs (timing not specified)

21Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Safety DatabaseSafety DatabaseSafety DatabaseSafety Database
• Additional Safety Data (Phase 2)– timed ECGs (multiple dose study, up to 44mcg
QD)– Holter monitors (n=72 patients, pre- and on-
treatment)
• Additional Safety Data (Phase 2)– timed ECGs (multiple dose study, up to 44mcg
QD)– Holter monitors (n=72 patients, pre- and on-
treatment)

22Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Safety DatabaseSafety DatabaseSafety DatabaseSafety Database
• Focus on one-year, placebo-controlled studies• Median exposure 10 days longer for tiotropium
patients (338 days) than for placebo patients (328 days).
• Focus on one-year, placebo-controlled studies• Median exposure 10 days longer for tiotropium
patients (338 days) than for placebo patients (328 days).

23Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Adverse Events with TiotropiumAdverse Events with Tiotropium(One-year, placebo-controlled studies)(One-year, placebo-controlled studies)Adverse Events with TiotropiumAdverse Events with Tiotropium
(One-year, placebo-controlled studies)(One-year, placebo-controlled studies)
• Gastrointestinal:– dry mouth (16% vs. 2.7%)– dyspepsia (5.8% vs. 4.6%)– abdominal pain (4.7% vs. 3.0%)– constipation (3.5% vs. 1.6%)– vomiting (3.5% vs. 2.4%)
• Gastrointestinal:– dry mouth (16% vs. 2.7%)– dyspepsia (5.8% vs. 4.6%)– abdominal pain (4.7% vs. 3.0%)– constipation (3.5% vs. 1.6%)– vomiting (3.5% vs. 2.4%)

24Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Adverse Events with TiotropiumAdverse Events with Tiotropium(One-year, placebo-controlled studies)(One-year, placebo-controlled studies)Adverse Events with TiotropiumAdverse Events with Tiotropium
(One-year, placebo-controlled studies)(One-year, placebo-controlled studies)
• Respiratory System:– upper respiratory tract infection (41.1% vs.
37.2%)– epistaxis (3.6% vs. 1.9%)– pharyngitis (8.9% vs. 7.3%)– sinusitis (11.3% vs. 9.4%)
• Chest pain (6.9% vs. 4.6%)• Rash (4.2% vs. 2.2%)• Urinary Tract Infection (7.3% vs. 5.1%)
• Respiratory System:– upper respiratory tract infection (41.1% vs.
37.2%)– epistaxis (3.6% vs. 1.9%)– pharyngitis (8.9% vs. 7.3%)– sinusitis (11.3% vs. 9.4%)
• Chest pain (6.9% vs. 4.6%)• Rash (4.2% vs. 2.2%)• Urinary Tract Infection (7.3% vs. 5.1%)

25Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Adverse Events with TiotropiumAdverse Events with Tiotropium(Six-month studies)(Six-month studies)
Adverse Events with TiotropiumAdverse Events with Tiotropium(Six-month studies)(Six-month studies)
• Fewer differences between tiotropium and placebo.
• AEs more common in tiotropium:– Dry mouth (8.2% vs. 2.3%)– Upper Respiratory Tract Infection (19.4%vs.
16%)– Pharyngitis (4.5% vs. 3.0%)– Sinusitis (3.2% vs. 2.5%) – Influenza-like symptoms (6.7% vs. 4%)
• Fewer differences between tiotropium and placebo.
• AEs more common in tiotropium:– Dry mouth (8.2% vs. 2.3%)– Upper Respiratory Tract Infection (19.4%vs.
16%)– Pharyngitis (4.5% vs. 3.0%)– Sinusitis (3.2% vs. 2.5%) – Influenza-like symptoms (6.7% vs. 4%)

26Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Safety Interactions with TiotropiumSafety Interactions with Tiotropium(One-year, placebo-controlled studies)(One-year, placebo-controlled studies)
Safety Interactions with TiotropiumSafety Interactions with Tiotropium(One-year, placebo-controlled studies)(One-year, placebo-controlled studies)
• Age (60, 61-70, 71):– Dry Mouth: 11%, 16%, 21% (Pbo values: 3%,
1.9%, 3.5%)– Constipation: 2%, 2.8%, 6% (Pbo values: 3%,
0.6%, 1.7%)– Urinary Tract Infection: 3.3%, 5.2%, 12% (Pbo
values: 2%, 3.9%, 6.1%)• Gender:
– Dry Mouth: women 23%, men 13% (Pbo values: 2.9% and 2.6%)
• Age (60, 61-70, 71):– Dry Mouth: 11%, 16%, 21% (Pbo values: 3%,
1.9%, 3.5%)– Constipation: 2%, 2.8%, 6% (Pbo values: 3%,
0.6%, 1.7%)– Urinary Tract Infection: 3.3%, 5.2%, 12% (Pbo
values: 2%, 3.9%, 6.1%)• Gender:
– Dry Mouth: women 23%, men 13% (Pbo values: 2.9% and 2.6%)

27Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Other Safety ObservationsOther Safety Observations(One-year, placebo-controlled studies)(One-year, placebo-controlled studies)
Other Safety ObservationsOther Safety Observations(One-year, placebo-controlled studies)(One-year, placebo-controlled studies)
• Urinary Retention:– 4 patients, all treated with tiotropium– all required Foley catheter; three were started
on medication for BPH following the event• “Micturation disorder” or “micturation
frequency”– 6 (1.1%) tiotropium patients vs. 0 placebo
patients
• Urinary Retention:– 4 patients, all treated with tiotropium– all required Foley catheter; three were started
on medication for BPH following the event• “Micturation disorder” or “micturation
frequency”– 6 (1.1%) tiotropium patients vs. 0 placebo
patients
28Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Other Safety ObservationsOther Safety Observations(One-year, placebo-controlled studies)(One-year, placebo-controlled studies)
Other Safety ObservationsOther Safety Observations(One-year, placebo-controlled studies)(One-year, placebo-controlled studies)
• Constipation:– one patient treated with tiotropium was
hospitalized with fecal impaction• “Diabetes mellitus”, “diabetes mellitus
aggravated,” or “hyperglycemia”– 14 (2.5%) tiotropium patients vs. 1 (0.3%)
placebo patients
• Constipation:– one patient treated with tiotropium was
hospitalized with fecal impaction• “Diabetes mellitus”, “diabetes mellitus
aggravated,” or “hyperglycemia”– 14 (2.5%) tiotropium patients vs. 1 (0.3%)
placebo patients

29Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Other Safety ObservationsOther Safety Observations(One-year, placebo-controlled studies)(One-year, placebo-controlled studies)
Other Safety ObservationsOther Safety Observations(One-year, placebo-controlled studies)(One-year, placebo-controlled studies)
• Cardiovascular Effects– “Heart Rate and Rhythm Disorders”:
• AEs: 24 (4.4%) tiotropium patients vs. 8 (2.2%) placebo patients
• SAEs: 1.3% tiotropium patients vs. 0.5%placebo patients
• (signal not seen in ipratropium-controlled studies)
– No safety signal on ECGs
• Cardiovascular Effects– “Heart Rate and Rhythm Disorders”:
• AEs: 24 (4.4%) tiotropium patients vs. 8 (2.2%) placebo patients
• SAEs: 1.3% tiotropium patients vs. 0.5%placebo patients
• (signal not seen in ipratropium-controlled studies)
– No safety signal on ECGs
30Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Other Safety ObservationsOther Safety Observations(One-year studies)(One-year studies)
Other Safety ObservationsOther Safety Observations(One-year studies)(One-year studies)
• Deaths– One-year studies:
– incidence of death similar in all groups– placebo-controlled: 5/7 tiotropium deaths
were attributable to cardiac ischemia or arrhythmia (compared with 1/7 placebo deaths)
– ipratropium-controlled: deaths due to MI = 3/9 tiotropium deaths, 0/3 ipratropium deaths
• Deaths– One-year studies:
– incidence of death similar in all groups– placebo-controlled: 5/7 tiotropium deaths
were attributable to cardiac ischemia or arrhythmia (compared with 1/7 placebo deaths)
– ipratropium-controlled: deaths due to MI = 3/9 tiotropium deaths, 0/3 ipratropium deaths

31Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Other Safety ObservationsOther Safety ObservationsOther Safety ObservationsOther Safety Observations
Phase 2 Study:– No safety signal on Holter monitors
• N=72 patients, pre- and on-treatment– compared with n = 284 patients during
five, 24-hour periods described in Serevent MDI label
• One subject developed a four-fold increase in ventricular ectopy on-treatment (tiotropium).
Phase 2 Study:– No safety signal on Holter monitors
• N=72 patients, pre- and on-treatment– compared with n = 284 patients during
five, 24-hour periods described in Serevent MDI label
• One subject developed a four-fold increase in ventricular ectopy on-treatment (tiotropium).

32Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Adverse Events with TiotropiumAdverse Events with Tiotropium(One-year, ipratropium-controlled studies)(One-year, ipratropium-controlled studies)
Adverse Events with TiotropiumAdverse Events with Tiotropium(One-year, ipratropium-controlled studies)(One-year, ipratropium-controlled studies)
Event Tiotropium IpratropiumChest Pain 5.3% 2.2%Dry Mouth 12.1% 6.1%Dyspepsia 1.4% 0.6%Moniliasis 2.8% 1.7%Pharyngitis 6.5% 2.8%Sinusitis 3.4% 2.2%URTI 43% 34.6%UTI 3.9% 2.2%
Event Tiotropium IpratropiumChest Pain 5.3% 2.2%Dry Mouth 12.1% 6.1%Dyspepsia 1.4% 0.6%Moniliasis 2.8% 1.7%Pharyngitis 6.5% 2.8%Sinusitis 3.4% 2.2%URTI 43% 34.6%UTI 3.9% 2.2%
33Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
OutlineOutlineOutlineOutline
• Background• PK/PD characteristics• Overview of P3 clinical program• Safety findings• Efficacy findings
– Bronchodilator efficacy– Dyspnea efficacy– Other efficacy findings
• Summary
• Background• PK/PD characteristics• Overview of P3 clinical program• Safety findings• Efficacy findings
– Bronchodilator efficacy– Dyspnea efficacy– Other efficacy findings
• Summary

34Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
OutlineOutlineOutlineOutline
• Background• PK/PD characteristics• Overview of P3 clinical program• Safety findings• Efficacy findings
– Bronchodilator efficacy– Dyspnea efficacy– Other efficacy findings
• Summary
• Background• PK/PD characteristics• Overview of P3 clinical program• Safety findings• Efficacy findings
– Bronchodilator efficacy– Dyspnea efficacy– Other efficacy findings
• Summary

35Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Bronchodilator Efficacy:Bronchodilator Efficacy:Studies 114 and 115Studies 114 and 115
Bronchodilator Efficacy:Bronchodilator Efficacy:Studies 114 and 115Studies 114 and 115
• Trough FEV1 statistically superior on all other clinic visits (1, 7, 25, 37, and 49 weeks), with mean effect sizes of 0.11 - 0.16 liters.
• Tiotropium was also statistically superior to placebo on peak FEV1, and average FEV1 during the 3-hour serial spirometry performed on all clinic visits.
• Trough FEV1 statistically superior on all other clinic visits (1, 7, 25, 37, and 49 weeks), with mean effect sizes of 0.11 - 0.16 liters.
• Tiotropium was also statistically superior to placebo on peak FEV1, and average FEV1 during the 3-hour serial spirometry performed on all clinic visits.
Primary Endpoint:Trough FEV1 Response (liters), Week 13Study Tiotropium Placebo p-value Difference
114 0.11 -0.03 0.0001 0.14
115 0.13 -0.01 0.0001 0.14

36Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Bronchodilator Efficacy:Bronchodilator Efficacy:Studies 114 and 115Studies 114 and 115
Bronchodilator Efficacy:Bronchodilator Efficacy:Studies 114 and 115Studies 114 and 115
• Peak FEV1 Data– Mean Peak FEV1 response was 0.24 liters on Day 1 and
0.25 - 0.31 liters on subsequent clinic visits.– On Day 1, the mean peak FEV1 at each time point (0.5, 1,
2, and 3 hours) was <0.20 liters– This is because patients reached their personal peak
FEV1 at differing time points:
• Peak FEV1 Data– Mean Peak FEV1 response was 0.24 liters on Day 1 and
0.25 - 0.31 liters on subsequent clinic visits.– On Day 1, the mean peak FEV1 at each time point (0.5, 1,
2, and 3 hours) was <0.20 liters– This is because patients reached their personal peak
FEV1 at differing time points:
Percentage of Tiotropium Patients Who Reached TheirPeak FEV1 at Each Timepoint (Test Day 1)
Time (hours) Study 114 Study 1150.5123
14.7%20.4%29.7%35.1%
18.8%19.2%29.2%32.8%
37Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Bronchodilator Efficacy:Bronchodilator Efficacy:Studies 114 and 115Studies 114 and 115
Bronchodilator Efficacy:Bronchodilator Efficacy:Studies 114 and 115Studies 114 and 115
• Tiotropium was statistically superior to placebo:– FVC response (trough, average, and peak)– AM and PM PEFR, for most weeks, with mean effect
sizes of 8 - 31 liters/minute (morning) and 13 to 40 liters/minute (evening)
• Tiotropium was statistically superior to placebo:– FVC response (trough, average, and peak)– AM and PM PEFR, for most weeks, with mean effect
sizes of 8 - 31 liters/minute (morning) and 13 to 40 liters/minute (evening)

38Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Bronchodilator Efficacy:Bronchodilator Efficacy:Studies 122A and 122BStudies 122A and 122B
Bronchodilator Efficacy:Bronchodilator Efficacy:Studies 122A and 122BStudies 122A and 122B
• Primary Efficacy Endpoint: Trough FEV1 at 13 weeks– Note: Ipratropium not expected to show significant
efficacy at this time point– Tiotropium was superior to ipratropium on this variable
at all clinic visits, with mean effect sizes of 0.11 to 0.18 liters (over ipratropium)
• Primary Efficacy Endpoint: Trough FEV1 at 13 weeks– Note: Ipratropium not expected to show significant
efficacy at this time point– Tiotropium was superior to ipratropium on this variable
at all clinic visits, with mean effect sizes of 0.11 to 0.18 liters (over ipratropium)

39Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Bronchodilator Efficacy:Bronchodilator Efficacy:Studies 130 and 137Studies 130 and 137
Bronchodilator Efficacy:Bronchodilator Efficacy:Studies 130 and 137Studies 130 and 137
• Trough FEV1 was statistically superior on all other clinic visits (Day 1, and Weeks 2, 8, and 16), with mean effect sizes of 0.11 - 0.15 liters.
• Tiotropium was also statistically superior to placebo on peak FEV1, and average FEV1 during the 12- or 3-hour serial spirometry performed on all clinic visits.
• Trough FEV1 was statistically superior on all other clinic visits (Day 1, and Weeks 2, 8, and 16), with mean effect sizes of 0.11 - 0.15 liters.
• Tiotropium was also statistically superior to placebo on peak FEV1, and average FEV1 during the 12- or 3-hour serial spirometry performed on all clinic visits.
Co-primary Endpoint:Trough FEV1 Response (liters), Week 24Study Tiotropium Placebo p-value Difference
130 0.11 -0.03 0.0001 0.14
137 0.07 -0.03 0.0001 0.11
40Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Bronchodilator Efficacy:Bronchodilator Efficacy:Studies 130 and 137Studies 130 and 137
Bronchodilator Efficacy:Bronchodilator Efficacy:Studies 130 and 137Studies 130 and 137
• Tiotropium was statistically superior to placebo:– FVC response (trough, average, and peak)– AM and PM PEFR, with mean effect sizes of 14.9 - 27
liters/minute (morning) and 21 - 33 liters/minute (evening)
• Tiotropium was statistically superior to placebo:– FVC response (trough, average, and peak)– AM and PM PEFR, with mean effect sizes of 14.9 - 27
liters/minute (morning) and 21 - 33 liters/minute (evening)

41Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
OutlineOutlineOutlineOutline
• Background• PK/PD characteristics• Overview of P3 clinical program• Safety findings• Efficacy findings
– Bronchodilator efficacy– Dyspnea efficacy– Other efficacy findings
• Summary
• Background• PK/PD characteristics• Overview of P3 clinical program• Safety findings• Efficacy findings
– Bronchodilator efficacy– Dyspnea efficacy– Other efficacy findings
• Summary

42Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Dyspnea Efficacy:Dyspnea Efficacy:Studies 130 and 137Studies 130 and 137Dyspnea Efficacy:Dyspnea Efficacy:
Studies 130 and 137Studies 130 and 137
TDI “responders” at 6 months (Co-primary Endpoint)
Study Tiotropium Placebo Salmeterol 130 42%** 26% 35% 137 45%* 33% 48%**
*p<0.05 (placebo comparison) **p<0.01 (placebo comparison)
[Responders defined as patients with TDI score 1]
TDI “responders” at 6 months (Co-primary Endpoint)
Study Tiotropium Placebo Salmeterol 130 42%** 26% 35% 137 45%* 33% 48%**
*p<0.05 (placebo comparison) **p<0.01 (placebo comparison)
[Responders defined as patients with TDI score 1]

43Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Exclusions from TDI Data SetExclusions from TDI Data SetExclusions from TDI Data SetExclusions from TDI Data Set
Study Population Tiotropium Placebo Salmeterol
TDI Data Set 184 148 179130
Randomized 209 201 213
TDI Data Set 164 161 161137
Randomized 193 199 192

44Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Dyspnea Efficacy:Dyspnea Efficacy:Studies 130 and 137Studies 130 and 137Dyspnea Efficacy:Dyspnea Efficacy:
Studies 130 and 137Studies 130 and 137
Number Needed to Treat (NNT) Analyses*
Study NNT130 6.45137 8.6Combined 7.5
*To achieve one “responder,” defined as TDI 1
Number Needed to Treat (NNT) Analyses*
Study NNT130 6.45137 8.6Combined 7.5
*To achieve one “responder,” defined as TDI 1

45Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Dyspnea Efficacy:Dyspnea Efficacy:Studies 130 and 137Studies 130 and 137Dyspnea Efficacy:Dyspnea Efficacy:
Studies 130 and 137Studies 130 and 137TDI “responders” at 8 and 16 weeks
(Secondary Endpoints)8 WeeksStudy Tiotropium Placebo Salmeterol 130 40%* 24% 34% 137 44%* 31% 47%**
16 WeeksStudy Tiotropium Placebo Salmeterol 130 43%* 27% 34% 137 42%* 30% 47%*** p<0.05 (placebo comparison) **p<0.01 (placebo comparison)
TDI “responders” at 8 and 16 weeks(Secondary Endpoints)
8 WeeksStudy Tiotropium Placebo Salmeterol 130 40%* 24% 34% 137 44%* 31% 47%**
16 WeeksStudy Tiotropium Placebo Salmeterol 130 43%* 27% 34% 137 42%* 30% 47%*** p<0.05 (placebo comparison) **p<0.01 (placebo comparison)

46Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Dyspnea Efficacy:Dyspnea Efficacy:TDI - Analyses of Mean ValuesTDI - Analyses of Mean Values
Dyspnea Efficacy:Dyspnea Efficacy:TDI - Analyses of Mean ValuesTDI - Analyses of Mean Values
Statistically Difference Superior 1 (Weeks) (Weeks)
• Study 130 8, 16, 24 (all) 8, 24
• Study 137 8, 16, 24 (all) 8, 16, 24 (all)
• Study 114 7, 13, 25, 37, 49 (all) 49
• Study 115 7, 13, 25, 37, 49 (all) 37, 49
• Study 122A* 1, 26, 39, 52 (not 7, 13) -
• Study 122B* 1,7,13,26,39,52 (all) 1, 26, 29, 52*comparison: ipratropium
Statistically Difference Superior 1 (Weeks) (Weeks)
• Study 130 8, 16, 24 (all) 8, 24
• Study 137 8, 16, 24 (all) 8, 16, 24 (all)
• Study 114 7, 13, 25, 37, 49 (all) 49
• Study 115 7, 13, 25, 37, 49 (all) 37, 49
• Study 122A* 1, 26, 39, 52 (not 7, 13) -
• Study 122B* 1,7,13,26,39,52 (all) 1, 26, 29, 52*comparison: ipratropium
47Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Dyspnea Efficacy:Dyspnea Efficacy:Shuttle Walk Test/ Borg Dyspnea ScaleShuttle Walk Test/ Borg Dyspnea Scale
Dyspnea Efficacy:Dyspnea Efficacy:Shuttle Walk Test/ Borg Dyspnea ScaleShuttle Walk Test/ Borg Dyspnea Scale
• Studies 130 and 137 included a post-dose Shuttle Walk Test on Day 1, and Weeks 8, 16, and 25.
• Shuttle Walk Test (SWT): a standardized test in which patients walk at a steady pace on a 10-meter course until they are unable to maintain the required speed without becoming unduly breathless.
• The Modified Borg Dyspnea Scale was administered before and after each SWT.– Scale: ranges from 0 (“nothing at all”) to 10
(“maximal”)
• Studies 130 and 137 included a post-dose Shuttle Walk Test on Day 1, and Weeks 8, 16, and 25.
• Shuttle Walk Test (SWT): a standardized test in which patients walk at a steady pace on a 10-meter course until they are unable to maintain the required speed without becoming unduly breathless.
• The Modified Borg Dyspnea Scale was administered before and after each SWT.– Scale: ranges from 0 (“nothing at all”) to 10
(“maximal”)

48Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Dyspnea Efficacy:Dyspnea Efficacy:Shuttle Walk Test/ Borg Dyspnea ScaleShuttle Walk Test/ Borg Dyspnea Scale
Dyspnea Efficacy:Dyspnea Efficacy:Shuttle Walk Test/ Borg Dyspnea ScaleShuttle Walk Test/ Borg Dyspnea Scale
• SWT (Walking Distance)– No difference between groups in either study– Placebo numerically superior in 1 study– Walking distance did not increase during the study in
any of the groups
• Modified Borg Dyspnea Scale– Study 130: No differences between tiotropium and
placebo, except Week 8 (Difference: 0.24 pre-exercise, 0.32 post-exercise)
– Study 137: No differences between tiotropium and placebo
• SWT (Walking Distance)– No difference between groups in either study– Placebo numerically superior in 1 study– Walking distance did not increase during the study in
any of the groups
• Modified Borg Dyspnea Scale– Study 130: No differences between tiotropium and
placebo, except Week 8 (Difference: 0.24 pre-exercise, 0.32 post-exercise)
– Study 137: No differences between tiotropium and placebo

49Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Dyspnea Efficacy:Dyspnea Efficacy:“COPD Symptom Score”“COPD Symptom Score”
Dyspnea Efficacy:Dyspnea Efficacy:“COPD Symptom Score”“COPD Symptom Score”
• Studies 130/137 and 114/115• Investigator’s assessment of the prior week• Wheezing, Shortness of Breath, Coughing, and
Tightness of Chest• Each scored from 0-3• Results: Tiotropium statistically superior to
placebo for “Shortness of Breath” at most visits• Effect Size: 0.13 to 0.36• Interpretation: Uncertain significance (validation,
effect size)
• Studies 130/137 and 114/115• Investigator’s assessment of the prior week• Wheezing, Shortness of Breath, Coughing, and
Tightness of Chest• Each scored from 0-3• Results: Tiotropium statistically superior to
placebo for “Shortness of Breath” at most visits• Effect Size: 0.13 to 0.36• Interpretation: Uncertain significance (validation,
effect size)

50Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
OutlineOutlineOutlineOutline
• Background• PK/PD characteristics• Overview of P3 clinical program• Safety findings• Efficacy findings
– Bronchodilator efficacy– Dyspnea efficacy– Other efficacy findings
• Summary
• Background• PK/PD characteristics• Overview of P3 clinical program• Safety findings• Efficacy findings
– Bronchodilator efficacy– Dyspnea efficacy– Other efficacy findings
• Summary
51Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Other Efficacy FindingsOther Efficacy FindingsOther Efficacy FindingsOther Efficacy Findings
• Studies 114 and 115– Tiotropium was statistically superior to
placebo:• Physician’s Global Evaluation (effect size of
0.25 to 0.59 on a scale of 1-8)• As-needed albuterol (5-6 fewer doses per
week)– No consistent meaningful difference shown:
• COPD exacerbations or hospitalizations• St. George’s Hospital Respiratory
Questionnaire• Medical Outcomes Study SF-36
• Studies 114 and 115– Tiotropium was statistically superior to
placebo:• Physician’s Global Evaluation (effect size of
0.25 to 0.59 on a scale of 1-8)• As-needed albuterol (5-6 fewer doses per
week)– No consistent meaningful difference shown:
• COPD exacerbations or hospitalizations• St. George’s Hospital Respiratory
Questionnaire• Medical Outcomes Study SF-36

52Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Other Efficacy FindingsOther Efficacy FindingsOther Efficacy FindingsOther Efficacy Findings
• Studies 122A and 122B (ipratropium-controlled)– No consistent effect:
• as-needed albuterol use• COPD exacerbations or hospitalizations
• Studies 122A and 122B (ipratropium-controlled)– No consistent effect:
• as-needed albuterol use• COPD exacerbations or hospitalizations
53Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Other Efficacy FindingsOther Efficacy FindingsOther Efficacy FindingsOther Efficacy Findings
• Studies 130 and 137– Tiotropium was statistically superior to
placebo: • Physician’s Global Evaluation (all test days
except one; effect size of 0.11 to 0.59 on a scale of 1-8)
– No consistent, meaningful difference shown:• As-needed albuterol• COPD exacerbations or hospitalizations• St. George’s Hospital Respiratory
Questionnaire• Patient Satisfaction Questionnaire
• Studies 130 and 137– Tiotropium was statistically superior to
placebo: • Physician’s Global Evaluation (all test days
except one; effect size of 0.11 to 0.59 on a scale of 1-8)
– No consistent, meaningful difference shown:• As-needed albuterol• COPD exacerbations or hospitalizations• St. George’s Hospital Respiratory
Questionnaire• Patient Satisfaction Questionnaire

54Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
OutlineOutlineOutlineOutline
• Background• PK/PD characteristics• Overview of P3 clinical program• Safety findings• Efficacy findings
– Bronchodilator efficacy– Dyspnea efficacy– Other efficacy findings
• Summary
• Background• PK/PD characteristics• Overview of P3 clinical program• Safety findings• Efficacy findings
– Bronchodilator efficacy– Dyspnea efficacy– Other efficacy findings
• Summary

55Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
SummarySummarySummarySummary
• PK features of tiotropium are somewhat unique among inhaled bronchodilators– Very large volume of distribution – Very long terminal elimination half-life– Apparent tight tissue binding with slow release
back into the circulation
• PK features of tiotropium are somewhat unique among inhaled bronchodilators– Very large volume of distribution – Very long terminal elimination half-life– Apparent tight tissue binding with slow release
back into the circulation

56Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
SummarySummarySummarySummary• Safety:
– Dry mouth is common, shows an age and gender interaction, and is more frequent than with ipratropium
– Several AEs occurred more frequently with tiotropium than placebo. Based on the mechanism of action and the observed age interaction, constipation and urinary tract infection may be important.
– Possible effect on heart rate/rhythm may merit further evaluation
• Safety:– Dry mouth is common, shows an age and
gender interaction, and is more frequent than with ipratropium
– Several AEs occurred more frequently with tiotropium than placebo. Based on the mechanism of action and the observed age interaction, constipation and urinary tract infection may be important.
– Possible effect on heart rate/rhythm may merit further evaluation
57Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
SummarySummarySummarySummary• Efficacy:
– Appears to provide clinically meaningful bronchodilation
– Duration of action supports once-daily dosing– Maximum bronchodilator effect reached after
multiple daily doses – Demonstrable effect on TDI. However, the
clinical significance of this effect is not known.• Issues with the instrument and its
implementation in the studies• Effect size (NNT)
• Efficacy:– Appears to provide clinically meaningful
bronchodilation– Duration of action supports once-daily dosing– Maximum bronchodilator effect reached after
multiple daily doses – Demonstrable effect on TDI. However, the
clinical significance of this effect is not known.• Issues with the instrument and its
implementation in the studies• Effect size (NNT)
58Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
SummarySummarySummarySummary
• Other:– Safety/efficacy of concurrent “as-needed”
ipratropium not addressed
• Other:– Safety/efficacy of concurrent “as-needed”
ipratropium not addressed

59Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002

60Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002

61Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Questions for the CommitteeQuestions for the CommitteeQuestions for the CommitteeQuestions for the Committee
1. Is the safety database for tiotropium bromide inhalation powder for the treatment of COPD patients adequate?A) If not, what further safety data should be obtained?B) Which of the safety data should be obtained prior to approval?
2. Are there specific safety concerns regarding the use of tiotropium bromide inhalation powder in the COPD patient population that merit specific attention in the product label?
1. Is the safety database for tiotropium bromide inhalation powder for the treatment of COPD patients adequate?A) If not, what further safety data should be obtained?B) Which of the safety data should be obtained prior to approval?
2. Are there specific safety concerns regarding the use of tiotropium bromide inhalation powder in the COPD patient population that merit specific attention in the product label?

62Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Questions for the CommitteeQuestions for the CommitteeQuestions for the CommitteeQuestions for the Committee
3. Do the data provide substantial and convincing evidence that tiotropium bromide inhalation powder provides a clinically meaningful bronchodilator effect when used in the chronic treatment of patients with COPD?
3. Do the data provide substantial and convincing evidence that tiotropium bromide inhalation powder provides a clinically meaningful bronchodilator effect when used in the chronic treatment of patients with COPD?

63Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002
Questions for the CommitteeQuestions for the CommitteeQuestions for the CommitteeQuestions for the Committee
4. Do the data provide substantial and convincing evidence that tiotropium bromide inhalation powder provides a clinically meaningful effect for the symptom of dyspnea in patients with COPD?
5. In general, what quality and quantity of data would constitute substantial and convincing evidence of a clinically meaningful benefit for the symptom of dyspnea in patients with COPD?
4. Do the data provide substantial and convincing evidence that tiotropium bromide inhalation powder provides a clinically meaningful effect for the symptom of dyspnea in patients with COPD?
5. In general, what quality and quantity of data would constitute substantial and convincing evidence of a clinically meaningful benefit for the symptom of dyspnea in patients with COPD?

64Pulmonary-Allergy Drugs Advisory Committee Pulmonary-Allergy Drugs Advisory Committee September 6, 2002September 6, 2002