Primary hepatic non-Hodgkin lymphoma presenting as acute ...
3
case report Hematol Oncol Stem Cell Ther 2(1) First Quarter 2009 hemoncstem.edmgr.com 299 N on-Hodgkin lymphoma (NHL) is the third most common childhood malignancy with an overall incidence of 10.5 per million. 1 Its incidence is higher in the Middle East as a result of an increased incidence of endemic Burkitt lymphoma. It is usually restricted to lymphoid tissue such as lymph modes, Peyer patches, and the spleen. 1 Primary hepatic NHL is very rare in the pediatric age range. It may be asymptomatic and discovered accidentally or present with non-specific symptoms like abdominal discomfort and/or pain with some constitutional manifestation. 2 We report a rare case of primary hepatic NHL present- ing as acute hepatitis in a child aged 2.5 years who re- sponded to chemotherapy. CASE A 2.5-year-old boy was admitted to our hospital with jaundice, a disturbed level of consciousness and irrita- bility. On examination he had jaundice and was drowsy, with a coma score of 12/15 (Glascow coma score), edema of the lower limbs with no bleeding tendency or lymphadenopathy. ere was low-grade fever of 38ºC to 38.5ºC. Blood pressure was 100/70 mm Hg with good perfusion. Urine output was about 1.2 mL/kg/h. Abdominal examination found a generalized abdomi- nal enlargement, hepatomegaly (liver span 14 cm), with a firm, smooth nontender surface, no splenomegaly, and with moderate ascites. Laboratory investigations were as follows: random blood glucose was 80 mg/dL, blood gases and electro- lytes were normal (pH of 7.36, sodium of 135 mEq/L, potassium of 3.5 mEq/L), creatinine of 1.7 mg/dL, erythrocyte sedimentation rate of 3/7 mm/h (hours 1 and 2), serum albumin of 3.3 gm/dL, total serum bilirubin of 8.6 mg/dL (direct bilirubin of 6.5 mg/dL), AST of 942 U/L, and ALT of 1018 U/L. e complete blood count was as follows: total leukocytic count 7100 mm 3 (lymphocytes of 2000 mm 3 , granulocytes of 4300 Primary hepatic non-Hodgkin lymphoma presenting as acute hepatitis in a 2-year-old male Youssef Al-Tonbary, Ashraf Fouda, Rasha El-Ashry, Khaled Zalata from the hematology/oncology/bmt unit, mansoura university children’s hospital, mansoura, egypt0 correspondence: prof. Youssef al-tonbary · hematology/oncology/bmt unit, mansoura university children’s hospital, mansoura, egypt · t: +20123165302 · y[email protected] · accepted for publication march 2009 hematol oncol stem cel ther 2009; 2(1): 299-301 mm 3 ), platelets of 440 000/cm 3 . Prothrombin time was 18.5/12.5 seconds, prothrombin activity was 44%, INR was 1.9. e Paul Bunnel test for Ebstein-Barr virus in- fection was negative and bone marrow examination was normal. He was provisionally misdiagnosed as having hepatic encephalopathy, post-hepatitis A viral infec- tion, but serologic analysis revealed that hepatitis A vi- rus IgM (HAV IgM) was negative. Hepatitis B and C viruses markers were also negative. e patient was treated for encephalopathy by IV fluids and branched amino acids, IV mannitol, IV flu- mazenil, lactulose oral and enemas for four days with improvement in the level of consciousness, but the ab- dominal enlargement increased so an abdominal ultra- sound was done (Figure 1). e abdominal ultrasound revealed a hypo-echoic lesion 6×4 cm at the left lobe of the liver with similar smaller multiple lesions at the right lobe suggestive of abscess or infarctions, with moderate ascites with internal echoes suggestive of infection. Aspirated ascitic fluid was thick and turbid, with protein 370 mg/dL, glucose 23 mg/dL, and WBC of 10 000 (80% polymorphs and 20% lymphocytes). erefore, septic peritonitis was suspected, and the Figure 1. Two masses in the right and left lobe of the liver.
