![Schmitz v. Natl. Collegiate Athletic Assn. · [Cite as Schmitz v. Natl. Collegiate Athletic Assn., 2016-Ohio-8041.] Court of Appeals of Ohio EIGHTH APPELLATE DISTRICT COUNTY OF CUYAHOGA](https://static.fdocuments.us/doc/165x107/5af904d67f8b9ad2208d5a99/schmitz-v-natl-collegiate-athletic-assn-cite-as-schmitz-v-natl-collegiate-athletic.jpg)
PRESCRIPTION DRUG OVERDOSE EPIDEMIC: … · o Ohio ACEP o Ohio State Medical Assn. o Ohio Hospital...
34
RESPONSE TO OHIO’S PRESCRIPTION DRUG OVERDOSE EPIDEMIC: PRESCRIBING GUIDELINES Ohio Department of Health MIPA CONFERENCE PREVENTING INJURY: FROM RESEARCH TO PRACTICE TO PEOPLE SEPTEMBER 30, 2013 Christy Beeghly, MPH Program Administrator Violence and Injury Prevention Program Ohio Department of Health
Transcript of PRESCRIPTION DRUG OVERDOSE EPIDEMIC: … · o Ohio ACEP o Ohio State Medical Assn. o Ohio Hospital...

RESPONSE TO OHIO’S
PRESCRIPTION DRUG
OVERDOSE EPIDEMIC:
PRESCRIBING GUIDELINES
Ohio Department of Health
MIPA CONFERENCE
PREVENTING INJURY: FROM RESEARCH TO PRACTICE TO PEOPLE
SEPTEMBER 30, 2013
Christy Beeghly, MPH
Program Administrator
Violence and Injury Prevention Program
Ohio Department of Health

OVERVIEW
• Ohio Emergency and Acute Care
Facility Opioid and Other Controlled
Substances Prescribing Guidelines
• 80 MED “Trigger Point” Opioid
Prescribing Guidelines
Ohio Department of Health 2

327 411
555
702 658
904
1,020
1,261 1,351
1,475 1,423
1,544
1,765
0
2
4
6
8
10
12
14
16
0
300
600
900
1200
1500
1800
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
Death
rate
per
100,0
00
Nu
mb
er
of
dru
g o
ve
rdo
se d
eath
s
Year
Death Rate per 100,000
Number of Deaths
OHIO DEATHS AND DEATH RATES PER 100,000 DUE TO
UNINTENTIONAL DRUG OVERDOSE BY YEAR, 1999-20111
1Source: ODH Office of Vital Statistics, 3
The number of drug overdose
deaths in Ohio increased
440% from 1999-2011.
~5
deaths
per day
~1 per
day

Unintentional drug overdose deaths of Ohio residents by
specific drug(s) involved, by year, 2000-20111,2
4 2Multiple substances are usually involved in one death.
Still more deaths from prescription opioids than
from cocaine, heroin, and marijuana combined.
138 199
257 221
319
388
462 508
546 550
694
789
-
100
200
300
400
500
600
700
800
900
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
Nu
mb
er
of
death
s
Year
cocaine
benzodiazepines
heroin
prescription opioids
Ohio Department of Health

OHIO DATA
5
There is a strong relationship between increases in exposure
to prescription opioids and fatal unintentional overdose rates.
Sources: 1. Ohio Vital Statistics; 2. DEA, ARCOS Reports, Retail Drug Summary Reports by State, Cumulative Distribution Reports (Report 4) Ohio, 1997-2007
http://www.deadiversion.usdoj.gov/arcos/retail_drug_summary/index.html; 3. Calculation of oral morphine equivalents used the following assumptions: (1) All drugs
other than fentanyl are taken orally; fentanyl is applied transdermally. 2) These doses are approximately equianalgesic: morphine: 30 mg; codeine 200 mg; oxycodone
and hydrocodone: 30 mg; hydromorphone; 7.5 mg; methadone: 4 mg; fentanyl: 0.4 mg; meperidine: 300 mg ; 4. US Census Bureau, Ohio population estimates 1997-
2007; 5. preliminary data for 2007
Drugs distributed – 643% increase
Death rate – 365% increase
CONTRIBUTING FACTORS:
-
2
4
6
8
10
12
14
16
-
20,000
40,000
60,000
80,000
100,000
1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
de
ath
ra
te p
er
10
0,0
00
op
ioid
s d
istr
ibu
ted
in
gra
ms
p
er
100,0
00 p
op
ula
tio
n
Year
Unintentional drug overdose death rates and distribution rates of prescription opioids in grams per 100,000 population by year, Ohio,
1997-20111-3
Total Rx Opioid Grams (MME)per 100,000
Unintentional overdose deathrate
Ohio Department of Health

