Classical Hodgkin Lymphoma - relapse
45
Classical Hodgkin Lymphoma- relapse Rifca Le Dieu Clinical Reader/Honorary Consultant
Transcript of Classical Hodgkin Lymphoma - relapse

Classical Hodgkin Lymphoma- relapse
Rifca Le DieuClinical Reader/Honorary Consultant

Learning Objectives
• To understand the relevance of prognostic factors at relapse• To understand the treatment pathway in R/R Hodgkins• To appreciate the (lack of) evidence base for what is done• To understand how new agents are changing the treatment
paradigm in relapsed disease

3

Scale of the problem
• 10% early stage and 15-30% of advanced stage will have primary refractory disease or experience relapse
• ~70% of relapses occur within 2 years of primary therapy• Of these, ~50% will be cured with salvage therapy
Primary refractory disease: Progression or non-response during induction treatment or within 90 days of completion
Kuruvilla 2011

Relapsed/refractory disease
• Small but challenging population• Repeat biopsy recommended
• In all relapse ?change in histology • Consider in those with residual FDG-avid lesions post therapy -
confirm active disease
• Tissue type patient and siblings
Collins 2013

Prognostic factors at relapse
• Intensity of 1st line therapy (Josting 2010)
• Relapse post BEACOPP more challenging than relapse post ABVD
• Time to relapse (Josting 2000, Pfreundschuh 1994)
• 5y OS• Primary refractory: 26%• Early relapse (<12m): 46% • Late relapse (>12m): 71%
• Extranodal involvement prior to salvage (Martin 2001)
• Presence/absence of systemic symptoms prior to salvage (Moskowitz 2001)
• PS at time of salvage (Ferme 1995)
Allow informed consent onlyDo not impact on therapy decisions

Prognostic factorsPET status post salvage:
probably the most important predictor of outcome
PET –ve post salvage – 3-5y PFS of > 70%PET +ve post salvage – 3-5y PFS 25-30%
Jabbour 2007, Moskowitz 2010

First line salvage treatment
8

Salvage chemotherapy
induce PET –ve CR (Deauville score 1-3)
minimize toxicity to stem cell compartmentCollins 2013
Aim of treatment in younger patients with no significant comorbidities : induce remission and proceed to ASCT
Meta-analysis of 11 studies – overall survival: pre-transplant PET positive: 17-77% pre-transplant PET negative: 78-100%
Adams & Kwee, 2016

Salvage chemotherapy
• First-line salvage – all single arm phase II trials
ORR:70-89%CRR: 21-54%

Salvage – how do you choose?
• Use an established regimen which is familiar to treating centre
• Tailor to individual patient needs– Avoid cisplatin in renal impairment– Avoid ifosfamide in patients at high risk of ifosphamide-induced
encephalopathy (previous cisplatin / concomitant opioids or CYP2B6 inhibitors)
Collins 2013

Salvage – how much?
• No published evidence
• Consensus: 2 cycles of a multi-agent regimen then re-evaluation using CT-PET
Collins 2013

Salvage – what next?
PET –ve stem cell harvest (?after #3 salvage) and ASCT
PET +ve 2nd line salvage

Second line salvage…introducing the novel agents
14

Which second line salvage regimen?
• No difference in outcome in those achieving a –ve pre-ASCT PET irrespective of whether 1 or 2 lines required to achieve it (EFS>80%)
• Choose another – GEM-P, ICE, DHAP….– Original paper (Moskowitz 2012) used standard or augmented dose
ICE and if PET +ve – GVD
• Brentuximab vedotin (BV)
15

Brentuximab vedotin
Anti-CD30 monoclonal antibody conjugated to MMAE (= vinca alkaloid)1.8mg/kg IV D1 every 21 days up to 16 cyclesRe-evaluate after 3-4 cyclesSEs: peripheral neuropathy, bone marrow toxicity, lung toxicity (don’t give with gemcitabine/bleomycin or concurrently with mediastinal RT)
Monomethyl auristatin EIn 2011, first new drug to be approved in Hodgkins since 1977

Efficacy of BV as bridge to ASCT• Eyre, BJH 2017
– UK-wide retrospective study– 99 SCT-naïve R/R– Non-toxic bridge to SCT in 34%– Deferred SCT (inadequate response to BV) in 27%– 39% never reached SCT with PFS of 3.0 months
• Approved by NICE for R/R HL after at least 2 previous therapies when ASCT or multi-agent chemotherapy not an option (pre-SCT)(as of June 2018)

