Pneumonia
17
7/17/2019 Pneumonia http://slidepdf.com/reader/full/pneumonia-568f5d4002e1c 1/17 36 Pneumonia Kai Man Chan and Charles D Gomersall The management of pneumonia is based on four nd- ings and premises: • Pneumonia is associated with a wide range of largely non-specic clinical features. 1 • Pneumonia can be caused by over 100 organisms. • The relationship between specic clinical features and aetiological organism is insufciently strong to allow a clinical diagnosis of the causative organism. 2 • Early administration of appropriate antibiotics is important. 2 The net result is that the differential diagnosis is wide and treatment should be started before the aetiological agent is known. The differential diagnosis and the likely causative organisms can be narrowed by using epidemiological clues, the most important of which are whether the pneumonia is community-acquired or healthcare-associated and whether the patient is immu- nocompromised. Note that the ora and antibiotic resistance patterns vary from country to country, hos- pital to hospital and even ICU to ICU within a hospital and this must be taken into account. COMMUNITY-ACQUIRED PNEUMONIA Evidence-based guidelines have been issued by the British Thoracic Society, 3 the Infectious Diseases Society of America (IDSA) and American Thoracic Society (ATS) 2 and the European Respiratory Society. 4 Links to these and other pneumonia-related guidelines can be found at the following ‘link page’: http://www. aic.cuhk.edu.hk/web8/Pneumonia%20guidelines.htm. DEFINITION An acute infection of the pulmonary parenchyma that is associated with at least some symptoms of acute infection, accompanied by an acute inltrate on a chest radiograph (CXR), or auscultatory ndings consistent with pneumonia (e.g. altered breath sounds, localised crackles) in a patient not hospitalised or residing in a long-term care facility for ≥14 days prior to the onset of symptoms. The overall incidence is 3–40 per 1000 inhabitants per year, with 40–60% requiring hospital admission. Overall, 10% of patients are admitted to ICU. The overall mortality of hospitalised patient is approxi- mately 10%. 5 AETIOLOGY Table 36.1 gives possible aetiological agents based on epidemiological clues. Streptococcus pneumoniae is the most commonly isolated organism. The next most common bacterial pathogens in patients admitted to ICU are: Legionella species, Haemophilus infuenzae, Enterobacteriaceae species, Staphylococcus aureus and Pseudomonas species. 2 CLINICAL PRESENTATION Pneumonia produces both systemic and respiratory manifestations. Common clinical ndings include fever, sweats, rigors, cough, sputum production, pleuritic chest pain, dyspnoea, tachypnoea, pleural rub and inspiratory crackles. Classic signs of consolidation occur in less than 25% of cases. Multi-organ dysfunc- tion or failure may occur depending on the type and severity of pneumonia. The diagnosis of pneumonia may be more difcult in the elderly. Although the vast majority of elderly patients with pneumonia have respiratory symptoms and signs, over 50% may also have non-respiratory symptoms and over a third may have no systemic signs of infection. INVESTIGATIONS 2,4 Investigations should not delay administration of anti- biotics as delays are associated with an increase in mor- tality. 2 Important investigations include: 1. Chest X-ray (CXR) 2. Arterial blood gases or oximetry 3. Full blood count 4. Serum creatinine, urea and electrolytes 5. Liver function tests 6. Blood cultures (×2) prior to the administration of antimicrobials 7. Sputum (if immediately available) for urgent Gram stain and culture. The usefulness of sputum tests remains debatable because of contamination by upper respiratory tract commensals. However, a
-
Upload
ramadhien-jufran -
Category
Documents
-
view
46 -
download
0
description
Pneumonia
Transcript of Pneumonia

7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 117
36
PneumoniaKai Man Chan and Charles D Gomersall
The management of pneumonia is based on four nd-ings and premises
bull Pneumonia is associated with a wide range of largelynon-specic clinical features1
bull Pneumonia can be caused by over 100 organisms
bull The relationship between specic clinical featuresand aetiological organism is insufciently strong
to allow a clinical diagnosis of the causativeorganism2
bull Early administration of appropriate antibiotics isimportant2
The net result is that the differential diagnosis is wideand treatment should be started before the aetiologicalagent is known The differential diagnosis and thelikely causative organisms can be narrowed by usingepidemiological clues the most important of which arewhether the pneumonia is community-acquired orhealthcare-associated and whether the patient is immu-nocompromised Note that the ora and antibioticresistance patterns vary from country to country hos-pital to hospital and even ICU to ICU within a hospitaland this must be taken into account
COMMUNITY-ACQUIRED PNEUMONIA
Evidence-based guidelines have been issued by theBritish Thoracic Society3 the Infectious Diseases Societyof America (IDSA) and American Thoracic Society(ATS)2 and the European Respiratory Society4 Linksto these and other pneumonia-related guidelines canbe found at the following lsquolink pagersquo httpwww aiccuhkeduhkweb8Pneumonia20guidelineshtm
DEFINITION
An acute infection of the pulmonary parenchyma thatis associated with at least some symptoms of acuteinfection accompanied by an acute inltrate on a chestradiograph (CXR) or auscultatory ndings consistentwith pneumonia (eg altered breath sounds localisedcrackles) in a patient not hospitalised or residing in along-term care facility for ge14 days prior to the onset ofsymptoms
The overall incidence is 3ndash40 per 1000 inhabitantsper year with 40ndash60 requiring hospital admission
Overall 10 of patients are admitted to ICU Theoverall mortality of hospitalised patient is approxi-mately 105
AETIOLOGY
Table 361 gives possible aetiological agents based onepidemiological clues Streptococcus pneumoniae is the
most commonly isolated organism The next mostcommon bacterial pathogens in patients admitted toICU are Legionella species Haemophilus infuenzae Enterobacteriaceae species Staphylococcus aureus and Pseudomonas species2
CLINICAL PRESENTATION
Pneumonia produces both systemic and respiratorymanifestations Common clinical ndings include feversweats rigors cough sputum production pleuriticchest pain dyspnoea tachypnoea pleural rub andinspiratory crackles Classic signs of consolidationoccur in less than 25 of cases Multi-organ dysfunc-tion or failure may occur depending on the type andseverity of pneumonia
The diagnosis of pneumonia may be more difcultin the elderly Although the vast majority of elderlypatients with pneumonia have respiratory symptomsand signs over 50 may also have non-respiratorysymptoms and over a third may have no systemic signsof infection
INVESTIGATIONS24
Investigations should not delay administration of anti-biotics as delays are associated with an increase in mor-
tality2 Important investigations include
1 Chest X-ray (CXR)2 Arterial blood gases or oximetry3 Full blood count4 Serum creatinine urea and electrolytes5 Liver function tests6 Blood cultures (times2) prior to the administration of
antimicrobials7 Sputum (if immediately available) for urgent Gram
stain and culture The usefulness of sputum testsremains debatable because of contamination byupper respiratory tract commensals However a
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 217
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 317
416 Pneumonia
9 Urinary Legionella antigen This test is specic(gt95) In patients with severe Legionnaires diseasesensitivity is 88ndash100 for L pneumophilia serogroup1 (the most commonly reported cause of Legionella infection) Thus a positive result is virtually
single or predominant organism on a Gram stain ofa fresh sample or a heavy growth on culture ofpurulent sputum is likely to be the organismresponsible The nding of many polymorphonu-clear cells (PMN) with no bacteria in a patient whohas not already received antibiotics can reliablyexclude infection by most ordinary bacterial patho-gens Specimens should be obtained by deep coughand be grossly purulent Ideally the specimenshould be obtained before treatment with antimi-crobials if this does not delay administration ofantibiotics and be transported to the laboratoryimmediately for prompt processing to minimise thechance of missing fastidious organisms (eg Strep pneumoniae) Acceptable specimens (in patientswith normal or raised white blood cell counts)should contain gt25 PMN per low-power eld (LPF)and lt10ndash25 squamous epithelial cells (SEC)LPF orgt10 PMN per SEC These criteria should not beused for Mycobacteria and Legionella infectionCertain organisms are virtually always pathogenswhen recovered from respiratory secretions (Box 361) Patients with risk factors for tuberculosis (TB)(Box 362) and particularly those with cough for
more than a month other common symptoms of TBand suggestive radiographic changes should havesputum examined for acid-fast bacilli Sputumcannot be processed for culture for anaerobesowing to contamination by the endogenous anaero-bic ora of the upper respiratory tract In additionto the factors listed in Table 361 foul-smellingsputum lung abscess and empyema should raisesuspicion of anaerobic infection
8 Aspiration of pleural uid for Gram stain culturepH and leucocyte count ndash all patients with a pleuraleffusion gt1 cm thick on a lateral decubitus chestX-ray
Table 361 Possible aetiological agents based on epidemiological cluesmdashcontrsquod
EXPOSURE ORGANISM
Lung abscess Community-acquired meticillin-resistant S aureus oralanaerobes endemic fungi M tuberculosis atypicalmycobacteria
Endobronchial obstruction Anaerobes Strep pneumoniae H influenzae S aureus
Intravenous drug addict S aureus CA-MRSA anaerobes M tuberculosis Streppneumoniae
End-stage renal failure CA-MRSA
OTHERS
Epidemic M pneumoniae influenza virus
Air-conditioning cooling towers hot tubs or hotel or cruise shipstay in previous 2 weeks
Legionella pneumophilia
Presentation of a cluster of cases over a very short periodof time
Bioterrorist agents B anthracis F tularensis Y pestis
Box 361 Organisms that are virtually alwayspathogens when recovered fromrespiratory secretions
LegionellaChlamydiaTBInfluenza para-influenza virus RSV adenovirus hantavirus
SARS coronavirusStronglyloides stercoralisToxoplasma gondi Histoplasma capsulatum
Coccidiodes immitisBlastomycoses dermatitidisCryptococcus neoformans
Box 362 Risk factors for pulmonary tuberculosis
Living in or originating from a developing countryAge (lt5 years middle-aged and elderly men)Alcoholism andor drug addictionHIV infectionDiabetes mellitusLodging-house dwellers
ImmunosuppressionClose contact with smear-positive patientsSilicosisPoverty andor malnutritionPrevious gastrectomySmoking
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 417
Community-acquired pneumonia 417
contamination and colonisation PCR assays are moresensitive than culture for Mycoplasma and Chlamydia species and at least as sensitive for Legionella7 PCRassays also detect Legionella strains other than sero-group 1 The BTS guidelines3 recommend PCR of lowerrespiratory tract sample or if unavailable throat swabfor the diagnosis of Mycoplasma pneumonia PCR for
Chlamydophilia should be performed when invasiverespiratory samples were collected from patients withsevere community-acquired pneumonia The role ofPCR in diagnosing PCP is mainly limited to non-HIVpatients in whom conventional microscopy and stain-ing of induced sputum and BAL have a lower sensitiv-ity than in HIV patients9
MANAGEMENT
GENERAL SUPPORTIVE MEASURES Intravenous uids may be required to correct dehydra-
tion and provide maintenance uid A general approachshould be made to organ support with an emphasis oncorrecting hypoxia
ANTIMICROBIAL REGIMENS Increased mortality among those who do not receiveempirical antibiotics that cover the infecting pathogen(s)is well documented11 Each unit should have its ownregimens tailored to the local ora and antibiotic resist-ance patterns In the absence of such regimens theregimen outlined in Figure 361 may be helpful This
diagnostic of Legionella infection but a negativeresult does not exclude it In areas (eg South Aus-tralia) where other Legionella species are morecommon this test is less helpful
10 Urinary pneumococcal antigen has moderate sensi-tivity (50ndash80) and high specicity (gt90)
11 Microimmunouorescence serology for Chlamydia
pneumoniae IgM A titre ge1 16 is signicant12 HIV serological status
Other investigations should be considered in patientswith risk factors for infection with unusual organismsBronchoalveolar lavage may be useful in immunocom-promised patients those who fail to respond to antibi-otics or those in whom sputum samples cannot beobtained6
Molecular diagnosis (eg PCR-based methods) hasthe advantages of quick results (within 3 hours)enhanced sensitivity independence from organismviability and hence previous antibiotics and theoretical
possibility for determination of antimicrobial suscepti-bility7 Of note it is important to test for genes specicfor the organism in question10 and the sampling siteremains important PCR is most useful when performedon specimens from a normally sterile site For examplePCR for Pneumococcus is positive in 62 of bloodsamples from adult patients with conrmed or proba-ble pneumococcal pneumonia8 whereas blood culturesare positive in only 37 For respiratory specimensunder most circumstances interpretation remainsproblematic due to low specicity related to oral
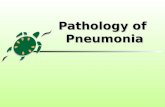
Figure 361 Antibiotic regimens for treatment of severe community-acquired pneumonia in critically ill patients24 Respiratory fluoroquinolones include moxifloxacin and levofloxacin Advanced macrolides include azithromycin andclarithromycin Non-antipseudomonal third-generation cephalosporins include cefotaxime and ceftriaxone
Severe CAP
Aztreonam
and
levofloxacin
Piperacillin-tazobactam or
meropenem or imipenem or
cefepime and ciprofloxacin or
aminoglycoside plus
advanced macrolide
Respiratory
fluoroquinolone
plusmn clindamycin
Non anti-pseudomonal
third-generation cephalosporin
or ampicillin-sulbactam
and respiratory fluoroquinolone
or advanced macrolide
Risk of Pseudomonas
(COPDbronchiectasis
recent hospitalisation
recent antimicrobial
therapy or gross aspiration)
β-lactam
allergy
β-lactam
allergy
NoYes
NoYesNoYes
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 517
418 Pneumonia
should be modied in the light of risk factors (see Table 361) Quinolones may be less appropriate in areas witha high prevalence of TB as their use may mask concur-rent TB infection Appropriate antimicrobial therapyshould be administered within 1 hour of diagnosis412 There is controversy regarding the appropriate changeto empirical therapy based on microbiological nd-
ings24
Changing to narrower-spectrum antimicrobialcover may result in inadequate treatment of the 5ndash38of patients with polymicrobial infection Increasing evi-dence demonstrates improved outcome with combina-tion antimicrobial as compared with monotherapyparticularly in severely ill patients with bacteraemicpneumococcal pneumonia5 Odds ratio of death was15 to 6 for monotherapy as compared with com-bination therapy Benets were seen only in combina-tion therapy with macrolide as part of the regimen butnot in combination with uroquinolone regimen13 For the treatment of drug-resistant Strep pneumoniae (DRSP) the regimens in Figure 361 are probably suit-
able for isolates with a penicillin MIC lt 4 mgL2 Ifthe MIC is ge4 mgL an antipneumococcal uoroqui-nolone vancomycin teicoplanin or linezolid should begiven4
DURATION OF THERAPY No clinical trial has specically addressed this issueCourses as short as 5 days may be sufcient14 IDSAATS guidelines recommend stopping after a minimumof 5 days if the patient is afebrile for 48ndash72 hoursand organ dysfunction has largely resolved2 Shortcourses may be suboptimal for patients with bacterae-mic S aureus pneumonia meningitis or endocarditiscomplicating pneumonia or infection with less commonorganisms (eg Burkholderia pseudomallei or fungi) orPseudomonas aeruginosa Procalcitonin may be useful toguide antibiotic therapy but not all studies have dem-onstrated a benet15
RESPONSE TO THERAPY 2
This can be assessed subjectively (a response is usuallyseen within 1ndash3 days of starting therapy) or objectivelyon the basis of respiratory symptoms fever oxygena-tion WBC count bacteriology CXR changes C-reactiveprotein reduction and procalcitonin reduction of
80ndash90 from peak value The average time to deferves-cence varies with organism severity and patient age(7 days in elderly patients 25 days in young patientswith pneumococcal pneumonia 6ndash7 days in bacterae-mic patients with pneumococcal pneumonia 1ndash2 daysin patients with M pneumoniae pneumonia and 5 daysin patients with Legionella pneumonia) Both blood andsputum cultures are usually negative within 24ndash48hours of treatment although P aeruginosa and M pneu-moniae may persist in the sputum despite effectivetherapy CXR changes lag behind clinical changes withthe speed of change depending on the organism theage of the patient and the presence or absence of comor-
bid illnesses The CXR of most young or middle-aged
patients with bacteraemic pneumococcal pneumonia isclear by 4 weeks but resolution is slower in elderlypatients and patients with underlying illness extensivepneumonia on presentation or Legionella pneumophilia pneumonia
If the patient fails to respond consider the followingquestions
bull Has the patient got pneumonia
bull Are there host factors that explain the failure (egobstruction of bronchus by a foreign body or tumourinadequate host response)
bull Has a complication developed (eg empyema super-infection bronchiolitis obliterans organising pneu-monia metastatic abscess)
bull Is the right drug being given in an adequate dose bythe right route
bull Is the organism resistant to the drug being given
bull Are there other organisms
bull Is the fever a drug fever
Useful investigations include computerised tomogra-phy (CT) of the chest thoracocentesis bronchoalveolarlavage (Table 362) and transbronchial or open-lungbiopsy
PREDICTION OF ADVERSE OUTCOME ANDADMISSION TO ICU Scoring systems have been developed to predictadverse outcome and ICU admission including pneu-monia severity index (PSI) CURB-65 CRB-65 modiedATS major and minor criteria SCAP prediction ruleSMART-COP REA-ICU index and CAP-PIRO16
Although they may help identify the sicker patientsthey should not be used as a sole determinant of ICUadmission as local admission criteria will be affectedby local facilities both in and outside ICU It shouldbe noted that none of the criteria has been prospec-tively demonstrated to avoid late transfers or lowermortality
INFLUENZA PNEUMONIA
Inuenza pneumonia may present with severe respira-tory failure and multi-organ failure However the
pattern of organ failure appears to vary between strainswith H5N1 being associated with a much higher mor-tality and a higher incidence of multi-organ failure thanpandemic H1N117 which itself presented differently toseasonal inuenza In particular trophism for lowerrespiratory tract a higher rate of ICU admission18 anda higher rate of extrapulmonary complications19 wereobserved
Early initiation of oseltamivir is recommended forcritically ill patients although there is no direct evidenceof outcome benet Glucocorticoids do not appear tobe useful and may prolong viral replication20 Bacterialsuperinfection should be considered with Gram-
positive cocci being most frequently isolated21
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 617
Healthcare-associated pneumonia 419
failure and cancer) can cause inltrates on a chest X-rayIdentication of the organism responsible is even moredifcult than in patients with community-acquiredpneumonia owing to the high incidence of oropharyn-
geal colonisation by Gram-negative bacteria Blood cul-tures are positive in only about 6 of cases of nosocomialpneumonia Ventilator-associated pneumonia (VAP) isnosocomial pneumonia arising gt48ndash72 hours after intu-bation Reported incidence of VAP is between 10 and20 for those receiving mechanical ventilation for morethan 48 hours22 It is associated with a higher incidenceof multi-drug-resistant organisms1
PATHOGENESIS
Nosocomial pneumonia is thought to result from micro-aspiration of bacteria colonising the upper respiratory
tract Other routes of infection include macroaspiration
Although there are data demonstrating that surgicalmasks are as effective as N95 (FFP 2) masks in prevent-ing transmission of seasonal inuenza in non-ICU set-tings it is important to note that the capacity for airborne
transmission (and hence the need for N95 masks) isdependent on the exact characteristics of the organismand the frequency of aerosol-generating procedures sothese data should not be extrapolated to other inuenzaviruses and ICU settings
HEALTHCARE-ASSOCIATED PNEUMONIA
Nosocomial pneumonia occurs in 05ndash5 of hospitalpatients with a higher incidence in certain groups(eg postoperative patients and patients in ICU) Diag-nosis may be difcult the clinical features of pneumo-nia are non-specic and many non-infectious conditions
(eg atelectasis pulmonary embolus aspiration heart
Table 362 Procedure for obtaining microbiological samples using bronchoscopy and protected specimen brushingandor bronchoalveolar lavage3549
Infection control In patients suspected of having a disease that is transmitted by the airborne route (egtuberculosis)
bull the risk of transmission should be carefully weighed against the benefits ofbronchoscopy which may generate large numbers of airborne particles
bull perform bronchoscopy in a negative-pressure isolation room
bull consider the use of a muscle relaxant in ventilated patients to prevent coughingbull staff should wear personal protective equipment which should include a fit-tested
negative-pressure respirator (N95 FFP2 or above) as a minimum use of a poweredair-purifying respirator should be considered
General recommendations Suction through the endotracheal tube should be performed before bronchoscopyAvoid suction or injection through the working channel of the bronchoscopePerform protected specimen brushing before bronchoalveolar lavage
Ventilated patients Set F iO2 at 10
Set peak pressure alarm at a level that allows adequate ventilationTitrate ventilator settings against exhaled tidal volumeConsider neuromuscular blockade in addition to sedation in patients at high risk of
complications who are undergoing prolonged bronchoscopy
Protected specimen brushing (PSB) Sample the consolidated segment of lung at subsegmental levelIf purulent secretions are not seen advance the brush until it can no longer be seen but
avoid wedging it in a peripheral positionMove brush back and forth and rotate it several times
Bronchoalveolar lavage (BAL) Wedge tip of bronchoscope into a subsegment of the consolidated segment of lungInject aspirate and collect 20 mL of sterile isotonic saline Do not use this sample for
quantitative microbiology or identification of intracellular organisms It can be used forother microbiological analysis
Inject aspirate and collect additional aliquots of 20ndash60 mLThe total volume of saline injected should be 60ndash200 mL
Complications Hypoxaemia (possibly less with smaller BAL volumes)Arrhythmia
Transient worsening in pulmonary infiltratesBleeding (particularly following PSB)Fever (more common after BAL)
Positive results gt5 of cells in cytocentrifuge preparations of BAL fluid contain intracellular bacteria ORge103 colony-forming unitsmL in PSB specimen ORge104 colony-forming unitsmL in BAL fluid
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 717
420 Pneumonia
worse prognosis In 50 of patients with severehospital-acquired pneumonia and positive bloodcultures there is another source of sepsis
MANAGEMENT
Management is based on the nding that early treat-
ment with antimicrobials that cover all likely patho-gens results in a reduction in morbidity and mortality2 The initial selection of antimicrobials is made on thebasis of epidemiological clues (Fig 362 Table 363)Antimicrobials should be administered within 1 hourof diagnosis12 The results of microbiological investiga-tions are used to narrow antimicrobial cover laterTreatment should be reassessed after 2ndash3 days orsooner if the patient deteriorates (Fig 363) An outlineof management based on an invasive approach is givenin Figure 364
DURATION OF THERAPY
Current ATS guidelines recommend 7 daysrsquo treatmentprovided the aetiological agent is not P aeruginosa orother non-lactose fermenter and the patient has a goodclinical response with resolution of clinical features ofinfection1 The outcome of patients who receive appro-priate initial empirical therapy for ventilator-associatedpneumonia for 8 days is similar to those who receivetreatment for 15 days1
of gastric contents inhaled aerosols haematogenousspread spread from pleural space and direct inocula-tion from ICU personnel
CLINICAL DIAGNOSIS
Diagnosis is based on time of onset (gt48 hours afteradmission to a healthcare facility1) CXR changes (newor progressive inltrates) and either clinical featuresand simple laboratory investigations or the results ofquantitative microbiology Using a clinical approachpneumonia is diagnosed by the nding of a new inl-trate or a change in an inltrate on chest radiographand growth of pathogenic organisms from sputum plusone of the following white-blood-cell (WBC) countgreater than 12times l05L core temperature ge383degCsputum Gram stain with scores of more than two on ascale of four of polymorphonuclear leucocytes andbacteria
INVESTIGATIONSThese are broadly similar to those required incommunity-acquired pneumonia
bull Chest X-ray although studies using a histologicaldiagnosis as the gold standard have demonstratedthat pneumonia may be present despite a normalCXR most denitions of nosocomial pneumoniarequire the presence of new persistent inltrates ona CXR
bull Respiratory secretions considerable controversy sur-rounds the issue of whether invasive bronchoscopicsampling (Table 362) of respiratory secretions is nec-
essary Whether invasive sampling is employed ortracheal aspirates are used empirical broad-spectrumantibiotics should be started while results areawaited The results of microbiological analysis ofrespiratory secretions are used to either stop antibi-otics or narrow the spectrum1 Although the use ofan invasive strategy is associated with a higher like-lihood of modication of initial antimicrobials23 theeffect on important clinical outcome such as mortal-ity antibiotic-free days and organ dysfunction isvariable1 Although tracheal aspirates may predomi-nantly reect the organisms colonising the upper
airway they may be useful in indicating whichorganisms are not responsible for the pneumoniathus allowing the antimicrobial cover to be nar-rowed1 This interpretation is based on the premisethat the predominant route of infection is via theupper respiratory tract From this it can be assumedthat if the organism is not present in the upper res-piratory tract the probability of it being present inthe lung parenchyma is low Certain organisms arevirtually always pathogens when recovered fromrespiratory secretions (see Box 361)
bull Blood cultures identify the aetiological agent in8ndash20 of patients Bacteraemia is associated with a
Figure 362 An outline of initial management ofnosocomial pneumonia based on a non-invasive clinicalapproach1
Two ofuarr or darr WCC
purulent sputum
temp gt38degC
New CXR
infiltrates
Consider acute
tracheobronchitis
Obtain lower respiratory
tract specimens and blood for
microbiological investigations
Risk factorsfor multidrug-resistant
pathogens
Early broad-spectrum
antibiotic therapy
to cover multidrug-
resistant pathogens
Early limited-spectrum
antibiotic therapy
Yes
Yes
No
No
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 817
Healthcare-associated pneumonia 421
inltrate in 48 hours new cavitation or a signicantnew pleural effusion should raise concern If the patientfails to respond consider the diagnosis host factors (egimmunosuppressed debilitated) bacterial factors (egvirulent organism) and therapeutic factors (eg wrongdrug inadequate dose) Review the antibiotics andrepeat cultures It may be useful to broaden the antimi-crobial cover while waiting for the results of investiga-tions Consider invasive sampling of respiratorysecretions computerised tomography or ultrasound ofthe chest (to look for an empyema or abscess) anothersource of infection open-lung biopsy to establish diag-nosis and aetiology or administration of steroids
MORTALITY AND MORBIDITY ATTRIBUTABLE TO VAP Substantial morbidity and mortality associated withVAP have previously been reported22 However acausal relationship is difcult to establish It should benoted that patients who developed VAP tend to be
more severely ill and at higher risk of death not onlyon ICU admission but throughout the course of theirillness Most of the relevant studies were observationaland failed to adequately control confounders likedisease severity evolution of disease progression andICU length of stay with mortality In addition signi-cant heterogeneity exists among these studies Althoughthe presence of VAP is associated with a signicantlylonger ICU length of stay (mean of 61 days 95 CI532ndash687) and increased healthcare cost22 more recentstudies reported that mortality attributable to VAPtends to be small if any2425 The attributable mortalityhas been reported to be 1 on the 30th day of ICU and
RESPONSE TO THERAPY Clinical improvement is usually not apparent for 48ndash72hours and therapy should not be changed during thistime The CXR is of limited value for assessing responseinitial deterioration is common and improvement oftenlags behind clinical response However a rapidly dete-riorating CXR pattern with a gt50 increase in size of
Figure 363 Subsequent management of nosocomialpneumonia based on a non-invasive clinical approach1
Pathogens isolated
from respiratory
specimen
Antibiotics
changedstarted in 7 h
prior to sampling
Adjust antibiotics
according to sensitivities
Continue antibiotics if
high clinical suspicion of
nosocomial pneumonia
Bacterial pneumonia
unlikely
Investigate for other cause
of sepsis and CXR changes
Consider unusual causes
of nosocomial pneumonia
(eg Legionella viruses fungi
Pneumocystis carinii )
Yes
Yes
No
No
Table 363 Recommended initial empirical treatment for nosocomial pneumonia1
SITUATION ANTIBIOTICS
No risk factors for multidrug-resistant pathogens Ceftriaxone or Levofloxacin moxifloxacin or ciprofloxacin or Ampicillinsulbactam or Ertapenem
Antimicrobial therapy in previous 90 days or Current hospitalization for ge5 days or High frequency of antibiotic resistance in the specific
hospital unit or Hospitalisation for 2 days or more in previous 90 days or Residence in nursing home or extended care facility or Home infusion therapy (including antibiotics) or Chronic dialysis within 30 days or Home wound care or Family member with multidrug-resistant pathogen o rImmunosuppression or Bronchiectasis
One ofAntipseudomonal cephalosporin (cefepime or ceftazidime) or Antipseudomonal carbapenem (meropenem or imipenemndash
cilastin) or szlig-lactamszlig-lactamase inhibitor (eg piperacillinndashtazobactam or
cefaperazonendashsulbactam)plus one ofAminoglycoside or Antipseudomonal quinolone (levofloxacin or ciprofloxacin)plus one of the following for patients at high risk of meticillin-
resistant Staphylococcus aureus (MRSA) infectionLinezolid or Vancomycin or
TeicoplaninThe use of dual therapy is not well supported by evidence but it does reduce the probability that the pathogen is resistant to the drugsbeing given If an extended spectrum β-lactamase-producing strain or an Acinetobacter sp is suspected a carbapenem should be givenIf Legionella pneumophilia is suspected use a quinolone Risk factors for MRSA infection in areas with a high incidence of MRSA includediabetes mellitus head trauma coma and renal failure
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 917
422 Pneumonia
or with enlarged cervical nodes or other manifestationsof extrapulmonary disease Clinical disease is seldomfound in asymptomatic individuals even those withstrongly positive tuberculin test (Heaf grade III or IV)The outlook for patients with tuberculosis who requireICU admission is poor In one retrospective study thein-hospital mortality for all patients with tuberculosisrequiring ICU admission was 67 but in those withacute respiratory failure it rose to 8131 The presenta-tion and management of TB in HIV-positive patientsare different (see below)
INVESTIGATION OF PULMONARYTUBERCULOSIS
IDENTIFICATION OF MYCOBACTERIA
Multiple
3233
sputum samples should be collected pref-erably on different days for microscopy for acid-fastbacilli and culture If sputum is not available bronchialwashings taken at bronchoscopy and gastric lavage oraspirate samples should be obtained Gastric aspiratesneed to be neutralised immediately on collection Bron-choscopy and transbronchial biopsy may be useful inpatients with suspected TB but negative sputum smearPleural biopsy is often helpful and mediastinoscopyis occasionally needed in patients with mediastinallymphadenopathy Part of any biopsy specimen shouldalways be sent for culture Nucleic acid amplicationtests on sputum have sensitivity similar to culture in
15 on the 60th day of ICU in a recent study using amulticentre high-quality database and incorporatingnovel statistical methodology to control evolution ofseverity of illness25
PREVENTION
Several guidelines for prevention of ventilator-associated pneumonia and hospital-acquired pneumo-nia have been published26ndash30 Interventions can bedivided into general infection control measures andspecic measures General measures include alcohol-based hand disinfection hospital education programmeon infection control the use of microbiological sur-veillance and a programme to reduce antibiotic pre-scription The major specic recommendations aresummarised in Table 364 There is no evidence that
lsquobundlesrsquo of recommendations are more effective thanthe sum of the individual components
TUBERCULOSIS
The main risk factors are listed in Box 362 Typicalclinical features include fever sweating weight losslassitude anorexia cough productive of mucoid orpurulent sputum haemoptysis chest wall pain dysp-noea localised wheeze and apical crackles Patientsmay also present with unresolved pneumonia pleuraleffusions spontaneous pneumothorax and hoarseness
Figure 364 Management of suspected nosocomial pneumonia based on invasive sampling of respiratory secretions
Bacteria onGram stain
Yes
Yes
No
Yes No Yes No
No
Start antibiotics immediatelyusing PSBBAL specimen
and Gram stain results
Start antibioticsimmediately based onepidemiological clues
Observe look forother infection
Signs ofsevere sepsis
Immediate PSB or BAL beforechangingstarting antimicrobial therapy
+ve cultures +ve cultures
Adjust therapybased on
culture results
Continueadjustantibiotics Look for
other infection
Start antibioticson basisof results
Look forother infection
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1017
Tuberculosis 423
Table 364 Strategies for prevention of ventilator-associated pneumonia
LEVELS OF
RECOMMENDATIONS SPECIFIC INTERVENTIONS REMARKS
Universally recommendedby all guidelines27ndash30
1 Semirecumbent position to 45deg At least 30ndash45deg2 Avoidance of endotracheal intubation3 Preference of oral tracheal route
4 New circuit for a new patient and noschedule change unless soiled or damaged5 Avoidance of flushing of condensate into
lower airway or in-line medication6 HME changes no more frequently than 5ndash7
days7 Continuous aspiration of subglottic suctioning For patients expected to require mechanical
ventilation for gt72 hours
Generally recommendedby most guidelines
1 Preferential use of non-invasiveventilation272830
2 Avoidance of unplanned re-intubation272830
3 Maintenance of endotracheal cuff pressureof about 20 mmHg (266 kPa)272830
4 Closed suctioning2829
No effect on VAP mainly for staff safety5 Chlorhexidine oral decontamination272930
6 Sedation vacation and weaning protocol2728
7 Judicious use of stress ulcer prophylaxis272830
8 Restrictive blood transfusion28
Benefits less clear 1 Preference of HME over heatedhumidifier2830
HME associated with reduction in VAP inpatients ventilated for gt7 days lower cost
2 Silver-sulfadiazine-coated endotrachealtube272830
3 Early tracheostomy (within 7 days ofmechanical ventilation)29
4 Selective decontamination of digestive tract(SDD)272830
Mortality reduction demonstrated when topicalantimicrobials combined with short-course
systemic antibiotics BSAC recommendedSDD in patients expected to requiremechanical ventilation for gt48 hours ETFdiscourage routine use due to concern ofemergence of resistant organisms
Not yet reviewed byguidelines50
1 High-volume low-pressure ultrathin membraneendotracheal tube cuff with SSD
2 Ultrathin membrane cuff with tapered shapeand SSD
3 Low-volume low-pressure endotracheal tubecuff with SSD
4 Balloon device for biofilm removal5 Saline instillation before tracheal suctioning
HME= heat moist exchanger SSD= subglottic secretion drainage
smear-negative patients with pulmonary tuberculosisbut have the advantage of a much more rapid resultThere is however a signicant false-negative rate32
CHEST X-RAY (CXR)A normal CXR almost excludes TB (except inHIV-infected patients) but endobronchial lesionsmay not be apparent and early apical lesions can bemissed Common appearances include patchynodular
shadowing in the upper zones (often bilateral) cavita-tion calcication hilar or mediastinal lymphadenopa-thy (may cause segmental or lobar collapse) pleuraleffusion tuberculomas (dense round or oval shadows)and diffuse ne nodular shadowing throughout thelung elds in miliary TB Inactivity of disease cannot beinferred from the CXR alone This requires three nega-tive sputum samples and failure of any lesion seen onCXR to progress CXR appearances in HIV-positive
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1117
424 Pneumonia
t-tested negative-pressure respirator (N95 FFP2 orhigher) Use of a powered air-purifying respiratorshould be considered when bronchoscopy is being per-formed35 Detailed infection control advice can beobtained via the lsquolink pagersquo (httpwwwaiccuhk eduhkweb8Pneumonia20guidelineshtm)
PNEUMONIA IN THEIMMUNOCOMPROMISED
The lungs are amongst the most frequent targetorgans for infectious complications in the immuno-compromised The incidence of pneumonia is highestamongst patients with haematological malignanciesbone marrow transplant (BMT) recipients and patientswith AIDS
The speed of progression of pneumonia the CXRchanges (Table 365) and the type of immune defectprovide clues to the aetiology Bacterial pneumonias
progress rapidly (1ndash2 days) whereas fungal and proto-zoal pneumonias are less fulminant (several days to aweek or more) Viral pneumonias are usually not ful-minant but on occasions may develop quite rapidlyBronchoscopy is a major component of the investiga-tion of these patients Empirical management based onCXR appearances is outlined in Table 365 Early non-invasive ventilation may improve outcome amongstimmunocompromised patients with fever and bilateralinltrates36
PNEUMOCYSTIS JIROVECI PNEUMONIA (PCP)37
The incidence of this common opportunistic infectionhas fallen substantially in patients with AIDS whoare receiving prophylaxis and effective antiretroviraltherapy with most cases occurring in patients who arenot receiving HIV care or among patients with advancedimmunosuppression The onset is usually insidiouswith dry cough dyspnoea and fever on a backgroundof fatigue and weight loss Crackles in the chest are rareApproximately 15 of patients have a concurrent causefor respiratory failure (eg Kaposi sarcoma TB bacte-rial pneumonia) Useful investigations are
1 CXR classical appearance is diffuse bilateral perihi-
lar interstitial shadowing but in the early stages thisis very subtle and easily missed The initial CXR isnormal in 10 In a further 10 the changes areatypical with focal consolidation or coarse patchyshadowing None of the changes are specic for PCPand may be seen in other lung diseases associatedwith AIDS Pleural effusions hilar or mediastinallymphadenopathy are unusual in PCP but commonin mycobacterial infection or Kaposirsquos sarcoma orlymphoma
2 Induced sputum in this technique the patient inhalesnebulised hypertonic saline from an ultrasonic neb-uliser This provokes bronchorrhoea and the patient
patients with TB differ from those in non-HIV-infectedpatients
TREATMENT OF PULMONARY TB32ndash34
The decision to initiate anti-TB treatment should bebased on level of clinical suspicion results of AFBsmear and sometimes mycobacterial culture If the
initial clinical suspicion is strong and the patient is seri-ously ill attributable to possible TB treatment shouldbe initiated promptly sometimes before the result ofAFB smear Subsequent positivity of AFB smear ornucleic acid amplication test provides support to thecontinuation of treatment Combination chemotherapyconsisting of four drugs is necessary for maximal ef-cacy Treatment is divided into initial phase and con-tinuation phase The most commonly used initialregimen consists of 8 weeks of rifampicin 600 mg daily(450 mg for patients lt50 kg) isoniazid 300 mg dailypyrazinamide 2 g daily (15 g for patients lt50 kg) and
ethambutol 15 mgkg daily as initial phase treatmentEthambutol should be used only in patients who havereasonable visual acuity and who are able to appreciateand report visual disturbances This mandates carefulconsideration in patients who require heavy sedationVisual acuity and colour perception must be assessed(if ethambutol is to be used) and liver and renal func-tion checked before treatment is started Steroids arerecommended for children with endobronchial diseaseand possibly for patients with tuberculous pleuraleffusions Pyridoxine 10 mg daily should be given toprevent isoniazid-induced neuropathy to those atincreased risk (eg patients with diabetes mellitus
chronic renal failure or malnutrition or alcoholic orHIV-positive patients) Negative AFB smear should notdelay initial treatment if clinical suspicion remainshigh Supporting features included chronic coughweight loss characteristic chest X-ray ndings emigra-tion from a high-incidence country no other immediatediagnosis and positive tuberculin test
INFECTION CONTROL
Patients admitted to an ICU with infectious TB or sus-pected of having active pulmonary TB should bemanaged in an isolation room with special ventilation
characteristics including negative pressure Patientsshould be considered infectious if they are coughing orundergoing cough-inducing procedures or if they havepositive AFB smears and they are not on or have juststarted chemotherapy or have a poor clinical or bacte-riological response to chemotherapy3235 Patients withnon-drug-resistant TB should be non-infectious after 2weeks of treatment which includes rifampicin and iso-niazid32 As TB spreads through aerosols it is probablyappropriate to isolate patients who are intubated evenif only their bronchial washings are smear-positiveStaff caring for patients who are smear-positive shouldwear personal protective equipment including a
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1217
Pneumonia in the immunocompromised 425
andor diuretics (patients often uid-overloaded)Approximately 40 of patients with HIV-related PCPwho require mechanical ventilation survive to hospitaldischarge38
Initiation of antiretroviral therapy in patients pre-senting with HIV-related PCP is controversial TheCenters for Disease Control and Prevention (CDC) rec-ommend against doing so in the acute phase but recent
data suggest that the outcome may be improved byinitiation within the rst 4 days of ICU admission39
BACTERIAL PNEUMONIA37
This is the most common cause of acute respiratoryfailure in HIV-positive patients Bacterial pneumonia ismore common in HIV-infected patients than in thegeneral population and tends to be more severe Strep pneumoniae H infuenza Pseudomonas aeruginosa and Saureus are the commonest organisms Nocardia andGram negatives should also be considered Atypicalpathogens (eg Legionella) are rare Response to appro-
priate antibiotics is usually good but may require pro-tracted courses of antibiotics because of high tendencyto relapse Patients with severe immunodeciency(CD4+ T lymphocyte count lt100983221L) and a history ofPseudomonas infection or bronchiectasis or neutropeniashould receive antibiotics that cover P aeruginosa aswell as other Gram negatives The possibility of concur-rent PCP or tuberculosis should be excluded
TUBERCULOSIS
TB may be the initial presentation of AIDS particularlyin sub-Saharan Africa The pattern of TB in HIV patients
coughs up material containing cysts and tropho-zoites The technique is time-consuming and requiresmeticulous technique and is less sensitive thanbronchoscopy but less invasive The possibility ofconcurrent tuberculosis should be consideredand steps taken to minimise the risk of spread ofinfection
3 Bronchoscopy with bronchoalveolar lavage leads to
the diagnosis in over 90 of cases Specimens shouldbe sent for cytology Transbronchial biopsy is notnecessary in most cases PCR using bronchial lavagespecimens may be useful in non-HIV patients withsuspected PCP
Antipneumocystis treatment should be started as soonas the diagnosis is suspected Treatment of choice istrimethoprim plus sulfamethoxazole (co-trimoxazole)20 mgkgday+ 100 mgkgday for 3 weeks plusprednisolone 40 mg orally twice daily for 5 days fol-lowed by 20 mg twice daily for 5 days and then 20 mgper day until the end of PCP treatment Side-effects of
co-trimoxazole are common in HIV patients (nauseavomiting skin rash myelotoxicity) The dose should bereduced by 25 if the WBC count falls Patients whoare intolerant of co-trimoxazole should be treated with
bull pentamidine 4 mgkgday iv or
bull primaquine with clindamycin or
bull trimetrexate with leucovorin (plusmnoral dapsone)
Response to treatment is usually excellent with aresponse time of 4ndash7 days If the patient deteriorates orfails to improve consider (re-)bronchoscopy (is thediagnosis correct) treat co-pathogens and considera short course of high-dose iv methylprednisolone
Table 365 Causes of CXR changes and empirical treatment of pneumonia in the immunocompromised
CHEST X-RAY
APPEARANCE CAUSES
EMPIRICAL TREATMENT FOR
SUSPECTED PNEUMONIA
Diffuse infiltrate CMV and other herpes virusesPneumocystis carinii Bacteria
Aspergillus (advanced)Cryptococcus (uncommon)Non-infectious causes eg drug reaction non-specific
interstitial pneumonitis radiation pneumonitis(uncommon) malignancy leucoagglutinin reaction
Broad-spectrum antibiotics for at least 48 h(eg 3rd-generation cephalosporin andaminoglycoside)
Co-trimoxazoleLung biopsy or lavage within 48 h or full2-week course of co-trimoxazole (dependson patient tolerance of invasive procedure)
Focal infiltrate Gram-negative rodsS aureusAspergillusCryptococcusNocardiaMucorP carinii (uncommon)Tuberculosis
LegionellaNon-infectious causes (eg malignancy non-specificinterstitial pneumonitis radiation pneumonitis)
Broad-spectrum antibioticsIf response seen continue treatment for
2 weeksIf disease progresses lung biopsyaspirate
within 48ndash72 hours or empirical trial ofantifungalplusmn macrolide
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1317
426 Pneumonia
reaction are the most useful tests for demonstratingCMV disease Using thresholds of 10300 000ndash50200 000 positive circulating peripheral WBC the posi-tive predictive value for CMV-pp65 ranges from64 to 82 and the negative predictive value from70 to 954344 Treatment consists of intravenous gan-ciclovir for at least 14 days Foscarnet can be used if
ganciclovir fails
FUNGAL PNEUMONIA
Fungi are rare but important causes of pneumoniaThey can be divided into two main groups based on theimmune response required to combat infection withthese organisms Histoplasma blastomycosis coccidi-oidomycosis paracoccidioidomycosis and Cryptococcus require specic cell-mediated immunity for their controland thus in contrast to infections that are controlled byphagocytic activity the diseases caused by these organ-isms can occur in otherwise healthy individuals
although they cause much more severe illness inpatients with impaired cell-mediated immunity (egpatients infected with HIV and organ transplant recipi-ents) With the exception of Cryptococcus these organ-isms are rarely seen outside North America Aspergillus and Mucor spores are killed by non-immune phago-cytes and as a result these fungi rarely result in clinicalillness in patients with normal neutrophil numbers andfunction
CANDIDIASIS This is effectively a combination of the two types offungal infection in which impaired cell-mediatedimmunity predisposes to mucosal overgrowth withCandida but impaired phagocytic function or numbersis usually required before deep invasion of tissuesoccurs Primary Candida pneumonia (ie isolated lunginfection) is uncommon4145 and more commonly pul-monary lesions are only one manifestation of dissemi-nated candidiasis Even more common is benigncolonisation of the airway with Candida In mostreported cases of primary Candida pneumonia ampho-tericin B has been used In disseminated candidiasistreatment should be directed to treatment of dissemi-nated disease rather than Candida pneumonia per se45
INVASIVE ASPERGILLOSIS 46
This is a highly lethal condition in the immunocom-promised despite treatment and therefore investiga-tion and treatment should be prompt and aggressiveIt is associated with exposure to construction workDenitive diagnosis requires both histological evidenceof acute-angle branching septated non-pigmentedhyphae measuring 2ndash4 983221m in width and cultures yield-ing Aspergillus species from biopsy specimens ofinvolved organs Recovery of Aspergillus species fromrespiratory secretions in immunocompromised butnot immunocompetent patients may indicate invasive
disease with a positive predictive value as high as
depends on the degree of immunosuppression Inpatients with CD4+ T lymphocytes gt350 cells983221L theclinical presentation is similar to TB in non-HIV-infectedpatients although extrapulmonary disease is morecommon In patients with CD4+ T lymphocytes lt350cells983221L extrapulmonary disease (pleuritis pericardi-tis meningitis) is common Severely immunocompro-
mised patients (CD4+
T lymphocytes lt100 cells983221L)may present with severe systemic disease with highfever rapid progression and systemic sepsis In thesepatients lower and middle lobe disease is more commonmiliary disease is common and cavitation is lesscommon Sputum smears and culture may be positiveeven with a normal CXR
Response to treatment is usually rapid Managementof TB in HIV is complex owing to numerous druginteractions consultation with an expert in treatment ofHIV-related TB should be strongly considered Complexinteractions occur between rifamycins (eg rifampicinand rifabutin) and protease inhibitors and non-
nucleoside reverse transcriptase inhibitors used to treatpatients infected with HIV The choice of rifampicin orrifabutin depends on a number of factors includingthe unique and synergistic adverse effects for each indi-vidual combination of rifampicin and anti-HIV drugsand consultation with a physician with experiencein treating both TB and HIV is advised40 IDSA-recommended dosage adjustment for patients receivingantiretrovirals and rifabutin37 can be obtained viathe lsquolink pagersquo (httpwwwaiccuhkeduhkweb8Pneumonia20guidelineshtm) The optimal time forinitiating antiretroviral therapy in patients with TB iscontroversial Early therapy may decrease HIV disease
progression but may be associated with a high inci-dence of adverse effects and an immune reconstitutionreaction37
CMV PNEUMONITIS4142
Risk of infection is highest following allogeneic stemcell transplantation followed by lung transplantationpancreas transplantation and then liver heart and renaltransplantation and advanced AIDS If both the recipi-ent and the donor are seronegative then the risk of bothinfection and disease are negligible If the recipient is
seropositive the risk of infection is approximately 70but the risk of disease is only 20 regardless of theserostatus of the donor However if the recipient isseronegative and the donor is seropositive the risk ofdisease is 70 If steroid pulses and antilymphocyteglobulin are given for treatment of acute rejection therisk of developing disease is markedly increased Infec-tion may be the result of primary infection or reactiva-tion of latent infection It is clinically important butoften difcult to distinguish between CMV infectionand CMV disease and a denitive diagnosis can bemade only histologically Detection of CMV-pp65antigen in peripheral WBC and detection of CMV DNA
or RNA in the blood by quantitative polymerase chain
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1417
Parapneumonic effusion 427
needle aspiration or if there is debris within the uiddrainage using an intercostal drain The diagnosis isconrmed by aspiration of pus
TREATMENT The mainstay of treatment is drainage either by inter-costal drain or by surgical intervention Patients whopresent before the pus is loculated and a brinous peelhas formed on the lung can usually be treated bysimple drainage The combination with intrapleuralbrinolysis may be benecial Optimal surgical man-agement which consists of decortication (open or tho-racoscopic) is indicated if the empyema is moreadvanced or if simple drainage fails This is a majorprocedure and many patients with cardiac or chronicrespiratory disease will not tolerate it Alternatives forthese patients are instillation of thrombolytics into thepleural space or thoracostomy Antibiotics have onlyan adjunctive role Broad-spectrum antibiotic regimenswith anaerobic cover should be used until the resultsof microbiological analysis of the aspirated pus areavailable
AcknowledgementsAll tables and gures are reproduced from ICU web(wwwaiccuhkeduhkweb8) with permission of theauthors
80ndash90 in patients with leukaemia or bone marrowtransplant recipients Bronchoalveolar lavage withsmear culture and antigen detection has excellent spe-cicity and reasonably good positive predictive valuefor invasive aspergillosis in immunocompromisedpatients Although radiological features may give a clueto the diagnosis they are not sufciently specic to be
diagnosticIn acutely ill immunocompromised patients intrave-nous therapy should be initiated if there is suggestiveevidence of invasive aspergillosis while further investi-gations to conrm or refute the diagnosis are carriedout First-line therapy is voriconazole47 Echinocandinsand amphotericin are alternatives
PARAPNEUMONIC EFFUSION
This may be an uncomplicated effusion that resolveswith appropriate treatment of the underlying pneumo-nia or a complicated effusion that develops into an
empyema unless drained Complicated effusions tendto develop 7ndash14 days after initial uid formation Theyare characterised by increasing pleural uid volumecontinued fever and pleural uid of low pH (lt73) thatcontains a large number of neutrophils and may revealorganisms on Gram staining or culture An outline ofmanagement is given in Figure 365
EMPYEMA48
DEFINITION Collection of pus in the pleural space
AETIOLOGY Follows infection of the structures surrounding thepleural space including subdiaphragmatic structuresand chest trauma or may be associated with malig-nancy Anaerobic bacteria usually streptococci orGram-negative rods are responsible for 76 of cases
DIAGNOSIS The diagnosis is usually simple The patient is usuallyseptic and may have a productive cough and chest painThe chest X-ray may show features suggestive of apleural effusion and underlying consolidation but may
also show an abscess cavity with a uid level in whichcase CT scanning will be required to distinguishbetween an abscess and an empyema Ultrasound canbe useful to conrm the presence of uid in the pleuralspace and to determine whether it can be drained by
Figure 365 An approach to the management of
parapneumonic effusions
Parapneumonic effusion
gt 1 cm thick
on lateral decubitus
film
Pleural aspirate
turbid or purulent or
Gram stain +ve
Pleural aspirate
pH
Serial thoracocentesis Treat as empyemaObserve
No
gt72 lt70
70ndash72
No
Yes
Yes
httpwwwexpertconsultcomAccess the complete references list online at
1 American Thoracic Society and Infectious Diseases Society of America Guidelines for the manage-ment of adults with hospital-acquired ventilator-associated and healthcare associated pneumonia
Am J Respir Crit Care Med 2005171388ndash416
2 Mandell LA Wunderink RG Anzueto A et al Infec-tious Diseases Society of AmericaAmerican Tho-racic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin
Infect Dis 200744S27ndash72
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1517
428 Pneumonia
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1617
References 428e1
REFERENCES 1 American Thoracic Society and Infectious Diseases
Society of America Guidelines for the management of adults with hospital-acquired ventilator-associated and healthcare associated pneumonia Am J Respir Crit Care Med 2005171388ndash416
2 Mandell LA Wunderink RG Anzueto A et al Infec-tious Diseases Society of AmericaAmerican Tho-racic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744S27ndash72
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
4 Woodhead M Blasi F Ewig S et al Guidelines for the management of adult lower respiratory tract infections Eur Respir J 2005261138ndash80
5 Torres A Rello J Update in community-acquired and nosocomial pneumonia 2009 Am J Respir Crit
Care Med 2010181782ndash76 Van der Eerden MM Vlaspolder F de Graaff CS et
al Value of intensive diagnostic microbiological investigation in low- and high-risk patients with community-acquired pneumonia Eur J Clin Micro Infect Dis 200524241ndash9
7 Murdoch DR Nucleic acid amplication tests for the diagnosis of pneumonia Clin Infect Dis 2003361162ndash70
8 Blaschke AJ Interpreting assays for the detection of Streptococcus pneumonia Clin Infect Dis 201152(S4)S331ndash7
9 Rello J Lisboa T Lujan M Severity of pneumococcal
pneumonia associated with genomic bacterial load Chest 2009136832ndash4010 Azoulay E Bergeron A Polymerase chain reaction
for diagnosing pneumocystis pneumonia in non-HIV immunocompromised patients with pulmonary inl-trates Chest 2009135(3)655
11 Garcia-Vidal C Fernandez-Sabe N Carratala J Early mortality in patients with community-acquired pneumonia causes and risk factors Eur Respir J200832733ndash9
12 Dellinger RP Carlet JM Masur H et al Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock Intensive Care Med200430536ndash55
13 Metersky ML Ma A Houck PM et al Antibiotics for bacteremic pneumonia improved outcomes with macrolides but not uoroquinolones Chest 2007131466ndash73
14 Dunbar LM Wunderink RG Habib MP High-dose short-course levooxacin for community-acquired pneumonia a new treatment paradigm Clin Infect Dis 200337752ndash60
15 Matthaiou DK Ntani G An ESICM systematic review and meta-analysis of procalcitonin-guided antibiotic therapy algorithms in adult critically ill patients Intensive Care Med 201238940ndash9
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
17 Gruber PC Gomersall CD Joynt GM Avian inu-enza (H5N1) implications for intensive care Inten-sive Care Med 200632823ndash9
18 Belongia EA Irving SA Clinical characteristics and 30-day outcomes for inuenza A 2009 (H1N1) 2008ndash2009 (H1N1) and 2007ndash8 (H3N2) infections JAMA2010304(10)1091
19 Lee N Chan PKS Complications and outcomes of pandemic 2009 inuenza A (H1N1) virus infection in hospitalized adults how do they differ from those in seasonal inuenza J Infect Dis 20112031739ndash47
20 Kim SH Hong SB Corticosteroid treatment in critically ill patients with pandemic inuenza AH1N1 2009 infection analytic strategy using pro-pensity scores Am J Respir Crit Care Med 20111831207ndash14
21 Centers for Disease Control and Prevention (CDC) Bacterial coinfections in lung tissue specimens from
fatal cases of 2009 pandemic inuenza A (H1N1) ndash United States MayndashAugust 2009 MMWR 2009581071ndash4
22 Safdar N Dezfulian C Clinical and economic conse-quences of ventilator-associated pneumonia A sys-tematic review Crit Care Med 200533(10)2184ndash93
23 Shorr AF Sherner JH Invasive approaches to the diagnosis of ventilator-associated pneumonia A meta-analysis Crit Care Med 200533(1)46ndash53
24 Melsen WG Rovers MM Ventilator-associated pneumonia and mortality A systematic review of observational studies Crit Care Med 2009372709ndash18
25 Bekaert M Timsit JF Attributable mortality of ventilator-associated pneumonia A reappraisal using causal analysis Am J Respir Crit Care Med20111841133ndash9
26 CDC Healthcare Infection Control Practices AdvisoryCommittee Guidelines for preventing health-care-associated pneumonia 2003 Recommendations ofCDC and the Healthcare Infection Control PracticesAdvisory Committee Online Available httpwwwcdcgovmmwrpreviewmmwrhtmlrr5303a1htm
27 Cofn SE Klompas M SHEAIDSA practice recom-mendation strategies to prevent ventilator-associated pneumonia in acute care hospitals Infect Control
Hosp Epidemiol 200829S31ndash4028 Masterton RG Galloway A Guidelines for the man-
agement of hospital-acquired pneumonia in the UK Report of the Working Party on Hospital-Acquired Pneumonia of the British Society for Antimicrobial Chemotherapy J Antimicrob Chemother 2008625ndash34
29 VAP Guidelines Committee and the Canadian Critical Care Trials Group Comprehensive evidence-based clinical practice guidelines for ventilator-associated pneumonia prevention J Crit Care 200823126ndash37
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1717
428e2 Pneumonia
30 Torres A Ewig S Dening treating and preventing hospital acquired pneumonia European perspective Intensive Care Med 2009359ndash29
31 Frame RN Johnson MC Eichenhorn MS et al Active tuberculosis in the medical intensive care unit a 15-year retrospective analysis Crit Care Med 1987151012ndash14
32 National Collaborating Centre for Chronic Condi-tions Tuberculosis Clinical diagnosis and manage-ment of tuberculosis and measures for its prevention and control London Royal College of Physicians 2006
