بسم الله الرحمن الرحيم. Postoperative care - Post Anesthesia Care Unit “PACU”
34
م ي ح ر ل ا ن م ح ر ل ه ا ل ل م ا س ب
-
Upload
bryan-griffin -
Category
Documents
-
view
224 -
download
1
Transcript of بسم الله الرحمن الرحيم. Postoperative care - Post Anesthesia Care Unit “PACU”
الرحيم الرحمن الله بسم
Postoperative carePostoperative care- -
Post Anesthesia Care UnitPost Anesthesia Care Unit
“PACU”“PACU”
PACU
• Design should match function
• Location:• Close to the operating suite.
• Access to x-ray, blood bank & clinical labs.
• Monitoring equipment
• Emergency equipment
• Personnel

Admission to PACU
• Coordinate prior to arrival,
• Assess airway,
• Administer oxygen,
• Apply monitors,
• Obtain vital signs,
• Receive report from anesthesia personnel.
PACU - ASA Standards
1. Standard IAll patients should receive appropriate care
2. Standard IIAll patients will be accompanied by one of anesthesia team
3. Standard IIIThe patient will be reevaluated & report given to the nurse
4. Standard IVThe patient shall be continually monitored in the PACU
5. Standard VA physician will signing for the patient out of the PACU
Patient Care in the PACU
• Admission
