Chemistry 17.2-Protein-degradation-and-amino-acid-catabolism
Upload
chhabra-namrataCategory
view
1.690download
3description

Amino acid catabolism- Part IIAmino acid catabolism- Part II(Urea cycle with Clinical (Urea cycle with Clinical
Significance)Significance)
Biochemistry For Medics- Lecture notesProfessor(Dr.) Namrata Chhabra
www.namrata.co

Urea cycleUrea cycle• The continuous degradation and synthesis of
cellular proteins occur in all forms of life. • Each day, humans turn over 1–2% of their total
body protein, principally muscle protein.• Of the liberated amino acids, approximately 75%
are reutilized.• Since excess amino acids are not stored, those
not immediately incorporated into new protein are rapidly degraded to amphibolic intermediates.
• The excess nitrogen forms urea.
04/07/23 2Biochemistry for Medics- Lecture notes

04/07/23 3Biochemistry for Medics- Lecture notes

Urea formation (Urea cycle)Urea formation (Urea cycle)
Characteristics of urea cycle• Urea is the major disposal form of amino groups• It accounts for 90% of the nitrogen containing
components of urine• The urea cycle is the sole source of endogenous
production of arginine • Urea formation takes place in liver, • Urea excretion occurs through kidney
04/07/23 4Biochemistry for Medics- Lecture notes

Urea formation (Urea cycle)Urea formation (Urea cycle)o 6 amino acids participate in urea formation,
which are-• Ornithine• Citrulline• Aspartic acid• Argino succinic acid• Arginine and• N-Acetyl Glutamate
04/07/23 5Biochemistry for Medics- Lecture notes

Urea formationUrea formation• Synthesis of 1 mol of urea requires 3 mol of ATP • 1 mol each of ammonium ion and of the α-amino
nitrogen of aspartate. • Five enzymes catalyze the reactions of urea cycle• Of the six participating amino acids, N-acetyl
glutamate functions solely as an enzyme activator.
• The others serve as carriers of the atoms that ultimately become urea.
04/07/23 6Biochemistry for Medics- Lecture notes

Urea cycle- An overviewUrea cycle- An overview• Urea synthesis is a cyclic process. • The first two reactions of urea synthesis occur in the
matrix of the mitochondrion, the remaining reactions occur in the cytosol
• Since the Ornithine consumed in 2nd reaction is regenerated in last reaction, so there is no net loss or gain of Ornithine, Citrulline, argininosuccinate, or arginine.
• Ammonium ion, CO2, ATP, and aspartate are, however, consumed.
• Aspartate can however be resynthesized from the released fumarate by a series of reactions
04/07/23 7Biochemistry for Medics- Lecture notes

Steps of urea formationSteps of urea formationStep-1- Formation of Carbamoyl-Phosphateo Condensation of CO2, ammonia, and ATP to form
Carbamoyl phosphate is catalyzed by mitochondrial Carbamoyl phosphate synthase I (CPS-1)
o Formation of Carbamoyl phosphate requires 2 mol of ATP, one of which serves as a phosphoryl donor.
o Carbamoyl phosphate synthase I, the rate-limiting enzyme of the urea cycle, is active only in the presence of its allosteric activator N-acetyl glutamate, which enhances the affinity of the synthase for ATP.
04/07/23 8Biochemistry for Medics- Lecture notes

Step-1- Formation of Carbamoyl-Step-1- Formation of Carbamoyl-PhosphatePhosphate
• The reaction proceeds stepwise. • Reaction of bicarbonate with ATP forms carbonyl
phosphate and ADP. • Ammonia then displaces ADP, forming carbamate
and orthophosphate.• Phosphorylation of carbamate by the second ATP
then forms carbamoyl phosphate. • A cytosolic form of this enzyme, Carbamoyl
phosphate synthase II, uses glutamine rather than ammonia as the nitrogen donor and functions in pyrimidine biosynthesis.
04/07/23 9Biochemistry for Medics- Lecture notes

Step-1- Formation of Carbamoyl-Step-1- Formation of Carbamoyl-PhosphatePhosphate
• CPS1 is strongly activated by N-acetyl glutamate, which controls the overall rate of urea production.
04/07/23 10Biochemistry for Medics- Lecture notes

