بسم الله الرحمن الرحيم. Postoperative care - Post Anesthesia Care Unit “PACU”
Upload
hirangerCategory
view
11.883download
1
ATLAS HOSPITAL
P.O BOX 1101, Postal Code : 133, MBD East,
RUWI. Sultanate Of Oman.
Phone: 24811706
Fax:24811812
Email: [email protected]
12/4/2015 3:47:40 PM

HOSPITALS
Life Long Health Care
www.AtlasEra.com
During The Presentation
PLEASE:
• Put cell-phones on silent/vibrate mode.
• Take emergency calls outside.
• Maintain silence.
HOSPITALS
Post- Anaesthesia Care
(PAC)
DR RAJESH T EAPEN
ANESTHESIOLOGIST
ATLAS HOSPITAL, RUWI
Introduction
Recovery from anesthesia can range from
completely uncomplicated to life-threatening.
Must be managed by skilled medical and
nursing personnel.
Anesthesiologist plays a key role in optimizing
safe recovery from anesthesia
Must be carried out in a well planned, protocol
based fashion
2/4/2015 3:47:52 PM 5
PAC
Definition
It is the specialized care given
to the patients who have
undergone anaesthetic
management, by a team of
well trained professionals, in a
specially designed, equipped
and designated area of the
hospital
2/4/2015 3:47:52 PM 6

PURPOSES
To enable a successful and faster recovery of the patient post operatively.
To reduce post operative mortality rate.
To reduce the length of hospital stay of the patient.
To provide quality care service.
To reduce hospital and patient cost during post operative period.
2/4/2015 3:47:53 PM 7
PAC Vs. Post operative care
PAC is provided to
anyone who has undergone anaesthesia
anaesthesia might not be for a surgical
procedure
patients undergoing ECT, Narco analysis
patients under going Endoscopies
+
all the patients who have undergone
surgeries
2/4/2015 3:47:53 PM 8
PACU
Definition : It is the
Specially designated
Specially designed
Specially located
Specially staffed
Specially equipped
for a
Specific purpose !
2/4/2015 3:47:53 PM 9
History of the PACU Methods of anesthesia have been available for more
than 160 years, but the PACU has only been common for the past 70 years.
One can trace it to “Lady of the lamp”: F. N.
1920’s and 30’s: several PACU’s opened in the US and abroad.
It was not until after WW II that the number of PACUs increased significantly. This was due to the shortage of nurses in the US.
In 1947 a study was released which showed that over an 11 year period, nearly half of the deaths that occurred during the first 24 hours after surgery were preventable.
1949: having a PACU was considered a standard of care.
2/4/2015 3:47:55 PM 10
PACU Location Should be located close to the Operating Theater
Immediate access to x-ray, blood bank, blood gas and clinical
labs.
An open ward is optimal for patient observation, with at least
one isolation room.
Central nursing station.
Requires good ventilation, because the exposure to waste
anesthetic gases may be hazardous.
National Institute of Occupational Safety (NIOSH) has
established recommended exposure limits of 25 ppm for
nitrous oxide and 2 ppm for volatile anesthetics.
2/4/2015 3:47:55 PM 11
Design of PACU
Size:
Ideal 1.5 PACU bed for every Operating Room
120 square foot per patient
Minimum of 7 feet between beds
Facilities:
Fowler’s cot with side rails
Piped Oxygen, Vacuum and Air
Multiple electrical outlets
Large doors
Good lighting
Isolation for Immuno-compromised patients
2/4/2015 3:47:55 PM 12
PACU
PACU should be sound
proof, painted in soft colour,
isolated and these features
will help the patient to
reduce anxiety and promote
comfort.
2/4/2015 3:47:55 PM 13


2/4/2015 3:47:56 PM 15

2/4/2015 3:47:56 PM 16
PACU Staffing
One nurse to one patient for the first 15
minutes of recovery.
Then one nurse for every two patients.
The anesthesiologist responsible for the
anesthetic remains responsible for managing
the patient in the PACU.