33 Small PM Fujiwara PI Management of tuberculosis in the United States N Engl J Med 2001345189ndash200
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
35 Centers for Disease Control and Prevention Guide-lines for preventing the transmission of Mycobacte-rium tuberculosis in health-care settings 2005 MMWR
2005541ndash11936 Hilbert G Gruson D Vargas F et al Noninvasive
ventilation in immunosuppressed patients with pul-monary inltrates fever and acute respiratory failure N Engl J Med 2001344481ndash7
37 Benson CA Kaplan JE Masur H Treating oppor-tunistic infections among HIV-infected adults and adolescents recommendations from CDC the National Institutes of Health and the HIV Medicine AssociationInfectious Diseases Society of America Clin Infect Dis 200540S131ndash235
38 Randall CJ Yarnold PR Schwartz DN et al Improve-ments in outcomes of acute respiratory failure for
patients with human immunodeciency virus-related Pneumocystis carinii pneumonia Am J Respir Crit Care Med 2000162393ndash8
39 Croda J Croda MG Neves A et al Benet of antiret-roviral therapy on survival of human immunode-ciency virus-infected patients admitted to an intensive care unit Crit Care Med 200937(5)1605
40 Centers for Disease Control Updated guidelines for the use of rifabutin or rifampicin for the treatment and prevention of tuberculosis among HIV-infected patients taking protease inhibitors or nonnucleoside reverse transcriptase inhibitors MMWR 200049185ndash9
41 Tamm M The lung in the immunocompromised patient Infectious complications part 2 Respiration199966199ndash207
42 Van der Bij W Speich R Management of cytomega-lovirus infection and disease after solid-organ trans-plantation Clin Infect Dis 200133(Suppl 1)S32ndash7
43 Schaumlfer P Tenschert W Cremaschi L et al Area under the viraemia curve versus absolute viral load utility for predicting symptomatic cytomegalovirus infections in kidney transplant patients J Med Virol20016585ndash9
44 Meyer-Koenig U Weidmann M Kirste G et al Cytomegalovirus infection in organ-transplant recip-ients diagnostic value of pp65 antigen test qualita-tive polymerase chain reaction (PCR) and quantitative
Taqman PCR Transplantation 2004771692ndash8
45 Pappas PG Rex JH Sobel JD Guidelines for treat-ment of candidiasis Clin Infect Dis 200438161ndash89
46 Stevens DA Kan VL Judson MA Practice guidelines for diseases caused by Aspergillus Clin Infect Dis200030696ndash709
47 Herbrecht R Denning DW Patterson TF Voricona-zole versus amphotericin B for primary therapy of invasive aspergillosis N Engl J Med 2002347408ndash15
48 Peek GJ Morcos S Cooper G The pleural cavity BMJ20003201318ndash21
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6

7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 217
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 317
416 Pneumonia
9 Urinary Legionella antigen This test is specic(gt95) In patients with severe Legionnaires diseasesensitivity is 88ndash100 for L pneumophilia serogroup1 (the most commonly reported cause of Legionella infection) Thus a positive result is virtually
single or predominant organism on a Gram stain ofa fresh sample or a heavy growth on culture ofpurulent sputum is likely to be the organismresponsible The nding of many polymorphonu-clear cells (PMN) with no bacteria in a patient whohas not already received antibiotics can reliablyexclude infection by most ordinary bacterial patho-gens Specimens should be obtained by deep coughand be grossly purulent Ideally the specimenshould be obtained before treatment with antimi-crobials if this does not delay administration ofantibiotics and be transported to the laboratoryimmediately for prompt processing to minimise thechance of missing fastidious organisms (eg Strep pneumoniae) Acceptable specimens (in patientswith normal or raised white blood cell counts)should contain gt25 PMN per low-power eld (LPF)and lt10ndash25 squamous epithelial cells (SEC)LPF orgt10 PMN per SEC These criteria should not beused for Mycobacteria and Legionella infectionCertain organisms are virtually always pathogenswhen recovered from respiratory secretions (Box 361) Patients with risk factors for tuberculosis (TB)(Box 362) and particularly those with cough for
more than a month other common symptoms of TBand suggestive radiographic changes should havesputum examined for acid-fast bacilli Sputumcannot be processed for culture for anaerobesowing to contamination by the endogenous anaero-bic ora of the upper respiratory tract In additionto the factors listed in Table 361 foul-smellingsputum lung abscess and empyema should raisesuspicion of anaerobic infection
8 Aspiration of pleural uid for Gram stain culturepH and leucocyte count ndash all patients with a pleuraleffusion gt1 cm thick on a lateral decubitus chestX-ray
Table 361 Possible aetiological agents based on epidemiological cluesmdashcontrsquod
EXPOSURE ORGANISM
Lung abscess Community-acquired meticillin-resistant S aureus oralanaerobes endemic fungi M tuberculosis atypicalmycobacteria
Endobronchial obstruction Anaerobes Strep pneumoniae H influenzae S aureus
Intravenous drug addict S aureus CA-MRSA anaerobes M tuberculosis Streppneumoniae
End-stage renal failure CA-MRSA
OTHERS
Epidemic M pneumoniae influenza virus
Air-conditioning cooling towers hot tubs or hotel or cruise shipstay in previous 2 weeks
Legionella pneumophilia
Presentation of a cluster of cases over a very short periodof time
Bioterrorist agents B anthracis F tularensis Y pestis
Box 361 Organisms that are virtually alwayspathogens when recovered fromrespiratory secretions
LegionellaChlamydiaTBInfluenza para-influenza virus RSV adenovirus hantavirus
SARS coronavirusStronglyloides stercoralisToxoplasma gondi Histoplasma capsulatum
Coccidiodes immitisBlastomycoses dermatitidisCryptococcus neoformans
Box 362 Risk factors for pulmonary tuberculosis
Living in or originating from a developing countryAge (lt5 years middle-aged and elderly men)Alcoholism andor drug addictionHIV infectionDiabetes mellitusLodging-house dwellers
ImmunosuppressionClose contact with smear-positive patientsSilicosisPoverty andor malnutritionPrevious gastrectomySmoking
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 417
Community-acquired pneumonia 417
contamination and colonisation PCR assays are moresensitive than culture for Mycoplasma and Chlamydia species and at least as sensitive for Legionella7 PCRassays also detect Legionella strains other than sero-group 1 The BTS guidelines3 recommend PCR of lowerrespiratory tract sample or if unavailable throat swabfor the diagnosis of Mycoplasma pneumonia PCR for
Chlamydophilia should be performed when invasiverespiratory samples were collected from patients withsevere community-acquired pneumonia The role ofPCR in diagnosing PCP is mainly limited to non-HIVpatients in whom conventional microscopy and stain-ing of induced sputum and BAL have a lower sensitiv-ity than in HIV patients9
MANAGEMENT
GENERAL SUPPORTIVE MEASURES Intravenous uids may be required to correct dehydra-
tion and provide maintenance uid A general approachshould be made to organ support with an emphasis oncorrecting hypoxia
ANTIMICROBIAL REGIMENS Increased mortality among those who do not receiveempirical antibiotics that cover the infecting pathogen(s)is well documented11 Each unit should have its ownregimens tailored to the local ora and antibiotic resist-ance patterns In the absence of such regimens theregimen outlined in Figure 361 may be helpful This
diagnostic of Legionella infection but a negativeresult does not exclude it In areas (eg South Aus-tralia) where other Legionella species are morecommon this test is less helpful
10 Urinary pneumococcal antigen has moderate sensi-tivity (50ndash80) and high specicity (gt90)
11 Microimmunouorescence serology for Chlamydia
pneumoniae IgM A titre ge1 16 is signicant12 HIV serological status
Other investigations should be considered in patientswith risk factors for infection with unusual organismsBronchoalveolar lavage may be useful in immunocom-promised patients those who fail to respond to antibi-otics or those in whom sputum samples cannot beobtained6
Molecular diagnosis (eg PCR-based methods) hasthe advantages of quick results (within 3 hours)enhanced sensitivity independence from organismviability and hence previous antibiotics and theoretical
possibility for determination of antimicrobial suscepti-bility7 Of note it is important to test for genes specicfor the organism in question10 and the sampling siteremains important PCR is most useful when performedon specimens from a normally sterile site For examplePCR for Pneumococcus is positive in 62 of bloodsamples from adult patients with conrmed or proba-ble pneumococcal pneumonia8 whereas blood culturesare positive in only 37 For respiratory specimensunder most circumstances interpretation remainsproblematic due to low specicity related to oral
Figure 361 Antibiotic regimens for treatment of severe community-acquired pneumonia in critically ill patients24 Respiratory fluoroquinolones include moxifloxacin and levofloxacin Advanced macrolides include azithromycin andclarithromycin Non-antipseudomonal third-generation cephalosporins include cefotaxime and ceftriaxone
Severe CAP
Aztreonam
and
levofloxacin
Piperacillin-tazobactam or
meropenem or imipenem or
cefepime and ciprofloxacin or
aminoglycoside plus
advanced macrolide
Respiratory
fluoroquinolone
plusmn clindamycin
Non anti-pseudomonal
third-generation cephalosporin
or ampicillin-sulbactam
and respiratory fluoroquinolone
or advanced macrolide
Risk of Pseudomonas
(COPDbronchiectasis
recent hospitalisation
recent antimicrobial
therapy or gross aspiration)
β-lactam
allergy
β-lactam
allergy
NoYes
NoYesNoYes
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 517
418 Pneumonia
should be modied in the light of risk factors (see Table 361) Quinolones may be less appropriate in areas witha high prevalence of TB as their use may mask concur-rent TB infection Appropriate antimicrobial therapyshould be administered within 1 hour of diagnosis412 There is controversy regarding the appropriate changeto empirical therapy based on microbiological nd-
ings24
Changing to narrower-spectrum antimicrobialcover may result in inadequate treatment of the 5ndash38of patients with polymicrobial infection Increasing evi-dence demonstrates improved outcome with combina-tion antimicrobial as compared with monotherapyparticularly in severely ill patients with bacteraemicpneumococcal pneumonia5 Odds ratio of death was15 to 6 for monotherapy as compared with com-bination therapy Benets were seen only in combina-tion therapy with macrolide as part of the regimen butnot in combination with uroquinolone regimen13 For the treatment of drug-resistant Strep pneumoniae (DRSP) the regimens in Figure 361 are probably suit-
able for isolates with a penicillin MIC lt 4 mgL2 Ifthe MIC is ge4 mgL an antipneumococcal uoroqui-nolone vancomycin teicoplanin or linezolid should begiven4
DURATION OF THERAPY No clinical trial has specically addressed this issueCourses as short as 5 days may be sufcient14 IDSAATS guidelines recommend stopping after a minimumof 5 days if the patient is afebrile for 48ndash72 hoursand organ dysfunction has largely resolved2 Shortcourses may be suboptimal for patients with bacterae-mic S aureus pneumonia meningitis or endocarditiscomplicating pneumonia or infection with less commonorganisms (eg Burkholderia pseudomallei or fungi) orPseudomonas aeruginosa Procalcitonin may be useful toguide antibiotic therapy but not all studies have dem-onstrated a benet15
RESPONSE TO THERAPY 2
This can be assessed subjectively (a response is usuallyseen within 1ndash3 days of starting therapy) or objectivelyon the basis of respiratory symptoms fever oxygena-tion WBC count bacteriology CXR changes C-reactiveprotein reduction and procalcitonin reduction of
80ndash90 from peak value The average time to deferves-cence varies with organism severity and patient age(7 days in elderly patients 25 days in young patientswith pneumococcal pneumonia 6ndash7 days in bacterae-mic patients with pneumococcal pneumonia 1ndash2 daysin patients with M pneumoniae pneumonia and 5 daysin patients with Legionella pneumonia) Both blood andsputum cultures are usually negative within 24ndash48hours of treatment although P aeruginosa and M pneu-moniae may persist in the sputum despite effectivetherapy CXR changes lag behind clinical changes withthe speed of change depending on the organism theage of the patient and the presence or absence of comor-
bid illnesses The CXR of most young or middle-aged
patients with bacteraemic pneumococcal pneumonia isclear by 4 weeks but resolution is slower in elderlypatients and patients with underlying illness extensivepneumonia on presentation or Legionella pneumophilia pneumonia
If the patient fails to respond consider the followingquestions
bull Has the patient got pneumonia
bull Are there host factors that explain the failure (egobstruction of bronchus by a foreign body or tumourinadequate host response)
bull Has a complication developed (eg empyema super-infection bronchiolitis obliterans organising pneu-monia metastatic abscess)
bull Is the right drug being given in an adequate dose bythe right route
bull Is the organism resistant to the drug being given
bull Are there other organisms
bull Is the fever a drug fever
Useful investigations include computerised tomogra-phy (CT) of the chest thoracocentesis bronchoalveolarlavage (Table 362) and transbronchial or open-lungbiopsy
PREDICTION OF ADVERSE OUTCOME ANDADMISSION TO ICU Scoring systems have been developed to predictadverse outcome and ICU admission including pneu-monia severity index (PSI) CURB-65 CRB-65 modiedATS major and minor criteria SCAP prediction ruleSMART-COP REA-ICU index and CAP-PIRO16
Although they may help identify the sicker patientsthey should not be used as a sole determinant of ICUadmission as local admission criteria will be affectedby local facilities both in and outside ICU It shouldbe noted that none of the criteria has been prospec-tively demonstrated to avoid late transfers or lowermortality
INFLUENZA PNEUMONIA
Inuenza pneumonia may present with severe respira-tory failure and multi-organ failure However the
pattern of organ failure appears to vary between strainswith H5N1 being associated with a much higher mor-tality and a higher incidence of multi-organ failure thanpandemic H1N117 which itself presented differently toseasonal inuenza In particular trophism for lowerrespiratory tract a higher rate of ICU admission18 anda higher rate of extrapulmonary complications19 wereobserved
Early initiation of oseltamivir is recommended forcritically ill patients although there is no direct evidenceof outcome benet Glucocorticoids do not appear tobe useful and may prolong viral replication20 Bacterialsuperinfection should be considered with Gram-
positive cocci being most frequently isolated21
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 617
Healthcare-associated pneumonia 419
failure and cancer) can cause inltrates on a chest X-rayIdentication of the organism responsible is even moredifcult than in patients with community-acquiredpneumonia owing to the high incidence of oropharyn-
geal colonisation by Gram-negative bacteria Blood cul-tures are positive in only about 6 of cases of nosocomialpneumonia Ventilator-associated pneumonia (VAP) isnosocomial pneumonia arising gt48ndash72 hours after intu-bation Reported incidence of VAP is between 10 and20 for those receiving mechanical ventilation for morethan 48 hours22 It is associated with a higher incidenceof multi-drug-resistant organisms1
PATHOGENESIS
Nosocomial pneumonia is thought to result from micro-aspiration of bacteria colonising the upper respiratory
tract Other routes of infection include macroaspiration
Although there are data demonstrating that surgicalmasks are as effective as N95 (FFP 2) masks in prevent-ing transmission of seasonal inuenza in non-ICU set-tings it is important to note that the capacity for airborne
transmission (and hence the need for N95 masks) isdependent on the exact characteristics of the organismand the frequency of aerosol-generating procedures sothese data should not be extrapolated to other inuenzaviruses and ICU settings
HEALTHCARE-ASSOCIATED PNEUMONIA
Nosocomial pneumonia occurs in 05ndash5 of hospitalpatients with a higher incidence in certain groups(eg postoperative patients and patients in ICU) Diag-nosis may be difcult the clinical features of pneumo-nia are non-specic and many non-infectious conditions
(eg atelectasis pulmonary embolus aspiration heart
Table 362 Procedure for obtaining microbiological samples using bronchoscopy and protected specimen brushingandor bronchoalveolar lavage3549
Infection control In patients suspected of having a disease that is transmitted by the airborne route (egtuberculosis)
bull the risk of transmission should be carefully weighed against the benefits ofbronchoscopy which may generate large numbers of airborne particles
bull perform bronchoscopy in a negative-pressure isolation room
bull consider the use of a muscle relaxant in ventilated patients to prevent coughingbull staff should wear personal protective equipment which should include a fit-tested
negative-pressure respirator (N95 FFP2 or above) as a minimum use of a poweredair-purifying respirator should be considered
General recommendations Suction through the endotracheal tube should be performed before bronchoscopyAvoid suction or injection through the working channel of the bronchoscopePerform protected specimen brushing before bronchoalveolar lavage
Ventilated patients Set F iO2 at 10
Set peak pressure alarm at a level that allows adequate ventilationTitrate ventilator settings against exhaled tidal volumeConsider neuromuscular blockade in addition to sedation in patients at high risk of
complications who are undergoing prolonged bronchoscopy
Protected specimen brushing (PSB) Sample the consolidated segment of lung at subsegmental levelIf purulent secretions are not seen advance the brush until it can no longer be seen but
avoid wedging it in a peripheral positionMove brush back and forth and rotate it several times
Bronchoalveolar lavage (BAL) Wedge tip of bronchoscope into a subsegment of the consolidated segment of lungInject aspirate and collect 20 mL of sterile isotonic saline Do not use this sample for
quantitative microbiology or identification of intracellular organisms It can be used forother microbiological analysis
Inject aspirate and collect additional aliquots of 20ndash60 mLThe total volume of saline injected should be 60ndash200 mL
Complications Hypoxaemia (possibly less with smaller BAL volumes)Arrhythmia
Transient worsening in pulmonary infiltratesBleeding (particularly following PSB)Fever (more common after BAL)
Positive results gt5 of cells in cytocentrifuge preparations of BAL fluid contain intracellular bacteria ORge103 colony-forming unitsmL in PSB specimen ORge104 colony-forming unitsmL in BAL fluid
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 717
420 Pneumonia
worse prognosis In 50 of patients with severehospital-acquired pneumonia and positive bloodcultures there is another source of sepsis
MANAGEMENT
Management is based on the nding that early treat-
ment with antimicrobials that cover all likely patho-gens results in a reduction in morbidity and mortality2 The initial selection of antimicrobials is made on thebasis of epidemiological clues (Fig 362 Table 363)Antimicrobials should be administered within 1 hourof diagnosis12 The results of microbiological investiga-tions are used to narrow antimicrobial cover laterTreatment should be reassessed after 2ndash3 days orsooner if the patient deteriorates (Fig 363) An outlineof management based on an invasive approach is givenin Figure 364
DURATION OF THERAPY
Current ATS guidelines recommend 7 daysrsquo treatmentprovided the aetiological agent is not P aeruginosa orother non-lactose fermenter and the patient has a goodclinical response with resolution of clinical features ofinfection1 The outcome of patients who receive appro-priate initial empirical therapy for ventilator-associatedpneumonia for 8 days is similar to those who receivetreatment for 15 days1
of gastric contents inhaled aerosols haematogenousspread spread from pleural space and direct inocula-tion from ICU personnel
CLINICAL DIAGNOSIS
Diagnosis is based on time of onset (gt48 hours afteradmission to a healthcare facility1) CXR changes (newor progressive inltrates) and either clinical featuresand simple laboratory investigations or the results ofquantitative microbiology Using a clinical approachpneumonia is diagnosed by the nding of a new inl-trate or a change in an inltrate on chest radiographand growth of pathogenic organisms from sputum plusone of the following white-blood-cell (WBC) countgreater than 12times l05L core temperature ge383degCsputum Gram stain with scores of more than two on ascale of four of polymorphonuclear leucocytes andbacteria
INVESTIGATIONSThese are broadly similar to those required incommunity-acquired pneumonia
bull Chest X-ray although studies using a histologicaldiagnosis as the gold standard have demonstratedthat pneumonia may be present despite a normalCXR most denitions of nosocomial pneumoniarequire the presence of new persistent inltrates ona CXR
bull Respiratory secretions considerable controversy sur-rounds the issue of whether invasive bronchoscopicsampling (Table 362) of respiratory secretions is nec-
essary Whether invasive sampling is employed ortracheal aspirates are used empirical broad-spectrumantibiotics should be started while results areawaited The results of microbiological analysis ofrespiratory secretions are used to either stop antibi-otics or narrow the spectrum1 Although the use ofan invasive strategy is associated with a higher like-lihood of modication of initial antimicrobials23 theeffect on important clinical outcome such as mortal-ity antibiotic-free days and organ dysfunction isvariable1 Although tracheal aspirates may predomi-nantly reect the organisms colonising the upper
airway they may be useful in indicating whichorganisms are not responsible for the pneumoniathus allowing the antimicrobial cover to be nar-rowed1 This interpretation is based on the premisethat the predominant route of infection is via theupper respiratory tract From this it can be assumedthat if the organism is not present in the upper res-piratory tract the probability of it being present inthe lung parenchyma is low Certain organisms arevirtually always pathogens when recovered fromrespiratory secretions (see Box 361)
bull Blood cultures identify the aetiological agent in8ndash20 of patients Bacteraemia is associated with a
Figure 362 An outline of initial management ofnosocomial pneumonia based on a non-invasive clinicalapproach1
Two ofuarr or darr WCC
purulent sputum
temp gt38degC
New CXR
infiltrates
Consider acute
tracheobronchitis
Obtain lower respiratory
tract specimens and blood for
microbiological investigations
Risk factorsfor multidrug-resistant
pathogens
Early broad-spectrum
antibiotic therapy
to cover multidrug-
resistant pathogens
Early limited-spectrum
antibiotic therapy
Yes
Yes
No
No
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 817
Healthcare-associated pneumonia 421
inltrate in 48 hours new cavitation or a signicantnew pleural effusion should raise concern If the patientfails to respond consider the diagnosis host factors (egimmunosuppressed debilitated) bacterial factors (egvirulent organism) and therapeutic factors (eg wrongdrug inadequate dose) Review the antibiotics andrepeat cultures It may be useful to broaden the antimi-crobial cover while waiting for the results of investiga-tions Consider invasive sampling of respiratorysecretions computerised tomography or ultrasound ofthe chest (to look for an empyema or abscess) anothersource of infection open-lung biopsy to establish diag-nosis and aetiology or administration of steroids
MORTALITY AND MORBIDITY ATTRIBUTABLE TO VAP Substantial morbidity and mortality associated withVAP have previously been reported22 However acausal relationship is difcult to establish It should benoted that patients who developed VAP tend to be
more severely ill and at higher risk of death not onlyon ICU admission but throughout the course of theirillness Most of the relevant studies were observationaland failed to adequately control confounders likedisease severity evolution of disease progression andICU length of stay with mortality In addition signi-cant heterogeneity exists among these studies Althoughthe presence of VAP is associated with a signicantlylonger ICU length of stay (mean of 61 days 95 CI532ndash687) and increased healthcare cost22 more recentstudies reported that mortality attributable to VAPtends to be small if any2425 The attributable mortalityhas been reported to be 1 on the 30th day of ICU and
RESPONSE TO THERAPY Clinical improvement is usually not apparent for 48ndash72hours and therapy should not be changed during thistime The CXR is of limited value for assessing responseinitial deterioration is common and improvement oftenlags behind clinical response However a rapidly dete-riorating CXR pattern with a gt50 increase in size of
Figure 363 Subsequent management of nosocomialpneumonia based on a non-invasive clinical approach1
Pathogens isolated
from respiratory
specimen
Antibiotics
changedstarted in 7 h
prior to sampling
Adjust antibiotics
according to sensitivities
Continue antibiotics if
high clinical suspicion of
nosocomial pneumonia
Bacterial pneumonia
unlikely
Investigate for other cause
of sepsis and CXR changes
Consider unusual causes
of nosocomial pneumonia
(eg Legionella viruses fungi
Pneumocystis carinii )
Yes
Yes
No
No
Table 363 Recommended initial empirical treatment for nosocomial pneumonia1
SITUATION ANTIBIOTICS
No risk factors for multidrug-resistant pathogens Ceftriaxone or Levofloxacin moxifloxacin or ciprofloxacin or Ampicillinsulbactam or Ertapenem
Antimicrobial therapy in previous 90 days or Current hospitalization for ge5 days or High frequency of antibiotic resistance in the specific
hospital unit or Hospitalisation for 2 days or more in previous 90 days or Residence in nursing home or extended care facility or Home infusion therapy (including antibiotics) or Chronic dialysis within 30 days or Home wound care or Family member with multidrug-resistant pathogen o rImmunosuppression or Bronchiectasis
One ofAntipseudomonal cephalosporin (cefepime or ceftazidime) or Antipseudomonal carbapenem (meropenem or imipenemndash
cilastin) or szlig-lactamszlig-lactamase inhibitor (eg piperacillinndashtazobactam or
cefaperazonendashsulbactam)plus one ofAminoglycoside or Antipseudomonal quinolone (levofloxacin or ciprofloxacin)plus one of the following for patients at high risk of meticillin-
resistant Staphylococcus aureus (MRSA) infectionLinezolid or Vancomycin or
TeicoplaninThe use of dual therapy is not well supported by evidence but it does reduce the probability that the pathogen is resistant to the drugsbeing given If an extended spectrum β-lactamase-producing strain or an Acinetobacter sp is suspected a carbapenem should be givenIf Legionella pneumophilia is suspected use a quinolone Risk factors for MRSA infection in areas with a high incidence of MRSA includediabetes mellitus head trauma coma and renal failure
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 917
422 Pneumonia
or with enlarged cervical nodes or other manifestationsof extrapulmonary disease Clinical disease is seldomfound in asymptomatic individuals even those withstrongly positive tuberculin test (Heaf grade III or IV)The outlook for patients with tuberculosis who requireICU admission is poor In one retrospective study thein-hospital mortality for all patients with tuberculosisrequiring ICU admission was 67 but in those withacute respiratory failure it rose to 8131 The presenta-tion and management of TB in HIV-positive patientsare different (see below)
INVESTIGATION OF PULMONARYTUBERCULOSIS
IDENTIFICATION OF MYCOBACTERIA
Multiple
3233
sputum samples should be collected pref-erably on different days for microscopy for acid-fastbacilli and culture If sputum is not available bronchialwashings taken at bronchoscopy and gastric lavage oraspirate samples should be obtained Gastric aspiratesneed to be neutralised immediately on collection Bron-choscopy and transbronchial biopsy may be useful inpatients with suspected TB but negative sputum smearPleural biopsy is often helpful and mediastinoscopyis occasionally needed in patients with mediastinallymphadenopathy Part of any biopsy specimen shouldalways be sent for culture Nucleic acid amplicationtests on sputum have sensitivity similar to culture in
15 on the 60th day of ICU in a recent study using amulticentre high-quality database and incorporatingnovel statistical methodology to control evolution ofseverity of illness25
PREVENTION
Several guidelines for prevention of ventilator-associated pneumonia and hospital-acquired pneumo-nia have been published26ndash30 Interventions can bedivided into general infection control measures andspecic measures General measures include alcohol-based hand disinfection hospital education programmeon infection control the use of microbiological sur-veillance and a programme to reduce antibiotic pre-scription The major specic recommendations aresummarised in Table 364 There is no evidence that
lsquobundlesrsquo of recommendations are more effective thanthe sum of the individual components
TUBERCULOSIS
The main risk factors are listed in Box 362 Typicalclinical features include fever sweating weight losslassitude anorexia cough productive of mucoid orpurulent sputum haemoptysis chest wall pain dysp-noea localised wheeze and apical crackles Patientsmay also present with unresolved pneumonia pleuraleffusions spontaneous pneumothorax and hoarseness
Figure 364 Management of suspected nosocomial pneumonia based on invasive sampling of respiratory secretions
Bacteria onGram stain
Yes
Yes
No
Yes No Yes No
No
Start antibiotics immediatelyusing PSBBAL specimen
and Gram stain results
Start antibioticsimmediately based onepidemiological clues
Observe look forother infection
Signs ofsevere sepsis
Immediate PSB or BAL beforechangingstarting antimicrobial therapy
+ve cultures +ve cultures
Adjust therapybased on
culture results
Continueadjustantibiotics Look for
other infection
Start antibioticson basisof results
Look forother infection
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1017
Tuberculosis 423
Table 364 Strategies for prevention of ventilator-associated pneumonia
LEVELS OF
RECOMMENDATIONS SPECIFIC INTERVENTIONS REMARKS
Universally recommendedby all guidelines27ndash30
1 Semirecumbent position to 45deg At least 30ndash45deg2 Avoidance of endotracheal intubation3 Preference of oral tracheal route
4 New circuit for a new patient and noschedule change unless soiled or damaged5 Avoidance of flushing of condensate into
lower airway or in-line medication6 HME changes no more frequently than 5ndash7
days7 Continuous aspiration of subglottic suctioning For patients expected to require mechanical
ventilation for gt72 hours
Generally recommendedby most guidelines
1 Preferential use of non-invasiveventilation272830
2 Avoidance of unplanned re-intubation272830
3 Maintenance of endotracheal cuff pressureof about 20 mmHg (266 kPa)272830
4 Closed suctioning2829
No effect on VAP mainly for staff safety5 Chlorhexidine oral decontamination272930
6 Sedation vacation and weaning protocol2728
7 Judicious use of stress ulcer prophylaxis272830
8 Restrictive blood transfusion28
Benefits less clear 1 Preference of HME over heatedhumidifier2830
HME associated with reduction in VAP inpatients ventilated for gt7 days lower cost
2 Silver-sulfadiazine-coated endotrachealtube272830
3 Early tracheostomy (within 7 days ofmechanical ventilation)29
4 Selective decontamination of digestive tract(SDD)272830
Mortality reduction demonstrated when topicalantimicrobials combined with short-course
systemic antibiotics BSAC recommendedSDD in patients expected to requiremechanical ventilation for gt48 hours ETFdiscourage routine use due to concern ofemergence of resistant organisms
Not yet reviewed byguidelines50
1 High-volume low-pressure ultrathin membraneendotracheal tube cuff with SSD
2 Ultrathin membrane cuff with tapered shapeand SSD
3 Low-volume low-pressure endotracheal tubecuff with SSD
4 Balloon device for biofilm removal5 Saline instillation before tracheal suctioning
HME= heat moist exchanger SSD= subglottic secretion drainage
smear-negative patients with pulmonary tuberculosisbut have the advantage of a much more rapid resultThere is however a signicant false-negative rate32
CHEST X-RAY (CXR)A normal CXR almost excludes TB (except inHIV-infected patients) but endobronchial lesionsmay not be apparent and early apical lesions can bemissed Common appearances include patchynodular
shadowing in the upper zones (often bilateral) cavita-tion calcication hilar or mediastinal lymphadenopa-thy (may cause segmental or lobar collapse) pleuraleffusion tuberculomas (dense round or oval shadows)and diffuse ne nodular shadowing throughout thelung elds in miliary TB Inactivity of disease cannot beinferred from the CXR alone This requires three nega-tive sputum samples and failure of any lesion seen onCXR to progress CXR appearances in HIV-positive
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1117
424 Pneumonia
t-tested negative-pressure respirator (N95 FFP2 orhigher) Use of a powered air-purifying respiratorshould be considered when bronchoscopy is being per-formed35 Detailed infection control advice can beobtained via the lsquolink pagersquo (httpwwwaiccuhk eduhkweb8Pneumonia20guidelineshtm)
PNEUMONIA IN THEIMMUNOCOMPROMISED
The lungs are amongst the most frequent targetorgans for infectious complications in the immuno-compromised The incidence of pneumonia is highestamongst patients with haematological malignanciesbone marrow transplant (BMT) recipients and patientswith AIDS
The speed of progression of pneumonia the CXRchanges (Table 365) and the type of immune defectprovide clues to the aetiology Bacterial pneumonias
progress rapidly (1ndash2 days) whereas fungal and proto-zoal pneumonias are less fulminant (several days to aweek or more) Viral pneumonias are usually not ful-minant but on occasions may develop quite rapidlyBronchoscopy is a major component of the investiga-tion of these patients Empirical management based onCXR appearances is outlined in Table 365 Early non-invasive ventilation may improve outcome amongstimmunocompromised patients with fever and bilateralinltrates36
PNEUMOCYSTIS JIROVECI PNEUMONIA (PCP)37
The incidence of this common opportunistic infectionhas fallen substantially in patients with AIDS whoare receiving prophylaxis and effective antiretroviraltherapy with most cases occurring in patients who arenot receiving HIV care or among patients with advancedimmunosuppression The onset is usually insidiouswith dry cough dyspnoea and fever on a backgroundof fatigue and weight loss Crackles in the chest are rareApproximately 15 of patients have a concurrent causefor respiratory failure (eg Kaposi sarcoma TB bacte-rial pneumonia) Useful investigations are
1 CXR classical appearance is diffuse bilateral perihi-
lar interstitial shadowing but in the early stages thisis very subtle and easily missed The initial CXR isnormal in 10 In a further 10 the changes areatypical with focal consolidation or coarse patchyshadowing None of the changes are specic for PCPand may be seen in other lung diseases associatedwith AIDS Pleural effusions hilar or mediastinallymphadenopathy are unusual in PCP but commonin mycobacterial infection or Kaposirsquos sarcoma orlymphoma
2 Induced sputum in this technique the patient inhalesnebulised hypertonic saline from an ultrasonic neb-uliser This provokes bronchorrhoea and the patient
patients with TB differ from those in non-HIV-infectedpatients
TREATMENT OF PULMONARY TB32ndash34
The decision to initiate anti-TB treatment should bebased on level of clinical suspicion results of AFBsmear and sometimes mycobacterial culture If the
initial clinical suspicion is strong and the patient is seri-ously ill attributable to possible TB treatment shouldbe initiated promptly sometimes before the result ofAFB smear Subsequent positivity of AFB smear ornucleic acid amplication test provides support to thecontinuation of treatment Combination chemotherapyconsisting of four drugs is necessary for maximal ef-cacy Treatment is divided into initial phase and con-tinuation phase The most commonly used initialregimen consists of 8 weeks of rifampicin 600 mg daily(450 mg for patients lt50 kg) isoniazid 300 mg dailypyrazinamide 2 g daily (15 g for patients lt50 kg) and
ethambutol 15 mgkg daily as initial phase treatmentEthambutol should be used only in patients who havereasonable visual acuity and who are able to appreciateand report visual disturbances This mandates carefulconsideration in patients who require heavy sedationVisual acuity and colour perception must be assessed(if ethambutol is to be used) and liver and renal func-tion checked before treatment is started Steroids arerecommended for children with endobronchial diseaseand possibly for patients with tuberculous pleuraleffusions Pyridoxine 10 mg daily should be given toprevent isoniazid-induced neuropathy to those atincreased risk (eg patients with diabetes mellitus
chronic renal failure or malnutrition or alcoholic orHIV-positive patients) Negative AFB smear should notdelay initial treatment if clinical suspicion remainshigh Supporting features included chronic coughweight loss characteristic chest X-ray ndings emigra-tion from a high-incidence country no other immediatediagnosis and positive tuberculin test
INFECTION CONTROL
Patients admitted to an ICU with infectious TB or sus-pected of having active pulmonary TB should bemanaged in an isolation room with special ventilation
characteristics including negative pressure Patientsshould be considered infectious if they are coughing orundergoing cough-inducing procedures or if they havepositive AFB smears and they are not on or have juststarted chemotherapy or have a poor clinical or bacte-riological response to chemotherapy3235 Patients withnon-drug-resistant TB should be non-infectious after 2weeks of treatment which includes rifampicin and iso-niazid32 As TB spreads through aerosols it is probablyappropriate to isolate patients who are intubated evenif only their bronchial washings are smear-positiveStaff caring for patients who are smear-positive shouldwear personal protective equipment including a
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1217
Pneumonia in the immunocompromised 425
andor diuretics (patients often uid-overloaded)Approximately 40 of patients with HIV-related PCPwho require mechanical ventilation survive to hospitaldischarge38
Initiation of antiretroviral therapy in patients pre-senting with HIV-related PCP is controversial TheCenters for Disease Control and Prevention (CDC) rec-ommend against doing so in the acute phase but recent
data suggest that the outcome may be improved byinitiation within the rst 4 days of ICU admission39
BACTERIAL PNEUMONIA37
This is the most common cause of acute respiratoryfailure in HIV-positive patients Bacterial pneumonia ismore common in HIV-infected patients than in thegeneral population and tends to be more severe Strep pneumoniae H infuenza Pseudomonas aeruginosa and Saureus are the commonest organisms Nocardia andGram negatives should also be considered Atypicalpathogens (eg Legionella) are rare Response to appro-
priate antibiotics is usually good but may require pro-tracted courses of antibiotics because of high tendencyto relapse Patients with severe immunodeciency(CD4+ T lymphocyte count lt100983221L) and a history ofPseudomonas infection or bronchiectasis or neutropeniashould receive antibiotics that cover P aeruginosa aswell as other Gram negatives The possibility of concur-rent PCP or tuberculosis should be excluded
TUBERCULOSIS
TB may be the initial presentation of AIDS particularlyin sub-Saharan Africa The pattern of TB in HIV patients
coughs up material containing cysts and tropho-zoites The technique is time-consuming and requiresmeticulous technique and is less sensitive thanbronchoscopy but less invasive The possibility ofconcurrent tuberculosis should be consideredand steps taken to minimise the risk of spread ofinfection
3 Bronchoscopy with bronchoalveolar lavage leads to
the diagnosis in over 90 of cases Specimens shouldbe sent for cytology Transbronchial biopsy is notnecessary in most cases PCR using bronchial lavagespecimens may be useful in non-HIV patients withsuspected PCP
Antipneumocystis treatment should be started as soonas the diagnosis is suspected Treatment of choice istrimethoprim plus sulfamethoxazole (co-trimoxazole)20 mgkgday+ 100 mgkgday for 3 weeks plusprednisolone 40 mg orally twice daily for 5 days fol-lowed by 20 mg twice daily for 5 days and then 20 mgper day until the end of PCP treatment Side-effects of
co-trimoxazole are common in HIV patients (nauseavomiting skin rash myelotoxicity) The dose should bereduced by 25 if the WBC count falls Patients whoare intolerant of co-trimoxazole should be treated with
bull pentamidine 4 mgkgday iv or
bull primaquine with clindamycin or
bull trimetrexate with leucovorin (plusmnoral dapsone)
Response to treatment is usually excellent with aresponse time of 4ndash7 days If the patient deteriorates orfails to improve consider (re-)bronchoscopy (is thediagnosis correct) treat co-pathogens and considera short course of high-dose iv methylprednisolone
Table 365 Causes of CXR changes and empirical treatment of pneumonia in the immunocompromised
CHEST X-RAY
APPEARANCE CAUSES
EMPIRICAL TREATMENT FOR
SUSPECTED PNEUMONIA
Diffuse infiltrate CMV and other herpes virusesPneumocystis carinii Bacteria
Aspergillus (advanced)Cryptococcus (uncommon)Non-infectious causes eg drug reaction non-specific
interstitial pneumonitis radiation pneumonitis(uncommon) malignancy leucoagglutinin reaction
Broad-spectrum antibiotics for at least 48 h(eg 3rd-generation cephalosporin andaminoglycoside)
Co-trimoxazoleLung biopsy or lavage within 48 h or full2-week course of co-trimoxazole (dependson patient tolerance of invasive procedure)
Focal infiltrate Gram-negative rodsS aureusAspergillusCryptococcusNocardiaMucorP carinii (uncommon)Tuberculosis
LegionellaNon-infectious causes (eg malignancy non-specificinterstitial pneumonitis radiation pneumonitis)
Broad-spectrum antibioticsIf response seen continue treatment for
2 weeksIf disease progresses lung biopsyaspirate
within 48ndash72 hours or empirical trial ofantifungalplusmn macrolide
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1317
426 Pneumonia
reaction are the most useful tests for demonstratingCMV disease Using thresholds of 10300 000ndash50200 000 positive circulating peripheral WBC the posi-tive predictive value for CMV-pp65 ranges from64 to 82 and the negative predictive value from70 to 954344 Treatment consists of intravenous gan-ciclovir for at least 14 days Foscarnet can be used if
ganciclovir fails
FUNGAL PNEUMONIA
Fungi are rare but important causes of pneumoniaThey can be divided into two main groups based on theimmune response required to combat infection withthese organisms Histoplasma blastomycosis coccidi-oidomycosis paracoccidioidomycosis and Cryptococcus require specic cell-mediated immunity for their controland thus in contrast to infections that are controlled byphagocytic activity the diseases caused by these organ-isms can occur in otherwise healthy individuals
although they cause much more severe illness inpatients with impaired cell-mediated immunity (egpatients infected with HIV and organ transplant recipi-ents) With the exception of Cryptococcus these organ-isms are rarely seen outside North America Aspergillus and Mucor spores are killed by non-immune phago-cytes and as a result these fungi rarely result in clinicalillness in patients with normal neutrophil numbers andfunction
CANDIDIASIS This is effectively a combination of the two types offungal infection in which impaired cell-mediatedimmunity predisposes to mucosal overgrowth withCandida but impaired phagocytic function or numbersis usually required before deep invasion of tissuesoccurs Primary Candida pneumonia (ie isolated lunginfection) is uncommon4145 and more commonly pul-monary lesions are only one manifestation of dissemi-nated candidiasis Even more common is benigncolonisation of the airway with Candida In mostreported cases of primary Candida pneumonia ampho-tericin B has been used In disseminated candidiasistreatment should be directed to treatment of dissemi-nated disease rather than Candida pneumonia per se45
INVASIVE ASPERGILLOSIS 46
This is a highly lethal condition in the immunocom-promised despite treatment and therefore investiga-tion and treatment should be prompt and aggressiveIt is associated with exposure to construction workDenitive diagnosis requires both histological evidenceof acute-angle branching septated non-pigmentedhyphae measuring 2ndash4 983221m in width and cultures yield-ing Aspergillus species from biopsy specimens ofinvolved organs Recovery of Aspergillus species fromrespiratory secretions in immunocompromised butnot immunocompetent patients may indicate invasive
disease with a positive predictive value as high as
depends on the degree of immunosuppression Inpatients with CD4+ T lymphocytes gt350 cells983221L theclinical presentation is similar to TB in non-HIV-infectedpatients although extrapulmonary disease is morecommon In patients with CD4+ T lymphocytes lt350cells983221L extrapulmonary disease (pleuritis pericardi-tis meningitis) is common Severely immunocompro-
mised patients (CD4+
T lymphocytes lt100 cells983221L)may present with severe systemic disease with highfever rapid progression and systemic sepsis In thesepatients lower and middle lobe disease is more commonmiliary disease is common and cavitation is lesscommon Sputum smears and culture may be positiveeven with a normal CXR
Response to treatment is usually rapid Managementof TB in HIV is complex owing to numerous druginteractions consultation with an expert in treatment ofHIV-related TB should be strongly considered Complexinteractions occur between rifamycins (eg rifampicinand rifabutin) and protease inhibitors and non-
nucleoside reverse transcriptase inhibitors used to treatpatients infected with HIV The choice of rifampicin orrifabutin depends on a number of factors includingthe unique and synergistic adverse effects for each indi-vidual combination of rifampicin and anti-HIV drugsand consultation with a physician with experiencein treating both TB and HIV is advised40 IDSA-recommended dosage adjustment for patients receivingantiretrovirals and rifabutin37 can be obtained viathe lsquolink pagersquo (httpwwwaiccuhkeduhkweb8Pneumonia20guidelineshtm) The optimal time forinitiating antiretroviral therapy in patients with TB iscontroversial Early therapy may decrease HIV disease
progression but may be associated with a high inci-dence of adverse effects and an immune reconstitutionreaction37
CMV PNEUMONITIS4142
Risk of infection is highest following allogeneic stemcell transplantation followed by lung transplantationpancreas transplantation and then liver heart and renaltransplantation and advanced AIDS If both the recipi-ent and the donor are seronegative then the risk of bothinfection and disease are negligible If the recipient is
seropositive the risk of infection is approximately 70but the risk of disease is only 20 regardless of theserostatus of the donor However if the recipient isseronegative and the donor is seropositive the risk ofdisease is 70 If steroid pulses and antilymphocyteglobulin are given for treatment of acute rejection therisk of developing disease is markedly increased Infec-tion may be the result of primary infection or reactiva-tion of latent infection It is clinically important butoften difcult to distinguish between CMV infectionand CMV disease and a denitive diagnosis can bemade only histologically Detection of CMV-pp65antigen in peripheral WBC and detection of CMV DNA
or RNA in the blood by quantitative polymerase chain
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1417
Parapneumonic effusion 427
needle aspiration or if there is debris within the uiddrainage using an intercostal drain The diagnosis isconrmed by aspiration of pus
TREATMENT The mainstay of treatment is drainage either by inter-costal drain or by surgical intervention Patients whopresent before the pus is loculated and a brinous peelhas formed on the lung can usually be treated bysimple drainage The combination with intrapleuralbrinolysis may be benecial Optimal surgical man-agement which consists of decortication (open or tho-racoscopic) is indicated if the empyema is moreadvanced or if simple drainage fails This is a majorprocedure and many patients with cardiac or chronicrespiratory disease will not tolerate it Alternatives forthese patients are instillation of thrombolytics into thepleural space or thoracostomy Antibiotics have onlyan adjunctive role Broad-spectrum antibiotic regimenswith anaerobic cover should be used until the resultsof microbiological analysis of the aspirated pus areavailable
AcknowledgementsAll tables and gures are reproduced from ICU web(wwwaiccuhkeduhkweb8) with permission of theauthors
80ndash90 in patients with leukaemia or bone marrowtransplant recipients Bronchoalveolar lavage withsmear culture and antigen detection has excellent spe-cicity and reasonably good positive predictive valuefor invasive aspergillosis in immunocompromisedpatients Although radiological features may give a clueto the diagnosis they are not sufciently specic to be
diagnosticIn acutely ill immunocompromised patients intrave-nous therapy should be initiated if there is suggestiveevidence of invasive aspergillosis while further investi-gations to conrm or refute the diagnosis are carriedout First-line therapy is voriconazole47 Echinocandinsand amphotericin are alternatives
PARAPNEUMONIC EFFUSION
This may be an uncomplicated effusion that resolveswith appropriate treatment of the underlying pneumo-nia or a complicated effusion that develops into an
empyema unless drained Complicated effusions tendto develop 7ndash14 days after initial uid formation Theyare characterised by increasing pleural uid volumecontinued fever and pleural uid of low pH (lt73) thatcontains a large number of neutrophils and may revealorganisms on Gram staining or culture An outline ofmanagement is given in Figure 365
EMPYEMA48
DEFINITION Collection of pus in the pleural space
AETIOLOGY Follows infection of the structures surrounding thepleural space including subdiaphragmatic structuresand chest trauma or may be associated with malig-nancy Anaerobic bacteria usually streptococci orGram-negative rods are responsible for 76 of cases
DIAGNOSIS The diagnosis is usually simple The patient is usuallyseptic and may have a productive cough and chest painThe chest X-ray may show features suggestive of apleural effusion and underlying consolidation but may
also show an abscess cavity with a uid level in whichcase CT scanning will be required to distinguishbetween an abscess and an empyema Ultrasound canbe useful to conrm the presence of uid in the pleuralspace and to determine whether it can be drained by
Figure 365 An approach to the management of
parapneumonic effusions
Parapneumonic effusion
gt 1 cm thick
on lateral decubitus
film
Pleural aspirate
turbid or purulent or
Gram stain +ve
Pleural aspirate
pH
Serial thoracocentesis Treat as empyemaObserve
No
gt72 lt70
70ndash72
No
Yes
Yes
httpwwwexpertconsultcomAccess the complete references list online at
1 American Thoracic Society and Infectious Diseases Society of America Guidelines for the manage-ment of adults with hospital-acquired ventilator-associated and healthcare associated pneumonia
Am J Respir Crit Care Med 2005171388ndash416
2 Mandell LA Wunderink RG Anzueto A et al Infec-tious Diseases Society of AmericaAmerican Tho-racic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin
Infect Dis 200744S27ndash72
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1517
428 Pneumonia
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1617
References 428e1
REFERENCES 1 American Thoracic Society and Infectious Diseases
Society of America Guidelines for the management of adults with hospital-acquired ventilator-associated and healthcare associated pneumonia Am J Respir Crit Care Med 2005171388ndash416
2 Mandell LA Wunderink RG Anzueto A et al Infec-tious Diseases Society of AmericaAmerican Tho-racic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744S27ndash72
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
4 Woodhead M Blasi F Ewig S et al Guidelines for the management of adult lower respiratory tract infections Eur Respir J 2005261138ndash80
5 Torres A Rello J Update in community-acquired and nosocomial pneumonia 2009 Am J Respir Crit
Care Med 2010181782ndash76 Van der Eerden MM Vlaspolder F de Graaff CS et
al Value of intensive diagnostic microbiological investigation in low- and high-risk patients with community-acquired pneumonia Eur J Clin Micro Infect Dis 200524241ndash9
7 Murdoch DR Nucleic acid amplication tests for the diagnosis of pneumonia Clin Infect Dis 2003361162ndash70
8 Blaschke AJ Interpreting assays for the detection of Streptococcus pneumonia Clin Infect Dis 201152(S4)S331ndash7
9 Rello J Lisboa T Lujan M Severity of pneumococcal
pneumonia associated with genomic bacterial load Chest 2009136832ndash4010 Azoulay E Bergeron A Polymerase chain reaction
for diagnosing pneumocystis pneumonia in non-HIV immunocompromised patients with pulmonary inl-trates Chest 2009135(3)655
11 Garcia-Vidal C Fernandez-Sabe N Carratala J Early mortality in patients with community-acquired pneumonia causes and risk factors Eur Respir J200832733ndash9
12 Dellinger RP Carlet JM Masur H et al Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock Intensive Care Med200430536ndash55
13 Metersky ML Ma A Houck PM et al Antibiotics for bacteremic pneumonia improved outcomes with macrolides but not uoroquinolones Chest 2007131466ndash73
14 Dunbar LM Wunderink RG Habib MP High-dose short-course levooxacin for community-acquired pneumonia a new treatment paradigm Clin Infect Dis 200337752ndash60
15 Matthaiou DK Ntani G An ESICM systematic review and meta-analysis of procalcitonin-guided antibiotic therapy algorithms in adult critically ill patients Intensive Care Med 201238940ndash9
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
17 Gruber PC Gomersall CD Joynt GM Avian inu-enza (H5N1) implications for intensive care Inten-sive Care Med 200632823ndash9
18 Belongia EA Irving SA Clinical characteristics and 30-day outcomes for inuenza A 2009 (H1N1) 2008ndash2009 (H1N1) and 2007ndash8 (H3N2) infections JAMA2010304(10)1091
19 Lee N Chan PKS Complications and outcomes of pandemic 2009 inuenza A (H1N1) virus infection in hospitalized adults how do they differ from those in seasonal inuenza J Infect Dis 20112031739ndash47
20 Kim SH Hong SB Corticosteroid treatment in critically ill patients with pandemic inuenza AH1N1 2009 infection analytic strategy using pro-pensity scores Am J Respir Crit Care Med 20111831207ndash14
21 Centers for Disease Control and Prevention (CDC) Bacterial coinfections in lung tissue specimens from
fatal cases of 2009 pandemic inuenza A (H1N1) ndash United States MayndashAugust 2009 MMWR 2009581071ndash4
22 Safdar N Dezfulian C Clinical and economic conse-quences of ventilator-associated pneumonia A sys-tematic review Crit Care Med 200533(10)2184ndash93
23 Shorr AF Sherner JH Invasive approaches to the diagnosis of ventilator-associated pneumonia A meta-analysis Crit Care Med 200533(1)46ndash53
24 Melsen WG Rovers MM Ventilator-associated pneumonia and mortality A systematic review of observational studies Crit Care Med 2009372709ndash18
25 Bekaert M Timsit JF Attributable mortality of ventilator-associated pneumonia A reappraisal using causal analysis Am J Respir Crit Care Med20111841133ndash9
26 CDC Healthcare Infection Control Practices AdvisoryCommittee Guidelines for preventing health-care-associated pneumonia 2003 Recommendations ofCDC and the Healthcare Infection Control PracticesAdvisory Committee Online Available httpwwwcdcgovmmwrpreviewmmwrhtmlrr5303a1htm
27 Cofn SE Klompas M SHEAIDSA practice recom-mendation strategies to prevent ventilator-associated pneumonia in acute care hospitals Infect Control
Hosp Epidemiol 200829S31ndash4028 Masterton RG Galloway A Guidelines for the man-
agement of hospital-acquired pneumonia in the UK Report of the Working Party on Hospital-Acquired Pneumonia of the British Society for Antimicrobial Chemotherapy J Antimicrob Chemother 2008625ndash34
29 VAP Guidelines Committee and the Canadian Critical Care Trials Group Comprehensive evidence-based clinical practice guidelines for ventilator-associated pneumonia prevention J Crit Care 200823126ndash37
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1717
428e2 Pneumonia
30 Torres A Ewig S Dening treating and preventing hospital acquired pneumonia European perspective Intensive Care Med 2009359ndash29
31 Frame RN Johnson MC Eichenhorn MS et al Active tuberculosis in the medical intensive care unit a 15-year retrospective analysis Crit Care Med 1987151012ndash14
32 National Collaborating Centre for Chronic Condi-tions Tuberculosis Clinical diagnosis and manage-ment of tuberculosis and measures for its prevention and control London Royal College of Physicians 2006
33 Small PM Fujiwara PI Management of tuberculosis in the United States N Engl J Med 2001345189ndash200
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
35 Centers for Disease Control and Prevention Guide-lines for preventing the transmission of Mycobacte-rium tuberculosis in health-care settings 2005 MMWR
2005541ndash11936 Hilbert G Gruson D Vargas F et al Noninvasive
ventilation in immunosuppressed patients with pul-monary inltrates fever and acute respiratory failure N Engl J Med 2001344481ndash7
37 Benson CA Kaplan JE Masur H Treating oppor-tunistic infections among HIV-infected adults and adolescents recommendations from CDC the National Institutes of Health and the HIV Medicine AssociationInfectious Diseases Society of America Clin Infect Dis 200540S131ndash235
38 Randall CJ Yarnold PR Schwartz DN et al Improve-ments in outcomes of acute respiratory failure for
patients with human immunodeciency virus-related Pneumocystis carinii pneumonia Am J Respir Crit Care Med 2000162393ndash8
39 Croda J Croda MG Neves A et al Benet of antiret-roviral therapy on survival of human immunode-ciency virus-infected patients admitted to an intensive care unit Crit Care Med 200937(5)1605
40 Centers for Disease Control Updated guidelines for the use of rifabutin or rifampicin for the treatment and prevention of tuberculosis among HIV-infected patients taking protease inhibitors or nonnucleoside reverse transcriptase inhibitors MMWR 200049185ndash9
41 Tamm M The lung in the immunocompromised patient Infectious complications part 2 Respiration199966199ndash207
42 Van der Bij W Speich R Management of cytomega-lovirus infection and disease after solid-organ trans-plantation Clin Infect Dis 200133(Suppl 1)S32ndash7
43 Schaumlfer P Tenschert W Cremaschi L et al Area under the viraemia curve versus absolute viral load utility for predicting symptomatic cytomegalovirus infections in kidney transplant patients J Med Virol20016585ndash9
44 Meyer-Koenig U Weidmann M Kirste G et al Cytomegalovirus infection in organ-transplant recip-ients diagnostic value of pp65 antigen test qualita-tive polymerase chain reaction (PCR) and quantitative
Taqman PCR Transplantation 2004771692ndash8
45 Pappas PG Rex JH Sobel JD Guidelines for treat-ment of candidiasis Clin Infect Dis 200438161ndash89
46 Stevens DA Kan VL Judson MA Practice guidelines for diseases caused by Aspergillus Clin Infect Dis200030696ndash709
47 Herbrecht R Denning DW Patterson TF Voricona-zole versus amphotericin B for primary therapy of invasive aspergillosis N Engl J Med 2002347408ndash15
48 Peek GJ Morcos S Cooper G The pleural cavity BMJ20003201318ndash21
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6

7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 317
416 Pneumonia
9 Urinary Legionella antigen This test is specic(gt95) In patients with severe Legionnaires diseasesensitivity is 88ndash100 for L pneumophilia serogroup1 (the most commonly reported cause of Legionella infection) Thus a positive result is virtually
single or predominant organism on a Gram stain ofa fresh sample or a heavy growth on culture ofpurulent sputum is likely to be the organismresponsible The nding of many polymorphonu-clear cells (PMN) with no bacteria in a patient whohas not already received antibiotics can reliablyexclude infection by most ordinary bacterial patho-gens Specimens should be obtained by deep coughand be grossly purulent Ideally the specimenshould be obtained before treatment with antimi-crobials if this does not delay administration ofantibiotics and be transported to the laboratoryimmediately for prompt processing to minimise thechance of missing fastidious organisms (eg Strep pneumoniae) Acceptable specimens (in patientswith normal or raised white blood cell counts)should contain gt25 PMN per low-power eld (LPF)and lt10ndash25 squamous epithelial cells (SEC)LPF orgt10 PMN per SEC These criteria should not beused for Mycobacteria and Legionella infectionCertain organisms are virtually always pathogenswhen recovered from respiratory secretions (Box 361) Patients with risk factors for tuberculosis (TB)(Box 362) and particularly those with cough for
more than a month other common symptoms of TBand suggestive radiographic changes should havesputum examined for acid-fast bacilli Sputumcannot be processed for culture for anaerobesowing to contamination by the endogenous anaero-bic ora of the upper respiratory tract In additionto the factors listed in Table 361 foul-smellingsputum lung abscess and empyema should raisesuspicion of anaerobic infection
8 Aspiration of pleural uid for Gram stain culturepH and leucocyte count ndash all patients with a pleuraleffusion gt1 cm thick on a lateral decubitus chestX-ray
Table 361 Possible aetiological agents based on epidemiological cluesmdashcontrsquod
EXPOSURE ORGANISM