Step-2- Formation of CitrullineStep-2- Formation of Citrulline• The Carbamoyl group of Carbamoyl phosphate is
transferred to ornithine, forming Citrulline and Ortho Phosphate
• The reaction is catalyzed by Ornithine trans Carbamoylase
• Subsequent metabolism of Citrulline take place in the cytosol.
• Entry of ornithine into mitochondria and exit of citrulline from mitochondria involves mitochondrial inner membrane transport systems
04/07/23 11Biochemistry for Medics- Lecture notes

Step-2- Formation of CitrullineStep-2- Formation of Citrulline
This enzyme has no regulatory significance. The remainder of the urea cycle steps take place in the cytosol. This requires the continuous export of citrulline and the uptake of ornithine across the inner mitochondrial membrane.
04/07/23 12Biochemistry for Medics- Lecture notes

Step-2- Formation of CitrullineStep-2- Formation of Citrulline
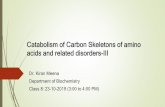
Clinical Significance• Ornithine Transcarbamoylase deficiency causes enhanced
excretion of Uracil. • Excessive excretion of Uracil or its precursor Orotic acid,
results from an accumulation of Carbamoyl phosphate in the mitochondria.
• In the absence of Ornithine Transcarbamoylase, Carbamoyl phosphate accumulates and leaks in to the cytoplasm, where it can be used to make Carbamoyl Aspartate, the first intermediate in the pathway of pyrimidine nucleotide biosynthesis.
04/07/23 13Biochemistry for Medics- Lecture notes

OTC Deficiency and Orotic aciduriaOTC Deficiency and Orotic aciduria
04/07/23 14Biochemistry for Medics- Lecture notes

Step-3- Formation of Argino succinateStep-3- Formation of Argino succinate
• Argininosuccinate synthase (ASS) links L- Aspartate and Citrulline via the amino group of aspartate and provides the second nitrogen of urea.
• The reaction requires ATP and involves intermediate formation of citrullyl-AMP. Subsequent displacement of AMP by aspartate then forms Argininosuccinate.
04/07/23 15Biochemistry for Medics- Lecture notes

Step-3- Formation of Argino succinateStep-3- Formation of Argino succinate
• Production of arginino-succinate is an energetically expensive process, since the ATP is split to AMP and pyrophosphate.
• The pyrophosphate is then cleaved to inorganic phosphate using pyrophosphatase, so the overall reaction costs two equivalents of high energy phosphate per mole.
04/07/23 16Biochemistry for Medics- Lecture notes

Step-4- Cleavage of Argino succinateStep-4- Cleavage of Argino succinate• Cleavage of argininosuccinate catalyzed by
argininosuccinate lyase (ASL), proceeds with retention of nitrogen in arginine and release of the aspartate skeleton as fumarate.
• Addition of water to fumarate forms L-malate, and subsequent NAD+-dependent oxidation of malate forms oxaloacetate.
• Transamination of oxaloacetate by glutamate aminotransferase then re-forms aspartate. carbon skeleton of aspartate-fumarate thus acts as a carrier of the nitrogen of glutamate into a precursor of urea
04/07/23 17Biochemistry for Medics- Lecture notes

Step-4- Cleavage of Argino succinateStep-4- Cleavage of Argino succinate
This reaction sequence is very similar to the conversion of IMP to AMP in the purine biosynthetic pathway. In each case fumarate is formed as a by-product. Fumarate is not transported by mitochondria, so this requires the presence of cytosolic fumarase to form malate.
04/07/23 18Biochemistry for Medics- Lecture notes

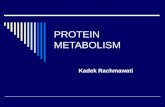
Relationship of Urea cycle and TCA Relationship of Urea cycle and TCA cyclecycle
04/07/23 19Biochemistry for Medics- Lecture notes

Step-5- Cleavage of Arginine Step-5- Cleavage of Arginine
• Hydrolytic cleavage of the guanidino group of arginine, catalyzed by liver arginase (ARG1) releases urea, the other product, Ornithine, reenters liver mitochondria for additional rounds of urea synthesis.
• Ornithine and lysine are potent inhibitors of arginase, competitive with arginine.
04/07/23 20Biochemistry for Medics- Lecture notes

