Public health in an ageing society - an ILC-UK debate
98
Public health in an ageing society Wednesday 4 th December 2013 This event is kindly funded by an unrestricted grant from Sanofi Pasteur MSD #pubhealthageing
-
Upload
ilc-uk -
Category
News & Politics
-
view
1.791 -
download
4
description
Wednesday 4 December, 9.00 (for 9.30) – 11.30, Royal Society of Medicine, 1 Wimpole Street, London, W1G 0AE Funded by an unrestricted grant from Sanofi Pasteur MSD The recent public health reforms have now been in action for a few months, with local areas taking advantage of their newfound responsibilities and taking strategic decisions on what their public health focusses should be. Demographic change presents multi-faceted challenges for these decision makers, so how are these new structures responding an ageing society in their public health planning? At this debate, we explored the extent to which the new public health structures in England are able to respond to an ageing population. The debate covered issues such as how public health spending should be allocated across the life-course. With the current climate of concern around intergenerational fairness, particularly across public spending, how can we ensure that the next steps in public health are fair for all age groups? During this debate we heard an overview of the public health changes at a nation level, and then a policy perspective from an ILC-UK speaker on some of the challenges facing the new structures in light of an ageing population. This was followed by a series of experts presenting key examples of important aspects of public health for an ageing society, and how these issues are being addressed thus far by the new structures.
Transcript of Public health in an ageing society - an ILC-UK debate

Public health in an ageing society
Wednesday 4th December 2013
This event is kindly funded by an unrestricted grant from
Sanofi Pasteur MSD
#pubhealthageing

Welcome
Baroness Sally Greengross
Chief ExecutiveILC-UK
This event is kindly funded by an unrestricted grant from
Sanofi Pasteur MSD
#pubhealthageing

Dr Mike Brannan
Adult Life Course LeadHealth and Wellbeing Directorate, Public Health England
National overview – how public health structures can respond to an ageing society
This event is kindly funded by an unrestricted grant from
Sanofi Pasteur MSD
#pubhealthageing

National overview:How public health structures can respond to an ageing society
4/12/2013
Dr Mike BrannanAdult life course Lead, Public Health England

5
Changing UK demographics
5
• Increasing number of people aged over 65:
2010 4.5m people (1 in 6)
2030 10 m
2050 19 m (1 in 4)
• Health and social care needs increase in older years
UK demographics 2008-30

6
Economic & social contribution of active ageing
6
Time use of older people in the UK

7
Less than 50% of people disability-free at 65 years
Public Health England (London) 27/08/2013 7 7

8
Disease risk factors in the UK

9
Changing global burden of disease over next 20 years
Source: WHO Global Burden of Disease 2004.

10
An integrated whole system approach to public health
10
Government
Public HealthEngland
Localauthorities
NHS

11
A ‘place’ based public health system
11
Public health advice
People and communities
Health and wellbeing boardsHealth and wellbeing boards
Local governmentLocal government CCGs & their support
CCGs & their support
PHEcentre
NHS Englandarea team
NHS & IS Providers
3rd sector providers
Commissioner of public health services

12
Role of public health system
• Anticipates changing nature of populations
• Enables wider mitigation of damage to health
• Harnesses evidence, knowledge and technological advances to improve health and wellbeing equitably
• Unites fragmented means of service delivery through good partnership and high quality commissioning
• Secures equitable access to appropriate care
• Achieves impact at scale 12

13
Role of Public Health England
• Articulating an authoritative national voice for public health in England
• Protecting the population from communicable disease and environmental hazards
• Providing knowledge, evidence, intelligence and research
• Influencing through national/international relationships and acting as opinion leaders for health
• Developing the public health specialist workforce
• Providing direct advice and services
13

14
Creating a sustainable approach to health and social care

15
An evidence-based approach

16
E.g. Mapping needs and service usage to deliver equity
North East England work mapping deprivation, service access and admissions for chest pain to plan equitable services and resources.

17
E.g. Commissioning systematic interventions at population scale
• Commissioning high impact interventions with system and scale to improve population level outcomes
• Tracking and evaluating outcomes

18
E.g. Cross-sector work on social determinants of health
Facilitating local government and voluntary sector collaborations on cold homes.

