Press Conference - International Association for the...
32
Press Conference Monday, Sept. 7, 2015 9:45 a.m. – 10:45 a.m. MDT Dial-In Information & Agenda: wclc2015.iaslc.org/press-media/ Please hold all questions until the end.
Transcript of Press Conference - International Association for the...
-
Press ConferenceMonday, Sept. 7, 2015
9:45 a.m. 10:45 a.m. MDTDial-In Information & Agenda:
wclc2015.iaslc.org/press-media/Please hold all questions until the end.
-
Lung Cancer Prevention and Screeningat the IASLC 2015 Meeting
Claudia I. Henschke, PhD, MDIcahn School of Medicine at Mount Sinai
New York, NY
-
Lung Cancer Prevention and Screening:IASLC 2015
Screening is a clinical activity that starts with early detection of suspicious findings on CT, followed by early diagnosis of lung cancer with the real benefit coming from the resulting early treatment
requires careful attention to all these details to maximize its benefit and minimize its potential harms Requires continuous evaluation and updating and integration of latest advances to remain state of the art
Screening leads to new definitions and new concepts, several of which have been important, large scale IASLC initiatives
Feature identification of small, early lung cancers and how they differ from non lung cancer findings Refine the pathology definitions of early lung cancers Define new staging criteria for lung cancer Identify and rapidly assess optimal treatments for early lung cancers Develop and test new screening tools Provide alternative study designs and when they should be used for rapid scientific assessment
Randomized trials, cohort studies, modeling
The Institute of Medicine of the US National Academy of Science new recommendations suggest that methodlogy for continuous evaluation and research in the context of delivering high quality screening should be done
Screening evaluation through collection of data in registries provide s a paradigm for such assessment
You will see all these topics addressed throughout the next days of the conference in the context of both cohort and randomized control trials performed over the past 20 years
-
Initial CT Screening Studies Early Lung Cancer Action Program (ELCAP)
1992-1999: Cohort study at 2 institutions in NYC, funded by an R01 from the NCI Compared CT with chest x-ray in a cohort of 1,000 smokers 60 and older, partially
funded by an R01 from the US National Cancer Institute Lancet 1999; 355: 99-105; PI: C. Henschke PhD,MD
Anti-Lung Association Project In Tokyo, Japan 9/1993: added CT as an additional option to the existing CXR screening program at
National Cancer Center Hospital, Tokyo, Japan Reported on the initial cohort of 1,611 smokers and never smokers age 40 and older Radiology 1996; 201: 798-802 PI: M. Kaneko MD
Nagano Population-based Lung Screening 1996-1998: Cohort study in the region using mobile CT scanner Cohort of 5,483 Smokers and never smokers 40 and older Lancet 1998; 251: 1242-5 PI: S. Sone MD
-
1992 1993 1994
Anti-Lung Cancer Association Japan N=1,611
Nagano Population-based lung screening, Japan N=5,483
European Institute of OncologyMilano, Italy N=5,201
I-ELCAP N=70,000+
1995 1998 1999 2000 20011996 1997 2002 2003 2004
Oct04 Oct05
2005 2006
Cohorts: Typically provide ongoing screening and produce continuous reports and updatesThe size of each bar approximates the number of screening participants
20152014..
