Protein Kinase C Regulates Urea Permeability in the Rat Inner Medullary Collecting Duct

of 6
description
kidney
Transcript of Protein Kinase C Regulates Urea Permeability in the Rat Inner Medullary Collecting Duct
-
Protein kinase C regulates urea permeability in the rat inner medullarycollecting duct
Yanhua Wang,1 Janet D. Klein,1 Carole M. Liedtke,2 and Jeff M. Sands11Department of Medicine, Renal Division, Emory University, Atlanta, Georgia; and 2Departments of Pediatricsand Physiology and Biophysics, Case Western Reserve University, Cleveland, OhioSubmitted 3 June 2010; accepted in final form 19 September 2010
Wang Y, Klein JD, Liedtke CM, Sands JM. Protein kinase Cregulates urea permeability in the rat inner medullary collecting duct.Am J Physiol Renal Physiol 299: F1401F1406, 2010. First publishedSeptember 22, 2010; doi:10.1152/ajprenal.00322.2010.Hypertonic-ity increases urea transport independently of, as well as synergisticallywith, vasopressin in the inner medullary collect duct (IMCD). Wepreviously showed that hypertonicity does not increase the level ofcAMP in the IMCD, but it does increase the level of intracellularcalcium. Since we also showed that hypertonicity increases both thephosphorylation and biotinylation of the urea transporters UT-A1 andUT-A3, this would suggest involvement of a calcium-dependentprotein kinase in the regulation of urea transport in the inner medulla.In this study, we investigated whether protein kinase C (PKC), whichis present in the IMCD, is a regulator of urea permeability. We testedthe effect of PKC inhibitors and activators on urea permeability in theisolated, perfused rat terminal IMCD. Increasing osmolality from 290to 690 mosmol/kgH2O significantly stimulated (doubled) urea perme-ability; it returned to control levels on inhibition of PKC with either10 M chelerythrine or 50 M rottlerin. To determine the potentialsynergy between vasopressin and PKC, phorbol dibutyrate (PDBu)was used to stimulate PKC. Vasopressin stimulated urea permeability247%. Although PDBu alone did not change basal urea permeability,in the presence of vasopressin, it significantly increased urea perme-ability an additional 92%. The vasopressin and PDBu-stimulated ureapermeability was reduced to AVP alone levels by inhibition of PKC.We conclude that hypertonicity stimulates urea transport through aPKC-mediated phosphorylation. Whether PKC directly phosphory-lates UT-A1 and/or UT-A3 or phosphorylates it as a consequence ofa cascade of activations remains to be determined.
tubule perfusion; calcium signaling; urine concentration; vasopressin;hypertonicity
UREA AND UREA TRANSPORTERS (UT) are crucial for the urinaryconcentrating mechanism. Since the first observation that ureais important in the control of water homeostasis by Gambleet al. in 1934 (6), many studies have reported the integral roleof urea in the production of a concentrated urine. Early studieslooked at the effect of varying the protein level in the diets ofanimals and people (5, 6, 12). The most rigorous method ofassessing urea transport is to perform ex vivo perfusion studiesto directly measure the movement of urea across the innermedullary collecting duct (IMCD). Tubule perfusion studiesestablished that there are UT involved in the movement of ureathrough the IMCD cells (20). The transporters perform at bothbasal and stimulated levels. The regulation of these transport-ers is an important determinant in the permeability of theIMCD to urea. Studies show that urea permeability can be
affected by vasopressin, angiotensin II, calcium, steroid hor-mones, and changes in tonicity (8, 14, 20, 21).
One of the earliest observations made using tubule perfusionstudies was that vasopressin is the primary hormone thatregulates urea permeability in the IMCD (20, 24). Vasopressinbinds to the V2 receptors on the basolateral plasma membraneof the IMCD, which results in stimulation of adenylyl cyclaseand generation of cAMP. cAMP stimulates two downstreamsignals: protein kinase A and exchange protein activated bycAMP (25), thereby resulting in an increase in urea permeabil-ity.
