Prasugrel et NSTEMI que faire en pratique?...2013/07/10 · Clopidogrel in Unstable Angina to...
18
Prasugrel et NSTEMI que faire en pratique? Loïc Belle Annecy
Transcript of Prasugrel et NSTEMI que faire en pratique?...2013/07/10 · Clopidogrel in Unstable Angina to...

Prasugrel et NSTEMIque faire en pratique?
Loïc BelleAnnecy


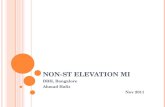
Stent Thrombosis(ARC Definite + Probable)
0
1
2
3
0 30 60 90 180 270 360 450
HR 0.48(0.36-0.64)P <0.0001
Prasugrel
Clopidogrel2.4
(142)
74 events
NNT= 77
1.1 (68)
Days
End
poin
t (%
)
Any Stent at Index PCIAny Stent at Index PCIN= 12,844N= 12,844
0
5
10
15
0 30 60 90 180 270 360 450
HR 0.81(0.73-0.90)P=0.0004
Prasugrel
Clopidogrel
Days
End
poin
t (%
)
12.1
9.9
HR 1.32(1.03-1.68)
P=0.03
Prasugrel
Clopidogrel1.82.4
138events
35events
Balance of Efficacy and Safety
CV Death / MI / Stroke
TIMI Major NonCABG Bleeds
NNT = 46
NNH = 167

Net Clinical BenefitDeath, MI, Stroke,
Major Bleed (non CABG)
0
5
10
15
0 30 60 90 180 270 360 450Days
End
poin
t (%
)
HR 0.87(0.79-0.95)
P=0.004
13.9
12.2
Prasugrel
ClopidogrelITT= 13,608ITT= 13,608

Clopidogrel in Unstable Angina
to Prevent Recurrent Ischemic
Events



25086 patients(70% UA or NSTEMI)
17263 PCI 7823 no PCI

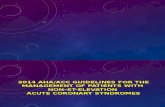
NSTEMI
600 mg de CLOPIDOGREL ( X 1 à 4 en fonction du VASP)
Coronarographie - PCI
ATCD AVC/AIT+ de 75 ans- de 60 Kgs
CLOPIDOGREL guidé parle VASP
Pas d’ATCD AVC/AIT-De 75 ans-+ de 60 Kgs
PRASUGRELAvec dose de charge si VASP>50%

RISQUE ISCHEMIQUE
• Diabète• Procédure interventionnelle• VASP• Résistance « génétique » au clopidogrel• Maladie diffuse.
RISQUE ISCHEMIQUE
• Diabète• Procédure interventionnelle• VASP• Résistance « génétique » au clopidogrel• Maladie diffuse.


RISQUE ISCHEMIQUE
• Diabète• Procédure interventionnelle• VASP• Résistance « génétique » au clopidogrel• Maladie diffuse.
HR 95% CI p valueAntiplatelet discontinuation 89,8 30-269 < 0,001Renal failure 6,49 2,6-16,1 < 0,001Bifurcation lesions 6,42 1,74-7,89 < 0,001Diabetes 3,71 1,74-7,89 < 0,001Low EF 1,09 1,05-1,36 < 0,001
Predictors of stent thrombosis after DES implantation
Predictors of stent thrombosis after Predictors of stent thrombosis after DES implantationDES implantation
Iakovou I JAMA 2005;293:2126-30Iakovou I JAMA 2005;293:2126Iakovou I JAMA 2005;293:2126 --3030

RISQUE ISCHEMIQUE
• Diabète• Procédure interventionnelle• VASP• Résistance « génétique » au clopidogrel• Maladie diffuse.
• Patients receiving aspirin and clopidogrel• Clopidogrel resistance defined by ADP-Ag >70% pre PCI
Geisler et al, EHJ 2006

RISQUE ISCHEMIQUE
• Diabète• Procédure interventionnelle• VASP• Résistance « génétique » au clopidogrel• Maladie diffuse.

RISQUE ISCHEMIQUE
• Diabète• Procédure interventionnelle• VASP• Résistance « génétique » au clopidogrel• Maladie diffuse.
NSTEMI
600 mg de CLOPIDOGREL ( X 1 à 4 en fonction du VASP)
Coronarographie - PCI
ATCD AVC/AIT+ de 75 ans- de 60 Kgs
CLOPIDOGREL guidé parle VASP
Pas d’ATCD AVC/AIT-De 75 ans-+ de 60 Kgs
PRASUGRELAvec dose de charge si VASP>50%
DiabèteProcédureVASPProfil génétique Maladie diffuse

Copyright ©2005 American Heart Association
Hochholzer, W. et al. Circulation 2005;111:2560-2564
Left, Maximal aggregation (5 {micro}mol/L ADP) at cardiac catheterization dependent on time since loading dose of clopidogrel
Bénéfice d’une dose de 600 mg de Clopidogrel chez p atients SCA non ST+
(agrégation et pronostic)
Cuisset and coll P 4554 World cardiology Congress Barcelona 200Cuisset and coll P 4554 World cardiology Congress Barcelona 20066
292 patients SCA non ST +292 patients SCA non ST +
300 mg Clopidogrel300 mg Clopidogrel 600 mg Clopidogrel600 mg Clopidogrel
Angioplastie
Agrégation optique ADP < 12 H (HRPP > 70 %)
AgrAgréégation = 61 % +/gation = 61 % +/-- 16 16 AgrAgréégation = 50 % +/gation = 50 % +/-- 19 19
HyperrHyperrééactivitactivitéé plaquettaire 25 %plaquettaire 25 % HyperrHyperrééactivitactivitéé plaquettaire 15 %plaquettaire 15 %
Events 18 ( 12 %)Events 18 ( 12 %) Events 7 ( 5 %)Events 7 ( 5 %)
1 m
ois
P < 0.0001P < 0.0001
P = 0.03P = 0.03
P = 0.02P = 0.02
> 12 hours > 12 hours before stentingbefore stenting

dose de charge et angioplastie sur le bénéfice clinique
5
Clopidogrel (300mg)
Délai en heure entre dose de charge et angioplastie
0 15 25
-5
Placebo
-6
-4
-3
-2
-1
0
10 20
P = 0.020Pour l’interaction traitement/délai (> 15h)
Log
odds
of d
eath
, MI o
r U
TV
R a
t 28
days
Steinhubl S et al.J Am Coll Cardiol 2006;47:939-43.

Patti, G. et al. Circulation 2005;111:2099-2106
ARMYDAARMYDA--2 STUDY Results: 2 STUDY Results: Comparison of postprocedural elevation of CK-MB and troponin I in the 2
study arms