Preventing Acute to Chronic Pain after Surgery
42
Colin J.L. McCartney Colin J.L. McCartney MBChB PhD FCARCSI FRCA FRCPC MBChB PhD FCARCSI FRCA FRCPC Professor and Chair of Anaesthesia Professor and Chair of Anaesthesia University of Ottawa University of Ottawa Head of Anaesthesia Head of Anaesthesia The Ottawa Hospital The Ottawa Hospital Scientist, Scientist, Ottawa Hospital Research Institute Ottawa Hospital Research Institute Chronic Pain after Surgery: Chronic Pain after Surgery: Does it exist and can we Does it exist and can we prevent it? prevent it?
-
Upload
colin-mccartney -
Category
Health & Medicine
-
view
307 -
download
3
Transcript of Preventing Acute to Chronic Pain after Surgery

Colin J.L. McCartney Colin J.L. McCartney MBChB PhD FCARCSI FRCA FRCPCMBChB PhD FCARCSI FRCA FRCPCProfessor and Chair of AnaesthesiaProfessor and Chair of AnaesthesiaUniversity of OttawaUniversity of OttawaHead of AnaesthesiaHead of AnaesthesiaThe Ottawa HospitalThe Ottawa HospitalScientist, Scientist, Ottawa Hospital Research InstituteOttawa Hospital Research Institute
Chronic Pain after Surgery: Chronic Pain after Surgery: Does it exist and can we Does it exist and can we
prevent it? prevent it?

Objectives (25 mins)Objectives (25 mins)
Understand incidence of CPSP (5 mins)Understand incidence of CPSP (5 mins) Who are the populations at risk? (5 mins)Who are the populations at risk? (5 mins) What new approaches exist for preventing What new approaches exist for preventing
CPSP? (10 mins)CPSP? (10 mins) What does the future hold? (5 mins)What does the future hold? (5 mins)

SummarySummary
CPSP common and varies by type of surgeryCPSP common and varies by type of surgery Preoperative pain and psychological factors Preoperative pain and psychological factors
major predictorsmajor predictors Prevention possible with high quality Prevention possible with high quality
perioperative pain relief including LA techniques perioperative pain relief including LA techniques and NMDA antagonists and surgical approachand NMDA antagonists and surgical approach
Future management possibilities include novel Future management possibilities include novel therapeutic, psychological and therapeutic, psychological and pharmacogenomic approaches pharmacogenomic approaches

Incidence of Incidence of Chronic Post-Surgical PainChronic Post-Surgical Pain
Pain after surgery of primary concern to Pain after surgery of primary concern to patients (Apfelbaum et al 1999)patients (Apfelbaum et al 1999)
Acute postoperative pain remains Acute postoperative pain remains undertreated undertreated
Incidence of severe acute pain a problemIncidence of severe acute pain a problem Severe acute pain associated with CPSPSevere acute pain associated with CPSP Definition: pain >2 months after surgeryDefinition: pain >2 months after surgery