Transcript of Primary hepatic non-Hodgkin lymphoma presenting as acute ...

case report
Hematol Oncol Stem Cell Ther 2(1) First Quarter 2009 hemoncstem.edmgr.com 299
Non-Hodgkin lymphoma (NHL) is the third most common childhood malignancy with an overall incidence of 10.5 per million.1 Its
incidence is higher in the Middle East as a result of an increased incidence of endemic Burkitt lymphoma. It is usually restricted to lymphoid tissue such as lymph modes, Peyer patches, and the spleen.1 Primary hepatic NHL is very rare in the pediatric age range. It may be asymptomatic and discovered accidentally or present with non-specific symptoms like abdominal discomfort and/or pain with some constitutional manifestation.2 We report a rare case of primary hepatic NHL present--ing as acute hepatitis in a child aged 2.5 years who re--sponded to chemotherapy.
CASEA 2.5-year-old boy was admitted to our hospital with jaundice, a disturbed level of consciousness and irrita--bility. On examination he had jaundice and was drowsy, with a coma score of 12/15 (Glascow coma score), edema of the lower limbs with no bleeding tendency or lymphadenopathy. There was low-grade fever of 38ºC to 38.5ºC. Blood pressure was 100/70 mm Hg with good perfusion. Urine output was about 1.2 mL/kg/h. Abdominal examination found a generalized abdomi--nal enlargement, hepatomegaly (liver span 14 cm), with a firm, smooth nontender surface, no splenomegaly, and with moderate ascites.
Laboratory investigations were as follows: random blood glucose was 80 mg/dL, blood gases and electro--lytes were normal (pH of 7.36, sodium of 135 mEq/L, potassium of 3.5 mEq/L), creatinine of 1.7 mg/dL, erythrocyte sedimentation rate of 3/7 mm/h (hours 1 and 2), serum albumin of 3.3 gm/dL, total serum bilirubin of 8.6 mg/dL (direct bilirubin of 6.5 mg/dL), AST of 942 U/L, and ALT of 1018 U/L. The complete blood count was as follows: total leukocytic count 7100 mm3 (lymphocytes of 2000 mm3, granulocytes of 4300
Primary hepatic non-Hodgkin lymphoma presenting as acute hepatitis in a 2-year-old maleYoussef Al-Tonbary, Ashraf Fouda, Rasha El-Ashry, Khaled Zalata
from the hematology/oncology/bmt unit, mansoura university children’s hospital, mansoura, egypt0
correspondence: prof. Youssef al-tonbary · hematology/oncology/bmt unit, mansoura university children’s hospital, mansoura, egypt · t: +20123165302 · [email protected] · accepted for publication march 2009
hematol oncol stem cel ther 2009; 2(1): 299-301
mm3), platelets of 440 000/cm3. Prothrombin time was 18.5/12.5 seconds, prothrombin activity was 44%, INR was 1.9. The Paul Bunnel test for Ebstein-Barr virus in--fection was negative and bone marrow examination was normal. He was provisionally misdiagnosed as having hepatic encephalopathy, post-hepatitis A viral infec--tion, but serologic analysis revealed that hepatitis A vi--rus IgM (HAV IgM) was negative. Hepatitis B and C viruses markers were also negative.
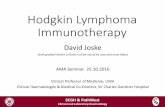
The patient was treated for encephalopathy by IV fluids and branched amino acids, IV mannitol, IV flu--mazenil, lactulose oral and enemas for four days with improvement in the level of consciousness, but the ab--dominal enlargement increased so an abdominal ultra--sound was done (Figure 1). The abdominal ultrasound revealed a hypo-echoic lesion 6×4 cm at the left lobe of the liver with similar smaller multiple lesions at the right lobe suggestive of abscess or infarctions, with moderate ascites with internal echoes suggestive of infection. Aspirated ascitic fluid was thick and turbid, with protein 370 mg/dL, glucose 23 mg/dL, and WBC of 10 000 (80% polymorphs and 20% lymphocytes).