Vasopressin stimulation of urea permeability is due, in largepart, to the stimulation of the UT-A1 and UT-A3 urea trans-porters in the IMCD (14). These urea transporters are membersof the SLC14A2 family. UT-A1 is the largest of the ureatransporters and is located at the apical plasma membraneof the IMCD. UT-A3 is essentially the NH2-terminal half ofUT-A1 and is located at the basolateral plasma membrane ofthe IMCD (18). UT-A3 is also present in the apical plasmamembrane when the animal has been treated with vasopressin,suggesting that UT-A3, as well as UT-A1, is regulated byvasopressin (3). The mechanism for vasopressins regulationinvolves vasopressin-stimulated increases in both the phos-phorylation and apical plasma membrane accumulation of theUT-A1 urea transporter (3, 4, 27).
Vasopressin is not the only regulatory stimulus for ureatransport, however. Several studies show that urea permeabilityin isolated, perfused IMCDs is also activated by hypertonicity(adding NaCl or mannitol) in the absence of vasopressin (7, 15,21). Increasing osmolality in the presence of vasopressin pro-duces an additive effect on urea permeability (7, 15, 21).Unlike vasopressin, hypertonicity increases intracellular cal-cium, but does not change cAMP accumulation (8). Thesefindings indicate that hypertonicity is an independent activatorof urea transport, and it acts through intracellular calciuminstead of cAMP. Hypertonicity increases the phosphorylationand plasma membrane accumulation of UT-A1 and UT-A3,which may result in an increase in urea permeability (2). Themanner by which hypertonicity stimulates the urea transportersor urea permeability is not yet understood.
The present study extends information about PKC signalingon urea permeability. We first determined whether PKC isinvolved in hypertonicity-stimulated urea permeability. Theprimary rationale for performing this aspect of our study is thathypertonicity increases urea permeability via changes in intra-cellular calcium, suggesting involvement of a calcium-depen-dent protein kinase in the urea transport response. Next, weexplored the mechanisms for PKC regulation and tested thehypothesis that PKC synergistically works with cAMP tostimulate urea permeability.
Address for reprint requests and other correspondence: Y. Wang, EmoryUniv. School of Medicine, Renal Div., 1639 Pierce Dr., NE, WMB Rm. 3304,Atlanta, GA 30322 (e-mail: [email protected]).
Am J Physiol Renal Physiol 299: F1401F1406, 2010.First published September 22, 2010; doi:10.1152/ajprenal.00322.2010.
0363-6127/10 Copyright 2010 the American Physiological Societyhttp://www.ajprenal.org F1401
-
METHODS
Animals. All animal protocols were approved by the Emory Uni-versity Institutional Animal Care and Use Committee. Male Sprague-Dawley rats (Charles River Laboratories, Wilmington, MA), weighing5075 g, were injected with furosemide (5 mg/kg body wt) 30 minbefore death. Kidneys were dissected to remove inner medullas.Single tubules from the terminal IMCD were microdissected at 17C.
Tubule perfusion. Single IMCDs were dissected, mounted on glasspipettes, and perfused as described previously (19, 20). In general, 45min after the tubules were warmed to 37C in 1 ml of bath solution,three 1-min collections of 3050 nl/min were made.
To measure the response to treatments, buffers were changed ortreatments were added to the bath, tubules were allowed to equilibratefor 15 min, then three further collections were made, and urea wasassessed using ultramicrofluorometry. Urea permeability was calcu-lated as described previously (19, 20).
To subject the tubules to hypertonic conditions, the osmolalities ofboth the perfusate and the bath were increased from 290 to 690mosmol/kgH2O by adding 200 mM NaCl. To assess the contributionof PKC, cell-permeable PKC inhibitors (10 M chelerythrine or 50M rottlerin) were added to the bath. Alternatively, the PKC stimu-lator phorbol-dibutyrate (PDBu; 200 nM) was added to the bath.
To test for synergistic effects of cAMP and PKC on urea perme-ability, basal urea permeability was measured followed by sequentialaddition of vasopressin and PDBu. First, 200 pM vasopressin wasadded to the bath and urea permeability was measured. Next, 200 nMPDBu was added to the bath in the presence of vasopressin, and ureapermeability was measured. In an additional approach, both 200 pMvasopressin and 200 nM PDBu were added simultaneously to the bath45 min after the tubule was warmed to 37C. After 15 min, ureapermeability was measured. To verify that the effects observed withsimultaneous PDBu/vasopressin treatment were due to PKC, 10 Mchelerythrine was added to the bath, and urea permeability wasmeasured.
