Prognostic factors and staging systems in parathyroid cancer: A multicenter cohort study
13
Prognostic factors and staging systems in parathyroid cancer: A multicenter cohort study Jes us Villar-del-Moral, PhD, MD, a Antonio Jim enez-Garc ıa, PhD, MD, b Pilar Salvador-Egea, PhD, MD, c Juan M. Martos-Mart ınez, MD, d Jos e M. Nu~ no-V azquez-Garza, MD, e Mario Serradilla-Mart ın, MD, f Angel G omez-Palacios, PhD, MD, g Pablo Moreno-Llorente, PhD, MD, h Joaqu ın Ortega-Serrano, PhD, MD, i and Aitor de la Quintana-Basarrate, MD, j Granada, Sevilla, Pamplona, Vigo, Jaen, Bilbao, Barcelona, Valencia, and Baracaldo, Spain Background. Parathyroid carcinoma (PC) is an uncommon disease that generally is detected postoperatively and traditionally is associated with a poor prognosis. Our purpose was to evaluate treatment outcomes, prognostic factors, and usefulness of some proposed staging systems for this disease. Methods. A multicenter review of patients with surgically resected PC was performed, led by the Spanish Association of Surgery. All surgical units affiliated with its endocrine surgery section were invited to answer a questionnaire that collected several hospital-related, clinical, biochemical, operative, pathologic, and follow-up data. Their relationships with prognosis were assessed by both univariate and multivariate analysis, as well as the effectiveness of three staging systems for parathyroid carcinoma. Result. Of the 6,863 patients undergoing parathyroidectomy, 62 (0.9%) had PC. Of them, 12 (19.3%) died, in 5 cases (8%) because of disease, and 14 (22.6%) suffered recurrence, after a median follow-up of 55 months. The most predictive independent variables on tumor recurrence were intraoperative tumor rupture (hazard ratio [HR] 6.22; 95% confidence interval [CI] 1.19–32.36; P = .030); the presence of mitotic figures within tumor parenchyma cells (HR 4.76; 95% CI 1.24–18.21; P = .022); and allo- cation in class III according to Schulte differentiated staging classification (HR 5.23; 95% CI 1.41–19.31; P = .013). As to disease-specific survival, poor outcomes were associated with intraoper- ative tumor rupture (HR 58.71; 95% CI 2.39–1,439.96; P = .013) and distant recurrence (HR 38.74; 95% CI 3.44–435.62; P = .003). Conclusion. In addition to factors associated with tumor histopathology and stage, prognosis of PC is greatly influenced by surgeon’s performance, which emphasizes the importance of preoperative diagnosis. (Surgery 2014;156:1132-44.) From the Endocrine Surgery Unit, Department of Surgery, a Virgen de las Nieves University Hospital, Granada; Endocrine Surgery Unit, Department of Surgery, b Virgen Macarena University Hospital, Sevilla; Endocrine Surgery Unit, Department of Surgery, c Complejo Hospitalario de Navarra, Pamplona; Endocrine Surgery Unit, Department of Surgery, d Virgen del Rocio University Hospital, Sevilla; Endocrine Surgery Unit, Department of Surgery, e Meixoeiro Hospital, Vigo; Department of Surgery, f Complejo Hospitalario de Jaen, Jaen; Endocrine Surgery Unit, Department of Surgery, g Basurto University Hospital, Bilbao; Endocrine Surgery Unit, Department of Surgery, h Bellvitge University Hospital, Barcelona; Endocrine Surgery Unit, Department of Surgery, i Clinic University Hospital, Valencia; and Endocrine Surgery Unit, Department of Surgery, j Cruces University Hospital, Baracaldo, Spain PARATHYROID CARCINOMA (PC) is an uncommon cause of primary hyperparathyroidism, accounting for less than 1% of cases. 1 According to the American National Surveillance, Epidemiology and End Results (SEER), the incidence of PC is 0.4–0.6 per million population per year. 2 Therefore, indi- vidual series are of limited value because of the small number of cases. Indeed, not a single center has ever reported data on more than 50 patients, 3 and the literature available is almost exclusively of retrospective nature. A preoperative diagnosis of PC is difficult, and most patients are operated for presumed benign adenoma. Distinguishing benign from ma- lignant parathyroid tissue during operative resec- tion also is hard: in SEER data, most parathyroid cancers (78.6%) were resected by simple Accepted for publication May 7, 2014. Reprint requests: Jes us Villar-del-Moral, PhD, MD, c/Hoya de la Mora, 9, 28 A. 18008 Granada, Spain. E-mail: jevillarmo@ yahoo.es. 0039-6060/$ - see front matter Ó 2014 Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.surg.2014.05.014 1132 SURGERY
Transcript of Prognostic factors and staging systems in parathyroid cancer: A multicenter cohort study
Accepte
Reprintla Morayahoo.e
0039-60
� 2014
http://d
1132
Prognostic factors and staging systemsin parathyroid cancer: A multicentercohort studyJes�us Villar-del-Moral, PhD, MD,a Antonio Jim�enez-Garc�ıa, PhD, MD,b
Pilar Salvador-Egea, PhD, MD,c Juan M. Martos-Mart�ınez, MD,d Jos�e M. Nu~no-V�azquez-Garza, MD,e
Mario Serradilla-Mart�ın, MD,f Angel G�omez-Palacios, PhD, MD,g Pablo Moreno-Llorente, PhD, MD,h
Joaqu�ın Ortega-Serrano, PhD, MD,i and Aitor de la Quintana-Basarrate, MD,j Granada, Sevilla,Pamplona, Vigo, Jaen, Bilbao, Barcelona, Valencia, and Baracaldo, Spain
Background. Parathyroid carcinoma (PC) is an uncommon disease that generally is detectedpostoperatively and traditionally is associated with a poor prognosis. Our purpose was to evaluatetreatment outcomes, prognostic factors, and usefulness of some proposed staging systems for this disease.Methods. A multicenter review of patients with surgically resected PC was performed, led by the SpanishAssociation of Surgery. All surgical units affiliated with its endocrine surgery section were invited toanswer a questionnaire that collected several hospital-related, clinical, biochemical, operative, pathologic,and follow-up data. Their relationships with prognosis were assessed by both univariate andmultivariate analysis, as well as the effectiveness of three staging systems for parathyroid carcinoma.Result. Of the 6,863 patients undergoing parathyroidectomy, 62 (0.9%) had PC. Of them, 12 (19.3%)died, in 5 cases (8%) because of disease, and 14 (22.6%) suffered recurrence, after a median follow-upof 55 months. The most predictive independent variables on tumor recurrence were intraoperative tumorrupture (hazard ratio [HR] 6.22; 95% confidence interval [CI] 1.19–32.36; P = .030); the presence ofmitotic figures within tumor parenchyma cells (HR 4.76; 95% CI 1.24–18.21; P = .022); and allo-cation in class III according to Schulte differentiated staging classification (HR 5.23; 95% CI1.41–19.31; P = .013). As to disease-specific survival, poor outcomes were associated with intraoper-ative tumor rupture (HR 58.71; 95% CI 2.39–1,439.96; P = .013) and distant recurrence (HR38.74; 95% CI 3.44–435.62; P = .003).Conclusion. In addition to factors associated with tumor histopathology and stage, prognosis of PC isgreatly influenced by surgeon’s performance, which emphasizes the importance of preoperative diagnosis.(Surgery 2014;156:1132-44.)
