Prescribing Guidance for Vitamins and Minerals in Primary Care
12
Vitamins and Minerals Prescribing Guidance V1.0 Approved November 2020 Review date: November 2022 Prescribing Guidance for Vitamins and Minerals in Primary Care
Transcript of Prescribing Guidance for Vitamins and Minerals in Primary Care

Vitamins and Minerals Prescribing Guidance
V1.0 Approved November 2020
Review date: November 2022
Prescribing Guidance for Vitamins and
Minerals in Primary Care
Vitamins and Minerals Prescribing Guidance
V1.0 Approved November 2020
Review date: November 2022
Review and Amendment Log / Version Control
Clinical Lead:
Dr Shane Beggan, Medicines Optimisation Clinical Lead
Author:
Susan Sheridan, Prescribing Support Dietitian, Medicines Optimisation
Team, NHS Bradford District and Craven Clinical Commissioning Group
(CCG) / Bradford Teaching Hospitals NHS Foundation Trust (BTHFT)
Date Approved:
November 2020
Approving Body:
Joint Formulary Group
Version:
1.0
Review Date:
November 2022
Version History
V no. Date Author Description Circulation
0.1 July 2020 Susan Sheridan Initial draft Tracey Gaston, Claire Kilburn
0.2 27/08/2020 Susan Sheridan Comments: DH, AM, MS, IH secondary care representatives
0.3 14/09/2020 Susan Sheridan Amendments following Joint Formulary Group meeting on 09/09/2020.
Joint Formulary Group
1.0 10/11/2020 As above Version approved by Joint Formulary Group
CCG wide

Vitamins and Minerals Prescribing Guidance
V1.0 Approved XXX 2020
Review date: XXX 2022
Prescribing Guidance for Vitamins and Minerals in Primary Care
In line with NHS England’s guidance on conditions for which over-the-counter items should not be routinely prescribed Bradford District and Craven CCG does not support the routine prescribing of vitamins and minerals on prescription unless indicated for actual vitamin or mineral deficiency. Vitamins and minerals should not be prescribed as a ‘general pick-me-up’ or as a dietary supplement. Exceptions:
Medically diagnosed deficiency, including for those patients who may have a lifelong or chronic condition or have undergone surgery that results in malabsorption. Continuing need should be reviewed on a regular basis (NB maintenance or preventative treatment is not an exception).
Calcium and vitamin D for osteoporosis.
Malnutrition including alcoholism. Vitamins and minerals are essential nutrients which most people should be able to get from eating a healthy, varied and balanced diet. The Eatwell Guide https://www.nhs.uk/live-well/eat-well/the-eatwell-guide/ is a useful tool which can be used to demonstrate to people how a healthy, varied and balanced diet can be achieved.
Many vitamin and mineral supplements are classified as foods, not medicines, and therefore do not have to go through the strict criteria laid down by the Medicines and Healthcare products Regulatory Agency (MHRA) to confirm their quality, safety and efficacy before reaching the market. It is therefore not deemed appropriate for such preparations to be routinely funded on the NHS.
There is insufficient high quality evidence to demonstrate clinical effectiveness of vitamins and minerals.
Taking too many vitamins and minerals, or for too long could be harmful.
Recommendations for prescribers:
Discontinue prescribing vitamins and minerals on FP10 for patients where treatment is not in line with recommendations.
If patients still want to take vitamins and minerals for dietary supplementation or as a ‘pick-me-up’, they should be advised that these can be purchased as self-care over-the-counter with the support of the community pharmacist. For information on daily amounts and dietary sources sign post patients to https://www.nhs.uk/conditions/vitamins-and-minerals/
NHS Healthy Start vitamins are recommended for pregnant and breast-feeding women and children under 5, as a preventative measure. These vitamins are not on prescription. In Bradford, Airedale and Wharfedale all infants up to 6 months age receive free Healthy Start vitamin drops, after 6 months age infants and children can receive the vitamins through either of the following ways:
1. Free vitamins via the Health Start scheme if eligible. Information can be found on the Healthy Start website
2. Purchased at designated local health centres/community pharmacies 3. Health Visitors can issue free vitamins up to 2yrs age for children at high risk of deficiency.