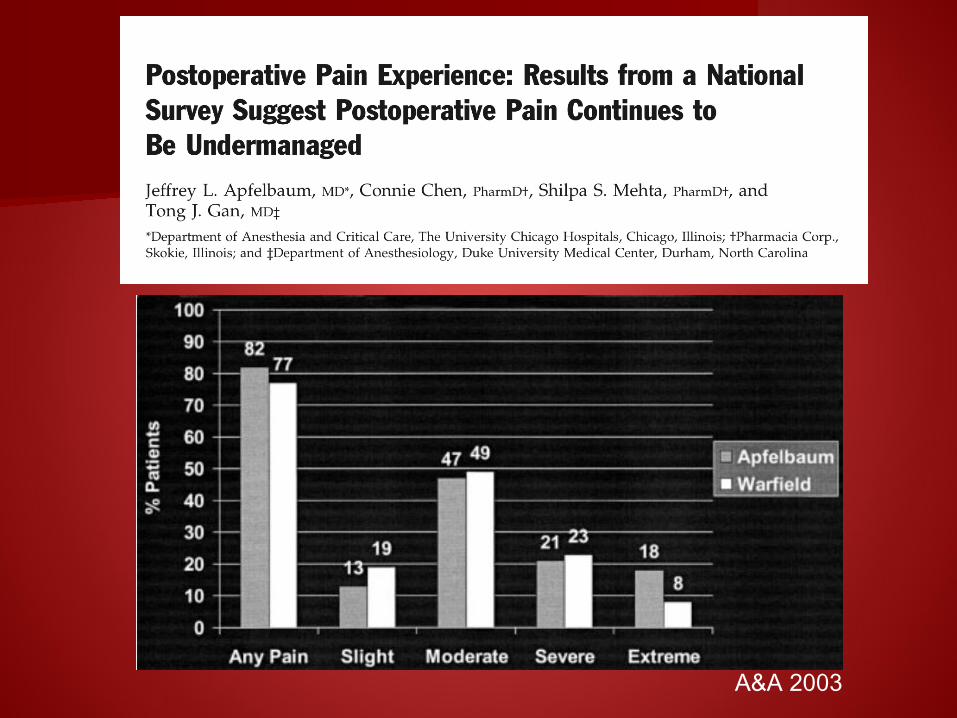
A&A 2003

300 patients300 patients 2/3 had moderate-severe pain after 2/3 had moderate-severe pain after
surgerysurgery No change from 10 years earlierNo change from 10 years earlier
Gan TJ et al CMRO 2014

Or does it?


5130 patients attending chronic pain 5130 patients attending chronic pain clinicsclinics
Surgery contributed to pain in 22.5%Surgery contributed to pain in 22.5% Research needed into: aetiology and Research needed into: aetiology and
procedures contributing to highest risk of procedures contributing to highest risk of CPSP.CPSP.
Preventive strategiesPreventive strategiesPain 1998

Prevalence of persistent postsurgical painPrevalence of persistent postsurgical pain 12982 participants/3111 undergone surgery 12982 participants/3111 undergone surgery
within 3 yearswithin 3 years Persistent pain in 40.4%. Mod-Severe 18.3%Persistent pain in 40.4%. Mod-Severe 18.3%


Poulakka PA et al EJA 2010

Differentiating CPSPDifferentiating CPSP

Systematic review. 281 studies assessed Systematic review. 281 studies assessed investigating PSPS in 11 surgical typesinvestigating PSPS in 11 surgical types
Prevalence of NeuP determined using NeuP Prevalence of NeuP determined using NeuP grading systemgrading system
Prevalence of NeuP high after thoracic and Prevalence of NeuP high after thoracic and breast surgery (66/68%). 31% after groin hernia breast surgery (66/68%). 31% after groin hernia repair and 6% after THA and TKArepair and 6% after THA and TKA
Prevalence of PneuP varies by type of surgery Prevalence of PneuP varies by type of surgery and probability of nerve injuryand probability of nerve injury

Risk Factors for CPSP?Risk Factors for CPSP? Preoperative: Pain, Repeat surgery, Preoperative: Pain, Repeat surgery,
Psychological factors, Female gender and Psychological factors, Female gender and younger age, Genetic predispositionyounger age, Genetic predisposition
Intraoperative: Surgical approach and Intraoperative: Surgical approach and risks of nerve injuryrisks of nerve injury
Postoperative: Acute Pain, Radiation Rx, Postoperative: Acute Pain, Radiation Rx, Neurotoxic chemotherapy, Anxiety and Neurotoxic chemotherapy, Anxiety and Depression, NeuroticismDepression, Neuroticism
McIntyre et al 2010
What can we do about the What can we do about the problem?problem?
Regional anaesthesia techniquesRegional anaesthesia techniques Systemic drug interventionsSystemic drug interventions Modified surgical techniquesModified surgical techniques Focus on postoperative pain controlFocus on postoperative pain control

Regional anesthesia techniquesRegional anesthesia techniques

23 RCTs in total23 RCTs in total Pooled 3 studies for epidural after Pooled 3 studies for epidural after
thoracotomy and 2 for PVB after breast thoracotomy and 2 for PVB after breast surgerysurgery
Unable to pool data from other studies due Unable to pool data from other studies due to marked heterogeneityto marked heterogeneity