Western blot analysis. Identical samples of whole inner medullaryprotein lysate (20 g/lane) were size separated by SDS-PAGE on10% gels and then electroblotted to polyvinylidene difluoride mem-branes (Immobilon, Millipore, Bedford, MA). Blots were blockedwith 5% nonfat dry milk in Tris-buffered saline (20 mM TrisHCl, 0.5M NaCl, pH 7.5) and then incubated with primary antibodies over-night at 4C. Attached primary antibodies were identified using AlexaFluor 680-linked anti-rabbit IgG (Molecular Probes, Eugene, OR) andvisualized using infrared detection with the LICOR Odyssey proteinanalysis system (Lincoln, NE). Antibodies to PKC , , , , , , and were purchased from Cell Signaling Technology (Danvers, MA).
Statistics. All data are presented as means SE. Data from tubuleperfusion studies were analyzed using a paired Students t-test orrepeated-measures ANOVA, depending on whether two conditions ormore than two conditions were assessed in each tubule (22). Eachtubule serves as its own control, allowing a paired analysis of the data.The criterion for statistical significance is P 0.05.
RESULTS
Urea permeability in hypertonic conditions. Increasing theosmolality of the perfusate and bath solutions from 290 to 690mosmol/kgH2O resulted in a significant increase in urea per-meability from 24 2 to 49 4 105 cm/s (n 4, P
0.01; Fig. 1A). The increased urea permeability was signifi-cantly reduced to 30 3 105 cm/s by addition of the PKCinhibitor chelerythrine (10 M) to the hypertonic bath solution(n 4, P 0.01; Fig. 1A). The bar graph in Fig. 1B shows theurea permeabilities as a percent of control levels. Hypertonicityincreased urea permeability to 208% of the level in isotonicconditions. Urea permeability was returned to nearly controllevels (129%) by inhibition of PKC with chelerythrine.
To further confirm the role of PKC in the regulation of ureapermeability, 50 M rottlerin (a second chemical inhibitor ofPKC that inhibits a wide spectrum of PKCs at 50 M) wasadded to the hypertonic bath. As before, hypertonicity in-creased urea permeability from 23 2 to 43 3 105 cm/s(n 4, P 0.01; Fig. 2A). Addition of rottlerin significantlydecreased urea permeability to 21 2 105 cm/s (n 4,P 0.01; Fig. 2A). The changes in permeability as percent ofcontrol are presented in bar graph form in Fig. 2B. Hyperto-nicity increased urea permeability by 191%. Urea permeabilitywas returned to nearly control levels (90%) by inhibition ofPKC with rottlerin.
Urea permeability stimulated by PDBu. To verify the effectsof the PKC inhibitors, we measured urea permeability whenPKC was stimulated using a phorbol ester, PDBu (200 nM),which is known to stimulate the regulatory domain of PKC(16). The urea permeability after PDBu treatment (32 3 105 cm/s) was not different from basal urea permeability (29 1 105 cm/s, n 4).
Three approaches were designed to test for synergistic ef-fects of PDBu and vasopressin. First, urea permeabilities were
Fig. 1. Urea permeability in terminal inner med-ullary collecting ducts (IMCDs) was increasedby hypertonicity. A: terminal IMCDs were per-fused with isotonic buffer (290 mosmol/kgH2O),then switched to hypertonic buffer (690 mosmol/kgH2O), and then supplemented with 10 Mchelerythrine (Chel). Each line represents a sep-arate IMCD from a different rat. B: bar graphshows the percent change from isotonic controllevels. Bars means SE. *P 0.01 vs. 290mosmol/kgH2O; #P 0.01 vs. 690 mosmol/kgH2O without inhibitor; n 4 rats/condition.
