EKG rounds
25
EKG rounds Rebecca Burton-MacLeod R5, Emerg Med Dec 13 th , 2007
-
Upload
clayton-ayala -
Category
Documents
-
view
61 -
download
1
description
EKG rounds. Rebecca Burton-MacLeod R5, Emerg Med Dec 13 th , 2007. Case. 67y Caucasian F presents to ED c/o exertional SOB Worsening over last 8d No other assoc symptoms PMHx: HTN, DM, hyperlipidemia O/e: HR 88 BP 140/85 RR 20 sats 96% Nil acute on examination. Case cont’d. - PowerPoint PPT Presentation
Transcript of EKG rounds
EKG rounds
Rebecca Burton-MacLeod
R5, Emerg Med
Dec 13th, 2007
Case
• 67y Caucasian F presents to ED c/o exertional SOB
• Worsening over last 8d
• No other assoc symptoms
• PMHx: HTN, DM, hyperlipidemia
• O/e: HR 88 BP 140/85 RR 20 sats 96%
• Nil acute on examination
Case cont’d
• Any investigations?
• PS. Don’t forget…this is “EKG rounds”…
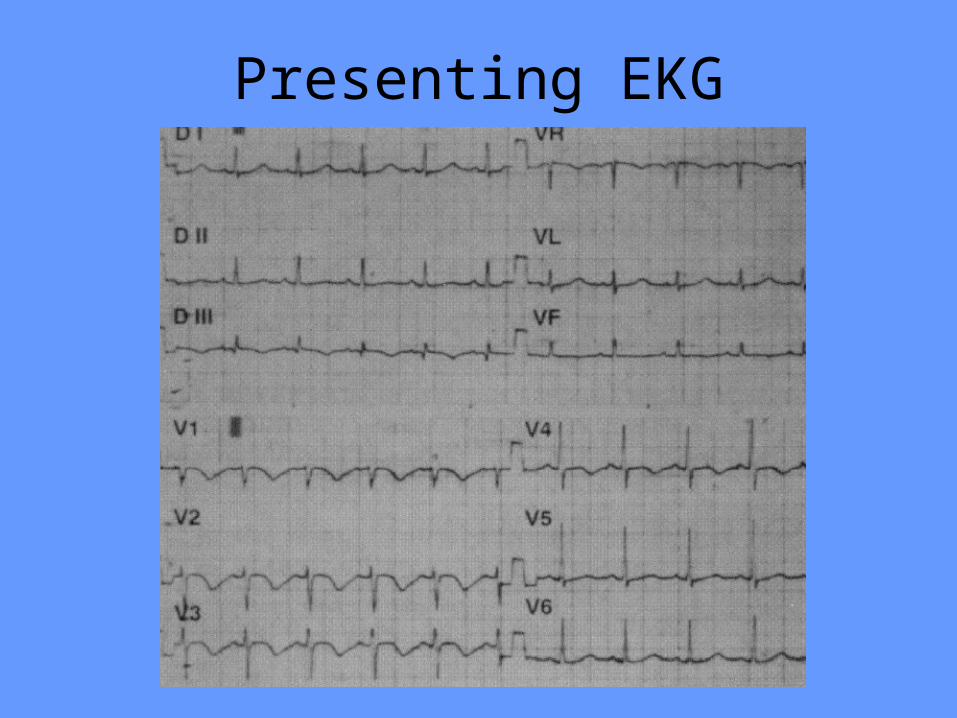
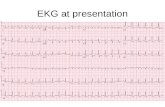
Presenting EKG
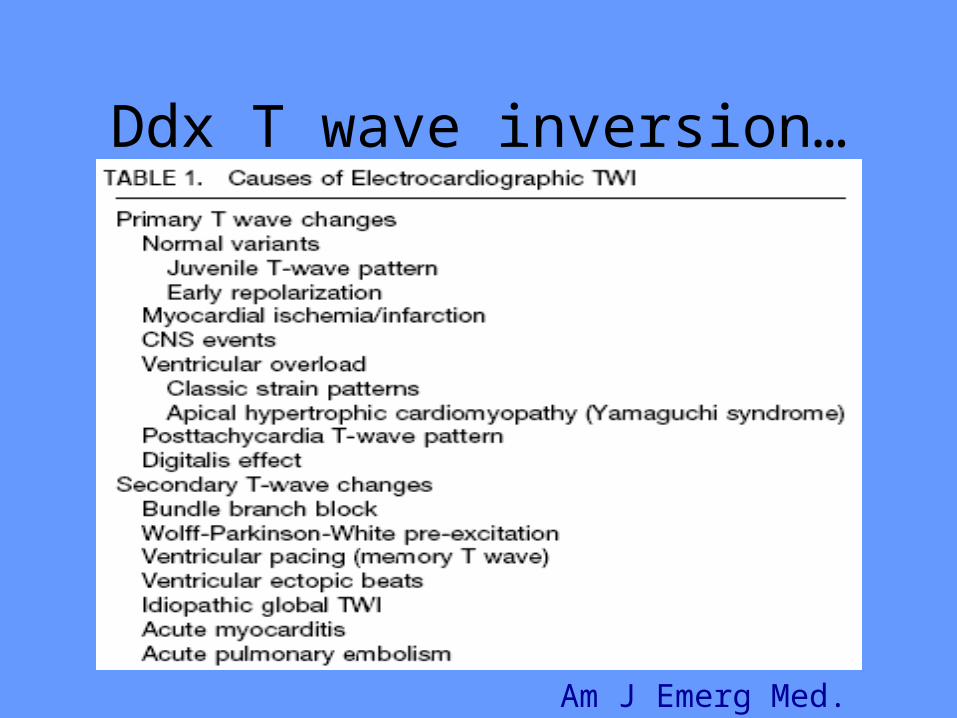
Ddx T wave inversion…
Am J Emerg Med. 2002.
Case cont’d
• Blwk:– TNT normal– D-dimer 3.27
• Investigations:– Echo: RV systolic dysfxn, mod-severe pulm
hypertension– CT confirmed PE
PE and EKG findings
• Classic findings:– Sinus tachycardia– S1Q3T3– Rt heart strain
Why T inversion with PE ?
• Possible mechanisms: – Due to acute cor pulmonale from RV
enlargement and RV ischemia– Other factors such as hypoxemia and chemical
mediator release in RV may lead to T wave inversion
• T inversion occurs in 42-89% of acute PE cases
• N=80 pts hospitalized for PE
• Analysis of admission EKG’s and those during course of hospitalization
• T wave inversion is most common abnormality (68%) and best correlates to severity of PE
Chest. 1997.
• Retrospective cohort study of pts with PE and age- and sex-matched controls (n=98)
• All pts had CT PE done (no d-dimers available at that time in their institute)
• All EKG reviewed by 2 cardiologists
• ?discrete EKG findings for ED pts to rule-in vs. rule-out PE?
J Emerg Med. 2004.