STATE
RESPONSE TO
EPIDEMIC
6
Ohio Department of Health
STATE LEGISLATION
HB 93 addresses (Became law April 2011):
• Pain management clinic licensure (i.e., Pill mills)
and related changes
• Sets In-office physician dispensing limits
• Medicaid and Bureau of Workers’ Comp Lock-in
Programs
• Required changes to OARRS rules (Ohio’s PMP)
7
Link to Bill Analysis:
http://www.lsc.state.oh.us/analyses129/11-hb93-129.pdf

GOVERNOR’S CABINET
OPIATE ACTION TEAM
(GCOAT)
Established fall of 2011 to address the continuing
epidemic of misuse, abuse and overdose from
prescription opioids.
Five work groups:
1. Treatment – includes Medication Assisted Treatment
2. Professional Education
3. Public Education
4. Enforcement
5. Recovery Supports
8
Professional Education
Workgroup

GCOAT PROFESSIONAL
EDUCATION WORKGROUP
Co-Chaired by
• Ted Wymyslo, M.D., Director, Ohio Department of Health
• Bonnie Kantor-Burman, Director, Ohio Department of Aging
Two subcommittees formed:
• Opioid Prescribing Guidelines for Ohio Emergency/Acute Care Facilities - Lead: Director Wymyslo
• Reforming Prescribing Practices in Ohio– Lead: Director Kantor-Burman
9
Professional Education
Workgroup

OHIO EMERGENCY AND ACUTE
CARE FACILITY OPIOID AND OTHER
CONTROLLED SUBSTANCES
PRESCRIBING GUIDELINES
(ED GUIDELINES)
PROFESSIONAL EDUCATION
WORKGROUP: INITIATIVE #1
10
Ohio Department of Health
Professional Education
Workgroup

11
Professional Education
Workgroup
Ohio Process
o ED treatment of pain is frequently indicated without the benefit of an
established doctor-patient relationship and often in an environment of
limited resources. Closure of pill mills may lead to increased doctor
shopping in EDs.
o Active ED Physicians brought this issue to the PEW and requested
action.
o Based project on Washington State ED Guidelines.
OPIOID PRESCRIBING
GUIDELINES FOR E.D.s &
URGENT CARE FACILITIES

o Ohio ACEP
o Ohio State Medical Assn.
o Ohio Hospital Assn.
o Urgent Care Facilities
o Ohio Pharmacists Assn.
o Ohio Osteopathic Assn.
o Ohio Association of PAs
o Ohio ENA
o Ohio BWC
o Ohio Medicaid
o Ohio Assn. of Health Plans
o State Medical Board
o Board of Pharmacy
12
Professional Education
Workgroup
Consensus-based process developed in partnership with key
medical/health care organizations as members of the work group:
OPIOID PRESCRIBING
GUIDELINES FOR E.D.s &
URGENT CARE FACILITIES
Ohio Process

OPIOID PRESCRIBING
GUIDELINES FOR ED’S & ACUTE
CARE FACILITIES
GUIDELINES
PATIENT HANDOUT
Ohio Opiate Action Team – Public Education Work Group 13
Professional Education
Workgroup
OPIOID
PRESCRIBING
GUIDELINES FOR
E.D.’S & ACUTE
CARE FACILITIES
POCKET CARDS
14
Professional Education
Workgroup
Distributed in partnership with the Ohio Hospital Association and the Ohio
Chapter, American College of Emergency Physicians, and upon request.

ED GUIDELINES:
SUPPORTING MATERIALS
Background document
Patient Handout
Pocket Cards
Sample Tools
• Discharge Instructions
• SBIRT resources
• Pain Agreement
Frequently Asked Questions
Promotional materials:
• Introductory Letter for
Professional Organizations
• Facebook Posts
• Website Content
• Press Release template
• Newsletter Article
15
Professional
Education Workgroup
16
Professional Education
Workgroup
o Pubic announcement and press
conference in May 2012 at Ohio Opiate
Summit
o Promotion through:
o Endorsing organizations and committee
members
o Health care association communications
(e.g., websites, newsletters, webinars, etc.)
o Pocket card mailing
o Continuing education courses
o Media and social networking sites
o Organization press releases
o April 16, 2013 Webinar on Lessons
Learned in Implementing EDGs.
DISSEMINATION &
PROMOTION…
SOME OF THE OHIO
HOSPITAL SYSTEMS ADOPTING
THE ED GUIDELINES
Ohio Opiate Action Team – Public Education Work Group 17
Professional Education
Workgroup