Lung abscess Community-acquired meticillin-resistant S aureus oralanaerobes endemic fungi M tuberculosis atypicalmycobacteria
Endobronchial obstruction Anaerobes Strep pneumoniae H influenzae S aureus
Intravenous drug addict S aureus CA-MRSA anaerobes M tuberculosis Streppneumoniae
End-stage renal failure CA-MRSA
OTHERS
Epidemic M pneumoniae influenza virus
Air-conditioning cooling towers hot tubs or hotel or cruise shipstay in previous 2 weeks
Legionella pneumophilia
Presentation of a cluster of cases over a very short periodof time
Bioterrorist agents B anthracis F tularensis Y pestis
Box 361 Organisms that are virtually alwayspathogens when recovered fromrespiratory secretions
LegionellaChlamydiaTBInfluenza para-influenza virus RSV adenovirus hantavirus
SARS coronavirusStronglyloides stercoralisToxoplasma gondi Histoplasma capsulatum
Coccidiodes immitisBlastomycoses dermatitidisCryptococcus neoformans
Box 362 Risk factors for pulmonary tuberculosis
Living in or originating from a developing countryAge (lt5 years middle-aged and elderly men)Alcoholism andor drug addictionHIV infectionDiabetes mellitusLodging-house dwellers
ImmunosuppressionClose contact with smear-positive patientsSilicosisPoverty andor malnutritionPrevious gastrectomySmoking
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 417
Community-acquired pneumonia 417
contamination and colonisation PCR assays are moresensitive than culture for Mycoplasma and Chlamydia species and at least as sensitive for Legionella7 PCRassays also detect Legionella strains other than sero-group 1 The BTS guidelines3 recommend PCR of lowerrespiratory tract sample or if unavailable throat swabfor the diagnosis of Mycoplasma pneumonia PCR for
Chlamydophilia should be performed when invasiverespiratory samples were collected from patients withsevere community-acquired pneumonia The role ofPCR in diagnosing PCP is mainly limited to non-HIVpatients in whom conventional microscopy and stain-ing of induced sputum and BAL have a lower sensitiv-ity than in HIV patients9
MANAGEMENT
GENERAL SUPPORTIVE MEASURES Intravenous uids may be required to correct dehydra-
tion and provide maintenance uid A general approachshould be made to organ support with an emphasis oncorrecting hypoxia
ANTIMICROBIAL REGIMENS Increased mortality among those who do not receiveempirical antibiotics that cover the infecting pathogen(s)is well documented11 Each unit should have its ownregimens tailored to the local ora and antibiotic resist-ance patterns In the absence of such regimens theregimen outlined in Figure 361 may be helpful This
diagnostic of Legionella infection but a negativeresult does not exclude it In areas (eg South Aus-tralia) where other Legionella species are morecommon this test is less helpful
10 Urinary pneumococcal antigen has moderate sensi-tivity (50ndash80) and high specicity (gt90)
11 Microimmunouorescence serology for Chlamydia
pneumoniae IgM A titre ge1 16 is signicant12 HIV serological status
Other investigations should be considered in patientswith risk factors for infection with unusual organismsBronchoalveolar lavage may be useful in immunocom-promised patients those who fail to respond to antibi-otics or those in whom sputum samples cannot beobtained6
Molecular diagnosis (eg PCR-based methods) hasthe advantages of quick results (within 3 hours)enhanced sensitivity independence from organismviability and hence previous antibiotics and theoretical
possibility for determination of antimicrobial suscepti-bility7 Of note it is important to test for genes specicfor the organism in question10 and the sampling siteremains important PCR is most useful when performedon specimens from a normally sterile site For examplePCR for Pneumococcus is positive in 62 of bloodsamples from adult patients with conrmed or proba-ble pneumococcal pneumonia8 whereas blood culturesare positive in only 37 For respiratory specimensunder most circumstances interpretation remainsproblematic due to low specicity related to oral
Figure 361 Antibiotic regimens for treatment of severe community-acquired pneumonia in critically ill patients24 Respiratory fluoroquinolones include moxifloxacin and levofloxacin Advanced macrolides include azithromycin andclarithromycin Non-antipseudomonal third-generation cephalosporins include cefotaxime and ceftriaxone
Severe CAP
Aztreonam
and
levofloxacin
Piperacillin-tazobactam or
meropenem or imipenem or
cefepime and ciprofloxacin or
aminoglycoside plus
advanced macrolide
Respiratory
fluoroquinolone
plusmn clindamycin
Non anti-pseudomonal
third-generation cephalosporin
or ampicillin-sulbactam
and respiratory fluoroquinolone
or advanced macrolide
Risk of Pseudomonas
(COPDbronchiectasis
recent hospitalisation
recent antimicrobial
therapy or gross aspiration)
β-lactam
allergy
β-lactam
allergy
NoYes
NoYesNoYes
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 517
418 Pneumonia
should be modied in the light of risk factors (see Table 361) Quinolones may be less appropriate in areas witha high prevalence of TB as their use may mask concur-rent TB infection Appropriate antimicrobial therapyshould be administered within 1 hour of diagnosis412 There is controversy regarding the appropriate changeto empirical therapy based on microbiological nd-
ings24
Changing to narrower-spectrum antimicrobialcover may result in inadequate treatment of the 5ndash38of patients with polymicrobial infection Increasing evi-dence demonstrates improved outcome with combina-tion antimicrobial as compared with monotherapyparticularly in severely ill patients with bacteraemicpneumococcal pneumonia5 Odds ratio of death was15 to 6 for monotherapy as compared with com-bination therapy Benets were seen only in combina-tion therapy with macrolide as part of the regimen butnot in combination with uroquinolone regimen13 For the treatment of drug-resistant Strep pneumoniae (DRSP) the regimens in Figure 361 are probably suit-
able for isolates with a penicillin MIC lt 4 mgL2 Ifthe MIC is ge4 mgL an antipneumococcal uoroqui-nolone vancomycin teicoplanin or linezolid should begiven4
DURATION OF THERAPY No clinical trial has specically addressed this issueCourses as short as 5 days may be sufcient14 IDSAATS guidelines recommend stopping after a minimumof 5 days if the patient is afebrile for 48ndash72 hoursand organ dysfunction has largely resolved2 Shortcourses may be suboptimal for patients with bacterae-mic S aureus pneumonia meningitis or endocarditiscomplicating pneumonia or infection with less commonorganisms (eg Burkholderia pseudomallei or fungi) orPseudomonas aeruginosa Procalcitonin may be useful toguide antibiotic therapy but not all studies have dem-onstrated a benet15
RESPONSE TO THERAPY 2
This can be assessed subjectively (a response is usuallyseen within 1ndash3 days of starting therapy) or objectivelyon the basis of respiratory symptoms fever oxygena-tion WBC count bacteriology CXR changes C-reactiveprotein reduction and procalcitonin reduction of
80ndash90 from peak value The average time to deferves-cence varies with organism severity and patient age(7 days in elderly patients 25 days in young patientswith pneumococcal pneumonia 6ndash7 days in bacterae-mic patients with pneumococcal pneumonia 1ndash2 daysin patients with M pneumoniae pneumonia and 5 daysin patients with Legionella pneumonia) Both blood andsputum cultures are usually negative within 24ndash48hours of treatment although P aeruginosa and M pneu-moniae may persist in the sputum despite effectivetherapy CXR changes lag behind clinical changes withthe speed of change depending on the organism theage of the patient and the presence or absence of comor-
bid illnesses The CXR of most young or middle-aged
patients with bacteraemic pneumococcal pneumonia isclear by 4 weeks but resolution is slower in elderlypatients and patients with underlying illness extensivepneumonia on presentation or Legionella pneumophilia pneumonia
If the patient fails to respond consider the followingquestions
bull Has the patient got pneumonia
bull Are there host factors that explain the failure (egobstruction of bronchus by a foreign body or tumourinadequate host response)
bull Has a complication developed (eg empyema super-infection bronchiolitis obliterans organising pneu-monia metastatic abscess)
bull Is the right drug being given in an adequate dose bythe right route
bull Is the organism resistant to the drug being given
bull Are there other organisms
bull Is the fever a drug fever
Useful investigations include computerised tomogra-phy (CT) of the chest thoracocentesis bronchoalveolarlavage (Table 362) and transbronchial or open-lungbiopsy
PREDICTION OF ADVERSE OUTCOME ANDADMISSION TO ICU Scoring systems have been developed to predictadverse outcome and ICU admission including pneu-monia severity index (PSI) CURB-65 CRB-65 modiedATS major and minor criteria SCAP prediction ruleSMART-COP REA-ICU index and CAP-PIRO16
Although they may help identify the sicker patientsthey should not be used as a sole determinant of ICUadmission as local admission criteria will be affectedby local facilities both in and outside ICU It shouldbe noted that none of the criteria has been prospec-tively demonstrated to avoid late transfers or lowermortality
INFLUENZA PNEUMONIA
Inuenza pneumonia may present with severe respira-tory failure and multi-organ failure However the
pattern of organ failure appears to vary between strainswith H5N1 being associated with a much higher mor-tality and a higher incidence of multi-organ failure thanpandemic H1N117 which itself presented differently toseasonal inuenza In particular trophism for lowerrespiratory tract a higher rate of ICU admission18 anda higher rate of extrapulmonary complications19 wereobserved
Early initiation of oseltamivir is recommended forcritically ill patients although there is no direct evidenceof outcome benet Glucocorticoids do not appear tobe useful and may prolong viral replication20 Bacterialsuperinfection should be considered with Gram-
positive cocci being most frequently isolated21
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 617
Healthcare-associated pneumonia 419
failure and cancer) can cause inltrates on a chest X-rayIdentication of the organism responsible is even moredifcult than in patients with community-acquiredpneumonia owing to the high incidence of oropharyn-
geal colonisation by Gram-negative bacteria Blood cul-tures are positive in only about 6 of cases of nosocomialpneumonia Ventilator-associated pneumonia (VAP) isnosocomial pneumonia arising gt48ndash72 hours after intu-bation Reported incidence of VAP is between 10 and20 for those receiving mechanical ventilation for morethan 48 hours22 It is associated with a higher incidenceof multi-drug-resistant organisms1
PATHOGENESIS
Nosocomial pneumonia is thought to result from micro-aspiration of bacteria colonising the upper respiratory
tract Other routes of infection include macroaspiration
Although there are data demonstrating that surgicalmasks are as effective as N95 (FFP 2) masks in prevent-ing transmission of seasonal inuenza in non-ICU set-tings it is important to note that the capacity for airborne
transmission (and hence the need for N95 masks) isdependent on the exact characteristics of the organismand the frequency of aerosol-generating procedures sothese data should not be extrapolated to other inuenzaviruses and ICU settings
HEALTHCARE-ASSOCIATED PNEUMONIA
Nosocomial pneumonia occurs in 05ndash5 of hospitalpatients with a higher incidence in certain groups(eg postoperative patients and patients in ICU) Diag-nosis may be difcult the clinical features of pneumo-nia are non-specic and many non-infectious conditions
(eg atelectasis pulmonary embolus aspiration heart
Table 362 Procedure for obtaining microbiological samples using bronchoscopy and protected specimen brushingandor bronchoalveolar lavage3549
Infection control In patients suspected of having a disease that is transmitted by the airborne route (egtuberculosis)
bull the risk of transmission should be carefully weighed against the benefits ofbronchoscopy which may generate large numbers of airborne particles
bull perform bronchoscopy in a negative-pressure isolation room
bull consider the use of a muscle relaxant in ventilated patients to prevent coughingbull staff should wear personal protective equipment which should include a fit-tested
negative-pressure respirator (N95 FFP2 or above) as a minimum use of a poweredair-purifying respirator should be considered
General recommendations Suction through the endotracheal tube should be performed before bronchoscopyAvoid suction or injection through the working channel of the bronchoscopePerform protected specimen brushing before bronchoalveolar lavage
Ventilated patients Set F iO2 at 10
Set peak pressure alarm at a level that allows adequate ventilationTitrate ventilator settings against exhaled tidal volumeConsider neuromuscular blockade in addition to sedation in patients at high risk of
complications who are undergoing prolonged bronchoscopy
Protected specimen brushing (PSB) Sample the consolidated segment of lung at subsegmental levelIf purulent secretions are not seen advance the brush until it can no longer be seen but
avoid wedging it in a peripheral positionMove brush back and forth and rotate it several times
Bronchoalveolar lavage (BAL) Wedge tip of bronchoscope into a subsegment of the consolidated segment of lungInject aspirate and collect 20 mL of sterile isotonic saline Do not use this sample for
quantitative microbiology or identification of intracellular organisms It can be used forother microbiological analysis
Inject aspirate and collect additional aliquots of 20ndash60 mLThe total volume of saline injected should be 60ndash200 mL
Complications Hypoxaemia (possibly less with smaller BAL volumes)Arrhythmia
Transient worsening in pulmonary infiltratesBleeding (particularly following PSB)Fever (more common after BAL)
Positive results gt5 of cells in cytocentrifuge preparations of BAL fluid contain intracellular bacteria ORge103 colony-forming unitsmL in PSB specimen ORge104 colony-forming unitsmL in BAL fluid
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 717
420 Pneumonia
worse prognosis In 50 of patients with severehospital-acquired pneumonia and positive bloodcultures there is another source of sepsis
MANAGEMENT
Management is based on the nding that early treat-
ment with antimicrobials that cover all likely patho-gens results in a reduction in morbidity and mortality2 The initial selection of antimicrobials is made on thebasis of epidemiological clues (Fig 362 Table 363)Antimicrobials should be administered within 1 hourof diagnosis12 The results of microbiological investiga-tions are used to narrow antimicrobial cover laterTreatment should be reassessed after 2ndash3 days orsooner if the patient deteriorates (Fig 363) An outlineof management based on an invasive approach is givenin Figure 364
DURATION OF THERAPY
Current ATS guidelines recommend 7 daysrsquo treatmentprovided the aetiological agent is not P aeruginosa orother non-lactose fermenter and the patient has a goodclinical response with resolution of clinical features ofinfection1 The outcome of patients who receive appro-priate initial empirical therapy for ventilator-associatedpneumonia for 8 days is similar to those who receivetreatment for 15 days1
of gastric contents inhaled aerosols haematogenousspread spread from pleural space and direct inocula-tion from ICU personnel
CLINICAL DIAGNOSIS
Diagnosis is based on time of onset (gt48 hours afteradmission to a healthcare facility1) CXR changes (newor progressive inltrates) and either clinical featuresand simple laboratory investigations or the results ofquantitative microbiology Using a clinical approachpneumonia is diagnosed by the nding of a new inl-trate or a change in an inltrate on chest radiographand growth of pathogenic organisms from sputum plusone of the following white-blood-cell (WBC) countgreater than 12times l05L core temperature ge383degCsputum Gram stain with scores of more than two on ascale of four of polymorphonuclear leucocytes andbacteria
INVESTIGATIONSThese are broadly similar to those required incommunity-acquired pneumonia
bull Chest X-ray although studies using a histologicaldiagnosis as the gold standard have demonstratedthat pneumonia may be present despite a normalCXR most denitions of nosocomial pneumoniarequire the presence of new persistent inltrates ona CXR
bull Respiratory secretions considerable controversy sur-rounds the issue of whether invasive bronchoscopicsampling (Table 362) of respiratory secretions is nec-
essary Whether invasive sampling is employed ortracheal aspirates are used empirical broad-spectrumantibiotics should be started while results areawaited The results of microbiological analysis ofrespiratory secretions are used to either stop antibi-otics or narrow the spectrum1 Although the use ofan invasive strategy is associated with a higher like-lihood of modication of initial antimicrobials23 theeffect on important clinical outcome such as mortal-ity antibiotic-free days and organ dysfunction isvariable1 Although tracheal aspirates may predomi-nantly reect the organisms colonising the upper
airway they may be useful in indicating whichorganisms are not responsible for the pneumoniathus allowing the antimicrobial cover to be nar-rowed1 This interpretation is based on the premisethat the predominant route of infection is via theupper respiratory tract From this it can be assumedthat if the organism is not present in the upper res-piratory tract the probability of it being present inthe lung parenchyma is low Certain organisms arevirtually always pathogens when recovered fromrespiratory secretions (see Box 361)
bull Blood cultures identify the aetiological agent in8ndash20 of patients Bacteraemia is associated with a
Figure 362 An outline of initial management ofnosocomial pneumonia based on a non-invasive clinicalapproach1
Two ofuarr or darr WCC
purulent sputum
temp gt38degC
New CXR
infiltrates
Consider acute
tracheobronchitis
Obtain lower respiratory
tract specimens and blood for
microbiological investigations
Risk factorsfor multidrug-resistant
pathogens
Early broad-spectrum
antibiotic therapy
to cover multidrug-
resistant pathogens
Early limited-spectrum
antibiotic therapy
Yes
Yes
No
No
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 817
Healthcare-associated pneumonia 421
inltrate in 48 hours new cavitation or a signicantnew pleural effusion should raise concern If the patientfails to respond consider the diagnosis host factors (egimmunosuppressed debilitated) bacterial factors (egvirulent organism) and therapeutic factors (eg wrongdrug inadequate dose) Review the antibiotics andrepeat cultures It may be useful to broaden the antimi-crobial cover while waiting for the results of investiga-tions Consider invasive sampling of respiratorysecretions computerised tomography or ultrasound ofthe chest (to look for an empyema or abscess) anothersource of infection open-lung biopsy to establish diag-nosis and aetiology or administration of steroids
MORTALITY AND MORBIDITY ATTRIBUTABLE TO VAP Substantial morbidity and mortality associated withVAP have previously been reported22 However acausal relationship is difcult to establish It should benoted that patients who developed VAP tend to be
more severely ill and at higher risk of death not onlyon ICU admission but throughout the course of theirillness Most of the relevant studies were observationaland failed to adequately control confounders likedisease severity evolution of disease progression andICU length of stay with mortality In addition signi-cant heterogeneity exists among these studies Althoughthe presence of VAP is associated with a signicantlylonger ICU length of stay (mean of 61 days 95 CI532ndash687) and increased healthcare cost22 more recentstudies reported that mortality attributable to VAPtends to be small if any2425 The attributable mortalityhas been reported to be 1 on the 30th day of ICU and
RESPONSE TO THERAPY Clinical improvement is usually not apparent for 48ndash72hours and therapy should not be changed during thistime The CXR is of limited value for assessing responseinitial deterioration is common and improvement oftenlags behind clinical response However a rapidly dete-riorating CXR pattern with a gt50 increase in size of
Figure 363 Subsequent management of nosocomialpneumonia based on a non-invasive clinical approach1
Pathogens isolated
from respiratory
specimen
Antibiotics
changedstarted in 7 h
prior to sampling
Adjust antibiotics
according to sensitivities
Continue antibiotics if
high clinical suspicion of
nosocomial pneumonia
Bacterial pneumonia
unlikely
Investigate for other cause
of sepsis and CXR changes
Consider unusual causes
of nosocomial pneumonia
(eg Legionella viruses fungi
Pneumocystis carinii )
Yes
Yes
No
No
Table 363 Recommended initial empirical treatment for nosocomial pneumonia1
SITUATION ANTIBIOTICS
No risk factors for multidrug-resistant pathogens Ceftriaxone or Levofloxacin moxifloxacin or ciprofloxacin or Ampicillinsulbactam or Ertapenem
Antimicrobial therapy in previous 90 days or Current hospitalization for ge5 days or High frequency of antibiotic resistance in the specific
hospital unit or Hospitalisation for 2 days or more in previous 90 days or Residence in nursing home or extended care facility or Home infusion therapy (including antibiotics) or Chronic dialysis within 30 days or Home wound care or Family member with multidrug-resistant pathogen o rImmunosuppression or Bronchiectasis
One ofAntipseudomonal cephalosporin (cefepime or ceftazidime) or Antipseudomonal carbapenem (meropenem or imipenemndash
cilastin) or szlig-lactamszlig-lactamase inhibitor (eg piperacillinndashtazobactam or
cefaperazonendashsulbactam)plus one ofAminoglycoside or Antipseudomonal quinolone (levofloxacin or ciprofloxacin)plus one of the following for patients at high risk of meticillin-
resistant Staphylococcus aureus (MRSA) infectionLinezolid or Vancomycin or
TeicoplaninThe use of dual therapy is not well supported by evidence but it does reduce the probability that the pathogen is resistant to the drugsbeing given If an extended spectrum β-lactamase-producing strain or an Acinetobacter sp is suspected a carbapenem should be givenIf Legionella pneumophilia is suspected use a quinolone Risk factors for MRSA infection in areas with a high incidence of MRSA includediabetes mellitus head trauma coma and renal failure
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 917
422 Pneumonia
or with enlarged cervical nodes or other manifestationsof extrapulmonary disease Clinical disease is seldomfound in asymptomatic individuals even those withstrongly positive tuberculin test (Heaf grade III or IV)The outlook for patients with tuberculosis who requireICU admission is poor In one retrospective study thein-hospital mortality for all patients with tuberculosisrequiring ICU admission was 67 but in those withacute respiratory failure it rose to 8131 The presenta-tion and management of TB in HIV-positive patientsare different (see below)
INVESTIGATION OF PULMONARYTUBERCULOSIS
IDENTIFICATION OF MYCOBACTERIA
Multiple
3233
sputum samples should be collected pref-erably on different days for microscopy for acid-fastbacilli and culture If sputum is not available bronchialwashings taken at bronchoscopy and gastric lavage oraspirate samples should be obtained Gastric aspiratesneed to be neutralised immediately on collection Bron-choscopy and transbronchial biopsy may be useful inpatients with suspected TB but negative sputum smearPleural biopsy is often helpful and mediastinoscopyis occasionally needed in patients with mediastinallymphadenopathy Part of any biopsy specimen shouldalways be sent for culture Nucleic acid amplicationtests on sputum have sensitivity similar to culture in
15 on the 60th day of ICU in a recent study using amulticentre high-quality database and incorporatingnovel statistical methodology to control evolution ofseverity of illness25
PREVENTION
Several guidelines for prevention of ventilator-associated pneumonia and hospital-acquired pneumo-nia have been published26ndash30 Interventions can bedivided into general infection control measures andspecic measures General measures include alcohol-based hand disinfection hospital education programmeon infection control the use of microbiological sur-veillance and a programme to reduce antibiotic pre-scription The major specic recommendations aresummarised in Table 364 There is no evidence that
lsquobundlesrsquo of recommendations are more effective thanthe sum of the individual components
TUBERCULOSIS
The main risk factors are listed in Box 362 Typicalclinical features include fever sweating weight losslassitude anorexia cough productive of mucoid orpurulent sputum haemoptysis chest wall pain dysp-noea localised wheeze and apical crackles Patientsmay also present with unresolved pneumonia pleuraleffusions spontaneous pneumothorax and hoarseness
Figure 364 Management of suspected nosocomial pneumonia based on invasive sampling of respiratory secretions
Bacteria onGram stain
Yes
Yes
No
Yes No Yes No
No
Start antibiotics immediatelyusing PSBBAL specimen
and Gram stain results
Start antibioticsimmediately based onepidemiological clues
Observe look forother infection
Signs ofsevere sepsis
Immediate PSB or BAL beforechangingstarting antimicrobial therapy
+ve cultures +ve cultures
Adjust therapybased on
culture results
Continueadjustantibiotics Look for
other infection
Start antibioticson basisof results
Look forother infection
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1017
Tuberculosis 423
Table 364 Strategies for prevention of ventilator-associated pneumonia
LEVELS OF
RECOMMENDATIONS SPECIFIC INTERVENTIONS REMARKS
Universally recommendedby all guidelines27ndash30
1 Semirecumbent position to 45deg At least 30ndash45deg2 Avoidance of endotracheal intubation3 Preference of oral tracheal route
4 New circuit for a new patient and noschedule change unless soiled or damaged5 Avoidance of flushing of condensate into
lower airway or in-line medication6 HME changes no more frequently than 5ndash7
days7 Continuous aspiration of subglottic suctioning For patients expected to require mechanical
ventilation for gt72 hours
Generally recommendedby most guidelines
1 Preferential use of non-invasiveventilation272830
2 Avoidance of unplanned re-intubation272830
3 Maintenance of endotracheal cuff pressureof about 20 mmHg (266 kPa)272830
4 Closed suctioning2829
No effect on VAP mainly for staff safety5 Chlorhexidine oral decontamination272930
6 Sedation vacation and weaning protocol2728
7 Judicious use of stress ulcer prophylaxis272830
8 Restrictive blood transfusion28
Benefits less clear 1 Preference of HME over heatedhumidifier2830
HME associated with reduction in VAP inpatients ventilated for gt7 days lower cost
2 Silver-sulfadiazine-coated endotrachealtube272830
3 Early tracheostomy (within 7 days ofmechanical ventilation)29
4 Selective decontamination of digestive tract(SDD)272830
Mortality reduction demonstrated when topicalantimicrobials combined with short-course
systemic antibiotics BSAC recommendedSDD in patients expected to requiremechanical ventilation for gt48 hours ETFdiscourage routine use due to concern ofemergence of resistant organisms
Not yet reviewed byguidelines50
1 High-volume low-pressure ultrathin membraneendotracheal tube cuff with SSD
2 Ultrathin membrane cuff with tapered shapeand SSD
3 Low-volume low-pressure endotracheal tubecuff with SSD
4 Balloon device for biofilm removal5 Saline instillation before tracheal suctioning
HME= heat moist exchanger SSD= subglottic secretion drainage
smear-negative patients with pulmonary tuberculosisbut have the advantage of a much more rapid resultThere is however a signicant false-negative rate32
CHEST X-RAY (CXR)A normal CXR almost excludes TB (except inHIV-infected patients) but endobronchial lesionsmay not be apparent and early apical lesions can bemissed Common appearances include patchynodular
shadowing in the upper zones (often bilateral) cavita-tion calcication hilar or mediastinal lymphadenopa-thy (may cause segmental or lobar collapse) pleuraleffusion tuberculomas (dense round or oval shadows)and diffuse ne nodular shadowing throughout thelung elds in miliary TB Inactivity of disease cannot beinferred from the CXR alone This requires three nega-tive sputum samples and failure of any lesion seen onCXR to progress CXR appearances in HIV-positive
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1117
424 Pneumonia
t-tested negative-pressure respirator (N95 FFP2 orhigher) Use of a powered air-purifying respiratorshould be considered when bronchoscopy is being per-formed35 Detailed infection control advice can beobtained via the lsquolink pagersquo (httpwwwaiccuhk eduhkweb8Pneumonia20guidelineshtm)
PNEUMONIA IN THEIMMUNOCOMPROMISED
The lungs are amongst the most frequent targetorgans for infectious complications in the immuno-compromised The incidence of pneumonia is highestamongst patients with haematological malignanciesbone marrow transplant (BMT) recipients and patientswith AIDS
The speed of progression of pneumonia the CXRchanges (Table 365) and the type of immune defectprovide clues to the aetiology Bacterial pneumonias
progress rapidly (1ndash2 days) whereas fungal and proto-zoal pneumonias are less fulminant (several days to aweek or more) Viral pneumonias are usually not ful-minant but on occasions may develop quite rapidlyBronchoscopy is a major component of the investiga-tion of these patients Empirical management based onCXR appearances is outlined in Table 365 Early non-invasive ventilation may improve outcome amongstimmunocompromised patients with fever and bilateralinltrates36
PNEUMOCYSTIS JIROVECI PNEUMONIA (PCP)37
The incidence of this common opportunistic infectionhas fallen substantially in patients with AIDS whoare receiving prophylaxis and effective antiretroviraltherapy with most cases occurring in patients who arenot receiving HIV care or among patients with advancedimmunosuppression The onset is usually insidiouswith dry cough dyspnoea and fever on a backgroundof fatigue and weight loss Crackles in the chest are rareApproximately 15 of patients have a concurrent causefor respiratory failure (eg Kaposi sarcoma TB bacte-rial pneumonia) Useful investigations are
1 CXR classical appearance is diffuse bilateral perihi-
lar interstitial shadowing but in the early stages thisis very subtle and easily missed The initial CXR isnormal in 10 In a further 10 the changes areatypical with focal consolidation or coarse patchyshadowing None of the changes are specic for PCPand may be seen in other lung diseases associatedwith AIDS Pleural effusions hilar or mediastinallymphadenopathy are unusual in PCP but commonin mycobacterial infection or Kaposirsquos sarcoma orlymphoma
2 Induced sputum in this technique the patient inhalesnebulised hypertonic saline from an ultrasonic neb-uliser This provokes bronchorrhoea and the patient
patients with TB differ from those in non-HIV-infectedpatients
TREATMENT OF PULMONARY TB32ndash34
The decision to initiate anti-TB treatment should bebased on level of clinical suspicion results of AFBsmear and sometimes mycobacterial culture If the
initial clinical suspicion is strong and the patient is seri-ously ill attributable to possible TB treatment shouldbe initiated promptly sometimes before the result ofAFB smear Subsequent positivity of AFB smear ornucleic acid amplication test provides support to thecontinuation of treatment Combination chemotherapyconsisting of four drugs is necessary for maximal ef-cacy Treatment is divided into initial phase and con-tinuation phase The most commonly used initialregimen consists of 8 weeks of rifampicin 600 mg daily(450 mg for patients lt50 kg) isoniazid 300 mg dailypyrazinamide 2 g daily (15 g for patients lt50 kg) and
ethambutol 15 mgkg daily as initial phase treatmentEthambutol should be used only in patients who havereasonable visual acuity and who are able to appreciateand report visual disturbances This mandates carefulconsideration in patients who require heavy sedationVisual acuity and colour perception must be assessed(if ethambutol is to be used) and liver and renal func-tion checked before treatment is started Steroids arerecommended for children with endobronchial diseaseand possibly for patients with tuberculous pleuraleffusions Pyridoxine 10 mg daily should be given toprevent isoniazid-induced neuropathy to those atincreased risk (eg patients with diabetes mellitus
chronic renal failure or malnutrition or alcoholic orHIV-positive patients) Negative AFB smear should notdelay initial treatment if clinical suspicion remainshigh Supporting features included chronic coughweight loss characteristic chest X-ray ndings emigra-tion from a high-incidence country no other immediatediagnosis and positive tuberculin test
INFECTION CONTROL
Patients admitted to an ICU with infectious TB or sus-pected of having active pulmonary TB should bemanaged in an isolation room with special ventilation
characteristics including negative pressure Patientsshould be considered infectious if they are coughing orundergoing cough-inducing procedures or if they havepositive AFB smears and they are not on or have juststarted chemotherapy or have a poor clinical or bacte-riological response to chemotherapy3235 Patients withnon-drug-resistant TB should be non-infectious after 2weeks of treatment which includes rifampicin and iso-niazid32 As TB spreads through aerosols it is probablyappropriate to isolate patients who are intubated evenif only their bronchial washings are smear-positiveStaff caring for patients who are smear-positive shouldwear personal protective equipment including a
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1217
Pneumonia in the immunocompromised 425
andor diuretics (patients often uid-overloaded)Approximately 40 of patients with HIV-related PCPwho require mechanical ventilation survive to hospitaldischarge38
Initiation of antiretroviral therapy in patients pre-senting with HIV-related PCP is controversial TheCenters for Disease Control and Prevention (CDC) rec-ommend against doing so in the acute phase but recent
data suggest that the outcome may be improved byinitiation within the rst 4 days of ICU admission39
BACTERIAL PNEUMONIA37
This is the most common cause of acute respiratoryfailure in HIV-positive patients Bacterial pneumonia ismore common in HIV-infected patients than in thegeneral population and tends to be more severe Strep pneumoniae H infuenza Pseudomonas aeruginosa and Saureus are the commonest organisms Nocardia andGram negatives should also be considered Atypicalpathogens (eg Legionella) are rare Response to appro-
priate antibiotics is usually good but may require pro-tracted courses of antibiotics because of high tendencyto relapse Patients with severe immunodeciency(CD4+ T lymphocyte count lt100983221L) and a history ofPseudomonas infection or bronchiectasis or neutropeniashould receive antibiotics that cover P aeruginosa aswell as other Gram negatives The possibility of concur-rent PCP or tuberculosis should be excluded
TUBERCULOSIS
TB may be the initial presentation of AIDS particularlyin sub-Saharan Africa The pattern of TB in HIV patients
coughs up material containing cysts and tropho-zoites The technique is time-consuming and requiresmeticulous technique and is less sensitive thanbronchoscopy but less invasive The possibility ofconcurrent tuberculosis should be consideredand steps taken to minimise the risk of spread ofinfection
3 Bronchoscopy with bronchoalveolar lavage leads to
the diagnosis in over 90 of cases Specimens shouldbe sent for cytology Transbronchial biopsy is notnecessary in most cases PCR using bronchial lavagespecimens may be useful in non-HIV patients withsuspected PCP
Antipneumocystis treatment should be started as soonas the diagnosis is suspected Treatment of choice istrimethoprim plus sulfamethoxazole (co-trimoxazole)20 mgkgday+ 100 mgkgday for 3 weeks plusprednisolone 40 mg orally twice daily for 5 days fol-lowed by 20 mg twice daily for 5 days and then 20 mgper day until the end of PCP treatment Side-effects of
co-trimoxazole are common in HIV patients (nauseavomiting skin rash myelotoxicity) The dose should bereduced by 25 if the WBC count falls Patients whoare intolerant of co-trimoxazole should be treated with
bull pentamidine 4 mgkgday iv or
bull primaquine with clindamycin or
bull trimetrexate with leucovorin (plusmnoral dapsone)
Response to treatment is usually excellent with aresponse time of 4ndash7 days If the patient deteriorates orfails to improve consider (re-)bronchoscopy (is thediagnosis correct) treat co-pathogens and considera short course of high-dose iv methylprednisolone
Table 365 Causes of CXR changes and empirical treatment of pneumonia in the immunocompromised
CHEST X-RAY
APPEARANCE CAUSES
EMPIRICAL TREATMENT FOR
SUSPECTED PNEUMONIA
Diffuse infiltrate CMV and other herpes virusesPneumocystis carinii Bacteria
Aspergillus (advanced)Cryptococcus (uncommon)Non-infectious causes eg drug reaction non-specific
interstitial pneumonitis radiation pneumonitis(uncommon) malignancy leucoagglutinin reaction
Broad-spectrum antibiotics for at least 48 h(eg 3rd-generation cephalosporin andaminoglycoside)
Co-trimoxazoleLung biopsy or lavage within 48 h or full2-week course of co-trimoxazole (dependson patient tolerance of invasive procedure)
Focal infiltrate Gram-negative rodsS aureusAspergillusCryptococcusNocardiaMucorP carinii (uncommon)Tuberculosis
LegionellaNon-infectious causes (eg malignancy non-specificinterstitial pneumonitis radiation pneumonitis)
Broad-spectrum antibioticsIf response seen continue treatment for
2 weeksIf disease progresses lung biopsyaspirate
within 48ndash72 hours or empirical trial ofantifungalplusmn macrolide
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1317
426 Pneumonia
reaction are the most useful tests for demonstratingCMV disease Using thresholds of 10300 000ndash50200 000 positive circulating peripheral WBC the posi-tive predictive value for CMV-pp65 ranges from64 to 82 and the negative predictive value from70 to 954344 Treatment consists of intravenous gan-ciclovir for at least 14 days Foscarnet can be used if
ganciclovir fails
FUNGAL PNEUMONIA
Fungi are rare but important causes of pneumoniaThey can be divided into two main groups based on theimmune response required to combat infection withthese organisms Histoplasma blastomycosis coccidi-oidomycosis paracoccidioidomycosis and Cryptococcus require specic cell-mediated immunity for their controland thus in contrast to infections that are controlled byphagocytic activity the diseases caused by these organ-isms can occur in otherwise healthy individuals
although they cause much more severe illness inpatients with impaired cell-mediated immunity (egpatients infected with HIV and organ transplant recipi-ents) With the exception of Cryptococcus these organ-isms are rarely seen outside North America Aspergillus and Mucor spores are killed by non-immune phago-cytes and as a result these fungi rarely result in clinicalillness in patients with normal neutrophil numbers andfunction
CANDIDIASIS This is effectively a combination of the two types offungal infection in which impaired cell-mediatedimmunity predisposes to mucosal overgrowth withCandida but impaired phagocytic function or numbersis usually required before deep invasion of tissuesoccurs Primary Candida pneumonia (ie isolated lunginfection) is uncommon4145 and more commonly pul-monary lesions are only one manifestation of dissemi-nated candidiasis Even more common is benigncolonisation of the airway with Candida In mostreported cases of primary Candida pneumonia ampho-tericin B has been used In disseminated candidiasistreatment should be directed to treatment of dissemi-nated disease rather than Candida pneumonia per se45
INVASIVE ASPERGILLOSIS 46
This is a highly lethal condition in the immunocom-promised despite treatment and therefore investiga-tion and treatment should be prompt and aggressiveIt is associated with exposure to construction workDenitive diagnosis requires both histological evidenceof acute-angle branching septated non-pigmentedhyphae measuring 2ndash4 983221m in width and cultures yield-ing Aspergillus species from biopsy specimens ofinvolved organs Recovery of Aspergillus species fromrespiratory secretions in immunocompromised butnot immunocompetent patients may indicate invasive
disease with a positive predictive value as high as
depends on the degree of immunosuppression Inpatients with CD4+ T lymphocytes gt350 cells983221L theclinical presentation is similar to TB in non-HIV-infectedpatients although extrapulmonary disease is morecommon In patients with CD4+ T lymphocytes lt350cells983221L extrapulmonary disease (pleuritis pericardi-tis meningitis) is common Severely immunocompro-
mised patients (CD4+
T lymphocytes lt100 cells983221L)may present with severe systemic disease with highfever rapid progression and systemic sepsis In thesepatients lower and middle lobe disease is more commonmiliary disease is common and cavitation is lesscommon Sputum smears and culture may be positiveeven with a normal CXR
Response to treatment is usually rapid Managementof TB in HIV is complex owing to numerous druginteractions consultation with an expert in treatment ofHIV-related TB should be strongly considered Complexinteractions occur between rifamycins (eg rifampicinand rifabutin) and protease inhibitors and non-
nucleoside reverse transcriptase inhibitors used to treatpatients infected with HIV The choice of rifampicin orrifabutin depends on a number of factors includingthe unique and synergistic adverse effects for each indi-vidual combination of rifampicin and anti-HIV drugsand consultation with a physician with experiencein treating both TB and HIV is advised40 IDSA-recommended dosage adjustment for patients receivingantiretrovirals and rifabutin37 can be obtained viathe lsquolink pagersquo (httpwwwaiccuhkeduhkweb8Pneumonia20guidelineshtm) The optimal time forinitiating antiretroviral therapy in patients with TB iscontroversial Early therapy may decrease HIV disease
progression but may be associated with a high inci-dence of adverse effects and an immune reconstitutionreaction37
CMV PNEUMONITIS4142
Risk of infection is highest following allogeneic stemcell transplantation followed by lung transplantationpancreas transplantation and then liver heart and renaltransplantation and advanced AIDS If both the recipi-ent and the donor are seronegative then the risk of bothinfection and disease are negligible If the recipient is
seropositive the risk of infection is approximately 70but the risk of disease is only 20 regardless of theserostatus of the donor However if the recipient isseronegative and the donor is seropositive the risk ofdisease is 70 If steroid pulses and antilymphocyteglobulin are given for treatment of acute rejection therisk of developing disease is markedly increased Infec-tion may be the result of primary infection or reactiva-tion of latent infection It is clinically important butoften difcult to distinguish between CMV infectionand CMV disease and a denitive diagnosis can bemade only histologically Detection of CMV-pp65antigen in peripheral WBC and detection of CMV DNA
or RNA in the blood by quantitative polymerase chain
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1417
Parapneumonic effusion 427
needle aspiration or if there is debris within the uiddrainage using an intercostal drain The diagnosis isconrmed by aspiration of pus
TREATMENT The mainstay of treatment is drainage either by inter-costal drain or by surgical intervention Patients whopresent before the pus is loculated and a brinous peelhas formed on the lung can usually be treated bysimple drainage The combination with intrapleuralbrinolysis may be benecial Optimal surgical man-agement which consists of decortication (open or tho-racoscopic) is indicated if the empyema is moreadvanced or if simple drainage fails This is a majorprocedure and many patients with cardiac or chronicrespiratory disease will not tolerate it Alternatives forthese patients are instillation of thrombolytics into thepleural space or thoracostomy Antibiotics have onlyan adjunctive role Broad-spectrum antibiotic regimenswith anaerobic cover should be used until the resultsof microbiological analysis of the aspirated pus areavailable
AcknowledgementsAll tables and gures are reproduced from ICU web(wwwaiccuhkeduhkweb8) with permission of theauthors
80ndash90 in patients with leukaemia or bone marrowtransplant recipients Bronchoalveolar lavage withsmear culture and antigen detection has excellent spe-cicity and reasonably good positive predictive valuefor invasive aspergillosis in immunocompromisedpatients Although radiological features may give a clueto the diagnosis they are not sufciently specic to be
diagnosticIn acutely ill immunocompromised patients intrave-nous therapy should be initiated if there is suggestiveevidence of invasive aspergillosis while further investi-gations to conrm or refute the diagnosis are carriedout First-line therapy is voriconazole47 Echinocandinsand amphotericin are alternatives
PARAPNEUMONIC EFFUSION
This may be an uncomplicated effusion that resolveswith appropriate treatment of the underlying pneumo-nia or a complicated effusion that develops into an
empyema unless drained Complicated effusions tendto develop 7ndash14 days after initial uid formation Theyare characterised by increasing pleural uid volumecontinued fever and pleural uid of low pH (lt73) thatcontains a large number of neutrophils and may revealorganisms on Gram staining or culture An outline ofmanagement is given in Figure 365
EMPYEMA48
DEFINITION Collection of pus in the pleural space
AETIOLOGY Follows infection of the structures surrounding thepleural space including subdiaphragmatic structuresand chest trauma or may be associated with malig-nancy Anaerobic bacteria usually streptococci orGram-negative rods are responsible for 76 of cases
DIAGNOSIS The diagnosis is usually simple The patient is usuallyseptic and may have a productive cough and chest painThe chest X-ray may show features suggestive of apleural effusion and underlying consolidation but may
also show an abscess cavity with a uid level in whichcase CT scanning will be required to distinguishbetween an abscess and an empyema Ultrasound canbe useful to conrm the presence of uid in the pleuralspace and to determine whether it can be drained by
Figure 365 An approach to the management of
parapneumonic effusions
Parapneumonic effusion
gt 1 cm thick
on lateral decubitus
film
Pleural aspirate
turbid or purulent or
Gram stain +ve
Pleural aspirate
pH
Serial thoracocentesis Treat as empyemaObserve
No
gt72 lt70
70ndash72
No
Yes
Yes
httpwwwexpertconsultcomAccess the complete references list online at
1 American Thoracic Society and Infectious Diseases Society of America Guidelines for the manage-ment of adults with hospital-acquired ventilator-associated and healthcare associated pneumonia
Am J Respir Crit Care Med 2005171388ndash416
2 Mandell LA Wunderink RG Anzueto A et al Infec-tious Diseases Society of AmericaAmerican Tho-racic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin
Infect Dis 200744S27ndash72
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1517
428 Pneumonia
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1617
References 428e1
REFERENCES 1 American Thoracic Society and Infectious Diseases
Society of America Guidelines for the management of adults with hospital-acquired ventilator-associated and healthcare associated pneumonia Am J Respir Crit Care Med 2005171388ndash416
2 Mandell LA Wunderink RG Anzueto A et al Infec-tious Diseases Society of AmericaAmerican Tho-racic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744S27ndash72
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
4 Woodhead M Blasi F Ewig S et al Guidelines for the management of adult lower respiratory tract infections Eur Respir J 2005261138ndash80
5 Torres A Rello J Update in community-acquired and nosocomial pneumonia 2009 Am J Respir Crit
Care Med 2010181782ndash76 Van der Eerden MM Vlaspolder F de Graaff CS et
al Value of intensive diagnostic microbiological investigation in low- and high-risk patients with community-acquired pneumonia Eur J Clin Micro Infect Dis 200524241ndash9
7 Murdoch DR Nucleic acid amplication tests for the diagnosis of pneumonia Clin Infect Dis 2003361162ndash70
8 Blaschke AJ Interpreting assays for the detection of Streptococcus pneumonia Clin Infect Dis 201152(S4)S331ndash7
9 Rello J Lisboa T Lujan M Severity of pneumococcal
pneumonia associated with genomic bacterial load Chest 2009136832ndash4010 Azoulay E Bergeron A Polymerase chain reaction
for diagnosing pneumocystis pneumonia in non-HIV immunocompromised patients with pulmonary inl-trates Chest 2009135(3)655
11 Garcia-Vidal C Fernandez-Sabe N Carratala J Early mortality in patients with community-acquired pneumonia causes and risk factors Eur Respir J200832733ndash9
12 Dellinger RP Carlet JM Masur H et al Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock Intensive Care Med200430536ndash55
13 Metersky ML Ma A Houck PM et al Antibiotics for bacteremic pneumonia improved outcomes with macrolides but not uoroquinolones Chest 2007131466ndash73
14 Dunbar LM Wunderink RG Habib MP High-dose short-course levooxacin for community-acquired pneumonia a new treatment paradigm Clin Infect Dis 200337752ndash60
15 Matthaiou DK Ntani G An ESICM systematic review and meta-analysis of procalcitonin-guided antibiotic therapy algorithms in adult critically ill patients Intensive Care Med 201238940ndash9
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
17 Gruber PC Gomersall CD Joynt GM Avian inu-enza (H5N1) implications for intensive care Inten-sive Care Med 200632823ndash9
18 Belongia EA Irving SA Clinical characteristics and 30-day outcomes for inuenza A 2009 (H1N1) 2008ndash2009 (H1N1) and 2007ndash8 (H3N2) infections JAMA2010304(10)1091
19 Lee N Chan PKS Complications and outcomes of pandemic 2009 inuenza A (H1N1) virus infection in hospitalized adults how do they differ from those in seasonal inuenza J Infect Dis 20112031739ndash47
20 Kim SH Hong SB Corticosteroid treatment in critically ill patients with pandemic inuenza AH1N1 2009 infection analytic strategy using pro-pensity scores Am J Respir Crit Care Med 20111831207ndash14
21 Centers for Disease Control and Prevention (CDC) Bacterial coinfections in lung tissue specimens from
fatal cases of 2009 pandemic inuenza A (H1N1) ndash United States MayndashAugust 2009 MMWR 2009581071ndash4
22 Safdar N Dezfulian C Clinical and economic conse-quences of ventilator-associated pneumonia A sys-tematic review Crit Care Med 200533(10)2184ndash93
23 Shorr AF Sherner JH Invasive approaches to the diagnosis of ventilator-associated pneumonia A meta-analysis Crit Care Med 200533(1)46ndash53
24 Melsen WG Rovers MM Ventilator-associated pneumonia and mortality A systematic review of observational studies Crit Care Med 2009372709ndash18
25 Bekaert M Timsit JF Attributable mortality of ventilator-associated pneumonia A reappraisal using causal analysis Am J Respir Crit Care Med20111841133ndash9
26 CDC Healthcare Infection Control Practices AdvisoryCommittee Guidelines for preventing health-care-associated pneumonia 2003 Recommendations ofCDC and the Healthcare Infection Control PracticesAdvisory Committee Online Available httpwwwcdcgovmmwrpreviewmmwrhtmlrr5303a1htm
27 Cofn SE Klompas M SHEAIDSA practice recom-mendation strategies to prevent ventilator-associated pneumonia in acute care hospitals Infect Control
Hosp Epidemiol 200829S31ndash4028 Masterton RG Galloway A Guidelines for the man-
agement of hospital-acquired pneumonia in the UK Report of the Working Party on Hospital-Acquired Pneumonia of the British Society for Antimicrobial Chemotherapy J Antimicrob Chemother 2008625ndash34
29 VAP Guidelines Committee and the Canadian Critical Care Trials Group Comprehensive evidence-based clinical practice guidelines for ventilator-associated pneumonia prevention J Crit Care 200823126ndash37
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1717
428e2 Pneumonia
30 Torres A Ewig S Dening treating and preventing hospital acquired pneumonia European perspective Intensive Care Med 2009359ndash29
31 Frame RN Johnson MC Eichenhorn MS et al Active tuberculosis in the medical intensive care unit a 15-year retrospective analysis Crit Care Med 1987151012ndash14
32 National Collaborating Centre for Chronic Condi-tions Tuberculosis Clinical diagnosis and manage-ment of tuberculosis and measures for its prevention and control London Royal College of Physicians 2006
33 Small PM Fujiwara PI Management of tuberculosis in the United States N Engl J Med 2001345189ndash200
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
35 Centers for Disease Control and Prevention Guide-lines for preventing the transmission of Mycobacte-rium tuberculosis in health-care settings 2005 MMWR
2005541ndash11936 Hilbert G Gruson D Vargas F et al Noninvasive
ventilation in immunosuppressed patients with pul-monary inltrates fever and acute respiratory failure N Engl J Med 2001344481ndash7
37 Benson CA Kaplan JE Masur H Treating oppor-tunistic infections among HIV-infected adults and adolescents recommendations from CDC the National Institutes of Health and the HIV Medicine AssociationInfectious Diseases Society of America Clin Infect Dis 200540S131ndash235
38 Randall CJ Yarnold PR Schwartz DN et al Improve-ments in outcomes of acute respiratory failure for
patients with human immunodeciency virus-related Pneumocystis carinii pneumonia Am J Respir Crit Care Med 2000162393ndash8
39 Croda J Croda MG Neves A et al Benet of antiret-roviral therapy on survival of human immunode-ciency virus-infected patients admitted to an intensive care unit Crit Care Med 200937(5)1605
40 Centers for Disease Control Updated guidelines for the use of rifabutin or rifampicin for the treatment and prevention of tuberculosis among HIV-infected patients taking protease inhibitors or nonnucleoside reverse transcriptase inhibitors MMWR 200049185ndash9
41 Tamm M The lung in the immunocompromised patient Infectious complications part 2 Respiration199966199ndash207
42 Van der Bij W Speich R Management of cytomega-lovirus infection and disease after solid-organ trans-plantation Clin Infect Dis 200133(Suppl 1)S32ndash7
43 Schaumlfer P Tenschert W Cremaschi L et al Area under the viraemia curve versus absolute viral load utility for predicting symptomatic cytomegalovirus infections in kidney transplant patients J Med Virol20016585ndash9
44 Meyer-Koenig U Weidmann M Kirste G et al Cytomegalovirus infection in organ-transplant recip-ients diagnostic value of pp65 antigen test qualita-tive polymerase chain reaction (PCR) and quantitative
Taqman PCR Transplantation 2004771692ndash8
45 Pappas PG Rex JH Sobel JD Guidelines for treat-ment of candidiasis Clin Infect Dis 200438161ndash89
46 Stevens DA Kan VL Judson MA Practice guidelines for diseases caused by Aspergillus Clin Infect Dis200030696ndash709
47 Herbrecht R Denning DW Patterson TF Voricona-zole versus amphotericin B for primary therapy of invasive aspergillosis N Engl J Med 2002347408ndash15
48 Peek GJ Morcos S Cooper G The pleural cavity BMJ20003201318ndash21
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6

7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 417
Community-acquired pneumonia 417
contamination and colonisation PCR assays are moresensitive than culture for Mycoplasma and Chlamydia species and at least as sensitive for Legionella7 PCRassays also detect Legionella strains other than sero-group 1 The BTS guidelines3 recommend PCR of lowerrespiratory tract sample or if unavailable throat swabfor the diagnosis of Mycoplasma pneumonia PCR for
Chlamydophilia should be performed when invasiverespiratory samples were collected from patients withsevere community-acquired pneumonia The role ofPCR in diagnosing PCP is mainly limited to non-HIVpatients in whom conventional microscopy and stain-ing of induced sputum and BAL have a lower sensitiv-ity than in HIV patients9
MANAGEMENT
GENERAL SUPPORTIVE MEASURES Intravenous uids may be required to correct dehydra-
tion and provide maintenance uid A general approachshould be made to organ support with an emphasis oncorrecting hypoxia
ANTIMICROBIAL REGIMENS Increased mortality among those who do not receiveempirical antibiotics that cover the infecting pathogen(s)is well documented11 Each unit should have its ownregimens tailored to the local ora and antibiotic resist-ance patterns In the absence of such regimens theregimen outlined in Figure 361 may be helpful This
diagnostic of Legionella infection but a negativeresult does not exclude it In areas (eg South Aus-tralia) where other Legionella species are morecommon this test is less helpful
10 Urinary pneumococcal antigen has moderate sensi-tivity (50ndash80) and high specicity (gt90)
11 Microimmunouorescence serology for Chlamydia
pneumoniae IgM A titre ge1 16 is signicant12 HIV serological status
Other investigations should be considered in patientswith risk factors for infection with unusual organismsBronchoalveolar lavage may be useful in immunocom-promised patients those who fail to respond to antibi-otics or those in whom sputum samples cannot beobtained6
Molecular diagnosis (eg PCR-based methods) hasthe advantages of quick results (within 3 hours)enhanced sensitivity independence from organismviability and hence previous antibiotics and theoretical
possibility for determination of antimicrobial suscepti-bility7 Of note it is important to test for genes specicfor the organism in question10 and the sampling siteremains important PCR is most useful when performedon specimens from a normally sterile site For examplePCR for Pneumococcus is positive in 62 of bloodsamples from adult patients with conrmed or proba-ble pneumococcal pneumonia8 whereas blood culturesare positive in only 37 For respiratory specimensunder most circumstances interpretation remainsproblematic due to low specicity related to oral
Figure 361 Antibiotic regimens for treatment of severe community-acquired pneumonia in critically ill patients24 Respiratory fluoroquinolones include moxifloxacin and levofloxacin Advanced macrolides include azithromycin andclarithromycin Non-antipseudomonal third-generation cephalosporins include cefotaxime and ceftriaxone
Severe CAP
Aztreonam
and
levofloxacin
Piperacillin-tazobactam or
meropenem or imipenem or
cefepime and ciprofloxacin or
aminoglycoside plus
advanced macrolide
Respiratory
fluoroquinolone
plusmn clindamycin
Non anti-pseudomonal
third-generation cephalosporin
or ampicillin-sulbactam
and respiratory fluoroquinolone
or advanced macrolide
Risk of Pseudomonas
(COPDbronchiectasis
recent hospitalisation
recent antimicrobial
therapy or gross aspiration)
β-lactam
allergy
β-lactam
allergy
NoYes
NoYesNoYes
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 517
418 Pneumonia
should be modied in the light of risk factors (see Table 361) Quinolones may be less appropriate in areas witha high prevalence of TB as their use may mask concur-rent TB infection Appropriate antimicrobial therapyshould be administered within 1 hour of diagnosis412 There is controversy regarding the appropriate changeto empirical therapy based on microbiological nd-
ings24
Changing to narrower-spectrum antimicrobialcover may result in inadequate treatment of the 5ndash38of patients with polymicrobial infection Increasing evi-dence demonstrates improved outcome with combina-tion antimicrobial as compared with monotherapyparticularly in severely ill patients with bacteraemicpneumococcal pneumonia5 Odds ratio of death was15 to 6 for monotherapy as compared with com-bination therapy Benets were seen only in combina-tion therapy with macrolide as part of the regimen butnot in combination with uroquinolone regimen13 For the treatment of drug-resistant Strep pneumoniae (DRSP) the regimens in Figure 361 are probably suit-
able for isolates with a penicillin MIC lt 4 mgL2 Ifthe MIC is ge4 mgL an antipneumococcal uoroqui-nolone vancomycin teicoplanin or linezolid should begiven4
DURATION OF THERAPY No clinical trial has specically addressed this issueCourses as short as 5 days may be sufcient14 IDSAATS guidelines recommend stopping after a minimumof 5 days if the patient is afebrile for 48ndash72 hoursand organ dysfunction has largely resolved2 Shortcourses may be suboptimal for patients with bacterae-mic S aureus pneumonia meningitis or endocarditiscomplicating pneumonia or infection with less commonorganisms (eg Burkholderia pseudomallei or fungi) orPseudomonas aeruginosa Procalcitonin may be useful toguide antibiotic therapy but not all studies have dem-onstrated a benet15
RESPONSE TO THERAPY 2
This can be assessed subjectively (a response is usuallyseen within 1ndash3 days of starting therapy) or objectivelyon the basis of respiratory symptoms fever oxygena-tion WBC count bacteriology CXR changes C-reactiveprotein reduction and procalcitonin reduction of
80ndash90 from peak value The average time to deferves-cence varies with organism severity and patient age(7 days in elderly patients 25 days in young patientswith pneumococcal pneumonia 6ndash7 days in bacterae-mic patients with pneumococcal pneumonia 1ndash2 daysin patients with M pneumoniae pneumonia and 5 daysin patients with Legionella pneumonia) Both blood andsputum cultures are usually negative within 24ndash48hours of treatment although P aeruginosa and M pneu-moniae may persist in the sputum despite effectivetherapy CXR changes lag behind clinical changes withthe speed of change depending on the organism theage of the patient and the presence or absence of comor-
bid illnesses The CXR of most young or middle-aged
patients with bacteraemic pneumococcal pneumonia isclear by 4 weeks but resolution is slower in elderlypatients and patients with underlying illness extensivepneumonia on presentation or Legionella pneumophilia pneumonia
If the patient fails to respond consider the followingquestions
bull Has the patient got pneumonia
bull Are there host factors that explain the failure (egobstruction of bronchus by a foreign body or tumourinadequate host response)
bull Has a complication developed (eg empyema super-infection bronchiolitis obliterans organising pneu-monia metastatic abscess)