19
Key messages
• Changing demographics require a new approach– Adapting systems to older people (e.g. expectations, new technologies)– Valuing contribution of older people & focus on functionality in later life– Addressing inequalities (e.g. disability, dependency)
• New public health system can facilitate this process– Integrated, cross-sector working– Focus on people, place & outcomes (including life course approach)– Needs-led, evidence-based interventions
• Public Health England will provide evidence, knowledge, advice to the NHS and local government and advocacy to enable more age friendly societal development

Jessica WatsonResearch and Public Affairs Officer
ILC-UK
Planning tomorrow’s health: policy challenges for public health in an
ageing society
This event is kindly funded by an unrestricted grant from
Sanofi Pasteur MSD
#pubhealthageing

The International Longevity Centre-UK is an independent, non-partisan think-tank
dedicated to addressing issues of longevity, ageing and population change.
Planning tomorrow’s health:policy challenges for public health in an ageing society
Jessica Watson, International Longevity Centre – UK
@ilcuk #pubhealthageing

The International Longevity Centre-UK is an independent, non-partisan think-tank
dedicated to addressing issues of longevity, ageing and population change.
ILC-UK Planning Tomorrow, Today
think tank evidence based policy focussed independent respected experts international life course intergenerational

The International Longevity Centre-UK is an independent, non-partisan think-tank
dedicated to addressing issues of longevity, ageing and population change.
Interests
Report and event kindly funded by an unrestricted
grant from Sanofi Pasteur MSD.

The International Longevity Centre-UK is an independent, non-partisan think-tank
dedicated to addressing issues of longevity, ageing and population change.
Public health
http://exhibits.hsl.virginia.edu/hands/http://profiles.nlm.nih.gov/ps/access/VCBBBS.jpghttp://aphl.smugmug.com/Other/Miscellaneous/i-wfRGwTQ/0/M/SyphilisPoster-M.jpg

The International Longevity Centre-UK is an independent, non-partisan think-tank
dedicated to addressing issues of longevity, ageing and population change.
Public health
http://static.guim.co.uk/sys-images/Guardian/Pix/pictures/2011/6/8/1307555290051/British-Heart-Foundation--007.jpghttp://costcutter.co.uk/images/change4life-logo.jpghttp://4.bp.blogspot.com/_sUJR6CdA52Y/SSj3x_w2woI/AAAAAAAAAAc/wR16mRgxrHU/s1600-h/cigarette_penis_2.jpg

The International Longevity Centre-UK is an independent, non-partisan think-tank
dedicated to addressing issues of longevity, ageing and population change.
Policy brief
Challenges of ageing society
Need to approach holistically (highlighted by Select Committee on Public Service and Demographic Change)
Case studies
ILC-UK focus

The International Longevity Centre-UK is an independent, non-partisan think-tank
dedicated to addressing issues of longevity, ageing and population change.
Planning tomorrow’s health

The International Longevity Centre-UK is an independent, non-partisan think-tank
dedicated to addressing issues of longevity, ageing and population change.
Public health post reforms
An exciting time
Integration of public health with the delivery of other services
Legal responsibility to Local Authorities
Knowledge of the local area and its needs
Popular with public and local authority workers

The International Longevity Centre-UK is an independent, non-partisan think-tank
dedicated to addressing issues of longevity, ageing and population change.
The case for a local approach
http://www.ons.gov.uk/ons/interactive/healthy-life-expectancy-at-birth-for-upper-tier-local-authorities--england-2009-11/index.html

The International Longevity Centre-UK is an independent, non-partisan think-tank
dedicated to addressing issues of longevity, ageing and population change.
The case for a local approach
http://www.ons.gov.uk/ons/interactive/healthy-life-expectancy-at-birth-for-upper-tier-local-authorities--england-2009-11/index.html

The International Longevity Centre-UK is an independent, non-partisan think-tank
dedicated to addressing issues of longevity, ageing and population change.
Challenges

The International Longevity Centre-UK is an independent, non-partisan think-tank
dedicated to addressing issues of longevity, ageing and population change.
Politics and public health
Public health decisions – and outcomes – are not necessarily election-friendly
Results and payoffs are long term
– Particularly for ageing
Budget constraints and ring-fencing
Intergenerational fairness

