pph Pain 2013 (1)
34
Psychological factors in Pain 1 Dr Sinead O’Toole UCD Sinead.otoole@ucd. ie 7166431
description
LECTURE by Dr.Sinead
Transcript of pph Pain 2013 (1)
2
Learning outcomes
To develop an understanding of the components of psychological care that can be integrated with physical care.
To develop an understanding of the role of psychology in understanding pain

Introduction
The role of psychology in understanding pain
Theoretical perspectivesPsychological processes
involved in painTen guiding principles
relating psychological factors to the management of pain
Measuring pain – optional
3

4
Role of Psychology
The experience of pain is shaped by a host of psychological factors
These factors are not completely understood
The translation of their use in clinical work remains a challenge
5
Early pain theories
Early models of pain described pain within a biomedical framework as an automatic response to an external factor Descartes – direct
pathway Von Frey (1895) -
Specificity theory Goldschneider (1920)-
Pattern theory

6
Gate control theory of pain
Introduced a role for psychology and described a multidimensional process rather than a simple linear process
Evidence illustrating the mechanisms to increase and decrease pain

7
Gate control theory Melzack & Wall
Gate functioning is based in part on descending influences from the brain
1. Cognitive processes
2. Affective processes

8
Psychological effects on & of Pain
Emotions
Cognition Behaviour

9
Summary of Psychological Processes involved in Pain Linton S J , and Shaw W S PHYS THER 2011;91:700-711

10
Dr Barbara Coughlan, UCD School of Nursing, Midwifery and Health Sytems
11
Helping people cope with pain
The first line of treatment for acute pain is generally some form of pharmacological treatment.
Psychological interventions generally form a second level intervention in the management of acute pain-i.e.... have high levels of anxiety or have incomplete pain relief.
12
Guiding Principle Clinical Implication
1. Psychological factors that may affect pain outcomes are not routinely assessed by many treating clinicians
Better methods of screening and early intervention are needed to improve feasibility and utility in usual care settings
Ten Guiding Principles Relating Psychological Factors to the Management of Pain - Assessment
13
Guiding Principle Clinical Implication
2. Persistent pain naturally leads to emotional and behavioural consequences for the majority of individuals
Psychological concepts of learning can be useful to provide empathy and support without reinforcing pain behaviour
Ten Guiding Principles Relating Psychological Factors to the Management of Pain - Assessment

14
Guiding Principle Clinical Implication
3. Clients who are depressed or have a history of depression may have more difficulty dealing with pain
A brief assessment of mood symptoms should be part of routine screening and intake procedures for pain conditions
Ten Guiding Principles Relating Psychological Factors to the Management of Pain - Assessment

15
Guiding Principle Clinical Implication
4. Persistent pain problems can lead to hypervigilance and avoidance, but simple distraction techniques are not enough to counter these behaviours
Clinicians should avoid inadvertent messages that escape or avoidance from pain is necessary in order to preserve function
Ten Guiding Principles Relating Psychological Factors to the Management of Pain – Treatment Planning
16
Guiding Principle Clinical Implication
5. Individuals hold very different attitudes and beliefs about the origins of pain, the seriousness of pain, and how to react to pain
Assessment and treatment planning should take into account individual differences in pain beliefs and attitude
Ten Guiding Principles Relating Psychological Factors to the Management of Pain – Treatment Planning
17
Guiding Principle Clinical Implication
6. Personal expectations about the course of pain recovery and treatment benefits are associated with pain outcome
Providing realistic expectations (positive, but frank and not overly reassuring) may be a very important aspect of treatment
Ten Guiding Principles Relating Psychological Factors to the Management of Pain – Treatment Planning
18
Guiding Principle Clinical Implication
7. Catastrophic thinking about pain is an important marker for the development of long-term problems as well as for poor treatment outcomes
Clinicians should listen for expressions of catastrophic thoughts and offer less exaggerated beliefs as an alternative. A brief assessment might be part of routine intake procedures
Ten Guiding Principles Relating Psychological Factors to the Management of Pain – Treatment Planning
19
Guiding Principle Clinical Implication
8. Personal acceptance and commitment to self- manage pain problems are associated with better pain outcomes
Over-attention to diagnostic details and biomedical explanations may reinforce futile searches for cure and delay pain self management
Ten Guiding Principles Relating Psychological Factors to the Management of Pain – Treatment implementation

20
Guiding Principle Clinical Implication
9. Psychosocial aspects of the workplace may represent barriers for returning to work while pain problems linger
Return-to-work planning should include attention to aspects of organizational support, job stress, and workplace communication
Ten Guiding Principles Relating Psychological Factors to the Management of Pain – Treatment implementation

