POC nucleic acid tests for rapid identification of Leishmania · POC nucleic acid tests for rapid...
3
Leishmaniasis: disease, distribution and impact Leishmaniasis is a disease caused by infection with protozoan parasites of the genus Leishmania. These parasites are transmitted to humans by the bite of the female sandfly (genus Phlebotomus or Lutzomyia) that is the vector for transmission between vertebrate hosts. Within the vertebrate hosts, the motile promastigotes from the sandfly gut are phagocytosed by macrophages and change into the non-motile amastigote form [Figure 1]. The amastigotes reproduce, killing host cells: the clinical symptoms of the patient (cutaneous, mucocuta- neous, or visceral) are determined, in part, by the infected cell type. There are about 21 different species of Leishmania that infect humans, and the clinical features of the disease vary with the infecting species and the site of infection [Table 1]. Cutaneous leishmaniasis is common in Afghanistan, Iraq, Iran, Saudi Arabia, Syria, Algeria, Peru, and Brazil. In the Old World (Africa, Asia, Europe) it results primarily from infection with L. major, L. tropica and L. aethiopica. While Leishmania infection in the United States is limited to a few cases, American soldiers engaged in conflicts in the Middle East have seen a number of cutaneous leishmaniasis infections in recent years (about 1,000 cases during Operation Iraqi Freedom) and a few cases of visceral leishmaniasis, prompting the U.S. government to fund the devel- opment of improved leishmaniasis diagnostics. Cutaneous leishmania lesions caused by L. major generally heal faster than lesions from L. tropica infection. L. braziliensis, L. pana- mensis, and L. guyanensis can often cause mucocutaneous leishmania- sis following initial symptoms of cutaneous disease. Visceral leish- maniasis is caused by L. donovani, L. infantum, and L. chagasi infec- tion; L. tropica infection may also result in a viscerotropic leishmani- asis. Therefore, infection with cer- tain strains demands a more aggressive treatment and calls for diagnostic methods that can accu- rately differentiate Leishmania species. Diagnostic options Several facilities for centralised leishmaniasis diagnosis exist worldwide that specialise in microscopy, culture, and nucleic acid testing. The College of American Pathologists (CAP) accredited Leishmania Diagnos- tics Laboratory at the Walter Reed Army Institute of Research (WRAIR) is recognised as an innovator in this field. However, the bulk of diagno- sis in endemic areas is currently performed at local clin- ics, where only traditional methods may be available. L eishmaniasis POC nucleic acid tests for rapid identification of Leishmania 6 Leishmaniasis is endemic in 88 countries with an estimate of at least 1.5 million new infections annually. Treatment depends on accurate diagnosis, often made by a physician familiar with the disease and confirmed by microscopic identification of the parasite from specimens pre- or post-culture. In recent years, faster and more sensitive molecular tests have been devel- oped, but are often inaccessible to local clinics. The release of fully-automated molecular testing systems has the potential to deliver such assays to near-patient sites, improving diagnosis and treatment. disease focus by Dr E.M. Joseph and Dr M. Zillman Figure 1. Fluorescence micrograph images of Giemsa stained (left) or green fluorescent protein (GFP)-expressing L. major pro- mastigotes grown in culture (middle) and amastigotes within a macrophage (right) from a lymph node in a GFP-L. major infected mouse (Giemsa image courtesy of Ltc Peter Weina, MD, PhD, Experimental Therapeutics, Walter Reed Army Institute of Research and fluorescent images courtesy of Abhay Satoskar, MD, PhD, Department of Microbiology, Ohio State University). Table 1. Brief overview of disease types and symptoms asso- ciated with Leishmania infection at different sites. Different species of Leishmania are associated with differ- ent disease types (i.e. L. donovani with kala-azar). Table 2. Survey of published Leishmania diagnostic techniques. Reported time to result and sensitivity may vary greatly between investigators and are presented as a median value. PMID = PubMed identifier which can be used to find original text. Literature reference is meant to be exemplary and not exhaustive. As published in CLI December 2005
-
Upload
phungthien -
Category
Documents
-
view
215 -
download
0
Transcript of POC nucleic acid tests for rapid identification of Leishmania · POC nucleic acid tests for rapid...