BV Combinations
• Combination Benda + BV as 1st line salvage (LaCasce Blood 2018)
– Phase I/II single arm study– N=55– ORR 92.5%, CR 73.6%– Infusion-related reactions 56.4% (severe in 14.5%)
18
Not approved by NICE. As of Oct 2020, Bendamustine not funded by NHSE for R/R Hodgkins.
Only in the context of a clinical trial
Presenter
Presentation Notes
Ash 2020: Paediatric study examined this combination in 29 R/R patients CR rate 62% and ORR 79%

Checkpoint Inhibitors (CPI)• Remove the T cell inhibition
induced by tumour cells
• Anti-PD1 monoclonal antibodies:• Nivolumab• Pembrolizumab
• Anti-PD-L1 monoclonal antibodies:• Avelumab
• Genetically determined vulnerability in HL – consistent amplification of 9p seen. Locus for PD-L1 and PD-L2 genes

Data on CPIs in R/R HL
Antibody ORR (%) CR (%) PFS Follow-up Reference
NivolumabN=243
69 (63-75) 16 (NR) mPFS 14.7m(11.3-18.5)
18m Armand JCO 2018
CheckMate 205
PembrolizumabN=210
69 (62-75) 22 (17-29) PFS@9m 63% At 12m Chen JCO 2017KEYNOTE 087
EHA Education Session 2018
Excellent single agent activity (lower CR rate) with favourable toxicity

Side effects of CPINivolumab• Fatigue (25%)• Infusion-related reactions (20%)• Rash (16%)• Pyrexia (14%• Arthralgias (14%)• Pruritus (10%)• Diarrhoea (10%)
• Asymptomatic lipase elevation• Neutropenia
• Pneumonitis in 2 patients that resolved with steroids
Pembrolizumab• Pyrexia (11%)• Hypothyroidism (10.5%)• Diarrhoea (6.7%)• Fatigue (6.7%)• Headache (6.2%)• Rash (6.2%)• Nausea (5.7%)
• Grade 3/4: neutropenia, dyspnoea, diarrhoea
• 4.3% discontinued due to TR-AEs: myocarditis, myelitis, myositis, pneumonitis, CRS
No deaths attributable to treatment in either study

Pembrolizumab
• Subgroup analysis showed that even in the 23 patients who were refractory to all prior lines of therapy, a response rate of 56% was observed
• NICE recommended as an option for patients who are unsuitable for SCT due to a failure to reach a suitable remission, co-morbidities or age and have failed BV
• 200mg IV every 3w
22

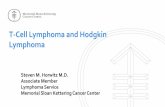
Brentuximab or Pembrolizumab?
• Keynote-204 (EHA 2020)– Open-label, randomised, phase 3 study – N=300 R/R– Pembrolizumab resulted in improved PFS
• 13.2m vs 8.3m• 12m PFS 53.9% vs 35.6%
– No statistical difference in ORR– Authors stated pembrolizumab should be the new standard of care at
relapse post ASCT or in those ineligible for ASCT
23
Brentuximab or Pembrolizumab?
24
Patients on Pembro also had improved HRQoL compared with
patients on BV (Zinzani, ASH 2020)

Autologous stem cell transplantation
25

Autologous stem cell transplantation
2 randomised trials demonstrated significant benefit of ASCT over chemo alone (FFTF not OS) • Linch, Lancet 1993
• BNLI: 3y EFS 53% vs 10%
• Schmitz, Lancet 2002• GHSG: FFTF at 3y 55% vs 34%
• Conditioning regimen: BEAM most popular worldwide

Maintenance post ASCT?• Brentuximab
– licensed for this indication if high risk features present (AETHERA study Moskowitz, Blood 2018 ):
• Primary refractory disease• Relapse within 1y of initial therapy• Extra-nodal disease pre-salvage
– 3y PFS 61% vs 43%– No OS advantage (?due to cross-over between arms)– Not approved by NICE for this indication
• Pembro + BV (ASH 2020)
27

