Jaipur Vidyut Vitran Nigam Limited Jodhpur Vidyut Vitran Nigam ...

HealthcareintheUnitedStates
• Whatisthesystemfor?• Whoarethekeyplayers,whataretheirroles,andwhataretheirinterests?
• Howdoesthesystemfunctioneconomically?• Whatarethetrends,failures,andopportunities?
• How,whereandwhy,aredataproduced?



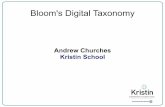
AnatomyoftheUSHealthcareSystem
Takeaminutetothink,thenworkwithyourneighbortoanswerthefollowingquestiononyourconceptmap:
Whatarethekindsofdatathateachoftheseentitiesgenerate?Forwhatpurpose?Example:individualpatientsgeneratefitnesstrackerdatafortheirownpersonalinterest

Whereandwhyarethedatagenerated?
claims
FitnesstrackersHomemonitorsForums
Sales
HealthrecordsDoctorsnotesQueries
DomainknowledgePublicdatabases
Domainknowledge
CensusanddemographicsEpidemiologicaldataEconomicdata
PublicusePolicymaking
Businessintelligencebilling
OperationsQualityBilling
OperationsMarketing
PersonalinterestCaregiverrecords
PublicuseProfessionalgain
MarketingBusinessintelligence

Weberetal,JAMA2014

• Publiclyavailabledatafrom1980to2011,onthesourceanduseoffunds.• In2011,UShealthcareemployed15.7%oftheworkforce,with
expendituresof$2.7trillion,andbeing17.9%ofGDP.
• Threefactorshaveproducedthemostchange:o consolidation,producingfinancialconcentrationo informationtechnology,inwhichinvestmenthasoccurredbutvalueiselusive;o patientempowerment,wherebyinfluenceissoughtoutsidetraditional
channels.
Followthemoney…itwillleadyoutotheproblemsthatreallyneedtobesolved

Conflictinginterests

Whenyouusethesedata:
• Knowthatprioritiesaredifferentforeachstakeholder,whichaffectsthedatathataregenerated.
• Designstudiestoleveragestrengthsandprotectfromweaknessesofthedata.Usingmultiplesourcesisbeneficial.
• Thinkaboutwhoisinterestedintheresults.Targetingstudiestotheintersectionsoftwoormoreinterestsisimpactful.

Whypredictcost?
• For“risk-adjustment”• Riskassessmentàmeasuringtheexpectedhealthcarecostsof
individualsenrolledinaplan.• Riskadjustmentàmovingfundsfromplansthathavelessthantheir
fair-shareofhigh-riskenrolleestoplansthathavemorehigh-riskenrollees.
• For“risk-contracting”• Inafeeforperformancemodel,wheretheproviderisassumingtotal
riskforcaringforanindividual,theyneedtoknowtheirriskexposure.
• Fordecidingwhichinsurancetobuy• Asanindividual,knowingyourtrueriskallowsyoutobuythe
appropriateplanwithadequatecoverage.• E.g.shouldyouenrollinahighdeductibleplanornot?

Costatthepopulationlevel

Whatisworthpredicting?
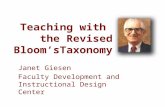
• Ifyouhaveahighcostyear,whatistheprobabilitythatthenextyearishighcost?• 0.26overall• 0.37inhighcostpopulation• 0.03inlowcostpopulationà Iftheybecomehigh-cost,it’sanunexpectedevent
• HighCostvs.aCostbloom

Anatomyof“highcost”
0 1 2 3 4 5 6 7 8
fraction total (high) costs by num expensive years
num expensive years (cost >= 50.4)
0.00
0.05
0.10
0.15
0.20
0.25
0.30

Anatomyof“highcost”
0 1 2 3 4 5 6 7 8
fraction patients vs number high cost years in CHF
number of high cost years (highest decile of annual cost)
fract
ion
of p
atie
nts
0.0
0.2
0.4
0.6
0.8
1.0
0 1 2 3 4 5 6 7 8
fraction patients vs number high cost years in COPD
number of high cost years (highest decile of annual cost)
fract
ion
of p
atie
nts
0.0
0.2
0.4
0.6
0.8
1.0
0 1 2 3 4 5 6 7 8
fraction patients vs number high cost years in DM
number of high cost years (highest decile of annual cost)
fract
ion
of p
atie
nts
0.0
0.2
0.4
0.6
0.8
1.0

Anatomyofthecost
ExpensiveinYear1
ExpensiveinYear2
60%- Bloomers
40%- Persistent

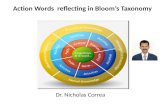
Predictingcostvs.costbloom

2,146,801Residents2004-2011
588,851
1,557,950
155,795
1,402,155
PredictionSample1
PredictionSample2
PredictionTask1:Population-levelHigh-Cost
PredictionTask2:CostBlooms
TrendAnalysis2004-2011
Task1:SelectionCriteria
Task2:SelectionCriteria
ComparisonofAlternativeCost-predictionModels2010-2011