EVALUATION OF
GUIDELINES
• Follow-up evaluation survey on implementation and
impact of the ED Guidelines planned:
• Process evaluation among ED administrators and ED physicians.
• Assess implementation, use and any reported prescribing
behavior change based on guidelines.
• Assess any changes made to ED Guidelines when implementing.
• Surveys developed and to be implemented in conjunction
with OHA and Ohio ACEP.
• Tracking OARRS (Ohio PMP data)
Ohio Department of Health 18
Professional Education
Workgroup

80MG MED OPIOID
“TRIGGER POINT”
GUIDELINES
PROFESSIONAL EDUCATION
WORKGROUP: INITIATIVE #2
19
Ohio Department of Health
Professional Education
Workgroup

THE GOALS
• Reduce the misuse and abuse of prescription opioids
in Ohio by:
• Establishing a “trigger point” for re-assessment and “pressing
pause” in opioid prescribing.
• Develop and implement guidelines for all prescribers of
opioids for chronic, non-terminal pain.
• Actively promote registration and use of OARRS.
20
REFORMING PRESCRIBING
PRACTICES COMMITTEE Professional Education
Workgroup
THE GOALS

REFORMING PRESCRIBING
PRACTICES COMMITTEE
Consensus Process with Key Stakeholders:
• Professional licensing boards
• State agencies (ODH, OhioMHAS, ODA, Medicaid,
BWC etc.)
• State professional associations
• Practicing pain and palliative care professionals
• State and federal public health agencies
Ohio Department of Health 21
Professional Education
Workgroup
REFORMING PRESCRIBING
PRACTICES COMMITTEE
• 80mg morphine equivalent daily dose (MED) for 3
consecutive months established as “trigger point” based
on CDC expertise and research studies finding:
• Increased mortality rates at 50-100+mg morphine
equivalent daily dose (MED).
• Other adverse effects for long-term use of high MEDs
for chronic, non-terminal (CNT) pain.
• Limited evidence on effectiveness of opioids for long-
term treatment of CNT pain.
• In 2011, over 50% of Ohio prescribers saw a patient with
an MED >80mg.
Ohio Department of Health 22
Professional Education
Workgroup
80 MED TRIGGER POINT
ACTION STEPS:
• 80 MED for 3 months is established “trigger point” at which
prescriber should “press pause” and consider the following action
steps:
• Re-establish informed consent
• Review patient’s functional status
• Review progress toward treatment objectives to determine
benefit of opioid therapy
• Re-check OARRS
• Consider a patient pain agreement
• Consider referral to a pain or other appropriate specialist
• OARRS data needed to determine MEDs.
Ohio Department of Health 23
Professional Education
Workgroup

CHANGES TO
OARRS REPORTS


OHIO OPIOID
TRIGGER
GUIDELINES
Officially Approved by:
• State Medical Board of Ohio
• Ohio State Dental Board
• Ohio Board of Nursing
• Ohio State Board of
Optometry
• Ohio Board of Pharmacy
http://www.med.ohio.gov/pdf/NEWS
/Prescribing%20Opioids%20Guidlin
es.pdf
Ohio Department of Health 28

SUPPORTIVE MATERIALS
• Education committee created a 1-hour CME training video
which will be available online:
• Scope of the problem – Director of Health
• Clinical guidelines – State Medical Board Representative
• Action steps – Pain Management Specialist
• Metrics & conclusion – Addiction Medicine Specialist
• Letter to describe guideline and changes to OARRS report for:
• Prescribers
• Pharmacists
• Patients
Ohio Department of Health 29
Professional Education
Workgroup