bull Is the right drug being given in an adequate dose bythe right route
bull Is the organism resistant to the drug being given
bull Are there other organisms
bull Is the fever a drug fever
Useful investigations include computerised tomogra-phy (CT) of the chest thoracocentesis bronchoalveolarlavage (Table 362) and transbronchial or open-lungbiopsy
PREDICTION OF ADVERSE OUTCOME ANDADMISSION TO ICU Scoring systems have been developed to predictadverse outcome and ICU admission including pneu-monia severity index (PSI) CURB-65 CRB-65 modiedATS major and minor criteria SCAP prediction ruleSMART-COP REA-ICU index and CAP-PIRO16
Although they may help identify the sicker patientsthey should not be used as a sole determinant of ICUadmission as local admission criteria will be affectedby local facilities both in and outside ICU It shouldbe noted that none of the criteria has been prospec-tively demonstrated to avoid late transfers or lowermortality
INFLUENZA PNEUMONIA
Inuenza pneumonia may present with severe respira-tory failure and multi-organ failure However the
pattern of organ failure appears to vary between strainswith H5N1 being associated with a much higher mor-tality and a higher incidence of multi-organ failure thanpandemic H1N117 which itself presented differently toseasonal inuenza In particular trophism for lowerrespiratory tract a higher rate of ICU admission18 anda higher rate of extrapulmonary complications19 wereobserved
Early initiation of oseltamivir is recommended forcritically ill patients although there is no direct evidenceof outcome benet Glucocorticoids do not appear tobe useful and may prolong viral replication20 Bacterialsuperinfection should be considered with Gram-
positive cocci being most frequently isolated21
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 617
Healthcare-associated pneumonia 419
failure and cancer) can cause inltrates on a chest X-rayIdentication of the organism responsible is even moredifcult than in patients with community-acquiredpneumonia owing to the high incidence of oropharyn-
geal colonisation by Gram-negative bacteria Blood cul-tures are positive in only about 6 of cases of nosocomialpneumonia Ventilator-associated pneumonia (VAP) isnosocomial pneumonia arising gt48ndash72 hours after intu-bation Reported incidence of VAP is between 10 and20 for those receiving mechanical ventilation for morethan 48 hours22 It is associated with a higher incidenceof multi-drug-resistant organisms1
PATHOGENESIS
Nosocomial pneumonia is thought to result from micro-aspiration of bacteria colonising the upper respiratory
tract Other routes of infection include macroaspiration
Although there are data demonstrating that surgicalmasks are as effective as N95 (FFP 2) masks in prevent-ing transmission of seasonal inuenza in non-ICU set-tings it is important to note that the capacity for airborne
transmission (and hence the need for N95 masks) isdependent on the exact characteristics of the organismand the frequency of aerosol-generating procedures sothese data should not be extrapolated to other inuenzaviruses and ICU settings
HEALTHCARE-ASSOCIATED PNEUMONIA
Nosocomial pneumonia occurs in 05ndash5 of hospitalpatients with a higher incidence in certain groups(eg postoperative patients and patients in ICU) Diag-nosis may be difcult the clinical features of pneumo-nia are non-specic and many non-infectious conditions
(eg atelectasis pulmonary embolus aspiration heart
Table 362 Procedure for obtaining microbiological samples using bronchoscopy and protected specimen brushingandor bronchoalveolar lavage3549
Infection control In patients suspected of having a disease that is transmitted by the airborne route (egtuberculosis)
bull the risk of transmission should be carefully weighed against the benefits ofbronchoscopy which may generate large numbers of airborne particles
bull perform bronchoscopy in a negative-pressure isolation room
bull consider the use of a muscle relaxant in ventilated patients to prevent coughingbull staff should wear personal protective equipment which should include a fit-tested
negative-pressure respirator (N95 FFP2 or above) as a minimum use of a poweredair-purifying respirator should be considered
General recommendations Suction through the endotracheal tube should be performed before bronchoscopyAvoid suction or injection through the working channel of the bronchoscopePerform protected specimen brushing before bronchoalveolar lavage
Ventilated patients Set F iO2 at 10
Set peak pressure alarm at a level that allows adequate ventilationTitrate ventilator settings against exhaled tidal volumeConsider neuromuscular blockade in addition to sedation in patients at high risk of
complications who are undergoing prolonged bronchoscopy
Protected specimen brushing (PSB) Sample the consolidated segment of lung at subsegmental levelIf purulent secretions are not seen advance the brush until it can no longer be seen but
avoid wedging it in a peripheral positionMove brush back and forth and rotate it several times
Bronchoalveolar lavage (BAL) Wedge tip of bronchoscope into a subsegment of the consolidated segment of lungInject aspirate and collect 20 mL of sterile isotonic saline Do not use this sample for
quantitative microbiology or identification of intracellular organisms It can be used forother microbiological analysis
Inject aspirate and collect additional aliquots of 20ndash60 mLThe total volume of saline injected should be 60ndash200 mL
Complications Hypoxaemia (possibly less with smaller BAL volumes)Arrhythmia
Transient worsening in pulmonary infiltratesBleeding (particularly following PSB)Fever (more common after BAL)
Positive results gt5 of cells in cytocentrifuge preparations of BAL fluid contain intracellular bacteria ORge103 colony-forming unitsmL in PSB specimen ORge104 colony-forming unitsmL in BAL fluid
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 717
420 Pneumonia
worse prognosis In 50 of patients with severehospital-acquired pneumonia and positive bloodcultures there is another source of sepsis
MANAGEMENT
Management is based on the nding that early treat-
ment with antimicrobials that cover all likely patho-gens results in a reduction in morbidity and mortality2 The initial selection of antimicrobials is made on thebasis of epidemiological clues (Fig 362 Table 363)Antimicrobials should be administered within 1 hourof diagnosis12 The results of microbiological investiga-tions are used to narrow antimicrobial cover laterTreatment should be reassessed after 2ndash3 days orsooner if the patient deteriorates (Fig 363) An outlineof management based on an invasive approach is givenin Figure 364
DURATION OF THERAPY
Current ATS guidelines recommend 7 daysrsquo treatmentprovided the aetiological agent is not P aeruginosa orother non-lactose fermenter and the patient has a goodclinical response with resolution of clinical features ofinfection1 The outcome of patients who receive appro-priate initial empirical therapy for ventilator-associatedpneumonia for 8 days is similar to those who receivetreatment for 15 days1
of gastric contents inhaled aerosols haematogenousspread spread from pleural space and direct inocula-tion from ICU personnel
CLINICAL DIAGNOSIS
Diagnosis is based on time of onset (gt48 hours afteradmission to a healthcare facility1) CXR changes (newor progressive inltrates) and either clinical featuresand simple laboratory investigations or the results ofquantitative microbiology Using a clinical approachpneumonia is diagnosed by the nding of a new inl-trate or a change in an inltrate on chest radiographand growth of pathogenic organisms from sputum plusone of the following white-blood-cell (WBC) countgreater than 12times l05L core temperature ge383degCsputum Gram stain with scores of more than two on ascale of four of polymorphonuclear leucocytes andbacteria
INVESTIGATIONSThese are broadly similar to those required incommunity-acquired pneumonia
bull Chest X-ray although studies using a histologicaldiagnosis as the gold standard have demonstratedthat pneumonia may be present despite a normalCXR most denitions of nosocomial pneumoniarequire the presence of new persistent inltrates ona CXR
bull Respiratory secretions considerable controversy sur-rounds the issue of whether invasive bronchoscopicsampling (Table 362) of respiratory secretions is nec-
essary Whether invasive sampling is employed ortracheal aspirates are used empirical broad-spectrumantibiotics should be started while results areawaited The results of microbiological analysis ofrespiratory secretions are used to either stop antibi-otics or narrow the spectrum1 Although the use ofan invasive strategy is associated with a higher like-lihood of modication of initial antimicrobials23 theeffect on important clinical outcome such as mortal-ity antibiotic-free days and organ dysfunction isvariable1 Although tracheal aspirates may predomi-nantly reect the organisms colonising the upper
airway they may be useful in indicating whichorganisms are not responsible for the pneumoniathus allowing the antimicrobial cover to be nar-rowed1 This interpretation is based on the premisethat the predominant route of infection is via theupper respiratory tract From this it can be assumedthat if the organism is not present in the upper res-piratory tract the probability of it being present inthe lung parenchyma is low Certain organisms arevirtually always pathogens when recovered fromrespiratory secretions (see Box 361)
bull Blood cultures identify the aetiological agent in8ndash20 of patients Bacteraemia is associated with a
Figure 362 An outline of initial management ofnosocomial pneumonia based on a non-invasive clinicalapproach1
Two ofuarr or darr WCC
purulent sputum
temp gt38degC
New CXR
infiltrates
Consider acute
tracheobronchitis
Obtain lower respiratory
tract specimens and blood for
microbiological investigations
Risk factorsfor multidrug-resistant
pathogens
Early broad-spectrum
antibiotic therapy
to cover multidrug-
resistant pathogens
Early limited-spectrum
antibiotic therapy
Yes
Yes
No
No
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 817
Healthcare-associated pneumonia 421
inltrate in 48 hours new cavitation or a signicantnew pleural effusion should raise concern If the patientfails to respond consider the diagnosis host factors (egimmunosuppressed debilitated) bacterial factors (egvirulent organism) and therapeutic factors (eg wrongdrug inadequate dose) Review the antibiotics andrepeat cultures It may be useful to broaden the antimi-crobial cover while waiting for the results of investiga-tions Consider invasive sampling of respiratorysecretions computerised tomography or ultrasound ofthe chest (to look for an empyema or abscess) anothersource of infection open-lung biopsy to establish diag-nosis and aetiology or administration of steroids
MORTALITY AND MORBIDITY ATTRIBUTABLE TO VAP Substantial morbidity and mortality associated withVAP have previously been reported22 However acausal relationship is difcult to establish It should benoted that patients who developed VAP tend to be
more severely ill and at higher risk of death not onlyon ICU admission but throughout the course of theirillness Most of the relevant studies were observationaland failed to adequately control confounders likedisease severity evolution of disease progression andICU length of stay with mortality In addition signi-cant heterogeneity exists among these studies Althoughthe presence of VAP is associated with a signicantlylonger ICU length of stay (mean of 61 days 95 CI532ndash687) and increased healthcare cost22 more recentstudies reported that mortality attributable to VAPtends to be small if any2425 The attributable mortalityhas been reported to be 1 on the 30th day of ICU and
RESPONSE TO THERAPY Clinical improvement is usually not apparent for 48ndash72hours and therapy should not be changed during thistime The CXR is of limited value for assessing responseinitial deterioration is common and improvement oftenlags behind clinical response However a rapidly dete-riorating CXR pattern with a gt50 increase in size of
Figure 363 Subsequent management of nosocomialpneumonia based on a non-invasive clinical approach1
Pathogens isolated
from respiratory
specimen
Antibiotics
changedstarted in 7 h
prior to sampling
Adjust antibiotics
according to sensitivities
Continue antibiotics if
high clinical suspicion of
nosocomial pneumonia
Bacterial pneumonia
unlikely
Investigate for other cause
of sepsis and CXR changes
Consider unusual causes
of nosocomial pneumonia
(eg Legionella viruses fungi
Pneumocystis carinii )
Yes
Yes
No
No
Table 363 Recommended initial empirical treatment for nosocomial pneumonia1
SITUATION ANTIBIOTICS
No risk factors for multidrug-resistant pathogens Ceftriaxone or Levofloxacin moxifloxacin or ciprofloxacin or Ampicillinsulbactam or Ertapenem
Antimicrobial therapy in previous 90 days or Current hospitalization for ge5 days or High frequency of antibiotic resistance in the specific
hospital unit or Hospitalisation for 2 days or more in previous 90 days or Residence in nursing home or extended care facility or Home infusion therapy (including antibiotics) or Chronic dialysis within 30 days or Home wound care or Family member with multidrug-resistant pathogen o rImmunosuppression or Bronchiectasis
One ofAntipseudomonal cephalosporin (cefepime or ceftazidime) or Antipseudomonal carbapenem (meropenem or imipenemndash
cilastin) or szlig-lactamszlig-lactamase inhibitor (eg piperacillinndashtazobactam or
cefaperazonendashsulbactam)plus one ofAminoglycoside or Antipseudomonal quinolone (levofloxacin or ciprofloxacin)plus one of the following for patients at high risk of meticillin-
resistant Staphylococcus aureus (MRSA) infectionLinezolid or Vancomycin or
TeicoplaninThe use of dual therapy is not well supported by evidence but it does reduce the probability that the pathogen is resistant to the drugsbeing given If an extended spectrum β-lactamase-producing strain or an Acinetobacter sp is suspected a carbapenem should be givenIf Legionella pneumophilia is suspected use a quinolone Risk factors for MRSA infection in areas with a high incidence of MRSA includediabetes mellitus head trauma coma and renal failure
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 917
422 Pneumonia
or with enlarged cervical nodes or other manifestationsof extrapulmonary disease Clinical disease is seldomfound in asymptomatic individuals even those withstrongly positive tuberculin test (Heaf grade III or IV)The outlook for patients with tuberculosis who requireICU admission is poor In one retrospective study thein-hospital mortality for all patients with tuberculosisrequiring ICU admission was 67 but in those withacute respiratory failure it rose to 8131 The presenta-tion and management of TB in HIV-positive patientsare different (see below)
INVESTIGATION OF PULMONARYTUBERCULOSIS
IDENTIFICATION OF MYCOBACTERIA
Multiple
3233
sputum samples should be collected pref-erably on different days for microscopy for acid-fastbacilli and culture If sputum is not available bronchialwashings taken at bronchoscopy and gastric lavage oraspirate samples should be obtained Gastric aspiratesneed to be neutralised immediately on collection Bron-choscopy and transbronchial biopsy may be useful inpatients with suspected TB but negative sputum smearPleural biopsy is often helpful and mediastinoscopyis occasionally needed in patients with mediastinallymphadenopathy Part of any biopsy specimen shouldalways be sent for culture Nucleic acid amplicationtests on sputum have sensitivity similar to culture in
15 on the 60th day of ICU in a recent study using amulticentre high-quality database and incorporatingnovel statistical methodology to control evolution ofseverity of illness25
PREVENTION
Several guidelines for prevention of ventilator-associated pneumonia and hospital-acquired pneumo-nia have been published26ndash30 Interventions can bedivided into general infection control measures andspecic measures General measures include alcohol-based hand disinfection hospital education programmeon infection control the use of microbiological sur-veillance and a programme to reduce antibiotic pre-scription The major specic recommendations aresummarised in Table 364 There is no evidence that
lsquobundlesrsquo of recommendations are more effective thanthe sum of the individual components
TUBERCULOSIS
The main risk factors are listed in Box 362 Typicalclinical features include fever sweating weight losslassitude anorexia cough productive of mucoid orpurulent sputum haemoptysis chest wall pain dysp-noea localised wheeze and apical crackles Patientsmay also present with unresolved pneumonia pleuraleffusions spontaneous pneumothorax and hoarseness
Figure 364 Management of suspected nosocomial pneumonia based on invasive sampling of respiratory secretions
Bacteria onGram stain
Yes
Yes
No
Yes No Yes No
No
Start antibiotics immediatelyusing PSBBAL specimen
and Gram stain results
Start antibioticsimmediately based onepidemiological clues
Observe look forother infection
Signs ofsevere sepsis
Immediate PSB or BAL beforechangingstarting antimicrobial therapy
+ve cultures +ve cultures
Adjust therapybased on
culture results
Continueadjustantibiotics Look for
other infection
Start antibioticson basisof results
Look forother infection
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1017
Tuberculosis 423
Table 364 Strategies for prevention of ventilator-associated pneumonia
LEVELS OF
RECOMMENDATIONS SPECIFIC INTERVENTIONS REMARKS
Universally recommendedby all guidelines27ndash30
1 Semirecumbent position to 45deg At least 30ndash45deg2 Avoidance of endotracheal intubation3 Preference of oral tracheal route
4 New circuit for a new patient and noschedule change unless soiled or damaged5 Avoidance of flushing of condensate into
lower airway or in-line medication6 HME changes no more frequently than 5ndash7
days7 Continuous aspiration of subglottic suctioning For patients expected to require mechanical
ventilation for gt72 hours
Generally recommendedby most guidelines
1 Preferential use of non-invasiveventilation272830
2 Avoidance of unplanned re-intubation272830
3 Maintenance of endotracheal cuff pressureof about 20 mmHg (266 kPa)272830
4 Closed suctioning2829
No effect on VAP mainly for staff safety5 Chlorhexidine oral decontamination272930
6 Sedation vacation and weaning protocol2728
7 Judicious use of stress ulcer prophylaxis272830
8 Restrictive blood transfusion28
Benefits less clear 1 Preference of HME over heatedhumidifier2830
HME associated with reduction in VAP inpatients ventilated for gt7 days lower cost
2 Silver-sulfadiazine-coated endotrachealtube272830
3 Early tracheostomy (within 7 days ofmechanical ventilation)29
4 Selective decontamination of digestive tract(SDD)272830
Mortality reduction demonstrated when topicalantimicrobials combined with short-course
systemic antibiotics BSAC recommendedSDD in patients expected to requiremechanical ventilation for gt48 hours ETFdiscourage routine use due to concern ofemergence of resistant organisms
Not yet reviewed byguidelines50
1 High-volume low-pressure ultrathin membraneendotracheal tube cuff with SSD
2 Ultrathin membrane cuff with tapered shapeand SSD
3 Low-volume low-pressure endotracheal tubecuff with SSD
4 Balloon device for biofilm removal5 Saline instillation before tracheal suctioning
HME= heat moist exchanger SSD= subglottic secretion drainage
smear-negative patients with pulmonary tuberculosisbut have the advantage of a much more rapid resultThere is however a signicant false-negative rate32
CHEST X-RAY (CXR)A normal CXR almost excludes TB (except inHIV-infected patients) but endobronchial lesionsmay not be apparent and early apical lesions can bemissed Common appearances include patchynodular
shadowing in the upper zones (often bilateral) cavita-tion calcication hilar or mediastinal lymphadenopa-thy (may cause segmental or lobar collapse) pleuraleffusion tuberculomas (dense round or oval shadows)and diffuse ne nodular shadowing throughout thelung elds in miliary TB Inactivity of disease cannot beinferred from the CXR alone This requires three nega-tive sputum samples and failure of any lesion seen onCXR to progress CXR appearances in HIV-positive
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1117
424 Pneumonia
t-tested negative-pressure respirator (N95 FFP2 orhigher) Use of a powered air-purifying respiratorshould be considered when bronchoscopy is being per-formed35 Detailed infection control advice can beobtained via the lsquolink pagersquo (httpwwwaiccuhk eduhkweb8Pneumonia20guidelineshtm)
PNEUMONIA IN THEIMMUNOCOMPROMISED
The lungs are amongst the most frequent targetorgans for infectious complications in the immuno-compromised The incidence of pneumonia is highestamongst patients with haematological malignanciesbone marrow transplant (BMT) recipients and patientswith AIDS
The speed of progression of pneumonia the CXRchanges (Table 365) and the type of immune defectprovide clues to the aetiology Bacterial pneumonias
progress rapidly (1ndash2 days) whereas fungal and proto-zoal pneumonias are less fulminant (several days to aweek or more) Viral pneumonias are usually not ful-minant but on occasions may develop quite rapidlyBronchoscopy is a major component of the investiga-tion of these patients Empirical management based onCXR appearances is outlined in Table 365 Early non-invasive ventilation may improve outcome amongstimmunocompromised patients with fever and bilateralinltrates36
PNEUMOCYSTIS JIROVECI PNEUMONIA (PCP)37
The incidence of this common opportunistic infectionhas fallen substantially in patients with AIDS whoare receiving prophylaxis and effective antiretroviraltherapy with most cases occurring in patients who arenot receiving HIV care or among patients with advancedimmunosuppression The onset is usually insidiouswith dry cough dyspnoea and fever on a backgroundof fatigue and weight loss Crackles in the chest are rareApproximately 15 of patients have a concurrent causefor respiratory failure (eg Kaposi sarcoma TB bacte-rial pneumonia) Useful investigations are
1 CXR classical appearance is diffuse bilateral perihi-
lar interstitial shadowing but in the early stages thisis very subtle and easily missed The initial CXR isnormal in 10 In a further 10 the changes areatypical with focal consolidation or coarse patchyshadowing None of the changes are specic for PCPand may be seen in other lung diseases associatedwith AIDS Pleural effusions hilar or mediastinallymphadenopathy are unusual in PCP but commonin mycobacterial infection or Kaposirsquos sarcoma orlymphoma
2 Induced sputum in this technique the patient inhalesnebulised hypertonic saline from an ultrasonic neb-uliser This provokes bronchorrhoea and the patient
patients with TB differ from those in non-HIV-infectedpatients
TREATMENT OF PULMONARY TB32ndash34
The decision to initiate anti-TB treatment should bebased on level of clinical suspicion results of AFBsmear and sometimes mycobacterial culture If the
initial clinical suspicion is strong and the patient is seri-ously ill attributable to possible TB treatment shouldbe initiated promptly sometimes before the result ofAFB smear Subsequent positivity of AFB smear ornucleic acid amplication test provides support to thecontinuation of treatment Combination chemotherapyconsisting of four drugs is necessary for maximal ef-cacy Treatment is divided into initial phase and con-tinuation phase The most commonly used initialregimen consists of 8 weeks of rifampicin 600 mg daily(450 mg for patients lt50 kg) isoniazid 300 mg dailypyrazinamide 2 g daily (15 g for patients lt50 kg) and
ethambutol 15 mgkg daily as initial phase treatmentEthambutol should be used only in patients who havereasonable visual acuity and who are able to appreciateand report visual disturbances This mandates carefulconsideration in patients who require heavy sedationVisual acuity and colour perception must be assessed(if ethambutol is to be used) and liver and renal func-tion checked before treatment is started Steroids arerecommended for children with endobronchial diseaseand possibly for patients with tuberculous pleuraleffusions Pyridoxine 10 mg daily should be given toprevent isoniazid-induced neuropathy to those atincreased risk (eg patients with diabetes mellitus
chronic renal failure or malnutrition or alcoholic orHIV-positive patients) Negative AFB smear should notdelay initial treatment if clinical suspicion remainshigh Supporting features included chronic coughweight loss characteristic chest X-ray ndings emigra-tion from a high-incidence country no other immediatediagnosis and positive tuberculin test
INFECTION CONTROL
Patients admitted to an ICU with infectious TB or sus-pected of having active pulmonary TB should bemanaged in an isolation room with special ventilation
characteristics including negative pressure Patientsshould be considered infectious if they are coughing orundergoing cough-inducing procedures or if they havepositive AFB smears and they are not on or have juststarted chemotherapy or have a poor clinical or bacte-riological response to chemotherapy3235 Patients withnon-drug-resistant TB should be non-infectious after 2weeks of treatment which includes rifampicin and iso-niazid32 As TB spreads through aerosols it is probablyappropriate to isolate patients who are intubated evenif only their bronchial washings are smear-positiveStaff caring for patients who are smear-positive shouldwear personal protective equipment including a
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1217
Pneumonia in the immunocompromised 425
andor diuretics (patients often uid-overloaded)Approximately 40 of patients with HIV-related PCPwho require mechanical ventilation survive to hospitaldischarge38
Initiation of antiretroviral therapy in patients pre-senting with HIV-related PCP is controversial TheCenters for Disease Control and Prevention (CDC) rec-ommend against doing so in the acute phase but recent
data suggest that the outcome may be improved byinitiation within the rst 4 days of ICU admission39
BACTERIAL PNEUMONIA37
This is the most common cause of acute respiratoryfailure in HIV-positive patients Bacterial pneumonia ismore common in HIV-infected patients than in thegeneral population and tends to be more severe Strep pneumoniae H infuenza Pseudomonas aeruginosa and Saureus are the commonest organisms Nocardia andGram negatives should also be considered Atypicalpathogens (eg Legionella) are rare Response to appro-
priate antibiotics is usually good but may require pro-tracted courses of antibiotics because of high tendencyto relapse Patients with severe immunodeciency(CD4+ T lymphocyte count lt100983221L) and a history ofPseudomonas infection or bronchiectasis or neutropeniashould receive antibiotics that cover P aeruginosa aswell as other Gram negatives The possibility of concur-rent PCP or tuberculosis should be excluded
TUBERCULOSIS
TB may be the initial presentation of AIDS particularlyin sub-Saharan Africa The pattern of TB in HIV patients
coughs up material containing cysts and tropho-zoites The technique is time-consuming and requiresmeticulous technique and is less sensitive thanbronchoscopy but less invasive The possibility ofconcurrent tuberculosis should be consideredand steps taken to minimise the risk of spread ofinfection
3 Bronchoscopy with bronchoalveolar lavage leads to
the diagnosis in over 90 of cases Specimens shouldbe sent for cytology Transbronchial biopsy is notnecessary in most cases PCR using bronchial lavagespecimens may be useful in non-HIV patients withsuspected PCP
Antipneumocystis treatment should be started as soonas the diagnosis is suspected Treatment of choice istrimethoprim plus sulfamethoxazole (co-trimoxazole)20 mgkgday+ 100 mgkgday for 3 weeks plusprednisolone 40 mg orally twice daily for 5 days fol-lowed by 20 mg twice daily for 5 days and then 20 mgper day until the end of PCP treatment Side-effects of
co-trimoxazole are common in HIV patients (nauseavomiting skin rash myelotoxicity) The dose should bereduced by 25 if the WBC count falls Patients whoare intolerant of co-trimoxazole should be treated with
bull pentamidine 4 mgkgday iv or
bull primaquine with clindamycin or
bull trimetrexate with leucovorin (plusmnoral dapsone)
Response to treatment is usually excellent with aresponse time of 4ndash7 days If the patient deteriorates orfails to improve consider (re-)bronchoscopy (is thediagnosis correct) treat co-pathogens and considera short course of high-dose iv methylprednisolone
Table 365 Causes of CXR changes and empirical treatment of pneumonia in the immunocompromised
CHEST X-RAY
APPEARANCE CAUSES
EMPIRICAL TREATMENT FOR
SUSPECTED PNEUMONIA
Diffuse infiltrate CMV and other herpes virusesPneumocystis carinii Bacteria
Aspergillus (advanced)Cryptococcus (uncommon)Non-infectious causes eg drug reaction non-specific
interstitial pneumonitis radiation pneumonitis(uncommon) malignancy leucoagglutinin reaction
Broad-spectrum antibiotics for at least 48 h(eg 3rd-generation cephalosporin andaminoglycoside)
Co-trimoxazoleLung biopsy or lavage within 48 h or full2-week course of co-trimoxazole (dependson patient tolerance of invasive procedure)
Focal infiltrate Gram-negative rodsS aureusAspergillusCryptococcusNocardiaMucorP carinii (uncommon)Tuberculosis
LegionellaNon-infectious causes (eg malignancy non-specificinterstitial pneumonitis radiation pneumonitis)
Broad-spectrum antibioticsIf response seen continue treatment for
2 weeksIf disease progresses lung biopsyaspirate
within 48ndash72 hours or empirical trial ofantifungalplusmn macrolide
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1317
426 Pneumonia
reaction are the most useful tests for demonstratingCMV disease Using thresholds of 10300 000ndash50200 000 positive circulating peripheral WBC the posi-tive predictive value for CMV-pp65 ranges from64 to 82 and the negative predictive value from70 to 954344 Treatment consists of intravenous gan-ciclovir for at least 14 days Foscarnet can be used if
ganciclovir fails
FUNGAL PNEUMONIA
Fungi are rare but important causes of pneumoniaThey can be divided into two main groups based on theimmune response required to combat infection withthese organisms Histoplasma blastomycosis coccidi-oidomycosis paracoccidioidomycosis and Cryptococcus require specic cell-mediated immunity for their controland thus in contrast to infections that are controlled byphagocytic activity the diseases caused by these organ-isms can occur in otherwise healthy individuals
although they cause much more severe illness inpatients with impaired cell-mediated immunity (egpatients infected with HIV and organ transplant recipi-ents) With the exception of Cryptococcus these organ-isms are rarely seen outside North America Aspergillus and Mucor spores are killed by non-immune phago-cytes and as a result these fungi rarely result in clinicalillness in patients with normal neutrophil numbers andfunction
CANDIDIASIS This is effectively a combination of the two types offungal infection in which impaired cell-mediatedimmunity predisposes to mucosal overgrowth withCandida but impaired phagocytic function or numbersis usually required before deep invasion of tissuesoccurs Primary Candida pneumonia (ie isolated lunginfection) is uncommon4145 and more commonly pul-monary lesions are only one manifestation of dissemi-nated candidiasis Even more common is benigncolonisation of the airway with Candida In mostreported cases of primary Candida pneumonia ampho-tericin B has been used In disseminated candidiasistreatment should be directed to treatment of dissemi-nated disease rather than Candida pneumonia per se45
INVASIVE ASPERGILLOSIS 46
This is a highly lethal condition in the immunocom-promised despite treatment and therefore investiga-tion and treatment should be prompt and aggressiveIt is associated with exposure to construction workDenitive diagnosis requires both histological evidenceof acute-angle branching septated non-pigmentedhyphae measuring 2ndash4 983221m in width and cultures yield-ing Aspergillus species from biopsy specimens ofinvolved organs Recovery of Aspergillus species fromrespiratory secretions in immunocompromised butnot immunocompetent patients may indicate invasive
disease with a positive predictive value as high as
depends on the degree of immunosuppression Inpatients with CD4+ T lymphocytes gt350 cells983221L theclinical presentation is similar to TB in non-HIV-infectedpatients although extrapulmonary disease is morecommon In patients with CD4+ T lymphocytes lt350cells983221L extrapulmonary disease (pleuritis pericardi-tis meningitis) is common Severely immunocompro-
mised patients (CD4+
T lymphocytes lt100 cells983221L)may present with severe systemic disease with highfever rapid progression and systemic sepsis In thesepatients lower and middle lobe disease is more commonmiliary disease is common and cavitation is lesscommon Sputum smears and culture may be positiveeven with a normal CXR
Response to treatment is usually rapid Managementof TB in HIV is complex owing to numerous druginteractions consultation with an expert in treatment ofHIV-related TB should be strongly considered Complexinteractions occur between rifamycins (eg rifampicinand rifabutin) and protease inhibitors and non-
nucleoside reverse transcriptase inhibitors used to treatpatients infected with HIV The choice of rifampicin orrifabutin depends on a number of factors includingthe unique and synergistic adverse effects for each indi-vidual combination of rifampicin and anti-HIV drugsand consultation with a physician with experiencein treating both TB and HIV is advised40 IDSA-recommended dosage adjustment for patients receivingantiretrovirals and rifabutin37 can be obtained viathe lsquolink pagersquo (httpwwwaiccuhkeduhkweb8Pneumonia20guidelineshtm) The optimal time forinitiating antiretroviral therapy in patients with TB iscontroversial Early therapy may decrease HIV disease
progression but may be associated with a high inci-dence of adverse effects and an immune reconstitutionreaction37
CMV PNEUMONITIS4142
Risk of infection is highest following allogeneic stemcell transplantation followed by lung transplantationpancreas transplantation and then liver heart and renaltransplantation and advanced AIDS If both the recipi-ent and the donor are seronegative then the risk of bothinfection and disease are negligible If the recipient is
seropositive the risk of infection is approximately 70but the risk of disease is only 20 regardless of theserostatus of the donor However if the recipient isseronegative and the donor is seropositive the risk ofdisease is 70 If steroid pulses and antilymphocyteglobulin are given for treatment of acute rejection therisk of developing disease is markedly increased Infec-tion may be the result of primary infection or reactiva-tion of latent infection It is clinically important butoften difcult to distinguish between CMV infectionand CMV disease and a denitive diagnosis can bemade only histologically Detection of CMV-pp65antigen in peripheral WBC and detection of CMV DNA
or RNA in the blood by quantitative polymerase chain
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1417
Parapneumonic effusion 427
needle aspiration or if there is debris within the uiddrainage using an intercostal drain The diagnosis isconrmed by aspiration of pus
TREATMENT The mainstay of treatment is drainage either by inter-costal drain or by surgical intervention Patients whopresent before the pus is loculated and a brinous peelhas formed on the lung can usually be treated bysimple drainage The combination with intrapleuralbrinolysis may be benecial Optimal surgical man-agement which consists of decortication (open or tho-racoscopic) is indicated if the empyema is moreadvanced or if simple drainage fails This is a majorprocedure and many patients with cardiac or chronicrespiratory disease will not tolerate it Alternatives forthese patients are instillation of thrombolytics into thepleural space or thoracostomy Antibiotics have onlyan adjunctive role Broad-spectrum antibiotic regimenswith anaerobic cover should be used until the resultsof microbiological analysis of the aspirated pus areavailable
AcknowledgementsAll tables and gures are reproduced from ICU web(wwwaiccuhkeduhkweb8) with permission of theauthors
80ndash90 in patients with leukaemia or bone marrowtransplant recipients Bronchoalveolar lavage withsmear culture and antigen detection has excellent spe-cicity and reasonably good positive predictive valuefor invasive aspergillosis in immunocompromisedpatients Although radiological features may give a clueto the diagnosis they are not sufciently specic to be
diagnosticIn acutely ill immunocompromised patients intrave-nous therapy should be initiated if there is suggestiveevidence of invasive aspergillosis while further investi-gations to conrm or refute the diagnosis are carriedout First-line therapy is voriconazole47 Echinocandinsand amphotericin are alternatives
PARAPNEUMONIC EFFUSION
This may be an uncomplicated effusion that resolveswith appropriate treatment of the underlying pneumo-nia or a complicated effusion that develops into an
empyema unless drained Complicated effusions tendto develop 7ndash14 days after initial uid formation Theyare characterised by increasing pleural uid volumecontinued fever and pleural uid of low pH (lt73) thatcontains a large number of neutrophils and may revealorganisms on Gram staining or culture An outline ofmanagement is given in Figure 365
EMPYEMA48
DEFINITION Collection of pus in the pleural space
AETIOLOGY Follows infection of the structures surrounding thepleural space including subdiaphragmatic structuresand chest trauma or may be associated with malig-nancy Anaerobic bacteria usually streptococci orGram-negative rods are responsible for 76 of cases
DIAGNOSIS The diagnosis is usually simple The patient is usuallyseptic and may have a productive cough and chest painThe chest X-ray may show features suggestive of apleural effusion and underlying consolidation but may
also show an abscess cavity with a uid level in whichcase CT scanning will be required to distinguishbetween an abscess and an empyema Ultrasound canbe useful to conrm the presence of uid in the pleuralspace and to determine whether it can be drained by
Figure 365 An approach to the management of
parapneumonic effusions
Parapneumonic effusion
gt 1 cm thick
on lateral decubitus
film
Pleural aspirate
turbid or purulent or
Gram stain +ve
Pleural aspirate
pH
Serial thoracocentesis Treat as empyemaObserve
No
gt72 lt70
70ndash72
No
Yes
Yes
httpwwwexpertconsultcomAccess the complete references list online at
1 American Thoracic Society and Infectious Diseases Society of America Guidelines for the manage-ment of adults with hospital-acquired ventilator-associated and healthcare associated pneumonia
Am J Respir Crit Care Med 2005171388ndash416
2 Mandell LA Wunderink RG Anzueto A et al Infec-tious Diseases Society of AmericaAmerican Tho-racic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin
Infect Dis 200744S27ndash72
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1517
428 Pneumonia
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1617
References 428e1
REFERENCES 1 American Thoracic Society and Infectious Diseases
Society of America Guidelines for the management of adults with hospital-acquired ventilator-associated and healthcare associated pneumonia Am J Respir Crit Care Med 2005171388ndash416
2 Mandell LA Wunderink RG Anzueto A et al Infec-tious Diseases Society of AmericaAmerican Tho-racic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744S27ndash72
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
4 Woodhead M Blasi F Ewig S et al Guidelines for the management of adult lower respiratory tract infections Eur Respir J 2005261138ndash80
5 Torres A Rello J Update in community-acquired and nosocomial pneumonia 2009 Am J Respir Crit
Care Med 2010181782ndash76 Van der Eerden MM Vlaspolder F de Graaff CS et
al Value of intensive diagnostic microbiological investigation in low- and high-risk patients with community-acquired pneumonia Eur J Clin Micro Infect Dis 200524241ndash9
7 Murdoch DR Nucleic acid amplication tests for the diagnosis of pneumonia Clin Infect Dis 2003361162ndash70
8 Blaschke AJ Interpreting assays for the detection of Streptococcus pneumonia Clin Infect Dis 201152(S4)S331ndash7
9 Rello J Lisboa T Lujan M Severity of pneumococcal
pneumonia associated with genomic bacterial load Chest 2009136832ndash4010 Azoulay E Bergeron A Polymerase chain reaction
for diagnosing pneumocystis pneumonia in non-HIV immunocompromised patients with pulmonary inl-trates Chest 2009135(3)655
11 Garcia-Vidal C Fernandez-Sabe N Carratala J Early mortality in patients with community-acquired pneumonia causes and risk factors Eur Respir J200832733ndash9
12 Dellinger RP Carlet JM Masur H et al Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock Intensive Care Med200430536ndash55
13 Metersky ML Ma A Houck PM et al Antibiotics for bacteremic pneumonia improved outcomes with macrolides but not uoroquinolones Chest 2007131466ndash73
14 Dunbar LM Wunderink RG Habib MP High-dose short-course levooxacin for community-acquired pneumonia a new treatment paradigm Clin Infect Dis 200337752ndash60
15 Matthaiou DK Ntani G An ESICM systematic review and meta-analysis of procalcitonin-guided antibiotic therapy algorithms in adult critically ill patients Intensive Care Med 201238940ndash9
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
17 Gruber PC Gomersall CD Joynt GM Avian inu-enza (H5N1) implications for intensive care Inten-sive Care Med 200632823ndash9
18 Belongia EA Irving SA Clinical characteristics and 30-day outcomes for inuenza A 2009 (H1N1) 2008ndash2009 (H1N1) and 2007ndash8 (H3N2) infections JAMA2010304(10)1091
19 Lee N Chan PKS Complications and outcomes of pandemic 2009 inuenza A (H1N1) virus infection in hospitalized adults how do they differ from those in seasonal inuenza J Infect Dis 20112031739ndash47
20 Kim SH Hong SB Corticosteroid treatment in critically ill patients with pandemic inuenza AH1N1 2009 infection analytic strategy using pro-pensity scores Am J Respir Crit Care Med 20111831207ndash14
21 Centers for Disease Control and Prevention (CDC) Bacterial coinfections in lung tissue specimens from
fatal cases of 2009 pandemic inuenza A (H1N1) ndash United States MayndashAugust 2009 MMWR 2009581071ndash4
22 Safdar N Dezfulian C Clinical and economic conse-quences of ventilator-associated pneumonia A sys-tematic review Crit Care Med 200533(10)2184ndash93
23 Shorr AF Sherner JH Invasive approaches to the diagnosis of ventilator-associated pneumonia A meta-analysis Crit Care Med 200533(1)46ndash53
24 Melsen WG Rovers MM Ventilator-associated pneumonia and mortality A systematic review of observational studies Crit Care Med 2009372709ndash18
25 Bekaert M Timsit JF Attributable mortality of ventilator-associated pneumonia A reappraisal using causal analysis Am J Respir Crit Care Med20111841133ndash9
26 CDC Healthcare Infection Control Practices AdvisoryCommittee Guidelines for preventing health-care-associated pneumonia 2003 Recommendations ofCDC and the Healthcare Infection Control PracticesAdvisory Committee Online Available httpwwwcdcgovmmwrpreviewmmwrhtmlrr5303a1htm
27 Cofn SE Klompas M SHEAIDSA practice recom-mendation strategies to prevent ventilator-associated pneumonia in acute care hospitals Infect Control
Hosp Epidemiol 200829S31ndash4028 Masterton RG Galloway A Guidelines for the man-
agement of hospital-acquired pneumonia in the UK Report of the Working Party on Hospital-Acquired Pneumonia of the British Society for Antimicrobial Chemotherapy J Antimicrob Chemother 2008625ndash34
29 VAP Guidelines Committee and the Canadian Critical Care Trials Group Comprehensive evidence-based clinical practice guidelines for ventilator-associated pneumonia prevention J Crit Care 200823126ndash37
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1717
428e2 Pneumonia
30 Torres A Ewig S Dening treating and preventing hospital acquired pneumonia European perspective Intensive Care Med 2009359ndash29
31 Frame RN Johnson MC Eichenhorn MS et al Active tuberculosis in the medical intensive care unit a 15-year retrospective analysis Crit Care Med 1987151012ndash14
32 National Collaborating Centre for Chronic Condi-tions Tuberculosis Clinical diagnosis and manage-ment of tuberculosis and measures for its prevention and control London Royal College of Physicians 2006
33 Small PM Fujiwara PI Management of tuberculosis in the United States N Engl J Med 2001345189ndash200
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
35 Centers for Disease Control and Prevention Guide-lines for preventing the transmission of Mycobacte-rium tuberculosis in health-care settings 2005 MMWR
2005541ndash11936 Hilbert G Gruson D Vargas F et al Noninvasive
ventilation in immunosuppressed patients with pul-monary inltrates fever and acute respiratory failure N Engl J Med 2001344481ndash7
37 Benson CA Kaplan JE Masur H Treating oppor-tunistic infections among HIV-infected adults and adolescents recommendations from CDC the National Institutes of Health and the HIV Medicine AssociationInfectious Diseases Society of America Clin Infect Dis 200540S131ndash235
38 Randall CJ Yarnold PR Schwartz DN et al Improve-ments in outcomes of acute respiratory failure for
patients with human immunodeciency virus-related Pneumocystis carinii pneumonia Am J Respir Crit Care Med 2000162393ndash8
39 Croda J Croda MG Neves A et al Benet of antiret-roviral therapy on survival of human immunode-ciency virus-infected patients admitted to an intensive care unit Crit Care Med 200937(5)1605
40 Centers for Disease Control Updated guidelines for the use of rifabutin or rifampicin for the treatment and prevention of tuberculosis among HIV-infected patients taking protease inhibitors or nonnucleoside reverse transcriptase inhibitors MMWR 200049185ndash9
41 Tamm M The lung in the immunocompromised patient Infectious complications part 2 Respiration199966199ndash207
42 Van der Bij W Speich R Management of cytomega-lovirus infection and disease after solid-organ trans-plantation Clin Infect Dis 200133(Suppl 1)S32ndash7
43 Schaumlfer P Tenschert W Cremaschi L et al Area under the viraemia curve versus absolute viral load utility for predicting symptomatic cytomegalovirus infections in kidney transplant patients J Med Virol20016585ndash9
44 Meyer-Koenig U Weidmann M Kirste G et al Cytomegalovirus infection in organ-transplant recip-ients diagnostic value of pp65 antigen test qualita-tive polymerase chain reaction (PCR) and quantitative
Taqman PCR Transplantation 2004771692ndash8
45 Pappas PG Rex JH Sobel JD Guidelines for treat-ment of candidiasis Clin Infect Dis 200438161ndash89
46 Stevens DA Kan VL Judson MA Practice guidelines for diseases caused by Aspergillus Clin Infect Dis200030696ndash709
47 Herbrecht R Denning DW Patterson TF Voricona-zole versus amphotericin B for primary therapy of invasive aspergillosis N Engl J Med 2002347408ndash15
48 Peek GJ Morcos S Cooper G The pleural cavity BMJ20003201318ndash21
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6

7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 517
418 Pneumonia
should be modied in the light of risk factors (see Table 361) Quinolones may be less appropriate in areas witha high prevalence of TB as their use may mask concur-rent TB infection Appropriate antimicrobial therapyshould be administered within 1 hour of diagnosis412 There is controversy regarding the appropriate changeto empirical therapy based on microbiological nd-
ings24
Changing to narrower-spectrum antimicrobialcover may result in inadequate treatment of the 5ndash38of patients with polymicrobial infection Increasing evi-dence demonstrates improved outcome with combina-tion antimicrobial as compared with monotherapyparticularly in severely ill patients with bacteraemicpneumococcal pneumonia5 Odds ratio of death was15 to 6 for monotherapy as compared with com-bination therapy Benets were seen only in combina-tion therapy with macrolide as part of the regimen butnot in combination with uroquinolone regimen13 For the treatment of drug-resistant Strep pneumoniae (DRSP) the regimens in Figure 361 are probably suit-
able for isolates with a penicillin MIC lt 4 mgL2 Ifthe MIC is ge4 mgL an antipneumococcal uoroqui-nolone vancomycin teicoplanin or linezolid should begiven4
DURATION OF THERAPY No clinical trial has specically addressed this issueCourses as short as 5 days may be sufcient14 IDSAATS guidelines recommend stopping after a minimumof 5 days if the patient is afebrile for 48ndash72 hoursand organ dysfunction has largely resolved2 Shortcourses may be suboptimal for patients with bacterae-mic S aureus pneumonia meningitis or endocarditiscomplicating pneumonia or infection with less commonorganisms (eg Burkholderia pseudomallei or fungi) orPseudomonas aeruginosa Procalcitonin may be useful toguide antibiotic therapy but not all studies have dem-onstrated a benet15
RESPONSE TO THERAPY 2
This can be assessed subjectively (a response is usuallyseen within 1ndash3 days of starting therapy) or objectivelyon the basis of respiratory symptoms fever oxygena-tion WBC count bacteriology CXR changes C-reactiveprotein reduction and procalcitonin reduction of
80ndash90 from peak value The average time to deferves-cence varies with organism severity and patient age(7 days in elderly patients 25 days in young patientswith pneumococcal pneumonia 6ndash7 days in bacterae-mic patients with pneumococcal pneumonia 1ndash2 daysin patients with M pneumoniae pneumonia and 5 daysin patients with Legionella pneumonia) Both blood andsputum cultures are usually negative within 24ndash48hours of treatment although P aeruginosa and M pneu-moniae may persist in the sputum despite effectivetherapy CXR changes lag behind clinical changes withthe speed of change depending on the organism theage of the patient and the presence or absence of comor-
bid illnesses The CXR of most young or middle-aged
patients with bacteraemic pneumococcal pneumonia isclear by 4 weeks but resolution is slower in elderlypatients and patients with underlying illness extensivepneumonia on presentation or Legionella pneumophilia pneumonia
If the patient fails to respond consider the followingquestions
bull Has the patient got pneumonia
bull Are there host factors that explain the failure (egobstruction of bronchus by a foreign body or tumourinadequate host response)
bull Has a complication developed (eg empyema super-infection bronchiolitis obliterans organising pneu-monia metastatic abscess)
bull Is the right drug being given in an adequate dose bythe right route
bull Is the organism resistant to the drug being given
bull Are there other organisms
bull Is the fever a drug fever
Useful investigations include computerised tomogra-phy (CT) of the chest thoracocentesis bronchoalveolarlavage (Table 362) and transbronchial or open-lungbiopsy
PREDICTION OF ADVERSE OUTCOME ANDADMISSION TO ICU Scoring systems have been developed to predictadverse outcome and ICU admission including pneu-monia severity index (PSI) CURB-65 CRB-65 modiedATS major and minor criteria SCAP prediction ruleSMART-COP REA-ICU index and CAP-PIRO16
Although they may help identify the sicker patientsthey should not be used as a sole determinant of ICUadmission as local admission criteria will be affectedby local facilities both in and outside ICU It shouldbe noted that none of the criteria has been prospec-tively demonstrated to avoid late transfers or lowermortality
INFLUENZA PNEUMONIA
Inuenza pneumonia may present with severe respira-tory failure and multi-organ failure However the
pattern of organ failure appears to vary between strainswith H5N1 being associated with a much higher mor-tality and a higher incidence of multi-organ failure thanpandemic H1N117 which itself presented differently toseasonal inuenza In particular trophism for lowerrespiratory tract a higher rate of ICU admission18 anda higher rate of extrapulmonary complications19 wereobserved
Early initiation of oseltamivir is recommended forcritically ill patients although there is no direct evidenceof outcome benet Glucocorticoids do not appear tobe useful and may prolong viral replication20 Bacterialsuperinfection should be considered with Gram-
positive cocci being most frequently isolated21
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 617
Healthcare-associated pneumonia 419
failure and cancer) can cause inltrates on a chest X-rayIdentication of the organism responsible is even moredifcult than in patients with community-acquiredpneumonia owing to the high incidence of oropharyn-
geal colonisation by Gram-negative bacteria Blood cul-tures are positive in only about 6 of cases of nosocomialpneumonia Ventilator-associated pneumonia (VAP) isnosocomial pneumonia arising gt48ndash72 hours after intu-bation Reported incidence of VAP is between 10 and20 for those receiving mechanical ventilation for morethan 48 hours22 It is associated with a higher incidenceof multi-drug-resistant organisms1
PATHOGENESIS
Nosocomial pneumonia is thought to result from micro-aspiration of bacteria colonising the upper respiratory
tract Other routes of infection include macroaspiration
Although there are data demonstrating that surgicalmasks are as effective as N95 (FFP 2) masks in prevent-ing transmission of seasonal inuenza in non-ICU set-tings it is important to note that the capacity for airborne
transmission (and hence the need for N95 masks) isdependent on the exact characteristics of the organismand the frequency of aerosol-generating procedures sothese data should not be extrapolated to other inuenzaviruses and ICU settings
HEALTHCARE-ASSOCIATED PNEUMONIA
Nosocomial pneumonia occurs in 05ndash5 of hospitalpatients with a higher incidence in certain groups(eg postoperative patients and patients in ICU) Diag-nosis may be difcult the clinical features of pneumo-nia are non-specic and many non-infectious conditions
(eg atelectasis pulmonary embolus aspiration heart
Table 362 Procedure for obtaining microbiological samples using bronchoscopy and protected specimen brushingandor bronchoalveolar lavage3549
Infection control In patients suspected of having a disease that is transmitted by the airborne route (egtuberculosis)
bull the risk of transmission should be carefully weighed against the benefits ofbronchoscopy which may generate large numbers of airborne particles
bull perform bronchoscopy in a negative-pressure isolation room
bull consider the use of a muscle relaxant in ventilated patients to prevent coughingbull staff should wear personal protective equipment which should include a fit-tested
negative-pressure respirator (N95 FFP2 or above) as a minimum use of a poweredair-purifying respirator should be considered
General recommendations Suction through the endotracheal tube should be performed before bronchoscopyAvoid suction or injection through the working channel of the bronchoscopePerform protected specimen brushing before bronchoalveolar lavage
Ventilated patients Set F iO2 at 10
Set peak pressure alarm at a level that allows adequate ventilationTitrate ventilator settings against exhaled tidal volumeConsider neuromuscular blockade in addition to sedation in patients at high risk of
complications who are undergoing prolonged bronchoscopy
Protected specimen brushing (PSB) Sample the consolidated segment of lung at subsegmental levelIf purulent secretions are not seen advance the brush until it can no longer be seen but
avoid wedging it in a peripheral positionMove brush back and forth and rotate it several times
Bronchoalveolar lavage (BAL) Wedge tip of bronchoscope into a subsegment of the consolidated segment of lungInject aspirate and collect 20 mL of sterile isotonic saline Do not use this sample for
quantitative microbiology or identification of intracellular organisms It can be used forother microbiological analysis
Inject aspirate and collect additional aliquots of 20ndash60 mLThe total volume of saline injected should be 60ndash200 mL
Complications Hypoxaemia (possibly less with smaller BAL volumes)Arrhythmia
Transient worsening in pulmonary infiltratesBleeding (particularly following PSB)Fever (more common after BAL)
Positive results gt5 of cells in cytocentrifuge preparations of BAL fluid contain intracellular bacteria ORge103 colony-forming unitsmL in PSB specimen ORge104 colony-forming unitsmL in BAL fluid
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 717
420 Pneumonia
worse prognosis In 50 of patients with severehospital-acquired pneumonia and positive bloodcultures there is another source of sepsis
MANAGEMENT
Management is based on the nding that early treat-
ment with antimicrobials that cover all likely patho-gens results in a reduction in morbidity and mortality2 The initial selection of antimicrobials is made on thebasis of epidemiological clues (Fig 362 Table 363)Antimicrobials should be administered within 1 hourof diagnosis12 The results of microbiological investiga-tions are used to narrow antimicrobial cover laterTreatment should be reassessed after 2ndash3 days orsooner if the patient deteriorates (Fig 363) An outlineof management based on an invasive approach is givenin Figure 364
DURATION OF THERAPY
Current ATS guidelines recommend 7 daysrsquo treatmentprovided the aetiological agent is not P aeruginosa orother non-lactose fermenter and the patient has a goodclinical response with resolution of clinical features ofinfection1 The outcome of patients who receive appro-priate initial empirical therapy for ventilator-associatedpneumonia for 8 days is similar to those who receivetreatment for 15 days1
of gastric contents inhaled aerosols haematogenousspread spread from pleural space and direct inocula-tion from ICU personnel
CLINICAL DIAGNOSIS
Diagnosis is based on time of onset (gt48 hours afteradmission to a healthcare facility1) CXR changes (newor progressive inltrates) and either clinical featuresand simple laboratory investigations or the results ofquantitative microbiology Using a clinical approachpneumonia is diagnosed by the nding of a new inl-trate or a change in an inltrate on chest radiographand growth of pathogenic organisms from sputum plusone of the following white-blood-cell (WBC) countgreater than 12times l05L core temperature ge383degCsputum Gram stain with scores of more than two on ascale of four of polymorphonuclear leucocytes andbacteria
INVESTIGATIONSThese are broadly similar to those required incommunity-acquired pneumonia
bull Chest X-ray although studies using a histologicaldiagnosis as the gold standard have demonstratedthat pneumonia may be present despite a normalCXR most denitions of nosocomial pneumoniarequire the presence of new persistent inltrates ona CXR
bull Respiratory secretions considerable controversy sur-rounds the issue of whether invasive bronchoscopicsampling (Table 362) of respiratory secretions is nec-
essary Whether invasive sampling is employed ortracheal aspirates are used empirical broad-spectrumantibiotics should be started while results areawaited The results of microbiological analysis ofrespiratory secretions are used to either stop antibi-otics or narrow the spectrum1 Although the use ofan invasive strategy is associated with a higher like-lihood of modication of initial antimicrobials23 theeffect on important clinical outcome such as mortal-ity antibiotic-free days and organ dysfunction isvariable1 Although tracheal aspirates may predomi-nantly reect the organisms colonising the upper
airway they may be useful in indicating whichorganisms are not responsible for the pneumoniathus allowing the antimicrobial cover to be nar-rowed1 This interpretation is based on the premisethat the predominant route of infection is via theupper respiratory tract From this it can be assumedthat if the organism is not present in the upper res-piratory tract the probability of it being present inthe lung parenchyma is low Certain organisms arevirtually always pathogens when recovered fromrespiratory secretions (see Box 361)
bull Blood cultures identify the aetiological agent in8ndash20 of patients Bacteraemia is associated with a
Figure 362 An outline of initial management ofnosocomial pneumonia based on a non-invasive clinicalapproach1
Two ofuarr or darr WCC
purulent sputum
temp gt38degC
New CXR
infiltrates
Consider acute
tracheobronchitis
Obtain lower respiratory
tract specimens and blood for
microbiological investigations
Risk factorsfor multidrug-resistant
pathogens
Early broad-spectrum
antibiotic therapy
to cover multidrug-
resistant pathogens
Early limited-spectrum
antibiotic therapy
Yes
Yes
No
No
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 817
Healthcare-associated pneumonia 421
inltrate in 48 hours new cavitation or a signicantnew pleural effusion should raise concern If the patientfails to respond consider the diagnosis host factors (egimmunosuppressed debilitated) bacterial factors (egvirulent organism) and therapeutic factors (eg wrongdrug inadequate dose) Review the antibiotics andrepeat cultures It may be useful to broaden the antimi-crobial cover while waiting for the results of investiga-tions Consider invasive sampling of respiratorysecretions computerised tomography or ultrasound ofthe chest (to look for an empyema or abscess) anothersource of infection open-lung biopsy to establish diag-nosis and aetiology or administration of steroids
MORTALITY AND MORBIDITY ATTRIBUTABLE TO VAP Substantial morbidity and mortality associated withVAP have previously been reported22 However acausal relationship is difcult to establish It should benoted that patients who developed VAP tend to be
more severely ill and at higher risk of death not onlyon ICU admission but throughout the course of theirillness Most of the relevant studies were observationaland failed to adequately control confounders likedisease severity evolution of disease progression andICU length of stay with mortality In addition signi-cant heterogeneity exists among these studies Althoughthe presence of VAP is associated with a signicantlylonger ICU length of stay (mean of 61 days 95 CI532ndash687) and increased healthcare cost22 more recentstudies reported that mortality attributable to VAPtends to be small if any2425 The attributable mortalityhas been reported to be 1 on the 30th day of ICU and