From the Endocrine Surgery Unit, Department of Surgery,a Virgen de las Nieves University Hospital,Granada; Endocrine Surgery Unit, Department of Surgery,b Virgen Macarena University Hospital, Sevilla;Endocrine Surgery Unit, Department of Surgery,c Complejo Hospitalario de Navarra, Pamplona; EndocrineSurgery Unit, Department of Surgery,d Virgen del Rocio University Hospital, Sevilla; Endocrine Surgery Unit,Department of Surgery,e Meixoeiro Hospital, Vigo; Department of Surgery,f Complejo Hospitalario de Jaen,Jaen; Endocrine Surgery Unit, Department of Surgery,g Basurto University Hospital, Bilbao; EndocrineSurgery Unit, Department of Surgery,h Bellvitge University Hospital, Barcelona; Endocrine Surgery Unit,Department of Surgery,i Clinic University Hospital, Valencia; and Endocrine Surgery Unit, Department ofSurgery,j Cruces University Hospital, Baracaldo, Spain
PARATHYROID CARCINOMA (PC) is an uncommon causeof primary hyperparathyroidism, accounting forless than 1% of cases.1 According to the AmericanNational Surveillance, Epidemiology and End
d for publication May 7, 2014.
requests: Jes�us Villar-del-Moral, PhD, MD, c/Hoya de, 9, 28 A. 18008 Granada, Spain. E-mail: jevillarmo@s.
60/$ - see front matter
Elsevier Inc. All rights reserved.
x.doi.org/10.1016/j.surg.2014.05.014
SURGERY
Results (SEER), the incidence of PC is 0.4–0.6per million population per year.2 Therefore, indi-vidual series are of limited value because of thesmall number of cases. Indeed, not a single centerhas ever reported data on more than 50 patients,3
and the literature available is almost exclusively ofretrospective nature.
A preoperative diagnosis of PC is difficult,and most patients are operated for presumedbenign adenoma. Distinguishing benign from ma-lignant parathyroid tissue during operative resec-tion also is hard: in SEER data, most parathyroidcancers (78.6%) were resected by simple

SurgeryVolume 156, Number 5
Villar-del-Moral et al 1133
parathyroidectomy.1,2 Incomplete excisions resultin very high recurrence rates, but there is noconsensus on the optimal extent of surgery.However, current recommendations are en-blocresection that includes involved neighboring struc-tures, thus avoiding tumor rupture and spillage.4
Five-year survival rates for case series and registrydata of the past two decades are consistent at76–85%, and 10-year survival rates range from49 to 77%.5,6
In contrast, the prognostic factors for thisneoplasm have not been clearly defined nor astandard clinical or pathologic staging system. Inthe American National Cancer Database report,which was based on a sample of 286 cases of PC,investigators found that tumor size or lymph nodestatus did not have any prognostic value.7 Recentstudies from King’s College Hospital in Londonhave highlighted the relevance of some histopath-ologic criteria like vascular invasion on prog-nosis.3,8 In fact, two staging systems based onhistopathologic criteria have been designed, tobe added to the scheme previously described byShaha and Shah in 1999. The latter was developedbased on the tumor, node, metastasis (TNM) clas-sification system of the Union for InternationalCancer Control.9
To obtain further insights into this disease, theSpanish Parathyroid Carcinoma Study Group(SPCSG) was established in January 2012 as amulti-institutional registry that collects, analyzes,and reviews all the information on PC available inSpain. Data were obtained by sending a question-naire to several Spanish institutions affiliated tothe Endocrine Surgery Section (ESS) of the Span-ish Association of Surgery. The purpose of thisarticle is to analyze the data obtained from thiscohort of PC patients to determine treatmentoutcomes and prognostic factors with impact onsurvival, as well as to evaluate the usefulness of theproposed staging systems for this disease.
METHODS
Study design. This is a cohort study based on amulti-institutional review of patients surgicallytreated for PC and followed-up along the time,carried out by the ESS. This is the first study to usethe SGSPC database. The manuscript has beenstructured according to the STROBE (eg,Strengthening the Reporting of ObservationalStudies in Epidemiology) checklist for observa-tional studies.10
Setting. In January 2012, the SPCSG designed adatabase to collect and analyze relevant informa-tion on patients with PC. In February 2012, a
questionnaire with several variables was sent to 54ESS-affiliated Spanish institutions having an Endo-crine Surgery Unit. Before participating in thestudy, the units were requested to obtain previousapproval from the review board of their institution,39 of which (72.2%) were university hospitals.
Questionnaires were collected until January 31,2013. The 35 centers (64.8%) that responded tothe questionnaire attended a total population of13,100,000 inhabitants (27.5% of the country’spopulation).11 The surgeons of these units re-viewed a total of 6,863 parathyroidectomy reportsrecorded in prospectively collected databases andentered data about patients with PC into theSGSPC database. The median number of yearsthat patients were included in these records was14 (25th and 75th percentile range 10–18), withthe oldest dataset dating back to 1980. Ten hospi-tals (28.5%) had no records on surgery performedon patient with PC, whereas 25 centers providedinformation on 70 patients diagnosed with PC.Follow-up was updated until April 30, 2013.
Participants. Inclusion criteria for eligible pa-tients included the following:
1. Unambiguous histopathologic diagnosis of a primary
nonrecurrent PC established by an expert pathologist
and based on the 2004 World Health Organization
criteria. The minimal criteria for defining PC were
infiltrative growth (capsular and soft-tissue invasion).
Major diagnostic criteria were histologic proof of
vascular invasion, invasion of vital organs (trachea,
esophagus, major vessel), or the presence of locore-
gional or distant metastases.12
2. Availability of a complete dataset and pathology
report with known margin status, during the inclu-
sion period.
3. Patient follow-up period of at least 6 months.
The majority of institutions scheduled targetedfollow-up exams at 6-month intervals. Follow-upwas updated by the attending surgeon in everyinstitution and was recorded based on patient lastvisit to outpatient clinic, death, or loss to follow-up.
Variables. Data collected in the questionnairewere entered into a database created by EESmembers. Source data and a copy of the originalpathology report were sent to an independentreviewer (M.S.M.), who was an expert parathyroidsurgeon from a unit that had not contributed anycase to the study. The reviewer confirmed patienteligibility of patients or excluded them if they didnot meet all the inclusion criteria.