EDUCATIONAL
PACKET
OHIO STATE BOARD OF PHARMACY 77 South High Street, Room 1702; Columbus, Ohio 43215-6126
-Equal Opportunity Employer and Service Provider-
PHONE: 614/466-4143 FAX: 614/752-4836 E-MAIL: [email protected]
TTY/TDD: Use the Ohio Relay Service: 1-800/750-0750 URL: http://www.pharmacy.ohio.gov
September 12, 2013
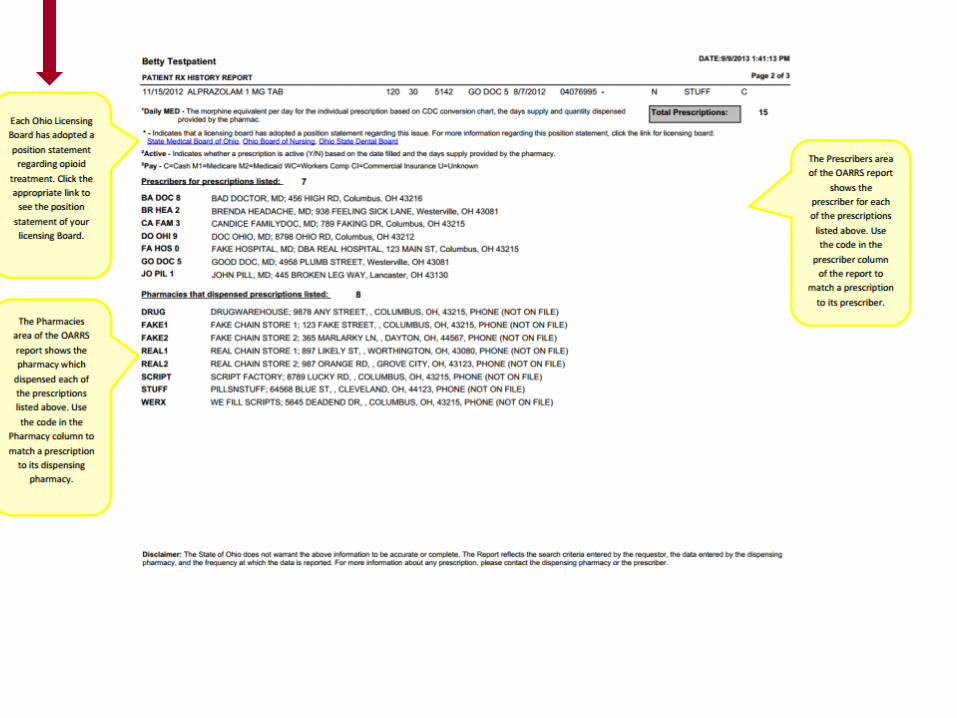
Attention Pharmacists: Major change in the O.A.R.R.S. report to address the “M.E.D.”
Ohio initiative
This letter is intended to educate you on the “M.E.D.” initiative which was created to curtail
the prescription drug epidemic and rising overdose death rates from opiates and
combinations therein. M.E.D. stands for morphine equivalency dosing. This is essentially
a system to equate different opiates and potencies into a standard morphine equivalent
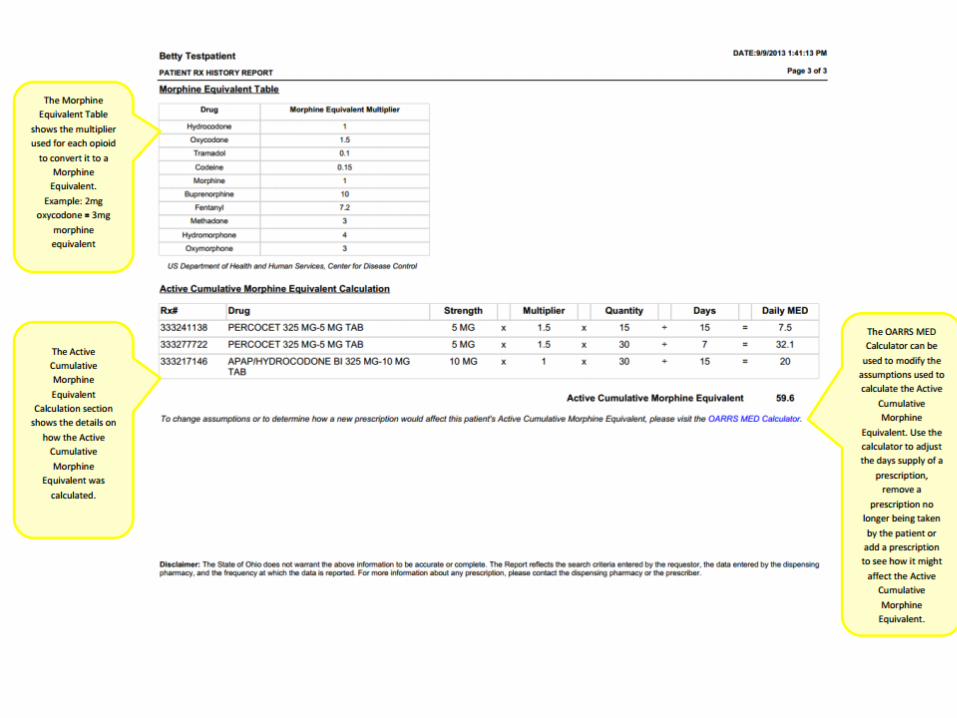
value via a conversion chart created by the Centers for Disease Control (CDC). This chart
will be located on the last page of the new O.A.R.R.S. report. Each active opiate
prescription (identified by having days supply remaining), will have a daily M.E.D. value. All
active (concurrent) prescription values are then combined into one daily “M.E.D.” value,
which will be bolded and located on the upper right portion of the O.A.R.R.S report. It is
important to note that this value is a snapshot of the day when you run the report. It is
not a “90 day average”. This could mean that something may not show up on the report
(due to lag in report time to O.A.R.R.S versus the fill date) or that tomorrow the score may
lower due to “active” prescriptions running out the next day. These are scenarios that you
should understand when viewing this M.E.D. value.
Where did the “80” M.E.D. threshold recommendation come from? The threshold of equal
to or greater than 80 M.E.D. was identified by a team of pain management physicians and
specialists that were convened by the Governor’s office. For a specific example, #16, 5mg
Hydrocodone tablets taken in one day would equate to a M.E.D. value of exactly 80.
However, be aware that normal dosing (Oxycontin 40mg twice daily) may also generate a
value of 80 M.E.D. for that prescription.
At 80 M.E.D., it was deemed that prescribers should “press pause” before prescribing the
opiate. This includes a number of clinical considerations that the prescriber should take
into account prior to issuing the prescription, as specified in the Medical Board’s
statement on this issue. This can be viewed via the link
at http://www.med.ohio.gov/pdf/NEWS/Prescribing%20Opioids%20Guidlines.pdf. That is
all that is required. If a patient’s M.E.D. value is greater than 80, it does NOT preclude
the prescriber from issuing or the pharmacist from filling the prescription, just that
you should “press pause”, making sure that your patient absolutely requires this
treatment. For pharmacists, things to consider when pressing pause may include: review
of the O.A.R.R.S. report, review of the drug profile in your system, prior knowledge of this
patient and physician, and professional judgement. Remember that this is a tool, not a
definitive number to determine whether you fill or do not fill the prescription. However, if
after review of the OARRS report you suspect a legitimacy issue, do not fill the prescription
and notify us of your concern. There are a number of nice additions to the O.A.R.R.S.
report that have been added to assist you. Please see the following O.A.R.R.S. report
example with explanations for each section.
Kyle Parker, M.B.A, R.Ph Executive Director Ohio State Board of Pharmacy