F1402 PKC REGULATES UREA PERMEABILITY
AJP-Renal Physiol VOL 299 DECEMBER 2010 www.ajprenal.org
-
assessed under conditions where vasopressin-stimulatedIMCDs were then treated with a PKC stimulant. Figure 3shows this approach. Vasopressin significantly increased ureapermeability from 21 2 to 74 16 105 cm/s (n 6,P 0.05; Fig. 3A). Subsequent addition of 200 nM PDBu tothe bath (to stimulate PKC with vasopressin present) furtherincreased urea permeability to 94 18 105 cm/s (n 5,P 0.05; Fig. 3A). The changes in permeability as percent ofcontrol are presented in bar graph form in Fig. 3B. Vasopressinincreased urea permeability from 100% (basal control) to347%. Urea permeability was further increased to 439% bystimulation of PKC with PDBu. We also performed the timecontrol experiment where vasopressin was added after theinitial 45-min warming period (basal readings), and urea per-meability was monitored periodically over an additional 45min. Within 15 min following addition of vasopressin to thebath, urea permeability increased from 15 1 to 60 7 105 cm/s, where it was maintained for an additional 30 min(data not shown).
The second approach was to stimulate urea permeability byadding vasopressin and PDBu together, and then assesswhether inhibition of PKC removed the stimulation of ureapermeability. The tubules were treated initially with both 200pM vasopressin and 200 nM PDBu and urea permeability wasmeasured (80 8 105 cm/s, n 4; Fig. 4A). To verify
that the effects observed with simultaneous PDBu/vasopressin treatment include a PKC-mediated stimulation,10 M chelerythrine was added to the bath. Urea perme-ability significantly decreased to 58 6 105 cm/s (n 4, P 0.01 by paired t-test; Fig. 4A). The changes inpermeability as percent of control are presented in bar graphform in Fig. 4B. Chelerythrine decreased urea permeabilityfrom 100% (vasopressinPDBu control) to 72%. To ensurethat the changes observed with chelerythrine were not due tothe prolonged exposure to PDBu, we performed a timecontrol in which PDBu and vasopressin were both present inboth periods. Urea permeability was 72 7 105 cm/s inperiod 1 and showed a slight increase to 84 4 105cm/s in period 2 (n 3, P NS).
The third approach to determining the potential synergybetween vasopressin and PKC was to determine whether inhi-bition of PKC would block the action of PDBu on ureapermeability. To ensure that chelerythrine was inhibiting byblocking PKC and not directly affecting vasopressin-mediatedurea permeability, tubules were first treated with 200 pMvasopressin, then incubated with 10 M chelerythrine, andfinally treated with 200 nM PDBu. Chelerythrine significantlydecreased urea permeability from 61 6 to 53 7 105cm/s in the IMCDs initially treated with 200 pM vasopressinalone (n 4, P 0.05; Fig. 5A). Subsequent addition of 200
Fig. 2. Hypertonicity-induced increase in ureapermeability was reversed by inhibition of pro-tein kinase C (PKC) with rottlerin (Rott).A: terminal IMCDs were perfused with iso-tonic buffer (290 mosmol/kgH2O), thenswitched to hypertonic buffer (690 mosmol/kgH2O), and then supplemented with 50 MRott. Each line represents a separate IMCDfrom a different rat. B: bar graph showingthe percent change from isotonic controllevels. Bars means SE. *P 0.01 vs.290 mosmol/kgH2O; #P 0.01 vs. 690mosmol/kgH2O without inhibitor; n 4rats/condition.
Fig. 3. PKC stimulates urea permeabilityabove cAMP-stimulated levels. A: perfusedIMCDs after 45 min with buffer withoutstimulants (basal), then with 200 pM vaso-pressin (AVP) added to the bath for 15 min,and finally with 200 nM phorbol dibutyrate(PDBu) added to the bath for a further 15min. Each line represents a separate IMCDfrom a different rat. B: bar graph showingthe percent change from basal control levels.Bars means SE. *P 0.05 vs. basal(unstimulated) conditions; #P 0.05 vs.AVP-stimulated levels; n 5 separate ratterminal IMCDs.