The International Longevity Centre-UK is an independent, non-partisan think-tank
dedicated to addressing issues of longevity, ageing and population change.
Getting public health front of mind
Breaking down administrative and mental barriers
Ensuring good knowledge and evidence
Realising the potential for what might be achieved

The International Longevity Centre-UK is an independent, non-partisan think-tank
dedicated to addressing issues of longevity, ageing and population change.
Example – pedestrian road safety
Older people suffer greater injuries as a pedestrian in a road accident compared to younger age groups
Association with lack of confidence and isolation
Potential for coordination with control over road crossing timings, speed control measures on roads

The International Longevity Centre-UK is an independent, non-partisan think-tank
dedicated to addressing issues of longevity, ageing and population change.
Who else could be involved?
Employers
– Extending working lives agenda
– Occupational health to play a role?
Insurance industry
– Some interesting use of incentives

The International Longevity Centre-UK is an independent, non-partisan think-tank
dedicated to addressing issues of longevity, ageing and population change.

The International Longevity Centre-UK is an independent, non-partisan think-tank
dedicated to addressing issues of longevity, ageing and population change.
Many thanks
Jessica Watson
Research and Public Affairs Officer
International Longevity Centre-UK
02073400440
Twitter: @ilcuk #pubhealthageing

Helen Donovan
Public Health Nursing AdvisorRoyal College of Nursing
Vaccination
This event is kindly funded by an unrestricted grant from
Sanofi Pasteur MSD
#pubhealthageing

Immunisation
Helen DonovanRCN UK Public Health nursing advisor
Not just for Children.....

• Joint Strategic Needs Assessments should take a life-course approach to Immunisation,
• Health and Wellbeing Boards should ensure that that life-course vaccination is adequately considered as part of health planning and commissioning,
• Commissioning arrangements for immunisation should support the uptake of adult vaccination.

Build on the success of children's immunisation
F Disease rates have fallen but cases of VPD remain.
- Pertussis - increase in number of cases
- Polio - outbreaks in Syria
- Diphtheria and diphtheria like illness and deaths in unvaccinated PHA health protection report http://www.hpa.org.uk/hpr/archives/2008/hpr1908.pdf
F Tetanus requires individual immunity - risks for the older age group.

Vaccines for AdultsF Influenza,
pneumococcal and now shingles
Also check;F Tetanus Diphtheria
and polio?F MMR?F Pregnant? - PertussisF Meningiococcal C <25
years

CDC adult immunization schedule

Check adults are up to date?

PH nursing ‘Making every contact count’
F Travel vaccinationF Health screensF Use other opportunities to check, discussion with
parents and grandparents?
F Information and resources on vaccination available?F Ask routinely about vaccination history?F Accurate records of vaccination history? –
Reminders and recall?F All health care professionals responsibility?

UK Office for National Statistics: Travel Trends 1992 – 2012
Source: International Passenger Survey (IPS) - Office for National Statistics
http://www.ons.gov.uk/ons/rel/ott/travel-trends/2012/rpt-travel-trends--2012.html#tab-Trends-in-visits-abroad-by-UK-residents

Recognised barriers to immunisation?
F Difficulty in getting access
F Discrimination
F Administrative
F Financial problems
F Language or literacy limitations
F Lack of cultural health beliefs and knowledge
F Lack of knowledge on health and vaccination
F Religious reasons
F Fatalistic approach to life
F Distorted perceptions of risks vs benefits

ResourcesF NHS Choices - under adult vaccination;
http://www.nhs.uk/Conditions/vaccinations/Pages/vaccination-saves-lives.aspx
F PHE Immunisation series on .Gov; https://www.gov.uk/government/collections/immunisation
F Immunisation against infectious disease (The Green Book) – on line; https://www.gov.uk/government/collections/immunisation-against-infectious-disease-the-green-book
F NaTHNaC; http://www.nathnac.org/pro/ F PHE Algorithm;
http://www.hpa.org.uk/webc/HPAwebFile/HPAweb_C/1194947406156
F CDC; http://www.cdc.gov/vaccines/