In the Craven area, all Healthy Start vitamin drops need to be purchased or accessed via the Healthy Start scheme. All pregnant women receive free NHS healthy Start vitamin tablets: Breast feeding women can purchase the vitamins at designated local health centres/community pharmacies or via the Healthy Start scheme if eligible.

Vitamins and Minerals Prescribing Guidance
V1.0 Approved XXX 2020
Review date: XXX 2022
Nutrient
Indication
Dose
Review
Multivitamin and minerals - Adults
Forceval
Renavit Water soluble vitamins
Medically diagnosed deficiency Malnutrition Malabsorption Adults with renal failure on dialysis
One capsule daily Advised by secondary care
3-6 months Continued need should be reviewed regularly If patients wish to have multivitamins and minerals in the absence of proven deficiency these should be purchased OTC Monitored by secondary care
Multivitamin and minerals - Paediatric
Abidec/Dalivit/Paediatric Seravit/Fruitivits/Phlexyvits/ Ketovite liquid and tablets
Metabolic conditions Enteral tube feeds Therapeutic restricted diets e.g. multiple allergy
Advised by secondary care
Monitored by secondary care Annual review minimum
A – Z Vitamins
Vitamin A (Retinol)
Deficiency is associated with ocular defects and an increased susceptibility to infections, but deficiency is rare in the UK.
Advised by secondary care
Monitored by secondary care
Thiamine (Vitamin B1)
Deficiency related to chronic alcoholism Wernicke-Korsakoff
100mg three times daily 100mg three times daily
Annually, based on alcohol intake, continue until 3 months abstinent / varied diet. Chronic alcohol dependence may need to be continued indefinitely. If patients move into care/nursing home and are no longer drinking alcohol, can be stopped. With Wernicke-Korsakoff, supplementation will need to continue
Vitamins and Minerals Prescribing Guidance
V1.0 Approved XXX 2020
Review date: XXX 2022
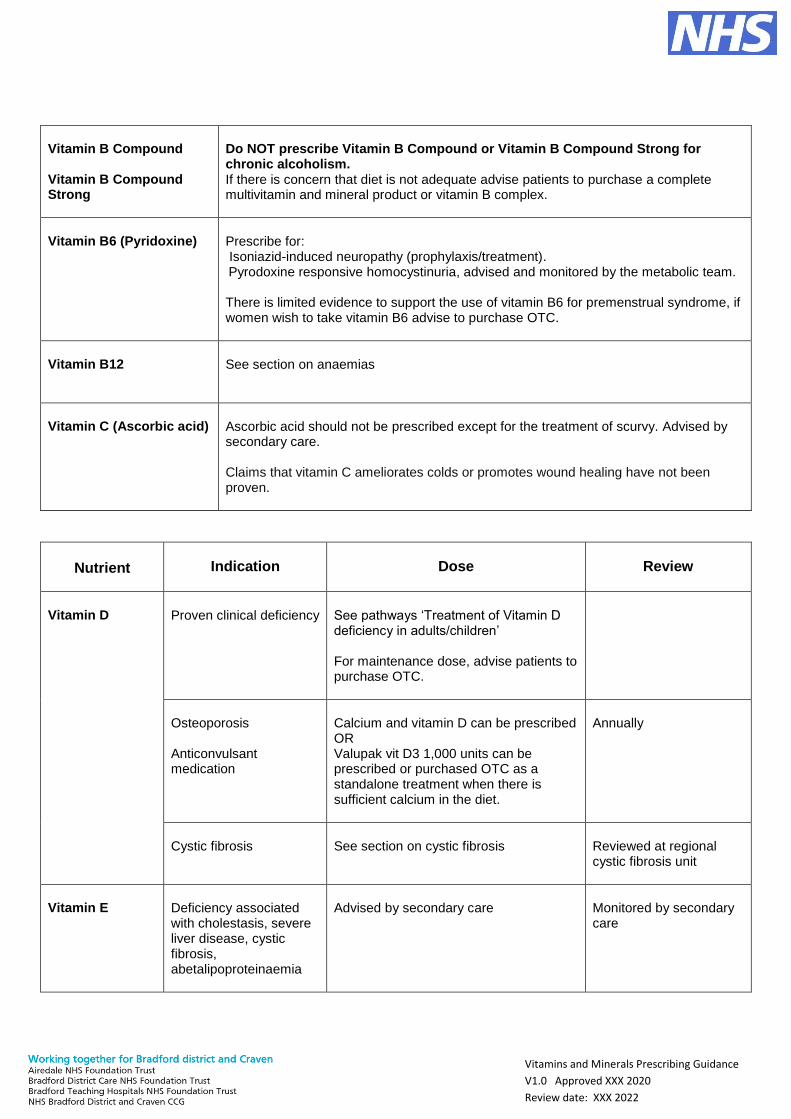
Vitamin B Compound Vitamin B Compound Strong
Do NOT prescribe Vitamin B Compound or Vitamin B Compound Strong for chronic alcoholism. If there is concern that diet is not adequate advise patients to purchase a complete multivitamin and mineral product or vitamin B complex.