Step-5-Cleavage of Arginine Step-5-Cleavage of Arginine
• Arginine also serves as the precursor of the potent muscle relaxant nitric oxide (NO) in a Ca2+-dependent reaction catalyzed by NO synthase.
04/07/23 21Biochemistry for Medics- Lecture notes

Regulation of Urea formationRegulation of Urea formation
• The activity of Carbamoyl phosphate synthase I is determined by N-acetyl glutamate, whose steady-state level is dictated by its rate of synthesis from acetyl-CoA and glutamate and its rate of hydrolysis to acetate and glutamate.
• These reactions are catalyzed by N-acetyl glutamate synthase and N-acetyl glutamate Hydrolase, respectively.
04/07/23 22Biochemistry for Medics- Lecture notes

Role of N-Acetyl GlutamateRole of N-Acetyl Glutamate
04/07/23 23Biochemistry for Medics- Lecture notes

Synthesis and Degradation of NAGSynthesis and Degradation of NAG
• N- Acetyl Glutamate Synthase catalyzes the synthesis of NAG.
• Degradation is catalyzed by NAG- Hydrolase enzyme04/07/23 24Biochemistry for Medics- Lecture notes

Regulation of Urea formationRegulation of Urea formation
• Major changes in diet can increase the concentrations of individual urea cycle enzymes 10- to 20-fold.
• Starvation, for example, elevates enzyme levels, presumably to cope with the increased production of ammonia that accompanies enhanced protein degradation
• Regulation is also achieved by linkage of mitochondrial glutamate dehydrogenase with CPS-1
04/07/23 25Biochemistry for Medics- Lecture notes

04/07/23 26Biochemistry for Medics- Lecture notes

Fate of UreaFate of Urea
• Urea formed in the liver is transported through circulation to kidneys for excretion through urine.
• It is also transported to intestine where it is decomposed by Urease produced by microbial action.
• Ammonia liberated by this activity is transported by portal circulation to liver where it is detoxified back to urea.
• A fraction of ammonia goes to systemic circulation.
04/07/23 27Biochemistry for Medics- Lecture notes

Fate of UreaFate of Urea
04/07/23 28Biochemistry for Medics- Lecture notes

Urea cycle disordersUrea cycle disordersCarbamoyl Phosphate synthetase (CPS-1) deficiency
• Along with OTC deficiency, deficiency of CPS-I is the most severe of the urea cycle disorders.
• Defects in the enzyme carbamoyl phosphate synthase I are responsible for the relatively rare (estimated frequency 1:62,000) metabolic disease termed "hyperammonemia type 1."
• Individuals with complete CPS-I deficiency rapidly develop hyperammonemia in the newborn period.
• Children who are successfully rescued from crisis are chronically at risk for repeated bouts of hyperammonemia
04/07/23 29Biochemistry for Medics- Lecture notes

Ornithine Transcarbamoylase Ornithine Transcarbamoylase deficiency (OTC deficiency)deficiency (OTC deficiency)
• The disease is characterized as X linked dominant because most females are also somewhat affected.
• A significant number of carrier females have hyperammonemia and neurologic compromise.
• The risk for hyperammonemia is particularly high in pregnancy and the postpartum period.
• The disease is much more severe in males than in females.
• The enzyme activity can range from 0% to 30% of the normal.
04/07/23 30Biochemistry for Medics- Lecture notes

Citrullinemia (ASS deficiency)Citrullinemia (ASS deficiency)
• The hyperammonemia in this disorder is quite severe.
• Affected individuals are able to incorporate some waste nitrogen into urea cycle intermediates,
• which makes treatment slightly easier.
04/07/23 31Biochemistry for Medics- Lecture notes

Argininosuccinic aciduria (ASL Argininosuccinic aciduria (ASL deficiency)deficiency)
• This disorder also presents with rapid-onset hyperammonemia in the newborn period.
• This enzyme defect is past the point in the metabolic pathway at which all the waste nitrogen has been incorporated into the cycle.
• Treatment of affected individuals often requires only supplementation of arginine.
• Affected individuals can also develop trichorrhexis nodosa, a node-like appearance of fragile hair, which usually responds to arginine supplementation.
• ASL deficiency is marked by chronic hepatic enlargement and elevation of transaminases.
04/07/23 32Biochemistry for Medics- Lecture notes