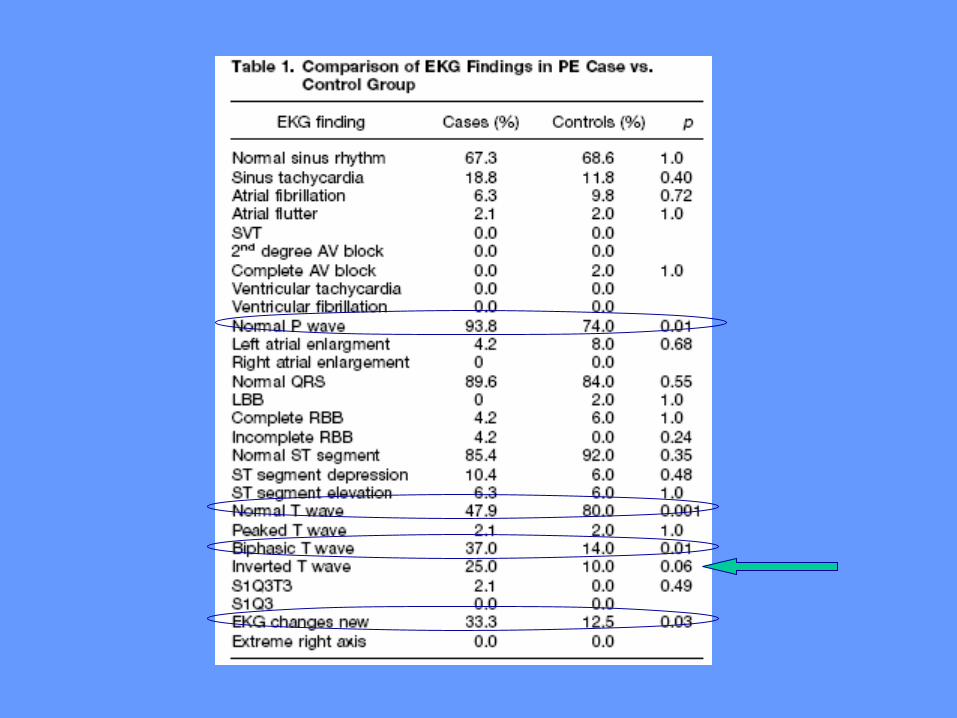
EKG and PE
• Kappa values were calculated for each EKG finding and varied from 0.14 to 1.0
• For normal T waves (k=0.17) and biphasic T waves (k=0.14)
• Conclusion: no EKG findings specific or sensitive enough to help dx PE in ED.
• N=40 consecutive pts with PE and 87 consecutive pts with ACS
• All pts had negative T waves >=1mm in 2+ contiguous precordial leads (V1-4)
• Exclusion criteria: ST elevation>=2mm on 2+ precordial leads, Q wave MI, conditions precluding evaluation of ST segments, hx cardiopulmonary disease