Vitamin B6 (Pyridoxine)
Prescribe for: Isoniazid-induced neuropathy (prophylaxis/treatment). Pyrodoxine responsive homocystinuria, advised and monitored by the metabolic team. There is limited evidence to support the use of vitamin B6 for premenstrual syndrome, if women wish to take vitamin B6 advise to purchase OTC.
Vitamin B12
See section on anaemias
Vitamin C (Ascorbic acid)
Ascorbic acid should not be prescribed except for the treatment of scurvy. Advised by secondary care. Claims that vitamin C ameliorates colds or promotes wound healing have not been proven.
Nutrient
Indication
Dose
Review
Vitamin D
Proven clinical deficiency
See pathways ‘Treatment of Vitamin D deficiency in adults/children’ For maintenance dose, advise patients to purchase OTC.
Osteoporosis Anticonvulsant medication
Calcium and vitamin D can be prescribed OR Valupak vit D3 1,000 units can be prescribed or purchased OTC as a standalone treatment when there is sufficient calcium in the diet.
Annually
Cystic fibrosis
See section on cystic fibrosis
Reviewed at regional cystic fibrosis unit
Vitamin E
Deficiency associated with cholestasis, severe liver disease, cystic fibrosis, abetalipoproteinaemia
Advised by secondary care
Monitored by secondary care

Vitamins and Minerals Prescribing Guidance
V1.0 Approved XXX 2020
Review date: XXX 2022
Nutrient
Indication
Dose
Review
Minerals
Magnesium
Hypomagnesaemia,
prevent recurrence of magnesium deficit
Magnesium aspartate (magnesium
10mmol) oral powder sachet
Magnesium glycerophosphate (magnesium 97.2mg (4 mmol)) chewable
tablets sugar free
Dose advised by secondary care
Monitored by secondary care.
Selenium
Only prescribe for
deficiency
Advised by secondary care
Monitored by secondary care
Zinc
Only prescribe for
deficiency
Advised by secondary care
Monitored by secondary care

Vitamins and Minerals Prescribing Guidance
V1.0 Approved XXX 2020
Review date: XXX 2022
Anaemias
Nutrient
Indication
Dose
Review
Vitamin B12
Megaloblastic anaemia, most common cause is pernicious anaemia. Other less common causes include malabsorption, drugs (metformin, PPIs) Dietary deficiency, e.g. vegan diet, restricted vegetarian diet
Hydroxocobalamin 1mg intramuscular injection (IM) 3 x /week for 2 weeks, followed by hydroxocobalamin 1mg IM every 2-3 months. Hydroxocobalamin 1mg intramuscular injection (IM) 3 x /week for 2 weeks followed by maintenance oral vitamin B12 (cyanocobalamin) 50-150 micrograms. Advise patients to purchase oral vitamin B12 (cyanocobalamin) OTC.