Adequate no. of ancillary staff, such as
technicians, ward boys and female attenders.
2/4/2015 3:47:56 PM 17
PACU Equipment
Multi-parametric monitors (Automated BP,
pulse ox, ECG) and intravenous supports
should be located at each bed.
Area for charting, bed-side supply storage,
suction, and oxygen flow meter at each bed-
side.
Immediately available - Emergency
equipment, Crash cart, Defibrillator.
2/4/2015 3:47:56 PM 18
2/4/2015 3:47:56 PM 19
Routine Post-Anaesthesia Care
Criteria for shifting from
OR---to---PACU
Haemo dynamic stability
Clinical evaluation and
complete recovery from
NM blockade
Maintenance of Oxygen
Saturation
Normothermia
2/4/2015 3:47:56 PM 20
PACU Standards
1. All patients who have received general anesthesia, regional anesthesia, or monitored anesthesia care should receive post-anesthesia management.
2. The patient should be transported to the PACU by a member of the anesthesia care team that is knowledgeable about the patient’s condition.
3. Upon arrival in the PACU, the patient should be re-evaluated and a verbal report should be provided to the nurse.
4. The patient shall be evaluated continually in the PACU.
5. Anaesthesiogist, concerned is responsible for discharge of the patient.
2/4/2015 3:47:56 PM 21
PHASES OF POST OP UNIT
Two phases-
Phase I
Phase II
2/4/2015 3:47:56 PM 22

Phase I
It is the immediate recovery phase and requires intensive nursing care to detect early signs of complication.
Receive a complete patient record from the operating room which to plan post operative care.