• Dx of PE made with pulm angio, V/Q, or spiral CT• Dx of ACS made with cardiac cath
Am J Cardiol. 2007.
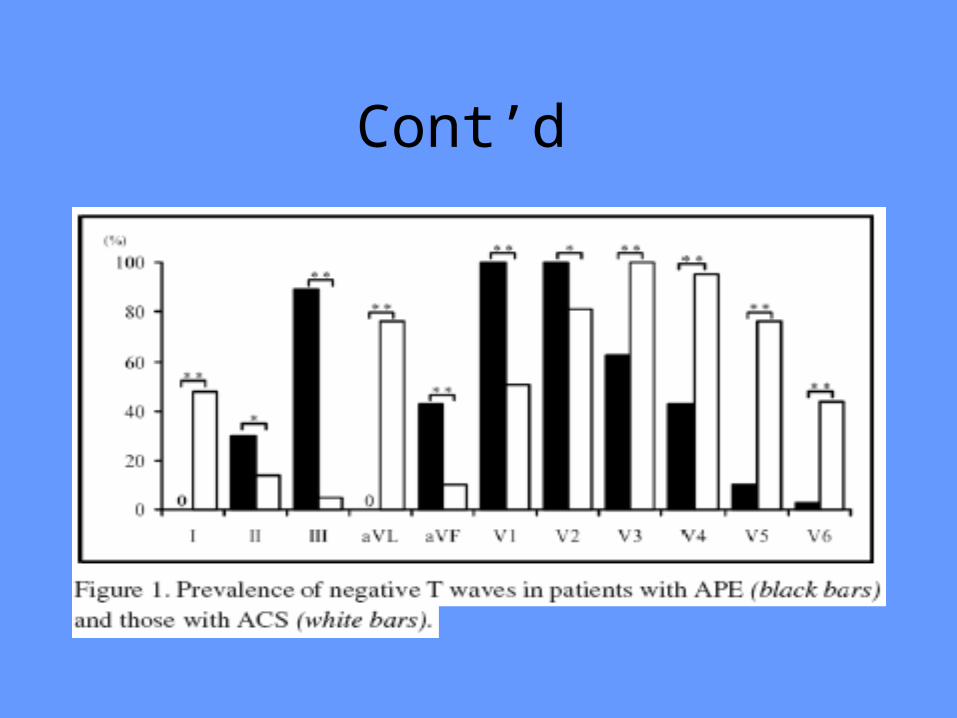
Cont’d
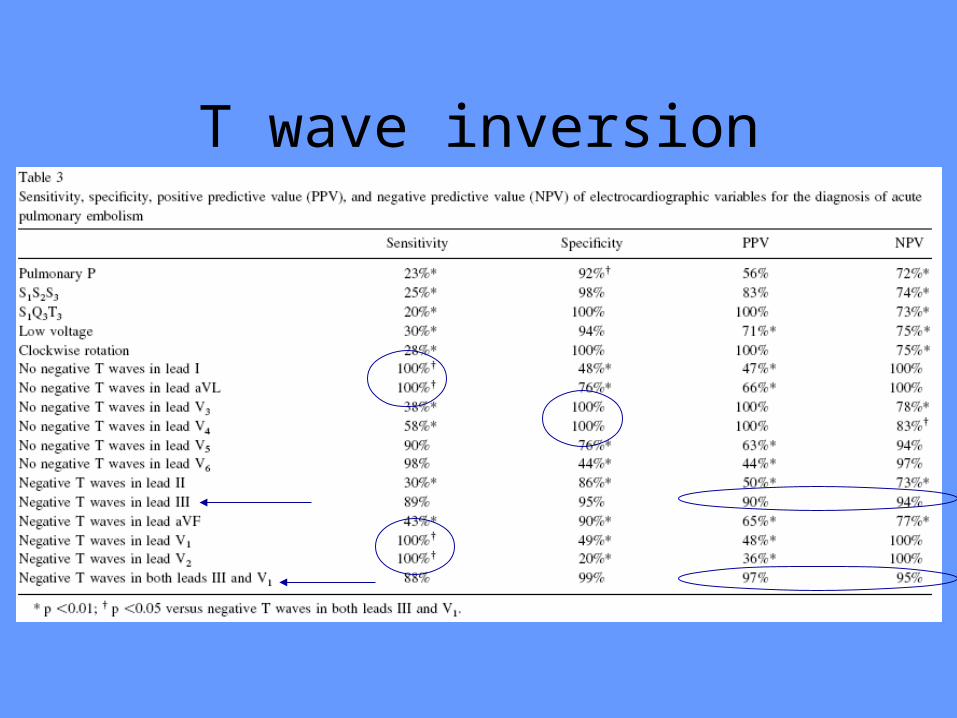
T wave inversion
Conclusions
• Combination of T inversion in V1 and III was more sensitive and specific for PE and rarely found in ACS (1%)
""Excuse me. ... I Excuse me. ... I
know the game's know the game's almost over; but almost over; but just for the record, just for the record, I don't think my I don't think my buzzer was buzzer was working properlyworking properly..