F1403PKC REGULATES UREA PERMEABILITY
AJP-Renal Physiol VOL 299 DECEMBER 2010 www.ajprenal.org
-
nM PDBu (with vasopressin and chelerythrine present) to thebath did not increase the urea permeability. Instead, ureapermeability continued to decrease to 43 6 105 cm/s(n 4, P 0.01; Fig. 5A). The changes in urea permeabilityas percent of control are presented in bar graph form in Fig. 5B.Urea permeability was decreased from 100% (vasopressincontrol) to 87% by addition of chelerythrine, and continued todecrease to 71% during the 15 min after addition of PDBu.
To ensure that the decrease in urea permeability was not dueto an effect of the PKC inhibitor that was greater during thethird compared with the second set of collections, we per-formed a time control in which PDBu and vasopressin wereboth present in periods 2 and 3. Urea permeability was 84 4 105 cm/s in period 2 and 90 2 105 cm/s in period3 (n 3, P NS).
Effect of PKC inhibition under isotonic conditions. To ex-amine the effect of PKC antagonists on urea permeability in theabsence of hypertonicity, we perfused tubules using isotonic(290 mosmol/kgH2O) solutions. The PKC inhibitor cheleryth-rine (10 M) did not change urea permeability (basal: 15 1,chelerythrine: 12 1 105 cm/s, n 3, P NS; Fig. 6A).Subsequent addition of vasopressin (200 pM) with cheleryth-rine still present did not change urea permeability (13 1 105 cm/s, n 3, P NS; Fig. 6B).
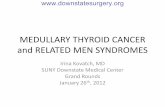
PKC isoforms in kidney inner medulla. The identity of thePKC isoform that is involved in the increase of urea perme-ability in the inner medulla is unknown. There are several PKCisoforms that are expressed in the inner medulla (Fig. 7)including conventional PKC isoforms that are responsive tocalcium and diacylglycerol (PKC, PKC, and PKC), as wellas novel isoforms (PKC, PKC, PKC, and PKC) which arecalcium independent, and the atypical isoform, PKC. Ofthese, both conventional and novel PKC isoforms are respon-sive to phorbol ester activation and thus would be potentialactivators of urea permeability in the inner medulla.
DISCUSSION
It is well-established that urea permeability is regulated byvasopressin via cAMP-dependent signaling pathways. Thisstudy provides evidence that hypertonicity increases urea per-meability through a PKC-signaling pathway. In addition, directactivation of PKC by a phorbol ester, PDBu, requires thesynergy of vasopressin to stimulate urea permeability. To-gether with findings from previous studies (14, 27), the presentstudy suggests that maximal increases in urea transport in ratterminal IMCDs require stimulation of both cAMP and PKC-signaling pathways.
Fig. 4. Stimulation of urea permeability by AVPand PDBu is decreased on inhibition of PKC withChel. A: IMCDs were perfused with buffer con-taining both 200 pM AVP and 200 nM PDBu for15 min and then treated for an additional 15 minwith 10 M Chel. Each line represents a separateIMCD from a different rat. B: bar graph showingthe percent change in urea permeability on inhibi-tion of PKC. Bars means SE. *P 0.01 vs.AVP PDBu, n 4 rat terminal IMCDs.
Fig. 5. Inhibition of PKC blocks stimulation ofurea permeability by phorbol esters. A: IMCDswere stimulated with 200 pM AVP for 15 min,then 10 M Chel was added for 15 min, andfinally 200 nM PDBu was added for 15 min.Each line represents a separate IMCD from adifferent rat. B: bar graph showing the percentchange in AVP-stimulated urea permeability oninhibition of PKC with Chel, and then stimula-tion of PKC with PDBu. Bars means SE.*P 0.05 vs. AVP; #P 0.01 vs. AVPChel;n 4 rat terminal IMCDs.