If unfit for ASCT (and failed BV and pembro)…
• No prospective studies• Survival without ASCT (if in CR post salvage) (Longo 1992, Bonfante 1997)
• Primary refractory: 0-8% survive >8y• Early relapse (<12m): 11% 20y OS• Late relapse (>12m): 22% 20y OS
• Combined modality therapy• Single agent chemotherapy (vinblastine, lomustine, etoposide, gemcitabine)• Multiagent oral regimens
• PECC (Prednisolone, etoposide, CCNU (lomustine), chlorambucil)• ChlVPP (chlorambucil, vinblastine, procarbazine, prednisolone)• LD56 (Vinblastine, methotrexate, lomustine, chlorambucil, dexamethasone, bleomycin)
• Consider clinical trial options

Other potential agentsN ORR, % CR, % Median
PFSReference
Lenalidomide Immuno-modulatory agent
38 19% 3% 4 months Fehniger, Blood 2011
Everolimus mTORinhibitor
57 42% 8% 9 months JohnstonBlood 2012
Panobinostat HDAC inhibitor 129 23% 4% 6.1months
YounesJCO 2012
Adapted from LaCasce, Hematol Oncol 2019

Relapse post ASCT
30

• Outcomes poor, especially if within 6-12 m• Median OS 25-32 months• Aim: to attain sufficient response to allow alloSCT
Collins 2013
Options now:(1) Brentuximab if you haven’t used it before(2) Re-use of brentuximab(3) Nivolumab if previous brentuximab (and no pembro)

Brentuximab for relapse post ASCT
• Pivotal phase II study (Younes 2012)
• In 102 CD30+ relapsed patients post SCT• Objective responses in 75%• CR in 34% (median duration of response 20.5 m in this group)• Median PFS 5.6m• Of note, patients who did not achieve CR at first re-staging were unlikely to achieve CR with further
therapy• Only 8 proceeded to alloSCT
• Chen, Blood 2012• Retrospective cohort of patients (n=18) who proceeded to RIC alloSCT after BV
• One yr PFS and OS 92% and 100%; TRM 0%
Re-treatment with Brentuximab
• Bartlett 2014– Phase 2 – N=21– ORR 60%, CR 30%– Median duration of response 9.5 months– If in CR, 45% had response durations>1y– Higher rate of peripheral neuropathy – 28%
33

Nivolumab
• Nivolumab: – 3mg/kg IV every 2w for up to 2y– NICE approved in July 2017 for R/R Hodgkins after treatment with
ASCT and BV

Response assessment post CPI
• Use LyRIC (Lymphoma response to immunologic therapy) criteria in PET assessment– ‘indeterminate’ response due to pseudo-progression (Cheson 2016)
• Concept of ‘treatment beyond progression’• If clinical response and no significant SEs• Of 70 patients treated beyond conventional PET-defined progression, 61%
had stabilisation or reduction of their target lesions at the subsequent response assessment (Armand, 2018)
35

The future for new agents• Lots of combination studies ongoing• Durability of responses and toxicities need further investigation• ?Is this really a better strategy than sequential use
– BV + Nivolumab (Herrara, ASH 2018)• 62 R/R patients• ORR 82%, CR 61%• IRRs in 44% • 8% treated with steroids for immune-related AEs
– BV + Ipilumumab + Nivolumab (Diefenbach, ASH 2018)• 22 R/R patients• ORR 82%, CR 68%• in 9 patients post ASCT, ORR 95% and CR 79%• Large number of grade 3 AEs
Randomised phase 2 study of doublet vs triplet
ongoing

Allogeneic stem cell transplantation• Reduced intensity conditioning• Chemo-sensitivity at time of transplant most important
prognostic indicator• TRM has improved over time
• <10% in <50y• 15% in 50-70y
• PFS 20-40% at 2-4 yrs; OS 35-60% 2y post • Donor availability: no significant difference in PFS/OS between
donor types (EBMT Registry study, Martinez JCO 2017)
Collins 2013

CPI and alloSCT• Possibility of increased GvHD due to modulation of antigen-specific T cell responses• Multicentre retrospective study (Merryman Blood 2017)
– n=39 (79% with HL)– Median of 62d (range 7-260) between last dose CPI and allo– Grade 2-4 aGVHD in 44%; Grade 3-4 aGVHD in 23%– cGVHD in 41% by 1y– 1 year non-relapse mortality 11%
• Meta-analysis 2019: does not increase mortality but does increase grade 3-4 GvHD• ICML-15: stop CPI 2m pre allo and give cyclo as additional GvHD prophylaxis
Remain vigilant