Andreae MH et al BJA 2013

Perioperative pharmacotherapyPerioperative pharmacotherapy
KetamineKetamine LidocaineLidocaine GabapentinoidsGabapentinoids NSAIDSNSAIDS

KetamineKetamine

2013 Cochrane Collaboration


No long term benefit for:No long term benefit for:– GabapentinGabapentin– PregabalinPregabalin– NSAIDSNSAIDS– CorticosteroidsCorticosteroids– MexilitineMexilitine
2013 Cochrane Collaboration

Modified Surgical TechniquesModified Surgical Techniques



Future PossibilitiesFuture Possibilities
Impact of psychological factorsImpact of psychological factors Pharmacogenomics and personalized Pharmacogenomics and personalized
medicinemedicine Novel ‘analgesic’ agentsNovel ‘analgesic’ agents

Psychological FactorsPsychological Factors

Preoperative painPreoperative pain Pain catastrophizingPain catastrophizing Mental healthMental health Pain at other sitesPain at other sites

Pain 2013

Predictive Factors Post-Predictive Factors Post-MastectomyMastectomy
Schreiber et al Pain 2013


Pain GeneticsPain Genetics

PharmacogenomicsPharmacogenomics

Genetics of PainGenetics of Pain 3 variants (haplotypes) of gene encoding 3 variants (haplotypes) of gene encoding
COMT predicting low, moderate and high COMT predicting low, moderate and high sensitivity to painsensitivity to pain
Encompass 96% of humansEncompass 96% of humans Low COMT levels predict high pain Low COMT levels predict high pain
sensitivity and risk of developing TMDsensitivity and risk of developing TMD Inhibition of COMT in rat model increases Inhibition of COMT in rat model increases
pain sensitivitypain sensitivityDiatchenko L et al 2005

CPSP is likely 50% influenced by genetic CPSP is likely 50% influenced by genetic determinantsdeterminants
Identifying genetic basis of CPSP could Identifying genetic basis of CPSP could lead to significant improvement in lead to significant improvement in treatmenttreatment
Prediction of CPSP, PharmacogenomicsPrediction of CPSP, Pharmacogenomics Improved treatmentsImproved treatments
CJA: published ahead of print

Novel neuroactive agentsNovel neuroactive agents
Not analgesic per seNot analgesic per se Prevent mechanism of transition to chronic Prevent mechanism of transition to chronic
painpain rhBDNF, neuroprotective agents (e.g. rhBDNF, neuroprotective agents (e.g.
acetyl l-carnitine) and anti-oxidantsacetyl l-carnitine) and anti-oxidants Early promising resultsEarly promising results
Bordet T et al Neurotherapeutics 2009

SummarySummary
CPSP common and varies by type of surgeryCPSP common and varies by type of surgery Preoperative pain and psychological factors Preoperative pain and psychological factors
major predictorsmajor predictors Prevention possible with high quality Prevention possible with high quality
perioperative pain relief including LA techniques perioperative pain relief including LA techniques and NMDA antagonists and surgical approachand NMDA antagonists and surgical approach
Future management possibilities include novel Future management possibilities include novel therapeutic, psychological and therapeutic, psychological and pharmacogenomic approaches pharmacogenomic approaches

Good Acute Pain Control Major Good Acute Pain Control Major Concern for PatientsConcern for Patients
Apfelbaum et al A&A 2003

Acute pain controlAcute pain control Use regional anaesthesia where possibleUse regional anaesthesia where possible Use NSAIDS, paracetamol in multimodal Use NSAIDS, paracetamol in multimodal
regimenregimen For higher risk cases use ketamine and/or For higher risk cases use ketamine and/or
lidocaine infusion during surgerylidocaine infusion during surgery Gabapentin/Pregabalin useful for acute Gabapentin/Pregabalin useful for acute
pain control and reduction of opioid pain control and reduction of opioid consumptionconsumption