RESPONSE TO THERAPY Clinical improvement is usually not apparent for 48ndash72hours and therapy should not be changed during thistime The CXR is of limited value for assessing responseinitial deterioration is common and improvement oftenlags behind clinical response However a rapidly dete-riorating CXR pattern with a gt50 increase in size of
Figure 363 Subsequent management of nosocomialpneumonia based on a non-invasive clinical approach1
Pathogens isolated
from respiratory
specimen
Antibiotics
changedstarted in 7 h
prior to sampling
Adjust antibiotics
according to sensitivities
Continue antibiotics if
high clinical suspicion of
nosocomial pneumonia
Bacterial pneumonia
unlikely
Investigate for other cause
of sepsis and CXR changes
Consider unusual causes
of nosocomial pneumonia
(eg Legionella viruses fungi
Pneumocystis carinii )
Yes
Yes
No
No
Table 363 Recommended initial empirical treatment for nosocomial pneumonia1
SITUATION ANTIBIOTICS
No risk factors for multidrug-resistant pathogens Ceftriaxone or Levofloxacin moxifloxacin or ciprofloxacin or Ampicillinsulbactam or Ertapenem
Antimicrobial therapy in previous 90 days or Current hospitalization for ge5 days or High frequency of antibiotic resistance in the specific
hospital unit or Hospitalisation for 2 days or more in previous 90 days or Residence in nursing home or extended care facility or Home infusion therapy (including antibiotics) or Chronic dialysis within 30 days or Home wound care or Family member with multidrug-resistant pathogen o rImmunosuppression or Bronchiectasis
One ofAntipseudomonal cephalosporin (cefepime or ceftazidime) or Antipseudomonal carbapenem (meropenem or imipenemndash
cilastin) or szlig-lactamszlig-lactamase inhibitor (eg piperacillinndashtazobactam or
cefaperazonendashsulbactam)plus one ofAminoglycoside or Antipseudomonal quinolone (levofloxacin or ciprofloxacin)plus one of the following for patients at high risk of meticillin-
resistant Staphylococcus aureus (MRSA) infectionLinezolid or Vancomycin or
TeicoplaninThe use of dual therapy is not well supported by evidence but it does reduce the probability that the pathogen is resistant to the drugsbeing given If an extended spectrum β-lactamase-producing strain or an Acinetobacter sp is suspected a carbapenem should be givenIf Legionella pneumophilia is suspected use a quinolone Risk factors for MRSA infection in areas with a high incidence of MRSA includediabetes mellitus head trauma coma and renal failure
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 917
422 Pneumonia
or with enlarged cervical nodes or other manifestationsof extrapulmonary disease Clinical disease is seldomfound in asymptomatic individuals even those withstrongly positive tuberculin test (Heaf grade III or IV)The outlook for patients with tuberculosis who requireICU admission is poor In one retrospective study thein-hospital mortality for all patients with tuberculosisrequiring ICU admission was 67 but in those withacute respiratory failure it rose to 8131 The presenta-tion and management of TB in HIV-positive patientsare different (see below)
INVESTIGATION OF PULMONARYTUBERCULOSIS
IDENTIFICATION OF MYCOBACTERIA
Multiple
3233
sputum samples should be collected pref-erably on different days for microscopy for acid-fastbacilli and culture If sputum is not available bronchialwashings taken at bronchoscopy and gastric lavage oraspirate samples should be obtained Gastric aspiratesneed to be neutralised immediately on collection Bron-choscopy and transbronchial biopsy may be useful inpatients with suspected TB but negative sputum smearPleural biopsy is often helpful and mediastinoscopyis occasionally needed in patients with mediastinallymphadenopathy Part of any biopsy specimen shouldalways be sent for culture Nucleic acid amplicationtests on sputum have sensitivity similar to culture in
15 on the 60th day of ICU in a recent study using amulticentre high-quality database and incorporatingnovel statistical methodology to control evolution ofseverity of illness25
PREVENTION
Several guidelines for prevention of ventilator-associated pneumonia and hospital-acquired pneumo-nia have been published26ndash30 Interventions can bedivided into general infection control measures andspecic measures General measures include alcohol-based hand disinfection hospital education programmeon infection control the use of microbiological sur-veillance and a programme to reduce antibiotic pre-scription The major specic recommendations aresummarised in Table 364 There is no evidence that
lsquobundlesrsquo of recommendations are more effective thanthe sum of the individual components
TUBERCULOSIS
The main risk factors are listed in Box 362 Typicalclinical features include fever sweating weight losslassitude anorexia cough productive of mucoid orpurulent sputum haemoptysis chest wall pain dysp-noea localised wheeze and apical crackles Patientsmay also present with unresolved pneumonia pleuraleffusions spontaneous pneumothorax and hoarseness
Figure 364 Management of suspected nosocomial pneumonia based on invasive sampling of respiratory secretions
Bacteria onGram stain
Yes
Yes
No
Yes No Yes No
No
Start antibiotics immediatelyusing PSBBAL specimen
and Gram stain results
Start antibioticsimmediately based onepidemiological clues
Observe look forother infection
Signs ofsevere sepsis
Immediate PSB or BAL beforechangingstarting antimicrobial therapy
+ve cultures +ve cultures
Adjust therapybased on
culture results
Continueadjustantibiotics Look for
other infection
Start antibioticson basisof results
Look forother infection
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1017
Tuberculosis 423
Table 364 Strategies for prevention of ventilator-associated pneumonia
LEVELS OF
RECOMMENDATIONS SPECIFIC INTERVENTIONS REMARKS
Universally recommendedby all guidelines27ndash30
1 Semirecumbent position to 45deg At least 30ndash45deg2 Avoidance of endotracheal intubation3 Preference of oral tracheal route
4 New circuit for a new patient and noschedule change unless soiled or damaged5 Avoidance of flushing of condensate into
lower airway or in-line medication6 HME changes no more frequently than 5ndash7
days7 Continuous aspiration of subglottic suctioning For patients expected to require mechanical
ventilation for gt72 hours
Generally recommendedby most guidelines
1 Preferential use of non-invasiveventilation272830
2 Avoidance of unplanned re-intubation272830
3 Maintenance of endotracheal cuff pressureof about 20 mmHg (266 kPa)272830
4 Closed suctioning2829
No effect on VAP mainly for staff safety5 Chlorhexidine oral decontamination272930
6 Sedation vacation and weaning protocol2728
7 Judicious use of stress ulcer prophylaxis272830
8 Restrictive blood transfusion28
Benefits less clear 1 Preference of HME over heatedhumidifier2830
HME associated with reduction in VAP inpatients ventilated for gt7 days lower cost
2 Silver-sulfadiazine-coated endotrachealtube272830
3 Early tracheostomy (within 7 days ofmechanical ventilation)29
4 Selective decontamination of digestive tract(SDD)272830
Mortality reduction demonstrated when topicalantimicrobials combined with short-course
systemic antibiotics BSAC recommendedSDD in patients expected to requiremechanical ventilation for gt48 hours ETFdiscourage routine use due to concern ofemergence of resistant organisms
Not yet reviewed byguidelines50
1 High-volume low-pressure ultrathin membraneendotracheal tube cuff with SSD
2 Ultrathin membrane cuff with tapered shapeand SSD
3 Low-volume low-pressure endotracheal tubecuff with SSD
4 Balloon device for biofilm removal5 Saline instillation before tracheal suctioning
HME= heat moist exchanger SSD= subglottic secretion drainage
smear-negative patients with pulmonary tuberculosisbut have the advantage of a much more rapid resultThere is however a signicant false-negative rate32
CHEST X-RAY (CXR)A normal CXR almost excludes TB (except inHIV-infected patients) but endobronchial lesionsmay not be apparent and early apical lesions can bemissed Common appearances include patchynodular
shadowing in the upper zones (often bilateral) cavita-tion calcication hilar or mediastinal lymphadenopa-thy (may cause segmental or lobar collapse) pleuraleffusion tuberculomas (dense round or oval shadows)and diffuse ne nodular shadowing throughout thelung elds in miliary TB Inactivity of disease cannot beinferred from the CXR alone This requires three nega-tive sputum samples and failure of any lesion seen onCXR to progress CXR appearances in HIV-positive
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1117
424 Pneumonia
t-tested negative-pressure respirator (N95 FFP2 orhigher) Use of a powered air-purifying respiratorshould be considered when bronchoscopy is being per-formed35 Detailed infection control advice can beobtained via the lsquolink pagersquo (httpwwwaiccuhk eduhkweb8Pneumonia20guidelineshtm)
PNEUMONIA IN THEIMMUNOCOMPROMISED
The lungs are amongst the most frequent targetorgans for infectious complications in the immuno-compromised The incidence of pneumonia is highestamongst patients with haematological malignanciesbone marrow transplant (BMT) recipients and patientswith AIDS
The speed of progression of pneumonia the CXRchanges (Table 365) and the type of immune defectprovide clues to the aetiology Bacterial pneumonias
progress rapidly (1ndash2 days) whereas fungal and proto-zoal pneumonias are less fulminant (several days to aweek or more) Viral pneumonias are usually not ful-minant but on occasions may develop quite rapidlyBronchoscopy is a major component of the investiga-tion of these patients Empirical management based onCXR appearances is outlined in Table 365 Early non-invasive ventilation may improve outcome amongstimmunocompromised patients with fever and bilateralinltrates36
PNEUMOCYSTIS JIROVECI PNEUMONIA (PCP)37
The incidence of this common opportunistic infectionhas fallen substantially in patients with AIDS whoare receiving prophylaxis and effective antiretroviraltherapy with most cases occurring in patients who arenot receiving HIV care or among patients with advancedimmunosuppression The onset is usually insidiouswith dry cough dyspnoea and fever on a backgroundof fatigue and weight loss Crackles in the chest are rareApproximately 15 of patients have a concurrent causefor respiratory failure (eg Kaposi sarcoma TB bacte-rial pneumonia) Useful investigations are
1 CXR classical appearance is diffuse bilateral perihi-
lar interstitial shadowing but in the early stages thisis very subtle and easily missed The initial CXR isnormal in 10 In a further 10 the changes areatypical with focal consolidation or coarse patchyshadowing None of the changes are specic for PCPand may be seen in other lung diseases associatedwith AIDS Pleural effusions hilar or mediastinallymphadenopathy are unusual in PCP but commonin mycobacterial infection or Kaposirsquos sarcoma orlymphoma
2 Induced sputum in this technique the patient inhalesnebulised hypertonic saline from an ultrasonic neb-uliser This provokes bronchorrhoea and the patient
patients with TB differ from those in non-HIV-infectedpatients
TREATMENT OF PULMONARY TB32ndash34
The decision to initiate anti-TB treatment should bebased on level of clinical suspicion results of AFBsmear and sometimes mycobacterial culture If the
initial clinical suspicion is strong and the patient is seri-ously ill attributable to possible TB treatment shouldbe initiated promptly sometimes before the result ofAFB smear Subsequent positivity of AFB smear ornucleic acid amplication test provides support to thecontinuation of treatment Combination chemotherapyconsisting of four drugs is necessary for maximal ef-cacy Treatment is divided into initial phase and con-tinuation phase The most commonly used initialregimen consists of 8 weeks of rifampicin 600 mg daily(450 mg for patients lt50 kg) isoniazid 300 mg dailypyrazinamide 2 g daily (15 g for patients lt50 kg) and
ethambutol 15 mgkg daily as initial phase treatmentEthambutol should be used only in patients who havereasonable visual acuity and who are able to appreciateand report visual disturbances This mandates carefulconsideration in patients who require heavy sedationVisual acuity and colour perception must be assessed(if ethambutol is to be used) and liver and renal func-tion checked before treatment is started Steroids arerecommended for children with endobronchial diseaseand possibly for patients with tuberculous pleuraleffusions Pyridoxine 10 mg daily should be given toprevent isoniazid-induced neuropathy to those atincreased risk (eg patients with diabetes mellitus
chronic renal failure or malnutrition or alcoholic orHIV-positive patients) Negative AFB smear should notdelay initial treatment if clinical suspicion remainshigh Supporting features included chronic coughweight loss characteristic chest X-ray ndings emigra-tion from a high-incidence country no other immediatediagnosis and positive tuberculin test
INFECTION CONTROL
Patients admitted to an ICU with infectious TB or sus-pected of having active pulmonary TB should bemanaged in an isolation room with special ventilation
characteristics including negative pressure Patientsshould be considered infectious if they are coughing orundergoing cough-inducing procedures or if they havepositive AFB smears and they are not on or have juststarted chemotherapy or have a poor clinical or bacte-riological response to chemotherapy3235 Patients withnon-drug-resistant TB should be non-infectious after 2weeks of treatment which includes rifampicin and iso-niazid32 As TB spreads through aerosols it is probablyappropriate to isolate patients who are intubated evenif only their bronchial washings are smear-positiveStaff caring for patients who are smear-positive shouldwear personal protective equipment including a
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1217
Pneumonia in the immunocompromised 425
andor diuretics (patients often uid-overloaded)Approximately 40 of patients with HIV-related PCPwho require mechanical ventilation survive to hospitaldischarge38
Initiation of antiretroviral therapy in patients pre-senting with HIV-related PCP is controversial TheCenters for Disease Control and Prevention (CDC) rec-ommend against doing so in the acute phase but recent
data suggest that the outcome may be improved byinitiation within the rst 4 days of ICU admission39
BACTERIAL PNEUMONIA37
This is the most common cause of acute respiratoryfailure in HIV-positive patients Bacterial pneumonia ismore common in HIV-infected patients than in thegeneral population and tends to be more severe Strep pneumoniae H infuenza Pseudomonas aeruginosa and Saureus are the commonest organisms Nocardia andGram negatives should also be considered Atypicalpathogens (eg Legionella) are rare Response to appro-
priate antibiotics is usually good but may require pro-tracted courses of antibiotics because of high tendencyto relapse Patients with severe immunodeciency(CD4+ T lymphocyte count lt100983221L) and a history ofPseudomonas infection or bronchiectasis or neutropeniashould receive antibiotics that cover P aeruginosa aswell as other Gram negatives The possibility of concur-rent PCP or tuberculosis should be excluded
TUBERCULOSIS
TB may be the initial presentation of AIDS particularlyin sub-Saharan Africa The pattern of TB in HIV patients
coughs up material containing cysts and tropho-zoites The technique is time-consuming and requiresmeticulous technique and is less sensitive thanbronchoscopy but less invasive The possibility ofconcurrent tuberculosis should be consideredand steps taken to minimise the risk of spread ofinfection
3 Bronchoscopy with bronchoalveolar lavage leads to
the diagnosis in over 90 of cases Specimens shouldbe sent for cytology Transbronchial biopsy is notnecessary in most cases PCR using bronchial lavagespecimens may be useful in non-HIV patients withsuspected PCP
Antipneumocystis treatment should be started as soonas the diagnosis is suspected Treatment of choice istrimethoprim plus sulfamethoxazole (co-trimoxazole)20 mgkgday+ 100 mgkgday for 3 weeks plusprednisolone 40 mg orally twice daily for 5 days fol-lowed by 20 mg twice daily for 5 days and then 20 mgper day until the end of PCP treatment Side-effects of
co-trimoxazole are common in HIV patients (nauseavomiting skin rash myelotoxicity) The dose should bereduced by 25 if the WBC count falls Patients whoare intolerant of co-trimoxazole should be treated with
bull pentamidine 4 mgkgday iv or
bull primaquine with clindamycin or
bull trimetrexate with leucovorin (plusmnoral dapsone)
Response to treatment is usually excellent with aresponse time of 4ndash7 days If the patient deteriorates orfails to improve consider (re-)bronchoscopy (is thediagnosis correct) treat co-pathogens and considera short course of high-dose iv methylprednisolone
Table 365 Causes of CXR changes and empirical treatment of pneumonia in the immunocompromised
CHEST X-RAY
APPEARANCE CAUSES
EMPIRICAL TREATMENT FOR
SUSPECTED PNEUMONIA
Diffuse infiltrate CMV and other herpes virusesPneumocystis carinii Bacteria
Aspergillus (advanced)Cryptococcus (uncommon)Non-infectious causes eg drug reaction non-specific
interstitial pneumonitis radiation pneumonitis(uncommon) malignancy leucoagglutinin reaction
Broad-spectrum antibiotics for at least 48 h(eg 3rd-generation cephalosporin andaminoglycoside)
Co-trimoxazoleLung biopsy or lavage within 48 h or full2-week course of co-trimoxazole (dependson patient tolerance of invasive procedure)
Focal infiltrate Gram-negative rodsS aureusAspergillusCryptococcusNocardiaMucorP carinii (uncommon)Tuberculosis
LegionellaNon-infectious causes (eg malignancy non-specificinterstitial pneumonitis radiation pneumonitis)
Broad-spectrum antibioticsIf response seen continue treatment for
2 weeksIf disease progresses lung biopsyaspirate
within 48ndash72 hours or empirical trial ofantifungalplusmn macrolide
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1317
426 Pneumonia
reaction are the most useful tests for demonstratingCMV disease Using thresholds of 10300 000ndash50200 000 positive circulating peripheral WBC the posi-tive predictive value for CMV-pp65 ranges from64 to 82 and the negative predictive value from70 to 954344 Treatment consists of intravenous gan-ciclovir for at least 14 days Foscarnet can be used if
ganciclovir fails
FUNGAL PNEUMONIA
Fungi are rare but important causes of pneumoniaThey can be divided into two main groups based on theimmune response required to combat infection withthese organisms Histoplasma blastomycosis coccidi-oidomycosis paracoccidioidomycosis and Cryptococcus require specic cell-mediated immunity for their controland thus in contrast to infections that are controlled byphagocytic activity the diseases caused by these organ-isms can occur in otherwise healthy individuals
although they cause much more severe illness inpatients with impaired cell-mediated immunity (egpatients infected with HIV and organ transplant recipi-ents) With the exception of Cryptococcus these organ-isms are rarely seen outside North America Aspergillus and Mucor spores are killed by non-immune phago-cytes and as a result these fungi rarely result in clinicalillness in patients with normal neutrophil numbers andfunction
CANDIDIASIS This is effectively a combination of the two types offungal infection in which impaired cell-mediatedimmunity predisposes to mucosal overgrowth withCandida but impaired phagocytic function or numbersis usually required before deep invasion of tissuesoccurs Primary Candida pneumonia (ie isolated lunginfection) is uncommon4145 and more commonly pul-monary lesions are only one manifestation of dissemi-nated candidiasis Even more common is benigncolonisation of the airway with Candida In mostreported cases of primary Candida pneumonia ampho-tericin B has been used In disseminated candidiasistreatment should be directed to treatment of dissemi-nated disease rather than Candida pneumonia per se45
INVASIVE ASPERGILLOSIS 46
This is a highly lethal condition in the immunocom-promised despite treatment and therefore investiga-tion and treatment should be prompt and aggressiveIt is associated with exposure to construction workDenitive diagnosis requires both histological evidenceof acute-angle branching septated non-pigmentedhyphae measuring 2ndash4 983221m in width and cultures yield-ing Aspergillus species from biopsy specimens ofinvolved organs Recovery of Aspergillus species fromrespiratory secretions in immunocompromised butnot immunocompetent patients may indicate invasive
disease with a positive predictive value as high as
depends on the degree of immunosuppression Inpatients with CD4+ T lymphocytes gt350 cells983221L theclinical presentation is similar to TB in non-HIV-infectedpatients although extrapulmonary disease is morecommon In patients with CD4+ T lymphocytes lt350cells983221L extrapulmonary disease (pleuritis pericardi-tis meningitis) is common Severely immunocompro-
mised patients (CD4+
T lymphocytes lt100 cells983221L)may present with severe systemic disease with highfever rapid progression and systemic sepsis In thesepatients lower and middle lobe disease is more commonmiliary disease is common and cavitation is lesscommon Sputum smears and culture may be positiveeven with a normal CXR
Response to treatment is usually rapid Managementof TB in HIV is complex owing to numerous druginteractions consultation with an expert in treatment ofHIV-related TB should be strongly considered Complexinteractions occur between rifamycins (eg rifampicinand rifabutin) and protease inhibitors and non-
nucleoside reverse transcriptase inhibitors used to treatpatients infected with HIV The choice of rifampicin orrifabutin depends on a number of factors includingthe unique and synergistic adverse effects for each indi-vidual combination of rifampicin and anti-HIV drugsand consultation with a physician with experiencein treating both TB and HIV is advised40 IDSA-recommended dosage adjustment for patients receivingantiretrovirals and rifabutin37 can be obtained viathe lsquolink pagersquo (httpwwwaiccuhkeduhkweb8Pneumonia20guidelineshtm) The optimal time forinitiating antiretroviral therapy in patients with TB iscontroversial Early therapy may decrease HIV disease
progression but may be associated with a high inci-dence of adverse effects and an immune reconstitutionreaction37
CMV PNEUMONITIS4142
Risk of infection is highest following allogeneic stemcell transplantation followed by lung transplantationpancreas transplantation and then liver heart and renaltransplantation and advanced AIDS If both the recipi-ent and the donor are seronegative then the risk of bothinfection and disease are negligible If the recipient is
seropositive the risk of infection is approximately 70but the risk of disease is only 20 regardless of theserostatus of the donor However if the recipient isseronegative and the donor is seropositive the risk ofdisease is 70 If steroid pulses and antilymphocyteglobulin are given for treatment of acute rejection therisk of developing disease is markedly increased Infec-tion may be the result of primary infection or reactiva-tion of latent infection It is clinically important butoften difcult to distinguish between CMV infectionand CMV disease and a denitive diagnosis can bemade only histologically Detection of CMV-pp65antigen in peripheral WBC and detection of CMV DNA
or RNA in the blood by quantitative polymerase chain
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1417
Parapneumonic effusion 427
needle aspiration or if there is debris within the uiddrainage using an intercostal drain The diagnosis isconrmed by aspiration of pus
TREATMENT The mainstay of treatment is drainage either by inter-costal drain or by surgical intervention Patients whopresent before the pus is loculated and a brinous peelhas formed on the lung can usually be treated bysimple drainage The combination with intrapleuralbrinolysis may be benecial Optimal surgical man-agement which consists of decortication (open or tho-racoscopic) is indicated if the empyema is moreadvanced or if simple drainage fails This is a majorprocedure and many patients with cardiac or chronicrespiratory disease will not tolerate it Alternatives forthese patients are instillation of thrombolytics into thepleural space or thoracostomy Antibiotics have onlyan adjunctive role Broad-spectrum antibiotic regimenswith anaerobic cover should be used until the resultsof microbiological analysis of the aspirated pus areavailable
AcknowledgementsAll tables and gures are reproduced from ICU web(wwwaiccuhkeduhkweb8) with permission of theauthors
80ndash90 in patients with leukaemia or bone marrowtransplant recipients Bronchoalveolar lavage withsmear culture and antigen detection has excellent spe-cicity and reasonably good positive predictive valuefor invasive aspergillosis in immunocompromisedpatients Although radiological features may give a clueto the diagnosis they are not sufciently specic to be
diagnosticIn acutely ill immunocompromised patients intrave-nous therapy should be initiated if there is suggestiveevidence of invasive aspergillosis while further investi-gations to conrm or refute the diagnosis are carriedout First-line therapy is voriconazole47 Echinocandinsand amphotericin are alternatives
PARAPNEUMONIC EFFUSION
This may be an uncomplicated effusion that resolveswith appropriate treatment of the underlying pneumo-nia or a complicated effusion that develops into an
empyema unless drained Complicated effusions tendto develop 7ndash14 days after initial uid formation Theyare characterised by increasing pleural uid volumecontinued fever and pleural uid of low pH (lt73) thatcontains a large number of neutrophils and may revealorganisms on Gram staining or culture An outline ofmanagement is given in Figure 365
EMPYEMA48
DEFINITION Collection of pus in the pleural space
AETIOLOGY Follows infection of the structures surrounding thepleural space including subdiaphragmatic structuresand chest trauma or may be associated with malig-nancy Anaerobic bacteria usually streptococci orGram-negative rods are responsible for 76 of cases
DIAGNOSIS The diagnosis is usually simple The patient is usuallyseptic and may have a productive cough and chest painThe chest X-ray may show features suggestive of apleural effusion and underlying consolidation but may
also show an abscess cavity with a uid level in whichcase CT scanning will be required to distinguishbetween an abscess and an empyema Ultrasound canbe useful to conrm the presence of uid in the pleuralspace and to determine whether it can be drained by
Figure 365 An approach to the management of
parapneumonic effusions
Parapneumonic effusion
gt 1 cm thick
on lateral decubitus
film
Pleural aspirate
turbid or purulent or
Gram stain +ve
Pleural aspirate
pH
Serial thoracocentesis Treat as empyemaObserve
No
gt72 lt70
70ndash72
No
Yes
Yes
httpwwwexpertconsultcomAccess the complete references list online at
1 American Thoracic Society and Infectious Diseases Society of America Guidelines for the manage-ment of adults with hospital-acquired ventilator-associated and healthcare associated pneumonia
Am J Respir Crit Care Med 2005171388ndash416
2 Mandell LA Wunderink RG Anzueto A et al Infec-tious Diseases Society of AmericaAmerican Tho-racic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin
Infect Dis 200744S27ndash72
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1517
428 Pneumonia
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1617
References 428e1
REFERENCES 1 American Thoracic Society and Infectious Diseases
Society of America Guidelines for the management of adults with hospital-acquired ventilator-associated and healthcare associated pneumonia Am J Respir Crit Care Med 2005171388ndash416
2 Mandell LA Wunderink RG Anzueto A et al Infec-tious Diseases Society of AmericaAmerican Tho-racic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744S27ndash72
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
4 Woodhead M Blasi F Ewig S et al Guidelines for the management of adult lower respiratory tract infections Eur Respir J 2005261138ndash80
5 Torres A Rello J Update in community-acquired and nosocomial pneumonia 2009 Am J Respir Crit
Care Med 2010181782ndash76 Van der Eerden MM Vlaspolder F de Graaff CS et
al Value of intensive diagnostic microbiological investigation in low- and high-risk patients with community-acquired pneumonia Eur J Clin Micro Infect Dis 200524241ndash9
7 Murdoch DR Nucleic acid amplication tests for the diagnosis of pneumonia Clin Infect Dis 2003361162ndash70
8 Blaschke AJ Interpreting assays for the detection of Streptococcus pneumonia Clin Infect Dis 201152(S4)S331ndash7
9 Rello J Lisboa T Lujan M Severity of pneumococcal
pneumonia associated with genomic bacterial load Chest 2009136832ndash4010 Azoulay E Bergeron A Polymerase chain reaction
for diagnosing pneumocystis pneumonia in non-HIV immunocompromised patients with pulmonary inl-trates Chest 2009135(3)655
11 Garcia-Vidal C Fernandez-Sabe N Carratala J Early mortality in patients with community-acquired pneumonia causes and risk factors Eur Respir J200832733ndash9
12 Dellinger RP Carlet JM Masur H et al Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock Intensive Care Med200430536ndash55
13 Metersky ML Ma A Houck PM et al Antibiotics for bacteremic pneumonia improved outcomes with macrolides but not uoroquinolones Chest 2007131466ndash73
14 Dunbar LM Wunderink RG Habib MP High-dose short-course levooxacin for community-acquired pneumonia a new treatment paradigm Clin Infect Dis 200337752ndash60
15 Matthaiou DK Ntani G An ESICM systematic review and meta-analysis of procalcitonin-guided antibiotic therapy algorithms in adult critically ill patients Intensive Care Med 201238940ndash9
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
17 Gruber PC Gomersall CD Joynt GM Avian inu-enza (H5N1) implications for intensive care Inten-sive Care Med 200632823ndash9
18 Belongia EA Irving SA Clinical characteristics and 30-day outcomes for inuenza A 2009 (H1N1) 2008ndash2009 (H1N1) and 2007ndash8 (H3N2) infections JAMA2010304(10)1091
19 Lee N Chan PKS Complications and outcomes of pandemic 2009 inuenza A (H1N1) virus infection in hospitalized adults how do they differ from those in seasonal inuenza J Infect Dis 20112031739ndash47
20 Kim SH Hong SB Corticosteroid treatment in critically ill patients with pandemic inuenza AH1N1 2009 infection analytic strategy using pro-pensity scores Am J Respir Crit Care Med 20111831207ndash14
21 Centers for Disease Control and Prevention (CDC) Bacterial coinfections in lung tissue specimens from
fatal cases of 2009 pandemic inuenza A (H1N1) ndash United States MayndashAugust 2009 MMWR 2009581071ndash4
22 Safdar N Dezfulian C Clinical and economic conse-quences of ventilator-associated pneumonia A sys-tematic review Crit Care Med 200533(10)2184ndash93
23 Shorr AF Sherner JH Invasive approaches to the diagnosis of ventilator-associated pneumonia A meta-analysis Crit Care Med 200533(1)46ndash53
24 Melsen WG Rovers MM Ventilator-associated pneumonia and mortality A systematic review of observational studies Crit Care Med 2009372709ndash18
25 Bekaert M Timsit JF Attributable mortality of ventilator-associated pneumonia A reappraisal using causal analysis Am J Respir Crit Care Med20111841133ndash9
26 CDC Healthcare Infection Control Practices AdvisoryCommittee Guidelines for preventing health-care-associated pneumonia 2003 Recommendations ofCDC and the Healthcare Infection Control PracticesAdvisory Committee Online Available httpwwwcdcgovmmwrpreviewmmwrhtmlrr5303a1htm
27 Cofn SE Klompas M SHEAIDSA practice recom-mendation strategies to prevent ventilator-associated pneumonia in acute care hospitals Infect Control
Hosp Epidemiol 200829S31ndash4028 Masterton RG Galloway A Guidelines for the man-
agement of hospital-acquired pneumonia in the UK Report of the Working Party on Hospital-Acquired Pneumonia of the British Society for Antimicrobial Chemotherapy J Antimicrob Chemother 2008625ndash34
29 VAP Guidelines Committee and the Canadian Critical Care Trials Group Comprehensive evidence-based clinical practice guidelines for ventilator-associated pneumonia prevention J Crit Care 200823126ndash37
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1717
428e2 Pneumonia
30 Torres A Ewig S Dening treating and preventing hospital acquired pneumonia European perspective Intensive Care Med 2009359ndash29
31 Frame RN Johnson MC Eichenhorn MS et al Active tuberculosis in the medical intensive care unit a 15-year retrospective analysis Crit Care Med 1987151012ndash14
32 National Collaborating Centre for Chronic Condi-tions Tuberculosis Clinical diagnosis and manage-ment of tuberculosis and measures for its prevention and control London Royal College of Physicians 2006
33 Small PM Fujiwara PI Management of tuberculosis in the United States N Engl J Med 2001345189ndash200
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
35 Centers for Disease Control and Prevention Guide-lines for preventing the transmission of Mycobacte-rium tuberculosis in health-care settings 2005 MMWR
2005541ndash11936 Hilbert G Gruson D Vargas F et al Noninvasive
ventilation in immunosuppressed patients with pul-monary inltrates fever and acute respiratory failure N Engl J Med 2001344481ndash7
37 Benson CA Kaplan JE Masur H Treating oppor-tunistic infections among HIV-infected adults and adolescents recommendations from CDC the National Institutes of Health and the HIV Medicine AssociationInfectious Diseases Society of America Clin Infect Dis 200540S131ndash235
38 Randall CJ Yarnold PR Schwartz DN et al Improve-ments in outcomes of acute respiratory failure for
patients with human immunodeciency virus-related Pneumocystis carinii pneumonia Am J Respir Crit Care Med 2000162393ndash8
39 Croda J Croda MG Neves A et al Benet of antiret-roviral therapy on survival of human immunode-ciency virus-infected patients admitted to an intensive care unit Crit Care Med 200937(5)1605
40 Centers for Disease Control Updated guidelines for the use of rifabutin or rifampicin for the treatment and prevention of tuberculosis among HIV-infected patients taking protease inhibitors or nonnucleoside reverse transcriptase inhibitors MMWR 200049185ndash9
41 Tamm M The lung in the immunocompromised patient Infectious complications part 2 Respiration199966199ndash207
42 Van der Bij W Speich R Management of cytomega-lovirus infection and disease after solid-organ trans-plantation Clin Infect Dis 200133(Suppl 1)S32ndash7
43 Schaumlfer P Tenschert W Cremaschi L et al Area under the viraemia curve versus absolute viral load utility for predicting symptomatic cytomegalovirus infections in kidney transplant patients J Med Virol20016585ndash9
44 Meyer-Koenig U Weidmann M Kirste G et al Cytomegalovirus infection in organ-transplant recip-ients diagnostic value of pp65 antigen test qualita-tive polymerase chain reaction (PCR) and quantitative
Taqman PCR Transplantation 2004771692ndash8
45 Pappas PG Rex JH Sobel JD Guidelines for treat-ment of candidiasis Clin Infect Dis 200438161ndash89
46 Stevens DA Kan VL Judson MA Practice guidelines for diseases caused by Aspergillus Clin Infect Dis200030696ndash709
47 Herbrecht R Denning DW Patterson TF Voricona-zole versus amphotericin B for primary therapy of invasive aspergillosis N Engl J Med 2002347408ndash15
48 Peek GJ Morcos S Cooper G The pleural cavity BMJ20003201318ndash21
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6

7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 617
Healthcare-associated pneumonia 419
failure and cancer) can cause inltrates on a chest X-rayIdentication of the organism responsible is even moredifcult than in patients with community-acquiredpneumonia owing to the high incidence of oropharyn-
geal colonisation by Gram-negative bacteria Blood cul-tures are positive in only about 6 of cases of nosocomialpneumonia Ventilator-associated pneumonia (VAP) isnosocomial pneumonia arising gt48ndash72 hours after intu-bation Reported incidence of VAP is between 10 and20 for those receiving mechanical ventilation for morethan 48 hours22 It is associated with a higher incidenceof multi-drug-resistant organisms1
PATHOGENESIS
Nosocomial pneumonia is thought to result from micro-aspiration of bacteria colonising the upper respiratory
tract Other routes of infection include macroaspiration
Although there are data demonstrating that surgicalmasks are as effective as N95 (FFP 2) masks in prevent-ing transmission of seasonal inuenza in non-ICU set-tings it is important to note that the capacity for airborne
transmission (and hence the need for N95 masks) isdependent on the exact characteristics of the organismand the frequency of aerosol-generating procedures sothese data should not be extrapolated to other inuenzaviruses and ICU settings
HEALTHCARE-ASSOCIATED PNEUMONIA
Nosocomial pneumonia occurs in 05ndash5 of hospitalpatients with a higher incidence in certain groups(eg postoperative patients and patients in ICU) Diag-nosis may be difcult the clinical features of pneumo-nia are non-specic and many non-infectious conditions
(eg atelectasis pulmonary embolus aspiration heart
Table 362 Procedure for obtaining microbiological samples using bronchoscopy and protected specimen brushingandor bronchoalveolar lavage3549
Infection control In patients suspected of having a disease that is transmitted by the airborne route (egtuberculosis)
bull the risk of transmission should be carefully weighed against the benefits ofbronchoscopy which may generate large numbers of airborne particles
bull perform bronchoscopy in a negative-pressure isolation room
bull consider the use of a muscle relaxant in ventilated patients to prevent coughingbull staff should wear personal protective equipment which should include a fit-tested
negative-pressure respirator (N95 FFP2 or above) as a minimum use of a poweredair-purifying respirator should be considered
General recommendations Suction through the endotracheal tube should be performed before bronchoscopyAvoid suction or injection through the working channel of the bronchoscopePerform protected specimen brushing before bronchoalveolar lavage
Ventilated patients Set F iO2 at 10
Set peak pressure alarm at a level that allows adequate ventilationTitrate ventilator settings against exhaled tidal volumeConsider neuromuscular blockade in addition to sedation in patients at high risk of
complications who are undergoing prolonged bronchoscopy
Protected specimen brushing (PSB) Sample the consolidated segment of lung at subsegmental levelIf purulent secretions are not seen advance the brush until it can no longer be seen but
avoid wedging it in a peripheral positionMove brush back and forth and rotate it several times
Bronchoalveolar lavage (BAL) Wedge tip of bronchoscope into a subsegment of the consolidated segment of lungInject aspirate and collect 20 mL of sterile isotonic saline Do not use this sample for
quantitative microbiology or identification of intracellular organisms It can be used forother microbiological analysis
Inject aspirate and collect additional aliquots of 20ndash60 mLThe total volume of saline injected should be 60ndash200 mL
Complications Hypoxaemia (possibly less with smaller BAL volumes)Arrhythmia
Transient worsening in pulmonary infiltratesBleeding (particularly following PSB)Fever (more common after BAL)
Positive results gt5 of cells in cytocentrifuge preparations of BAL fluid contain intracellular bacteria ORge103 colony-forming unitsmL in PSB specimen ORge104 colony-forming unitsmL in BAL fluid
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 717
420 Pneumonia
worse prognosis In 50 of patients with severehospital-acquired pneumonia and positive bloodcultures there is another source of sepsis
MANAGEMENT
Management is based on the nding that early treat-
ment with antimicrobials that cover all likely patho-gens results in a reduction in morbidity and mortality2 The initial selection of antimicrobials is made on thebasis of epidemiological clues (Fig 362 Table 363)Antimicrobials should be administered within 1 hourof diagnosis12 The results of microbiological investiga-tions are used to narrow antimicrobial cover laterTreatment should be reassessed after 2ndash3 days orsooner if the patient deteriorates (Fig 363) An outlineof management based on an invasive approach is givenin Figure 364
DURATION OF THERAPY
Current ATS guidelines recommend 7 daysrsquo treatmentprovided the aetiological agent is not P aeruginosa orother non-lactose fermenter and the patient has a goodclinical response with resolution of clinical features ofinfection1 The outcome of patients who receive appro-priate initial empirical therapy for ventilator-associatedpneumonia for 8 days is similar to those who receivetreatment for 15 days1
of gastric contents inhaled aerosols haematogenousspread spread from pleural space and direct inocula-tion from ICU personnel
CLINICAL DIAGNOSIS
Diagnosis is based on time of onset (gt48 hours afteradmission to a healthcare facility1) CXR changes (newor progressive inltrates) and either clinical featuresand simple laboratory investigations or the results ofquantitative microbiology Using a clinical approachpneumonia is diagnosed by the nding of a new inl-trate or a change in an inltrate on chest radiographand growth of pathogenic organisms from sputum plusone of the following white-blood-cell (WBC) countgreater than 12times l05L core temperature ge383degCsputum Gram stain with scores of more than two on ascale of four of polymorphonuclear leucocytes andbacteria
INVESTIGATIONSThese are broadly similar to those required incommunity-acquired pneumonia
bull Chest X-ray although studies using a histologicaldiagnosis as the gold standard have demonstratedthat pneumonia may be present despite a normalCXR most denitions of nosocomial pneumoniarequire the presence of new persistent inltrates ona CXR
bull Respiratory secretions considerable controversy sur-rounds the issue of whether invasive bronchoscopicsampling (Table 362) of respiratory secretions is nec-
essary Whether invasive sampling is employed ortracheal aspirates are used empirical broad-spectrumantibiotics should be started while results areawaited The results of microbiological analysis ofrespiratory secretions are used to either stop antibi-otics or narrow the spectrum1 Although the use ofan invasive strategy is associated with a higher like-lihood of modication of initial antimicrobials23 theeffect on important clinical outcome such as mortal-ity antibiotic-free days and organ dysfunction isvariable1 Although tracheal aspirates may predomi-nantly reect the organisms colonising the upper
airway they may be useful in indicating whichorganisms are not responsible for the pneumoniathus allowing the antimicrobial cover to be nar-rowed1 This interpretation is based on the premisethat the predominant route of infection is via theupper respiratory tract From this it can be assumedthat if the organism is not present in the upper res-piratory tract the probability of it being present inthe lung parenchyma is low Certain organisms arevirtually always pathogens when recovered fromrespiratory secretions (see Box 361)
bull Blood cultures identify the aetiological agent in8ndash20 of patients Bacteraemia is associated with a
Figure 362 An outline of initial management ofnosocomial pneumonia based on a non-invasive clinicalapproach1
Two ofuarr or darr WCC
purulent sputum
temp gt38degC
New CXR
infiltrates
Consider acute
tracheobronchitis
Obtain lower respiratory
tract specimens and blood for
microbiological investigations
Risk factorsfor multidrug-resistant
pathogens
Early broad-spectrum
antibiotic therapy
to cover multidrug-
resistant pathogens
Early limited-spectrum
antibiotic therapy
Yes
Yes
No
No
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 817
Healthcare-associated pneumonia 421
inltrate in 48 hours new cavitation or a signicantnew pleural effusion should raise concern If the patientfails to respond consider the diagnosis host factors (egimmunosuppressed debilitated) bacterial factors (egvirulent organism) and therapeutic factors (eg wrongdrug inadequate dose) Review the antibiotics andrepeat cultures It may be useful to broaden the antimi-crobial cover while waiting for the results of investiga-tions Consider invasive sampling of respiratorysecretions computerised tomography or ultrasound ofthe chest (to look for an empyema or abscess) anothersource of infection open-lung biopsy to establish diag-nosis and aetiology or administration of steroids
MORTALITY AND MORBIDITY ATTRIBUTABLE TO VAP Substantial morbidity and mortality associated withVAP have previously been reported22 However acausal relationship is difcult to establish It should benoted that patients who developed VAP tend to be
more severely ill and at higher risk of death not onlyon ICU admission but throughout the course of theirillness Most of the relevant studies were observationaland failed to adequately control confounders likedisease severity evolution of disease progression andICU length of stay with mortality In addition signi-cant heterogeneity exists among these studies Althoughthe presence of VAP is associated with a signicantlylonger ICU length of stay (mean of 61 days 95 CI532ndash687) and increased healthcare cost22 more recentstudies reported that mortality attributable to VAPtends to be small if any2425 The attributable mortalityhas been reported to be 1 on the 30th day of ICU and
RESPONSE TO THERAPY Clinical improvement is usually not apparent for 48ndash72hours and therapy should not be changed during thistime The CXR is of limited value for assessing responseinitial deterioration is common and improvement oftenlags behind clinical response However a rapidly dete-riorating CXR pattern with a gt50 increase in size of
Figure 363 Subsequent management of nosocomialpneumonia based on a non-invasive clinical approach1
Pathogens isolated
from respiratory
specimen
Antibiotics
changedstarted in 7 h
prior to sampling
Adjust antibiotics
according to sensitivities
Continue antibiotics if
high clinical suspicion of
nosocomial pneumonia
Bacterial pneumonia
unlikely
Investigate for other cause
of sepsis and CXR changes
Consider unusual causes
of nosocomial pneumonia
(eg Legionella viruses fungi
Pneumocystis carinii )
Yes
Yes
No
No
Table 363 Recommended initial empirical treatment for nosocomial pneumonia1
SITUATION ANTIBIOTICS
No risk factors for multidrug-resistant pathogens Ceftriaxone or Levofloxacin moxifloxacin or ciprofloxacin or Ampicillinsulbactam or Ertapenem
Antimicrobial therapy in previous 90 days or Current hospitalization for ge5 days or High frequency of antibiotic resistance in the specific
hospital unit or Hospitalisation for 2 days or more in previous 90 days or Residence in nursing home or extended care facility or Home infusion therapy (including antibiotics) or Chronic dialysis within 30 days or Home wound care or Family member with multidrug-resistant pathogen o rImmunosuppression or Bronchiectasis
One ofAntipseudomonal cephalosporin (cefepime or ceftazidime) or Antipseudomonal carbapenem (meropenem or imipenemndash
cilastin) or szlig-lactamszlig-lactamase inhibitor (eg piperacillinndashtazobactam or
cefaperazonendashsulbactam)plus one ofAminoglycoside or Antipseudomonal quinolone (levofloxacin or ciprofloxacin)plus one of the following for patients at high risk of meticillin-
resistant Staphylococcus aureus (MRSA) infectionLinezolid or Vancomycin or
TeicoplaninThe use of dual therapy is not well supported by evidence but it does reduce the probability that the pathogen is resistant to the drugsbeing given If an extended spectrum β-lactamase-producing strain or an Acinetobacter sp is suspected a carbapenem should be givenIf Legionella pneumophilia is suspected use a quinolone Risk factors for MRSA infection in areas with a high incidence of MRSA includediabetes mellitus head trauma coma and renal failure
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 917
422 Pneumonia
or with enlarged cervical nodes or other manifestationsof extrapulmonary disease Clinical disease is seldomfound in asymptomatic individuals even those withstrongly positive tuberculin test (Heaf grade III or IV)The outlook for patients with tuberculosis who requireICU admission is poor In one retrospective study thein-hospital mortality for all patients with tuberculosisrequiring ICU admission was 67 but in those withacute respiratory failure it rose to 8131 The presenta-tion and management of TB in HIV-positive patientsare different (see below)
INVESTIGATION OF PULMONARYTUBERCULOSIS
IDENTIFICATION OF MYCOBACTERIA
Multiple
3233
sputum samples should be collected pref-erably on different days for microscopy for acid-fastbacilli and culture If sputum is not available bronchialwashings taken at bronchoscopy and gastric lavage oraspirate samples should be obtained Gastric aspiratesneed to be neutralised immediately on collection Bron-choscopy and transbronchial biopsy may be useful inpatients with suspected TB but negative sputum smearPleural biopsy is often helpful and mediastinoscopyis occasionally needed in patients with mediastinallymphadenopathy Part of any biopsy specimen shouldalways be sent for culture Nucleic acid amplicationtests on sputum have sensitivity similar to culture in
15 on the 60th day of ICU in a recent study using amulticentre high-quality database and incorporatingnovel statistical methodology to control evolution ofseverity of illness25
PREVENTION
Several guidelines for prevention of ventilator-associated pneumonia and hospital-acquired pneumo-nia have been published26ndash30 Interventions can bedivided into general infection control measures andspecic measures General measures include alcohol-based hand disinfection hospital education programmeon infection control the use of microbiological sur-veillance and a programme to reduce antibiotic pre-scription The major specic recommendations aresummarised in Table 364 There is no evidence that
lsquobundlesrsquo of recommendations are more effective thanthe sum of the individual components
TUBERCULOSIS
The main risk factors are listed in Box 362 Typicalclinical features include fever sweating weight losslassitude anorexia cough productive of mucoid orpurulent sputum haemoptysis chest wall pain dysp-noea localised wheeze and apical crackles Patientsmay also present with unresolved pneumonia pleuraleffusions spontaneous pneumothorax and hoarseness
Figure 364 Management of suspected nosocomial pneumonia based on invasive sampling of respiratory secretions
Bacteria onGram stain
Yes
Yes
No
Yes No Yes No
No
Start antibiotics immediatelyusing PSBBAL specimen
and Gram stain results
Start antibioticsimmediately based onepidemiological clues
Observe look forother infection
Signs ofsevere sepsis
Immediate PSB or BAL beforechangingstarting antimicrobial therapy
+ve cultures +ve cultures
Adjust therapybased on
culture results
Continueadjustantibiotics Look for
other infection
Start antibioticson basisof results
Look forother infection
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1017
Tuberculosis 423
Table 364 Strategies for prevention of ventilator-associated pneumonia
LEVELS OF
RECOMMENDATIONS SPECIFIC INTERVENTIONS REMARKS
Universally recommendedby all guidelines27ndash30
1 Semirecumbent position to 45deg At least 30ndash45deg2 Avoidance of endotracheal intubation3 Preference of oral tracheal route
4 New circuit for a new patient and noschedule change unless soiled or damaged5 Avoidance of flushing of condensate into
lower airway or in-line medication6 HME changes no more frequently than 5ndash7
days7 Continuous aspiration of subglottic suctioning For patients expected to require mechanical
ventilation for gt72 hours
Generally recommendedby most guidelines
1 Preferential use of non-invasiveventilation272830
2 Avoidance of unplanned re-intubation272830
3 Maintenance of endotracheal cuff pressureof about 20 mmHg (266 kPa)272830
4 Closed suctioning2829
No effect on VAP mainly for staff safety5 Chlorhexidine oral decontamination272930
6 Sedation vacation and weaning protocol2728
7 Judicious use of stress ulcer prophylaxis272830
8 Restrictive blood transfusion28
Benefits less clear 1 Preference of HME over heatedhumidifier2830
HME associated with reduction in VAP inpatients ventilated for gt7 days lower cost
2 Silver-sulfadiazine-coated endotrachealtube272830
3 Early tracheostomy (within 7 days ofmechanical ventilation)29
4 Selective decontamination of digestive tract(SDD)272830
Mortality reduction demonstrated when topicalantimicrobials combined with short-course
systemic antibiotics BSAC recommendedSDD in patients expected to requiremechanical ventilation for gt48 hours ETFdiscourage routine use due to concern ofemergence of resistant organisms
Not yet reviewed byguidelines50
1 High-volume low-pressure ultrathin membraneendotracheal tube cuff with SSD
2 Ultrathin membrane cuff with tapered shapeand SSD
3 Low-volume low-pressure endotracheal tubecuff with SSD
4 Balloon device for biofilm removal5 Saline instillation before tracheal suctioning
HME= heat moist exchanger SSD= subglottic secretion drainage
smear-negative patients with pulmonary tuberculosisbut have the advantage of a much more rapid resultThere is however a signicant false-negative rate32
CHEST X-RAY (CXR)A normal CXR almost excludes TB (except inHIV-infected patients) but endobronchial lesionsmay not be apparent and early apical lesions can bemissed Common appearances include patchynodular
shadowing in the upper zones (often bilateral) cavita-tion calcication hilar or mediastinal lymphadenopa-thy (may cause segmental or lobar collapse) pleuraleffusion tuberculomas (dense round or oval shadows)and diffuse ne nodular shadowing throughout thelung elds in miliary TB Inactivity of disease cannot beinferred from the CXR alone This requires three nega-tive sputum samples and failure of any lesion seen onCXR to progress CXR appearances in HIV-positive
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1117
424 Pneumonia
t-tested negative-pressure respirator (N95 FFP2 orhigher) Use of a powered air-purifying respiratorshould be considered when bronchoscopy is being per-formed35 Detailed infection control advice can beobtained via the lsquolink pagersquo (httpwwwaiccuhk eduhkweb8Pneumonia20guidelineshtm)
PNEUMONIA IN THEIMMUNOCOMPROMISED
The lungs are amongst the most frequent targetorgans for infectious complications in the immuno-compromised The incidence of pneumonia is highestamongst patients with haematological malignanciesbone marrow transplant (BMT) recipients and patientswith AIDS
The speed of progression of pneumonia the CXRchanges (Table 365) and the type of immune defectprovide clues to the aetiology Bacterial pneumonias
progress rapidly (1ndash2 days) whereas fungal and proto-zoal pneumonias are less fulminant (several days to aweek or more) Viral pneumonias are usually not ful-minant but on occasions may develop quite rapidlyBronchoscopy is a major component of the investiga-tion of these patients Empirical management based onCXR appearances is outlined in Table 365 Early non-invasive ventilation may improve outcome amongstimmunocompromised patients with fever and bilateralinltrates36
PNEUMOCYSTIS JIROVECI PNEUMONIA (PCP)37
The incidence of this common opportunistic infectionhas fallen substantially in patients with AIDS whoare receiving prophylaxis and effective antiretroviraltherapy with most cases occurring in patients who arenot receiving HIV care or among patients with advancedimmunosuppression The onset is usually insidiouswith dry cough dyspnoea and fever on a backgroundof fatigue and weight loss Crackles in the chest are rareApproximately 15 of patients have a concurrent causefor respiratory failure (eg Kaposi sarcoma TB bacte-rial pneumonia) Useful investigations are
1 CXR classical appearance is diffuse bilateral perihi-
lar interstitial shadowing but in the early stages thisis very subtle and easily missed The initial CXR isnormal in 10 In a further 10 the changes areatypical with focal consolidation or coarse patchyshadowing None of the changes are specic for PCPand may be seen in other lung diseases associatedwith AIDS Pleural effusions hilar or mediastinallymphadenopathy are unusual in PCP but commonin mycobacterial infection or Kaposirsquos sarcoma orlymphoma
2 Induced sputum in this technique the patient inhalesnebulised hypertonic saline from an ultrasonic neb-uliser This provokes bronchorrhoea and the patient
patients with TB differ from those in non-HIV-infectedpatients
TREATMENT OF PULMONARY TB32ndash34
The decision to initiate anti-TB treatment should bebased on level of clinical suspicion results of AFBsmear and sometimes mycobacterial culture If the
initial clinical suspicion is strong and the patient is seri-ously ill attributable to possible TB treatment shouldbe initiated promptly sometimes before the result ofAFB smear Subsequent positivity of AFB smear ornucleic acid amplication test provides support to thecontinuation of treatment Combination chemotherapyconsisting of four drugs is necessary for maximal ef-cacy Treatment is divided into initial phase and con-tinuation phase The most commonly used initialregimen consists of 8 weeks of rifampicin 600 mg daily(450 mg for patients lt50 kg) isoniazid 300 mg dailypyrazinamide 2 g daily (15 g for patients lt50 kg) and
ethambutol 15 mgkg daily as initial phase treatmentEthambutol should be used only in patients who havereasonable visual acuity and who are able to appreciateand report visual disturbances This mandates carefulconsideration in patients who require heavy sedationVisual acuity and colour perception must be assessed(if ethambutol is to be used) and liver and renal func-tion checked before treatment is started Steroids arerecommended for children with endobronchial diseaseand possibly for patients with tuberculous pleuraleffusions Pyridoxine 10 mg daily should be given toprevent isoniazid-induced neuropathy to those atincreased risk (eg patients with diabetes mellitus
chronic renal failure or malnutrition or alcoholic orHIV-positive patients) Negative AFB smear should notdelay initial treatment if clinical suspicion remainshigh Supporting features included chronic coughweight loss characteristic chest X-ray ndings emigra-tion from a high-incidence country no other immediatediagnosis and positive tuberculin test
INFECTION CONTROL
Patients admitted to an ICU with infectious TB or sus-pected of having active pulmonary TB should bemanaged in an isolation room with special ventilation
characteristics including negative pressure Patientsshould be considered infectious if they are coughing orundergoing cough-inducing procedures or if they havepositive AFB smears and they are not on or have juststarted chemotherapy or have a poor clinical or bacte-riological response to chemotherapy3235 Patients withnon-drug-resistant TB should be non-infectious after 2weeks of treatment which includes rifampicin and iso-niazid32 As TB spreads through aerosols it is probablyappropriate to isolate patients who are intubated evenif only their bronchial washings are smear-positiveStaff caring for patients who are smear-positive shouldwear personal protective equipment including a
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1217
Pneumonia in the immunocompromised 425
andor diuretics (patients often uid-overloaded)Approximately 40 of patients with HIV-related PCPwho require mechanical ventilation survive to hospitaldischarge38
Initiation of antiretroviral therapy in patients pre-senting with HIV-related PCP is controversial TheCenters for Disease Control and Prevention (CDC) rec-ommend against doing so in the acute phase but recent
data suggest that the outcome may be improved byinitiation within the rst 4 days of ICU admission39
BACTERIAL PNEUMONIA37
This is the most common cause of acute respiratoryfailure in HIV-positive patients Bacterial pneumonia ismore common in HIV-infected patients than in thegeneral population and tends to be more severe Strep pneumoniae H infuenza Pseudomonas aeruginosa and Saureus are the commonest organisms Nocardia andGram negatives should also be considered Atypicalpathogens (eg Legionella) are rare Response to appro-
priate antibiotics is usually good but may require pro-tracted courses of antibiotics because of high tendencyto relapse Patients with severe immunodeciency(CD4+ T lymphocyte count lt100983221L) and a history ofPseudomonas infection or bronchiectasis or neutropeniashould receive antibiotics that cover P aeruginosa aswell as other Gram negatives The possibility of concur-rent PCP or tuberculosis should be excluded
TUBERCULOSIS
TB may be the initial presentation of AIDS particularlyin sub-Saharan Africa The pattern of TB in HIV patients
coughs up material containing cysts and tropho-zoites The technique is time-consuming and requiresmeticulous technique and is less sensitive thanbronchoscopy but less invasive The possibility ofconcurrent tuberculosis should be consideredand steps taken to minimise the risk of spread ofinfection
3 Bronchoscopy with bronchoalveolar lavage leads to
the diagnosis in over 90 of cases Specimens shouldbe sent for cytology Transbronchial biopsy is notnecessary in most cases PCR using bronchial lavagespecimens may be useful in non-HIV patients withsuspected PCP
Antipneumocystis treatment should be started as soonas the diagnosis is suspected Treatment of choice istrimethoprim plus sulfamethoxazole (co-trimoxazole)20 mgkgday+ 100 mgkgday for 3 weeks plusprednisolone 40 mg orally twice daily for 5 days fol-lowed by 20 mg twice daily for 5 days and then 20 mgper day until the end of PCP treatment Side-effects of
co-trimoxazole are common in HIV patients (nauseavomiting skin rash myelotoxicity) The dose should bereduced by 25 if the WBC count falls Patients whoare intolerant of co-trimoxazole should be treated with
bull pentamidine 4 mgkgday iv or
bull primaquine with clindamycin or
bull trimetrexate with leucovorin (plusmnoral dapsone)
Response to treatment is usually excellent with aresponse time of 4ndash7 days If the patient deteriorates orfails to improve consider (re-)bronchoscopy (is thediagnosis correct) treat co-pathogens and considera short course of high-dose iv methylprednisolone
Table 365 Causes of CXR changes and empirical treatment of pneumonia in the immunocompromised
CHEST X-RAY
APPEARANCE CAUSES
EMPIRICAL TREATMENT FOR
SUSPECTED PNEUMONIA
Diffuse infiltrate CMV and other herpes virusesPneumocystis carinii Bacteria
Aspergillus (advanced)Cryptococcus (uncommon)Non-infectious causes eg drug reaction non-specific