CAR T cells• Ramos JCO Nov 2020
• CD30 CAR-T• Fludarabine-based lymphodepletion• N=41• Median 7 prior lines of therapy• ORR in 32 patients with active disease 72%• 19 patients in CR• 1y PFS 36%; OS 94%• 10 CRS (all grade 1), no neurotoxicity
• Other trials underway:2018 – 3, 2019 – 9, 2020 –13, 2021 – 21• None currently in the UK
Microenvironment/tumourimmunology clearly different to B NHLs

Current clinical trials open in the UKANIMATE:Nivolumab monotherapy in patients failing to achieve CMR following 2 cycles of salvageNCT03337919
Phase II UCL CTC/BMS Numerous sites
CheckMate 744: Nivolumab + BV after failure of first line therapy followed by BV + Benda in those with sub-optimal responseNCT02927769
Phase IIAge 5-3080 patients
BMS Numerous sites
ADCT-301:Following 3 lines of therapy inc BV and CPINCT04052997
Phase II100 patients
ADC Therapeutics Manchester, Oxford, UCL, Plymouth
SEA-TGT:Advanced cancer inc HodgkinsNCT04254107
Phase I Seagen Inc Royal Marsden
https://clinicaltrials.gov
41
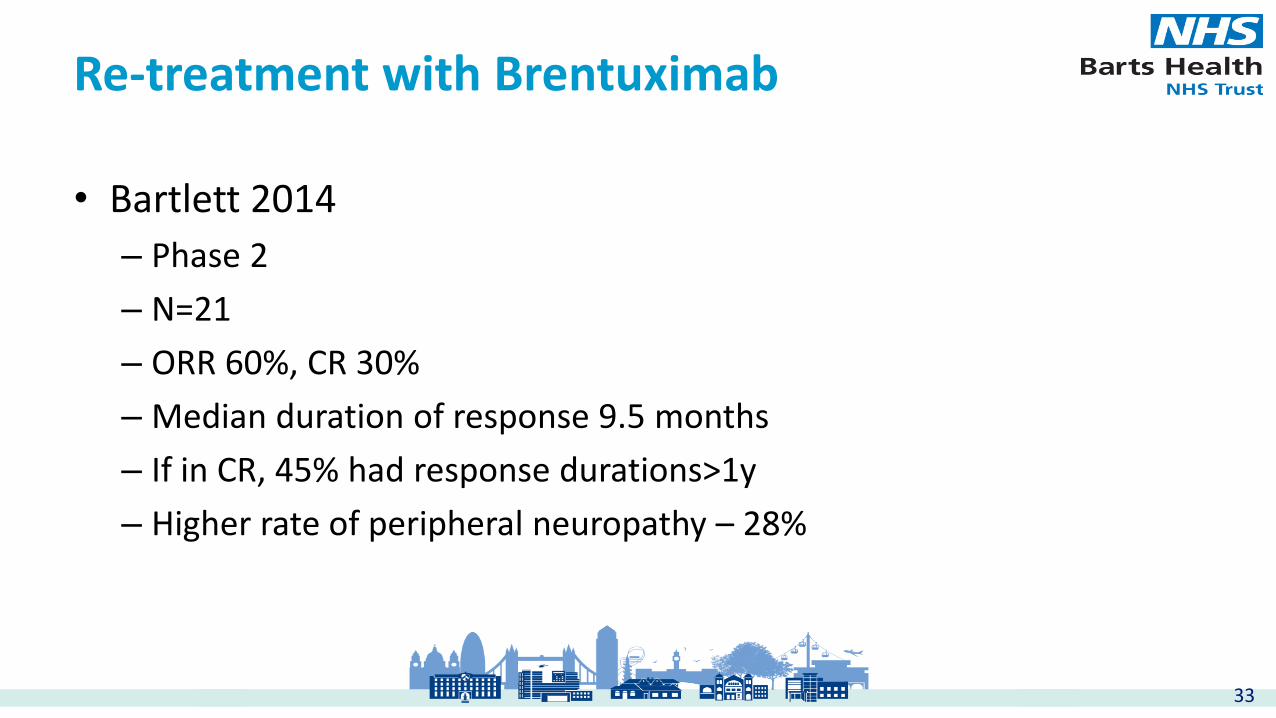
We are getting better at this….
Outcomes in patients relapsing post ASCT
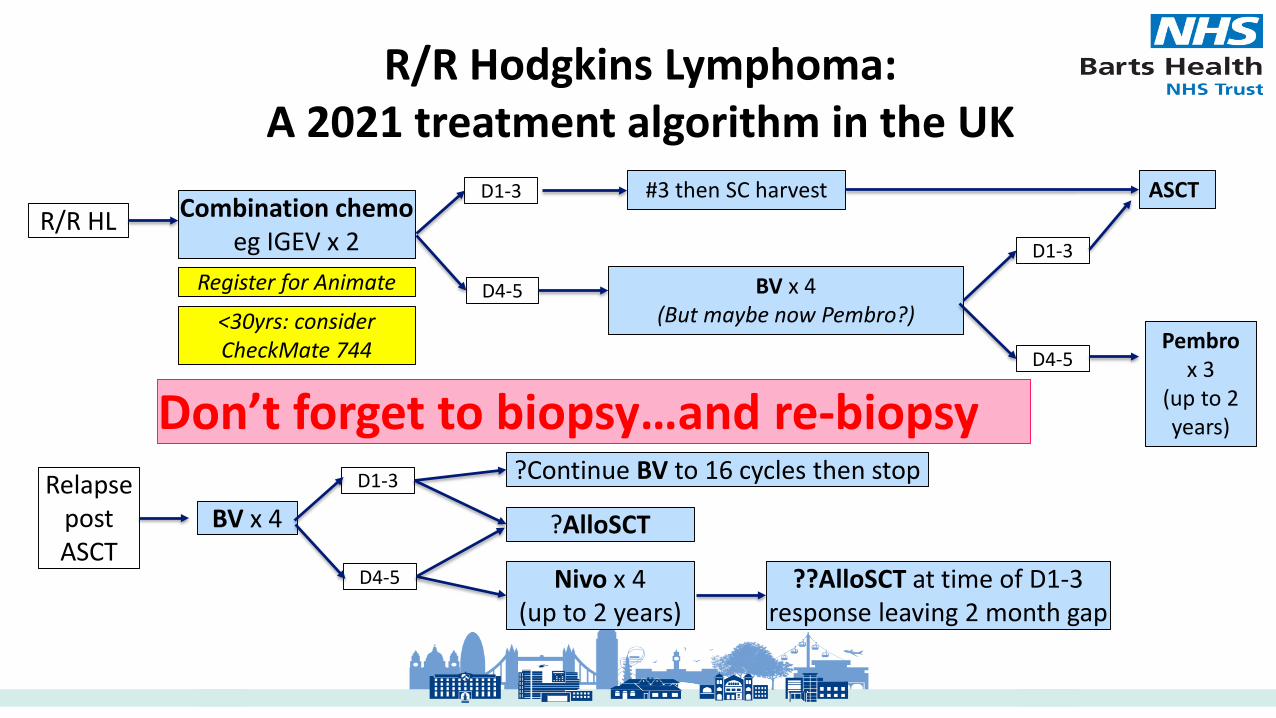
R/R HL Combination chemoeg IGEV x 2
D1-3
D4-5
#3 then SC harvest ASCT
BV x 4 (But maybe now Pembro?)