Lifelong treatment Vegan diet, maintenance oral vitamin B12 may need to continue, in other less restricted diets replacement treatment can be stopped once vitamin B12 levels are corrected and diet improved. Provide dietary advice to patients https://www.nhs.uk/conditions/vitamin-b12-or-folate-deficiency-anaemia/
Folate
Folate deficient megaloblastic anaemia Prevention of methotrexate-induced folate deficiency For at least 3 months before and for the first trimester of pregnancy in the following women: Obese (BMI>30) Diabetes Woman or partner has neural tube defect (NTD), previous pregnancy affected by NTD, family history of NTD. Taking anti-epilepsy medication Coeliac disease or other malabsorption states For at least 3 months before and throughout pregnancy in women with sickle cell disease, thalassaemia, thalassaemia trait Can also be used in the management of Homocystinuria
Folic acid 5mg daily for 4 months Folic acid 5mg daily except on methotrexate days Folic acid 5mg daily for at least 3 months before and for the first trimester of pregnancy Folic acid 5mg daily for at least 3 months before and throughout pregnancy Advised by the metabolic team
Provide dietary advice to patients to minimise risk of reoccurrence of deficiency https://www.bda.uk.com/resourceDetail/printPdf/?resource=folic-acid Monitored by the metabolic team

Vitamins and Minerals Prescribing Guidance
V1.0 Approved XXX 2020
Review date: XXX 2022
Iron
Iron deficiency anaemia - treatment Iron deficiency anaemia – prophylaxis
Adults: 210mg ferrous fumarate (68 mg elemental iron), 200mg ferrous sulfate (65 mg elemental iron) once daily. Once daily elemental iron is effective and better tolerated than 2–3 times doses daily. Children: sodium federate oral solution (Sytron) Tips to improve absorption:
Ensure not taking at the same time as a PPI, antacid
Take with a source of vitamin C eg orange juice
Advise patients to purchase OTC.
Check Hb after 2-3 weeks to ensure adequate response. Treatment should continue for 3 months after iron deficiency is corrected to allow stores to be replenished. Monitor to ensure that there is an adequate response to iron treatment. Provide dietary advice to patients to minimise risk of reoccurrence of deficiency https://www.bda.uk.com/resourceDetail/printPdf/?resource=iron-rich-foods-iron-deficiency