Dr Emma Stanmore
Lecturer in NursingUniversity of Manchester
Falls
This event is kindly funded by an unrestricted grant from
Sanofi Pasteur MSD
#pubhealthageing

Falls – Implementing best practice
Dr Emma Stanmore
www.profound.eu.com

In > 75s, falls are the leading cause of death resulting from injury.
500 admitted to Hospital every day, 33 never go home
1 in 3 >65’s and 1 in 2 >80’s fall p.a.
Fractures costs £1.8 billion p.a.
1 Hip Fracture every 10 mins1 Wrist Fracture every 9 mins1 Spine Fracture every 3 mins
(World Health Organization (2007)WHO Global report on falls prevention in older age. Masud, Morris Age & Ageing 2001; 30-S4 3-7
Rubenstein. Age & Ageing; 2006; 35-S2; ii37-41
)
Older people at risk of falls

Falls most serious frequent home accident
Fatal injuries in the EU amongst older people (65+) by cause and gender
EuroSafe/IDB Injuries in the EU 2005-2007 (2009)

ww
w.io
fbon
ehea
lth.o
rg

ww
w.io
fbon
ehea
lth.o
rg
Cooper C, Campion G, Melton LJ 3rd. Hip fractures in the elderly: a world-wide projection. Osteoporos Int. 1992;2:285-9.
Projected number of hip fractures worldwide 2050

ww
w.io
fbon
ehea
lth.o
rg
EVOS/EPOS Group
Falls explain between-center differences in the incidence of limb fracture across Europe. JBMR 2002
Low BMD is less predictive than risk of falling for future limb fractures in women across Europe. Bone 2005
Osteoporosis, falls and fractures

Falls can be prevented!
• Multiple-component group exercise
• Multiple-component home-based exercise
• Tai Chi• Multifactorial intervention
individual risk assessment • Vitamin D NB low Vit D• Home safety interventions by
OT Gillespie et al 2012, 159 trials, 79193 pts

Modifiable risk factors for fallsIntrinsicHistory of fallsMedicationsMedical conditionsAgeImpaired mobilityPostural instabilityDepressionVisual impairmentsFoot problemsIncontinenceNutritional deficiences
ExtrinsicEnvironmental hazardsWalking aids/assistive devicesFootwear and clothing
ExposurePhysical activityBehaviour

• Prevention programmes are efficacious• Implementation gap
– Falls prevention not a priority– Services not available – Evidence not used or modified
• Training needs to be challenging, progressive & regular• Programmes often too short term
– Refusal/non-adherence=50-90%; prevention not effective?

Resources
ProFaNE: http:/profane.co (Prevention of Falls Network Earth) - Online Community of healthcare professionals committed to the Prevention of Falls.
Later Life Training: www.laterlifetraining.co.uk Training programmes, Advice, Booklets, Videos/training DVDs, Websites
ProFouND: http://profound.eu.com disseminate best practice in falls prevention

• 21 partners 12 countries (+associate members)• disseminate best practice in falls prevention• embed evidence based programmes in at least 10
countries/15 regions by 2015 • use internet & ICT to facilitate widespread implementation • collate resources library• create PFPApp - distribute tailored, customised, best
practice guidance• cascade model e-learning to create cadre of accredited
exercise trainers across Europe• create “ICT for Falls Forum”
www.profound.eu.org


Kate Jopling
DirectorCampaign to End Loneliness
Loneliness
This event is kindly funded by an unrestricted grant from
Sanofi Pasteur MSD
#pubhealthageing

www.campaigntoendloneliness.org.uk
Kate JoplingCampaign to End Loneliness
Loneliness as a public health issue

What is loneliness
• Loneliness: “an individual’s subjective evaluation of his or her social participation or social isolation and is the outcome of …having a mismatch between the quantity and quality of existing relationships on the one hand and relationship standards on the other” [Perlman and Peplau, 1981]• Social or emotional loneliness• Can be transient, situational or chronic
• Social isolation: is objective – a measure of contacts or interactions • Solitude: “Language... has created the word "loneliness" to express the
pain of being alone. And it has created the word "solitude" to express the glory of being alone.” [Paul Johannes Tillich]