Arginase deficiencyArginase deficiency (hyperargininemia; ARG deficiency)(hyperargininemia; ARG deficiency)
• This disorder is not typically characterized by rapid-onset hyperammonemia.
• Affected individuals develop progressive spasticity and can also develop tremor, ataxia, and choreoathetosis.
• Growth is affected
04/07/23 33Biochemistry for Medics- Lecture notes

NAG Synthase deficiencyNAG Synthase deficiency
• Deficiency of this enzyme has been described in a number of affected individuals.
• Symptoms mimic those of CPSI deficiency; since CPSI is rendered inactive in the absence of NAG
• N-Acetyl glutamate is essential for Carbamoyl phosphate synthase I activity
• The NAGS gene encodes N-acetyl glutamate synthase, which catalyzes the condensation of acetyl-CoA with glutamate.
• Defects in the NAGS gene result in severe hyperammonemia, which in this specific instance may respond to administered N-acetyl glutamate.
04/07/23 34Biochemistry for Medics- Lecture notes

Ornithine Transporter deficiencyOrnithine Transporter deficiency
• Hyperornithinemia, hyperammonemia, and homocitrullinuria syndrome (HHH syndrome) results from mutation of the ORNT1 gene that encodes the mitochondrial membrane ornithine transporter.
• The failure to import cytosolic ornithine into the mitochondrial matrix renders the urea cycle inoperable, with consequent hyperammonemia, and the accompanying accumulation of cytosolic ornithine results in Hyperornithinemia.
• In the absence of its normal acceptor ornithine, mitochondrial carbamoyl phosphate carbamoylates lysine to homocitrulline with a resulting homocitrullinuria.
04/07/23 35Biochemistry for Medics- Lecture notes

Clinical manifestations in urea cycle Clinical manifestations in urea cycle disordersdisorders
• Infants with a urea cycle disorder often appear normal initially but rapidly develop-
o cerebral edema o lethargyo anorexiao hyperventilation or hypoventilation,o hypothermiao slurring of the speech, o blurring of visiono seizureso neurologic posturing and o coma.04/07/23 36Biochemistry for Medics- Lecture notes

Clinical manifestations in urea cycle Clinical manifestations in urea cycle disordersdisorders
• In milder (or partial) urea cycle enzyme deficiencies, ammonia accumulation may be triggered by illness or stress at almost any time of life, resulting in multiple mild elevations of plasma ammonia concentration; the hyperammonemia is less severe and the symptoms are more subtle.
• In individuals with partial enzyme deficiencies, the first recognized clinical episode may be delayed for months or years.
04/07/23 37Biochemistry for Medics- Lecture notes

Laboratory diagnosis of UCDLaboratory diagnosis of UCD
• The diagnosis of a urea cycle disorder(UCD) is based on evaluation of clinical, biochemical, and molecular genetic data.
• A plasma ammonia concentration of 150 mmol/L or higher is a strong indication for the presence of a UCD.
• Plasma quantitative amino acid analysis can be used to diagnose a specific urea cycle disorder
04/07/23 38Biochemistry for Medics- Lecture notes

Laboratory diagnosis of UCDLaboratory diagnosis of UCD
• Plasma concentration of Citrulline helps discriminate between the proximal and distal urea cycle defects
• as Citrulline is the product of the proximal enzymes (OTC and CPSI) and a substrate for the distal enzymes (ASS, ASL, ARG).
• Urinary Orotic acid is measured to distinguish CPSI deficiency and NAGS (N-Acetyl Glutamate Synthase) deficiency from OTC deficiency.
• The combination of family history, clinical presentation, amino acid and Orotic acid testing, and, in some cases, molecular genetic testing is often sufficient for diagnostic confirmation, eliminating the risks of liver biopsy.
04/07/23 39Biochemistry for Medics- Lecture notes

TreatmentTreatment
The mainstays of treatment for urea cycle disorders include-• Dialysis to reduce plasma ammonia concentration, • Intravenous administration of arginine chloride and nitrogen
scavenger drugs to allow alternative pathway excretion of excess nitrogen-
• Excess nitrogen is removed by intravenous phenyl acetate and that conjugate with glutamine and glycine, respectively, to form phenylacetylglutamine and Hippuric acid, water-soluble molecules efficiently excreted in urine.
• Arginine becomes an essential amino acid (except in arginase deficiency) and should be provided intravenously to resume protein synthesis.
04/07/23 40Biochemistry for Medics- Lecture notes