Pembrox 3
(up to 2 years)
D1-3
D4-5
R/R Hodgkins Lymphoma: A 2021 treatment algorithm in the UK
Don’t forget to biopsy…and re-biopsy
Register for Animate
<30yrs: consider CheckMate 744
Relapse post ASCT
BV x 4 ?AlloSCT
D1-3
D4-5 Nivo x 4(up to 2 years)
??AlloSCT at time of D1-3 response leaving 2 month gap
?Continue BV to 16 cycles then stop

Key messages
• Cure is currently possible in 50% of R/R patients • PET post salvage most important predictor of outcome• No data to support one salvage regimen over another• Aim to induce remission and proceed to ASCT• Relapse post ASCT: new drugs – BV and Nivolumab; aim for
allo• Non-transplant candidates: BV, Pembro, single agents, multi-
agent PO regimens

Challenges• The lack of evidence!
– How do we integrate the data out there to direct patient care?• The need for validated biomarkers to aid clinical decision making
– Can we predict who will get R/R disease? And then how they will respond to salvage?
– (But if we could, would we treat them differently?)• Improving our CR rate with salvage (…to get more to ASCT)• Better understanding of the roles of BV/CPI
– More may not necessarily be better….• Optimal timing of alloSCT…is it wise to delay?

Thank you for your attention