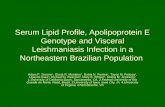
Leishmaniasis: disease, distribution and impactLeishmaniasis is a disease caused by infection withprotozoan parasites of the genus Leishmania. Theseparasites are transmitted to humans by the bite ofthe female sandfly (genus Phlebotomus orLutzomyia) that is the vector for transmissionbetween vertebrate hosts. Within the vertebratehosts, the motile promastigotes from the sandfly gutare phagocytosed by macrophages and change intothe non-motile amastigote form [Figure 1]. Theamastigotes reproduce, killing host cells: the clinicalsymptoms of the patient (cutaneous, mucocuta-neous, or visceral) are determined, in part, by theinfected cell type.
There are about 21 different species of Leishmaniathat infect humans, and the clinical features of thedisease vary with the infecting species and the site ofinfection [Table 1]. Cutaneous leishmaniasis iscommon in Afghanistan, Iraq, Iran, Saudi Arabia,Syria, Algeria, Peru, and Brazil. In the Old World(Africa, Asia, Europe) it results primarily frominfection with L. major, L. tropica and L. aethiopica.While Leishmania infection in the United States islimited to a few cases, American soldiers engaged inconflicts in the Middle East have seen a number ofcutaneous leishmaniasis infections in recent years
(about 1,000 cases during Operation IraqiFreedom) and a few cases of visceral leishmaniasis,prompting the U.S. government to fund the devel-opment of improved leishmaniasis diagnostics.
Cutaneous leishmania lesionscaused by L. major generally healfaster than lesions from L. tropicainfection. L. braziliensis, L. pana-mensis, and L. guyanensis can oftencause mucocutaneous leishmania-sis following initial symptoms ofcutaneous disease. Visceral leish-maniasis is caused by L. donovani,L. infantum, and L. chagasi infec-tion; L. tropica infection may alsoresult in a viscerotropic leishmani-asis. Therefore, infection with cer-tain strains demands a moreaggressive treatment and calls fordiagnostic methods that can accu-rately differentiate Leishmaniaspecies.
Diagnostic optionsSeveral facilities for centralisedleishmaniasis diagnosis existworldwide that specialise inmicroscopy, culture, and nucleicacid testing. The College ofAmerican Pathologists (CAP)accredited Leishmania Diagnos-tics Laboratory at the Walter Reed
Army Institute of Research (WRAIR) is recognised asan innovator in this field. However, the bulk of diagno-sis in endemic areas is currently performed at local clin-ics, where only traditional methods may be available.
L eishmaniasis
POC nucleic acid tests for rapididentification of Leishmania
6
Leishmaniasis is endemic in 88 countries with an estimate of at least 1.5 million new infections annually. Treatment depends
on accurate diagnosis, often made by a physician familiar with the disease and confirmed by microscopic identification of
the parasite from specimens pre- or post-culture. In recent years, faster and more sensitive molecular tests have been devel-
oped, but are often inaccessible to local clinics. The release of fully-automated molecular testing systems has the potential
to deliver such assays to near-patient sites, improving diagnosis and treatment.
dis
ease
fo
cus
by Dr E.M. Joseph and Dr M. Zillman
Figure 1. Fluorescence micrograph images of Giemsa stained (left) or green fluorescent protein (GFP)-expressing L. major pro-mastigotes grown in culture (middle) and amastigotes within a macrophage (right) from a lymph node in a GFP-L. major infectedmouse (Giemsa image courtesy of Ltc Peter Weina, MD, PhD, Experimental Therapeutics, Walter Reed Army Institute of Researchand fluorescent images courtesy of Abhay Satoskar, MD, PhD, Department of Microbiology, Ohio State University).
Table 1. Brief overview of disease types and symptoms asso-ciated with Leishmania infection at different sites.Different species of Leishmania are associated with differ-ent disease types (i.e. L. donovani with kala-azar).
Table 2. Survey of published Leishmania diagnostic techniques. Reported time toresult and sensitivity may vary greatly between investigators and are presented as amedian value. PMID = PubMed identifier which can be used to find original text.Literature reference is meant to be exemplary and not exhaustive.
As published in CLI December 2005

The gold standards for the diagnosis of leishmaniasishave been the traditional parasitology methods of tis-sue biopsy and in vitro culture, but these methods arerapidly giving way to nucleic acid-based tests that offerthe advantages of speed and sensitivity as well as thepotential for near-patient testing by minimally trainedoperators. Available diagnostic methods for all types ofleishmaniasis and their (rough) performance are sum-marised in Table 2, but the main text will focus only onthe diagnosis of cutaneous leishmaniasis.