Therefore, septic peritonitis was suspected, and the
Figure 1. Two masses in the right and left lobe of the liver.

case report NHL HEPATITIS
Hematol Oncol Stem Cell Ther 2(1) First Quarter 2009 hemoncstem.edmgr.com300
patient received cefotaxime and IV metronidazole. A drain was introduced, which drained about 500 mL of ascitic fluid per day. A triphasic CT scan of the chest and abdomen revealed marked enlargement of the liver with diffuse hypo-dense areas in the right and left lobes, main--ly at the porta-hepatis, with moderate ascites (Figure 2). An ultrasound-guided liver biopsy revealed diffuse infil--tration by tumor tissue (Figure 3), which was formed of densely arranged medium sized neoplastic rounded cells, uniform in size and shape with slightly indented nuclei and a small rim of cytoplasm (malignant round cells in--filtration, which is highly consistent with non-Hodgkin lymphoma, Burkitt type). The same finding was con--firmed in the peritoneal aspirate (Figure 4). We per--formed immunohistochemical staining for CD3, CD10 and CD20, applying monoclonal antibodies from Dako (Denmark) and Envision detection system. Diamino Benzedin (DAB) was applied as chromogen. CD20 and CD10 were diffusely positive, and CD3 was negative. A positive CD10 and CD20 supported the diagnosis of Burkitt lymphoma. On these bases, a diagnosis of Non-Hodgkin lymphoma (Burkitt type) was made.
The patient received chemotherapy (COMP proto--col: IV cyclophosphamide, IV vincristine, IV and intra--thecal methotrexate, and oral prednisone). We applied half of the dose due to the elevated bilirubin and liver enzymes. Then the full dose was given when these el--evations were normalized and he achieved remission.
DISCUSSIONNon-Hodgkin lymphoma (NHL) accounts for 6% to 7% of malignant diseases in childhood in Europe and the United States. It represents about 45% of all lym--phomas in children.1 Lymphomas are a diverse collec--tion of different diseases with varying histologies and clinical presentations. Although secondary involvement of the liver is commonly found in advanced lymphoma, primary hepatic NHL is a rare and poorly character--ized disease.2
Lymphoma that presents with disease confined to the liver appears to be extremely rare. A retrospective cancer registry study published 30 years ago identified only 1467 cases of primary extranodal disease in a da--tabase of 12 447 white patients with lymphoma (12%). Only 6 of the extranodal lymphomas (0.05% of the to--tal) were said to arise from the liver or biliary system.3 Similarly, a prospective population-based Dutch survey identified 580 newly diagnosed cases of lymphoma from 1981 through 1986, none of which were considered to be primarily hepatic.4 Fewer than 150 cases have been reported in the worldwide literature.2
Primary hepatic NHL occurs over a wide age range
Figure 2. marked enlargement of the liver with diffuse hypo-dense areas (CT abdomen).
Figure 3. Hematoxylin-eosin stain of the liver biopsy: atypical lymphoid cells with frequent apoptotic bodies infiltrating the liver tissue.
Figure 4. Hematoxylin-eosin stain of peritoneal aspirate: atypical lymphoid cells in the peritoneal aspirate.