• Apply oxygen and monitor
• Receive report
• Monitor & Observe & Manage
To Achieve
• Cardiovascular stability
• Respiratory stability
• Pain control
• Discharge from PACU
Monitoring in the PACU
• Baseline vital signs.
• Respiration• RR/min, Rythm• Pulse oximetry
• Circulation• PR/min & Blood pressure• ECG
• Level of consciousness
• Pain scores
Initial Assessment
1. Color
2. Respiration
3. Circulation
4. Consciousness
5. Activity
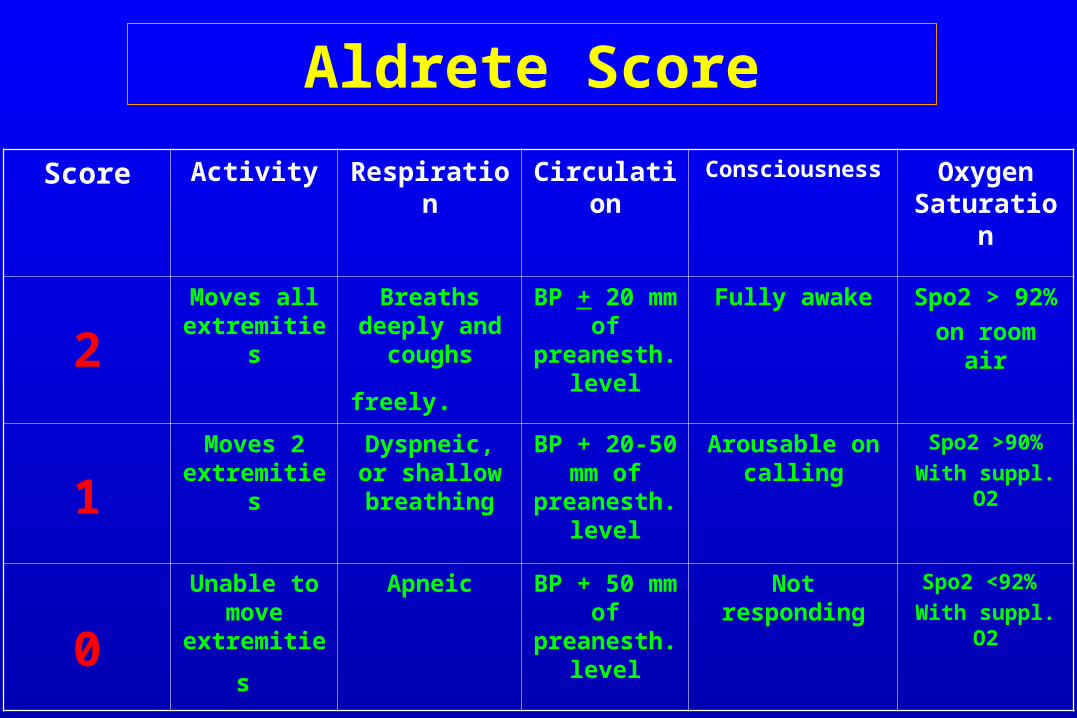
Aldrete Score
Score Activity Respiration Circulation Consciousness Oxygen Saturation
2Moves all
extremitiesBreaths
deeply and coughs
freely.
BP + 20 mm of
preanesth. level
Fully awake Spo2 > 92%
on room air
1Moves 2
extremitiesDyspneic, or
shallow breathing
BP + 20-50 mm of
preanesth. level
Arousable on calling
Spo2 >90%
With suppl. O2
0
Unable to move
extremities
Apneic BP + 50 mm of
preanesth. level
Not responding Spo2 <92%
With suppl. O2
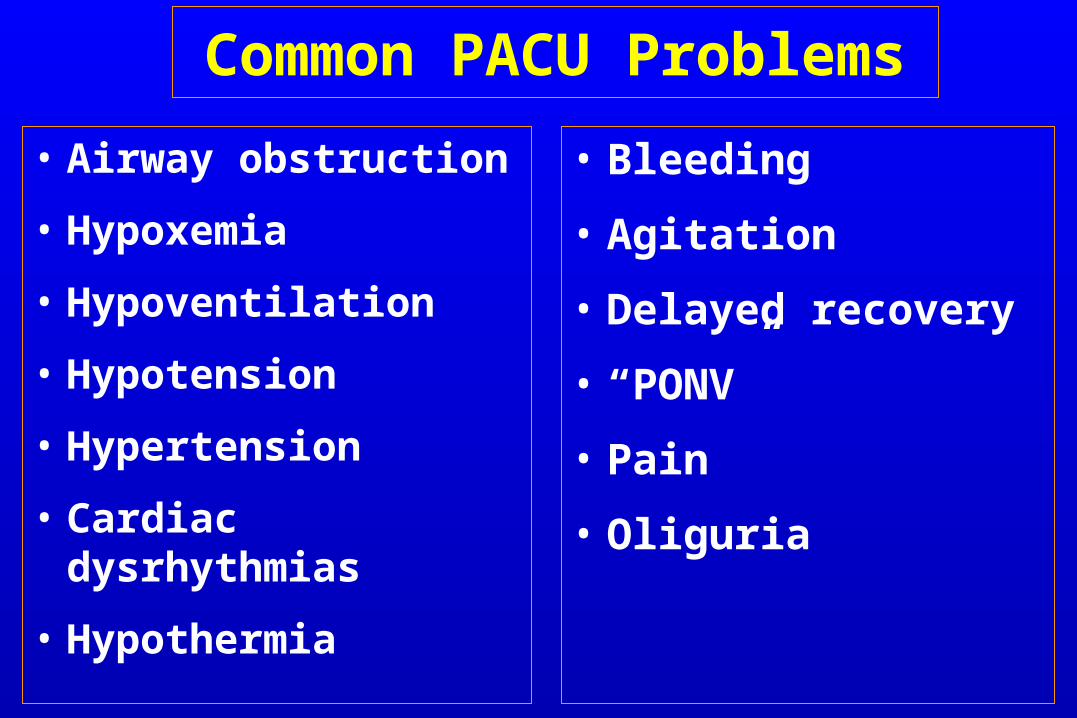
Common PACU Problems
• Airway obstruction
• Hypoxemia
• Hypoventilation
• Hypotension
• Hypertension
• Cardiac dysrhythmias
• Hypothermia
• Bleeding
• Agitation
• Delayed recovery
• “PONV”
• Pain
• Oliguria