We focused on the potential impact of a set ofvariables on prognosis, such as surgical volume ofthe institution, demographics (age, sex, history of

Table I. Proposed staging systems for patients with parathyroid carcinoma
Shaha and Shah classification9 Differentiated Schulte classification8 Risk Schulte classification8
T Tx No information available Low risk Capsular invasioncombined with invasionof surrounding softtissue
T1 Primary tumor <3 cm T1 Evidence of capsularinvasion
T2 Primary tumor >3 cm T2 Invasion of surroundingsoft tissues excludingthe vital organs oftrachea, larynx, andesophagus
T3 Primary tumor of any sizewith invasion of thesurrounding softtissues, such as thethyroid gland, strapmuscles, etc
T3 Evidence of vascularinvasion
T4 Massive centralcompartment diseaseinvading the tracheaand esophagus orrecurrent parathyroidcarcinoma
T4 Invasion of vital organs—hypopharynx, trachea,esophagus, larynx,recurrent laryngealnerve, carotid artery
N Nx Lymph node not assessed High risk Vascular invasion and/orlymph node metastasesand/or invasion of vitalorgans and/or distantmetastases
N0 No regional lymph nodemetastases
N0 No regional lymph nodemetastases
N1 Regional lymph nodemetastases
N1 Regional lymph nodemetastases
M Mx Distant metastases notassessed
M0 No evidence of distantmetastases
M0 No evidence of distantmetastases
M1 Evidence of distantmetastases
M1 Evidence of distantmetastases
Stage I T1N0M0 I T1 or T2 N0M0II T2N0M0 II T3 N0 M0IIIA T3N0M0 III Any T, N1 M0, or T4IIIB T4N0M0IIIC Any T, N1M0IV Any T, Any N, M1 IV Any N, M1
SurgeryNovember 2014
1134 Villar-del-Moral et al
previous neoplasia), symptoms and signs,biochemistry (corrected calcium, expressed inmg/dL, and parathyroid hormone [PTH], ex-pressed in pg/mL), preoperative localizationstudies, and diagnosis (suspicion or not of PC).Intraoperative variables considered for statisticalanalysis were type of resection (parathyroidectomyalone or en-bloc resection with macroscopicallyinvolved neighboring structures), margin status(macroscopic involvement, microscopic invasion,or free margins), and occurrence of intraoperativetumor rupture. Other operative factors analyzedwere the type of lymph node clearance performed(formal central compartment dissection, nodalsampling or not done) and the rate of descent of
preoperative PTH levels 10 minutes after the endof resection.
Some pathologic features also were evaluated,including tumor size and presence or absence offibrous bands, mitotic figures within parenchymacells, capsular invasion, vascular invasion, spread tosurrounding tissues, and nodal invasion. Evalua-tion of the presence of distant metastases also wasincluded to stage the tumor according to the threeproposed systems (Table I). Postoperative andfollow-up variables included operative morbidity,tumor recurrence (presence of locoregional and/or distant recurrence), treatment for recurrence(if any), death (due to PC), and duration offollow-up in months.

Table II. Overview of hospital-related, clinical,biochemical, and operative findings
Factor Value (%)
Patients withavailable
information
Hospital volume 62High 30 (48.3)Low 32 (51.7)
Age, y 62Median 5925th and 75th percentile
range51–70
Sex 62Male 38 (61.3)Female 24 (38.7)
Clinical profile 62Fatigue 38 (61.3)Nephrolithiasis 35 (56.4)Bone pain or fractures 32 (51.6)Renal dysfunction 29 (46.7)Neck mass 21 (33.8)Osteopenia/osteoporosis 20 (32.2)Hypercalcemic crisis 17 (27.4)Arterial hypertension 13 (21.0)Previous malignant neoplasia 9 (14.5)
Calcium, mg/dL 62Median 13.025th and 75th percentile
range11.6–14.6
PTH, pg/mL 60Median 50725th and 75th percentile
range225–934
Preoperative diagnosis 62PHPT, no suspicion of PC 48 (77.4)SHPT, no suspicion of PC 4 (6.5)Suspicion of PC 10 (16.1)
Type of resection 62Parathyroidectomy alone 18 (29.0)En-bloc resection 44 (71.0)
Intraoperative tumor rupture 62No 59 (95.2)Yes 3 (4.8)
Type of lymph node clearanceperformed
62
Not done 42 (67.7)Node sampling 5 (8.0)Central compartment
dissection15 (24.1)
Percentage of descent ofpreoperative PTH levels*
17
Median 89.025th and 75th percentile
range85.0–90.0
*Ten minutes after the end of resection.PC, Parathyroid carcinoma; PHPT, primary hyperparathyroidism; PTC,parathyroid carcinoma; PTH, parathyroid hormone; SHPT, secondaryhyperparathyroidism.
SurgeryVolume 156, Number 5
Villar-del-Moral et al 1135
The primary end point was death due to disease.Disease-specific survival (DSS) was defined as timefrom the operation to death due to PC. Thesecondary end point was tumor relapse.Recurrence-free survival (RFS) was defined as thetime elapsed until locally or distantly recurringdisease was identified during follow-up.
Bias. To avoid selection bias, only those patientswho had been prospectively included by eachparticipating institution in a systematic databaseof parathyroid surgery were included. To increasedata reliability, all source data were checked by anindependent reviewer. Cases that were ambiguousin the original pathologic report were excluded.To reduce confounding variables, we did notconsider patients who died of other causes thanPC in the survival study.
Quantitative variables. Quantitative variablesare described by median and by 25–75th percentilerange. Regarding institutions, high-volume centerswere defined as those where more than 25 para-thyroidectomies were performed per year. This wasone of the requirements for institutions to beconsidered as a referral center in the ‘‘Certificationsystem for thyroid and parathyroid surgery Units’’of the German Society of General and DigestiveSurgery.13 This requirement has been establishedas a suitable grouping criterion by the SPCSG.The remaining quantitative variables were consid-ered a continuum for statistical analysis.
Statistical methods. Survival analysis was per-formed according to the Kaplan-Meier method.14
Patients who were alive at the time of analysisand patients who died of causes unrelated to PCwere censored for DSS analysis. The Cox propor-tional hazards model was used for multivariate sur-vival analysis to validate statistically significantvariables in univariate analysis, by calculating thehazard ratio and the 95% confidence interval.15
The log rank (Mantel-Cox) test was used to analyzeand compare the effectiveness of some proposedstaging systems in our cohort.16
When data were missing, we have indicated theexact number of patients on whom information wasavailable and who were included in the calculation(Tables II and III). Patients lost to follow-up weretreated as if they had withdrawn alive from the studyat the date of loss. Data were analyzed with SPSS20.0 software (SPSS, Chicago, IL).
RESULTS
Participants. From a total of 6,863 patientsundergoing parathyroidectomy, we received com-plete questionnaires from 70 cases diagnosed with

Table III. Pathologic and follow-up features in thecohort of patients with PC
FactorValue
(percentage)
Patients withavailable
information
Margin status 62Free margins 55 (88.7)Macroscopic ormicroscopic invasion
7 (11.3)
Tumor size, mm 62Median 28.025th and 75th percentilerange
20.0–38.0
Pathologic featuresFibrous bands 33 (53.2) 62Mitotic figures in tumorparenchyma cells
32 (51.6) 62
Capsular invasion 56 (90.3) 62Vascular invasion 42 (67.7) 62Invasion of surroundingtissues
31 (50.0) 62
Nodal invasion 8 (40.0) 20Stage according Shaha and
Shah classification962
I 22 (35.5)II 16 (25.8)III 23 (37.1)IV 1 (1.6)
Stage according Schultedifferentiatedclassification8
62
I 17 (27.4)II 35 (56.5)III 9 (14.5)IV 1 (1.6)
Stage according Schulte riskclassification8
62
Low risk 16 (25.8)High risk 46 (74.2)
Follow-up, mo 62Median 52.025th and 75th percentilerange
16.0–97.0
Recurrence 62Locoregional 13 (20.1)Distant 3 (4.8)All 14 (22.6)
Death 62Due to PC 5 (8.1)Unrelated to PC 7 (11.3)All 12 (19.4)
PC, Parathyroid carcinoma.