Lesions which are not on delicate skin may be sam-pled by careful removal of any exudates and adherentmaterial with sterile gauze. The lesion exhibits a raisedmargin and sunken bottom; there is some evidencethat scalpel scrapings obtained with a scalpel from thebottom yield better test samples than margin scrap-ings for both microscopy and PCR [1]. Alternatively,3mm punch biopsies may be taken from the activeborder. Specimens for microscopy are prepareddirectly from scrapings by dispersion of the materialon a slide and imprints of punch-biopsy samples are
produced by rolling thetissue plug along the slide.Slides are fixed, Giemsastained, and examinedunder a high power opti-cal microscope to identifyamastigotes. Theseamastigotes appear round,3µm in diameter, with anintensely stained kineto-plast. Experienced labora-tory personnel are neededto perform microscopicanalysis and the proceduretakes hours, especially forsamples with a low para-site burden. There is a highrate of false negatives[Table 2].
In vitro culture beginswith scraping, punch-biopsy, or needle aspirate(from nodular lesions)samples. The sample iscultured in media under
conditions which allow the promastigote form of theparasite to grow if the parasite is present; promastig-otes are about 20µm in length, 3µm in diameter, witha kinetoplast and obvious flagellum, and are identi-fied via microscopy. Experienced laboratory person-nel are needed to perform culture analysis and theprocedure takes two to three weeks. There are a largenumber of false negative results from such analysis[Table 2].
As neither microscopy nor culture can discriminatebetween morphologically similar Leishmania species,additional diagnostic techniques are used for specia-tion. Isoenzyme analysis, a biochemical method forcharacterising protein variants, is the traditionalmethod used to distinguish species. In this procedure,electrophoretic mobility of different groups ofenzymes from promastigote cultures are compared toLeishmania reference strains. Monoclonal antibodiescan be used to confirm the results of isoenzyme char-acterisation. Identification of the infecting species candrive treatment decisions.
An immunochemistry-based test (rK39 dipstick)[Table 2] is useful for thedetection of visceral leish-maniasis, but not cuta-neous leishmaniasis, sinceeven positive samples donot usually have enoughantibody present to give apositive result. In recentyears, major players in thediagnostics arena havemade nucleic acid testing(NAT) instrumentationand diagnostics availableto larger laboratories. NATdiagnostics rely on thegenetic information (DNAor RNA) of the parasite to
provide detection and/or quantitation, whereas tradi-tional diagnostics have relied on protein. The bulk ofNAT diagnostics utilise polymerase chain reaction(PCR) to amplify the amount of signal in the sample,either directly, or after the enzymatic conversion ofRNA to DNA. Multiple readout technologies havebeen used for the detection of the Leishmania parasite[Table 3] and these differ greatly in sensitivity, ease ofuse, ability to multiplex, and time to result. PublishedNAT tests utilise a number of nucleic acid loci [Table4] that may be more appropriate for either sensitivedetection or species discrimination; the most sensitivetests utilise high copy number targets and are capableof detecting less than a single genome of Leishmaniaparasite.
The NAT assays described in Table 3 all require dedi-cated instrumentation: amplicon length-based analy-ses require slab or capillary electrophoretic instru-mentation and fluorescence-based methods requirespecialised thermocyclers or fluorometers. NAT test-ing traditionally begins with purified nucleic acid,which also requires either dedicated instrumentation,or significant hands-on time. As such instrumenta-tion is large, expensive, and requires skilled operators,NAT testing is usually confined to a laboratory settingand is not readily available in more rural or near-patient settings, meaning that cutaneous leishmania-sis must be diagnosed without the aid of NAT tech-nologies or that samples must be sent to a remote
L eishmaniasis As published in CLI December 2005
Table 3. Survey of nucleic acid tests for Leishmania described in the literature. PMID =PubMed identifier which can be used to find original text. Literature reference is meant tobe exemplary and not exhaustive.
Figure 2. Analysis of fresh or ethanol-preservedLeishmania skin scraping samples in the Liat Analyzer.Sample is added (1), barcoded sample and assay infor-mation is scanned (2), and assay is analysed to providedetected/not detected/indeterminate outcome (3).
Table 4. Survey of nucleic acid diagnostic test targets for Leishmania described in the liter-ature. # Species sequenced is relative to NCBI sequences on 30/11/05 and may not beexhaustive. PMID = PubMed identifier and can be used to find original text. Literature ref-erence is meant to be exemplary and not exhaustive.
Figure 3. Real-time fluorescence detection of Leishmaniatropica DNA in ~10 mg of ethanol-preserved human skinscraping sample using Liat Analyzer. Procedure requires 1hour. Red signal is from Leishmania SSU target and greensignal is from process control DNA contained in the assaythat undergoes all processing steps in parallel with theadded sample.