University of Navarra, Spain
Hadassah Medical University, Israel
I-ELCAP collaborationPOOL data via common protocol72 institutions in 8 countriesN=70,000+
NY-ELCAP
OTHER INSTITUTIONS
ELCAP
Japan has provided national screening for many years, either by chest x-ray or CT; initial 2 reported studies on CT are listed below
-
2000 2001 2002
National Lung Screening TrialN=53,454 (CT arm: 26,722)
NELSONN=15,822 (CT arm: 7,557)
Italian Lung Cancer CT Screening Trial (ITALUNG)N=3,206 (CT arm: 1406)
Danish Lung Cancer Screening Trial (DLCST)N=4,104 (CT arm:2,052)
DANTEN=2,472 (CT arm: 1276)
German Lung Cancer Screening Intervention Study (LUSI)N=4,052 (CT arm: 2,029)
United Kingdom Lung Cancer Screening Trial (UKLS)N=5,201, pilot project
Aug02-Apr04 RESULT IN 2011
Dec03-Jul06 RESULT EXPECTED IN 2016
Oct04-Mar06
Oct07-Apr11 NO RESULT YET
Sep05-Jan11
2003 2006 2007 2008 20092004 2005 2010 2011 2012
2004-2006
2001-2006
2011-ongoing
2013 2014
Multicentric Italian Lung Detection (MILD)N=4,099 (CT arm: 2,376)
Randomized Control Trials: screen for a limited time, results available years laterThe size of each bar approximates the number of screening participants
RESULT 2015
-
Time
Sept 02
Sept 03
Sept 04
Sept 05
Sept 06
Sept 07
Sept 08
Sept 09
Sept 10
Round T2
Round T1
Baseline T0
UNDER SCREENINGFOLLOW-UP
1st subject entered the
study in Aug 02
Enrolled last subject
Apr 04
Study was halted Oct 10
1st subject entered
follow-up period
Last enrolled subject entered
follow-up period
John. E. Niederhuberextended for a critical additional year
Sep 2006 Jul 2010
Harold VarmusStopped and reported results
Jul 2010-Mar 2015
Richard KlausnerR. Wittes,
P. Greenwald
Aug 1999 Sep 2001
NCI Directors
Jan 2002 Jun 2006
Andrew von Eschenbachstarted the NLST
NCI Directors
Lung cancers diagnosed in CT arm:67% by screening
and33% without screening after it stopped
-
National Lung Screening Trial The largest RCT trial on CT screening for lung cancer led
to the acceptance of screening in the US. Achieved its goal to show that CT screening met the stated
mortality reduction threshold of 20% needed to provide national screening
However, it was not designed to measure the full magnitude of its benefit nor to identify who should be screened
Nor could it incorporate the latest advances needed for future implementation of screening Thus its screening process is not state of the art when
screening is to be implemented
-
2013- 2015Development of Insurance Coverage in US
December 2013: USPSTF report recommending screening Thus, private insurance coverage started Jan 2014
Centers for Medicare and Medicaid Services (CMS) Started coverage in Feb 2015, not yet fully implemented
Veterans Administration Will start coverage in 2016
Required additional intensive efforts by advocacy organizations and medical associations Lung Cancer Alliance, L. Fenton, President Prevent Cancer Foundation, C. Aldige, Founder and President American Legacy Foundation, C. Healton, President American College of Radiology, E. Kazerooni, Prof. U of Michigan Society of Thoracic Surgeons, D. Wood, Prof. U of Washington And many others
-
Implementation of Screening Needs contribution from all these efforts
NLST results and ongoing cohort studies provide the needed evidence and state of the art screening
Identification of whom to screen and many other needed considerations
For example, alternative approaches to nodule measurement
Diameter vs. volumetrics Assessment of accuracy of each measurement
Identification of optimum smoking cessation approaches
Use of registries for continued improvement and quality assurance
-
2016 and Beyond:Lung Cancer Prevention and Screening Smoking cessation fully integrated in all screening programs More nimble methodology for assessing new potential
screening tests to existing screening programs Integration of potential screening tests in programs of CT
screening Assessment would be available after 2 rounds of screening
(baseline and first annual repeat) and Thus a useful test could be quickly identified
Collection of biologic samples for future integration in screening for discovery and validation blood, sputum, urine, buccal cells,
If proven to be of value, new tests can rapidly be integrated into screening programs
-
Why is IASLC issuing a new Tobacco Declaration Statement?