SurgeryNovember 2014
1136 Villar-del-Moral et al
PC (potentially eligible patients). Two were notassessed for eligibility because their questionnaireswere sent after the submission deadline. After anextensive review of pathology reports, of the 68eligible cases, six did not fulfill all World Health
Organization 2004 criteria for PC. Finally, 62patients having completed a minimum follow-upperiod of 6 months were included in the study foranalysis.
Descriptive data. Tables II and III include adescription of the relevant characteristics testedfor impact on prognosis, together with the numberof patients on whom data for each variable wereavailable. Four PCs (6.5%) occurred in patientswith genetic predisposition: one had hyper-parathyroidism-jaw tumor syndrome, another casehad familial isolated hyperparathyroidism, anotherpatient suffered from multiple endocrineneoplasia 1 syndrome, and the last case had multi-ple endocrine neoplasia 2A syndrome. Another pa-tient had a history of previous neck irradiationduring childhood. Parathyroid glands mostfrequently involved were right inferior (41.2%),left inferior (25.1%), right superior (17.6%), andleft superior (16.1%). One of the five casesdeveloped from secondary hyperparathyroidismappeared in the form of multifocal PC affectingtwo glands.
Regarding preoperative localization studies, themost widely used was ultrasound (90.3% of pa-tients), followed by scintigraphy with sestamibi(69.4%) and computed tomography (30.6%).The use of nuclear magnetic resonance andpositron emission tomography scan was anecdotic.The most sensitive technique for the detection ofpathologic glands was scintigraphy (95.3% ofsensitivity) followed by ultrasound (69.6%) andcomputed tomography (68.4%). Nevertheless, themost sensitive technique for the detection ofpossible signs of malignancy was computed tomog-raphy (21%), followed by ultrasound (19%) andsestamibi scan (4.7%).
‘‘En-bloc’’ resection included the thyroid glandin 44 cases (71.0%): partial lobectomy in threecases (4.8%), total lobectomy in 36 patients(58%), and total thyroidectomy in five cases(8%). Other resected structures included strapmuscles in six patients (9.7%), recurrent laryn-geal nerve in four cases (6.5%), and superficialmuscular layer of esophagus in one patient(1.6%). The median operative time was 90 mi-nutes (interquartile range, 65–150). The medianhospital stay was 4 days (interquartile range, 3–7).There were postoperative complications in 28patients (45.2%): 21 (33.9%) had transient hypo-parathyroidism and 13 (25%) had unilateral vocalcord palsy that was permanent in eight cases(13%); half of them had presented preoperativepalsy. No patients developed bilateral vocal cordpalsy or died within 30 days after surgery. Only

SurgeryVolume 156, Number 5
Villar-del-Moral et al 1137
one patient underwent primary tumor excision inthe presence of synchronic resectable bonemetastasis.
Outcome data. During the 364.1 person-years offollow-up (median 54 months, interquartile range,18–97), three patients were lost at 26, 40, and50 months, respectively, without evidence ofrelapse. Recurrent disease was documented in 14patients (22.6%). Locoregional recurrence wasfound in 13 cases, with neck involvement in 10cases and mediastinal nodal invasion in threepatients. Distant disease (metachronic bone me-tastases) was detected in three cases. In patientswith disease relapse, the median time to firstrecurrence was 17 months (25th and 75th percen-tile range 10–44): 14 months for locoregionalrecurrence and 11 months for distant metastases.Interestingly, no patient had first recurrence after5 years of follow-up.
The treatment for recurrent disease includedsurgery for locoregional relapse in 9 of 13 cases(69.2%) and radiotherapy in two patients (15.3%).The median number of reoperations per patientwas 1.9 (range, 1–5). Regarding the only fourpatients with recurrent disease and whose PTHlevels were reported, a close relationship wasobserved between PTH levels and structuralrecurrence. All four patients underwent re-operation, with reported preoperative PTH levelsof 410 pg/mL, 462 pg/mL, 934 pg/mL and1.707 pg/mL, respectively.
Five patients (55.5%) undergoing redo surgerywere disease-free at the end of follow-up. Cinacal-cet and/or bisphosphonates were used in sevenpatients (50%), and chemotherapy with Adria-mycin was administered to one patient. Treatmentsoften were used in combination. Two patients withrecurrent disease received no specific treatment.
Five patients died from PC, whereas sevenpassed away due to other causes. Forty-four pa-tients were free of recurrence at the time of lastfollow-up, whereas three were survived with diseaserelapse. Figure 1 presents overall disease-specificand recurrence-free survival in two Kaplan-Meiertables. Five and ten-year disease-specific survivaland recurrence-free survival were 92.2%, 69.1%,91.1%, and 69.1%, respectively.
Main results. Table IV presents univariate Coxanalysis for tumor recurrence and death due todisease for selected variables. Regarding deathrelated to PC, margin invasion, intraoperative tu-mor rupture, nodal invasion, and locoregionaland distant relapse were found to have prognosticimpact and were included in multivariate analysis.With respect to tumor recurrence, relevant factors
were margin invasion, tumor rupture during sur-gery, degree of intraoperative decrease of PTH,presence of mitotic figures within the tumor pa-renchyma cells, nodal invasion, and advancedstages in Shaha and differentiated Schultesystems.
Neither a history of malignancy nor any clinicalvariable were found to have prognostic influence.Related to the rate of PTH compared with preop-erative levels, the two shortest descents (3% and21%) were associated with nodal invasion, earlylocoregional recurrence, metastases, and death.
Table V shows the variables that emerge as pre-dictive factors for tumor relapse and death due todisease, which were identified using Cox’s regres-sion multivariate analysis, with a substantial in-crease in the risk of recurrence for patients withintraoperative tumor rupture, presence of mitoticfigures in tumor cells, and Stage III in the Schultedifferentiated classification. Disease-specific deathwas related to intraoperative tumor rupture anddistant relapse.
The power of the proposed PC staging systemsto predict outcomes was assessed with the log-ranktest. For DSS (Fig 2), the Shaha and Shah stagingsystem (P = .013), and the Schulte differentiatedsystem (P = .008) but not with the risk patternSchulte system (P = .128) showed meaningful dif-ferences regarding survival between stages. Incontrast, RFS (Fig 3) was best predicted using thestages of Schulte differentiated system (P = .008)and Schulte risk staging (P = .050), comparedwith the Shaha classification system (P = .285).
