# 3 UREA CYCLE Reactions of the Urea Cycle Enzyme Regulation of the Urea Cycle Nutritional...
22
# 3 UREA CYCLE # 3 UREA CYCLE •Reactions of the Urea Cycle •Enzyme Regulation of the Urea Cycle •Nutritional Regulation of Urea Synthesis •Urea Cycle Disorders & Treatment
-
Upload
ireland-grubbs -
Category
Documents
-
view
346 -
download
2
Transcript of # 3 UREA CYCLE Reactions of the Urea Cycle Enzyme Regulation of the Urea Cycle Nutritional...

# 3 UREA CYCLE# 3 UREA CYCLE
• Reactions of the Urea Cycle
• Enzyme Regulation of the Urea Cycle
• Nutritional Regulation of Urea Synthesis
• Urea Cycle Disorders & Treatment

Urea CycleUrea Cycle1. GDH is the major agency responsible for ammonium
production.2. Ammonium is toxic (N = 15 - 40M , max 70M)
Urine: organic acids and orotic acid3. Liver: Principal site but also in small intestine4. Excretion NH4
+ by kidneys important for acid-base balance but Normally 80-90% N urine as urea.
5. Hyperammonium >500M plasma [NH4+] = TOXIC
related to inborn errors of metabolism (genetic defects) as well as induced (liver failure) Usually detected in the newborn period.Blood: measure ammonium, AA, lactate
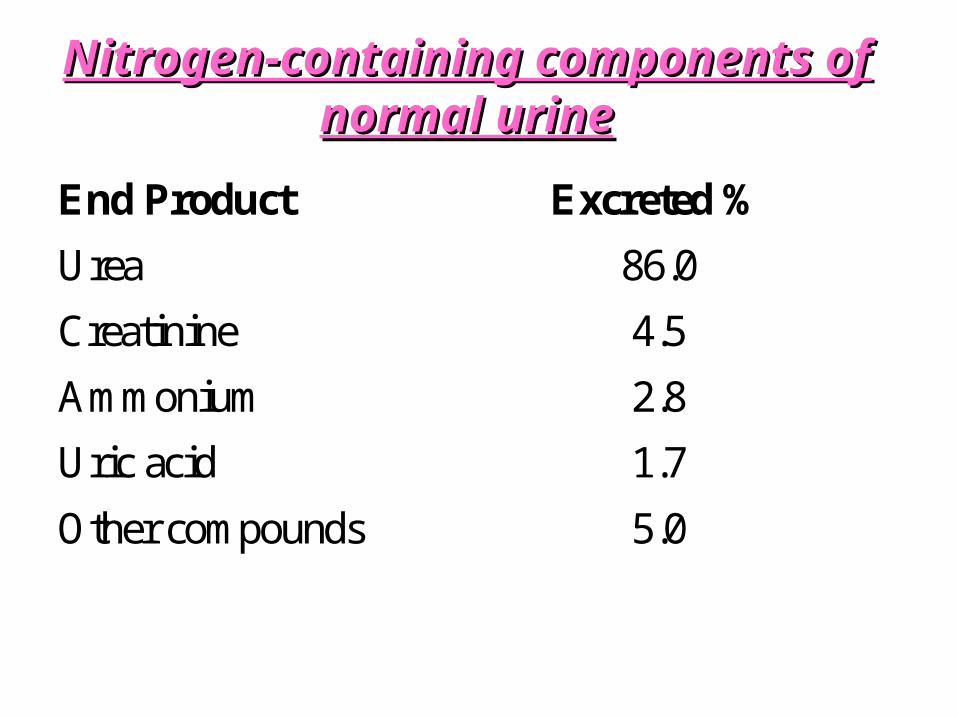
Nitrogen-containing components of normal urineNitrogen-containing components of normal urine
End Product Excreted %
Urea 86.0
Creatinine 4.5
Ammonium 2.8
Uric acid 1.7
Other compounds 5.0