F1404 PKC REGULATES UREA PERMEABILITY
AJP-Renal Physiol VOL 299 DECEMBER 2010 www.ajprenal.org
-
Previous studies show that hypertonicity increases urea per-meability (21) and plasma membrane accumulation of bothUT-A1 and UT-A3 in rat terminal IMCDs (2). The responsesto hypertonicity occur through increases in intracellular cal-cium and activation of PKC has been suggested to play a role(8, 14). To determine the role of PKC in hypertonicity-stimu-lated urea permeability, hypertonicity (690 mosmol/kgH2O)was used as a means to stimulate PKC in the present study. Ourdata show that hypertonicity significantly increases urea per-meability (Figs. 1 and 2), which is consistent with a previousstudy (21). To verify that the increase in urea permeability is inresponse to activation of PKC, two PKC inhibitors, cheleryth-rine and rottlerin, were used to decrease urea permeability.Chelerythrine acts on the catalytic domain of PKC and is abroad-type inhibitor of PKC. Rottlerin is a PKC-specificinhibitor. However, at the higher concentration (50 M) usedin this study, rottlerin also inhibits a broad spectrum of PKCisoforms, including PKC, PKC, PKC, and PKC, andPKC, PKC, and PKC with a reduced inhibitory activity(911, 23). The data in the present study show that both PKCinhibitors reversed the increase by hypertonicity to nearly basallevels of urea permeability (Figs. 1 and 2), which stronglysupports the concept that hypertonicity increases urea perme-ability by stimulating PKC.
To understand the mechanism by which the PKC pathwayregulates urea permeability, we also used the phorbol esterPDBu to directly stimulate PKC. PDBu binds to the regulatorydomain of PKC and thereby activates it (16). The present studyshows that PDBu alone does not change urea permeability.However, PDBu significantly increased vasopressin-stimulated
urea permeability (Fig. 3). These data suggest that an interac-tion between vasopressin and PKC is necessary for PKC tostimulate urea permeability.
Angiotensin II has been shown to exert its effects throughPKC-mediated pathways. Liu and Cogan (17) showed thatPKC may be involved in as much as one-third of the angio-tensin II-stimulated bicarbonate and water transport in the S1and S2 segments of the proximal tubule. Amlal et al. (1)reported that a high concentration (5 1011 M) of angio-tensin II stimulates Na-K-NH4-2Cl cotransport via PKCin the medullary thick ascending limb. In rat IMCDs, angio-tensin II significantly increases urea permeability above vaso-pressin-stimulated levels (14), similar to the effects observed inthe present study for PDBu. Angiotensin II has also beenshown to increase UT-A1 phosphorylation in rat IMCD sus-pensions (14). The angiotensin II-mediated increases in func-tion and phosphorylation can be blocked by a PKC inhibitor(14), suggesting a role for PKC-mediated signaling in theregulation of urea transport.
Interestingly, our previous data showed that angiotensin IIalone, which can activate PKC in several renal tubule segments(1, 17), had no effect on basal (no added vasopressin) ureapermeability (14). However, angiotensin II significantly in-creased vasopressin-stimulated urea permeability (14). Thecomparable pattern of regulation by PDBu and by angiotensinII adds more credence to the hypothesis that PKC is involvedin regulation of urea permeability by supplementing or enhanc-ing vasopressin-stimulated urea permeability. The increase inurea permeability observed with simultaneous PDBu/vasopres-sin treatment was significantly reversed by chelerythrine, con-
Fig. 6. Chel does not inhibit urea permeabilityunder isotonic conditions and AVP fails to in-crease urea permeability in the presence of Chel.A: IMCDs were equilibrated at 290 mosmol/kgH2O, then 10 M Chel was added for 15 min,and finally 200 pM AVP was added for 15 min.Each line represents a separate IMCD from adifferent rat. B: bar graph showing the percentchange in urea permeability on inhibition of PKCwith Chel, and then stimulation of PKC withAVP. Bars means SE. P NS; n 3 ratterminal IMCDs.
Fig. 7. Seven PKC isoforms are present in ratinner medulla. Lysate from whole rat innermedulla was analyzed by Western blot usingPKC isoform-specific antibodies. An arrowidentifies the PKC protein bands.
F1405PKC REGULATES UREA PERMEABILITY
AJP-Renal Physiol VOL 299 DECEMBER 2010 www.ajprenal.org
-
sistent with PKC-mediated stimulation (Fig. 4). Finally, afterPKC was blocked with chelerythrine, PDBu treatment did notincrease vasopressin-stimulated urea permeability (Fig. 5). Theagreement of the inhibitor and stimulator results stronglysupports the idea of an interaction between vasopressin andPKC.