DISCUSSION
In a disease with an incidence as low as PC,individual series have little value for analysis ofprognostic factors.17-19 Accordingly, the SPCSG de-signed this multi-institutional study, whose mainobjectives were the detection of clinicopathologicfactors with an impact on relapse and survival,and assessment of the usefulness of different stag-ing systems. The first factor that predicts recur-rence was the occurrence of intraoperative tumorrupture. The second factor with the greatest pre-dictive value was the existence of a locally advancedtumor framed in stage III according to differenti-ated Schulte classification and characterized inour series by recurrent nerve or esophageal wall in-vasion and/or presence of lymph node metastases.The last factor was the presence of mitotic figuresin tumor parenchyma cells.
Disease-specific death was related with intra-operative tumor rupture and distant diseaserelapse (not local, because it is safely treated with

Fig 1. Kaplan-Meier’s disease-specific (left) and recurrence-free (right) survival analyses for the cohort of patients withparathyroid carcinoma.
SurgeryNovember 2014
1138 Villar-del-Moral et al
redo surgery in selected cases). Unlike most recentclassifications based on the histopathologic criteriaproposed by Talat and Schulte,3,8 the TNM Shahaand Shah staging system9 was unable to predict dis-ease relapse in our cohort. Conversely, Shaha andShah and differentiated Schulte schemes were pre-dictive of disease-related death.
PCs generally have an indolent, slow, progres-sive course; therefore, patient follow-up is critical,and it is recommended to be performed at 4- to6-month intervals. Local relapse affects regionallymph nodes or surgical site, whereas distantmetastases usually involve lungs and bones.1 Therate of recurrent disease after surgery rangesbetween 33% and 63%.2,3,7,8,17,20 Despite recur-rence, prolonged survival is possible. The firstlarge multi-institutional PC cohort study20 re-ported a 10-year survival rate of 70%, whereasthis percentage was 49% in the American NationalCancer Database Survey.7 The SEER report esti-mates a 10-year overall survival rate of 66%,whereas the 10-year disease-specific survival raterose to 87%.2 Talat and Schulte, in a systematic re-view that included 330 cases, found an overallrecurrence of 63% with a mortality rate of 35%.Our results compare positively with these out-comes, with a 10-year DSS of 91% and 10-yearRFS of 69%. No patient had first recurrencebeyond 5 years after surgery, which may have prac-tical implications for the follow-up of these pa-tients. Some of the proposed factors affectingprognosis are discussed more extensively in theparagraphs to follow.
Hospital volume and expertise were solely testedby Harari et al,19 who performed a single-center
cohort study with 37 PC cases. In this cohort, thefirst operation in an academic endocrine surgeryreferral center was found to have a positive prog-nostic impact. In our study, no differences wereobserved regarding long-term outcomes betweensurgical units of high-and low-volume centers. Thismay be due to the fact that even low-volume centershad experienced endocrine surgery units devotedto parathyroid diseases.
There is contradictory evidence about the rela-tionship between age and PC-related mortality. Leeet al2 observed greater rates of mortality in olderpatients. On the other hand, Talat and Schulte3
reported greater rates of recurrence amongyounger patients, although age was not found tohave any impact on mortality. Similarly, there isno consensus on the impact of sex. Some reportshave observed an association between male sexand worse prognosis in terms of death2,3 and recur-rence.3 However, neither age nor sex have beenfound to have any prognostic impact in our cohort.This could be conditioned by the small number ofpatients who relapsed or died due to PC.
Regarding preoperative biochemical markers,Talat and Schulte3 observed that calcium but notPTH levels predict overall recurrence and mortal-ity. Our results do not confirm that these markershave any prognostic value.
Although the prognostic impact of preoperativesuspicion of PC has not been discussed previously,it could affects long-term outcomes and be usefulin determining the extent of operation. In ourcohort, with a low percentage of preoperativelysuspected cancer (16%), this variable did notinfluence long-term outcomes. Suspicion signs
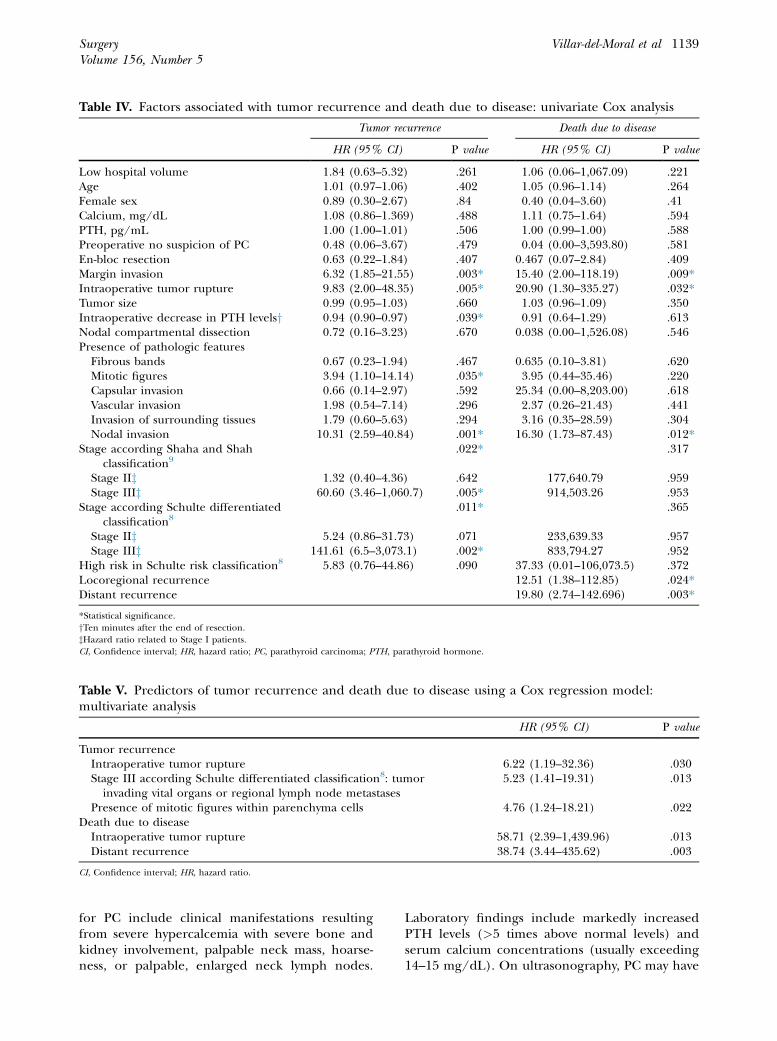
Table IV. Factors associated with tumor recurrence and death due to disease: univariate Cox analysis
Tumor recurrence Death due to disease
HR (95% CI) P value HR (95% CI) P value
Low hospital volume 1.84 (0.63–5.32) .261 1.06 (0.06–1,067.09) .221Age 1.01 (0.97–1.06) .402 1.05 (0.96–1.14) .264Female sex 0.89 (0.30–2.67) .84 0.40 (0.04–3.60) .41Calcium, mg/dL 1.08 (0.86–1.369) .488 1.11 (0.75–1.64) .594PTH, pg/mL 1.00 (1.00–1.01) .506 1.00 (0.99–1.00) .588Preoperative no suspicion of PC 0.48 (0.06–3.67) .479 0.04 (0.00–3,593.80) .581En-bloc resection 0.63 (0.22–1.84) .407 0.467 (0.07–2.84) .409Margin invasion 6.32 (1.85–21.55) .003* 15.40 (2.00–118.19) .009*Intraoperative tumor rupture 9.83 (2.00–48.35) .005* 20.90 (1.30–335.27) .032*Tumor size 0.99 (0.95–1.03) .660 1.03 (0.96–1.09) .350Intraoperative decrease in PTH levelsy 0.94 (0.90–0.97) .039* 0.91 (0.64–1.29) .613Nodal compartmental dissection 0.72 (0.16–3.23) .670 0.038 (0.00–1,526.08) .546Presence of pathologic features
Fibrous bands 0.67 (0.23–1.94) .467 0.635 (0.10–3.81) .620Mitotic figures 3.94 (1.10–14.14) .035* 3.95 (0.44–35.46) .220Capsular invasion 0.66 (0.14–2.97) .592 25.34 (0.00–8,203.00) .618Vascular invasion 1.98 (0.54–7.14) .296 2.37 (0.26–21.43) .441Invasion of surrounding tissues 1.79 (0.60–5.63) .294 3.16 (0.35–28.59) .304Nodal invasion 10.31 (2.59–40.84) .001* 16.30 (1.73–87.43) .012*
Stage according Shaha and Shahclassification9
.022* .317
Stage IIz 1.32 (0.40–4.36) .642 177,640.79 .959Stage IIIz 60.60 (3.46–1,060.7) .005* 914,503.26 .953