interstitial pneumonitis radiation pneumonitis(uncommon) malignancy leucoagglutinin reaction
Broad-spectrum antibiotics for at least 48 h(eg 3rd-generation cephalosporin andaminoglycoside)
Co-trimoxazoleLung biopsy or lavage within 48 h or full2-week course of co-trimoxazole (dependson patient tolerance of invasive procedure)
Focal infiltrate Gram-negative rodsS aureusAspergillusCryptococcusNocardiaMucorP carinii (uncommon)Tuberculosis
LegionellaNon-infectious causes (eg malignancy non-specificinterstitial pneumonitis radiation pneumonitis)
Broad-spectrum antibioticsIf response seen continue treatment for
2 weeksIf disease progresses lung biopsyaspirate
within 48ndash72 hours or empirical trial ofantifungalplusmn macrolide
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1317
426 Pneumonia
reaction are the most useful tests for demonstratingCMV disease Using thresholds of 10300 000ndash50200 000 positive circulating peripheral WBC the posi-tive predictive value for CMV-pp65 ranges from64 to 82 and the negative predictive value from70 to 954344 Treatment consists of intravenous gan-ciclovir for at least 14 days Foscarnet can be used if
ganciclovir fails
FUNGAL PNEUMONIA
Fungi are rare but important causes of pneumoniaThey can be divided into two main groups based on theimmune response required to combat infection withthese organisms Histoplasma blastomycosis coccidi-oidomycosis paracoccidioidomycosis and Cryptococcus require specic cell-mediated immunity for their controland thus in contrast to infections that are controlled byphagocytic activity the diseases caused by these organ-isms can occur in otherwise healthy individuals
although they cause much more severe illness inpatients with impaired cell-mediated immunity (egpatients infected with HIV and organ transplant recipi-ents) With the exception of Cryptococcus these organ-isms are rarely seen outside North America Aspergillus and Mucor spores are killed by non-immune phago-cytes and as a result these fungi rarely result in clinicalillness in patients with normal neutrophil numbers andfunction
CANDIDIASIS This is effectively a combination of the two types offungal infection in which impaired cell-mediatedimmunity predisposes to mucosal overgrowth withCandida but impaired phagocytic function or numbersis usually required before deep invasion of tissuesoccurs Primary Candida pneumonia (ie isolated lunginfection) is uncommon4145 and more commonly pul-monary lesions are only one manifestation of dissemi-nated candidiasis Even more common is benigncolonisation of the airway with Candida In mostreported cases of primary Candida pneumonia ampho-tericin B has been used In disseminated candidiasistreatment should be directed to treatment of dissemi-nated disease rather than Candida pneumonia per se45
INVASIVE ASPERGILLOSIS 46
This is a highly lethal condition in the immunocom-promised despite treatment and therefore investiga-tion and treatment should be prompt and aggressiveIt is associated with exposure to construction workDenitive diagnosis requires both histological evidenceof acute-angle branching septated non-pigmentedhyphae measuring 2ndash4 983221m in width and cultures yield-ing Aspergillus species from biopsy specimens ofinvolved organs Recovery of Aspergillus species fromrespiratory secretions in immunocompromised butnot immunocompetent patients may indicate invasive
disease with a positive predictive value as high as
depends on the degree of immunosuppression Inpatients with CD4+ T lymphocytes gt350 cells983221L theclinical presentation is similar to TB in non-HIV-infectedpatients although extrapulmonary disease is morecommon In patients with CD4+ T lymphocytes lt350cells983221L extrapulmonary disease (pleuritis pericardi-tis meningitis) is common Severely immunocompro-
mised patients (CD4+
T lymphocytes lt100 cells983221L)may present with severe systemic disease with highfever rapid progression and systemic sepsis In thesepatients lower and middle lobe disease is more commonmiliary disease is common and cavitation is lesscommon Sputum smears and culture may be positiveeven with a normal CXR
Response to treatment is usually rapid Managementof TB in HIV is complex owing to numerous druginteractions consultation with an expert in treatment ofHIV-related TB should be strongly considered Complexinteractions occur between rifamycins (eg rifampicinand rifabutin) and protease inhibitors and non-
nucleoside reverse transcriptase inhibitors used to treatpatients infected with HIV The choice of rifampicin orrifabutin depends on a number of factors includingthe unique and synergistic adverse effects for each indi-vidual combination of rifampicin and anti-HIV drugsand consultation with a physician with experiencein treating both TB and HIV is advised40 IDSA-recommended dosage adjustment for patients receivingantiretrovirals and rifabutin37 can be obtained viathe lsquolink pagersquo (httpwwwaiccuhkeduhkweb8Pneumonia20guidelineshtm) The optimal time forinitiating antiretroviral therapy in patients with TB iscontroversial Early therapy may decrease HIV disease
progression but may be associated with a high inci-dence of adverse effects and an immune reconstitutionreaction37
CMV PNEUMONITIS4142
Risk of infection is highest following allogeneic stemcell transplantation followed by lung transplantationpancreas transplantation and then liver heart and renaltransplantation and advanced AIDS If both the recipi-ent and the donor are seronegative then the risk of bothinfection and disease are negligible If the recipient is
seropositive the risk of infection is approximately 70but the risk of disease is only 20 regardless of theserostatus of the donor However if the recipient isseronegative and the donor is seropositive the risk ofdisease is 70 If steroid pulses and antilymphocyteglobulin are given for treatment of acute rejection therisk of developing disease is markedly increased Infec-tion may be the result of primary infection or reactiva-tion of latent infection It is clinically important butoften difcult to distinguish between CMV infectionand CMV disease and a denitive diagnosis can bemade only histologically Detection of CMV-pp65antigen in peripheral WBC and detection of CMV DNA
or RNA in the blood by quantitative polymerase chain
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1417
Parapneumonic effusion 427
needle aspiration or if there is debris within the uiddrainage using an intercostal drain The diagnosis isconrmed by aspiration of pus
TREATMENT The mainstay of treatment is drainage either by inter-costal drain or by surgical intervention Patients whopresent before the pus is loculated and a brinous peelhas formed on the lung can usually be treated bysimple drainage The combination with intrapleuralbrinolysis may be benecial Optimal surgical man-agement which consists of decortication (open or tho-racoscopic) is indicated if the empyema is moreadvanced or if simple drainage fails This is a majorprocedure and many patients with cardiac or chronicrespiratory disease will not tolerate it Alternatives forthese patients are instillation of thrombolytics into thepleural space or thoracostomy Antibiotics have onlyan adjunctive role Broad-spectrum antibiotic regimenswith anaerobic cover should be used until the resultsof microbiological analysis of the aspirated pus areavailable
AcknowledgementsAll tables and gures are reproduced from ICU web(wwwaiccuhkeduhkweb8) with permission of theauthors
80ndash90 in patients with leukaemia or bone marrowtransplant recipients Bronchoalveolar lavage withsmear culture and antigen detection has excellent spe-cicity and reasonably good positive predictive valuefor invasive aspergillosis in immunocompromisedpatients Although radiological features may give a clueto the diagnosis they are not sufciently specic to be
diagnosticIn acutely ill immunocompromised patients intrave-nous therapy should be initiated if there is suggestiveevidence of invasive aspergillosis while further investi-gations to conrm or refute the diagnosis are carriedout First-line therapy is voriconazole47 Echinocandinsand amphotericin are alternatives
PARAPNEUMONIC EFFUSION
This may be an uncomplicated effusion that resolveswith appropriate treatment of the underlying pneumo-nia or a complicated effusion that develops into an
empyema unless drained Complicated effusions tendto develop 7ndash14 days after initial uid formation Theyare characterised by increasing pleural uid volumecontinued fever and pleural uid of low pH (lt73) thatcontains a large number of neutrophils and may revealorganisms on Gram staining or culture An outline ofmanagement is given in Figure 365
EMPYEMA48
DEFINITION Collection of pus in the pleural space
AETIOLOGY Follows infection of the structures surrounding thepleural space including subdiaphragmatic structuresand chest trauma or may be associated with malig-nancy Anaerobic bacteria usually streptococci orGram-negative rods are responsible for 76 of cases
DIAGNOSIS The diagnosis is usually simple The patient is usuallyseptic and may have a productive cough and chest painThe chest X-ray may show features suggestive of apleural effusion and underlying consolidation but may
also show an abscess cavity with a uid level in whichcase CT scanning will be required to distinguishbetween an abscess and an empyema Ultrasound canbe useful to conrm the presence of uid in the pleuralspace and to determine whether it can be drained by
Figure 365 An approach to the management of
parapneumonic effusions
Parapneumonic effusion
gt 1 cm thick
on lateral decubitus
film
Pleural aspirate
turbid or purulent or
Gram stain +ve
Pleural aspirate
pH
Serial thoracocentesis Treat as empyemaObserve
No
gt72 lt70
70ndash72
No
Yes
Yes
httpwwwexpertconsultcomAccess the complete references list online at
1 American Thoracic Society and Infectious Diseases Society of America Guidelines for the manage-ment of adults with hospital-acquired ventilator-associated and healthcare associated pneumonia
Am J Respir Crit Care Med 2005171388ndash416
2 Mandell LA Wunderink RG Anzueto A et al Infec-tious Diseases Society of AmericaAmerican Tho-racic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin
Infect Dis 200744S27ndash72
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1517
428 Pneumonia
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1617
References 428e1
REFERENCES 1 American Thoracic Society and Infectious Diseases
Society of America Guidelines for the management of adults with hospital-acquired ventilator-associated and healthcare associated pneumonia Am J Respir Crit Care Med 2005171388ndash416
2 Mandell LA Wunderink RG Anzueto A et al Infec-tious Diseases Society of AmericaAmerican Tho-racic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744S27ndash72
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
4 Woodhead M Blasi F Ewig S et al Guidelines for the management of adult lower respiratory tract infections Eur Respir J 2005261138ndash80
5 Torres A Rello J Update in community-acquired and nosocomial pneumonia 2009 Am J Respir Crit
Care Med 2010181782ndash76 Van der Eerden MM Vlaspolder F de Graaff CS et
al Value of intensive diagnostic microbiological investigation in low- and high-risk patients with community-acquired pneumonia Eur J Clin Micro Infect Dis 200524241ndash9
7 Murdoch DR Nucleic acid amplication tests for the diagnosis of pneumonia Clin Infect Dis 2003361162ndash70
8 Blaschke AJ Interpreting assays for the detection of Streptococcus pneumonia Clin Infect Dis 201152(S4)S331ndash7
9 Rello J Lisboa T Lujan M Severity of pneumococcal
pneumonia associated with genomic bacterial load Chest 2009136832ndash4010 Azoulay E Bergeron A Polymerase chain reaction
for diagnosing pneumocystis pneumonia in non-HIV immunocompromised patients with pulmonary inl-trates Chest 2009135(3)655
11 Garcia-Vidal C Fernandez-Sabe N Carratala J Early mortality in patients with community-acquired pneumonia causes and risk factors Eur Respir J200832733ndash9
12 Dellinger RP Carlet JM Masur H et al Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock Intensive Care Med200430536ndash55
13 Metersky ML Ma A Houck PM et al Antibiotics for bacteremic pneumonia improved outcomes with macrolides but not uoroquinolones Chest 2007131466ndash73
14 Dunbar LM Wunderink RG Habib MP High-dose short-course levooxacin for community-acquired pneumonia a new treatment paradigm Clin Infect Dis 200337752ndash60
15 Matthaiou DK Ntani G An ESICM systematic review and meta-analysis of procalcitonin-guided antibiotic therapy algorithms in adult critically ill patients Intensive Care Med 201238940ndash9
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
17 Gruber PC Gomersall CD Joynt GM Avian inu-enza (H5N1) implications for intensive care Inten-sive Care Med 200632823ndash9
18 Belongia EA Irving SA Clinical characteristics and 30-day outcomes for inuenza A 2009 (H1N1) 2008ndash2009 (H1N1) and 2007ndash8 (H3N2) infections JAMA2010304(10)1091
19 Lee N Chan PKS Complications and outcomes of pandemic 2009 inuenza A (H1N1) virus infection in hospitalized adults how do they differ from those in seasonal inuenza J Infect Dis 20112031739ndash47
20 Kim SH Hong SB Corticosteroid treatment in critically ill patients with pandemic inuenza AH1N1 2009 infection analytic strategy using pro-pensity scores Am J Respir Crit Care Med 20111831207ndash14
21 Centers for Disease Control and Prevention (CDC) Bacterial coinfections in lung tissue specimens from
fatal cases of 2009 pandemic inuenza A (H1N1) ndash United States MayndashAugust 2009 MMWR 2009581071ndash4
22 Safdar N Dezfulian C Clinical and economic conse-quences of ventilator-associated pneumonia A sys-tematic review Crit Care Med 200533(10)2184ndash93
23 Shorr AF Sherner JH Invasive approaches to the diagnosis of ventilator-associated pneumonia A meta-analysis Crit Care Med 200533(1)46ndash53
24 Melsen WG Rovers MM Ventilator-associated pneumonia and mortality A systematic review of observational studies Crit Care Med 2009372709ndash18
25 Bekaert M Timsit JF Attributable mortality of ventilator-associated pneumonia A reappraisal using causal analysis Am J Respir Crit Care Med20111841133ndash9
26 CDC Healthcare Infection Control Practices AdvisoryCommittee Guidelines for preventing health-care-associated pneumonia 2003 Recommendations ofCDC and the Healthcare Infection Control PracticesAdvisory Committee Online Available httpwwwcdcgovmmwrpreviewmmwrhtmlrr5303a1htm
27 Cofn SE Klompas M SHEAIDSA practice recom-mendation strategies to prevent ventilator-associated pneumonia in acute care hospitals Infect Control
Hosp Epidemiol 200829S31ndash4028 Masterton RG Galloway A Guidelines for the man-
agement of hospital-acquired pneumonia in the UK Report of the Working Party on Hospital-Acquired Pneumonia of the British Society for Antimicrobial Chemotherapy J Antimicrob Chemother 2008625ndash34
29 VAP Guidelines Committee and the Canadian Critical Care Trials Group Comprehensive evidence-based clinical practice guidelines for ventilator-associated pneumonia prevention J Crit Care 200823126ndash37
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1717
428e2 Pneumonia
30 Torres A Ewig S Dening treating and preventing hospital acquired pneumonia European perspective Intensive Care Med 2009359ndash29
31 Frame RN Johnson MC Eichenhorn MS et al Active tuberculosis in the medical intensive care unit a 15-year retrospective analysis Crit Care Med 1987151012ndash14
32 National Collaborating Centre for Chronic Condi-tions Tuberculosis Clinical diagnosis and manage-ment of tuberculosis and measures for its prevention and control London Royal College of Physicians 2006
33 Small PM Fujiwara PI Management of tuberculosis in the United States N Engl J Med 2001345189ndash200
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
35 Centers for Disease Control and Prevention Guide-lines for preventing the transmission of Mycobacte-rium tuberculosis in health-care settings 2005 MMWR
2005541ndash11936 Hilbert G Gruson D Vargas F et al Noninvasive
ventilation in immunosuppressed patients with pul-monary inltrates fever and acute respiratory failure N Engl J Med 2001344481ndash7
37 Benson CA Kaplan JE Masur H Treating oppor-tunistic infections among HIV-infected adults and adolescents recommendations from CDC the National Institutes of Health and the HIV Medicine AssociationInfectious Diseases Society of America Clin Infect Dis 200540S131ndash235
38 Randall CJ Yarnold PR Schwartz DN et al Improve-ments in outcomes of acute respiratory failure for
patients with human immunodeciency virus-related Pneumocystis carinii pneumonia Am J Respir Crit Care Med 2000162393ndash8
39 Croda J Croda MG Neves A et al Benet of antiret-roviral therapy on survival of human immunode-ciency virus-infected patients admitted to an intensive care unit Crit Care Med 200937(5)1605
40 Centers for Disease Control Updated guidelines for the use of rifabutin or rifampicin for the treatment and prevention of tuberculosis among HIV-infected patients taking protease inhibitors or nonnucleoside reverse transcriptase inhibitors MMWR 200049185ndash9
41 Tamm M The lung in the immunocompromised patient Infectious complications part 2 Respiration199966199ndash207
42 Van der Bij W Speich R Management of cytomega-lovirus infection and disease after solid-organ trans-plantation Clin Infect Dis 200133(Suppl 1)S32ndash7
43 Schaumlfer P Tenschert W Cremaschi L et al Area under the viraemia curve versus absolute viral load utility for predicting symptomatic cytomegalovirus infections in kidney transplant patients J Med Virol20016585ndash9
44 Meyer-Koenig U Weidmann M Kirste G et al Cytomegalovirus infection in organ-transplant recip-ients diagnostic value of pp65 antigen test qualita-tive polymerase chain reaction (PCR) and quantitative
Taqman PCR Transplantation 2004771692ndash8
45 Pappas PG Rex JH Sobel JD Guidelines for treat-ment of candidiasis Clin Infect Dis 200438161ndash89
46 Stevens DA Kan VL Judson MA Practice guidelines for diseases caused by Aspergillus Clin Infect Dis200030696ndash709
47 Herbrecht R Denning DW Patterson TF Voricona-zole versus amphotericin B for primary therapy of invasive aspergillosis N Engl J Med 2002347408ndash15
48 Peek GJ Morcos S Cooper G The pleural cavity BMJ20003201318ndash21
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6

7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 717
420 Pneumonia
worse prognosis In 50 of patients with severehospital-acquired pneumonia and positive bloodcultures there is another source of sepsis
MANAGEMENT
Management is based on the nding that early treat-
ment with antimicrobials that cover all likely patho-gens results in a reduction in morbidity and mortality2 The initial selection of antimicrobials is made on thebasis of epidemiological clues (Fig 362 Table 363)Antimicrobials should be administered within 1 hourof diagnosis12 The results of microbiological investiga-tions are used to narrow antimicrobial cover laterTreatment should be reassessed after 2ndash3 days orsooner if the patient deteriorates (Fig 363) An outlineof management based on an invasive approach is givenin Figure 364
DURATION OF THERAPY
Current ATS guidelines recommend 7 daysrsquo treatmentprovided the aetiological agent is not P aeruginosa orother non-lactose fermenter and the patient has a goodclinical response with resolution of clinical features ofinfection1 The outcome of patients who receive appro-priate initial empirical therapy for ventilator-associatedpneumonia for 8 days is similar to those who receivetreatment for 15 days1
of gastric contents inhaled aerosols haematogenousspread spread from pleural space and direct inocula-tion from ICU personnel
CLINICAL DIAGNOSIS
Diagnosis is based on time of onset (gt48 hours afteradmission to a healthcare facility1) CXR changes (newor progressive inltrates) and either clinical featuresand simple laboratory investigations or the results ofquantitative microbiology Using a clinical approachpneumonia is diagnosed by the nding of a new inl-trate or a change in an inltrate on chest radiographand growth of pathogenic organisms from sputum plusone of the following white-blood-cell (WBC) countgreater than 12times l05L core temperature ge383degCsputum Gram stain with scores of more than two on ascale of four of polymorphonuclear leucocytes andbacteria
INVESTIGATIONSThese are broadly similar to those required incommunity-acquired pneumonia
bull Chest X-ray although studies using a histologicaldiagnosis as the gold standard have demonstratedthat pneumonia may be present despite a normalCXR most denitions of nosocomial pneumoniarequire the presence of new persistent inltrates ona CXR
bull Respiratory secretions considerable controversy sur-rounds the issue of whether invasive bronchoscopicsampling (Table 362) of respiratory secretions is nec-
essary Whether invasive sampling is employed ortracheal aspirates are used empirical broad-spectrumantibiotics should be started while results areawaited The results of microbiological analysis ofrespiratory secretions are used to either stop antibi-otics or narrow the spectrum1 Although the use ofan invasive strategy is associated with a higher like-lihood of modication of initial antimicrobials23 theeffect on important clinical outcome such as mortal-ity antibiotic-free days and organ dysfunction isvariable1 Although tracheal aspirates may predomi-nantly reect the organisms colonising the upper
airway they may be useful in indicating whichorganisms are not responsible for the pneumoniathus allowing the antimicrobial cover to be nar-rowed1 This interpretation is based on the premisethat the predominant route of infection is via theupper respiratory tract From this it can be assumedthat if the organism is not present in the upper res-piratory tract the probability of it being present inthe lung parenchyma is low Certain organisms arevirtually always pathogens when recovered fromrespiratory secretions (see Box 361)
bull Blood cultures identify the aetiological agent in8ndash20 of patients Bacteraemia is associated with a
Figure 362 An outline of initial management ofnosocomial pneumonia based on a non-invasive clinicalapproach1
Two ofuarr or darr WCC
purulent sputum
temp gt38degC
New CXR
infiltrates
Consider acute
tracheobronchitis
Obtain lower respiratory
tract specimens and blood for
microbiological investigations
Risk factorsfor multidrug-resistant
pathogens
Early broad-spectrum
antibiotic therapy
to cover multidrug-
resistant pathogens
Early limited-spectrum
antibiotic therapy
Yes
Yes
No
No
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 817
Healthcare-associated pneumonia 421
inltrate in 48 hours new cavitation or a signicantnew pleural effusion should raise concern If the patientfails to respond consider the diagnosis host factors (egimmunosuppressed debilitated) bacterial factors (egvirulent organism) and therapeutic factors (eg wrongdrug inadequate dose) Review the antibiotics andrepeat cultures It may be useful to broaden the antimi-crobial cover while waiting for the results of investiga-tions Consider invasive sampling of respiratorysecretions computerised tomography or ultrasound ofthe chest (to look for an empyema or abscess) anothersource of infection open-lung biopsy to establish diag-nosis and aetiology or administration of steroids
MORTALITY AND MORBIDITY ATTRIBUTABLE TO VAP Substantial morbidity and mortality associated withVAP have previously been reported22 However acausal relationship is difcult to establish It should benoted that patients who developed VAP tend to be
more severely ill and at higher risk of death not onlyon ICU admission but throughout the course of theirillness Most of the relevant studies were observationaland failed to adequately control confounders likedisease severity evolution of disease progression andICU length of stay with mortality In addition signi-cant heterogeneity exists among these studies Althoughthe presence of VAP is associated with a signicantlylonger ICU length of stay (mean of 61 days 95 CI532ndash687) and increased healthcare cost22 more recentstudies reported that mortality attributable to VAPtends to be small if any2425 The attributable mortalityhas been reported to be 1 on the 30th day of ICU and
RESPONSE TO THERAPY Clinical improvement is usually not apparent for 48ndash72hours and therapy should not be changed during thistime The CXR is of limited value for assessing responseinitial deterioration is common and improvement oftenlags behind clinical response However a rapidly dete-riorating CXR pattern with a gt50 increase in size of
Figure 363 Subsequent management of nosocomialpneumonia based on a non-invasive clinical approach1
Pathogens isolated
from respiratory
specimen
Antibiotics
changedstarted in 7 h
prior to sampling
Adjust antibiotics
according to sensitivities
Continue antibiotics if
high clinical suspicion of
nosocomial pneumonia
Bacterial pneumonia
unlikely
Investigate for other cause
of sepsis and CXR changes
Consider unusual causes
of nosocomial pneumonia
(eg Legionella viruses fungi
Pneumocystis carinii )
Yes
Yes
No
No
Table 363 Recommended initial empirical treatment for nosocomial pneumonia1
SITUATION ANTIBIOTICS
No risk factors for multidrug-resistant pathogens Ceftriaxone or Levofloxacin moxifloxacin or ciprofloxacin or Ampicillinsulbactam or Ertapenem
Antimicrobial therapy in previous 90 days or Current hospitalization for ge5 days or High frequency of antibiotic resistance in the specific
hospital unit or Hospitalisation for 2 days or more in previous 90 days or Residence in nursing home or extended care facility or Home infusion therapy (including antibiotics) or Chronic dialysis within 30 days or Home wound care or Family member with multidrug-resistant pathogen o rImmunosuppression or Bronchiectasis
One ofAntipseudomonal cephalosporin (cefepime or ceftazidime) or Antipseudomonal carbapenem (meropenem or imipenemndash
cilastin) or szlig-lactamszlig-lactamase inhibitor (eg piperacillinndashtazobactam or
cefaperazonendashsulbactam)plus one ofAminoglycoside or Antipseudomonal quinolone (levofloxacin or ciprofloxacin)plus one of the following for patients at high risk of meticillin-
resistant Staphylococcus aureus (MRSA) infectionLinezolid or Vancomycin or
TeicoplaninThe use of dual therapy is not well supported by evidence but it does reduce the probability that the pathogen is resistant to the drugsbeing given If an extended spectrum β-lactamase-producing strain or an Acinetobacter sp is suspected a carbapenem should be givenIf Legionella pneumophilia is suspected use a quinolone Risk factors for MRSA infection in areas with a high incidence of MRSA includediabetes mellitus head trauma coma and renal failure
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 917
422 Pneumonia
or with enlarged cervical nodes or other manifestationsof extrapulmonary disease Clinical disease is seldomfound in asymptomatic individuals even those withstrongly positive tuberculin test (Heaf grade III or IV)The outlook for patients with tuberculosis who requireICU admission is poor In one retrospective study thein-hospital mortality for all patients with tuberculosisrequiring ICU admission was 67 but in those withacute respiratory failure it rose to 8131 The presenta-tion and management of TB in HIV-positive patientsare different (see below)
INVESTIGATION OF PULMONARYTUBERCULOSIS
IDENTIFICATION OF MYCOBACTERIA
Multiple
3233
sputum samples should be collected pref-erably on different days for microscopy for acid-fastbacilli and culture If sputum is not available bronchialwashings taken at bronchoscopy and gastric lavage oraspirate samples should be obtained Gastric aspiratesneed to be neutralised immediately on collection Bron-choscopy and transbronchial biopsy may be useful inpatients with suspected TB but negative sputum smearPleural biopsy is often helpful and mediastinoscopyis occasionally needed in patients with mediastinallymphadenopathy Part of any biopsy specimen shouldalways be sent for culture Nucleic acid amplicationtests on sputum have sensitivity similar to culture in
15 on the 60th day of ICU in a recent study using amulticentre high-quality database and incorporatingnovel statistical methodology to control evolution ofseverity of illness25
PREVENTION
Several guidelines for prevention of ventilator-associated pneumonia and hospital-acquired pneumo-nia have been published26ndash30 Interventions can bedivided into general infection control measures andspecic measures General measures include alcohol-based hand disinfection hospital education programmeon infection control the use of microbiological sur-veillance and a programme to reduce antibiotic pre-scription The major specic recommendations aresummarised in Table 364 There is no evidence that
lsquobundlesrsquo of recommendations are more effective thanthe sum of the individual components
TUBERCULOSIS
The main risk factors are listed in Box 362 Typicalclinical features include fever sweating weight losslassitude anorexia cough productive of mucoid orpurulent sputum haemoptysis chest wall pain dysp-noea localised wheeze and apical crackles Patientsmay also present with unresolved pneumonia pleuraleffusions spontaneous pneumothorax and hoarseness
Figure 364 Management of suspected nosocomial pneumonia based on invasive sampling of respiratory secretions
Bacteria onGram stain
Yes
Yes
No
Yes No Yes No
No
Start antibiotics immediatelyusing PSBBAL specimen
and Gram stain results
Start antibioticsimmediately based onepidemiological clues
Observe look forother infection
Signs ofsevere sepsis
Immediate PSB or BAL beforechangingstarting antimicrobial therapy
+ve cultures +ve cultures
Adjust therapybased on
culture results
Continueadjustantibiotics Look for
other infection
Start antibioticson basisof results
Look forother infection
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1017
Tuberculosis 423
Table 364 Strategies for prevention of ventilator-associated pneumonia
LEVELS OF
RECOMMENDATIONS SPECIFIC INTERVENTIONS REMARKS
Universally recommendedby all guidelines27ndash30
1 Semirecumbent position to 45deg At least 30ndash45deg2 Avoidance of endotracheal intubation3 Preference of oral tracheal route
4 New circuit for a new patient and noschedule change unless soiled or damaged5 Avoidance of flushing of condensate into
lower airway or in-line medication6 HME changes no more frequently than 5ndash7
days7 Continuous aspiration of subglottic suctioning For patients expected to require mechanical
ventilation for gt72 hours
Generally recommendedby most guidelines
1 Preferential use of non-invasiveventilation272830
2 Avoidance of unplanned re-intubation272830
3 Maintenance of endotracheal cuff pressureof about 20 mmHg (266 kPa)272830
4 Closed suctioning2829
No effect on VAP mainly for staff safety5 Chlorhexidine oral decontamination272930
6 Sedation vacation and weaning protocol2728
7 Judicious use of stress ulcer prophylaxis272830
8 Restrictive blood transfusion28
Benefits less clear 1 Preference of HME over heatedhumidifier2830
HME associated with reduction in VAP inpatients ventilated for gt7 days lower cost
2 Silver-sulfadiazine-coated endotrachealtube272830
3 Early tracheostomy (within 7 days ofmechanical ventilation)29
4 Selective decontamination of digestive tract(SDD)272830
Mortality reduction demonstrated when topicalantimicrobials combined with short-course
systemic antibiotics BSAC recommendedSDD in patients expected to requiremechanical ventilation for gt48 hours ETFdiscourage routine use due to concern ofemergence of resistant organisms
Not yet reviewed byguidelines50
1 High-volume low-pressure ultrathin membraneendotracheal tube cuff with SSD
2 Ultrathin membrane cuff with tapered shapeand SSD
3 Low-volume low-pressure endotracheal tubecuff with SSD
4 Balloon device for biofilm removal5 Saline instillation before tracheal suctioning
HME= heat moist exchanger SSD= subglottic secretion drainage
smear-negative patients with pulmonary tuberculosisbut have the advantage of a much more rapid resultThere is however a signicant false-negative rate32
CHEST X-RAY (CXR)A normal CXR almost excludes TB (except inHIV-infected patients) but endobronchial lesionsmay not be apparent and early apical lesions can bemissed Common appearances include patchynodular
shadowing in the upper zones (often bilateral) cavita-tion calcication hilar or mediastinal lymphadenopa-thy (may cause segmental or lobar collapse) pleuraleffusion tuberculomas (dense round or oval shadows)and diffuse ne nodular shadowing throughout thelung elds in miliary TB Inactivity of disease cannot beinferred from the CXR alone This requires three nega-tive sputum samples and failure of any lesion seen onCXR to progress CXR appearances in HIV-positive
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1117
424 Pneumonia
t-tested negative-pressure respirator (N95 FFP2 orhigher) Use of a powered air-purifying respiratorshould be considered when bronchoscopy is being per-formed35 Detailed infection control advice can beobtained via the lsquolink pagersquo (httpwwwaiccuhk eduhkweb8Pneumonia20guidelineshtm)
PNEUMONIA IN THEIMMUNOCOMPROMISED
The lungs are amongst the most frequent targetorgans for infectious complications in the immuno-compromised The incidence of pneumonia is highestamongst patients with haematological malignanciesbone marrow transplant (BMT) recipients and patientswith AIDS
The speed of progression of pneumonia the CXRchanges (Table 365) and the type of immune defectprovide clues to the aetiology Bacterial pneumonias
progress rapidly (1ndash2 days) whereas fungal and proto-zoal pneumonias are less fulminant (several days to aweek or more) Viral pneumonias are usually not ful-minant but on occasions may develop quite rapidlyBronchoscopy is a major component of the investiga-tion of these patients Empirical management based onCXR appearances is outlined in Table 365 Early non-invasive ventilation may improve outcome amongstimmunocompromised patients with fever and bilateralinltrates36
PNEUMOCYSTIS JIROVECI PNEUMONIA (PCP)37
The incidence of this common opportunistic infectionhas fallen substantially in patients with AIDS whoare receiving prophylaxis and effective antiretroviraltherapy with most cases occurring in patients who arenot receiving HIV care or among patients with advancedimmunosuppression The onset is usually insidiouswith dry cough dyspnoea and fever on a backgroundof fatigue and weight loss Crackles in the chest are rareApproximately 15 of patients have a concurrent causefor respiratory failure (eg Kaposi sarcoma TB bacte-rial pneumonia) Useful investigations are
1 CXR classical appearance is diffuse bilateral perihi-
lar interstitial shadowing but in the early stages thisis very subtle and easily missed The initial CXR isnormal in 10 In a further 10 the changes areatypical with focal consolidation or coarse patchyshadowing None of the changes are specic for PCPand may be seen in other lung diseases associatedwith AIDS Pleural effusions hilar or mediastinallymphadenopathy are unusual in PCP but commonin mycobacterial infection or Kaposirsquos sarcoma orlymphoma
2 Induced sputum in this technique the patient inhalesnebulised hypertonic saline from an ultrasonic neb-uliser This provokes bronchorrhoea and the patient
patients with TB differ from those in non-HIV-infectedpatients
TREATMENT OF PULMONARY TB32ndash34
The decision to initiate anti-TB treatment should bebased on level of clinical suspicion results of AFBsmear and sometimes mycobacterial culture If the
initial clinical suspicion is strong and the patient is seri-ously ill attributable to possible TB treatment shouldbe initiated promptly sometimes before the result ofAFB smear Subsequent positivity of AFB smear ornucleic acid amplication test provides support to thecontinuation of treatment Combination chemotherapyconsisting of four drugs is necessary for maximal ef-cacy Treatment is divided into initial phase and con-tinuation phase The most commonly used initialregimen consists of 8 weeks of rifampicin 600 mg daily(450 mg for patients lt50 kg) isoniazid 300 mg dailypyrazinamide 2 g daily (15 g for patients lt50 kg) and
ethambutol 15 mgkg daily as initial phase treatmentEthambutol should be used only in patients who havereasonable visual acuity and who are able to appreciateand report visual disturbances This mandates carefulconsideration in patients who require heavy sedationVisual acuity and colour perception must be assessed(if ethambutol is to be used) and liver and renal func-tion checked before treatment is started Steroids arerecommended for children with endobronchial diseaseand possibly for patients with tuberculous pleuraleffusions Pyridoxine 10 mg daily should be given toprevent isoniazid-induced neuropathy to those atincreased risk (eg patients with diabetes mellitus
chronic renal failure or malnutrition or alcoholic orHIV-positive patients) Negative AFB smear should notdelay initial treatment if clinical suspicion remainshigh Supporting features included chronic coughweight loss characteristic chest X-ray ndings emigra-tion from a high-incidence country no other immediatediagnosis and positive tuberculin test
INFECTION CONTROL
Patients admitted to an ICU with infectious TB or sus-pected of having active pulmonary TB should bemanaged in an isolation room with special ventilation
characteristics including negative pressure Patientsshould be considered infectious if they are coughing orundergoing cough-inducing procedures or if they havepositive AFB smears and they are not on or have juststarted chemotherapy or have a poor clinical or bacte-riological response to chemotherapy3235 Patients withnon-drug-resistant TB should be non-infectious after 2weeks of treatment which includes rifampicin and iso-niazid32 As TB spreads through aerosols it is probablyappropriate to isolate patients who are intubated evenif only their bronchial washings are smear-positiveStaff caring for patients who are smear-positive shouldwear personal protective equipment including a
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1217
Pneumonia in the immunocompromised 425
andor diuretics (patients often uid-overloaded)Approximately 40 of patients with HIV-related PCPwho require mechanical ventilation survive to hospitaldischarge38
Initiation of antiretroviral therapy in patients pre-senting with HIV-related PCP is controversial TheCenters for Disease Control and Prevention (CDC) rec-ommend against doing so in the acute phase but recent
data suggest that the outcome may be improved byinitiation within the rst 4 days of ICU admission39
BACTERIAL PNEUMONIA37
This is the most common cause of acute respiratoryfailure in HIV-positive patients Bacterial pneumonia ismore common in HIV-infected patients than in thegeneral population and tends to be more severe Strep pneumoniae H infuenza Pseudomonas aeruginosa and Saureus are the commonest organisms Nocardia andGram negatives should also be considered Atypicalpathogens (eg Legionella) are rare Response to appro-
priate antibiotics is usually good but may require pro-tracted courses of antibiotics because of high tendencyto relapse Patients with severe immunodeciency(CD4+ T lymphocyte count lt100983221L) and a history ofPseudomonas infection or bronchiectasis or neutropeniashould receive antibiotics that cover P aeruginosa aswell as other Gram negatives The possibility of concur-rent PCP or tuberculosis should be excluded
TUBERCULOSIS
TB may be the initial presentation of AIDS particularlyin sub-Saharan Africa The pattern of TB in HIV patients
coughs up material containing cysts and tropho-zoites The technique is time-consuming and requiresmeticulous technique and is less sensitive thanbronchoscopy but less invasive The possibility ofconcurrent tuberculosis should be consideredand steps taken to minimise the risk of spread ofinfection
3 Bronchoscopy with bronchoalveolar lavage leads to
the diagnosis in over 90 of cases Specimens shouldbe sent for cytology Transbronchial biopsy is notnecessary in most cases PCR using bronchial lavagespecimens may be useful in non-HIV patients withsuspected PCP
Antipneumocystis treatment should be started as soonas the diagnosis is suspected Treatment of choice istrimethoprim plus sulfamethoxazole (co-trimoxazole)20 mgkgday+ 100 mgkgday for 3 weeks plusprednisolone 40 mg orally twice daily for 5 days fol-lowed by 20 mg twice daily for 5 days and then 20 mgper day until the end of PCP treatment Side-effects of
co-trimoxazole are common in HIV patients (nauseavomiting skin rash myelotoxicity) The dose should bereduced by 25 if the WBC count falls Patients whoare intolerant of co-trimoxazole should be treated with
bull pentamidine 4 mgkgday iv or
bull primaquine with clindamycin or
bull trimetrexate with leucovorin (plusmnoral dapsone)
Response to treatment is usually excellent with aresponse time of 4ndash7 days If the patient deteriorates orfails to improve consider (re-)bronchoscopy (is thediagnosis correct) treat co-pathogens and considera short course of high-dose iv methylprednisolone
Table 365 Causes of CXR changes and empirical treatment of pneumonia in the immunocompromised
CHEST X-RAY
APPEARANCE CAUSES
EMPIRICAL TREATMENT FOR
SUSPECTED PNEUMONIA
Diffuse infiltrate CMV and other herpes virusesPneumocystis carinii Bacteria
Aspergillus (advanced)Cryptococcus (uncommon)Non-infectious causes eg drug reaction non-specific
interstitial pneumonitis radiation pneumonitis(uncommon) malignancy leucoagglutinin reaction
Broad-spectrum antibiotics for at least 48 h(eg 3rd-generation cephalosporin andaminoglycoside)
Co-trimoxazoleLung biopsy or lavage within 48 h or full2-week course of co-trimoxazole (dependson patient tolerance of invasive procedure)
Focal infiltrate Gram-negative rodsS aureusAspergillusCryptococcusNocardiaMucorP carinii (uncommon)Tuberculosis
LegionellaNon-infectious causes (eg malignancy non-specificinterstitial pneumonitis radiation pneumonitis)
Broad-spectrum antibioticsIf response seen continue treatment for
2 weeksIf disease progresses lung biopsyaspirate
within 48ndash72 hours or empirical trial ofantifungalplusmn macrolide
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1317
426 Pneumonia
reaction are the most useful tests for demonstratingCMV disease Using thresholds of 10300 000ndash50200 000 positive circulating peripheral WBC the posi-tive predictive value for CMV-pp65 ranges from64 to 82 and the negative predictive value from70 to 954344 Treatment consists of intravenous gan-ciclovir for at least 14 days Foscarnet can be used if
ganciclovir fails
FUNGAL PNEUMONIA
Fungi are rare but important causes of pneumoniaThey can be divided into two main groups based on theimmune response required to combat infection withthese organisms Histoplasma blastomycosis coccidi-oidomycosis paracoccidioidomycosis and Cryptococcus require specic cell-mediated immunity for their controland thus in contrast to infections that are controlled byphagocytic activity the diseases caused by these organ-isms can occur in otherwise healthy individuals
although they cause much more severe illness inpatients with impaired cell-mediated immunity (egpatients infected with HIV and organ transplant recipi-ents) With the exception of Cryptococcus these organ-isms are rarely seen outside North America Aspergillus and Mucor spores are killed by non-immune phago-cytes and as a result these fungi rarely result in clinicalillness in patients with normal neutrophil numbers andfunction
CANDIDIASIS This is effectively a combination of the two types offungal infection in which impaired cell-mediatedimmunity predisposes to mucosal overgrowth withCandida but impaired phagocytic function or numbersis usually required before deep invasion of tissuesoccurs Primary Candida pneumonia (ie isolated lunginfection) is uncommon4145 and more commonly pul-monary lesions are only one manifestation of dissemi-nated candidiasis Even more common is benigncolonisation of the airway with Candida In mostreported cases of primary Candida pneumonia ampho-tericin B has been used In disseminated candidiasistreatment should be directed to treatment of dissemi-nated disease rather than Candida pneumonia per se45
INVASIVE ASPERGILLOSIS 46
This is a highly lethal condition in the immunocom-promised despite treatment and therefore investiga-tion and treatment should be prompt and aggressiveIt is associated with exposure to construction workDenitive diagnosis requires both histological evidenceof acute-angle branching septated non-pigmentedhyphae measuring 2ndash4 983221m in width and cultures yield-ing Aspergillus species from biopsy specimens ofinvolved organs Recovery of Aspergillus species fromrespiratory secretions in immunocompromised butnot immunocompetent patients may indicate invasive
disease with a positive predictive value as high as
depends on the degree of immunosuppression Inpatients with CD4+ T lymphocytes gt350 cells983221L theclinical presentation is similar to TB in non-HIV-infectedpatients although extrapulmonary disease is morecommon In patients with CD4+ T lymphocytes lt350cells983221L extrapulmonary disease (pleuritis pericardi-tis meningitis) is common Severely immunocompro-
mised patients (CD4+
T lymphocytes lt100 cells983221L)may present with severe systemic disease with highfever rapid progression and systemic sepsis In thesepatients lower and middle lobe disease is more commonmiliary disease is common and cavitation is lesscommon Sputum smears and culture may be positiveeven with a normal CXR
Response to treatment is usually rapid Managementof TB in HIV is complex owing to numerous druginteractions consultation with an expert in treatment ofHIV-related TB should be strongly considered Complexinteractions occur between rifamycins (eg rifampicinand rifabutin) and protease inhibitors and non-
nucleoside reverse transcriptase inhibitors used to treatpatients infected with HIV The choice of rifampicin orrifabutin depends on a number of factors includingthe unique and synergistic adverse effects for each indi-vidual combination of rifampicin and anti-HIV drugsand consultation with a physician with experiencein treating both TB and HIV is advised40 IDSA-recommended dosage adjustment for patients receivingantiretrovirals and rifabutin37 can be obtained viathe lsquolink pagersquo (httpwwwaiccuhkeduhkweb8Pneumonia20guidelineshtm) The optimal time forinitiating antiretroviral therapy in patients with TB iscontroversial Early therapy may decrease HIV disease
progression but may be associated with a high inci-dence of adverse effects and an immune reconstitutionreaction37
CMV PNEUMONITIS4142
Risk of infection is highest following allogeneic stemcell transplantation followed by lung transplantationpancreas transplantation and then liver heart and renaltransplantation and advanced AIDS If both the recipi-ent and the donor are seronegative then the risk of bothinfection and disease are negligible If the recipient is
seropositive the risk of infection is approximately 70but the risk of disease is only 20 regardless of theserostatus of the donor However if the recipient isseronegative and the donor is seropositive the risk ofdisease is 70 If steroid pulses and antilymphocyteglobulin are given for treatment of acute rejection therisk of developing disease is markedly increased Infec-tion may be the result of primary infection or reactiva-tion of latent infection It is clinically important butoften difcult to distinguish between CMV infectionand CMV disease and a denitive diagnosis can bemade only histologically Detection of CMV-pp65antigen in peripheral WBC and detection of CMV DNA
or RNA in the blood by quantitative polymerase chain
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1417
Parapneumonic effusion 427
needle aspiration or if there is debris within the uiddrainage using an intercostal drain The diagnosis isconrmed by aspiration of pus
TREATMENT The mainstay of treatment is drainage either by inter-costal drain or by surgical intervention Patients whopresent before the pus is loculated and a brinous peelhas formed on the lung can usually be treated bysimple drainage The combination with intrapleuralbrinolysis may be benecial Optimal surgical man-agement which consists of decortication (open or tho-racoscopic) is indicated if the empyema is moreadvanced or if simple drainage fails This is a majorprocedure and many patients with cardiac or chronicrespiratory disease will not tolerate it Alternatives forthese patients are instillation of thrombolytics into thepleural space or thoracostomy Antibiotics have onlyan adjunctive role Broad-spectrum antibiotic regimenswith anaerobic cover should be used until the resultsof microbiological analysis of the aspirated pus areavailable
AcknowledgementsAll tables and gures are reproduced from ICU web(wwwaiccuhkeduhkweb8) with permission of theauthors
80ndash90 in patients with leukaemia or bone marrowtransplant recipients Bronchoalveolar lavage withsmear culture and antigen detection has excellent spe-cicity and reasonably good positive predictive valuefor invasive aspergillosis in immunocompromisedpatients Although radiological features may give a clueto the diagnosis they are not sufciently specic to be
diagnosticIn acutely ill immunocompromised patients intrave-nous therapy should be initiated if there is suggestiveevidence of invasive aspergillosis while further investi-gations to conrm or refute the diagnosis are carriedout First-line therapy is voriconazole47 Echinocandinsand amphotericin are alternatives
PARAPNEUMONIC EFFUSION
This may be an uncomplicated effusion that resolveswith appropriate treatment of the underlying pneumo-nia or a complicated effusion that develops into an
empyema unless drained Complicated effusions tendto develop 7ndash14 days after initial uid formation Theyare characterised by increasing pleural uid volumecontinued fever and pleural uid of low pH (lt73) thatcontains a large number of neutrophils and may revealorganisms on Gram staining or culture An outline ofmanagement is given in Figure 365
EMPYEMA48
DEFINITION Collection of pus in the pleural space
AETIOLOGY Follows infection of the structures surrounding thepleural space including subdiaphragmatic structuresand chest trauma or may be associated with malig-nancy Anaerobic bacteria usually streptococci orGram-negative rods are responsible for 76 of cases
DIAGNOSIS The diagnosis is usually simple The patient is usuallyseptic and may have a productive cough and chest painThe chest X-ray may show features suggestive of apleural effusion and underlying consolidation but may
also show an abscess cavity with a uid level in whichcase CT scanning will be required to distinguishbetween an abscess and an empyema Ultrasound canbe useful to conrm the presence of uid in the pleuralspace and to determine whether it can be drained by
Figure 365 An approach to the management of
parapneumonic effusions
Parapneumonic effusion
gt 1 cm thick
on lateral decubitus
film
Pleural aspirate
turbid or purulent or
Gram stain +ve
Pleural aspirate
pH
Serial thoracocentesis Treat as empyemaObserve
No
gt72 lt70
70ndash72
No
Yes
Yes
httpwwwexpertconsultcomAccess the complete references list online at
1 American Thoracic Society and Infectious Diseases Society of America Guidelines for the manage-ment of adults with hospital-acquired ventilator-associated and healthcare associated pneumonia
Am J Respir Crit Care Med 2005171388ndash416
2 Mandell LA Wunderink RG Anzueto A et al Infec-tious Diseases Society of AmericaAmerican Tho-racic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin
Infect Dis 200744S27ndash72
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1517
428 Pneumonia
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1617
References 428e1
REFERENCES 1 American Thoracic Society and Infectious Diseases
Society of America Guidelines for the management of adults with hospital-acquired ventilator-associated and healthcare associated pneumonia Am J Respir Crit Care Med 2005171388ndash416
2 Mandell LA Wunderink RG Anzueto A et al Infec-tious Diseases Society of AmericaAmerican Tho-racic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744S27ndash72
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
4 Woodhead M Blasi F Ewig S et al Guidelines for the management of adult lower respiratory tract infections Eur Respir J 2005261138ndash80
5 Torres A Rello J Update in community-acquired and nosocomial pneumonia 2009 Am J Respir Crit
Care Med 2010181782ndash76 Van der Eerden MM Vlaspolder F de Graaff CS et
al Value of intensive diagnostic microbiological investigation in low- and high-risk patients with community-acquired pneumonia Eur J Clin Micro Infect Dis 200524241ndash9
7 Murdoch DR Nucleic acid amplication tests for the diagnosis of pneumonia Clin Infect Dis 2003361162ndash70
8 Blaschke AJ Interpreting assays for the detection of Streptococcus pneumonia Clin Infect Dis 201152(S4)S331ndash7
9 Rello J Lisboa T Lujan M Severity of pneumococcal
pneumonia associated with genomic bacterial load Chest 2009136832ndash4010 Azoulay E Bergeron A Polymerase chain reaction
for diagnosing pneumocystis pneumonia in non-HIV immunocompromised patients with pulmonary inl-trates Chest 2009135(3)655
11 Garcia-Vidal C Fernandez-Sabe N Carratala J Early mortality in patients with community-acquired pneumonia causes and risk factors Eur Respir J200832733ndash9
12 Dellinger RP Carlet JM Masur H et al Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock Intensive Care Med200430536ndash55
13 Metersky ML Ma A Houck PM et al Antibiotics for bacteremic pneumonia improved outcomes with macrolides but not uoroquinolones Chest 2007131466ndash73
14 Dunbar LM Wunderink RG Habib MP High-dose short-course levooxacin for community-acquired pneumonia a new treatment paradigm Clin Infect Dis 200337752ndash60
15 Matthaiou DK Ntani G An ESICM systematic review and meta-analysis of procalcitonin-guided antibiotic therapy algorithms in adult critically ill patients Intensive Care Med 201238940ndash9
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
17 Gruber PC Gomersall CD Joynt GM Avian inu-enza (H5N1) implications for intensive care Inten-sive Care Med 200632823ndash9
18 Belongia EA Irving SA Clinical characteristics and 30-day outcomes for inuenza A 2009 (H1N1) 2008ndash2009 (H1N1) and 2007ndash8 (H3N2) infections JAMA2010304(10)1091
19 Lee N Chan PKS Complications and outcomes of pandemic 2009 inuenza A (H1N1) virus infection in hospitalized adults how do they differ from those in seasonal inuenza J Infect Dis 20112031739ndash47
20 Kim SH Hong SB Corticosteroid treatment in critically ill patients with pandemic inuenza AH1N1 2009 infection analytic strategy using pro-pensity scores Am J Respir Crit Care Med 20111831207ndash14
21 Centers for Disease Control and Prevention (CDC) Bacterial coinfections in lung tissue specimens from
fatal cases of 2009 pandemic inuenza A (H1N1) ndash United States MayndashAugust 2009 MMWR 2009581071ndash4
22 Safdar N Dezfulian C Clinical and economic conse-quences of ventilator-associated pneumonia A sys-tematic review Crit Care Med 200533(10)2184ndash93
23 Shorr AF Sherner JH Invasive approaches to the diagnosis of ventilator-associated pneumonia A meta-analysis Crit Care Med 200533(1)46ndash53
24 Melsen WG Rovers MM Ventilator-associated pneumonia and mortality A systematic review of observational studies Crit Care Med 2009372709ndash18
25 Bekaert M Timsit JF Attributable mortality of ventilator-associated pneumonia A reappraisal using causal analysis Am J Respir Crit Care Med20111841133ndash9
26 CDC Healthcare Infection Control Practices AdvisoryCommittee Guidelines for preventing health-care-associated pneumonia 2003 Recommendations ofCDC and the Healthcare Infection Control PracticesAdvisory Committee Online Available httpwwwcdcgovmmwrpreviewmmwrhtmlrr5303a1htm
27 Cofn SE Klompas M SHEAIDSA practice recom-mendation strategies to prevent ventilator-associated pneumonia in acute care hospitals Infect Control
Hosp Epidemiol 200829S31ndash4028 Masterton RG Galloway A Guidelines for the man-
agement of hospital-acquired pneumonia in the UK Report of the Working Party on Hospital-Acquired Pneumonia of the British Society for Antimicrobial Chemotherapy J Antimicrob Chemother 2008625ndash34
29 VAP Guidelines Committee and the Canadian Critical Care Trials Group Comprehensive evidence-based clinical practice guidelines for ventilator-associated pneumonia prevention J Crit Care 200823126ndash37
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1717
428e2 Pneumonia
30 Torres A Ewig S Dening treating and preventing hospital acquired pneumonia European perspective Intensive Care Med 2009359ndash29
31 Frame RN Johnson MC Eichenhorn MS et al Active tuberculosis in the medical intensive care unit a 15-year retrospective analysis Crit Care Med 1987151012ndash14
32 National Collaborating Centre for Chronic Condi-tions Tuberculosis Clinical diagnosis and manage-ment of tuberculosis and measures for its prevention and control London Royal College of Physicians 2006
33 Small PM Fujiwara PI Management of tuberculosis in the United States N Engl J Med 2001345189ndash200
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
35 Centers for Disease Control and Prevention Guide-lines for preventing the transmission of Mycobacte-rium tuberculosis in health-care settings 2005 MMWR
2005541ndash11936 Hilbert G Gruson D Vargas F et al Noninvasive
ventilation in immunosuppressed patients with pul-monary inltrates fever and acute respiratory failure N Engl J Med 2001344481ndash7
37 Benson CA Kaplan JE Masur H Treating oppor-tunistic infections among HIV-infected adults and adolescents recommendations from CDC the National Institutes of Health and the HIV Medicine AssociationInfectious Diseases Society of America Clin Infect Dis 200540S131ndash235
38 Randall CJ Yarnold PR Schwartz DN et al Improve-ments in outcomes of acute respiratory failure for
patients with human immunodeciency virus-related Pneumocystis carinii pneumonia Am J Respir Crit Care Med 2000162393ndash8
39 Croda J Croda MG Neves A et al Benet of antiret-roviral therapy on survival of human immunode-ciency virus-infected patients admitted to an intensive care unit Crit Care Med 200937(5)1605
40 Centers for Disease Control Updated guidelines for the use of rifabutin or rifampicin for the treatment and prevention of tuberculosis among HIV-infected patients taking protease inhibitors or nonnucleoside reverse transcriptase inhibitors MMWR 200049185ndash9
41 Tamm M The lung in the immunocompromised patient Infectious complications part 2 Respiration199966199ndash207
42 Van der Bij W Speich R Management of cytomega-lovirus infection and disease after solid-organ trans-plantation Clin Infect Dis 200133(Suppl 1)S32ndash7
43 Schaumlfer P Tenschert W Cremaschi L et al Area under the viraemia curve versus absolute viral load utility for predicting symptomatic cytomegalovirus infections in kidney transplant patients J Med Virol20016585ndash9
44 Meyer-Koenig U Weidmann M Kirste G et al Cytomegalovirus infection in organ-transplant recip-ients diagnostic value of pp65 antigen test qualita-tive polymerase chain reaction (PCR) and quantitative
Taqman PCR Transplantation 2004771692ndash8
45 Pappas PG Rex JH Sobel JD Guidelines for treat-ment of candidiasis Clin Infect Dis 200438161ndash89
46 Stevens DA Kan VL Judson MA Practice guidelines for diseases caused by Aspergillus Clin Infect Dis200030696ndash709
47 Herbrecht R Denning DW Patterson TF Voricona-zole versus amphotericin B for primary therapy of invasive aspergillosis N Engl J Med 2002347408ndash15
48 Peek GJ Morcos S Cooper G The pleural cavity BMJ20003201318ndash21
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6

7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 817
Healthcare-associated pneumonia 421
inltrate in 48 hours new cavitation or a signicantnew pleural effusion should raise concern If the patientfails to respond consider the diagnosis host factors (egimmunosuppressed debilitated) bacterial factors (egvirulent organism) and therapeutic factors (eg wrongdrug inadequate dose) Review the antibiotics andrepeat cultures It may be useful to broaden the antimi-crobial cover while waiting for the results of investiga-tions Consider invasive sampling of respiratorysecretions computerised tomography or ultrasound ofthe chest (to look for an empyema or abscess) anothersource of infection open-lung biopsy to establish diag-nosis and aetiology or administration of steroids
MORTALITY AND MORBIDITY ATTRIBUTABLE TO VAP Substantial morbidity and mortality associated withVAP have previously been reported22 However acausal relationship is difcult to establish It should benoted that patients who developed VAP tend to be
more severely ill and at higher risk of death not onlyon ICU admission but throughout the course of theirillness Most of the relevant studies were observationaland failed to adequately control confounders likedisease severity evolution of disease progression andICU length of stay with mortality In addition signi-cant heterogeneity exists among these studies Althoughthe presence of VAP is associated with a signicantlylonger ICU length of stay (mean of 61 days 95 CI532ndash687) and increased healthcare cost22 more recentstudies reported that mortality attributable to VAPtends to be small if any2425 The attributable mortalityhas been reported to be 1 on the 30th day of ICU and
RESPONSE TO THERAPY Clinical improvement is usually not apparent for 48ndash72hours and therapy should not be changed during thistime The CXR is of limited value for assessing responseinitial deterioration is common and improvement oftenlags behind clinical response However a rapidly dete-riorating CXR pattern with a gt50 increase in size of
Figure 363 Subsequent management of nosocomialpneumonia based on a non-invasive clinical approach1
Pathogens isolated
from respiratory
specimen
Antibiotics
changedstarted in 7 h
prior to sampling
Adjust antibiotics
according to sensitivities
Continue antibiotics if
high clinical suspicion of
nosocomial pneumonia
Bacterial pneumonia
unlikely
Investigate for other cause
of sepsis and CXR changes
Consider unusual causes
of nosocomial pneumonia
(eg Legionella viruses fungi
Pneumocystis carinii )
Yes
Yes
No
No
Table 363 Recommended initial empirical treatment for nosocomial pneumonia1
SITUATION ANTIBIOTICS
No risk factors for multidrug-resistant pathogens Ceftriaxone or Levofloxacin moxifloxacin or ciprofloxacin or Ampicillinsulbactam or Ertapenem