by Gary Larsonby Gary Larson
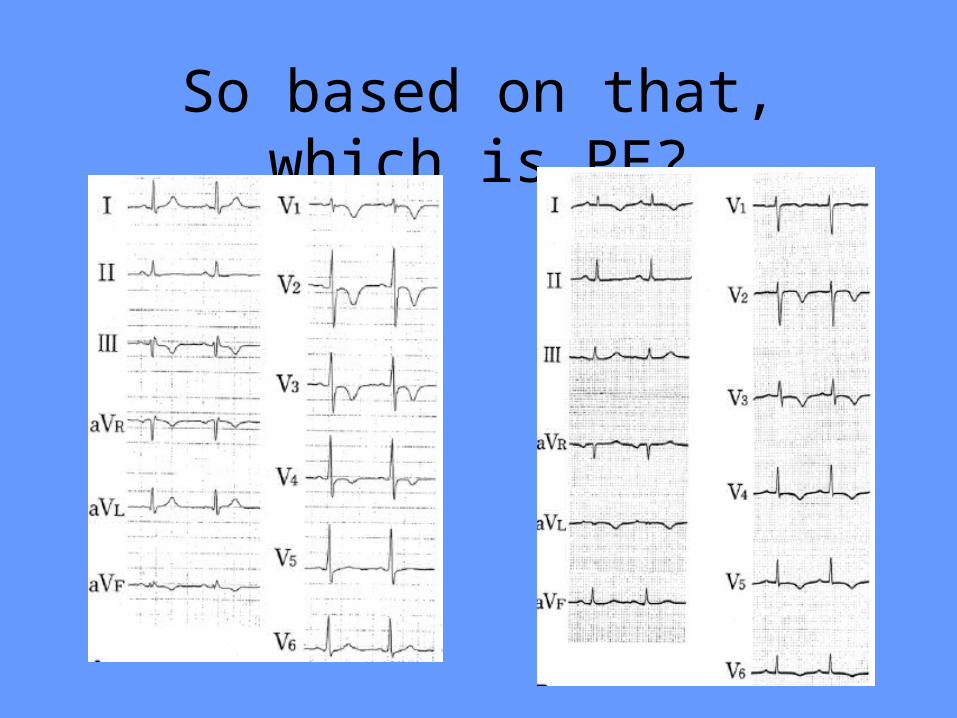
So based on that, which is PE?
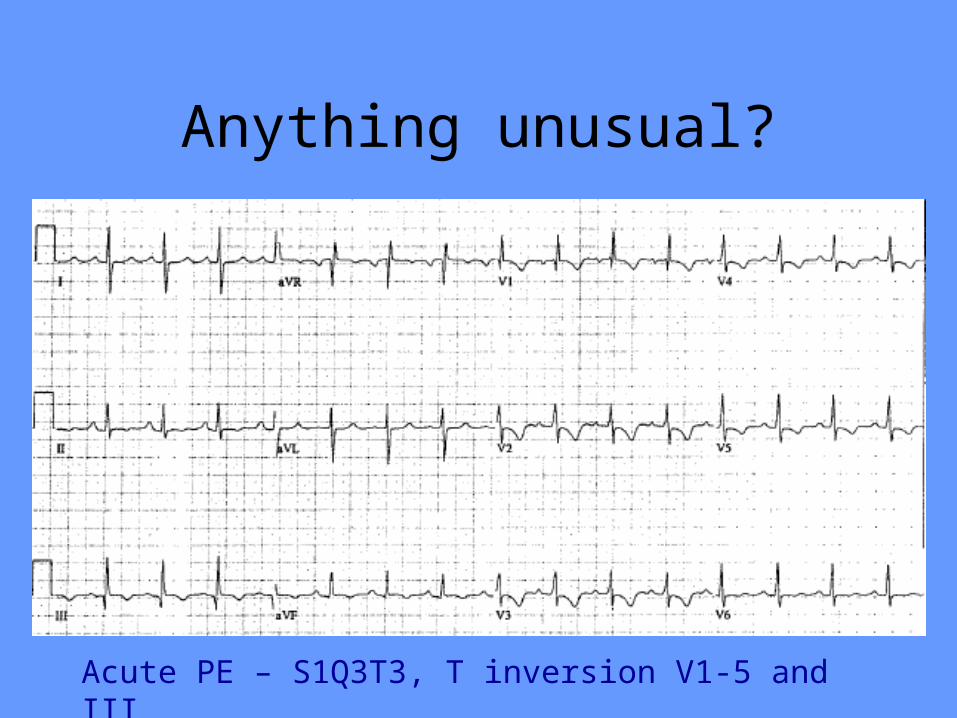
Anything unusual?