Urea CycleUrea Cycle1. The urea cycle was the first metabolic process to be
described as a cycle by Sir Hans Krebs who also described the TCA cycle.
2. Role of Urea cycle: rid the body of toxic NH 4 +
therefore permitting the use of AA as an energy source.
3. Liver major site of urea synthesis, major source of arginase, (small amounts in small intestine) and is the only tissue with the complete set of all 5 enzymes required
4. Other tissues have enzymes for reactions (iii) and (iv) only to make ARG or NO (important in blood pressure, neuro transmission, macrophage antibacterial action)

Urea Cycle

Urea CycleUrea Cycle
I. Compartmentation: mitochondria (rxn 1&2) cytosol (rxn 3-5)
II. CP = 20% mitochondrial protein
III. Cyclic inter conversion of ornithine / arginine.
IV. Ornithine is used in the same way as is oxaloacetate in the TCA cycle. It is the carrier of a substituent group that undergoes modification and is subsequently split off.

1. 2 N per urea molecule: 1 NH4+ (start) + 1 transferred from ARG
2. 4 high energy phosphate: 2 ATP ADP + Pi1 ATP AMP + PpiTherefore 2 ATP / amino (N) group
Overall catabolism: Catabolize 1 Leu 32 ATP (from TCA cycle)
Make urea from N 2 ATPNET ENERGY 30 ATP produced
Mathematics of equationMathematics of equation

Short term Regulation: CPS1Short term Regulation: CPS11. NAG(N-acetyl glutamate), a positive allsoteric regulator is absolutely
required.Alters enzyme conformation
2. NAG is synthesized in liver mitochondria from acetyl CoA and GLUFA or pyruvate acetyl CoADiet or tissue proteins AA GLU and ARGAcetyl CoA + GLU NAG (enzyme = NAG synthase)
3. NAG synthesis is markedly stimulated by ARG (allosteric) but not completely dependent ( V max) therefore AA NAG
4. Hyperammonemia that develops with acidemia NAG synthesis inhibition (propionic acidemia, isovaleric acidemia, nethylmalonic acidemia) due to competition for CoA (see figure)

Regulation via NAGRegulation via NAG

Regulation through MgRegulation through Mg2+2+
(i) Mg2+: CPS1 dependent Mg2+ ( both ATP and free)
Therefore changes in mitochondrial citrate can affect reaction since citrate chelates Mg2+
(ii) Zn2+ is present in mitochondria
Zn2+ decreases CPSI activity in vitro
However, AA (ornithine) can chelate Zn therefore preventing inhibition of CPS1.
(iii) CPS1 20% total liver protein (0.4 mM) [substrate] eg NH4
+, HCO3, ATP - Mg2+, NAG
Therefore not operating at maximum capacity and important to inhibit to keep some NH4
+ available to make GLN

Nutritional RegulationNutritional Regulation
“long term regulation”(i) Five Urea Cycle enzymes & NAG synthase
all with low P diets & with high P diets
Therefore regulated nutritionally (over the long term)
(ii) Note also during starvation due to AA catabolism therefore although muscle and liver protein the level of these enzymes due to increased urea synthesis
-increased enzyme synthesis
-decrease enzyme degradation
(iii) Changes take place over 3-7 days.

Urea Cycle DisordersUrea Cycle Disorders
Prevalence of disorders: 1/30,000 live births but may be more since some die undiagnosed.
Mode of inheritance = usually autosomal recessive (2 - ve genes) OTC (most common) X-linked, heterozygotes generally asymptomatic
(i) Deficiency enzymes rxn 1-4 hyperammonemia. In general: concentration of AA metabolites proximal & distal.
(ii) In all disorders: NH4, GLN, ALA
(iii) Less severe defects: (partial deficiencies) less side effects, manifested only in later childhood or adulthood.