21
Guiding Principle Clinical Implication
10. With proper instruction and support, psychological interventions can improve pain management outcomes
Psychological approaches can be incorporated into conventional treatment methods but require special training and support
Ten Guiding Principles Relating Psychological Factors to the Management of Pain – Treatment implementation

Measuring Pain22
Pain is very difficult to measure due to its’ multifaceted nature. When measuring pain we need to consider the following Can we objectively
measure tissue damage? Can do two people with the
same injury have different experiences of pain?
Multiple words used to describe the experience of pain e.g. throbbing, stinging, dragging, crushing, radiating….
Health related quality of life measures: include measures of pain
Dr Barbara Coughlan, UCD School of Nursing, Midwifery and Health Sytems
23
Short Form-36 Health Survey (SF-36) (Jenkinson & Coulter, 1993).
The SF-36 is a generic, self-completion health status questionnaire with eight distinct dimensions accessing most of the important dimensions of health status including bodily pain. The bodily pain scale has a range of 0 (poor health) to 100 (good health).
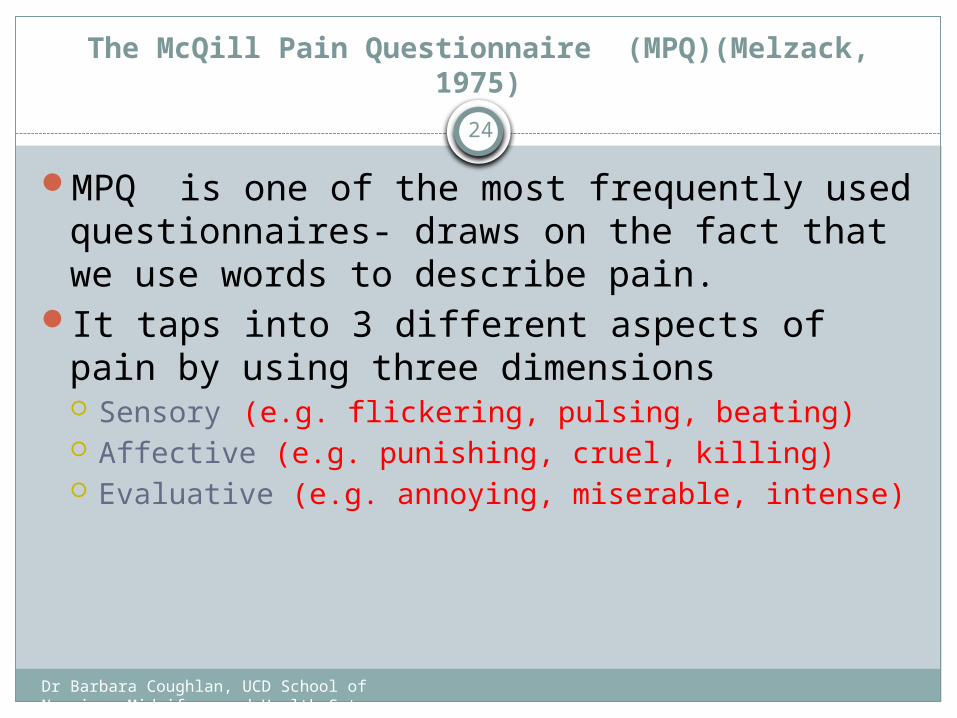
The McQill Pain Questionnaire (MPQ)(Melzack, 1975)
Dr Barbara Coughlan, UCD School of Nursing, Midwifery and Health Sytems
24
MPQ is one of the most frequently used questionnaires- draws on the fact that we use words to describe pain.
It taps into 3 different aspects of pain by using three dimensions Sensory (e.g. flickering, pulsing, beating) Affective (e.g. punishing, cruel, killing) Evaluative (e.g. annoying, miserable, intense)
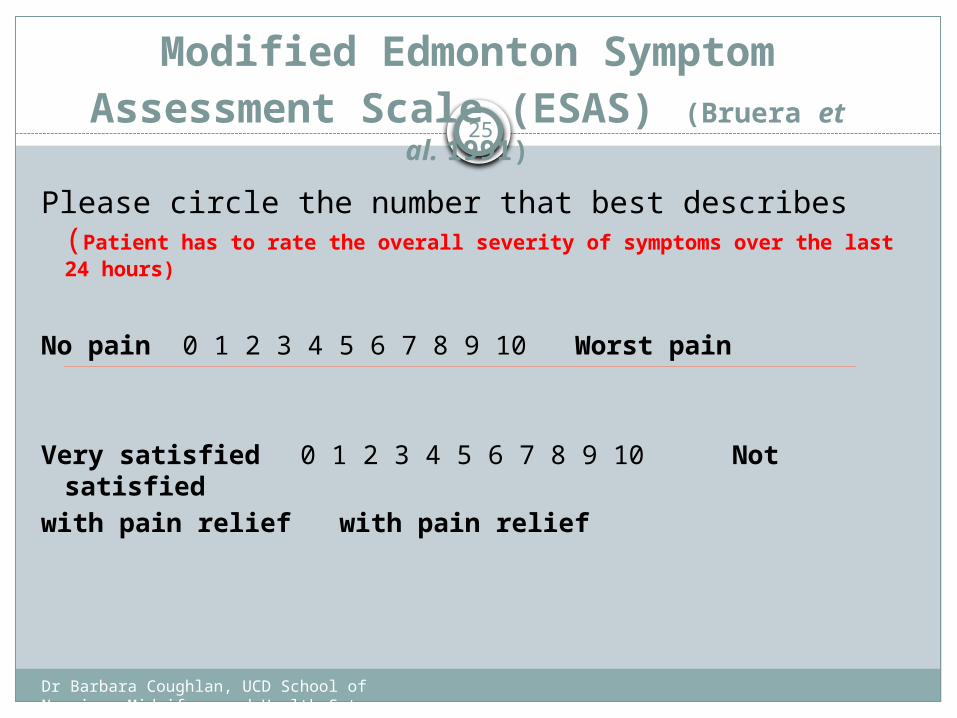
Modified Edmonton Symptom Assessment Scale (ESAS) (Bruera et
al. 1991)
Please circle the number that best describes (Patient has to rate the overall severity of symptoms over the last 24 hours)
No pain 0 1 2 3 4 5 6 7 8 9 10 Worst pain
Very satisfied 0 1 2 3 4 5 6 7 8 9 10 Not satisfied
with pain relief with pain relief
Dr Barbara Coughlan, UCD School of Nursing, Midwifery and Health Sytems
25