Antimicrobial therapy in previous 90 days or Current hospitalization for ge5 days or High frequency of antibiotic resistance in the specific
hospital unit or Hospitalisation for 2 days or more in previous 90 days or Residence in nursing home or extended care facility or Home infusion therapy (including antibiotics) or Chronic dialysis within 30 days or Home wound care or Family member with multidrug-resistant pathogen o rImmunosuppression or Bronchiectasis
One ofAntipseudomonal cephalosporin (cefepime or ceftazidime) or Antipseudomonal carbapenem (meropenem or imipenemndash
cilastin) or szlig-lactamszlig-lactamase inhibitor (eg piperacillinndashtazobactam or
cefaperazonendashsulbactam)plus one ofAminoglycoside or Antipseudomonal quinolone (levofloxacin or ciprofloxacin)plus one of the following for patients at high risk of meticillin-
resistant Staphylococcus aureus (MRSA) infectionLinezolid or Vancomycin or
TeicoplaninThe use of dual therapy is not well supported by evidence but it does reduce the probability that the pathogen is resistant to the drugsbeing given If an extended spectrum β-lactamase-producing strain or an Acinetobacter sp is suspected a carbapenem should be givenIf Legionella pneumophilia is suspected use a quinolone Risk factors for MRSA infection in areas with a high incidence of MRSA includediabetes mellitus head trauma coma and renal failure
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 917
422 Pneumonia
or with enlarged cervical nodes or other manifestationsof extrapulmonary disease Clinical disease is seldomfound in asymptomatic individuals even those withstrongly positive tuberculin test (Heaf grade III or IV)The outlook for patients with tuberculosis who requireICU admission is poor In one retrospective study thein-hospital mortality for all patients with tuberculosisrequiring ICU admission was 67 but in those withacute respiratory failure it rose to 8131 The presenta-tion and management of TB in HIV-positive patientsare different (see below)
INVESTIGATION OF PULMONARYTUBERCULOSIS
IDENTIFICATION OF MYCOBACTERIA
Multiple
3233
sputum samples should be collected pref-erably on different days for microscopy for acid-fastbacilli and culture If sputum is not available bronchialwashings taken at bronchoscopy and gastric lavage oraspirate samples should be obtained Gastric aspiratesneed to be neutralised immediately on collection Bron-choscopy and transbronchial biopsy may be useful inpatients with suspected TB but negative sputum smearPleural biopsy is often helpful and mediastinoscopyis occasionally needed in patients with mediastinallymphadenopathy Part of any biopsy specimen shouldalways be sent for culture Nucleic acid amplicationtests on sputum have sensitivity similar to culture in
15 on the 60th day of ICU in a recent study using amulticentre high-quality database and incorporatingnovel statistical methodology to control evolution ofseverity of illness25
PREVENTION
Several guidelines for prevention of ventilator-associated pneumonia and hospital-acquired pneumo-nia have been published26ndash30 Interventions can bedivided into general infection control measures andspecic measures General measures include alcohol-based hand disinfection hospital education programmeon infection control the use of microbiological sur-veillance and a programme to reduce antibiotic pre-scription The major specic recommendations aresummarised in Table 364 There is no evidence that
lsquobundlesrsquo of recommendations are more effective thanthe sum of the individual components
TUBERCULOSIS
The main risk factors are listed in Box 362 Typicalclinical features include fever sweating weight losslassitude anorexia cough productive of mucoid orpurulent sputum haemoptysis chest wall pain dysp-noea localised wheeze and apical crackles Patientsmay also present with unresolved pneumonia pleuraleffusions spontaneous pneumothorax and hoarseness
Figure 364 Management of suspected nosocomial pneumonia based on invasive sampling of respiratory secretions
Bacteria onGram stain
Yes
Yes
No
Yes No Yes No
No
Start antibiotics immediatelyusing PSBBAL specimen
and Gram stain results
Start antibioticsimmediately based onepidemiological clues
Observe look forother infection
Signs ofsevere sepsis
Immediate PSB or BAL beforechangingstarting antimicrobial therapy
+ve cultures +ve cultures
Adjust therapybased on
culture results
Continueadjustantibiotics Look for
other infection
Start antibioticson basisof results
Look forother infection
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1017
Tuberculosis 423
Table 364 Strategies for prevention of ventilator-associated pneumonia
LEVELS OF
RECOMMENDATIONS SPECIFIC INTERVENTIONS REMARKS
Universally recommendedby all guidelines27ndash30
1 Semirecumbent position to 45deg At least 30ndash45deg2 Avoidance of endotracheal intubation3 Preference of oral tracheal route
4 New circuit for a new patient and noschedule change unless soiled or damaged5 Avoidance of flushing of condensate into
lower airway or in-line medication6 HME changes no more frequently than 5ndash7
days7 Continuous aspiration of subglottic suctioning For patients expected to require mechanical
ventilation for gt72 hours
Generally recommendedby most guidelines
1 Preferential use of non-invasiveventilation272830
2 Avoidance of unplanned re-intubation272830
3 Maintenance of endotracheal cuff pressureof about 20 mmHg (266 kPa)272830
4 Closed suctioning2829
No effect on VAP mainly for staff safety5 Chlorhexidine oral decontamination272930
6 Sedation vacation and weaning protocol2728
7 Judicious use of stress ulcer prophylaxis272830
8 Restrictive blood transfusion28
Benefits less clear 1 Preference of HME over heatedhumidifier2830
HME associated with reduction in VAP inpatients ventilated for gt7 days lower cost
2 Silver-sulfadiazine-coated endotrachealtube272830
3 Early tracheostomy (within 7 days ofmechanical ventilation)29
4 Selective decontamination of digestive tract(SDD)272830
Mortality reduction demonstrated when topicalantimicrobials combined with short-course
systemic antibiotics BSAC recommendedSDD in patients expected to requiremechanical ventilation for gt48 hours ETFdiscourage routine use due to concern ofemergence of resistant organisms
Not yet reviewed byguidelines50
1 High-volume low-pressure ultrathin membraneendotracheal tube cuff with SSD
2 Ultrathin membrane cuff with tapered shapeand SSD
3 Low-volume low-pressure endotracheal tubecuff with SSD
4 Balloon device for biofilm removal5 Saline instillation before tracheal suctioning
HME= heat moist exchanger SSD= subglottic secretion drainage
smear-negative patients with pulmonary tuberculosisbut have the advantage of a much more rapid resultThere is however a signicant false-negative rate32
CHEST X-RAY (CXR)A normal CXR almost excludes TB (except inHIV-infected patients) but endobronchial lesionsmay not be apparent and early apical lesions can bemissed Common appearances include patchynodular
shadowing in the upper zones (often bilateral) cavita-tion calcication hilar or mediastinal lymphadenopa-thy (may cause segmental or lobar collapse) pleuraleffusion tuberculomas (dense round or oval shadows)and diffuse ne nodular shadowing throughout thelung elds in miliary TB Inactivity of disease cannot beinferred from the CXR alone This requires three nega-tive sputum samples and failure of any lesion seen onCXR to progress CXR appearances in HIV-positive
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1117
424 Pneumonia
t-tested negative-pressure respirator (N95 FFP2 orhigher) Use of a powered air-purifying respiratorshould be considered when bronchoscopy is being per-formed35 Detailed infection control advice can beobtained via the lsquolink pagersquo (httpwwwaiccuhk eduhkweb8Pneumonia20guidelineshtm)
PNEUMONIA IN THEIMMUNOCOMPROMISED
The lungs are amongst the most frequent targetorgans for infectious complications in the immuno-compromised The incidence of pneumonia is highestamongst patients with haematological malignanciesbone marrow transplant (BMT) recipients and patientswith AIDS
The speed of progression of pneumonia the CXRchanges (Table 365) and the type of immune defectprovide clues to the aetiology Bacterial pneumonias
progress rapidly (1ndash2 days) whereas fungal and proto-zoal pneumonias are less fulminant (several days to aweek or more) Viral pneumonias are usually not ful-minant but on occasions may develop quite rapidlyBronchoscopy is a major component of the investiga-tion of these patients Empirical management based onCXR appearances is outlined in Table 365 Early non-invasive ventilation may improve outcome amongstimmunocompromised patients with fever and bilateralinltrates36
PNEUMOCYSTIS JIROVECI PNEUMONIA (PCP)37
The incidence of this common opportunistic infectionhas fallen substantially in patients with AIDS whoare receiving prophylaxis and effective antiretroviraltherapy with most cases occurring in patients who arenot receiving HIV care or among patients with advancedimmunosuppression The onset is usually insidiouswith dry cough dyspnoea and fever on a backgroundof fatigue and weight loss Crackles in the chest are rareApproximately 15 of patients have a concurrent causefor respiratory failure (eg Kaposi sarcoma TB bacte-rial pneumonia) Useful investigations are
1 CXR classical appearance is diffuse bilateral perihi-
lar interstitial shadowing but in the early stages thisis very subtle and easily missed The initial CXR isnormal in 10 In a further 10 the changes areatypical with focal consolidation or coarse patchyshadowing None of the changes are specic for PCPand may be seen in other lung diseases associatedwith AIDS Pleural effusions hilar or mediastinallymphadenopathy are unusual in PCP but commonin mycobacterial infection or Kaposirsquos sarcoma orlymphoma
2 Induced sputum in this technique the patient inhalesnebulised hypertonic saline from an ultrasonic neb-uliser This provokes bronchorrhoea and the patient
patients with TB differ from those in non-HIV-infectedpatients
TREATMENT OF PULMONARY TB32ndash34
The decision to initiate anti-TB treatment should bebased on level of clinical suspicion results of AFBsmear and sometimes mycobacterial culture If the
initial clinical suspicion is strong and the patient is seri-ously ill attributable to possible TB treatment shouldbe initiated promptly sometimes before the result ofAFB smear Subsequent positivity of AFB smear ornucleic acid amplication test provides support to thecontinuation of treatment Combination chemotherapyconsisting of four drugs is necessary for maximal ef-cacy Treatment is divided into initial phase and con-tinuation phase The most commonly used initialregimen consists of 8 weeks of rifampicin 600 mg daily(450 mg for patients lt50 kg) isoniazid 300 mg dailypyrazinamide 2 g daily (15 g for patients lt50 kg) and
ethambutol 15 mgkg daily as initial phase treatmentEthambutol should be used only in patients who havereasonable visual acuity and who are able to appreciateand report visual disturbances This mandates carefulconsideration in patients who require heavy sedationVisual acuity and colour perception must be assessed(if ethambutol is to be used) and liver and renal func-tion checked before treatment is started Steroids arerecommended for children with endobronchial diseaseand possibly for patients with tuberculous pleuraleffusions Pyridoxine 10 mg daily should be given toprevent isoniazid-induced neuropathy to those atincreased risk (eg patients with diabetes mellitus
chronic renal failure or malnutrition or alcoholic orHIV-positive patients) Negative AFB smear should notdelay initial treatment if clinical suspicion remainshigh Supporting features included chronic coughweight loss characteristic chest X-ray ndings emigra-tion from a high-incidence country no other immediatediagnosis and positive tuberculin test
INFECTION CONTROL
Patients admitted to an ICU with infectious TB or sus-pected of having active pulmonary TB should bemanaged in an isolation room with special ventilation
characteristics including negative pressure Patientsshould be considered infectious if they are coughing orundergoing cough-inducing procedures or if they havepositive AFB smears and they are not on or have juststarted chemotherapy or have a poor clinical or bacte-riological response to chemotherapy3235 Patients withnon-drug-resistant TB should be non-infectious after 2weeks of treatment which includes rifampicin and iso-niazid32 As TB spreads through aerosols it is probablyappropriate to isolate patients who are intubated evenif only their bronchial washings are smear-positiveStaff caring for patients who are smear-positive shouldwear personal protective equipment including a
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1217
Pneumonia in the immunocompromised 425
andor diuretics (patients often uid-overloaded)Approximately 40 of patients with HIV-related PCPwho require mechanical ventilation survive to hospitaldischarge38
Initiation of antiretroviral therapy in patients pre-senting with HIV-related PCP is controversial TheCenters for Disease Control and Prevention (CDC) rec-ommend against doing so in the acute phase but recent
data suggest that the outcome may be improved byinitiation within the rst 4 days of ICU admission39
BACTERIAL PNEUMONIA37
This is the most common cause of acute respiratoryfailure in HIV-positive patients Bacterial pneumonia ismore common in HIV-infected patients than in thegeneral population and tends to be more severe Strep pneumoniae H infuenza Pseudomonas aeruginosa and Saureus are the commonest organisms Nocardia andGram negatives should also be considered Atypicalpathogens (eg Legionella) are rare Response to appro-
priate antibiotics is usually good but may require pro-tracted courses of antibiotics because of high tendencyto relapse Patients with severe immunodeciency(CD4+ T lymphocyte count lt100983221L) and a history ofPseudomonas infection or bronchiectasis or neutropeniashould receive antibiotics that cover P aeruginosa aswell as other Gram negatives The possibility of concur-rent PCP or tuberculosis should be excluded
TUBERCULOSIS
TB may be the initial presentation of AIDS particularlyin sub-Saharan Africa The pattern of TB in HIV patients
coughs up material containing cysts and tropho-zoites The technique is time-consuming and requiresmeticulous technique and is less sensitive thanbronchoscopy but less invasive The possibility ofconcurrent tuberculosis should be consideredand steps taken to minimise the risk of spread ofinfection
3 Bronchoscopy with bronchoalveolar lavage leads to
the diagnosis in over 90 of cases Specimens shouldbe sent for cytology Transbronchial biopsy is notnecessary in most cases PCR using bronchial lavagespecimens may be useful in non-HIV patients withsuspected PCP
Antipneumocystis treatment should be started as soonas the diagnosis is suspected Treatment of choice istrimethoprim plus sulfamethoxazole (co-trimoxazole)20 mgkgday+ 100 mgkgday for 3 weeks plusprednisolone 40 mg orally twice daily for 5 days fol-lowed by 20 mg twice daily for 5 days and then 20 mgper day until the end of PCP treatment Side-effects of
co-trimoxazole are common in HIV patients (nauseavomiting skin rash myelotoxicity) The dose should bereduced by 25 if the WBC count falls Patients whoare intolerant of co-trimoxazole should be treated with
bull pentamidine 4 mgkgday iv or
bull primaquine with clindamycin or
bull trimetrexate with leucovorin (plusmnoral dapsone)
Response to treatment is usually excellent with aresponse time of 4ndash7 days If the patient deteriorates orfails to improve consider (re-)bronchoscopy (is thediagnosis correct) treat co-pathogens and considera short course of high-dose iv methylprednisolone
Table 365 Causes of CXR changes and empirical treatment of pneumonia in the immunocompromised
CHEST X-RAY
APPEARANCE CAUSES
EMPIRICAL TREATMENT FOR
SUSPECTED PNEUMONIA
Diffuse infiltrate CMV and other herpes virusesPneumocystis carinii Bacteria
Aspergillus (advanced)Cryptococcus (uncommon)Non-infectious causes eg drug reaction non-specific
interstitial pneumonitis radiation pneumonitis(uncommon) malignancy leucoagglutinin reaction
Broad-spectrum antibiotics for at least 48 h(eg 3rd-generation cephalosporin andaminoglycoside)
Co-trimoxazoleLung biopsy or lavage within 48 h or full2-week course of co-trimoxazole (dependson patient tolerance of invasive procedure)
Focal infiltrate Gram-negative rodsS aureusAspergillusCryptococcusNocardiaMucorP carinii (uncommon)Tuberculosis
LegionellaNon-infectious causes (eg malignancy non-specificinterstitial pneumonitis radiation pneumonitis)
Broad-spectrum antibioticsIf response seen continue treatment for
2 weeksIf disease progresses lung biopsyaspirate
within 48ndash72 hours or empirical trial ofantifungalplusmn macrolide
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1317
426 Pneumonia
reaction are the most useful tests for demonstratingCMV disease Using thresholds of 10300 000ndash50200 000 positive circulating peripheral WBC the posi-tive predictive value for CMV-pp65 ranges from64 to 82 and the negative predictive value from70 to 954344 Treatment consists of intravenous gan-ciclovir for at least 14 days Foscarnet can be used if
ganciclovir fails
FUNGAL PNEUMONIA
Fungi are rare but important causes of pneumoniaThey can be divided into two main groups based on theimmune response required to combat infection withthese organisms Histoplasma blastomycosis coccidi-oidomycosis paracoccidioidomycosis and Cryptococcus require specic cell-mediated immunity for their controland thus in contrast to infections that are controlled byphagocytic activity the diseases caused by these organ-isms can occur in otherwise healthy individuals
although they cause much more severe illness inpatients with impaired cell-mediated immunity (egpatients infected with HIV and organ transplant recipi-ents) With the exception of Cryptococcus these organ-isms are rarely seen outside North America Aspergillus and Mucor spores are killed by non-immune phago-cytes and as a result these fungi rarely result in clinicalillness in patients with normal neutrophil numbers andfunction
CANDIDIASIS This is effectively a combination of the two types offungal infection in which impaired cell-mediatedimmunity predisposes to mucosal overgrowth withCandida but impaired phagocytic function or numbersis usually required before deep invasion of tissuesoccurs Primary Candida pneumonia (ie isolated lunginfection) is uncommon4145 and more commonly pul-monary lesions are only one manifestation of dissemi-nated candidiasis Even more common is benigncolonisation of the airway with Candida In mostreported cases of primary Candida pneumonia ampho-tericin B has been used In disseminated candidiasistreatment should be directed to treatment of dissemi-nated disease rather than Candida pneumonia per se45
INVASIVE ASPERGILLOSIS 46
This is a highly lethal condition in the immunocom-promised despite treatment and therefore investiga-tion and treatment should be prompt and aggressiveIt is associated with exposure to construction workDenitive diagnosis requires both histological evidenceof acute-angle branching septated non-pigmentedhyphae measuring 2ndash4 983221m in width and cultures yield-ing Aspergillus species from biopsy specimens ofinvolved organs Recovery of Aspergillus species fromrespiratory secretions in immunocompromised butnot immunocompetent patients may indicate invasive
disease with a positive predictive value as high as
depends on the degree of immunosuppression Inpatients with CD4+ T lymphocytes gt350 cells983221L theclinical presentation is similar to TB in non-HIV-infectedpatients although extrapulmonary disease is morecommon In patients with CD4+ T lymphocytes lt350cells983221L extrapulmonary disease (pleuritis pericardi-tis meningitis) is common Severely immunocompro-
mised patients (CD4+
T lymphocytes lt100 cells983221L)may present with severe systemic disease with highfever rapid progression and systemic sepsis In thesepatients lower and middle lobe disease is more commonmiliary disease is common and cavitation is lesscommon Sputum smears and culture may be positiveeven with a normal CXR
Response to treatment is usually rapid Managementof TB in HIV is complex owing to numerous druginteractions consultation with an expert in treatment ofHIV-related TB should be strongly considered Complexinteractions occur between rifamycins (eg rifampicinand rifabutin) and protease inhibitors and non-
nucleoside reverse transcriptase inhibitors used to treatpatients infected with HIV The choice of rifampicin orrifabutin depends on a number of factors includingthe unique and synergistic adverse effects for each indi-vidual combination of rifampicin and anti-HIV drugsand consultation with a physician with experiencein treating both TB and HIV is advised40 IDSA-recommended dosage adjustment for patients receivingantiretrovirals and rifabutin37 can be obtained viathe lsquolink pagersquo (httpwwwaiccuhkeduhkweb8Pneumonia20guidelineshtm) The optimal time forinitiating antiretroviral therapy in patients with TB iscontroversial Early therapy may decrease HIV disease
progression but may be associated with a high inci-dence of adverse effects and an immune reconstitutionreaction37
CMV PNEUMONITIS4142
Risk of infection is highest following allogeneic stemcell transplantation followed by lung transplantationpancreas transplantation and then liver heart and renaltransplantation and advanced AIDS If both the recipi-ent and the donor are seronegative then the risk of bothinfection and disease are negligible If the recipient is
seropositive the risk of infection is approximately 70but the risk of disease is only 20 regardless of theserostatus of the donor However if the recipient isseronegative and the donor is seropositive the risk ofdisease is 70 If steroid pulses and antilymphocyteglobulin are given for treatment of acute rejection therisk of developing disease is markedly increased Infec-tion may be the result of primary infection or reactiva-tion of latent infection It is clinically important butoften difcult to distinguish between CMV infectionand CMV disease and a denitive diagnosis can bemade only histologically Detection of CMV-pp65antigen in peripheral WBC and detection of CMV DNA
or RNA in the blood by quantitative polymerase chain
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1417
Parapneumonic effusion 427
needle aspiration or if there is debris within the uiddrainage using an intercostal drain The diagnosis isconrmed by aspiration of pus
TREATMENT The mainstay of treatment is drainage either by inter-costal drain or by surgical intervention Patients whopresent before the pus is loculated and a brinous peelhas formed on the lung can usually be treated bysimple drainage The combination with intrapleuralbrinolysis may be benecial Optimal surgical man-agement which consists of decortication (open or tho-racoscopic) is indicated if the empyema is moreadvanced or if simple drainage fails This is a majorprocedure and many patients with cardiac or chronicrespiratory disease will not tolerate it Alternatives forthese patients are instillation of thrombolytics into thepleural space or thoracostomy Antibiotics have onlyan adjunctive role Broad-spectrum antibiotic regimenswith anaerobic cover should be used until the resultsof microbiological analysis of the aspirated pus areavailable
AcknowledgementsAll tables and gures are reproduced from ICU web(wwwaiccuhkeduhkweb8) with permission of theauthors
80ndash90 in patients with leukaemia or bone marrowtransplant recipients Bronchoalveolar lavage withsmear culture and antigen detection has excellent spe-cicity and reasonably good positive predictive valuefor invasive aspergillosis in immunocompromisedpatients Although radiological features may give a clueto the diagnosis they are not sufciently specic to be
diagnosticIn acutely ill immunocompromised patients intrave-nous therapy should be initiated if there is suggestiveevidence of invasive aspergillosis while further investi-gations to conrm or refute the diagnosis are carriedout First-line therapy is voriconazole47 Echinocandinsand amphotericin are alternatives
PARAPNEUMONIC EFFUSION
This may be an uncomplicated effusion that resolveswith appropriate treatment of the underlying pneumo-nia or a complicated effusion that develops into an
empyema unless drained Complicated effusions tendto develop 7ndash14 days after initial uid formation Theyare characterised by increasing pleural uid volumecontinued fever and pleural uid of low pH (lt73) thatcontains a large number of neutrophils and may revealorganisms on Gram staining or culture An outline ofmanagement is given in Figure 365
EMPYEMA48
DEFINITION Collection of pus in the pleural space
AETIOLOGY Follows infection of the structures surrounding thepleural space including subdiaphragmatic structuresand chest trauma or may be associated with malig-nancy Anaerobic bacteria usually streptococci orGram-negative rods are responsible for 76 of cases
DIAGNOSIS The diagnosis is usually simple The patient is usuallyseptic and may have a productive cough and chest painThe chest X-ray may show features suggestive of apleural effusion and underlying consolidation but may
also show an abscess cavity with a uid level in whichcase CT scanning will be required to distinguishbetween an abscess and an empyema Ultrasound canbe useful to conrm the presence of uid in the pleuralspace and to determine whether it can be drained by
Figure 365 An approach to the management of
parapneumonic effusions
Parapneumonic effusion
gt 1 cm thick
on lateral decubitus
film
Pleural aspirate
turbid or purulent or
Gram stain +ve
Pleural aspirate
pH
Serial thoracocentesis Treat as empyemaObserve
No
gt72 lt70
70ndash72
No
Yes
Yes
httpwwwexpertconsultcomAccess the complete references list online at
1 American Thoracic Society and Infectious Diseases Society of America Guidelines for the manage-ment of adults with hospital-acquired ventilator-associated and healthcare associated pneumonia
Am J Respir Crit Care Med 2005171388ndash416
2 Mandell LA Wunderink RG Anzueto A et al Infec-tious Diseases Society of AmericaAmerican Tho-racic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin
Infect Dis 200744S27ndash72
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1517
428 Pneumonia
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1617
References 428e1
REFERENCES 1 American Thoracic Society and Infectious Diseases
Society of America Guidelines for the management of adults with hospital-acquired ventilator-associated and healthcare associated pneumonia Am J Respir Crit Care Med 2005171388ndash416
2 Mandell LA Wunderink RG Anzueto A et al Infec-tious Diseases Society of AmericaAmerican Tho-racic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744S27ndash72
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
4 Woodhead M Blasi F Ewig S et al Guidelines for the management of adult lower respiratory tract infections Eur Respir J 2005261138ndash80
5 Torres A Rello J Update in community-acquired and nosocomial pneumonia 2009 Am J Respir Crit
Care Med 2010181782ndash76 Van der Eerden MM Vlaspolder F de Graaff CS et
al Value of intensive diagnostic microbiological investigation in low- and high-risk patients with community-acquired pneumonia Eur J Clin Micro Infect Dis 200524241ndash9
7 Murdoch DR Nucleic acid amplication tests for the diagnosis of pneumonia Clin Infect Dis 2003361162ndash70
8 Blaschke AJ Interpreting assays for the detection of Streptococcus pneumonia Clin Infect Dis 201152(S4)S331ndash7
9 Rello J Lisboa T Lujan M Severity of pneumococcal
pneumonia associated with genomic bacterial load Chest 2009136832ndash4010 Azoulay E Bergeron A Polymerase chain reaction
for diagnosing pneumocystis pneumonia in non-HIV immunocompromised patients with pulmonary inl-trates Chest 2009135(3)655
11 Garcia-Vidal C Fernandez-Sabe N Carratala J Early mortality in patients with community-acquired pneumonia causes and risk factors Eur Respir J200832733ndash9
12 Dellinger RP Carlet JM Masur H et al Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock Intensive Care Med200430536ndash55
13 Metersky ML Ma A Houck PM et al Antibiotics for bacteremic pneumonia improved outcomes with macrolides but not uoroquinolones Chest 2007131466ndash73
14 Dunbar LM Wunderink RG Habib MP High-dose short-course levooxacin for community-acquired pneumonia a new treatment paradigm Clin Infect Dis 200337752ndash60
15 Matthaiou DK Ntani G An ESICM systematic review and meta-analysis of procalcitonin-guided antibiotic therapy algorithms in adult critically ill patients Intensive Care Med 201238940ndash9
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
17 Gruber PC Gomersall CD Joynt GM Avian inu-enza (H5N1) implications for intensive care Inten-sive Care Med 200632823ndash9
18 Belongia EA Irving SA Clinical characteristics and 30-day outcomes for inuenza A 2009 (H1N1) 2008ndash2009 (H1N1) and 2007ndash8 (H3N2) infections JAMA2010304(10)1091
19 Lee N Chan PKS Complications and outcomes of pandemic 2009 inuenza A (H1N1) virus infection in hospitalized adults how do they differ from those in seasonal inuenza J Infect Dis 20112031739ndash47
20 Kim SH Hong SB Corticosteroid treatment in critically ill patients with pandemic inuenza AH1N1 2009 infection analytic strategy using pro-pensity scores Am J Respir Crit Care Med 20111831207ndash14
21 Centers for Disease Control and Prevention (CDC) Bacterial coinfections in lung tissue specimens from
fatal cases of 2009 pandemic inuenza A (H1N1) ndash United States MayndashAugust 2009 MMWR 2009581071ndash4
22 Safdar N Dezfulian C Clinical and economic conse-quences of ventilator-associated pneumonia A sys-tematic review Crit Care Med 200533(10)2184ndash93
23 Shorr AF Sherner JH Invasive approaches to the diagnosis of ventilator-associated pneumonia A meta-analysis Crit Care Med 200533(1)46ndash53
24 Melsen WG Rovers MM Ventilator-associated pneumonia and mortality A systematic review of observational studies Crit Care Med 2009372709ndash18
25 Bekaert M Timsit JF Attributable mortality of ventilator-associated pneumonia A reappraisal using causal analysis Am J Respir Crit Care Med20111841133ndash9
26 CDC Healthcare Infection Control Practices AdvisoryCommittee Guidelines for preventing health-care-associated pneumonia 2003 Recommendations ofCDC and the Healthcare Infection Control PracticesAdvisory Committee Online Available httpwwwcdcgovmmwrpreviewmmwrhtmlrr5303a1htm
27 Cofn SE Klompas M SHEAIDSA practice recom-mendation strategies to prevent ventilator-associated pneumonia in acute care hospitals Infect Control
Hosp Epidemiol 200829S31ndash4028 Masterton RG Galloway A Guidelines for the man-
agement of hospital-acquired pneumonia in the UK Report of the Working Party on Hospital-Acquired Pneumonia of the British Society for Antimicrobial Chemotherapy J Antimicrob Chemother 2008625ndash34
29 VAP Guidelines Committee and the Canadian Critical Care Trials Group Comprehensive evidence-based clinical practice guidelines for ventilator-associated pneumonia prevention J Crit Care 200823126ndash37
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1717
428e2 Pneumonia
30 Torres A Ewig S Dening treating and preventing hospital acquired pneumonia European perspective Intensive Care Med 2009359ndash29
31 Frame RN Johnson MC Eichenhorn MS et al Active tuberculosis in the medical intensive care unit a 15-year retrospective analysis Crit Care Med 1987151012ndash14
32 National Collaborating Centre for Chronic Condi-tions Tuberculosis Clinical diagnosis and manage-ment of tuberculosis and measures for its prevention and control London Royal College of Physicians 2006
33 Small PM Fujiwara PI Management of tuberculosis in the United States N Engl J Med 2001345189ndash200
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
35 Centers for Disease Control and Prevention Guide-lines for preventing the transmission of Mycobacte-rium tuberculosis in health-care settings 2005 MMWR
2005541ndash11936 Hilbert G Gruson D Vargas F et al Noninvasive
ventilation in immunosuppressed patients with pul-monary inltrates fever and acute respiratory failure N Engl J Med 2001344481ndash7
37 Benson CA Kaplan JE Masur H Treating oppor-tunistic infections among HIV-infected adults and adolescents recommendations from CDC the National Institutes of Health and the HIV Medicine AssociationInfectious Diseases Society of America Clin Infect Dis 200540S131ndash235
38 Randall CJ Yarnold PR Schwartz DN et al Improve-ments in outcomes of acute respiratory failure for
patients with human immunodeciency virus-related Pneumocystis carinii pneumonia Am J Respir Crit Care Med 2000162393ndash8
39 Croda J Croda MG Neves A et al Benet of antiret-roviral therapy on survival of human immunode-ciency virus-infected patients admitted to an intensive care unit Crit Care Med 200937(5)1605
40 Centers for Disease Control Updated guidelines for the use of rifabutin or rifampicin for the treatment and prevention of tuberculosis among HIV-infected patients taking protease inhibitors or nonnucleoside reverse transcriptase inhibitors MMWR 200049185ndash9
41 Tamm M The lung in the immunocompromised patient Infectious complications part 2 Respiration199966199ndash207
42 Van der Bij W Speich R Management of cytomega-lovirus infection and disease after solid-organ trans-plantation Clin Infect Dis 200133(Suppl 1)S32ndash7
43 Schaumlfer P Tenschert W Cremaschi L et al Area under the viraemia curve versus absolute viral load utility for predicting symptomatic cytomegalovirus infections in kidney transplant patients J Med Virol20016585ndash9
44 Meyer-Koenig U Weidmann M Kirste G et al Cytomegalovirus infection in organ-transplant recip-ients diagnostic value of pp65 antigen test qualita-tive polymerase chain reaction (PCR) and quantitative
Taqman PCR Transplantation 2004771692ndash8
45 Pappas PG Rex JH Sobel JD Guidelines for treat-ment of candidiasis Clin Infect Dis 200438161ndash89
46 Stevens DA Kan VL Judson MA Practice guidelines for diseases caused by Aspergillus Clin Infect Dis200030696ndash709
47 Herbrecht R Denning DW Patterson TF Voricona-zole versus amphotericin B for primary therapy of invasive aspergillosis N Engl J Med 2002347408ndash15
48 Peek GJ Morcos S Cooper G The pleural cavity BMJ20003201318ndash21
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6

7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 917
422 Pneumonia
or with enlarged cervical nodes or other manifestationsof extrapulmonary disease Clinical disease is seldomfound in asymptomatic individuals even those withstrongly positive tuberculin test (Heaf grade III or IV)The outlook for patients with tuberculosis who requireICU admission is poor In one retrospective study thein-hospital mortality for all patients with tuberculosisrequiring ICU admission was 67 but in those withacute respiratory failure it rose to 8131 The presenta-tion and management of TB in HIV-positive patientsare different (see below)
INVESTIGATION OF PULMONARYTUBERCULOSIS
IDENTIFICATION OF MYCOBACTERIA
Multiple
3233
sputum samples should be collected pref-erably on different days for microscopy for acid-fastbacilli and culture If sputum is not available bronchialwashings taken at bronchoscopy and gastric lavage oraspirate samples should be obtained Gastric aspiratesneed to be neutralised immediately on collection Bron-choscopy and transbronchial biopsy may be useful inpatients with suspected TB but negative sputum smearPleural biopsy is often helpful and mediastinoscopyis occasionally needed in patients with mediastinallymphadenopathy Part of any biopsy specimen shouldalways be sent for culture Nucleic acid amplicationtests on sputum have sensitivity similar to culture in
15 on the 60th day of ICU in a recent study using amulticentre high-quality database and incorporatingnovel statistical methodology to control evolution ofseverity of illness25
PREVENTION
Several guidelines for prevention of ventilator-associated pneumonia and hospital-acquired pneumo-nia have been published26ndash30 Interventions can bedivided into general infection control measures andspecic measures General measures include alcohol-based hand disinfection hospital education programmeon infection control the use of microbiological sur-veillance and a programme to reduce antibiotic pre-scription The major specic recommendations aresummarised in Table 364 There is no evidence that
lsquobundlesrsquo of recommendations are more effective thanthe sum of the individual components
TUBERCULOSIS
The main risk factors are listed in Box 362 Typicalclinical features include fever sweating weight losslassitude anorexia cough productive of mucoid orpurulent sputum haemoptysis chest wall pain dysp-noea localised wheeze and apical crackles Patientsmay also present with unresolved pneumonia pleuraleffusions spontaneous pneumothorax and hoarseness
Figure 364 Management of suspected nosocomial pneumonia based on invasive sampling of respiratory secretions
Bacteria onGram stain
Yes
Yes
No
Yes No Yes No
No
Start antibiotics immediatelyusing PSBBAL specimen
and Gram stain results
Start antibioticsimmediately based onepidemiological clues
Observe look forother infection
Signs ofsevere sepsis
Immediate PSB or BAL beforechangingstarting antimicrobial therapy
+ve cultures +ve cultures
Adjust therapybased on
culture results
Continueadjustantibiotics Look for
other infection
Start antibioticson basisof results
Look forother infection
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1017
Tuberculosis 423
Table 364 Strategies for prevention of ventilator-associated pneumonia
LEVELS OF
RECOMMENDATIONS SPECIFIC INTERVENTIONS REMARKS
Universally recommendedby all guidelines27ndash30
1 Semirecumbent position to 45deg At least 30ndash45deg2 Avoidance of endotracheal intubation3 Preference of oral tracheal route
4 New circuit for a new patient and noschedule change unless soiled or damaged5 Avoidance of flushing of condensate into
lower airway or in-line medication6 HME changes no more frequently than 5ndash7
days7 Continuous aspiration of subglottic suctioning For patients expected to require mechanical
ventilation for gt72 hours
Generally recommendedby most guidelines
1 Preferential use of non-invasiveventilation272830
2 Avoidance of unplanned re-intubation272830
3 Maintenance of endotracheal cuff pressureof about 20 mmHg (266 kPa)272830
4 Closed suctioning2829
No effect on VAP mainly for staff safety5 Chlorhexidine oral decontamination272930
6 Sedation vacation and weaning protocol2728
7 Judicious use of stress ulcer prophylaxis272830
8 Restrictive blood transfusion28
Benefits less clear 1 Preference of HME over heatedhumidifier2830
HME associated with reduction in VAP inpatients ventilated for gt7 days lower cost
2 Silver-sulfadiazine-coated endotrachealtube272830
3 Early tracheostomy (within 7 days ofmechanical ventilation)29
4 Selective decontamination of digestive tract(SDD)272830
Mortality reduction demonstrated when topicalantimicrobials combined with short-course
systemic antibiotics BSAC recommendedSDD in patients expected to requiremechanical ventilation for gt48 hours ETFdiscourage routine use due to concern ofemergence of resistant organisms
Not yet reviewed byguidelines50
1 High-volume low-pressure ultrathin membraneendotracheal tube cuff with SSD
2 Ultrathin membrane cuff with tapered shapeand SSD
3 Low-volume low-pressure endotracheal tubecuff with SSD
4 Balloon device for biofilm removal5 Saline instillation before tracheal suctioning
HME= heat moist exchanger SSD= subglottic secretion drainage
smear-negative patients with pulmonary tuberculosisbut have the advantage of a much more rapid resultThere is however a signicant false-negative rate32
CHEST X-RAY (CXR)A normal CXR almost excludes TB (except inHIV-infected patients) but endobronchial lesionsmay not be apparent and early apical lesions can bemissed Common appearances include patchynodular
shadowing in the upper zones (often bilateral) cavita-tion calcication hilar or mediastinal lymphadenopa-thy (may cause segmental or lobar collapse) pleuraleffusion tuberculomas (dense round or oval shadows)and diffuse ne nodular shadowing throughout thelung elds in miliary TB Inactivity of disease cannot beinferred from the CXR alone This requires three nega-tive sputum samples and failure of any lesion seen onCXR to progress CXR appearances in HIV-positive
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1117
424 Pneumonia
t-tested negative-pressure respirator (N95 FFP2 orhigher) Use of a powered air-purifying respiratorshould be considered when bronchoscopy is being per-formed35 Detailed infection control advice can beobtained via the lsquolink pagersquo (httpwwwaiccuhk eduhkweb8Pneumonia20guidelineshtm)
PNEUMONIA IN THEIMMUNOCOMPROMISED
The lungs are amongst the most frequent targetorgans for infectious complications in the immuno-compromised The incidence of pneumonia is highestamongst patients with haematological malignanciesbone marrow transplant (BMT) recipients and patientswith AIDS
The speed of progression of pneumonia the CXRchanges (Table 365) and the type of immune defectprovide clues to the aetiology Bacterial pneumonias
progress rapidly (1ndash2 days) whereas fungal and proto-zoal pneumonias are less fulminant (several days to aweek or more) Viral pneumonias are usually not ful-minant but on occasions may develop quite rapidlyBronchoscopy is a major component of the investiga-tion of these patients Empirical management based onCXR appearances is outlined in Table 365 Early non-invasive ventilation may improve outcome amongstimmunocompromised patients with fever and bilateralinltrates36
PNEUMOCYSTIS JIROVECI PNEUMONIA (PCP)37
The incidence of this common opportunistic infectionhas fallen substantially in patients with AIDS whoare receiving prophylaxis and effective antiretroviraltherapy with most cases occurring in patients who arenot receiving HIV care or among patients with advancedimmunosuppression The onset is usually insidiouswith dry cough dyspnoea and fever on a backgroundof fatigue and weight loss Crackles in the chest are rareApproximately 15 of patients have a concurrent causefor respiratory failure (eg Kaposi sarcoma TB bacte-rial pneumonia) Useful investigations are
1 CXR classical appearance is diffuse bilateral perihi-
lar interstitial shadowing but in the early stages thisis very subtle and easily missed The initial CXR isnormal in 10 In a further 10 the changes areatypical with focal consolidation or coarse patchyshadowing None of the changes are specic for PCPand may be seen in other lung diseases associatedwith AIDS Pleural effusions hilar or mediastinallymphadenopathy are unusual in PCP but commonin mycobacterial infection or Kaposirsquos sarcoma orlymphoma
2 Induced sputum in this technique the patient inhalesnebulised hypertonic saline from an ultrasonic neb-uliser This provokes bronchorrhoea and the patient
patients with TB differ from those in non-HIV-infectedpatients
TREATMENT OF PULMONARY TB32ndash34
The decision to initiate anti-TB treatment should bebased on level of clinical suspicion results of AFBsmear and sometimes mycobacterial culture If the
initial clinical suspicion is strong and the patient is seri-ously ill attributable to possible TB treatment shouldbe initiated promptly sometimes before the result ofAFB smear Subsequent positivity of AFB smear ornucleic acid amplication test provides support to thecontinuation of treatment Combination chemotherapyconsisting of four drugs is necessary for maximal ef-cacy Treatment is divided into initial phase and con-tinuation phase The most commonly used initialregimen consists of 8 weeks of rifampicin 600 mg daily(450 mg for patients lt50 kg) isoniazid 300 mg dailypyrazinamide 2 g daily (15 g for patients lt50 kg) and
ethambutol 15 mgkg daily as initial phase treatmentEthambutol should be used only in patients who havereasonable visual acuity and who are able to appreciateand report visual disturbances This mandates carefulconsideration in patients who require heavy sedationVisual acuity and colour perception must be assessed(if ethambutol is to be used) and liver and renal func-tion checked before treatment is started Steroids arerecommended for children with endobronchial diseaseand possibly for patients with tuberculous pleuraleffusions Pyridoxine 10 mg daily should be given toprevent isoniazid-induced neuropathy to those atincreased risk (eg patients with diabetes mellitus
chronic renal failure or malnutrition or alcoholic orHIV-positive patients) Negative AFB smear should notdelay initial treatment if clinical suspicion remainshigh Supporting features included chronic coughweight loss characteristic chest X-ray ndings emigra-tion from a high-incidence country no other immediatediagnosis and positive tuberculin test
INFECTION CONTROL
Patients admitted to an ICU with infectious TB or sus-pected of having active pulmonary TB should bemanaged in an isolation room with special ventilation
characteristics including negative pressure Patientsshould be considered infectious if they are coughing orundergoing cough-inducing procedures or if they havepositive AFB smears and they are not on or have juststarted chemotherapy or have a poor clinical or bacte-riological response to chemotherapy3235 Patients withnon-drug-resistant TB should be non-infectious after 2weeks of treatment which includes rifampicin and iso-niazid32 As TB spreads through aerosols it is probablyappropriate to isolate patients who are intubated evenif only their bronchial washings are smear-positiveStaff caring for patients who are smear-positive shouldwear personal protective equipment including a
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1217
Pneumonia in the immunocompromised 425
andor diuretics (patients often uid-overloaded)Approximately 40 of patients with HIV-related PCPwho require mechanical ventilation survive to hospitaldischarge38
Initiation of antiretroviral therapy in patients pre-senting with HIV-related PCP is controversial TheCenters for Disease Control and Prevention (CDC) rec-ommend against doing so in the acute phase but recent
data suggest that the outcome may be improved byinitiation within the rst 4 days of ICU admission39
BACTERIAL PNEUMONIA37
This is the most common cause of acute respiratoryfailure in HIV-positive patients Bacterial pneumonia ismore common in HIV-infected patients than in thegeneral population and tends to be more severe Strep pneumoniae H infuenza Pseudomonas aeruginosa and Saureus are the commonest organisms Nocardia andGram negatives should also be considered Atypicalpathogens (eg Legionella) are rare Response to appro-
priate antibiotics is usually good but may require pro-tracted courses of antibiotics because of high tendencyto relapse Patients with severe immunodeciency(CD4+ T lymphocyte count lt100983221L) and a history ofPseudomonas infection or bronchiectasis or neutropeniashould receive antibiotics that cover P aeruginosa aswell as other Gram negatives The possibility of concur-rent PCP or tuberculosis should be excluded
TUBERCULOSIS
TB may be the initial presentation of AIDS particularlyin sub-Saharan Africa The pattern of TB in HIV patients
coughs up material containing cysts and tropho-zoites The technique is time-consuming and requiresmeticulous technique and is less sensitive thanbronchoscopy but less invasive The possibility ofconcurrent tuberculosis should be consideredand steps taken to minimise the risk of spread ofinfection
3 Bronchoscopy with bronchoalveolar lavage leads to
the diagnosis in over 90 of cases Specimens shouldbe sent for cytology Transbronchial biopsy is notnecessary in most cases PCR using bronchial lavagespecimens may be useful in non-HIV patients withsuspected PCP
Antipneumocystis treatment should be started as soonas the diagnosis is suspected Treatment of choice istrimethoprim plus sulfamethoxazole (co-trimoxazole)20 mgkgday+ 100 mgkgday for 3 weeks plusprednisolone 40 mg orally twice daily for 5 days fol-lowed by 20 mg twice daily for 5 days and then 20 mgper day until the end of PCP treatment Side-effects of
co-trimoxazole are common in HIV patients (nauseavomiting skin rash myelotoxicity) The dose should bereduced by 25 if the WBC count falls Patients whoare intolerant of co-trimoxazole should be treated with
bull pentamidine 4 mgkgday iv or
bull primaquine with clindamycin or
bull trimetrexate with leucovorin (plusmnoral dapsone)
Response to treatment is usually excellent with aresponse time of 4ndash7 days If the patient deteriorates orfails to improve consider (re-)bronchoscopy (is thediagnosis correct) treat co-pathogens and considera short course of high-dose iv methylprednisolone
Table 365 Causes of CXR changes and empirical treatment of pneumonia in the immunocompromised
CHEST X-RAY
APPEARANCE CAUSES
EMPIRICAL TREATMENT FOR
SUSPECTED PNEUMONIA
Diffuse infiltrate CMV and other herpes virusesPneumocystis carinii Bacteria
Aspergillus (advanced)Cryptococcus (uncommon)Non-infectious causes eg drug reaction non-specific
interstitial pneumonitis radiation pneumonitis(uncommon) malignancy leucoagglutinin reaction
Broad-spectrum antibiotics for at least 48 h(eg 3rd-generation cephalosporin andaminoglycoside)
Co-trimoxazoleLung biopsy or lavage within 48 h or full2-week course of co-trimoxazole (dependson patient tolerance of invasive procedure)
Focal infiltrate Gram-negative rodsS aureusAspergillusCryptococcusNocardiaMucorP carinii (uncommon)Tuberculosis
LegionellaNon-infectious causes (eg malignancy non-specificinterstitial pneumonitis radiation pneumonitis)
Broad-spectrum antibioticsIf response seen continue treatment for
2 weeksIf disease progresses lung biopsyaspirate
within 48ndash72 hours or empirical trial ofantifungalplusmn macrolide
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1317
426 Pneumonia
reaction are the most useful tests for demonstratingCMV disease Using thresholds of 10300 000ndash50200 000 positive circulating peripheral WBC the posi-tive predictive value for CMV-pp65 ranges from64 to 82 and the negative predictive value from70 to 954344 Treatment consists of intravenous gan-ciclovir for at least 14 days Foscarnet can be used if
ganciclovir fails
FUNGAL PNEUMONIA
Fungi are rare but important causes of pneumoniaThey can be divided into two main groups based on theimmune response required to combat infection withthese organisms Histoplasma blastomycosis coccidi-oidomycosis paracoccidioidomycosis and Cryptococcus require specic cell-mediated immunity for their controland thus in contrast to infections that are controlled byphagocytic activity the diseases caused by these organ-isms can occur in otherwise healthy individuals
although they cause much more severe illness inpatients with impaired cell-mediated immunity (egpatients infected with HIV and organ transplant recipi-ents) With the exception of Cryptococcus these organ-isms are rarely seen outside North America Aspergillus and Mucor spores are killed by non-immune phago-cytes and as a result these fungi rarely result in clinicalillness in patients with normal neutrophil numbers andfunction
CANDIDIASIS This is effectively a combination of the two types offungal infection in which impaired cell-mediatedimmunity predisposes to mucosal overgrowth withCandida but impaired phagocytic function or numbersis usually required before deep invasion of tissuesoccurs Primary Candida pneumonia (ie isolated lunginfection) is uncommon4145 and more commonly pul-monary lesions are only one manifestation of dissemi-nated candidiasis Even more common is benigncolonisation of the airway with Candida In mostreported cases of primary Candida pneumonia ampho-tericin B has been used In disseminated candidiasistreatment should be directed to treatment of dissemi-nated disease rather than Candida pneumonia per se45
INVASIVE ASPERGILLOSIS 46
This is a highly lethal condition in the immunocom-promised despite treatment and therefore investiga-tion and treatment should be prompt and aggressiveIt is associated with exposure to construction workDenitive diagnosis requires both histological evidenceof acute-angle branching septated non-pigmentedhyphae measuring 2ndash4 983221m in width and cultures yield-ing Aspergillus species from biopsy specimens ofinvolved organs Recovery of Aspergillus species fromrespiratory secretions in immunocompromised butnot immunocompetent patients may indicate invasive
disease with a positive predictive value as high as
depends on the degree of immunosuppression Inpatients with CD4+ T lymphocytes gt350 cells983221L theclinical presentation is similar to TB in non-HIV-infectedpatients although extrapulmonary disease is morecommon In patients with CD4+ T lymphocytes lt350cells983221L extrapulmonary disease (pleuritis pericardi-tis meningitis) is common Severely immunocompro-
mised patients (CD4+
T lymphocytes lt100 cells983221L)may present with severe systemic disease with highfever rapid progression and systemic sepsis In thesepatients lower and middle lobe disease is more commonmiliary disease is common and cavitation is lesscommon Sputum smears and culture may be positiveeven with a normal CXR
Response to treatment is usually rapid Managementof TB in HIV is complex owing to numerous druginteractions consultation with an expert in treatment ofHIV-related TB should be strongly considered Complexinteractions occur between rifamycins (eg rifampicinand rifabutin) and protease inhibitors and non-
nucleoside reverse transcriptase inhibitors used to treatpatients infected with HIV The choice of rifampicin orrifabutin depends on a number of factors includingthe unique and synergistic adverse effects for each indi-vidual combination of rifampicin and anti-HIV drugsand consultation with a physician with experiencein treating both TB and HIV is advised40 IDSA-recommended dosage adjustment for patients receivingantiretrovirals and rifabutin37 can be obtained viathe lsquolink pagersquo (httpwwwaiccuhkeduhkweb8Pneumonia20guidelineshtm) The optimal time forinitiating antiretroviral therapy in patients with TB iscontroversial Early therapy may decrease HIV disease
progression but may be associated with a high inci-dence of adverse effects and an immune reconstitutionreaction37
CMV PNEUMONITIS4142
Risk of infection is highest following allogeneic stemcell transplantation followed by lung transplantationpancreas transplantation and then liver heart and renaltransplantation and advanced AIDS If both the recipi-ent and the donor are seronegative then the risk of bothinfection and disease are negligible If the recipient is
seropositive the risk of infection is approximately 70but the risk of disease is only 20 regardless of theserostatus of the donor However if the recipient isseronegative and the donor is seropositive the risk ofdisease is 70 If steroid pulses and antilymphocyteglobulin are given for treatment of acute rejection therisk of developing disease is markedly increased Infec-tion may be the result of primary infection or reactiva-tion of latent infection It is clinically important butoften difcult to distinguish between CMV infectionand CMV disease and a denitive diagnosis can bemade only histologically Detection of CMV-pp65antigen in peripheral WBC and detection of CMV DNA
or RNA in the blood by quantitative polymerase chain
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1417
Parapneumonic effusion 427
needle aspiration or if there is debris within the uiddrainage using an intercostal drain The diagnosis isconrmed by aspiration of pus
TREATMENT The mainstay of treatment is drainage either by inter-costal drain or by surgical intervention Patients whopresent before the pus is loculated and a brinous peelhas formed on the lung can usually be treated bysimple drainage The combination with intrapleuralbrinolysis may be benecial Optimal surgical man-agement which consists of decortication (open or tho-racoscopic) is indicated if the empyema is moreadvanced or if simple drainage fails This is a majorprocedure and many patients with cardiac or chronicrespiratory disease will not tolerate it Alternatives forthese patients are instillation of thrombolytics into thepleural space or thoracostomy Antibiotics have onlyan adjunctive role Broad-spectrum antibiotic regimenswith anaerobic cover should be used until the resultsof microbiological analysis of the aspirated pus areavailable
AcknowledgementsAll tables and gures are reproduced from ICU web(wwwaiccuhkeduhkweb8) with permission of theauthors
80ndash90 in patients with leukaemia or bone marrowtransplant recipients Bronchoalveolar lavage withsmear culture and antigen detection has excellent spe-cicity and reasonably good positive predictive valuefor invasive aspergillosis in immunocompromisedpatients Although radiological features may give a clueto the diagnosis they are not sufciently specic to be
diagnosticIn acutely ill immunocompromised patients intrave-nous therapy should be initiated if there is suggestiveevidence of invasive aspergillosis while further investi-gations to conrm or refute the diagnosis are carriedout First-line therapy is voriconazole47 Echinocandinsand amphotericin are alternatives
PARAPNEUMONIC EFFUSION
This may be an uncomplicated effusion that resolveswith appropriate treatment of the underlying pneumo-nia or a complicated effusion that develops into an
empyema unless drained Complicated effusions tendto develop 7ndash14 days after initial uid formation Theyare characterised by increasing pleural uid volumecontinued fever and pleural uid of low pH (lt73) thatcontains a large number of neutrophils and may revealorganisms on Gram staining or culture An outline ofmanagement is given in Figure 365
EMPYEMA48
DEFINITION Collection of pus in the pleural space
AETIOLOGY Follows infection of the structures surrounding thepleural space including subdiaphragmatic structuresand chest trauma or may be associated with malig-nancy Anaerobic bacteria usually streptococci orGram-negative rods are responsible for 76 of cases
DIAGNOSIS The diagnosis is usually simple The patient is usuallyseptic and may have a productive cough and chest painThe chest X-ray may show features suggestive of apleural effusion and underlying consolidation but may
also show an abscess cavity with a uid level in whichcase CT scanning will be required to distinguishbetween an abscess and an empyema Ultrasound canbe useful to conrm the presence of uid in the pleuralspace and to determine whether it can be drained by
Figure 365 An approach to the management of
parapneumonic effusions
Parapneumonic effusion
gt 1 cm thick
on lateral decubitus
film
Pleural aspirate
turbid or purulent or
Gram stain +ve
Pleural aspirate
pH
Serial thoracocentesis Treat as empyemaObserve
No
gt72 lt70
70ndash72
No
Yes
Yes
httpwwwexpertconsultcomAccess the complete references list online at
1 American Thoracic Society and Infectious Diseases Society of America Guidelines for the manage-ment of adults with hospital-acquired ventilator-associated and healthcare associated pneumonia
Am J Respir Crit Care Med 2005171388ndash416
2 Mandell LA Wunderink RG Anzueto A et al Infec-tious Diseases Society of AmericaAmerican Tho-racic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin
Infect Dis 200744S27ndash72
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1517
428 Pneumonia
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1617
References 428e1
REFERENCES 1 American Thoracic Society and Infectious Diseases
Society of America Guidelines for the management of adults with hospital-acquired ventilator-associated and healthcare associated pneumonia Am J Respir Crit Care Med 2005171388ndash416
2 Mandell LA Wunderink RG Anzueto A et al Infec-tious Diseases Society of AmericaAmerican Tho-racic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744S27ndash72
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
4 Woodhead M Blasi F Ewig S et al Guidelines for the management of adult lower respiratory tract infections Eur Respir J 2005261138ndash80
5 Torres A Rello J Update in community-acquired and nosocomial pneumonia 2009 Am J Respir Crit
Care Med 2010181782ndash76 Van der Eerden MM Vlaspolder F de Graaff CS et
al Value of intensive diagnostic microbiological investigation in low- and high-risk patients with community-acquired pneumonia Eur J Clin Micro Infect Dis 200524241ndash9
7 Murdoch DR Nucleic acid amplication tests for the diagnosis of pneumonia Clin Infect Dis 2003361162ndash70
8 Blaschke AJ Interpreting assays for the detection of Streptococcus pneumonia Clin Infect Dis 201152(S4)S331ndash7
9 Rello J Lisboa T Lujan M Severity of pneumococcal
pneumonia associated with genomic bacterial load Chest 2009136832ndash4010 Azoulay E Bergeron A Polymerase chain reaction
for diagnosing pneumocystis pneumonia in non-HIV immunocompromised patients with pulmonary inl-trates Chest 2009135(3)655
11 Garcia-Vidal C Fernandez-Sabe N Carratala J Early mortality in patients with community-acquired pneumonia causes and risk factors Eur Respir J200832733ndash9
12 Dellinger RP Carlet JM Masur H et al Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock Intensive Care Med200430536ndash55
13 Metersky ML Ma A Houck PM et al Antibiotics for bacteremic pneumonia improved outcomes with macrolides but not uoroquinolones Chest 2007131466ndash73
14 Dunbar LM Wunderink RG Habib MP High-dose short-course levooxacin for community-acquired pneumonia a new treatment paradigm Clin Infect Dis 200337752ndash60
15 Matthaiou DK Ntani G An ESICM systematic review and meta-analysis of procalcitonin-guided antibiotic therapy algorithms in adult critically ill patients Intensive Care Med 201238940ndash9
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
17 Gruber PC Gomersall CD Joynt GM Avian inu-enza (H5N1) implications for intensive care Inten-sive Care Med 200632823ndash9
18 Belongia EA Irving SA Clinical characteristics and 30-day outcomes for inuenza A 2009 (H1N1) 2008ndash2009 (H1N1) and 2007ndash8 (H3N2) infections JAMA2010304(10)1091
19 Lee N Chan PKS Complications and outcomes of pandemic 2009 inuenza A (H1N1) virus infection in hospitalized adults how do they differ from those in seasonal inuenza J Infect Dis 20112031739ndash47
20 Kim SH Hong SB Corticosteroid treatment in critically ill patients with pandemic inuenza AH1N1 2009 infection analytic strategy using pro-pensity scores Am J Respir Crit Care Med 20111831207ndash14
21 Centers for Disease Control and Prevention (CDC) Bacterial coinfections in lung tissue specimens from
fatal cases of 2009 pandemic inuenza A (H1N1) ndash United States MayndashAugust 2009 MMWR 2009581071ndash4