Last statement issued nearly a decade ago (i.e., 2008) Much has changed since 2008
In the US, FDA now has authority to regulate tobacco products There has been a rapid evolution in the economics of tobacco in
different regions of the world, the types of tobacco products available to consumers, and tobacco use patterns
Most countries (n=180) have now ratified the WHO Framework Convention on Tobacco Control (FCTC) obligating them to implement evidenced-based policies that create smoke-free environments, cessation programs, warning labels, mass media campaigns, advertising bans, and taxation of tobacco
Press Conference 2 - ISALC Issues New Tobacco Declaration Statement - K. Michael Cummings, PhD, MPH
-
Press Conference 2 - ISALC Issues New Tobacco Declaration Statement - K. Michael Cummings, PhD, MPH
Source: 2013, WHO MPOWER report
Effective implementation of FCTC articles is now the primary focus of global tobacco control efforts
-
What has not changed
Lung cancer remains the leading cause of cancer death worldwide, killing approximately 1.6 million people annually.
At least 80% of lung cancer deaths are attributable to smoking.
-
Source: Globocan, 2012http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx?cancer=lung
Lung Cancer Mortality by Sex in 2012
http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx?cancer=lung
-
Solutions1. Advocate for the forceful implementation of the WHOs Framework Convention on
Tobacco Control, especially higher cigarette prices via taxation (to at least 70% of the retail price);
2. Support legal reforms that hold tobacco manufacturers civilly and criminally accountable for their actions;
3. Support policies that prevent tobacco initiation by youth such as raising the legal age for purchase of tobacco to 21 years;
4. Ensure the provision of evidence based tobacco cessation services to all who use tobacco, including cancer patients as a standard of care;
5. Support policies that address alternative nicotine delivery devices, such as aerosolized nicotine products that are evidence based and promote overall population health
-
Why increase cigarette taxes?
Tripling inflation adjusted specific excise taxes on tobacco would in many low and middle income countries double the price of cigarettes, which in turn would reduce consumption by about 1/3rd.. N Engl J Med, 2014, vol. 370 (1): p60-68.
The Lancet Commission on Investing in Health has identified a substantial increase in specific excise taxes on tobacco as the single most important intervention against noncommunicable diseases. The Lancet, 2013; Vol. 382, No. 9908, p18981955
-
Trade Policies & Tobacco Interference
IASLC also strongly supports keeping tobacco out of trade agreements such as the Trans-Pacific Partnership Agreement (TPP)
IASLC also strongly supports policies that prevent tobacco manufacturers from circumventing the freedom of sovereign nations to enact tobacco control policies that advance public health goals for their citizens (e.g., Australia, Ireland, UK standardized packaging legislation; Uruguays larger product warnings and ban on brand line extensions)
-
Symposium: Regulation of Tobacco Products Monday, September 7: 2:15-3:45pm, Rooms 201 + 203
Taxing tobacco Luk Joossen, Belgium FCTC Geoffrey Fong, Canada FDA regulation of tobacco Mitch Zeller, USA Tobacco litigation Richard Daynard, USA
-
Impact of time to drug approval on potential years of life lost: the compelling need for improved trial and regulatory efficiency. DJ
Stewart et al New anticancer drugs can prolong life expectancy Worldwide, steadily increasing regulatory complexity has:
Driven up the cost of drug development much faster than the rate of inflation, and this contributes directly to high health care costs
Minimal demonstrable impact on clinical trials safety Slows progress, leading to increased suffering & premature death
Accelerated Approval, Breakthrough Drug Designation, etc: Cut time to drug approval substantially (& this is important) But predominantly just remove the requirement for phase III trials Dont fix the escalating burden of clinical research bureaucracy Would be expected to have progressively less beneficial effect unless the clinical