Airway Obstruction
• Most common tongue in
posterior pharynx
• May be foreign body
• Inadequate relaxant reversal
• Residual anesthesia

Management of Airway Obstruction
• Patient’s stimulation,
• Suction,
• Oral Airway,
• Nasal Airway,
• Others:• Tracheal intubation• Cricothyroidotomy• Tracheotomy

Hypoventilation
• Residual anesthesia• Narcotics• Inhalation agent• Residual Relaxant
• Post oper - Analgesia• Intravenous• Epidural
Hypoventilation Treatment
• Close observation,
• Assess the problem,
• Treatment of the cause:
• Reverse relaxant
• Reverse narcotic
• Reverse midazolam

Hypertension
• Common causes: e.g. • Pain• Full Bladder
• Hypertensive patients
• Fluid overload
• Excessive use of vasopressors
Hypertension Treatment
• Effective pain control
• Sedation
• Anti-hypertensives:• Beta blockers• Alpha blockers• Hydralazine (Apresoline)• Calcium channel blockers
Hypotension
• Decreased venous return
• Hypovolemia, fluid intake losses
• Bleeding
• Sympathectomy,
• 3rd space loss,
• Left ventricular dysfunction

Treatment of Hypotension
• Initially treat with fluid bolus,
• + Vasopressors,
• + Correction of the cause
Dysrhythmias
• Secondary to
• hypoxemia
• hypercarbia
• Acidosis
• Catecholamines
• Electrolyte abnormalities
• Hypothermia

Dysrhythmia Treatment
• Identify and treat the cause,
• Assure oxygenation,
• Pharmacological

Urine Output
• Oliguria• Hypovolemia,• Surgical trauma,• Impaired renal function,• Mechanical blocking of catheter.
• Treatment:• Assess catheter patency• Fluid bolus• Diuretics e.g. Lasix

Post op Bleeding
Causes:• Usually surgical problem• Coagulopathy
Treatment:• Start i.v. lines push fluids• Blood sample,
- Cross matching, CBC,
- Coagulopathy
• Notify the surgeon,• Correction of the cause
Hypothermia
• Most of patients will arrive cold
• Treatment:
• Get baseline temperature
• Actively rewarm
• Administer oxygen if shivering
• Take care for: • Pediatric,
• Geriatric.
Altered Mental Status
• Reaction to drugs?• Drugs e.g. sedatives, anticholinergics• Intoxication / Drug abusers
• Pain
• Full bladder
• Hypoventilation
• Low COP
• CVA

Treatment of Altered Mental Status
• Reassurances,
• Always protect the patient,
• Evaluate the cause,
• Treatment of symptoms,
• Sedatives / Opioids if necessary.
Delayed Recovery
• Systematic evaluation
• Pre-op status
• Intraoperative events
• Ventilation
• Response to Stimulation
• Cardiovascular status
Delayed Recovery
• The most common cause:
• Residual anesthesia Consider reversal
• Hypothermia,
• Metabolic e.g. diabetic coma,
• Underlying psychiatric problem
• CVA

Postoperative Nausea & Vomiting “PONV”
• Risk factors
• Type & duration of surgery,
• Type of anesthesia,
• Drugs,
• Hormone levels,
• Medical problems,
• Autonomic involvement.