Acute PE – S1Q3T3, T inversion V1-5 and III
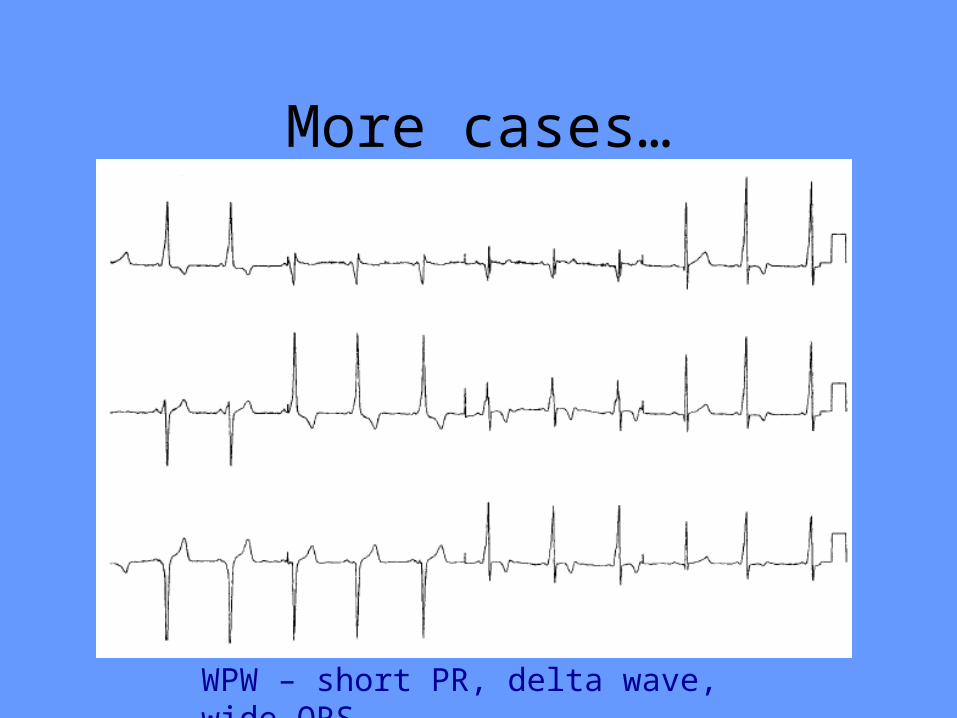
More cases…
WPW – short PR, delta wave, wide QRS
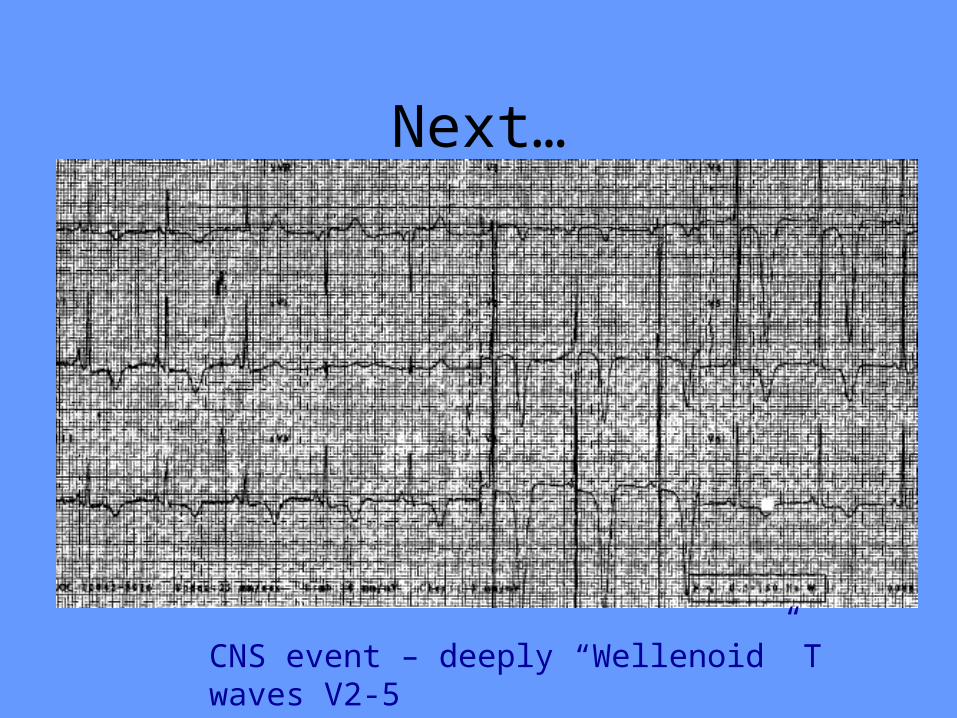