Resid
ents
High
Cost
CostBloo
m
PID1 0 0PID2 0 0PID3 1 1PID4… … …PIDN 1 NA
Training Tuning Testing
Features(20
08)
ModelDevelopmentandEvaluation
CostCapture
CostofPredictedHigh-CostGroup
Mod
elFeatures
PredictionModelTypes
Respon
ses(20
09)
Features(20
09)
Respon
ses(201
0)
Features(2
010)
Respon
ses(20
11)
CostofActual
High-CostGroup
_____________=100x
Model1:Age+Gender+CCS+CCIModel2:Model1+Hosp.Inpt &Outpt,DrugCostsModel3:Model2+PrimaryCareCostsModel4:FullFeatureSetwithoutCostsModel5:FullFeatureSet(1059totalfeatures)
StandardFeaturesBinaryLogisticRegression
EnhancedFeaturesBinaryLogisticRegression
EnhancedFeaturesElasticNetPenalizedLogisticRegression
Clinical Registries CivilReg. SystemSTANDARDFEATURES ENHANCEDFEATURES
Resid
ents
Age
Gend
er
Risk
Scores
Costs
Costs
Clinical
Code
Sets
Visits
Coun
ts
Recency
Social
Relatio
n-ship
Danish
Distric
t
PID1 45 F CCSdiseaseandCCIchronicconditionscores
All
HospitalandHospital
OutpatientClinic(HO)
Drug(Rx)
PrimaryCareandSpecialist
(PC)
ICD,NOMESCO,
ATCcategories
Hospital,OutpatientClinic,PrimaryCare,
Specialist,Medication,
TreatmentsandSurgeries
MovingAveragesofDiagnoses,Costs,Visits
Married-Widowed 1
PID2 34 F Unmarried 4PID3 22 M Unmarried 2PID4 32 M Married 2… … … … …PIDN 71 F Widowed 1
Models4&5Models1&2ModelDescriptions
Model3
Respon
ses

Results
PredictionTask
EvaluationMetric
Model1:Baseline
Model2:+HospInptandOutpt,Drug
Costs
Model3:+PrimaryCareCosts
Model4:AllFeatureswithoutCosts
Model5:AllFeatures
High-cost(N=1,557,950)
AUC 0.775 0.814 0.825 0.823 0.836CostCapture 0.495 0.559 0.577 0.578 0.600
Cost-bloom(N=1,402,155)
AUC 0.719 0.748 0.772 0.771 0.786CostCapture 0.376 0.443 0.455 0.466 0.487



PredictionsandActions
Take onRisk
Service
Intervention
List �
Cost-bloom Mortality ChronicPain Pre-diabetestoDiabetes
Risk ofOpioidabuse
Possiblefurtherwork:• Summarizethebloomers.• Exploratoryanalysestodesigninterventions.

Possibleinterventiontypes
• Relationship-basedInterventions:Suggesthighvalueinterventionstoattendingphysicians,healthcaresystemmedicaldirectors,and/orpatients.
• Rules-basedInterventions:Whererelationshipswithprovidersareinsufficientlydeveloped,alterationofplanrulesgoverningcoverage,pre-cert,providernetworkinclusion,providerincentives,patientincentives,formularytiers,and/orDURscreens.

Summary1. Importanttodistinguishcost-bloomersfrom
persistenthigh-costpatients.
2. 30%improvementincostcaptureoverastandarddiagnosis-basedclaimsmodel.
3. Includingapatient’ssocialrelationshipstatus,andtemporalinformationsuchasthefrequencyandrecency ofhealthcareevents,improvedprediction.
4. Predictionsenablesprecisetargetingofthesubsetofpatientswhoareatthemostriskofacostbloom.
5. Exampleofmachinelearningthatmatters.

Tipsforyourpredictivemodelingprojects
Datacleanupwilltakeabout80%ofthetime
• Ifyoutookashortcuthere,stop.
Trysimplethingsfirst• “Deeplearning”isnottheright
answereverytime!
Askwhether:• Moredatawillincrease
performance• Morefeatureswillincrease
performance• Errorsfromdifferentmodelsare
correlated
Don’tgetfooledbyAUC• Examineprecisionrecall,
calibration,net-reclassification
Don’tgetattachedtoonemodel
Rememberthatthedataarechangingunderyou
Thinkaboutmodeldeployment• Easeofapplyingthemodel• Thinkaboutthecostoftaking
action• Precision@K

Openresearchproblems
• Handlingdatanonstationarity• Localvs.Globalmodels• Handlingunstructureddata• Outcomeascertainment(andcensoring)• Evaluation:Lookingbeyonddiscrimination(calibration,net-reclassification)
• Bridgingthe“lastmile”

Credits
• SuzanneTamang• ArnoldMilstein• AlanGlaseroff• ThomasWang