TIMELINE
Rollout and education period
October 1 – December 31, 2013
Evaluation period
January 1 – December 31, 2014
Ohio Department of Health 31
Professional Education
Workgroup

METRICS
1. Percentage of prescribers of controlled substances
registered in OARRS.
2. Percentage of registered prescribers of controlled
substances using OARRS.
3. Proportion of patients at 80mg MED and above who have
at least one OARRS inquiry over specified time period.
4. Number and percentage of patients prescribed both
opioids and sedative/hypnotics.
5. Percentage of prescriptions filled with a quantity of 120 or
more capsules or pills per prescription.
6. Average MED per prescription.
Ohio Department of Health 32
Professional Education
Workgroup

BENEFITS OF GUIDELINES TO DATE
• Metrics committee established to review how guidelines’ impact would be measured.
• Additional resources provided by state to bring in an evaluation expert.
• Increased collaboration and critical use of PMP data as a public health tool for state level analysis.
• Functional changes to the OARRS report to serve as a more useful clinical tool to help curtail over- or inappropriate opioid prescribing.
• Increased education about OARRS to prescribers and pharmacists.
Ohio Department of Health 3
3

CONTACT ODH
Christy Beeghly, MPH, Program Administrator
Violence and Injury Prevention Program
Ohio Department of Health
(614) 728-4116









![Summit Gardens Assn. v. Lemongelli - Ohiosc.ohio.gov/rod/docs/pdf/11/2007/2007-Ohio-6720.pdf · [Cite as Summit Gardens Assn. v. Lemongelli, 2007-Ohio-6720.] ... {¶19} On March 29,](https://static.fdocuments.us/doc/165x107/5b776b677f8b9a4c438d183a/summit-gardens-assn-v-lemongelli-cite-as-summit-gardens-assn-v-lemongelli.jpg)


![Portage Cty. Educators Assn. for Dev. Disabilities - Unit B ......[Cite as Portage Cty.Educators Assn. for Dev. Disabilities - Unit B, OEA/NEA v. State Emp. Relations Bd., 2020-Ohio-7004.]](https://static.fdocuments.us/doc/165x107/60db9c0eaee598371e498638/portage-cty-educators-assn-for-dev-disabilities-unit-b-cite-as-portage.jpg)