Recently, Yano et al. (26) demonstrated that glucagon re-duces urea permeability and UT-A1 expression via a glucagonreceptor and by stimulating PKC with phorbol myristate. Thisdiffers from our finding where stimulating PKC with PDBuhad no effect on basal urea permeability. Their finding alsodiffers from Isozaki et al. (13) who found no effect of glucaconon urea permeability. We do not have an explanation for thesedifferences, but possibilities include the use of different ratstrains (Wistar by Yano et al. vs. Sprague-Dawley by Isozakiet al. and present study) and different agonists (phorbol my-ristate vs. PDBu).
We do not know why hypertonicity independently initiatesPKC activation in the absence of overt vasopressin stimulation.It is possible that it only requires the endogenous vasopressinlevel to support the action of PKC in response to hypertonicity.In light of this hypertonic response, it is unclear why stimula-tion of PKC with PDBu or angiotensin II (14) does not showany stimulation of urea permeability in the absence of addi-tional exogenous vasopressin. Perhaps hypertonicity activatesdifferent PKC isoform(s) than PDBu or angiotensin II, is abetter activator, or stimulates additional signaling pathways?Further studies are needed to test these possible mechanisms.Clearly, however, in the presence of vasopressin, PDBu stim-ulation of PKC causes a significant increase in urea permeabil-ity.
In conclusion, the findings from the present study show thatPKC regulates urea permeability in conjunction with vasopres-sin. These findings are likely to be physiologically significant.During antidiuresis, the inner medulla is often quite hypertonic.Under antidiuretic conditions, therefore, the increase in tonicitymay be instrumental in increasing urea permeability throughPKC-signaling pathways, in addition to the actions of vaso-pressin. We conclude that maximal stimulation of urea perme-ability in rat terminal IMCDs requires stimulation by bothcAMP and PKC. Whether PKC directly phosphorylates UT-A1and/or UT-A3, or phosphorylates as a consequence of a cas-cade of activations, remains to be determined.GRANTS
This work was supported by National Institutes of Health Grants R01-DK-41707, R01-DK-62081, and P01-DK-61521.
DISCLOSURESNo conflicts of interest, financial or otherwise, are declared by the author(s).
REFERENCES
1. Amlal H, Legoff C, Vernimmen C, Soleimani M, Paillard M, BicharaM. ANG II controls Na-K(NH4)-2Cl cotransport via 20-HETE andPKC in medullary thick ascending limb. Am J Physiol Cell Physiol 274:C1047C1056, 1998.
2. Blessing NW, Blount MA, Sands JM, Martin CF, Klein JD. Ureatransporters UT-A1 and UT-A3 accumulate in the plasma membrane inresponse to increased hypertonicity. Am J Physiol Renal Physiol 295:F1336F1341, 2008.
3. Blount MA, Klein JD, Martin CF, Tchapyjnikov D, Sands JM.Forskolin stimulates phosphorylation and membrane accumulation ofUT-A3. Am J Physiol Renal Physiol 293: F1308F1313, 2007.
4. Blount MA, Mistry AC, Frhlich O, Price SR, Chen G, Sands JM,Klein JD. Phosphorylation of UT-A1 urea transporter at serines 486 and499 is important for vasopressin-regulated activity and membrane accu-mulation. Am J Physiol Renal Physiol 295: F295F299, 2008.
5. Epstein FH, Kleeman CR, Pursel S, Hendrikx A. The effect of feedingprotein and urea on the renal concentrating process. J Clin Invest 36:635641, 1957.
6. Gamble JL, McKhann CF, Butler AM, Tuthill E. An economy of waterin renal function referable to urea. Am J Physiol 109: 139154, 1934.
7. Gillin AG, Sands JM. Characteristics of osmolarity-stimulated ureatransport in rat IMCD. Am J Physiol Renal Fluid Electrolyte Physiol 262:F1061F1067, 1992.
8. Gillin AG, Star RA, Sands JM. Osmolarity-stimulated urea transport inrat terminal IMCD: role of intracellular calcium. Am J Physiol Renal FluidElectrolyte Physiol 265: F272F277, 1993.
9. Gschwendt M, Kittstein W, Furstenberger G, Marks F. The mouse earedema: a quantitatively evaluable assay for tumor promoting compoundsand for inhibitors of tumor promotion. Cancer Lett 25: 177185, 1984.