Prevention of PONV
• NPO status
• Droperidol,
• Metoclopramide,
• H2 blockers,
• Ondansetron,
• Acupuncture
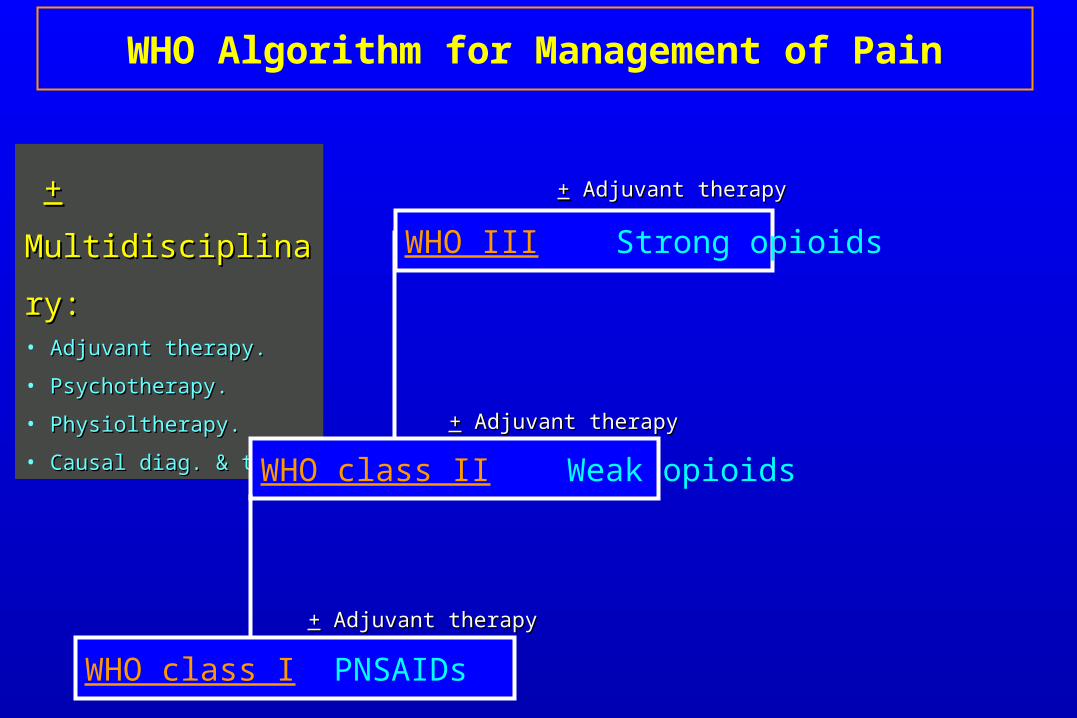
++ Multidisciplinary: Multidisciplinary:• Adjuvant therapy.Adjuvant therapy.
• Psychotherapy.Psychotherapy.
• Physioltherapy.Physioltherapy.
• Causal diag. & ttt.Causal diag. & ttt.
WHO class I PNSAIDs
WHO class II Weak opioids
WHO III Strong opioids
WHO Algorithm for Management of Pain
++ Adjuvant therapy Adjuvant therapy
++ Adjuvant therapy Adjuvant therapy
++ Adjuvant therapy Adjuvant therapy
Regional Blocks
• Local infiltration
• Peripheral nerve blocks
• Plexus block:• UL: Brachial PB• LL: Lumbar PB
• Thoracic: Intercostal, Interpleural, Paravertebral
• Epidural:• Thoracic• Lumbar• Caudal
PACU Discharge Criteria
• Fully Awake,
• Patent airway,
• Good respiratory function,
• Stable vital signs,
• Patency of tubes, catheters, IV’s
• Pain free,
• Reassurance of surgical site.

Postanesthesia Discharge Scoring System
Vital Signs
(PR & ABP)
Activity PONV Pain Surgical Bleeding
2: Within 20% of preoperative baseline
2: Steady gait, no dizziness
2: Minimal: treat with PO meds
2: Acceptable control per the patient; controlled with PO meds
2: Minimal: no dressing changes required
1: 20-40% of preoperative baseline
1: Requires assistance
1: Moderate: treat with IM medications
1: Not acceptable to the patient; not controlled with PO medications
1: Moderate: up to 2 dressing changes
0: >40% of preoperative baseline
0: Unable to ambulate
0: Continues: repeated treatment
0: Severe: more than 3 dressing changes

Thank YouThank YouThank YouThank You
Post-operative Care “PACU”Post-operative Care “PACU”Post-operative Care “PACU”Post-operative Care “PACU”