Is loneliness a public health issue?
• Department of Health: “Public health is about helping people to stay healthy, and protecting them from threats to their health”
• Faculty of Public Health:““The science and art of promoting and protecting health and well-being, preventing ill-health and prolonging life through the organised efforts of society”.
So…. Yes• It’s a threat to health• Lonely people struggle to make healthy choices• It requires a whole society response• Linked to a range of other recognised public health issues – e.g. alcohol,
healthy eating etc

www.campaigntoendloneliness.org.uk
Over half (51%) of all people aged 75 and over live alone (ONS, 2010)
A higher % of women than men report feeling lonely “some of the time” or “often” (ONS, 2013)
Loneliness in the UK

Loneliness and health: The evidence• Loneliness and isolation have a negative impact
on health: Research from the United Kingdom• Loneliness increases our risk of depression
(Green et al, 1992)• Loneliness has potentially adverse effects on
biological stress mechanisms, including greater fibrinogen (higher levels are associated with cardiovascular disease) and changes to cortisol levels (Steptoe et al., 2004)

Loneliness and health: The evidence• Loneliness and isolation have a negative impact
on healthResearch from Europe• Loneliness (not social isolation) is linked to an
64% increased risk of developing clinical dementia (Holwerda et al, 2012)
• Adults that feel lonely are more likely to suffer from psychological distress and poor self-rated health (Stickley et al., 2013)
• People that feel lonely are more likely to rate their health as poor (Stickley et al., 2013; Kaasa, 1998)

Loneliness and health: The evidence• Loneliness and isolation have a negative impact
on healthResearch from North America• Weak social connections are an equivalent risk
factor for early mortality to smoking 15 cigarettes a day, and have a great impact than other risk factors such as physical inactivity and obesity. (Holt-Lunstad, 2010)
• Loneliness increases the risk of high blood pressure, and this association increases with age (Hawkley et al, 2010)

Loneliness and health: The evidence• Loneliness and isolation contribute to harmful
health behavioursResearch from the United Kingdom• Loneliness can make older people uniquely
vulnerable to alcohol problems: alcohol may be used as a coping mechanism for loneliness, and may be linked to boredom (Wadd et al., 2011)
• Our relationships and friendships have an influence on our diet: Older adults who live alone and have infrequent contact with friends eat fewer vegetables each day. (Conklin et al., 2013)

Loneliness and health: The evidence• Loneliness and isolation contribute to harmful
health behavioursResearch from Australia • Lonely adults are more likely to be smokers and
more likely to be overweight (Lauder et al., 2006.)
Research from North America• Lonely adults are less likely to engage in physical
activity and exercise (Hawkley et al., 2009; Newall, et al.,2013)

What does a public health response to loneliness look like?
• Targeting health and wellbeing boards to put the issue on the agenda
• Need a whole community response with focus on both prevention and “cure”
• Some population-wide measures, and some targeted interventions
• Evidence based approaches – are group based, centre around people’s interests and involve older people in their design and delivery
• Build into plans for whole community – but not just about being “age friendly”, also about how other interventions are delivered (e.g. social care, but also alcohol services etc)

Julia Thrift
Project ManagerTown and Country Planning Association
Housing/planning
This event is kindly funded by an unrestricted grant from
Sanofi Pasteur MSD
#pubhealthageing

Julia Thrift, Project Manager
Town & Country Planning Association
www.tcpa.org.uk
Public Health in an Ageing Society:Planning and HousingICL

About the TCPA:
What we want to achieve?
- Decent, well designed homes for everyone
- Thriving, healthy, places
- People empowered to influence decisions about their places

About the TCPALeading the planning debate in the UK

Garden cities: health and prosperity

• Helps planners and public health practitioners understand implications of NHS and planning reforms.
• Maps out areas of overlap in planning and public health policy.
• Suggests ways in which the two professions could collaborate.
• Launched July 2012
Reuniting Health with Planning (Phase 1)

The built environment is a major factor in the ‘wider determinants’ of health.
‘Too often we intervene too late in the pathway to ill health and forget that health starts where we live, work and play.’
Institute for Health Equity
Reuniting Health with Planning (Phase 1)

Place-based approaches to health objectives

Reuniting Health with Planning (Phase 2)
Local planning, local health priorities
Place-based approaches in:
Stockport
Manchester
Knowsley
Hertfordshire
Lincolnshire
Bristol
Newham
West Midlands (published November 2013)

Reuniting Health with Planning (Phase 2)
Lincolnshire:
• Number of people aged 65+ expected to double by 2030
• Parts of the county will have very few people of working age
• This will have a significant impact on transport, services, etc.