location for testing. Several companies, including IQuum and Cepheid, are strivingto bring the diagnosis of leishmaniasis closer to the patient; IQuum has launched aclinical trial programme for its lab-in-a-tube (Liat) technology for Leishmaniadetection and DOD/WRAIR plans a clinical trial using Cepheid's SmartCyclertechnology.
The IQuum Liat Analyzer and disposable are shown in Figure 2. The instrumentis small, stand-alone, and easy to operate. The Liat Tube disposable contains allreagents separated by breakable seals. A fresh or ethanol-preserved cutaneousscraping sample is added to the Liat disposable, barcoded information associatedwith the sample and assay is scanned or entered into the instrument, and the dis-posable is inserted into the instrument for analysis [Figure 2]. The Liat Analyzerautomates all steps associated with nucleic acid purification and 4-colour real-time PCR fluorescence detection [Figure 3], providing the user with a direct read-out, in 1 hour, of whether Leishmania parasites were detected in the sample. TheLiat Leishmania genus assay utilises well-characterised technologies, includingthe Wortmann assay that detects conserved SSU sequence from multiple speciesof parasite [2]. A separate assay that targets the heavily sequenced and variable6GDH locus [Table 4] is being tested by IQuum to allow discrimination of L.major and L. tropica. The portability of the Liat Analyzer, coupled with a closed-tube processing and detection format, allow NAT diagnostics to be performed innon-laboratory environments and by non-specialised personnel.
Treatment optionsClinical symptoms and response to treatment vary greatly among leishmaniasispatients. Cutaneous sores can often heal without treatment; but the infection lasts formonths and can cause scarring. The decision about whether or not to give treatmentfor cutaneous leishmaniasis depends upon the number, size, and location of lesions.
The first-line of leishmaniasis treatment is parenteral administration of pen-tavalent antimony compounds, such as sodium stibogluconate (Pentostam) andmeglumine antimonite (Glucantime) [3]. These treatments work but theyrequire week(s) of treatment and have severe side effects. Alternative therapiesinclude amphotericin B deoxycholate and pentamidine, but these compoundshave even more severe side-effects. For some cases of cutaneous leishmaniasis, aless-aggressive treatment course of topical paromycin sulphate may be mostappropriate. The phosphocholine analogue, milefosine (Impavido) is now fre-quently used in India to combat visceral disease.
As a non-pharmaceutical alternative with negligible side-effects, ThermoMed marketsa device for controlled heat treatment of cutaneous leishmaniasis that has been shownin clinical trials to be effective for lesions caused by L. braziliensis and L. mexicana,with cure rates of about 70%, relative to about 30% for control patients.
There is currently no vaccine available for Leishmania, but the World HealthOrganisation Initiative for Vaccine Research recently initiated a plan for develop-ment of a live attenuated Leishmania vaccine.
ConclusionThe recent completion of sequencing of the L. major genome [4] and current sequencing of the L. infantum and L. braziliensis genomes(http://www.sanger.ac.uk/Projects/Protozoa/) facilitate the discovery of drug targetsnovel to Leishmania, and ultimately of a second generation of drugs with greaterselectivity. Synergy of treatment advances and improved molecular diagnostics for theLeishmania parasite has the potential for faster and more informed treatment deci-sions leading to improved patient outcome. The availability of near-patient nucleicacid testing instruments, such as the Liat Analyzer, will help to realise this vision andserve as a model for a wide range of additional clinical applications.
References1. Ramirez JR et al. Diagnosis of cutaneous leishmaniasis in Colombia: the sampling site withinlesions influences the sensitivity of parasitologic diagnosis. J Clin Microbiol 2000; 38: 3768-73.2. Wortmann G et al. Rapid diagnosis of leishmaniasis by fluorogenic polymerase chain reaction.Am J Trop Med Hyg 2001; 65: 583-7.3. Herwaldt BL. Leishmaniasis. Lancet 1999; 354: 1191-9.4. Ivens AC et al. The genome of the kinetoplastid parasite, Leishmania major. Science 2005; 309:436-42.5. Markle WH and Makhoul K. Cutaneous leishmaniasis: recognition and treatment. Am FamPhys 2004; 69: 1455-60.
The authorsElaine Joseph, PhD and Martin Zillmann, PhDIQuum, Inc.214 Lincoln Street, Suite 300,
L eishmaniasis As published in CLI December 2005