Vitamins and Minerals Prescribing Guidance
V1.0 Approved XXX 2020
Review date: XXX 2022
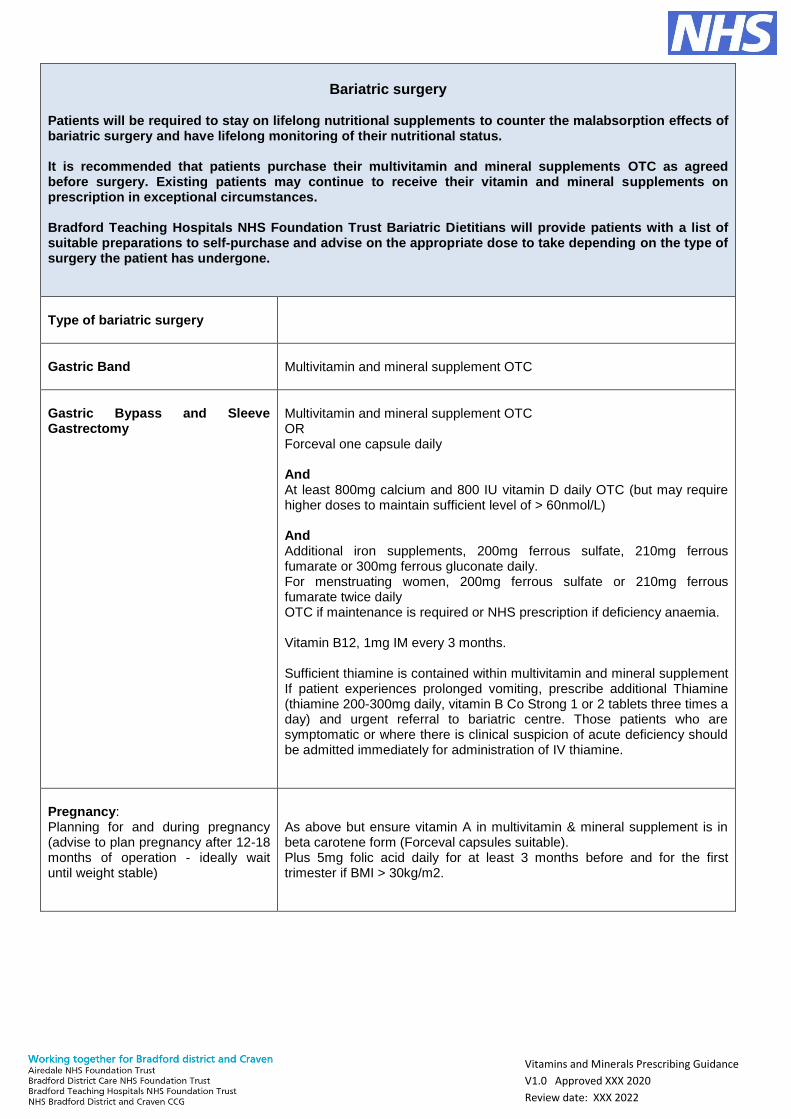
Bariatric surgery
Patients will be required to stay on lifelong nutritional supplements to counter the malabsorption effects of bariatric surgery and have lifelong monitoring of their nutritional status. It is recommended that patients purchase their multivitamin and mineral supplements OTC as agreed before surgery. Existing patients may continue to receive their vitamin and mineral supplements on prescription in exceptional circumstances. Bradford Teaching Hospitals NHS Foundation Trust Bariatric Dietitians will provide patients with a list of suitable preparations to self-purchase and advise on the appropriate dose to take depending on the type of surgery the patient has undergone.
Type of bariatric surgery
Gastric Band
Multivitamin and mineral supplement OTC
Gastric Bypass and Sleeve Gastrectomy
Multivitamin and mineral supplement OTC OR Forceval one capsule daily And At least 800mg calcium and 800 IU vitamin D daily OTC (but may require higher doses to maintain sufficient level of > 60nmol/L) And Additional iron supplements, 200mg ferrous sulfate, 210mg ferrous fumarate or 300mg ferrous gluconate daily. For menstruating women, 200mg ferrous sulfate or 210mg ferrous fumarate twice daily OTC if maintenance is required or NHS prescription if deficiency anaemia. Vitamin B12, 1mg IM every 3 months. Sufficient thiamine is contained within multivitamin and mineral supplement If patient experiences prolonged vomiting, prescribe additional Thiamine (thiamine 200-300mg daily, vitamin B Co Strong 1 or 2 tablets three times a day) and urgent referral to bariatric centre. Those patients who are symptomatic or where there is clinical suspicion of acute deficiency should be admitted immediately for administration of IV thiamine.
Pregnancy: Planning for and during pregnancy (advise to plan pregnancy after 12-18 months of operation - ideally wait until weight stable)
As above but ensure vitamin A in multivitamin & mineral supplement is in beta carotene form (Forceval capsules suitable). Plus 5mg folic acid daily for at least 3 months before and for the first trimester if BMI > 30kg/m2.