Next…
CNS event – deeply “Wellenoid” T waves V2-5
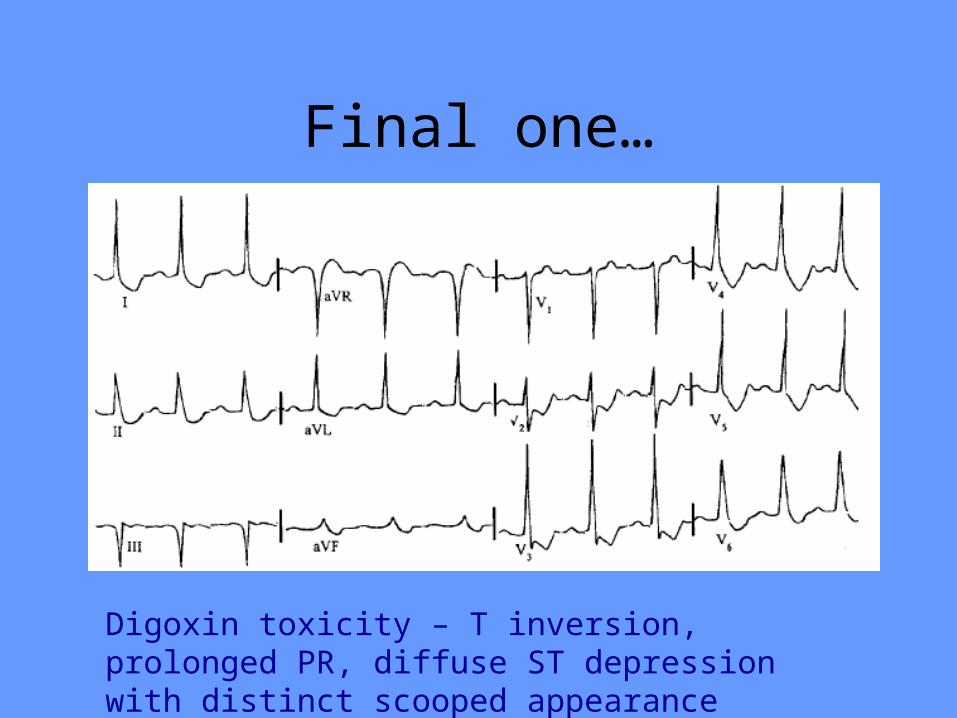
Final one…
Digoxin toxicity – T inversion, prolonged PR, diffuse ST depression