Stage according Schulte differentiatedclassification8
.011* .365
Stage IIz 5.24 (0.86–31.73) .071 233,639.33 .957Stage IIIz 141.61 (6.5–3,073.1) .002* 833,794.27 .952
High risk in Schulte risk classification8 5.83 (0.76–44.86) .090 37.33 (0.01–106,073.5) .372Locoregional recurrence 12.51 (1.38–112.85) .024*Distant recurrence 19.80 (2.74–142.696) .003*
*Statistical significance.yTen minutes after the end of resection.zHazard ratio related to Stage I patients.CI, Confidence interval; HR, hazard ratio; PC, parathyroid carcinoma; PTH, parathyroid hormone.
Table V. Predictors of tumor recurrence and death due to disease using a Cox regression model:multivariate analysis
HR (95% CI) P value
Tumor recurrenceIntraoperative tumor rupture 6.22 (1.19–32.36) .030Stage III according Schulte differentiated classification8: tumorinvading vital organs or regional lymph node metastases
5.23 (1.41–19.31) .013
Presence of mitotic figures within parenchyma cells 4.76 (1.24–18.21) .022Death due to disease
Intraoperative tumor rupture 58.71 (2.39–1,439.96) .013Distant recurrence 38.74 (3.44–435.62) .003
CI, Confidence interval; HR, hazard ratio.
SurgeryVolume 156, Number 5
Villar-del-Moral et al 1139
for PC include clinical manifestations resultingfrom severe hypercalcemia with severe bone andkidney involvement, palpable neck mass, hoarse-ness, or palpable, enlarged neck lymph nodes.
Laboratory findings include markedly increasedPTH levels (>5 times above normal levels) andserum calcium concentrations (usually exceeding14–15 mg/dL). On ultrasonography, PC may have

Fig 2. Comparative analysis of effectiveness of different staging systems predicting disease-specific survival (log ranktest). (A) Shaha and Shah system. (B) Schulte differentiated classification. (C) Schulte risk staging.
Fig 3. Comparative analysis of ability of different staging systems predicting recurrence-free survival (log rank test). (A)Shaha and Shah system. (B) Schulte differentiated classification. (C) Schulte risk staging.
SurgeryNovember 2014
1140 Villar-del-Moral et al
ill-defined margins and signs of invasion of sur-rounding structures, as well as lymph node metas-tases.1 Strategies to increase the accuracy ofpreoperative diagnosis include improving imagingtechniques and defining new serum or urine bio-markers.1,5,6,21 Bae et al4 found that tumor sizeand alkaline phosphatase levels can predict thebenignity or malignancy of a suspicious parathy-roid lesion. The cut-off level with highest discrimi-nation power was a tumor size of 3.0 cm and serumalkaline phosphatase level of 285 IU/L. Belowthese levels, the suspicious enlarged parathyroidgland is more likely to be benign.
According to different studies, the type ofresection performed (local vs en-bloc excision) isa key factor in long-term outcomes in terms oflocal relapse and mortality.3,20,22 In our cohort, thehigh rates of en-bloc resection reported werepossibly attributable to intraoperative detectionof a parathyroid gland suspected as malignant.Although this factor was not found to have anyprognostic value in multivariate analysis, these
high rates of radical surgery could explain differ-ences in terms of recurrence and mortalitybetween our data and some of the previously re-ported outcomes.
The effectiveness of intraoperative PTH assaysduring resection for PC remains unknown. Previ-ous studies focused on this topic are rare and havea small sample size.23,24 Miami criteria were used inall cases.25 To the extent of our knowledge, thereare no studies available on the potential power ofintraoperative PTH monitoring to predict recur-rence or death of PC. Thus, this survey study isthe first to analyze the power of intraoperativePTH monitoring to predict healing or incompletetumor resection. In our study, the largest seriesconsidering this factor, PTH levels decreasedmore than 60% with respect to preoperative valuespresented significance for prolonged recurrence-free survival on univariate analysis. However, thesmall sample size could have limited the relevanceof this potential tool for intraoperatively evaluatingcompleteness of resection in PC.

SurgeryVolume 156, Number 5
Villar-del-Moral et al 1141
Intraoperative tumor rupture and margininvolvement are potentially confounding factors.Rupture occurred in less than 5% of cases in thiscohort, although it is difficult to know the accuracyof this figure because rupture could be an under-reported feature in operative reports, constitutinga potential source of bias. Anyway, the evolution ofthese patients was marked by local recurrence andcancer-related death. Because of this, the surgeonmust take measures to avoid gland rupture andtumor spillage and should consider performingen-bloc resection for any suspicious lesion. On theother hand, it is well established that disease-positive resection margins are associated withincreased local recurrence rates. In our study,with a margin invasion rate of 11%, this variableemerges as a prognostic marker on univariateanalysis. However, as reported by Schulte et al8
for a cohort with 17% of positive-margins, theimpact of margin invasion disappears on multivar-iate test.
With respect to treatment of lymph nodemetastases, the majority of authors recommendipsilateral central cervical lymph node dissection aspart of initial surgery, although its implementationin surgical practice is limited.5,7 In the AmericanNational Cancer Data Base report, Hundahlet al7 found that nodal status was only evaluatedin 37% of cases. In the systematic review publishedby Talat and Schulte,3 of the 1,027 cases collectedfrom literature, only 193 (18.8%) provided adescription of some type of nodal dissection. Inour study, only 19 cases (30.6%) had undergonesome kind of nodal dissection, with a possible un-derestimation of nodal disease, which could biasTNM scheme results.9 Another factor with thesame potential effect is tumor size. This variablehas been reported to have no prognostic impactin any of the revised studies,3,7,20 which is consis-tent with our results.