Vitamins and Minerals Prescribing Guidance
V1.0 Approved XXX 2020
Review date: XXX 2022
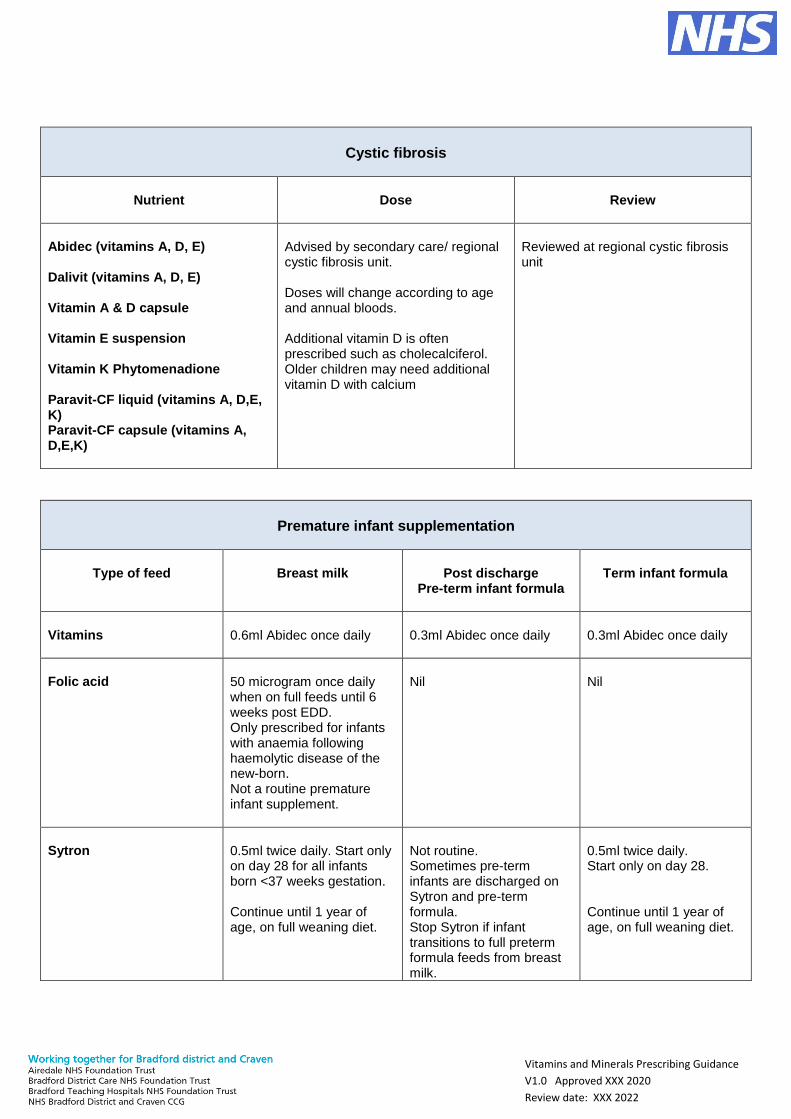
Cystic fibrosis
Nutrient
Dose
Review
Abidec (vitamins A, D, E) Dalivit (vitamins A, D, E) Vitamin A & D capsule Vitamin E suspension Vitamin K Phytomenadione Paravit-CF liquid (vitamins A, D,E, K) Paravit-CF capsule (vitamins A, D,E,K)
Advised by secondary care/ regional cystic fibrosis unit. Doses will change according to age and annual bloods. Additional vitamin D is often prescribed such as cholecalciferol. Older children may need additional vitamin D with calcium
Reviewed at regional cystic fibrosis unit
Premature infant supplementation
Type of feed
Breast milk
Post discharge
Pre-term infant formula
Term infant formula
Vitamins
0.6ml Abidec once daily
0.3ml Abidec once daily
0.3ml Abidec once daily
Folic acid
50 microgram once daily when on full feeds until 6 weeks post EDD. Only prescribed for infants with anaemia following haemolytic disease of the new-born. Not a routine premature infant supplement.
Nil
Nil
Sytron
0.5ml twice daily. Start only on day 28 for all infants born <37 weeks gestation. Continue until 1 year of age, on full weaning diet.
Not routine. Sometimes pre-term infants are discharged on Sytron and pre-term formula. Stop Sytron if infant transitions to full preterm formula feeds from breast milk.
0.5ml twice daily. Start only on day 28. Continue until 1 year of age, on full weaning diet.