with distinct scooped appearance
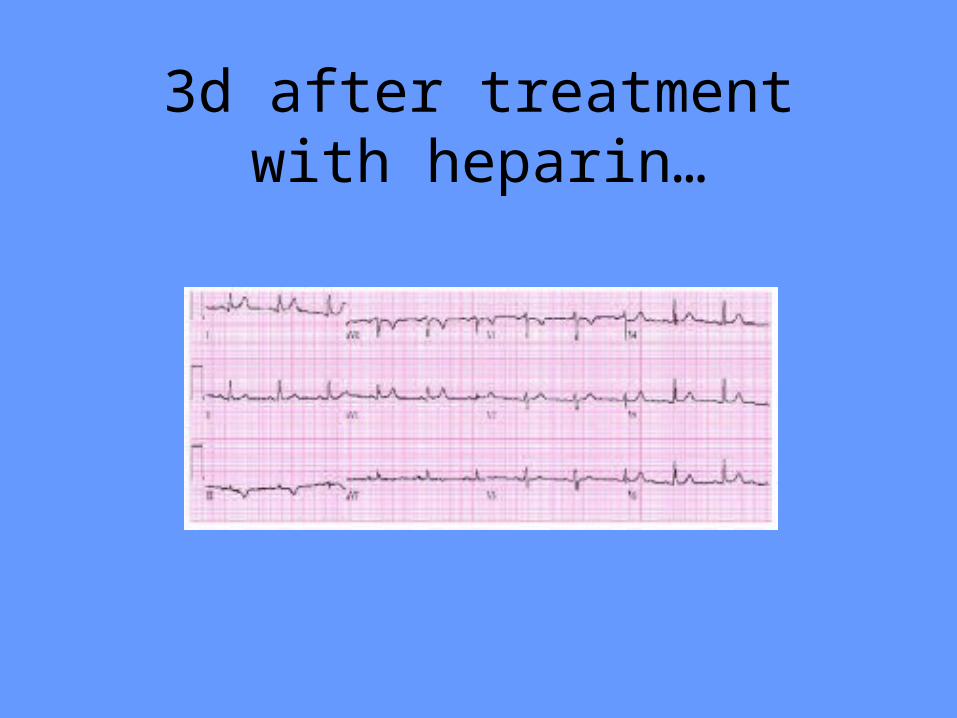
3d after treatment with heparin…
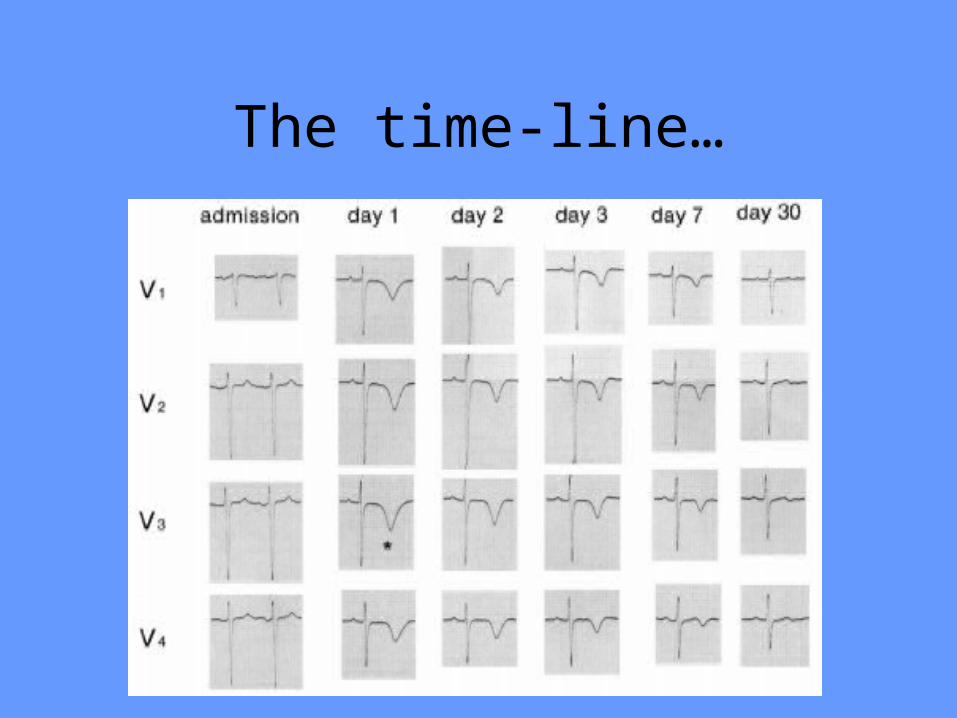
The time-line…
Questions ?