It is designated for care of surgical patient immediately after surgery and patient requiring close monitoring
2/4/2015 3:47:56 PM 23
Phase II
Care of the surgical patient who has been transferred from the Phase I post op unit.
Patient requiring less observation and less nursing care than Phase I
This phase is also known as Step down or progressive care unit.
2/4/2015 3:47:56 PM 24
Admission Report
Preoperative history
Intra-operative factors:
Procedure
Type of anesthesia
Estimated Blood Loss (EBL)
Urine output
Assessment and report of current status
Post-operative instructions
2/4/2015 3:47:56 PM 25

Postoperative Pain Management
Intravenous opioids
Diclofenac, I.V. Paracetamol and anti-
inflammatory drugs
Midazolam for anxiety
Epidural : LAAs and their adjuvants
Regional analgesic blocks
PCA (Patient controlled analgesia) and PCEA
2/4/2015 3:47:56 PM 26

2/4/2015 3:47:56 PM 27
2/4/2015 3:47:56 PM 28
2/4/2015 3:47:56 PM 29
2/4/2015 3:47:57 PM 30
2/4/2015 3:47:57 PM 31
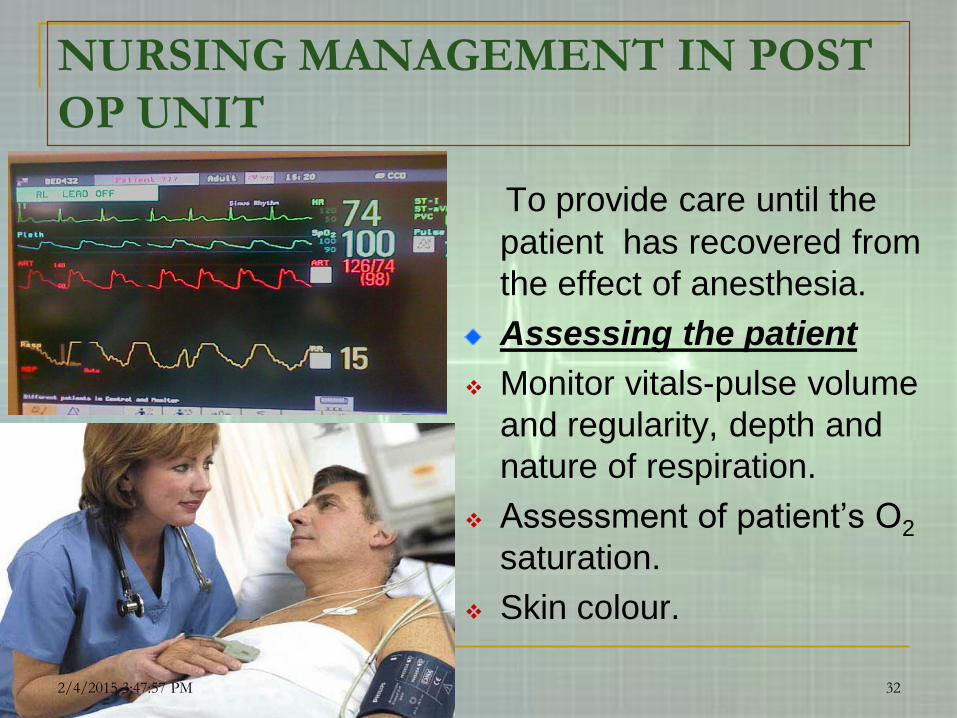
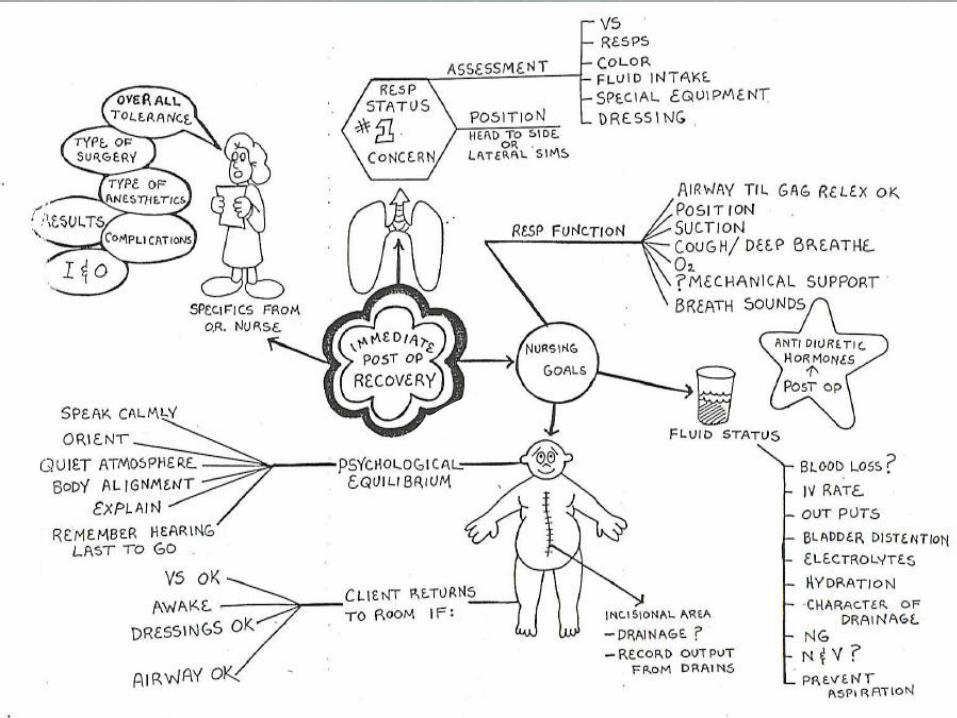
NURSING MANAGEMENT IN POST
OP UNIT
To provide care until the
patient has recovered from
the effect of anesthesia.
Assessing the patient
Monitor vitals-pulse volume
and regularity, depth and
nature of respiration.
Assessment of patient’s O2
saturation.
Skin colour.
2/4/2015 3:47:57 PM 32
KEEP MONITORING VITALS
2/4/2015 3:47:57 PM 33
Check the level of consciousness.
Ability to respond to commands.