Vitamins and Minerals Prescribing Guidance
V1.0 Approved XXX 2020
Review date: XXX 2022
Term Infant - Low birth weight infant (<2.5kg) supplementation
Type of feed
Breast milk
Post discharge
Pre-term infant formula
Term infant formula
Sytron
0.5ml twice daily. Start only on day 28 Continue until 1 year of age, on full weaning diet. Stop if formula feeds introduced
N/A
Nil
Refeeding syndrome
Nutrient
Dose
Review
Thiamine (Vitamin B1)
100mg three times daily Prescribed for the first ten days from when feeding recommences
Supply is provided on discharge: GP not to continue the prescription unless patient is alcohol dependant
Multivitamin and minerals
Forceval one capsule daily, or Forceval soluble one tablet daily dissolved in water if swallowing difficulties
Until adequate oral diet re-established, OTC is recommended following discharge.
References / Further reading
NHS England and NHS Clinical Commissioners. Conditions for which over the counter items should not routinely be
prescribed in primary care. Guidance for CCGs. March 2018. Available at: https://www.england.nhs.uk/wp-
content/uploads/2018/03/otc-guidance-for-ccgs.pdf
PrescQIPP Bulletin 227 October 2018 2.2 Over the counter items - GP guide to self-care
https://www.prescqipp.info/media/4055/227-over-the-counter-items-22.pdf
Regional Medicines Optimisation Committee (RMOC, North) November 2019, Position Statement, Oral vitamin B
supplementation in alcoholism https://www.sps.nhs.uk/wp-content/uploads/2019/12/RMOC-position-statement-oral-
vitamin-B-supplementation-in-alcoholism-v1.0-1.pdf

Vitamins and Minerals Prescribing Guidance
V1.0 Approved XXX 2020
Review date: XXX 2022
NICE CKS – Premenstrual syndrome, May 2019 https://cks.nice.org.uk/premenstrual-syndrome#!scenario
NICE, Anaemia – B12 and folate deficiency April 2018 https://cks.nice.org.uk/anaemia-b12-and-folate-deficiency
M. Muñoz et al, International consensus statement on the peri‐operative management of anaemia and iron deficiency.
Anaesthesia 2017, 72, 233 – 247
E Rimon et al, Are we giving too much iron? Low-dose iron therapy is effective in octogenarians. The American
Journal of Medicine (2005) 118, 1142 – 1147.
D Moretti et al, Iron supplements increase hepcidin and decrease iron absorption from daily or twice-daily doses in
iron-depleted young women. Blood, 22 October 2015, vol 126, number 17
British Obesity & Metabolic Surgery Society (BOMSS) Guidelines on peri-operative and postoperative biochemical
monitoring and micronutrient replacement for patients undergoing bariatric surgery, August 2020
https://www.bomss.org.uk/bomss-nutritional-guidance_2020/
Bradford Teaching Hospitals NHS Foundation Trust, Nutrition Policy for Adults: Appendix F Refeeding Syndrome
Sept.2019
British Dietetic Association Food Fact sheet: Supplements 2019 https://www.bda.uk.com/resource/supplements.html
Authors
Susan Sheridan, Prescribing Support Dietitian, Medicines Optimisation Team, NHS Bradford District and Craven
Clinical Commissioning Group (CCG) / Bradford Teaching Hospitals NHS Foundation Trust (BTHFT)
Tracey Gaston, Senior Head of Medicines Optimisation, NHS Bradford District & Craven CCG
Claire Kilburn, Senior Head of Medicines Optimisation, NHS Bradford District & Craven CCG
Acknowledgements
Amanda Musk, Neonatal & Paediatric Dietitian, BTHFT
Dalvinder Hellawell, Paediatric Dietitian, BTHFT
Inderdip Hunjan, Metabolic Dietitian, BTHFT
Michelle Soobayah, Bariatric Dietitian, BTHFT
Paul Bailey, Renal Dietitian, BTHFT
Dr Paul Southern, Consultant Hepatologist, BTHFT
Mr James Halstead, Consultant Surgeon, BTHFT
Dr Andrew Hanson, GP, Specialist Epilepsy Services, The Ridge Medical Practice, Bradford.
Nick Bergin, Specialist Nutrition Support Dietitian and Acute Team Leader, Airedale NHS Foundation Trust
Dr Nick Hayward, Associate Clinical Director for Quality Improvement, Bradford district & Craven CCG