TreatmentTreatment• If these measures fail to reduce ammonia, hemodialysis should
be initiated promptly.• Restriction of protein for 24-48 hours to reduce the amount of
nitrogen in the diet, providing calories as carbohydrates (intravenously as glucose) and fat (intralipid or as protein-free formula) to reduce catabolism,
• Physiologic stabilization with intravenous fluids • Chronic therapy consists of a protein-restricted diet, phenyl
butyrate (a more palatable precursor of phenyl acetate), arginine, or Citrulline supplements, depending on the specific diagnosis.
• Liver transplantation should be considered in patients with severe urea cycle defects that are difficult to control medically.
04/07/23 41Biochemistry for Medics- Lecture notes

Treatment of UCDTreatment of UCD
04/07/23 42Biochemistry for Medics- Lecture notes

Genetic counselingGenetic counseling
• Deficiencies of CPSI, ASS, ASL, NAGS, and ARG are inherited in an autosomal recessive manner.
• OTC deficiency is inherited in an X-linked manner.
• Prenatal testing using molecular genetic testing is available for five of the six urea cycle disorders
04/07/23 43Biochemistry for Medics- Lecture notes

Tandem Mass Spectrometry Tandem Mass Spectrometry
• The immensely powerful and sensitive technique of tandem mass spectrometry can screen for over two dozen metabolic diseases using only drops of neonate blood.
• The early detection of UCD is of primary importance.
• Early dietary intervention, however, can in many instances ameliorate the otherwise inevitable dire effects.
04/07/23 44Biochemistry for Medics- Lecture notes

Differential diagnosis of UCDDifferential diagnosis of UCD
• A number of other disorders that perturb the liver can result in hyperammonemia and mimic the effects of a urea cycle disorder.
• The most common/significant ones are viral infection of the liver and vascular bypass of the liver.
04/07/23 45Biochemistry for Medics- Lecture notes

Gene Therapy Gene Therapy
• Gene therapy for rectification of defects in the enzymes of the urea cycle is an area of active investigation.
• Encouraging preliminary results have been obtained, for example, in animal models using an adenoviral vector to treat citrullinemia.
04/07/23 46Biochemistry for Medics- Lecture notes

Variations in blood urea levelsVariations in blood urea levels
• Normal blood urea level ranges between 15-40 mg/dl.
• High blood urea level (uraemia)may be observed in-
o Pre renalo Renal ando Post renal conditions
04/07/23 47Biochemistry for Medics- Lecture notes

Variations in blood urea levelVariations in blood urea level
• Pre renal conditionso Salt and water depletiono Severe vomiting as in pyloric stenosis or intestinal
obstructiono Severe and prolonged diarrheao Addison’s diseaseo Ulcerative colitiso Haemorrhage and shock
04/07/23 48Biochemistry for Medics- Lecture notes

Variations in blood urea levelVariations in blood urea level
• Renal conditionso Acute glomerulonephritiso Renal failureo Nephrosclerosiso Renal tuberculosiso Mercurial poisoningo Chronic Pyelonephritiso Hydronephrosis
04/07/23 49Biochemistry for Medics- Lecture notes

Variations in blood urea levelVariations in blood urea level
• Post Renal conditions- There is obstruction to the outflow of urine. Retention of urine reduces effective filtration pressure at glomeruli. The important causes are-
o Enlarged prostateo Stones in urinary tracto Urethral strictures which may be congenital or
surgicalo Bladder tumors
04/07/23 50Biochemistry for Medics- Lecture notes

Variations in blood urea levelVariations in blood urea level
• Physiological conditions of high blood urea level
o Advancing ageo Starvation- Proteins are catabolized. The carbon
skeleton of amino acids is used for glucose, ketone bodies or energy production, whereas the amino group of amino acids is removed as ammonia which is later detoxified as urea.
04/07/23 51Biochemistry for Medics- Lecture notes

Variations in blood urea levelVariations in blood urea level
• Low blood urea level- is observed in following conditions
o Liver diseaseso Urea cycle disorderso Physiologically – in pregnancy and growing
stage
04/07/23 52Biochemistry for Medics- Lecture notes

04/07/23 53Biochemistry for Medics- Lecture notes