case reportNHL HEPATITIS
Hematol Oncol Stem Cell Ther 2(1) First Quarter 2009 hemoncstem.edmgr.com 301
but is most commonly a disease of middle age. It occurs twice as frequently and at a younger age in men than in women.5 It is very rare in pediatrics, having been re--ported only once in a 9-year-old child.6 Presentation is usually nonspecific, with the most frequently reported symptom being abdominal discomfort or right upper quadrant pain. Constitutional symptoms such as fever, anorexia, and weight loss are common. As many as 10% of patients will be asymptomatic; primary hepatic NHL will only be discovered after an evaluation for incidental hepatic abnormalities. The most common physical find--ing is hepatomegaly, which is present in 62% to 82% of cases. Jaundice is usually a late manifestation of disease progression and can be caused by periportal adenopa--thy or it can be related to underlying cirrhosis.5
Case series that have addressed the rare presenta--tion of rapidly progressive hepatic failure suggest that it is usually associated with widespread systemic disease. Fulminant liver failure from lymphoma is characterized by jaundice, encephalopathy, coagulopathy, and lactic acidosis. It is associated with an extremely poor out--come, with an average survival of only 10.7 days from diagnosis. In many cases, the correct diagnosis is not made until autopsy.7
Blood counts are usually normal in the early stages of primary hepatic NHL. As the disease progresses, hypersplenism and bone marrow involvement lead to more frequent abnormalities. Blood chemistry evalu--ations demonstrate increases in liver function tests in
75% to 85% of cases. As a well-established marker in lymphoid malignancy, the lactate dehydrogenase level is increased in 85% of cases whereas measurements of α-fetoprotein and carcinoembryonic antigen are usually normal.5 There is no identifiable laboratory pattern that is specific for hepatic lymphoma.2
Lymphoma can involve the liver as one or more dis--crete masses. In a series of 31 patients with primary he--patic NHL, a multinodular presentation was reported in the majority of patients (55%), followed by a solitary hepatic nodule in 39% and diffuse disease in 6%.8
Computed tomography (CT) usually demonstrates the presence of homogeneous low-attenuation masses that may have a thin enhancing rim after contrast ma--terial administration, and larger masses can have areas of very low-density reflective of necrosis. Diffusely infiltrative disease can present as hepatomegaly with little alteration in parenchymal density or architectural distortion. Ultrasonography usually demonstrates the presence of hypoechoic homogenous masses that cor--relate well with findings on CT imaging.9
More than half of all hepatic lymphomas fall within the category of diffuse large-cell lymphoma.10 Primary Burkitt lymphoma of the liver has been reported, some--times in association with human immunodeficiency virus (HIV) or hepatitis C virus (HCV).11 Mucosa-associated lymphoid tissue (MALT)-type lymphoma is the most common low-grade histology, although follicular and lym--phoplasmacytic lymphomas have also been described.
1. Lanzkowsky P: Non Hodgkin Lymphoma, In: manual of Pediatric Hematology and Oncology, 4th edition, Elservier Academic Press, San Diego, London, 2005; P 491-5112. Salmon JS, Thompson mA, Arildsen rC, Greer JP. Non-Hodgkin’s lymphoma involving the liver: clinical and therapeutic considerations. Clin Lym--phoma myeloma. 2006;6(4):273-280.3. Freeman C, Berg JW, Cutler SJ. Occurrence and prognosis of extranodal lymphomas. Cancer. 1972;29:252-260.4. Otter r, Gerritis WB, Sandt mm, et al. Primary extranodal and nodal non-Hodgkin’s lymphoma: a
survey of a population-based registry Eur J Cancer Clin Oncol; 1989;25:1203-1210.5. Lei KI. Primary non-Hodgkin’s lymphoma of the liver. Leuk Lymphoma; 1998;29:293-299.6. Fikri m and Dafiri r. Primary hepatic lymphoma: re--port of a pediatric case. J radiol. 2006;87(3):311-313.7. Lettieri CJ and Berg BW. Clinical features of non-Hodgkins lymphoma presenting with acute liver failure: a report of five cases and review of published experience. Am J Gastroenterol. 2003;98(7):1641-1646.8. Bronowicki JP, Bineau C, Feugier P, et al. Pri--mary lymphoma of the liver: clinical-pathological
features and relationship with HCV infection in French patients. Hepatology; 2003;37:781-787.9. Harisinghani mG and Hahn PF. Computed to--mography and magnetic resonance imaging evaluation of liver cancer. Gastroenterol Clin; 2002;31:759-776.10. Bagley Cm Jr, Thomas LB, Johnson rE, et al. Diagnosis of liver involvement by lymphoma: re--sults in 96 consecutive peritoneoscopies. Cancer; 1973;31:840-847. 11. Kuroda J, Omoto A, Fujiki H, et al. Primary he--patic Burkitt’s lymphoma with chronic hepatitis C. Acta Haematol; 2001;105:237-240.
REFERENCES