10. Gschwendt M, Kittstein W, Marks F. Elongation factor-2 kinase:effective inhibition by the novel protein kinase inhibitor rottlerin andrelative insensitivity towards staurosporine. FEBS Lett 338: 8588, 1994.
11. Gschwendt M, Muller, HJ, Kielbassa K, Zang R, Kittstein W, RinckeG, Marks F. Rottleriin, a novel protein kinase inhibitor. Biochem BiophysRes Commun 199: 9398, 1994.
12. Hendrikx A, Epstein FH. Effect of feeding protein and urea on renalconcentrating ability in the rat. Am J Physiol 195: 539542, 1958.
13. Isozaki T, Gillin AG, Swanson CE, Sands JM. Protein restrictionsequentially induces new urea transport processes in rat initial IMCDs. AmJ Physiol Renal Fluid Electrolyte Physiol 266: F756F761, 1994.
14. Kato A, Klein JD, Zhang C, Sands JM. Angiotensin II increasesvasopressin-stimulated facilitated urea permeability in rat terminalIMCDs. Am J Physiol Renal Physiol 279: F835F840, 2000.
15. Kudo LH, Csar KR, Ping WC, Rocha AS. Effect of peritubularhypertonicity on water and urea transport of inner medullary collectingduct. Am J Physiol Renal Fluid Electrolyte Physiol 262: F338F347,1992.
16. Li Q, Vaingankar SM, Green HM, Martins-Green M. Activation of the9E3/cCAF chemokine by phorbol esters occurs via multiple signal trans-duction pathways that converge to MEK/ERK2 and activate the Elk1transcription factor. J Biol Chem 274: 1545415465, 2010.
17. Liu FY, Cogan MG. Role of protein kinase C in proximal bicarbonatereabsorption and angiotensin signaling. Am J Physiol Renal Fluid Elec-trolyte Physiol 258: F927F933, 1990.
18. Sands JM. Molecular mechanisms of urea transport. J Membr Biol 191:149163, 2003.
19. Sands JM, Knepper MA. Urea permeability of mammalian inner med-ullary collecting duct system and papillary surface epithelium. J ClinInvest 79: 138147, 1987.
20. Sands JM, Nonoguchi H, Knepper MA. Vasopressin effects on urea andH2O transport in inner medullary collecting duct subsegments. Am JPhysiol Renal Fluid Electrolyte Physiol 253: F823F832, 1987.
21. Sands JM, Schrader DC. An independent effect of osmolality on ureatransport in rat terminal IMCDs. J Clin Invest 88: 137142, 1991.
22. Snedecor GW, Cochran WG. Statistical Methods. Ames, IA: Iowa StateUniv. Press, 1980.
23. Villalba M, Kasibhatla S, Genestier L, Mahboubi A, Green DR,Altman A. Protein kinase C cooperates with calcineurin to induce Fasligand expression during activation-induced T cell death. J Immunol 163:58135819, 1999.
24. Wall SM, Suk Han J, Chou CL, Knepper MA. Kinetics of urea andwater permeability activation by vasopressin in rat terminal IMCD. Am JPhysiol Renal Fluid Electrolyte Physiol 262: F989F998, 1992.
25. Wang Y, Klein JD, Blount MA, Martin CF, Kent KJ, Pech V, WallSM, Sands JM. Epac regulation of the UT-A1 urea transporter in ratIMCDs. J Am Soc Nephrol 20: 20182024, 2009.
26. Yano Y, Rodrigues AC Jr, de Braganca AC, Andrade LC, MagaldiAJ. PKC stimulated by glucagon decreases UT-A1 urea transporterexpression in rat IMCD. Pflgers Arch 456: 12291237, 2008.
27. Zhang C, Sands JM, Klein JD. Vasopressin rapidly increases thephosphorylation of the UT-A1 urea transporter activity in rat IMCDsthrough PKA. Am J Physiol Renal Physiol 282: F85F90, 2002.
F1406 PKC REGULATES UREA PERMEABILITY
AJP-Renal Physiol VOL 299 DECEMBER 2010 www.ajprenal.org