Defects of Urea CycleDefects of Urea Cycle
↑ orotic acid
III
IV
V
PresentationPresentationSevere Illness: First week
Usually normal first 24h
Symptoms of hyperammonemia within 1-3 days
Include: Feeding intolerance
Vomiting
Lethargy
Irritability
Respiratory Distress (hyperventilation)
Seizures
Coma

OutcomeOutcomeMortality
Improvements in treatment have increased 1 year survival rate. Once past the neonatal period, long term survival rate =
50% OTC (Type II)
75% CPS (Type I)
95% AS and AL (Steps 3+4)
Morbidity
75% mental retardation (mean IQ 50), Seizure disorders, Visual deficits (proportional to extent of NH4 ), Protein intolerance
Brain: NH4 causes increased permeability and TRP
serotonin behavior abnormalities
quinolininc acid neuronal injury
Also with type V block Arg but ~ NH4+ severely retarded
Treatment: Reduce N IntakeTreatment: Reduce N IntakeProvide sufficient for growth (need EAA ) but avoid NH4 using a
high calorie low P diet
Provide ARG supplement (except type V) since ARG synthesis therefore growth, N incorporation into AA therefore NH4
ARG also NAG synthase therefore CPSI (if not type I)
ARG also ornithine (ARG is precursor) especially important in type III and IV (where citrulline & arginosuccinate are lost in urine)
ARG also alternate NH4+ excretion (through alternate pathway)
Replacement with EAA (as keto acids to limit N intake) which can be formed into AA through transamination

Treatment (cont’d)Treatment (cont’d)
1. Compounds to Conjugate AA:( urea load) (see Diagram)
Benzoate: combines with GLY to generate hippurate urine
Phenylacetate: +GLN to produce phenylacetyl GLN urine
2. NAG Permeable Analog:
N carbamoyl glutamate enters mitochondrial.
3. Hemodialysis used to remove both AA & NH4 during hyperammonemia coma

Treatment:Treatment:Stimulate Alternate PathwaysStimulate Alternate Pathways
Stimulate Alternate Pathway: ARG ornithine citrulline arginino succinateCitrulline & argino succinate can be secreted in urine

FutureFuture(i) Enzyme Replacement Therapy
(Liver Transplant) but expensive and lack donors
(ii) Gene Therapy In mice to date, In OTC deficient mouse transfection using adeno
virus vector is successful
(iii) DiagnosisMolecular Diagnostics (RFLP) can reveal genetic defects by
prenatal diagnosis when indicated.
Direct enzyme determination in amniocytes or chorionic vilus biopsy to determine presence/absence enzyme
Reactive or anticipatory treatment if defect suspected

Case #3 DiscussionA 6-month-old infant began to vomit occasionally and
ceased to gain weight. At age 8½ months he was readmitted to the hospital. Routine examination and laboratory tests were normal, but after 1 week he became habitually drowsy, his temperature rose to 39.4oC, his pulse was elevated, and his liver was enlarged. The electroencephalogram was grossly abnormal.
Since the infant could not retain milk given by gavage feeding, intravenous glucose was administered. He improved rapidly and came out of the coma in 24 hours. Analysis of his urine showed abnormally high amounts of glutamine, uracil & orotic acid but ↓ urea, which suggested a high blood ammonium concentration. This was confirmed by the laboratory.

Discussion:Discussion: 1. Hereditary hyperammonemia can result from defects in genes for urea cycle enzymes. Which enzymes might be affected? 2. Considering the data (↑ uracil & orotic acid) which enzyme may be defective in this patient? 3. Why was the urine glutamine concentration elevated?
1. Hyperammonemia is characteristic of all steps (including NAG synthase) Most frequent OTC
2. N BUN ( blood urea N), ALSO uracil (& orotic acid) due to carbamoyl phosphate which leaks from mito cyto increased pyrimidine synthesis. Unusual: clinical symptoms slow (6 months old)
3 Why? Exceeds kidneys ability GLN GLU + NH4+

Cont’dCont’d4. Offer a genetic explanation for the observation that this
disease is usually lethal in males but not in affected females.5. This patient was treated using procedures available at
the time. He was given a daily diet of 1.5 g of protein/kg body weight. After 2 years on this diet, his height and weight were judged to be normal for his age. What is the effect of diet on a growing child in terms of nitrogen balance?
6. How would you treat a similar patient today?4. Disease is x linked, men have only 1 X chromosome, women have two X chromosomes. Therefore more severe in men than women (usually).
5. Growing child requires increased N, therefore load on urea P diet. Balance between P restriction (prevent NH4
+) and enough for growth. Not usually sufficient for patients -ve OTC
6. Hemodialysis / transfusion asap (prevent brain damage)IV benzoate, phenylacetate to act as NH4 traps