2/4/2015 3:47:57 PM 34
MAINTAIN INTAKE AND OUTPUT
2/4/2015 3:47:57 PM 35

Protect airway
By proper positioning of patient’s head.
By clearing airway.
Oxygen therapy.
Pharyngeal obstructioncan occur when the patient lies on the back as there are chances for
tongue to fall back.
2/4/2015 3:47:57 PM 36
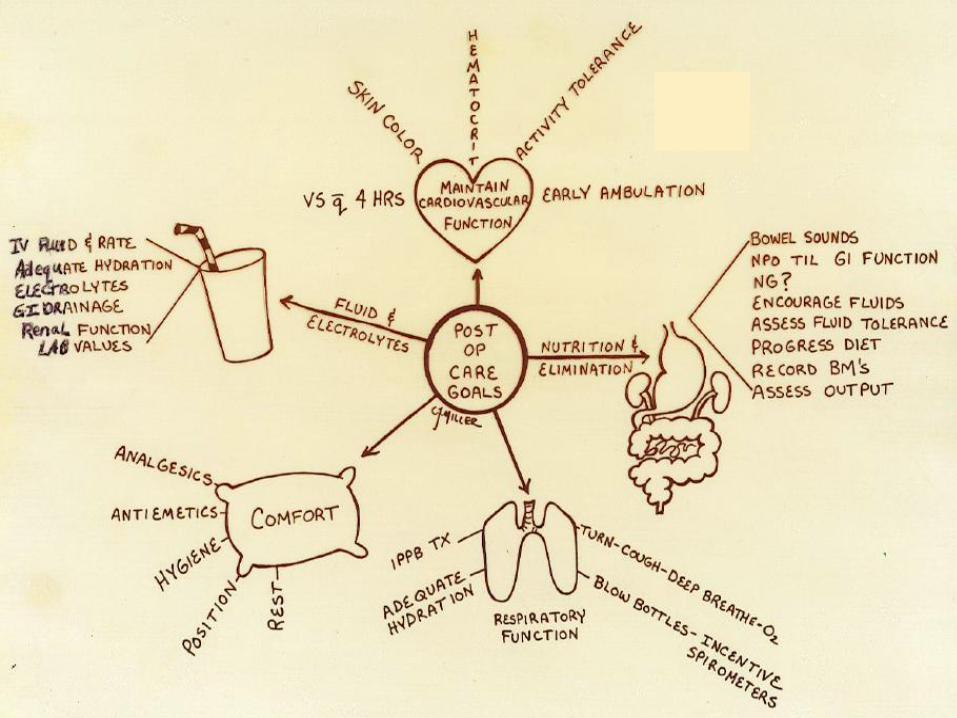
Maintaining IV Stability
Hypovolemic shock: can be avoided by timely administration of IV Fluids, blood and blood products and medication.
Replacement of fluids.[colloids and crystalloids]
Monitor intake and output balance.
2/4/2015 3:47:57 PM 37
ASSESSMENT OF THE SURGICAL SITE
Hemorrhage
It is a serious complication of surgery that can result in death.
It can occur in immediate post operatively or up to several days after surgery.
If left untreated cardiac output decreases and blood pressure and Hblevel will fall rapidly.
2/4/2015 3:47:57 PM 38
Blood transfusion if necessary.
The surgical site + incision should always be inspected.
If bleeding- pressure dressing placed.
If the bleeding is concealed, the patient is taken in OR for emergency exploration of concealed hemorrhage in body cavity.
2/4/2015 3:47:57 PM 39
KEEP THE PATIENT WARM
Use warmer(Bair
Hugger) blankets
Use warm lights
2/4/2015 3:47:58 PM 40

Relieving pain +Anxiety Administer opioid
analgesia as per
Doctor’s order.
Epidural analgesia.
NSAIDS.
Psychological support to
relieve fear+To give
support.