research bureaucracy is fixed: Shorter distance to the goal posts, but the mud on the way to these closer
goal posts keeps getting deeper
-
Method: Illustrative examples:
21 drugs that significantly prolonged survival in incurable malignancies in phase III trials published 2000-2015
Calculated life-years lost due to delays in drug approval Results: Cumulatively, worldwide:
Median of 12 years from drug discovery to approval 2,541,274 life-years lost per year of delay (1 every 12 seconds) 31,537,958 life-years lost from drug discovery until approval 19,355,028 life-years would have been saved by reducing time from
discovery to approval to 5 years Enhanced safety through more stringent clinical research regulation
estimated to have saved
-
Conclusions Huge number of life-years unnecessarily lost Even if only 1-10% of patients had drug access, losses still enormous Does not take into account added effect of:
Drugs abandoned prematurely Drugs that cant be accessed since high cost / no payer Ultimate impact of massive research costs on high health care costs
Accelerated Approval & Breakthrough Drug Designation, etc help, but we mustdo much more: Every additional step to further cut time to drug approval saves lives
There are solutions! (eg, Stewart et al: Clin Cancer Res 21:2015 In Press; J PopulTher Clin Pharm 21:e56, 2014; BMC Cancer 13:193, 2013; J Clin Oncol 28:2925, 2010; J Clin Oncol 27:328, 2009)
We all share the blame: investigators, research staff, institutions, IRBs, sponsors, CROs, regulators, tort systems, the press
We all share responsibility to solve this
It is time to act!www.lifesavingtherapies.com [email protected]
-
Change in Lean Body Mass and Hand Grip Strength over 12 weeks
Primary Endpoints, Median (95% CI)
ROMANA 1 ROMANA 2
Placebo(N = 161)
ANAM 100 mg(N = 323) p Value
Placebo(N = 165)
ANAM 100 mg(N = 330) p Value
Lean body mass, kg -0.44 (-0.88, 0.20)1.10
(0.75, 1.42)
-
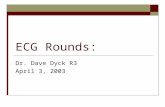
Change in FAACT Anorexia/Cachexia Domain over 12 weeks
Modified intent-to-treat population: All randomized patients who received any study drug and had at least 1 post-baseline lean body mass or hand grip strength measurement.ANAM: anamorelin HCl ; FAACT: Functional Assessment of Anorexia/Cachexia Therapy.
0
1
2
3
4
5
Mea
n ch
ange
fr
om b
asel
ine
Improving
N = 282N = 141
N = 133 N = 266
3.48
4.12
1.34
1.92
FAACT Anorexia/Cachexia Domain
I have a good appetite The amount I eat is sufficient to meet my needs I am worried about my weightMost food tastes unpleasant to meI am concerned about how thin I lookMy interest in food drops as soon as I try to eatI have difficulty eating rich or heavy foodsMy family or friends are pressuring me to eat I have been vomitingWhen I eat, I seem to get full quicklyI have pain in my stomach areaMy general health is improving
Placebo
ANAM
ROMANA 1
ROMANA 2
p=0.0004
p=0.0016
Chart1
000000
Placebo
ANAM
Mean change from baseline
-
Conclusions In NSCLC patients, ANAM treatment significantly improved LBM and BW compared
with placebo in ROMANA 1 and 2 Pre-specified exploratory responder analysis showed that approximately twice as many
ANAM-treated patients maintained or gained LBM compared with placebo
No significant difference in HGS change between ANAM and placebo arms was observed
ANAM significantly improved anorexia-cachexia symptoms in patients with advanced NSCLC and cachexia
Daily ANAM administration over 12 weeks was well tolerated Pooled median 1-year OS was similar between the two treatment arms, although
analysis by LBM responders revealed median 1-year OS was significantly improved in patients who maintain/gain LBM compared with those who lose LBM
ROMANA 1 and ROMANA 2 results concur, underlining the consistency between these two independent phase III clinical trials
ANAM: anamorelin HCl; BW: body weight; HGS: hand grip strength; LBM: lean body mass; NSCLC: non-small cell lung cancer; OS: overall survival.