Invasion of adjacent structures was analyzed bySandelin et al20 and was found to have an impacton recurrence, but not in mortality, for tumorswith this histologic feature. In our cohort, thisfactor did not showed prognostic influence evalu-ated separately. On the other hand, is one of thedefining criteria established by Schulte for PC tobe classified as class III, a stage that predicts dis-ease relapse in our patients.
Similarly, the presence of nodal invasion hasbeen shown to have no influence on cancer-relateddeath.7 However, according to Sandelin et al20 andHarari et al,19 nodal involvement was found to be apredictive factor of recurrence. Node involvementincidence is variable, ranging from 6 to 32% of
cases with nodal dissection.2,3 In our cohort, itwas present in 40% of patients undergoing sometype of lymph node sampling, being a featurethat increased the risk of recurrence, due to itsinvolvement in stage III according to Schulteclassification.
Histologic criteria of PC were first described bySchantz and Castleman in 1973.26 In this paper,the presence of mitoses in the tumor parenchymacells was the most valuable criterion for PC diag-nosis, although it is not pathognomonic, beingpresent in 81% of cases. Bondeson et al27 foundthis feature in 75% of patients in their multina-tional cohort. According to these authors, mitoticactivity constituted a prognostic risk factor (relatedto recurrence), but with limited diagnostic signifi-cance. In our cohort, 51% of patients exhibitedthis feature, entailing a 4.7-fold greater risk ofrelapse, thus underscoring the prognostic signifi-cance of this finding.
There was histologic evidence of vascular inva-sion in 37% of patients evaluated by Busaidyet al.28 In contrast, Schulte et al8 found this featurein 40% of cases, and observed a close relationshipbetween vascular invasion, distant metastases, andpoor prognosis. The scarcity of patients withdistant relapse in our cohort could have limitedthe prognostic power of vascular invasion, despitethe fact that it had a greater prevalence amongour patients (67%). Synchronic distant metastaseswere a negative prognostic factor in the SEER data-set analysis.2 In our cohort, only one patient suf-fered bone dissemination at the time ofdiagnosis. The occurrence of distant spread duringfollow-up was a prognostic factor of mortality,which is consistent with the results of Harariet al.19
In 1999, the American National Cancer DataBase reported that TNM-type staging systems hadpoor prognostic power because of their scarceability in predicting long-term survival.7 Despitethis, a TNM system was proposed by Shaha andShah.9 Its performance was tested on a systematicreview conducted by Talat and Schulte in 2010,3
who proposed two new staging systems (risk pat-terns and TNM-type) based on histological andanatomical cancer progression features. Unlikeschemes proposes by Talat and Schulte, in theShaha and Shah system a stepwise worsening ofprognosis was not associated with a greater stage.Our results support the greater effectiveness ofTalat and Schulte classification because it estab-lishes a closer correlation between high-risk oradvanced stage and poor prognosis in terms ofrecurrence, which is critical to this neoplasm.

SurgeryNovember 2014
1142 Villar-del-Moral et al
Regarding the limitations of the present study, asource of potential selection bias might be therecruitment scheme, which was focused on Endo-crine Surgery Units affiliated to the ESS. Thesecenters might have better outcomes than generalsurgery services. In contrast, despite having usedWorld Health Organization 2004 criteria fordefining PC, collecting histopathologic data fromformer pathology reports involves the risk of hav-ing an atypical adenoma incorrectly classified ascarcinoma. Both potential biases could lead to theunderestimation of relapse rates and death-relateddisease. Although the small cohort size limits firmconclusions regarding outcomes, our series is thelargest multi-institutional cohort study ever re-ported by a European country.
In our opinion, our results can be generalizableto other countries having a policy of referringcomplex patients to tertiary care centers withskilled endocrine surgery teams. It is needed toconduct further research based on national orcontinental prospective registries, with central his-topathology review of all specimens against anenhanced list of graded criteria. This plan mayhelp obtain an adequate cohort size that enablesthe analysis on unclear points regarding theprognostic impact of some histopathologic find-ings, intraoperative PTH decrease19 and nodal in-vasion. The improvement of the nodal yield willbe linked to a better preoperative diagnosis. Withthis goal, it will be critical the definition of bio-markers able to discriminate between benign andmalignant lesions. In addition, policies requiringthat patients suspicious with PC are referred tospecialized centers should be adopted.
In conclusion, there are several factors affectingthe prognosis of PC. Apart from cytological find-ings (tumor parenchyma cell mitoses) andanatomical cancer progression features (nodaland periglandular invasion), long-term outcomesare influenced greatly by surgeon’s performance,which emphasizes the importance of preoperativediagnosis. Patients with suspected PC should bereferred to centers with experienced surgeons whoare familiar with the treatment of this disease toimprove the chances of relapse-free survival.
The authors appreciate the methodologic and statis-tical support of Beatriz Valero Aguilera (FIBAO, Foun-dation of Biomedical Research of Oriental Andalusia),the critical review of the manuscript performed by JuanI. Arcelus Mart�ınez, MD, PhD, and the translationassistance from Daniel A. Perilat and Nuria Hernandez.Also, we acknowledge the cooperation of all surgeonsand units affiliated to the Endocrine Surgery Section of
the Spanish Association of Surgeons who have contrib-uted cases to the study.
REFERENCES
1. Fang SH, Lal G. Parathyroid cancer. Endocr Pract 2011;17(Suppl 1):36-43.
2. Lee PK, Jarosek SL, Virnig BA, Evasovich M, TuttleTM. Trends in the incidence and treatment of parathy-roid cancer in the United States. Cancer 2007;109:1736-41.
3. Talat N, Schulte KM. Clinical presentation, staging andlong-term evolution of parathyroid cancer. Ann Surg Oncol2010;17:2156-74.
4. Bae JH, Choi HJ, Lee Y, Moon MK, Park YJ, Shin CS, et al.Preoperative predictive factors for parathyroid carcinoma inpatients with primary hyperparathyroidism. J Korean MedSci 2012;27:890-5.
5. Owen RP, Silver CE, Pellitteri PK. Parathyroid carcinoma: areview. Head Neck 2011;33:429-36.
6. Sharretts JM, Kebebew E, Simonds WF. Parathyroid cancer.Semin Oncol 2010;37:580-90.
7. Hundahl SA, Fleming ID, Fremgen AM, Menck HR. Twohundred eighty-six cases of parathyroid carcinoma treatedin the U. S. between 1985-1995: a National Cancer DataBase Report. The American College of Surgeons Commis-sion on Cancer and the American Cancer Society. Cancer1999;86:538-44.
8. Schulte KM, Gill AJ, Barczynski M, Karakas E, Miyauchi A,Knoefel WT, et al. Classification of parathyroid cancer.Ann Surg Oncol 2012;19:2620-8.