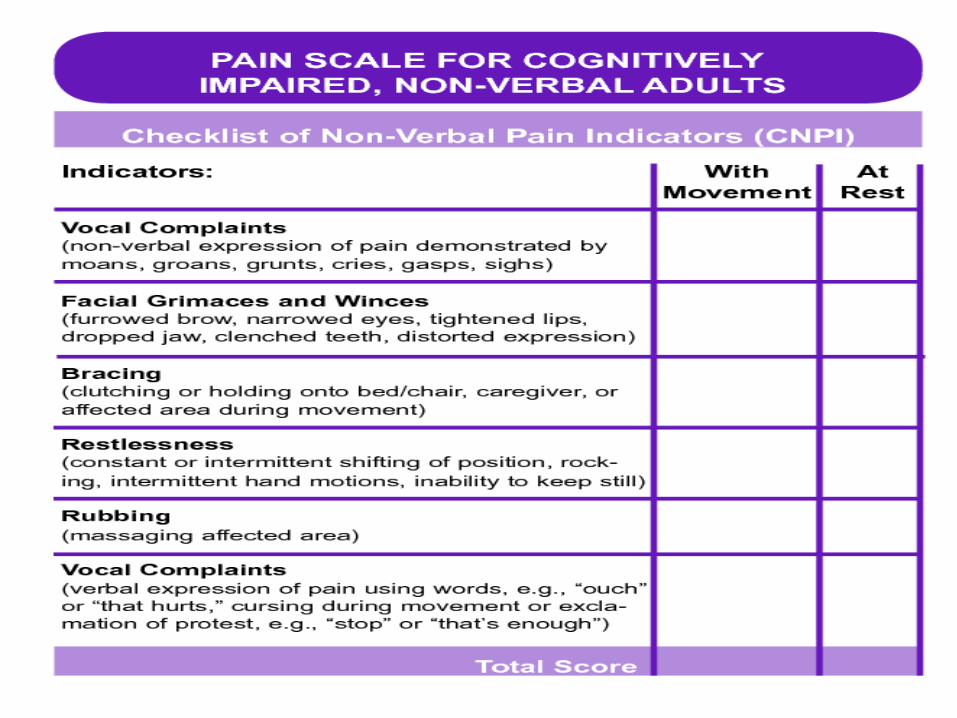
Questions to consider?
How do we measure pain if patient cannot comprehend the question? Young child Patient with dementia Patient Unconscious Patient does not speak English and there is no
interpreter available
Dr Barbara Coughlan, UCD School of Nursing, Midwifery and Health Sytems
26
27
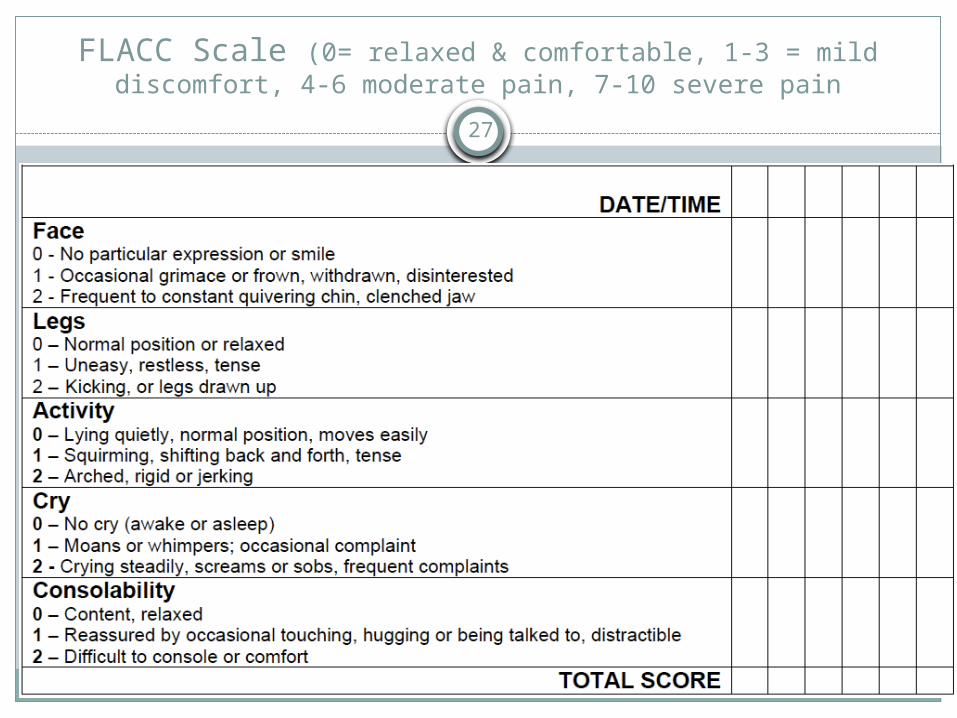
FLACC Scale (0= relaxed & comfortable, 1-3 = mild discomfort, 4-6 moderate pain, 7-10 severe pain