2/4/2015 3:47:58 PM 41
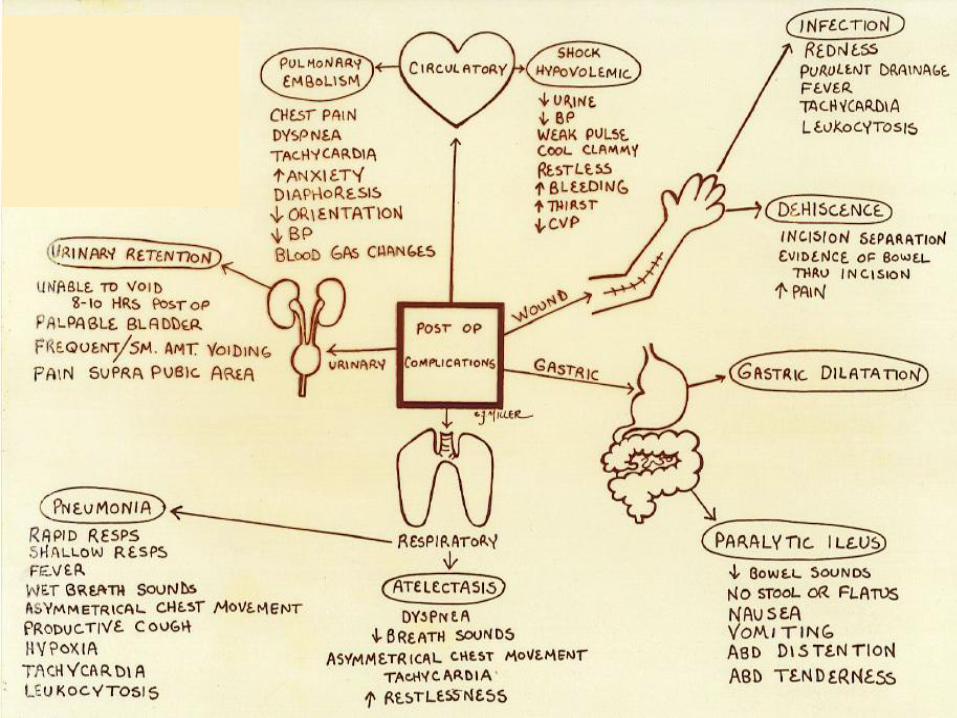
Post Operative Complications
Nausea and Vomiting
Respiratory Complications
Failure to Regain Consciousness
Circulatory Complications
Fever
2/4/2015 3:47:58 PM 42

Controlling Nausea + Vomiting
This is common problem in post operative period.
Medication can be administered as per doctor’s order.
Example:
Inj Metoclopramide
Inj Ondansetron
(Emeset /Zofran)
2/4/2015 3:47:58 PM 43
2/4/2015 3:47:58 PM 44
2/4/2015 3:47:58 PM 45
2/4/2015 3:47:58 PM 46
Discharge criteria from PACU
Neither an arbitrary time limit nor a discharge
score can be used to define a medically
appropriate length stay in the PACU accurately
All patients must be evaluated by
anesthesiologist/trained staff prior to discharge
from PACU
Criteria for discharge developed by the
Anesthesia department
Criteria depends on where the patient is sent –
ward, ICU, home
2/4/2015 3:47:58 PM 47
Discharge criteria from PACU
Easy arousability
Full orientation
Ability to maintain & protect airway
Stable vital signs for at least 15 – 30
minutes
The ability to call for help if necessary
No obvious surgical complication (active
bleeding)
2/4/2015 3:47:58 PM 48
Discharge From the PACU
Standard Aldrete Score: Simple sum of numerical values assigned to
activity, respiration, circulation, consciousness, and oxygen saturation.
A score of 9 out of 10 shows readiness for discharge.
Post-anesthesia Discharge Scoring System: Modification of the Aldrete score which also
includes an assessment of pain, N/V, and surgical bleeding, in addition to vital signs and activity.
Also, a score of 9 or 10 shows readiness for discharge.