Reuniting Health with Planning (Phase 2)
Knowsley - roundtable theme:
‘Take a co-ordinated approach to housing and health interventions across new and existing properties in Knowsley, espcially for an ageing population.’

NPPF
Planning reform: National Planning Policy Framework (2012)
‘Local planning authorities should... plan for a mix of housing based on current and future demographic trends, market trends and the needs of different groups in the community... such as... families with children, older people, people with disabilities...’
enable communities to achieve lasting growth in a way that meets all of their needs: economic, social and environmental.

A few final thoughts:
• We need to build 240,000 new homes a year.
• Building homes designed for older people might free up larger homes (which elderly often struggle to maintain & can cause poor health).
• But – new generations of old people will demand well-designed, desirable homes if they are to be tempted to move.
• Anecdotal evidence suggests some planning authorities refuse developments aimed at older people as they think they will be a burden on social services.

www.tcpa.org.uk
Julia Thrift, Project Manager
Town and Country Planning Association

Elizabeth Box
Head of ResearchRAC Foundation
Road safety
This event is kindly funded by an unrestricted grant from
Sanofi Pasteur MSD
#pubhealthageing

Road safety case study
Elizabeth Box
Head of Research
RAC Foundation
November 2013


11 April 2023Public health in an ageing society
Older drivers in GB
Over 4 million people over the age of 70 hold a full valid driving licence
Older drivers up the age of 80 have collision rates that are comparable to those of middle-aged drivers.
The increased frailty of older drivers means that they are more likely to be killed or injured in collisions than their younger counterparts
It has been estimated that 34% of older drivers give up driving too early, with only 10% giving up later than they should do.

1975/76
1985/86
1989/91
1992/94
1995/971
1998/002002
20032004
20052006
20072008
20092010
20112012
-
10
20
30
40
50
60
70
80
90
Licence holding amongst those aged 70+
AllMenWomen
% o
f pop
ulati
on w
ho h
old
a lic
ence

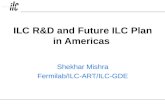
42.2
21.8
20.5
10.9
1.5 1.3 1.0 0.6 0.3
Car/van driverCar/van passengerWalkBusTaxiOther private transportRailBicycleOther public transport
Trips by mode of transport for those aged 70 and over

‘When you’re getting older, you don’t want to give up the things you’ve been doing foryears. You’ve got the time and leisure to do it. What else am I going to do?’Male participant, over 75s group, Banbury
‘I mean I wouldn’t move if that’s what you mean? Would I move into a town so that Icould get round on the transport? No.’Male participant, over 75s group, Banbury


1.18i - % of adult social care users who have as much social contact as they would like according to the Adult Social Care Users Survey
2.23i-iv. –Self-reported wellbeing (satisfaction/worthwhile/happiness/anxiety scores)
2.24. Injuries and falls in people aged 65 and over
1.10 Killed and seriously injured casualties on England’s roads
Hip fractures?
Cardiovascular disease?
Access to green spaces?
Physical activity?

11 April 2023Public health in an ageing society
Elizabeth Box MA MSc MCIHTHead of ResearchRAC Foundation89-91 Pall Mall,
LONDON. SW1Y 5HS
Tel no: 020 7747 3489Email: [email protected]: www.racfoundation.org
Thank you

Panel Debate and Q&A• How are the new structures responding to the varied public
health challenges of an ageing population?
• What should be their key focuses in order to ameliorate some of the health challenges an older age structure presents?
• Are the new public health structures focussing spending fairly across different generations?
• How should public health spending be allocated across the life course?
• How can we best evaluate, gather and disseminate evidence about what works in public health?

Public health in an ageing society
Wednesday 4th December 2013
This event is kindly funded by an unrestricted grant from
Sanofi Pasteur MSD
#pubhealthageing