28
29
30
Psychological Indicators of a poor prognosis
Pain catastrophising
Fear avoidance
Poor expectations for recovery

31
Questions or comments

32
Breitbart, W. S. Park, J. Katz, A.M. (2010) Pain. In Holland, J. Et al Psycho-Oncology Oxford University Press
Jarrett, C. (2011) Ouch! The different ways people experience pain. The Psychologist 24 (6) 416-420
Linton, S.J., Shaw, W.S (2011) Impact of Psychological Factors in the Experience of Pain Physical Therapy 91 (5) 700-711
http://www.iasp-pain.orghttp://www.ampainsoc.orghttp://pediatric-pain.ca
Dr Barbara Coughlan, UCD School of Nursing, Midwifery and Health Sytems
33
Resource text bookMorrison V. & Bennett P. (2006). An Introduction to health
Psychology. Pearson: England (Chapter 16 ) Ogden J. (2007) Health Psychology a Textbook 4th Edition.
Open University Press: England (Chapter 12). Breitbart, W. S. Park, J. Katz, A.M. (2010) Pain. In Holland, J. Et al Psycho-Oncology Oxford University Press
Jarrett, C. (2011) Ouch! The different ways people experience pain. The Psychologist 24 (6) 416-420
Linton, S.J., Shaw, W.S (2011) Impact of Psychological Factors in the Experience of Pain Physical Therapy 91 (5) 700-711
http://www.iasp-pain.org http://www.ampainsoc.org http://pediatric-pain.ca
Resources and references
Bowling, A. (2001) Measuring Disease: A Review of Disease-Specific Quality of Life Measurement Scales, Second Edition. Buckingham: Open University Press.
Bowling, A. (2005) Measuring Health: A review of quality of life measurement scales, Third Edition. Maidenhead: Open University Press.
Eccleston C. (2001) Role of Psychology in pain management. British Journal of Anaesthesia. 87 (1): 144-52
Melzack, R (1975) The McGill Pain Questionnaire: major properties and scoring methods. Pain, 1: 277- 299.
Melzack, R. (1987) The short form Mc Gill Pain Questionnaire, Pain (30): 191-197.
Melzack, R (2005) The Mc Gill Pain Questionnaire – from description to measurement, Anaesthesiology. (103): 199.
Melzack, R. and J. Katz (2001) The McGill Pain Questionnaire: Appraisal and current status, pp 15-34 in D.C. Turk and R. Melzack (eds) Handbook of Pain Measurement, Second Edition. New York: Guilford Press.
Dr Barbara Coughlan, UCD School of Nursing, Midwifery and Health Sytems
34