2/4/2015 3:47:58 PM 49
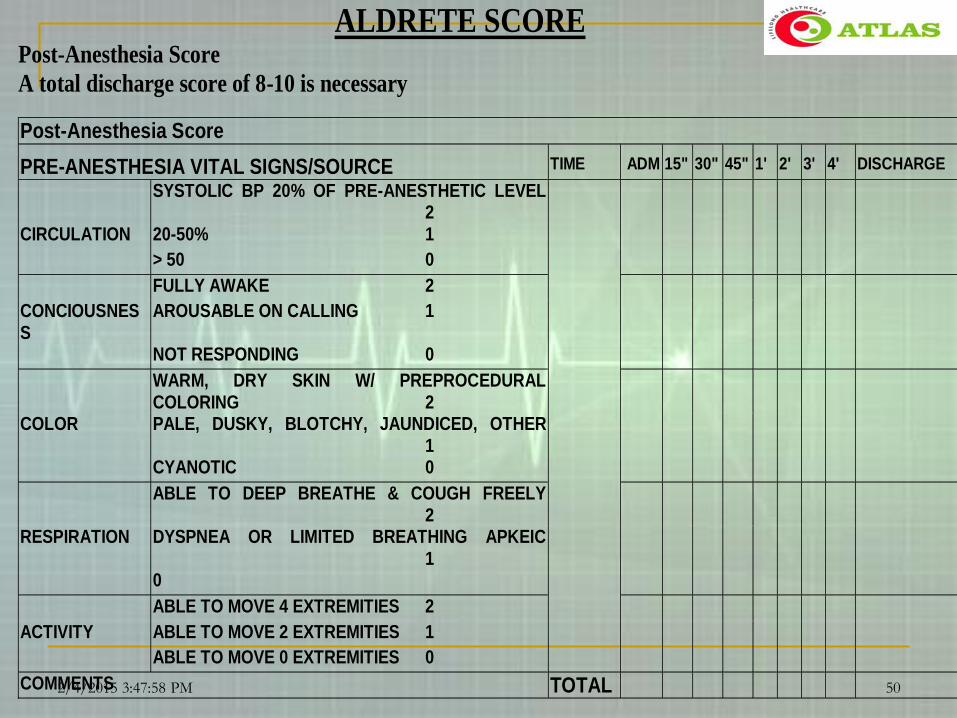
ALDRETE SCORE Post-Anesthesia Score
A total discharge score of 8-10 is necessary
Post-Anesthesia Score
PRE-ANESTHESIA VITAL SIGNS/SOURCE TIME ADM 15" 30" 45" 1' 2' 3' 4' DISCHARGE
SYSTOLIC BP 20% OF PRE-ANESTHETIC LEVEL 2
CIRCULATION 20-50% 1 > 50 0 FULLY AWAKE 2 CONCIOUSNESS
AROUSABLE ON CALLING 1
NOT RESPONDING 0 WARM, DRY SKIN W/ PREPROCEDURAL
COLORING 2
COLOR PALE, DUSKY, BLOTCHY, JAUNDICED, OTHER 1
CYANOTIC 0 ABLE TO DEEP BREATHE & COUGH FREELY
2
RESPIRATION DYSPNEA OR LIMITED BREATHING APKEIC 1
0 ABLE TO MOVE 4 EXTREMITIES 2 ACTIVITY ABLE TO MOVE 2 EXTREMITIES 1 ABLE TO MOVE 0 EXTREMITIES 0 COMMENTS TOTAL
2/4/2015 3:47:58 PM 50
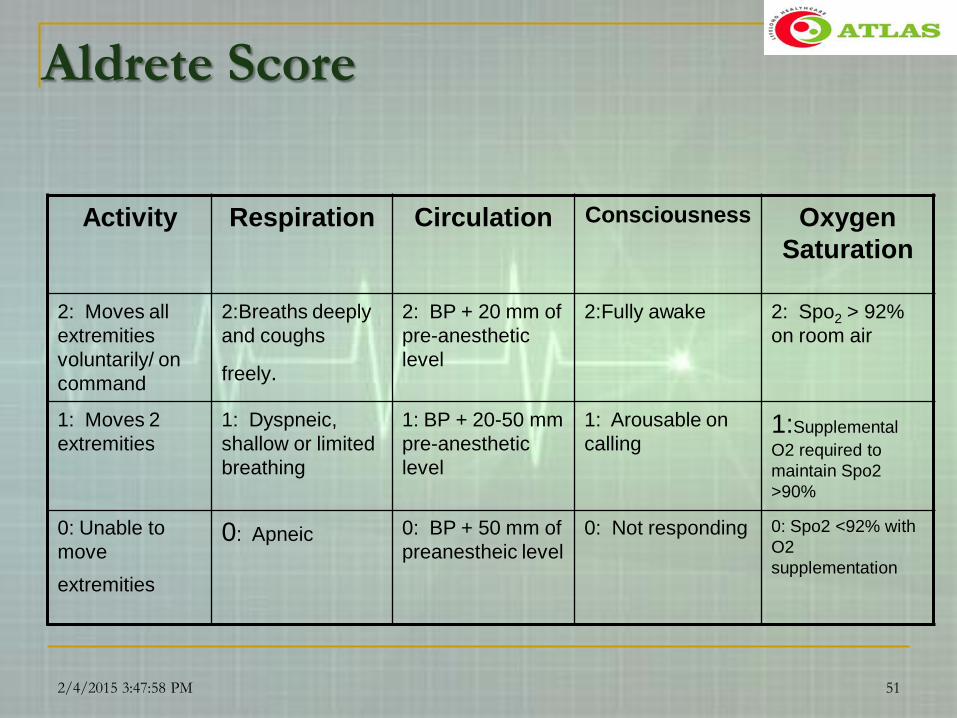
Aldrete Score
Activity Respiration Circulation Consciousness Oxygen
Saturation
2: Moves all
extremities
voluntarily/ on
command
2:Breaths deeply
and coughs
freely.
2: BP + 20 mm of
pre-anesthetic
level
2:Fully awake 2: Spo2 > 92%
on room air
1: Moves 2
extremities
1: Dyspneic,
shallow or limited
breathing
1: BP + 20-50 mm
pre-anesthetic
level
1: Arousable on
calling1:Supplemental
O2 required to
maintain Spo2
>90%
0: Unable to
move
extremities
0: Apneic 0: BP + 50 mm of
preanestheic level
0: Not responding 0: Spo2 <92% with
O2
supplementation
2/4/2015 3:47:58 PM 51
2/4/2015 3:48:01 PM 52
Interpretation of Aldrete’s score
Lowest score = 0 – 2
Score for patient to be shifted to next level of