9. Shaha AR, Shah JP. Parathyroid carcinoma: a diagnostic andtherapeutic challenge. Cancer 1999;86:378-80.
10. Vandenbroucke JP, von Elm E, Altman DG, Gøtzsche PC,Mulrow CD, Pocock SJ, et al. Strengthening the reportingof observational studies in epidemiology (STROBE): expla-nation and elaboration. PLoS Med 2007;4:1628.
11. Spanish Economy Ministry. Royal Decree 1697/2012, of 21December, on the official state population figures resultingfrom the municipal census referred to January 1, 2012.Available from: http://www.boe.es/boe/dias/2012/12/29/pdfs/BOE-A-2012-15714.pdf.
12. Bondeson L, Grimelius L, Delellis RA. World Health Orga-nization classification of tumors, pathology and genetics:tumor of endocrine organs. Lyon, France: IARC Press;2004.
13. Deusche gesellschaft f€ur allgemein und visceralchirurgie.Certification system for thyroid and parathyroid surgeryUnits. German Society of General and Digestive Surgery.Available from: http://www.dgav.de/fileadmin/media/texte_pdf/zertifizierung/CAEK_ZertAntrag.pdf.
14. Kaplan EL, Meier P. Nonparametric estimation from incom-plete observations. J Am Statist Assn 1958;53:457-81.
15. Cox DR. Regression models and life-tables. Journal of theRoyal Statistical Society. Series B (Methodological) 1972;34:187-220.
16. Mantel N. Evaluation of survival data and two new rank or-der statistics arising in its consideration. Cancer ChemotherRep 1966;50:163-70.
17. Erovic BM, Goldstein DP, Kim D, Mete O, Brierley J, TsangR, et al. Parathyroid cancer: outcome analysis of 16 patientstreated at the Princess Margaret Hospital. Head Neck 2013;35:35-9.
18. Brown S, O’Neill C, Suliburk J, Sidhu S, Sywak M,Gill A, et al. Parathyroid carcinoma: increasing

SurgeryVolume 156, Number 5
Villar-del-Moral et al 1143
incidence and changing presentation. ANZ J Surg2011;81:528-32.
19. Harari A, Waring A, Fernandez-Ranvier G, Hwang J, Mit-maker E, Shen W, et al. Parathyroid carcinoma: a 43-yearoutcome and survival analysis. J Clin Endocrinol Metab2011;96:3679-86.
20. Sandelin K, Auer G, Bondeson L, Grimelius L, Farnebo LO.Prognostic factors in parathyroid cancer: a review of 95cases. World J Surg 1992;16:724-31.
21. Rubin MR, Bilezikian JP, Birken S, Silverberg SJ.Human chorionic gonadotropin measurements inparathyroid carcinoma. Eur J Endocrinol 2008;159:469-74.
22. Koea JB, Shaw JH. Parathyroid cancer: biology and manage-ment. Surg Oncol 1999;8:155-65.
23. Sol�orzano CC, Carneiro-Pla DM, Lew JI, Rodgers SE, Mon-tano R, Irvin GL 3rd. Intra-operative parathyroid hormone
monitoring in patients with parathyroid cancer. Ann SurgOncol 2007;14:3216-22.
24. Adam MA, Untch BR, Olson JA. Parathyroid carcinoma:current understanding and new insights into gene expres-sion and intraoperative parathyroid hormone kinetics.Oncologist 2010;15:61-72.
25. Irvin GL 3rd, Dembrow VD, Prudhomme DL. Operativemonitoring of parathyroid gland hyperfunction. Am JSurg 1991;162:299-302.
26. Schantz A, Castleman B. Parathyroid carcinoma. A study of70 cases. Cancer 1973;31:600-5.
27. Bondeson L, Sandelin K, Grimelius L. Histopathologicalvariables and DNA cytometry in parathyroid carcinoma.Am J Surg Pathol 1993;17:820-9.
28. Busaidy NL, Jimenez C, Habra MA, Schultz PN, El-NaggarAK, Clayman GL, et al. Parathyroid carcinoma: a 22-yearexperience. Head Neck 2004;26:716-26.

APPENDIX
PARTICIPATING INVESTIGATORS OF THESPANISH PARATHYROID CARCINOMA STUDYGROUP:
Luis Oca~na-Wilhelmi, MD, Endocrine SurgeryUnit, Department of Surgery, Virgen de la VictoriaUniversity Hospital, Malaga, Spain. Scientificadvisor who contributed with critical review ofthe study proposal and collection of data.
Nuria Mu~noz-P�erez, MD, Endocrine SurgeryUnit, Department of Surgery, Virgen de las NievesUniversity Hospital, Granada, Spain. Scientificadvisor who contributed with critical review ofthe study proposal and collection of data.
Francisco Garc�ıa-Lorenzo, MD, Endocrine Sur-gery Unit, Department of Surgery, Xeral C�ıesHospital, Vigo, Spain. Contributed with criticalreview of the study proposal and collection of data.
Jos�e A. Ildefonso-Mart�ın, PhD, MD, EndocrineSurgery Unit, Department of Surgery, San CarlosUniversity Hospital, Madrid, Spain. Contributedwith critical review of the study proposal andcollection of data.
Adolfo Bas�a~nez-de-Amuch�astegui, PhD, MD,Endocrine Surgery Unit, Department of Surgery,
Galdakano Hospital, Bilbao, Spain. Contributedwith critical review of the study proposal andcollection of data.
David Fern�andez-San-Mill�an, MD, EndocrineSurgery Unit, Department of Surgery, InsularUniversity Hospital, Las Palmas, Spain. Contrib-uted with critical review of the study proposal andcollection of data.
Miguel A.Morl�an-L�opez,MD, Endocrine SurgeryUnit, Department of Surgery, Virgen de la SaludHospital, Toledo, Spain. Contributed with criticalreview of the study proposal and collection of data.
Roberto de la Plaza-Llamas, MD, Department ofSurgery, Guadalajara University Hospital, Spain.Contributed with critical review of the study pro-posal and collection of data.
Joaqu�ın G�omez-Ram�ırez, MD, Endocrine Sur-gery Unit, Department of Surgery, Princesa Uni-versity Hospital, Madrid, Spain. Contributed withcritical review of the study proposal and collectionof data.
Cristina Mart�ınez-Santos, PhD, MD, EndocrineSurgery Unit, Department of Surgery, Costa del SolHospital, Marbella, Spain. Contributed with crit-ical review of the study proposal and collection ofdata.
SurgeryNovember 2014
1144 Villar-del-Moral et al








![4. PARATHYROID HORMONE.ppt [Read-Only]ocw.usu.ac.id/.../mk_end_slide_parathyroid_hormone.pdf · Parathyroid Hormone (PTH) Peptide hormone secreted by parathyroid glands, which are](https://static.fdocuments.us/doc/165x107/5fd9a3fa6d8805309b4bc740/4-parathyroid-read-onlyocwusuacidmkendslideparathyroidhormonepdf.jpg)