-
Arnaud SCHERPEREEL*1, Julien MAZIERES, Jacques MARGERY, Laurent GREILLER, Clarisse AUDIGIER-VALETTE, Denis MORO-SIBILOT, Olivier MOLINIER, Romain CORRE, Isabelle MONNET, Valrie GOUNANT, Henri JANICOT, Radj GERVAIS, Chrystle LOCHER, Bernard MILLERON, Quan
TRAN, Marie-Paule LEBITASY, Franck MORIN, Christian CREVEUIL, Jean-Jacques PARIENTI & Grard ZALCMAN*,
on behalf of the French Cooperative Thoracic Intergroup (IFCT) *PI; 1Hospital of the University (CHRU) of LILLE, FRANCE [email protected]
Results of the IFCT-GFPC 0701 MAPS randomizedphase 3 trial: Bevacizumab 15mg/kg plus cisplatin
-pemetrexed (CP) triplet versus CP doublet in Malignant Pleural Mesothelioma (MPM)
EUDRACT N : 2007-002574-63 - ClinicalTrials.gov : NCT00651456
MPM: an aggressive cancer originating from parietal pleura with NO validated curative treatment (mOS
-
MPM proved by pleural biopsies (thoracoscopy...)
Written informed consent
Age 18 -
-
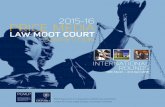
IFCT 0701 MAPS randomized phase 3 trial
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 10 20 30 40 50 60Time (months)
Arm A (PC; n=225): 7.48 mo, 95%CI [6.79-8.13]Arm B (PCB; n=223): 9.59 mo [8.49-10.59]
stratified HR=0.61 [0.50-0.75]; p
-
Conclusions - MAPS randomized phase 3 trial Adding bevacizumab 15 mg/kg to pemetrexedcisplatin doublet significantly
increased both PFS (by 2 months) and OS (by 2.75 months) with only a slight,manageable increase of toxicity (G3-4: 62 vs 71% of cases; p=0.04)
=> Therefore the triplet pemetrexed, cisplatin and bevacizumabis a new treatment paradigm for MPM patients eligible
for bevacizumab, and not candidate to curative surgery +++
Moreover, bevacizumab did not show a detrimental effect on QoL, despite itshigher specific non-hematological toxicity (HTA, arterial/venous thrombo-embolic events ...)
No significant difference between arms for %drug delivery or %2nd line treatment In this study, standard arm patients (P+C) had a longer OS than patients from
historical series or previous trials: role of eligibility criteria for bevacizumab? Talcpleurodesis?... But this was true for both arms and still beva arm did better !!!
No predictive clinical/biological marker found yet but other ongoing studies
-
Biomarkers ancillary studiesG. LEVALLET, E. CHEVALLIER, S. BROSSEAU, G. ZALCMAN (Caen)
A. SCHERPEREEL (Lille)
Programme Hospitalier de Recherche Clinique (PHRC) National 2007Statistical Group
F. CHAILLOT C. CREVEUILA.D. PHAM JJ PARIENTI
Clinical Research UnitB. MILLERON, A LANGLAIS, F. MORIN E. AMOUR, Q.TRAN & M.P. LEBITASY
ROCHE-France: Drug supplying Research grant on biomarkers
-
Q & A
Press ConferenceSlide Number 2Lung Cancer Prevention and Screening:IASLC 2015 Initial CT Screening Studies Slide Number 5Slide Number 6Slide Number 7Slide Number 8Slide Number 9Slide Number 10Slide Number 11Slide Number 12Slide Number 13Slide Number 14Slide Number 15Slide Number 16Slide Number 17Slide Number 18Slide Number 19Slide Number 20Slide Number 21Slide Number 22ConclusionsSlide Number 24Slide Number 25Slide Number 26Slide Number 27Slide Number 28Slide Number 29Conclusions - MAPS randomized phase 3 trialSlide Number 31Q & A