care = 9
Since some patients on arrival to PACU will meet the
score of 8, it is very illogical to fix a number for
shifting the patient
Ideally it should be decision of the Anesthesiologist
regarding the shifting from the PACU to next level of
care taking into account the anesthetic plan & the
drugs given intra-operatively as well as in PACU
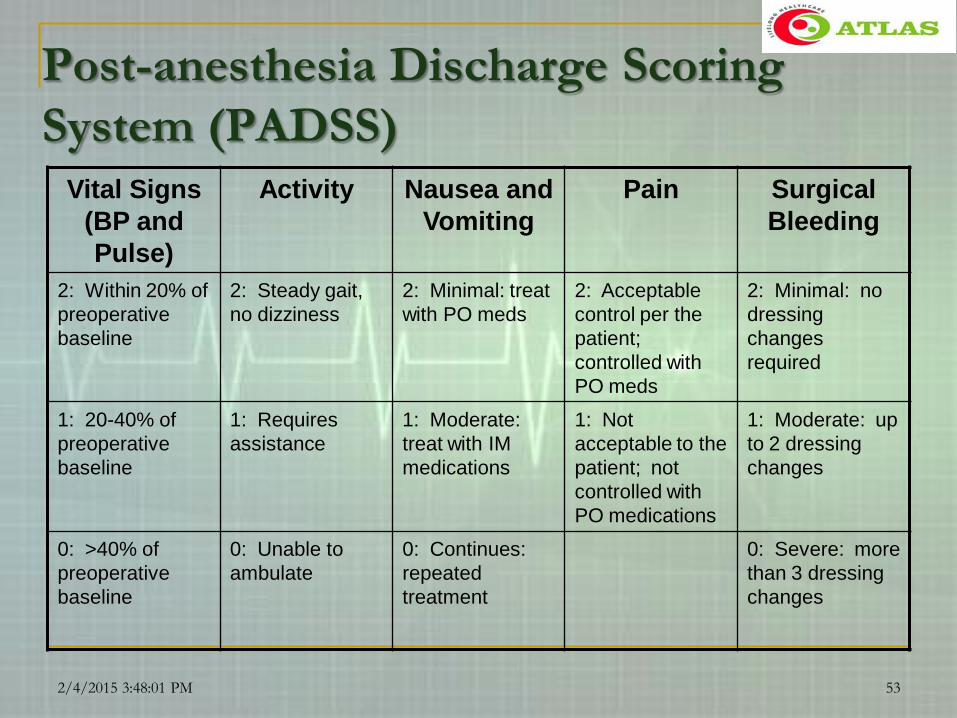
Post-anesthesia Discharge Scoring
System (PADSS)Vital Signs
(BP and
Pulse)
Activity Nausea and
Vomiting
Pain Surgical
Bleeding
2: Within 20% of
preoperative
baseline
2: Steady gait,
no dizziness
2: Minimal: treat
with PO meds
2: Acceptable
control per the
patient;
controlled with
PO meds
2: Minimal: no
dressing
changes
required
1: 20-40% of
preoperative
baseline
1: Requires
assistance
1: Moderate:
treat with IM
medications
1: Not
acceptable to the
patient; not
controlled with
PO medications
1: Moderate: up
to 2 dressing
changes
0: >40% of
preoperative
baseline
0: Unable to
ambulate
0: Continues:
repeated
treatment
0: Severe: more
than 3 dressing
changes
2/4/2015 3:48:01 PM 53

Discharge from the Post Operative Unit
A patient remains in the post op unit, until the patient has fully recovered from anesthesia.
Following measures are used to determine the patient ready for
discharge from post operative unit:-
Stable vital signs
Orientation to Person, Place
Time or events
Adequate oxygen saturation level.
Urine out put at least 30ml/hour
Minimal pain.
Adequate respiratory function.
Aldrete score more than ‘ 9 ‘
2/4/2015 3:48:01 PM 54

Teaching, Patient Self Care
Expected out comes
Immediate post
operative changes
Written instructions like
Wound care
Activity+dietary
recommendation
Medications
Follow up
2/4/2015 3:48:01 PM 55

Safe guidelines for discharging to
home after ambulatory surgery
Patient should be able to stand & take a few
steps ( sit on bed if C/ I for standing)
Should be able to sip fluids
Should be able to urinate
Should be able to repeat post-operative
management
Should be able to identify the escort
(cognitive function)
2/4/2015 3:48:01 PM 56
Summary & Conclusion
Anaesthesia is becoming very sophisticated!
PAC is an absolutely essential care given by a
team of professionals!!
Anaesthesiologists and Trained nursing staff
are the most important members of PACU!!!
Thorough understanding of pathophysiology of
this period is very essential!!!!
With a well organized PACU, one can prevent
lot of post-operative morbidity & mortality!!!!!!
2/4/2015 3:48:01 PM 57

2/4/2015 3:48:01 PM 58
![Comparison of intraoperative Ketamine vs. fentanyl use ... Of... · recovery room (post anesthesia care unit [paCu]; table 3) for each patient, we found that there were significantly](https://static.fdocuments.us/doc/165x107/5e2044fbdefb357fb219bccb/comparison-of-intraoperative-ketamine-vs-fentanyl-use-of-recovery-room.jpg)