22 Safdar N Dezfulian C Clinical and economic conse-quences of ventilator-associated pneumonia A sys-tematic review Crit Care Med 200533(10)2184ndash93
23 Shorr AF Sherner JH Invasive approaches to the diagnosis of ventilator-associated pneumonia A meta-analysis Crit Care Med 200533(1)46ndash53
24 Melsen WG Rovers MM Ventilator-associated pneumonia and mortality A systematic review of observational studies Crit Care Med 2009372709ndash18
25 Bekaert M Timsit JF Attributable mortality of ventilator-associated pneumonia A reappraisal using causal analysis Am J Respir Crit Care Med20111841133ndash9
26 CDC Healthcare Infection Control Practices AdvisoryCommittee Guidelines for preventing health-care-associated pneumonia 2003 Recommendations ofCDC and the Healthcare Infection Control PracticesAdvisory Committee Online Available httpwwwcdcgovmmwrpreviewmmwrhtmlrr5303a1htm
27 Cofn SE Klompas M SHEAIDSA practice recom-mendation strategies to prevent ventilator-associated pneumonia in acute care hospitals Infect Control
Hosp Epidemiol 200829S31ndash4028 Masterton RG Galloway A Guidelines for the man-
agement of hospital-acquired pneumonia in the UK Report of the Working Party on Hospital-Acquired Pneumonia of the British Society for Antimicrobial Chemotherapy J Antimicrob Chemother 2008625ndash34
29 VAP Guidelines Committee and the Canadian Critical Care Trials Group Comprehensive evidence-based clinical practice guidelines for ventilator-associated pneumonia prevention J Crit Care 200823126ndash37
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1717
428e2 Pneumonia
30 Torres A Ewig S Dening treating and preventing hospital acquired pneumonia European perspective Intensive Care Med 2009359ndash29
31 Frame RN Johnson MC Eichenhorn MS et al Active tuberculosis in the medical intensive care unit a 15-year retrospective analysis Crit Care Med 1987151012ndash14
32 National Collaborating Centre for Chronic Condi-tions Tuberculosis Clinical diagnosis and manage-ment of tuberculosis and measures for its prevention and control London Royal College of Physicians 2006
33 Small PM Fujiwara PI Management of tuberculosis in the United States N Engl J Med 2001345189ndash200
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
35 Centers for Disease Control and Prevention Guide-lines for preventing the transmission of Mycobacte-rium tuberculosis in health-care settings 2005 MMWR
2005541ndash11936 Hilbert G Gruson D Vargas F et al Noninvasive
ventilation in immunosuppressed patients with pul-monary inltrates fever and acute respiratory failure N Engl J Med 2001344481ndash7
37 Benson CA Kaplan JE Masur H Treating oppor-tunistic infections among HIV-infected adults and adolescents recommendations from CDC the National Institutes of Health and the HIV Medicine AssociationInfectious Diseases Society of America Clin Infect Dis 200540S131ndash235
38 Randall CJ Yarnold PR Schwartz DN et al Improve-ments in outcomes of acute respiratory failure for
patients with human immunodeciency virus-related Pneumocystis carinii pneumonia Am J Respir Crit Care Med 2000162393ndash8
39 Croda J Croda MG Neves A et al Benet of antiret-roviral therapy on survival of human immunode-ciency virus-infected patients admitted to an intensive care unit Crit Care Med 200937(5)1605
40 Centers for Disease Control Updated guidelines for the use of rifabutin or rifampicin for the treatment and prevention of tuberculosis among HIV-infected patients taking protease inhibitors or nonnucleoside reverse transcriptase inhibitors MMWR 200049185ndash9
41 Tamm M The lung in the immunocompromised patient Infectious complications part 2 Respiration199966199ndash207
42 Van der Bij W Speich R Management of cytomega-lovirus infection and disease after solid-organ trans-plantation Clin Infect Dis 200133(Suppl 1)S32ndash7
43 Schaumlfer P Tenschert W Cremaschi L et al Area under the viraemia curve versus absolute viral load utility for predicting symptomatic cytomegalovirus infections in kidney transplant patients J Med Virol20016585ndash9
44 Meyer-Koenig U Weidmann M Kirste G et al Cytomegalovirus infection in organ-transplant recip-ients diagnostic value of pp65 antigen test qualita-tive polymerase chain reaction (PCR) and quantitative
Taqman PCR Transplantation 2004771692ndash8
45 Pappas PG Rex JH Sobel JD Guidelines for treat-ment of candidiasis Clin Infect Dis 200438161ndash89
46 Stevens DA Kan VL Judson MA Practice guidelines for diseases caused by Aspergillus Clin Infect Dis200030696ndash709
47 Herbrecht R Denning DW Patterson TF Voricona-zole versus amphotericin B for primary therapy of invasive aspergillosis N Engl J Med 2002347408ndash15
48 Peek GJ Morcos S Cooper G The pleural cavity BMJ20003201318ndash21
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6

7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1017
Tuberculosis 423
Table 364 Strategies for prevention of ventilator-associated pneumonia
LEVELS OF
RECOMMENDATIONS SPECIFIC INTERVENTIONS REMARKS
Universally recommendedby all guidelines27ndash30
1 Semirecumbent position to 45deg At least 30ndash45deg2 Avoidance of endotracheal intubation3 Preference of oral tracheal route
4 New circuit for a new patient and noschedule change unless soiled or damaged5 Avoidance of flushing of condensate into
lower airway or in-line medication6 HME changes no more frequently than 5ndash7
days7 Continuous aspiration of subglottic suctioning For patients expected to require mechanical
ventilation for gt72 hours
Generally recommendedby most guidelines
1 Preferential use of non-invasiveventilation272830
2 Avoidance of unplanned re-intubation272830
3 Maintenance of endotracheal cuff pressureof about 20 mmHg (266 kPa)272830
4 Closed suctioning2829
No effect on VAP mainly for staff safety5 Chlorhexidine oral decontamination272930
6 Sedation vacation and weaning protocol2728
7 Judicious use of stress ulcer prophylaxis272830
8 Restrictive blood transfusion28
Benefits less clear 1 Preference of HME over heatedhumidifier2830
HME associated with reduction in VAP inpatients ventilated for gt7 days lower cost
2 Silver-sulfadiazine-coated endotrachealtube272830
3 Early tracheostomy (within 7 days ofmechanical ventilation)29
4 Selective decontamination of digestive tract(SDD)272830
Mortality reduction demonstrated when topicalantimicrobials combined with short-course
systemic antibiotics BSAC recommendedSDD in patients expected to requiremechanical ventilation for gt48 hours ETFdiscourage routine use due to concern ofemergence of resistant organisms
Not yet reviewed byguidelines50
1 High-volume low-pressure ultrathin membraneendotracheal tube cuff with SSD
2 Ultrathin membrane cuff with tapered shapeand SSD
3 Low-volume low-pressure endotracheal tubecuff with SSD
4 Balloon device for biofilm removal5 Saline instillation before tracheal suctioning
HME= heat moist exchanger SSD= subglottic secretion drainage
smear-negative patients with pulmonary tuberculosisbut have the advantage of a much more rapid resultThere is however a signicant false-negative rate32
CHEST X-RAY (CXR)A normal CXR almost excludes TB (except inHIV-infected patients) but endobronchial lesionsmay not be apparent and early apical lesions can bemissed Common appearances include patchynodular
shadowing in the upper zones (often bilateral) cavita-tion calcication hilar or mediastinal lymphadenopa-thy (may cause segmental or lobar collapse) pleuraleffusion tuberculomas (dense round or oval shadows)and diffuse ne nodular shadowing throughout thelung elds in miliary TB Inactivity of disease cannot beinferred from the CXR alone This requires three nega-tive sputum samples and failure of any lesion seen onCXR to progress CXR appearances in HIV-positive
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1117
424 Pneumonia
t-tested negative-pressure respirator (N95 FFP2 orhigher) Use of a powered air-purifying respiratorshould be considered when bronchoscopy is being per-formed35 Detailed infection control advice can beobtained via the lsquolink pagersquo (httpwwwaiccuhk eduhkweb8Pneumonia20guidelineshtm)
PNEUMONIA IN THEIMMUNOCOMPROMISED
The lungs are amongst the most frequent targetorgans for infectious complications in the immuno-compromised The incidence of pneumonia is highestamongst patients with haematological malignanciesbone marrow transplant (BMT) recipients and patientswith AIDS
The speed of progression of pneumonia the CXRchanges (Table 365) and the type of immune defectprovide clues to the aetiology Bacterial pneumonias
progress rapidly (1ndash2 days) whereas fungal and proto-zoal pneumonias are less fulminant (several days to aweek or more) Viral pneumonias are usually not ful-minant but on occasions may develop quite rapidlyBronchoscopy is a major component of the investiga-tion of these patients Empirical management based onCXR appearances is outlined in Table 365 Early non-invasive ventilation may improve outcome amongstimmunocompromised patients with fever and bilateralinltrates36
PNEUMOCYSTIS JIROVECI PNEUMONIA (PCP)37
The incidence of this common opportunistic infectionhas fallen substantially in patients with AIDS whoare receiving prophylaxis and effective antiretroviraltherapy with most cases occurring in patients who arenot receiving HIV care or among patients with advancedimmunosuppression The onset is usually insidiouswith dry cough dyspnoea and fever on a backgroundof fatigue and weight loss Crackles in the chest are rareApproximately 15 of patients have a concurrent causefor respiratory failure (eg Kaposi sarcoma TB bacte-rial pneumonia) Useful investigations are
1 CXR classical appearance is diffuse bilateral perihi-
lar interstitial shadowing but in the early stages thisis very subtle and easily missed The initial CXR isnormal in 10 In a further 10 the changes areatypical with focal consolidation or coarse patchyshadowing None of the changes are specic for PCPand may be seen in other lung diseases associatedwith AIDS Pleural effusions hilar or mediastinallymphadenopathy are unusual in PCP but commonin mycobacterial infection or Kaposirsquos sarcoma orlymphoma
2 Induced sputum in this technique the patient inhalesnebulised hypertonic saline from an ultrasonic neb-uliser This provokes bronchorrhoea and the patient
patients with TB differ from those in non-HIV-infectedpatients
TREATMENT OF PULMONARY TB32ndash34
The decision to initiate anti-TB treatment should bebased on level of clinical suspicion results of AFBsmear and sometimes mycobacterial culture If the
initial clinical suspicion is strong and the patient is seri-ously ill attributable to possible TB treatment shouldbe initiated promptly sometimes before the result ofAFB smear Subsequent positivity of AFB smear ornucleic acid amplication test provides support to thecontinuation of treatment Combination chemotherapyconsisting of four drugs is necessary for maximal ef-cacy Treatment is divided into initial phase and con-tinuation phase The most commonly used initialregimen consists of 8 weeks of rifampicin 600 mg daily(450 mg for patients lt50 kg) isoniazid 300 mg dailypyrazinamide 2 g daily (15 g for patients lt50 kg) and
ethambutol 15 mgkg daily as initial phase treatmentEthambutol should be used only in patients who havereasonable visual acuity and who are able to appreciateand report visual disturbances This mandates carefulconsideration in patients who require heavy sedationVisual acuity and colour perception must be assessed(if ethambutol is to be used) and liver and renal func-tion checked before treatment is started Steroids arerecommended for children with endobronchial diseaseand possibly for patients with tuberculous pleuraleffusions Pyridoxine 10 mg daily should be given toprevent isoniazid-induced neuropathy to those atincreased risk (eg patients with diabetes mellitus
chronic renal failure or malnutrition or alcoholic orHIV-positive patients) Negative AFB smear should notdelay initial treatment if clinical suspicion remainshigh Supporting features included chronic coughweight loss characteristic chest X-ray ndings emigra-tion from a high-incidence country no other immediatediagnosis and positive tuberculin test
INFECTION CONTROL
Patients admitted to an ICU with infectious TB or sus-pected of having active pulmonary TB should bemanaged in an isolation room with special ventilation
characteristics including negative pressure Patientsshould be considered infectious if they are coughing orundergoing cough-inducing procedures or if they havepositive AFB smears and they are not on or have juststarted chemotherapy or have a poor clinical or bacte-riological response to chemotherapy3235 Patients withnon-drug-resistant TB should be non-infectious after 2weeks of treatment which includes rifampicin and iso-niazid32 As TB spreads through aerosols it is probablyappropriate to isolate patients who are intubated evenif only their bronchial washings are smear-positiveStaff caring for patients who are smear-positive shouldwear personal protective equipment including a
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1217
Pneumonia in the immunocompromised 425
andor diuretics (patients often uid-overloaded)Approximately 40 of patients with HIV-related PCPwho require mechanical ventilation survive to hospitaldischarge38
Initiation of antiretroviral therapy in patients pre-senting with HIV-related PCP is controversial TheCenters for Disease Control and Prevention (CDC) rec-ommend against doing so in the acute phase but recent
data suggest that the outcome may be improved byinitiation within the rst 4 days of ICU admission39
BACTERIAL PNEUMONIA37
This is the most common cause of acute respiratoryfailure in HIV-positive patients Bacterial pneumonia ismore common in HIV-infected patients than in thegeneral population and tends to be more severe Strep pneumoniae H infuenza Pseudomonas aeruginosa and Saureus are the commonest organisms Nocardia andGram negatives should also be considered Atypicalpathogens (eg Legionella) are rare Response to appro-
priate antibiotics is usually good but may require pro-tracted courses of antibiotics because of high tendencyto relapse Patients with severe immunodeciency(CD4+ T lymphocyte count lt100983221L) and a history ofPseudomonas infection or bronchiectasis or neutropeniashould receive antibiotics that cover P aeruginosa aswell as other Gram negatives The possibility of concur-rent PCP or tuberculosis should be excluded
TUBERCULOSIS
TB may be the initial presentation of AIDS particularlyin sub-Saharan Africa The pattern of TB in HIV patients
coughs up material containing cysts and tropho-zoites The technique is time-consuming and requiresmeticulous technique and is less sensitive thanbronchoscopy but less invasive The possibility ofconcurrent tuberculosis should be consideredand steps taken to minimise the risk of spread ofinfection
3 Bronchoscopy with bronchoalveolar lavage leads to
the diagnosis in over 90 of cases Specimens shouldbe sent for cytology Transbronchial biopsy is notnecessary in most cases PCR using bronchial lavagespecimens may be useful in non-HIV patients withsuspected PCP
Antipneumocystis treatment should be started as soonas the diagnosis is suspected Treatment of choice istrimethoprim plus sulfamethoxazole (co-trimoxazole)20 mgkgday+ 100 mgkgday for 3 weeks plusprednisolone 40 mg orally twice daily for 5 days fol-lowed by 20 mg twice daily for 5 days and then 20 mgper day until the end of PCP treatment Side-effects of
co-trimoxazole are common in HIV patients (nauseavomiting skin rash myelotoxicity) The dose should bereduced by 25 if the WBC count falls Patients whoare intolerant of co-trimoxazole should be treated with
bull pentamidine 4 mgkgday iv or
bull primaquine with clindamycin or
bull trimetrexate with leucovorin (plusmnoral dapsone)
Response to treatment is usually excellent with aresponse time of 4ndash7 days If the patient deteriorates orfails to improve consider (re-)bronchoscopy (is thediagnosis correct) treat co-pathogens and considera short course of high-dose iv methylprednisolone
Table 365 Causes of CXR changes and empirical treatment of pneumonia in the immunocompromised
CHEST X-RAY
APPEARANCE CAUSES
EMPIRICAL TREATMENT FOR
SUSPECTED PNEUMONIA
Diffuse infiltrate CMV and other herpes virusesPneumocystis carinii Bacteria
Aspergillus (advanced)Cryptococcus (uncommon)Non-infectious causes eg drug reaction non-specific
interstitial pneumonitis radiation pneumonitis(uncommon) malignancy leucoagglutinin reaction
Broad-spectrum antibiotics for at least 48 h(eg 3rd-generation cephalosporin andaminoglycoside)
Co-trimoxazoleLung biopsy or lavage within 48 h or full2-week course of co-trimoxazole (dependson patient tolerance of invasive procedure)
Focal infiltrate Gram-negative rodsS aureusAspergillusCryptococcusNocardiaMucorP carinii (uncommon)Tuberculosis
LegionellaNon-infectious causes (eg malignancy non-specificinterstitial pneumonitis radiation pneumonitis)
Broad-spectrum antibioticsIf response seen continue treatment for
2 weeksIf disease progresses lung biopsyaspirate
within 48ndash72 hours or empirical trial ofantifungalplusmn macrolide
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1317
426 Pneumonia
reaction are the most useful tests for demonstratingCMV disease Using thresholds of 10300 000ndash50200 000 positive circulating peripheral WBC the posi-tive predictive value for CMV-pp65 ranges from64 to 82 and the negative predictive value from70 to 954344 Treatment consists of intravenous gan-ciclovir for at least 14 days Foscarnet can be used if
ganciclovir fails
FUNGAL PNEUMONIA
Fungi are rare but important causes of pneumoniaThey can be divided into two main groups based on theimmune response required to combat infection withthese organisms Histoplasma blastomycosis coccidi-oidomycosis paracoccidioidomycosis and Cryptococcus require specic cell-mediated immunity for their controland thus in contrast to infections that are controlled byphagocytic activity the diseases caused by these organ-isms can occur in otherwise healthy individuals
although they cause much more severe illness inpatients with impaired cell-mediated immunity (egpatients infected with HIV and organ transplant recipi-ents) With the exception of Cryptococcus these organ-isms are rarely seen outside North America Aspergillus and Mucor spores are killed by non-immune phago-cytes and as a result these fungi rarely result in clinicalillness in patients with normal neutrophil numbers andfunction
CANDIDIASIS This is effectively a combination of the two types offungal infection in which impaired cell-mediatedimmunity predisposes to mucosal overgrowth withCandida but impaired phagocytic function or numbersis usually required before deep invasion of tissuesoccurs Primary Candida pneumonia (ie isolated lunginfection) is uncommon4145 and more commonly pul-monary lesions are only one manifestation of dissemi-nated candidiasis Even more common is benigncolonisation of the airway with Candida In mostreported cases of primary Candida pneumonia ampho-tericin B has been used In disseminated candidiasistreatment should be directed to treatment of dissemi-nated disease rather than Candida pneumonia per se45
INVASIVE ASPERGILLOSIS 46
This is a highly lethal condition in the immunocom-promised despite treatment and therefore investiga-tion and treatment should be prompt and aggressiveIt is associated with exposure to construction workDenitive diagnosis requires both histological evidenceof acute-angle branching septated non-pigmentedhyphae measuring 2ndash4 983221m in width and cultures yield-ing Aspergillus species from biopsy specimens ofinvolved organs Recovery of Aspergillus species fromrespiratory secretions in immunocompromised butnot immunocompetent patients may indicate invasive
disease with a positive predictive value as high as
depends on the degree of immunosuppression Inpatients with CD4+ T lymphocytes gt350 cells983221L theclinical presentation is similar to TB in non-HIV-infectedpatients although extrapulmonary disease is morecommon In patients with CD4+ T lymphocytes lt350cells983221L extrapulmonary disease (pleuritis pericardi-tis meningitis) is common Severely immunocompro-
mised patients (CD4+
T lymphocytes lt100 cells983221L)may present with severe systemic disease with highfever rapid progression and systemic sepsis In thesepatients lower and middle lobe disease is more commonmiliary disease is common and cavitation is lesscommon Sputum smears and culture may be positiveeven with a normal CXR
Response to treatment is usually rapid Managementof TB in HIV is complex owing to numerous druginteractions consultation with an expert in treatment ofHIV-related TB should be strongly considered Complexinteractions occur between rifamycins (eg rifampicinand rifabutin) and protease inhibitors and non-
nucleoside reverse transcriptase inhibitors used to treatpatients infected with HIV The choice of rifampicin orrifabutin depends on a number of factors includingthe unique and synergistic adverse effects for each indi-vidual combination of rifampicin and anti-HIV drugsand consultation with a physician with experiencein treating both TB and HIV is advised40 IDSA-recommended dosage adjustment for patients receivingantiretrovirals and rifabutin37 can be obtained viathe lsquolink pagersquo (httpwwwaiccuhkeduhkweb8Pneumonia20guidelineshtm) The optimal time forinitiating antiretroviral therapy in patients with TB iscontroversial Early therapy may decrease HIV disease
progression but may be associated with a high inci-dence of adverse effects and an immune reconstitutionreaction37
CMV PNEUMONITIS4142
Risk of infection is highest following allogeneic stemcell transplantation followed by lung transplantationpancreas transplantation and then liver heart and renaltransplantation and advanced AIDS If both the recipi-ent and the donor are seronegative then the risk of bothinfection and disease are negligible If the recipient is
seropositive the risk of infection is approximately 70but the risk of disease is only 20 regardless of theserostatus of the donor However if the recipient isseronegative and the donor is seropositive the risk ofdisease is 70 If steroid pulses and antilymphocyteglobulin are given for treatment of acute rejection therisk of developing disease is markedly increased Infec-tion may be the result of primary infection or reactiva-tion of latent infection It is clinically important butoften difcult to distinguish between CMV infectionand CMV disease and a denitive diagnosis can bemade only histologically Detection of CMV-pp65antigen in peripheral WBC and detection of CMV DNA
or RNA in the blood by quantitative polymerase chain
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1417
Parapneumonic effusion 427
needle aspiration or if there is debris within the uiddrainage using an intercostal drain The diagnosis isconrmed by aspiration of pus
TREATMENT The mainstay of treatment is drainage either by inter-costal drain or by surgical intervention Patients whopresent before the pus is loculated and a brinous peelhas formed on the lung can usually be treated bysimple drainage The combination with intrapleuralbrinolysis may be benecial Optimal surgical man-agement which consists of decortication (open or tho-racoscopic) is indicated if the empyema is moreadvanced or if simple drainage fails This is a majorprocedure and many patients with cardiac or chronicrespiratory disease will not tolerate it Alternatives forthese patients are instillation of thrombolytics into thepleural space or thoracostomy Antibiotics have onlyan adjunctive role Broad-spectrum antibiotic regimenswith anaerobic cover should be used until the resultsof microbiological analysis of the aspirated pus areavailable
AcknowledgementsAll tables and gures are reproduced from ICU web(wwwaiccuhkeduhkweb8) with permission of theauthors
80ndash90 in patients with leukaemia or bone marrowtransplant recipients Bronchoalveolar lavage withsmear culture and antigen detection has excellent spe-cicity and reasonably good positive predictive valuefor invasive aspergillosis in immunocompromisedpatients Although radiological features may give a clueto the diagnosis they are not sufciently specic to be
diagnosticIn acutely ill immunocompromised patients intrave-nous therapy should be initiated if there is suggestiveevidence of invasive aspergillosis while further investi-gations to conrm or refute the diagnosis are carriedout First-line therapy is voriconazole47 Echinocandinsand amphotericin are alternatives
PARAPNEUMONIC EFFUSION
This may be an uncomplicated effusion that resolveswith appropriate treatment of the underlying pneumo-nia or a complicated effusion that develops into an
empyema unless drained Complicated effusions tendto develop 7ndash14 days after initial uid formation Theyare characterised by increasing pleural uid volumecontinued fever and pleural uid of low pH (lt73) thatcontains a large number of neutrophils and may revealorganisms on Gram staining or culture An outline ofmanagement is given in Figure 365
EMPYEMA48
DEFINITION Collection of pus in the pleural space
AETIOLOGY Follows infection of the structures surrounding thepleural space including subdiaphragmatic structuresand chest trauma or may be associated with malig-nancy Anaerobic bacteria usually streptococci orGram-negative rods are responsible for 76 of cases
DIAGNOSIS The diagnosis is usually simple The patient is usuallyseptic and may have a productive cough and chest painThe chest X-ray may show features suggestive of apleural effusion and underlying consolidation but may
also show an abscess cavity with a uid level in whichcase CT scanning will be required to distinguishbetween an abscess and an empyema Ultrasound canbe useful to conrm the presence of uid in the pleuralspace and to determine whether it can be drained by
Figure 365 An approach to the management of
parapneumonic effusions
Parapneumonic effusion
gt 1 cm thick
on lateral decubitus
film
Pleural aspirate
turbid or purulent or
Gram stain +ve
Pleural aspirate
pH
Serial thoracocentesis Treat as empyemaObserve
No
gt72 lt70
70ndash72
No
Yes
Yes
httpwwwexpertconsultcomAccess the complete references list online at
1 American Thoracic Society and Infectious Diseases Society of America Guidelines for the manage-ment of adults with hospital-acquired ventilator-associated and healthcare associated pneumonia
Am J Respir Crit Care Med 2005171388ndash416
2 Mandell LA Wunderink RG Anzueto A et al Infec-tious Diseases Society of AmericaAmerican Tho-racic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin
Infect Dis 200744S27ndash72
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1517
428 Pneumonia
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1617
References 428e1
REFERENCES 1 American Thoracic Society and Infectious Diseases
Society of America Guidelines for the management of adults with hospital-acquired ventilator-associated and healthcare associated pneumonia Am J Respir Crit Care Med 2005171388ndash416
2 Mandell LA Wunderink RG Anzueto A et al Infec-tious Diseases Society of AmericaAmerican Tho-racic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744S27ndash72
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
4 Woodhead M Blasi F Ewig S et al Guidelines for the management of adult lower respiratory tract infections Eur Respir J 2005261138ndash80
5 Torres A Rello J Update in community-acquired and nosocomial pneumonia 2009 Am J Respir Crit
Care Med 2010181782ndash76 Van der Eerden MM Vlaspolder F de Graaff CS et
al Value of intensive diagnostic microbiological investigation in low- and high-risk patients with community-acquired pneumonia Eur J Clin Micro Infect Dis 200524241ndash9
7 Murdoch DR Nucleic acid amplication tests for the diagnosis of pneumonia Clin Infect Dis 2003361162ndash70
8 Blaschke AJ Interpreting assays for the detection of Streptococcus pneumonia Clin Infect Dis 201152(S4)S331ndash7
9 Rello J Lisboa T Lujan M Severity of pneumococcal
pneumonia associated with genomic bacterial load Chest 2009136832ndash4010 Azoulay E Bergeron A Polymerase chain reaction
for diagnosing pneumocystis pneumonia in non-HIV immunocompromised patients with pulmonary inl-trates Chest 2009135(3)655
11 Garcia-Vidal C Fernandez-Sabe N Carratala J Early mortality in patients with community-acquired pneumonia causes and risk factors Eur Respir J200832733ndash9
12 Dellinger RP Carlet JM Masur H et al Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock Intensive Care Med200430536ndash55
13 Metersky ML Ma A Houck PM et al Antibiotics for bacteremic pneumonia improved outcomes with macrolides but not uoroquinolones Chest 2007131466ndash73
14 Dunbar LM Wunderink RG Habib MP High-dose short-course levooxacin for community-acquired pneumonia a new treatment paradigm Clin Infect Dis 200337752ndash60
15 Matthaiou DK Ntani G An ESICM systematic review and meta-analysis of procalcitonin-guided antibiotic therapy algorithms in adult critically ill patients Intensive Care Med 201238940ndash9
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
17 Gruber PC Gomersall CD Joynt GM Avian inu-enza (H5N1) implications for intensive care Inten-sive Care Med 200632823ndash9
18 Belongia EA Irving SA Clinical characteristics and 30-day outcomes for inuenza A 2009 (H1N1) 2008ndash2009 (H1N1) and 2007ndash8 (H3N2) infections JAMA2010304(10)1091
19 Lee N Chan PKS Complications and outcomes of pandemic 2009 inuenza A (H1N1) virus infection in hospitalized adults how do they differ from those in seasonal inuenza J Infect Dis 20112031739ndash47
20 Kim SH Hong SB Corticosteroid treatment in critically ill patients with pandemic inuenza AH1N1 2009 infection analytic strategy using pro-pensity scores Am J Respir Crit Care Med 20111831207ndash14
21 Centers for Disease Control and Prevention (CDC) Bacterial coinfections in lung tissue specimens from
fatal cases of 2009 pandemic inuenza A (H1N1) ndash United States MayndashAugust 2009 MMWR 2009581071ndash4
22 Safdar N Dezfulian C Clinical and economic conse-quences of ventilator-associated pneumonia A sys-tematic review Crit Care Med 200533(10)2184ndash93
23 Shorr AF Sherner JH Invasive approaches to the diagnosis of ventilator-associated pneumonia A meta-analysis Crit Care Med 200533(1)46ndash53
24 Melsen WG Rovers MM Ventilator-associated pneumonia and mortality A systematic review of observational studies Crit Care Med 2009372709ndash18
25 Bekaert M Timsit JF Attributable mortality of ventilator-associated pneumonia A reappraisal using causal analysis Am J Respir Crit Care Med20111841133ndash9
26 CDC Healthcare Infection Control Practices AdvisoryCommittee Guidelines for preventing health-care-associated pneumonia 2003 Recommendations ofCDC and the Healthcare Infection Control PracticesAdvisory Committee Online Available httpwwwcdcgovmmwrpreviewmmwrhtmlrr5303a1htm
27 Cofn SE Klompas M SHEAIDSA practice recom-mendation strategies to prevent ventilator-associated pneumonia in acute care hospitals Infect Control
Hosp Epidemiol 200829S31ndash4028 Masterton RG Galloway A Guidelines for the man-
agement of hospital-acquired pneumonia in the UK Report of the Working Party on Hospital-Acquired Pneumonia of the British Society for Antimicrobial Chemotherapy J Antimicrob Chemother 2008625ndash34
29 VAP Guidelines Committee and the Canadian Critical Care Trials Group Comprehensive evidence-based clinical practice guidelines for ventilator-associated pneumonia prevention J Crit Care 200823126ndash37
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1717
428e2 Pneumonia
30 Torres A Ewig S Dening treating and preventing hospital acquired pneumonia European perspective Intensive Care Med 2009359ndash29
31 Frame RN Johnson MC Eichenhorn MS et al Active tuberculosis in the medical intensive care unit a 15-year retrospective analysis Crit Care Med 1987151012ndash14
32 National Collaborating Centre for Chronic Condi-tions Tuberculosis Clinical diagnosis and manage-ment of tuberculosis and measures for its prevention and control London Royal College of Physicians 2006
33 Small PM Fujiwara PI Management of tuberculosis in the United States N Engl J Med 2001345189ndash200
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
35 Centers for Disease Control and Prevention Guide-lines for preventing the transmission of Mycobacte-rium tuberculosis in health-care settings 2005 MMWR
2005541ndash11936 Hilbert G Gruson D Vargas F et al Noninvasive
ventilation in immunosuppressed patients with pul-monary inltrates fever and acute respiratory failure N Engl J Med 2001344481ndash7
37 Benson CA Kaplan JE Masur H Treating oppor-tunistic infections among HIV-infected adults and adolescents recommendations from CDC the National Institutes of Health and the HIV Medicine AssociationInfectious Diseases Society of America Clin Infect Dis 200540S131ndash235
38 Randall CJ Yarnold PR Schwartz DN et al Improve-ments in outcomes of acute respiratory failure for
patients with human immunodeciency virus-related Pneumocystis carinii pneumonia Am J Respir Crit Care Med 2000162393ndash8
39 Croda J Croda MG Neves A et al Benet of antiret-roviral therapy on survival of human immunode-ciency virus-infected patients admitted to an intensive care unit Crit Care Med 200937(5)1605
40 Centers for Disease Control Updated guidelines for the use of rifabutin or rifampicin for the treatment and prevention of tuberculosis among HIV-infected patients taking protease inhibitors or nonnucleoside reverse transcriptase inhibitors MMWR 200049185ndash9
41 Tamm M The lung in the immunocompromised patient Infectious complications part 2 Respiration199966199ndash207
42 Van der Bij W Speich R Management of cytomega-lovirus infection and disease after solid-organ trans-plantation Clin Infect Dis 200133(Suppl 1)S32ndash7
43 Schaumlfer P Tenschert W Cremaschi L et al Area under the viraemia curve versus absolute viral load utility for predicting symptomatic cytomegalovirus infections in kidney transplant patients J Med Virol20016585ndash9
44 Meyer-Koenig U Weidmann M Kirste G et al Cytomegalovirus infection in organ-transplant recip-ients diagnostic value of pp65 antigen test qualita-tive polymerase chain reaction (PCR) and quantitative
Taqman PCR Transplantation 2004771692ndash8
45 Pappas PG Rex JH Sobel JD Guidelines for treat-ment of candidiasis Clin Infect Dis 200438161ndash89
46 Stevens DA Kan VL Judson MA Practice guidelines for diseases caused by Aspergillus Clin Infect Dis200030696ndash709
47 Herbrecht R Denning DW Patterson TF Voricona-zole versus amphotericin B for primary therapy of invasive aspergillosis N Engl J Med 2002347408ndash15
48 Peek GJ Morcos S Cooper G The pleural cavity BMJ20003201318ndash21
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6

7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1117
424 Pneumonia
t-tested negative-pressure respirator (N95 FFP2 orhigher) Use of a powered air-purifying respiratorshould be considered when bronchoscopy is being per-formed35 Detailed infection control advice can beobtained via the lsquolink pagersquo (httpwwwaiccuhk eduhkweb8Pneumonia20guidelineshtm)
PNEUMONIA IN THEIMMUNOCOMPROMISED
The lungs are amongst the most frequent targetorgans for infectious complications in the immuno-compromised The incidence of pneumonia is highestamongst patients with haematological malignanciesbone marrow transplant (BMT) recipients and patientswith AIDS
The speed of progression of pneumonia the CXRchanges (Table 365) and the type of immune defectprovide clues to the aetiology Bacterial pneumonias
progress rapidly (1ndash2 days) whereas fungal and proto-zoal pneumonias are less fulminant (several days to aweek or more) Viral pneumonias are usually not ful-minant but on occasions may develop quite rapidlyBronchoscopy is a major component of the investiga-tion of these patients Empirical management based onCXR appearances is outlined in Table 365 Early non-invasive ventilation may improve outcome amongstimmunocompromised patients with fever and bilateralinltrates36
PNEUMOCYSTIS JIROVECI PNEUMONIA (PCP)37
The incidence of this common opportunistic infectionhas fallen substantially in patients with AIDS whoare receiving prophylaxis and effective antiretroviraltherapy with most cases occurring in patients who arenot receiving HIV care or among patients with advancedimmunosuppression The onset is usually insidiouswith dry cough dyspnoea and fever on a backgroundof fatigue and weight loss Crackles in the chest are rareApproximately 15 of patients have a concurrent causefor respiratory failure (eg Kaposi sarcoma TB bacte-rial pneumonia) Useful investigations are
1 CXR classical appearance is diffuse bilateral perihi-
lar interstitial shadowing but in the early stages thisis very subtle and easily missed The initial CXR isnormal in 10 In a further 10 the changes areatypical with focal consolidation or coarse patchyshadowing None of the changes are specic for PCPand may be seen in other lung diseases associatedwith AIDS Pleural effusions hilar or mediastinallymphadenopathy are unusual in PCP but commonin mycobacterial infection or Kaposirsquos sarcoma orlymphoma
2 Induced sputum in this technique the patient inhalesnebulised hypertonic saline from an ultrasonic neb-uliser This provokes bronchorrhoea and the patient
patients with TB differ from those in non-HIV-infectedpatients
TREATMENT OF PULMONARY TB32ndash34
The decision to initiate anti-TB treatment should bebased on level of clinical suspicion results of AFBsmear and sometimes mycobacterial culture If the
initial clinical suspicion is strong and the patient is seri-ously ill attributable to possible TB treatment shouldbe initiated promptly sometimes before the result ofAFB smear Subsequent positivity of AFB smear ornucleic acid amplication test provides support to thecontinuation of treatment Combination chemotherapyconsisting of four drugs is necessary for maximal ef-cacy Treatment is divided into initial phase and con-tinuation phase The most commonly used initialregimen consists of 8 weeks of rifampicin 600 mg daily(450 mg for patients lt50 kg) isoniazid 300 mg dailypyrazinamide 2 g daily (15 g for patients lt50 kg) and
ethambutol 15 mgkg daily as initial phase treatmentEthambutol should be used only in patients who havereasonable visual acuity and who are able to appreciateand report visual disturbances This mandates carefulconsideration in patients who require heavy sedationVisual acuity and colour perception must be assessed(if ethambutol is to be used) and liver and renal func-tion checked before treatment is started Steroids arerecommended for children with endobronchial diseaseand possibly for patients with tuberculous pleuraleffusions Pyridoxine 10 mg daily should be given toprevent isoniazid-induced neuropathy to those atincreased risk (eg patients with diabetes mellitus
chronic renal failure or malnutrition or alcoholic orHIV-positive patients) Negative AFB smear should notdelay initial treatment if clinical suspicion remainshigh Supporting features included chronic coughweight loss characteristic chest X-ray ndings emigra-tion from a high-incidence country no other immediatediagnosis and positive tuberculin test
INFECTION CONTROL
Patients admitted to an ICU with infectious TB or sus-pected of having active pulmonary TB should bemanaged in an isolation room with special ventilation
characteristics including negative pressure Patientsshould be considered infectious if they are coughing orundergoing cough-inducing procedures or if they havepositive AFB smears and they are not on or have juststarted chemotherapy or have a poor clinical or bacte-riological response to chemotherapy3235 Patients withnon-drug-resistant TB should be non-infectious after 2weeks of treatment which includes rifampicin and iso-niazid32 As TB spreads through aerosols it is probablyappropriate to isolate patients who are intubated evenif only their bronchial washings are smear-positiveStaff caring for patients who are smear-positive shouldwear personal protective equipment including a
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1217
Pneumonia in the immunocompromised 425
andor diuretics (patients often uid-overloaded)Approximately 40 of patients with HIV-related PCPwho require mechanical ventilation survive to hospitaldischarge38
Initiation of antiretroviral therapy in patients pre-senting with HIV-related PCP is controversial TheCenters for Disease Control and Prevention (CDC) rec-ommend against doing so in the acute phase but recent
data suggest that the outcome may be improved byinitiation within the rst 4 days of ICU admission39
BACTERIAL PNEUMONIA37
This is the most common cause of acute respiratoryfailure in HIV-positive patients Bacterial pneumonia ismore common in HIV-infected patients than in thegeneral population and tends to be more severe Strep pneumoniae H infuenza Pseudomonas aeruginosa and Saureus are the commonest organisms Nocardia andGram negatives should also be considered Atypicalpathogens (eg Legionella) are rare Response to appro-
priate antibiotics is usually good but may require pro-tracted courses of antibiotics because of high tendencyto relapse Patients with severe immunodeciency(CD4+ T lymphocyte count lt100983221L) and a history ofPseudomonas infection or bronchiectasis or neutropeniashould receive antibiotics that cover P aeruginosa aswell as other Gram negatives The possibility of concur-rent PCP or tuberculosis should be excluded
TUBERCULOSIS
TB may be the initial presentation of AIDS particularlyin sub-Saharan Africa The pattern of TB in HIV patients
coughs up material containing cysts and tropho-zoites The technique is time-consuming and requiresmeticulous technique and is less sensitive thanbronchoscopy but less invasive The possibility ofconcurrent tuberculosis should be consideredand steps taken to minimise the risk of spread ofinfection
3 Bronchoscopy with bronchoalveolar lavage leads to
the diagnosis in over 90 of cases Specimens shouldbe sent for cytology Transbronchial biopsy is notnecessary in most cases PCR using bronchial lavagespecimens may be useful in non-HIV patients withsuspected PCP
Antipneumocystis treatment should be started as soonas the diagnosis is suspected Treatment of choice istrimethoprim plus sulfamethoxazole (co-trimoxazole)20 mgkgday+ 100 mgkgday for 3 weeks plusprednisolone 40 mg orally twice daily for 5 days fol-lowed by 20 mg twice daily for 5 days and then 20 mgper day until the end of PCP treatment Side-effects of
co-trimoxazole are common in HIV patients (nauseavomiting skin rash myelotoxicity) The dose should bereduced by 25 if the WBC count falls Patients whoare intolerant of co-trimoxazole should be treated with
bull pentamidine 4 mgkgday iv or
bull primaquine with clindamycin or
bull trimetrexate with leucovorin (plusmnoral dapsone)
Response to treatment is usually excellent with aresponse time of 4ndash7 days If the patient deteriorates orfails to improve consider (re-)bronchoscopy (is thediagnosis correct) treat co-pathogens and considera short course of high-dose iv methylprednisolone
Table 365 Causes of CXR changes and empirical treatment of pneumonia in the immunocompromised
CHEST X-RAY
APPEARANCE CAUSES
EMPIRICAL TREATMENT FOR
SUSPECTED PNEUMONIA
Diffuse infiltrate CMV and other herpes virusesPneumocystis carinii Bacteria
Aspergillus (advanced)Cryptococcus (uncommon)Non-infectious causes eg drug reaction non-specific
interstitial pneumonitis radiation pneumonitis(uncommon) malignancy leucoagglutinin reaction
Broad-spectrum antibiotics for at least 48 h(eg 3rd-generation cephalosporin andaminoglycoside)
Co-trimoxazoleLung biopsy or lavage within 48 h or full2-week course of co-trimoxazole (dependson patient tolerance of invasive procedure)
Focal infiltrate Gram-negative rodsS aureusAspergillusCryptococcusNocardiaMucorP carinii (uncommon)Tuberculosis
LegionellaNon-infectious causes (eg malignancy non-specificinterstitial pneumonitis radiation pneumonitis)
Broad-spectrum antibioticsIf response seen continue treatment for
2 weeksIf disease progresses lung biopsyaspirate
within 48ndash72 hours or empirical trial ofantifungalplusmn macrolide
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1317
426 Pneumonia
reaction are the most useful tests for demonstratingCMV disease Using thresholds of 10300 000ndash50200 000 positive circulating peripheral WBC the posi-tive predictive value for CMV-pp65 ranges from64 to 82 and the negative predictive value from70 to 954344 Treatment consists of intravenous gan-ciclovir for at least 14 days Foscarnet can be used if
ganciclovir fails
FUNGAL PNEUMONIA
Fungi are rare but important causes of pneumoniaThey can be divided into two main groups based on theimmune response required to combat infection withthese organisms Histoplasma blastomycosis coccidi-oidomycosis paracoccidioidomycosis and Cryptococcus require specic cell-mediated immunity for their controland thus in contrast to infections that are controlled byphagocytic activity the diseases caused by these organ-isms can occur in otherwise healthy individuals
although they cause much more severe illness inpatients with impaired cell-mediated immunity (egpatients infected with HIV and organ transplant recipi-ents) With the exception of Cryptococcus these organ-isms are rarely seen outside North America Aspergillus and Mucor spores are killed by non-immune phago-cytes and as a result these fungi rarely result in clinicalillness in patients with normal neutrophil numbers andfunction
CANDIDIASIS This is effectively a combination of the two types offungal infection in which impaired cell-mediatedimmunity predisposes to mucosal overgrowth withCandida but impaired phagocytic function or numbersis usually required before deep invasion of tissuesoccurs Primary Candida pneumonia (ie isolated lunginfection) is uncommon4145 and more commonly pul-monary lesions are only one manifestation of dissemi-nated candidiasis Even more common is benigncolonisation of the airway with Candida In mostreported cases of primary Candida pneumonia ampho-tericin B has been used In disseminated candidiasistreatment should be directed to treatment of dissemi-nated disease rather than Candida pneumonia per se45
INVASIVE ASPERGILLOSIS 46
This is a highly lethal condition in the immunocom-promised despite treatment and therefore investiga-tion and treatment should be prompt and aggressiveIt is associated with exposure to construction workDenitive diagnosis requires both histological evidenceof acute-angle branching septated non-pigmentedhyphae measuring 2ndash4 983221m in width and cultures yield-ing Aspergillus species from biopsy specimens ofinvolved organs Recovery of Aspergillus species fromrespiratory secretions in immunocompromised butnot immunocompetent patients may indicate invasive
disease with a positive predictive value as high as
depends on the degree of immunosuppression Inpatients with CD4+ T lymphocytes gt350 cells983221L theclinical presentation is similar to TB in non-HIV-infectedpatients although extrapulmonary disease is morecommon In patients with CD4+ T lymphocytes lt350cells983221L extrapulmonary disease (pleuritis pericardi-tis meningitis) is common Severely immunocompro-
mised patients (CD4+
T lymphocytes lt100 cells983221L)may present with severe systemic disease with highfever rapid progression and systemic sepsis In thesepatients lower and middle lobe disease is more commonmiliary disease is common and cavitation is lesscommon Sputum smears and culture may be positiveeven with a normal CXR
Response to treatment is usually rapid Managementof TB in HIV is complex owing to numerous druginteractions consultation with an expert in treatment ofHIV-related TB should be strongly considered Complexinteractions occur between rifamycins (eg rifampicinand rifabutin) and protease inhibitors and non-
nucleoside reverse transcriptase inhibitors used to treatpatients infected with HIV The choice of rifampicin orrifabutin depends on a number of factors includingthe unique and synergistic adverse effects for each indi-vidual combination of rifampicin and anti-HIV drugsand consultation with a physician with experiencein treating both TB and HIV is advised40 IDSA-recommended dosage adjustment for patients receivingantiretrovirals and rifabutin37 can be obtained viathe lsquolink pagersquo (httpwwwaiccuhkeduhkweb8Pneumonia20guidelineshtm) The optimal time forinitiating antiretroviral therapy in patients with TB iscontroversial Early therapy may decrease HIV disease
progression but may be associated with a high inci-dence of adverse effects and an immune reconstitutionreaction37
CMV PNEUMONITIS4142
Risk of infection is highest following allogeneic stemcell transplantation followed by lung transplantationpancreas transplantation and then liver heart and renaltransplantation and advanced AIDS If both the recipi-ent and the donor are seronegative then the risk of bothinfection and disease are negligible If the recipient is
seropositive the risk of infection is approximately 70but the risk of disease is only 20 regardless of theserostatus of the donor However if the recipient isseronegative and the donor is seropositive the risk ofdisease is 70 If steroid pulses and antilymphocyteglobulin are given for treatment of acute rejection therisk of developing disease is markedly increased Infec-tion may be the result of primary infection or reactiva-tion of latent infection It is clinically important butoften difcult to distinguish between CMV infectionand CMV disease and a denitive diagnosis can bemade only histologically Detection of CMV-pp65antigen in peripheral WBC and detection of CMV DNA
or RNA in the blood by quantitative polymerase chain
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1417
Parapneumonic effusion 427
needle aspiration or if there is debris within the uiddrainage using an intercostal drain The diagnosis isconrmed by aspiration of pus
TREATMENT The mainstay of treatment is drainage either by inter-costal drain or by surgical intervention Patients whopresent before the pus is loculated and a brinous peelhas formed on the lung can usually be treated bysimple drainage The combination with intrapleuralbrinolysis may be benecial Optimal surgical man-agement which consists of decortication (open or tho-racoscopic) is indicated if the empyema is moreadvanced or if simple drainage fails This is a majorprocedure and many patients with cardiac or chronicrespiratory disease will not tolerate it Alternatives forthese patients are instillation of thrombolytics into thepleural space or thoracostomy Antibiotics have onlyan adjunctive role Broad-spectrum antibiotic regimenswith anaerobic cover should be used until the resultsof microbiological analysis of the aspirated pus areavailable
AcknowledgementsAll tables and gures are reproduced from ICU web(wwwaiccuhkeduhkweb8) with permission of theauthors
80ndash90 in patients with leukaemia or bone marrowtransplant recipients Bronchoalveolar lavage withsmear culture and antigen detection has excellent spe-cicity and reasonably good positive predictive valuefor invasive aspergillosis in immunocompromisedpatients Although radiological features may give a clueto the diagnosis they are not sufciently specic to be
diagnosticIn acutely ill immunocompromised patients intrave-nous therapy should be initiated if there is suggestiveevidence of invasive aspergillosis while further investi-gations to conrm or refute the diagnosis are carriedout First-line therapy is voriconazole47 Echinocandinsand amphotericin are alternatives
PARAPNEUMONIC EFFUSION
This may be an uncomplicated effusion that resolveswith appropriate treatment of the underlying pneumo-nia or a complicated effusion that develops into an
empyema unless drained Complicated effusions tendto develop 7ndash14 days after initial uid formation Theyare characterised by increasing pleural uid volumecontinued fever and pleural uid of low pH (lt73) thatcontains a large number of neutrophils and may revealorganisms on Gram staining or culture An outline ofmanagement is given in Figure 365
EMPYEMA48
DEFINITION Collection of pus in the pleural space
AETIOLOGY Follows infection of the structures surrounding thepleural space including subdiaphragmatic structuresand chest trauma or may be associated with malig-nancy Anaerobic bacteria usually streptococci orGram-negative rods are responsible for 76 of cases
DIAGNOSIS The diagnosis is usually simple The patient is usuallyseptic and may have a productive cough and chest painThe chest X-ray may show features suggestive of apleural effusion and underlying consolidation but may
also show an abscess cavity with a uid level in whichcase CT scanning will be required to distinguishbetween an abscess and an empyema Ultrasound canbe useful to conrm the presence of uid in the pleuralspace and to determine whether it can be drained by
Figure 365 An approach to the management of
parapneumonic effusions
Parapneumonic effusion
gt 1 cm thick
on lateral decubitus
film
Pleural aspirate
turbid or purulent or
Gram stain +ve
Pleural aspirate
pH
Serial thoracocentesis Treat as empyemaObserve
No
gt72 lt70
70ndash72
No
Yes
Yes
httpwwwexpertconsultcomAccess the complete references list online at
1 American Thoracic Society and Infectious Diseases Society of America Guidelines for the manage-ment of adults with hospital-acquired ventilator-associated and healthcare associated pneumonia
Am J Respir Crit Care Med 2005171388ndash416
2 Mandell LA Wunderink RG Anzueto A et al Infec-tious Diseases Society of AmericaAmerican Tho-racic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin
Infect Dis 200744S27ndash72
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1517
428 Pneumonia
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1617
References 428e1
REFERENCES 1 American Thoracic Society and Infectious Diseases
Society of America Guidelines for the management of adults with hospital-acquired ventilator-associated and healthcare associated pneumonia Am J Respir Crit Care Med 2005171388ndash416
2 Mandell LA Wunderink RG Anzueto A et al Infec-tious Diseases Society of AmericaAmerican Tho-racic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744S27ndash72
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
4 Woodhead M Blasi F Ewig S et al Guidelines for the management of adult lower respiratory tract infections Eur Respir J 2005261138ndash80
5 Torres A Rello J Update in community-acquired and nosocomial pneumonia 2009 Am J Respir Crit
Care Med 2010181782ndash76 Van der Eerden MM Vlaspolder F de Graaff CS et
al Value of intensive diagnostic microbiological investigation in low- and high-risk patients with community-acquired pneumonia Eur J Clin Micro Infect Dis 200524241ndash9
7 Murdoch DR Nucleic acid amplication tests for the diagnosis of pneumonia Clin Infect Dis 2003361162ndash70
8 Blaschke AJ Interpreting assays for the detection of Streptococcus pneumonia Clin Infect Dis 201152(S4)S331ndash7
9 Rello J Lisboa T Lujan M Severity of pneumococcal
pneumonia associated with genomic bacterial load Chest 2009136832ndash4010 Azoulay E Bergeron A Polymerase chain reaction
for diagnosing pneumocystis pneumonia in non-HIV immunocompromised patients with pulmonary inl-trates Chest 2009135(3)655
11 Garcia-Vidal C Fernandez-Sabe N Carratala J Early mortality in patients with community-acquired pneumonia causes and risk factors Eur Respir J200832733ndash9
12 Dellinger RP Carlet JM Masur H et al Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock Intensive Care Med200430536ndash55
13 Metersky ML Ma A Houck PM et al Antibiotics for bacteremic pneumonia improved outcomes with macrolides but not uoroquinolones Chest 2007131466ndash73
14 Dunbar LM Wunderink RG Habib MP High-dose short-course levooxacin for community-acquired pneumonia a new treatment paradigm Clin Infect Dis 200337752ndash60
15 Matthaiou DK Ntani G An ESICM systematic review and meta-analysis of procalcitonin-guided antibiotic therapy algorithms in adult critically ill patients Intensive Care Med 201238940ndash9
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
17 Gruber PC Gomersall CD Joynt GM Avian inu-enza (H5N1) implications for intensive care Inten-sive Care Med 200632823ndash9
18 Belongia EA Irving SA Clinical characteristics and 30-day outcomes for inuenza A 2009 (H1N1) 2008ndash2009 (H1N1) and 2007ndash8 (H3N2) infections JAMA2010304(10)1091
19 Lee N Chan PKS Complications and outcomes of pandemic 2009 inuenza A (H1N1) virus infection in hospitalized adults how do they differ from those in seasonal inuenza J Infect Dis 20112031739ndash47
20 Kim SH Hong SB Corticosteroid treatment in critically ill patients with pandemic inuenza AH1N1 2009 infection analytic strategy using pro-pensity scores Am J Respir Crit Care Med 20111831207ndash14
21 Centers for Disease Control and Prevention (CDC) Bacterial coinfections in lung tissue specimens from
fatal cases of 2009 pandemic inuenza A (H1N1) ndash United States MayndashAugust 2009 MMWR 2009581071ndash4
22 Safdar N Dezfulian C Clinical and economic conse-quences of ventilator-associated pneumonia A sys-tematic review Crit Care Med 200533(10)2184ndash93
23 Shorr AF Sherner JH Invasive approaches to the diagnosis of ventilator-associated pneumonia A meta-analysis Crit Care Med 200533(1)46ndash53
24 Melsen WG Rovers MM Ventilator-associated pneumonia and mortality A systematic review of observational studies Crit Care Med 2009372709ndash18
25 Bekaert M Timsit JF Attributable mortality of ventilator-associated pneumonia A reappraisal using causal analysis Am J Respir Crit Care Med20111841133ndash9
26 CDC Healthcare Infection Control Practices AdvisoryCommittee Guidelines for preventing health-care-associated pneumonia 2003 Recommendations ofCDC and the Healthcare Infection Control PracticesAdvisory Committee Online Available httpwwwcdcgovmmwrpreviewmmwrhtmlrr5303a1htm
27 Cofn SE Klompas M SHEAIDSA practice recom-mendation strategies to prevent ventilator-associated pneumonia in acute care hospitals Infect Control
Hosp Epidemiol 200829S31ndash4028 Masterton RG Galloway A Guidelines for the man-
agement of hospital-acquired pneumonia in the UK Report of the Working Party on Hospital-Acquired Pneumonia of the British Society for Antimicrobial Chemotherapy J Antimicrob Chemother 2008625ndash34
29 VAP Guidelines Committee and the Canadian Critical Care Trials Group Comprehensive evidence-based clinical practice guidelines for ventilator-associated pneumonia prevention J Crit Care 200823126ndash37
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1717
428e2 Pneumonia
30 Torres A Ewig S Dening treating and preventing hospital acquired pneumonia European perspective Intensive Care Med 2009359ndash29
31 Frame RN Johnson MC Eichenhorn MS et al Active tuberculosis in the medical intensive care unit a 15-year retrospective analysis Crit Care Med 1987151012ndash14
32 National Collaborating Centre for Chronic Condi-tions Tuberculosis Clinical diagnosis and manage-ment of tuberculosis and measures for its prevention and control London Royal College of Physicians 2006
33 Small PM Fujiwara PI Management of tuberculosis in the United States N Engl J Med 2001345189ndash200
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
35 Centers for Disease Control and Prevention Guide-lines for preventing the transmission of Mycobacte-rium tuberculosis in health-care settings 2005 MMWR
2005541ndash11936 Hilbert G Gruson D Vargas F et al Noninvasive
ventilation in immunosuppressed patients with pul-monary inltrates fever and acute respiratory failure N Engl J Med 2001344481ndash7
37 Benson CA Kaplan JE Masur H Treating oppor-tunistic infections among HIV-infected adults and adolescents recommendations from CDC the National Institutes of Health and the HIV Medicine AssociationInfectious Diseases Society of America Clin Infect Dis 200540S131ndash235
38 Randall CJ Yarnold PR Schwartz DN et al Improve-ments in outcomes of acute respiratory failure for
patients with human immunodeciency virus-related Pneumocystis carinii pneumonia Am J Respir Crit Care Med 2000162393ndash8
39 Croda J Croda MG Neves A et al Benet of antiret-roviral therapy on survival of human immunode-ciency virus-infected patients admitted to an intensive care unit Crit Care Med 200937(5)1605
40 Centers for Disease Control Updated guidelines for the use of rifabutin or rifampicin for the treatment and prevention of tuberculosis among HIV-infected patients taking protease inhibitors or nonnucleoside reverse transcriptase inhibitors MMWR 200049185ndash9
41 Tamm M The lung in the immunocompromised patient Infectious complications part 2 Respiration199966199ndash207
42 Van der Bij W Speich R Management of cytomega-lovirus infection and disease after solid-organ trans-plantation Clin Infect Dis 200133(Suppl 1)S32ndash7
43 Schaumlfer P Tenschert W Cremaschi L et al Area under the viraemia curve versus absolute viral load utility for predicting symptomatic cytomegalovirus infections in kidney transplant patients J Med Virol20016585ndash9
44 Meyer-Koenig U Weidmann M Kirste G et al Cytomegalovirus infection in organ-transplant recip-ients diagnostic value of pp65 antigen test qualita-tive polymerase chain reaction (PCR) and quantitative
Taqman PCR Transplantation 2004771692ndash8
45 Pappas PG Rex JH Sobel JD Guidelines for treat-ment of candidiasis Clin Infect Dis 200438161ndash89
46 Stevens DA Kan VL Judson MA Practice guidelines for diseases caused by Aspergillus Clin Infect Dis200030696ndash709
47 Herbrecht R Denning DW Patterson TF Voricona-zole versus amphotericin B for primary therapy of invasive aspergillosis N Engl J Med 2002347408ndash15
48 Peek GJ Morcos S Cooper G The pleural cavity BMJ20003201318ndash21
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6

7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1217
Pneumonia in the immunocompromised 425
andor diuretics (patients often uid-overloaded)Approximately 40 of patients with HIV-related PCPwho require mechanical ventilation survive to hospitaldischarge38
Initiation of antiretroviral therapy in patients pre-senting with HIV-related PCP is controversial TheCenters for Disease Control and Prevention (CDC) rec-ommend against doing so in the acute phase but recent
data suggest that the outcome may be improved byinitiation within the rst 4 days of ICU admission39
BACTERIAL PNEUMONIA37
This is the most common cause of acute respiratoryfailure in HIV-positive patients Bacterial pneumonia ismore common in HIV-infected patients than in thegeneral population and tends to be more severe Strep pneumoniae H infuenza Pseudomonas aeruginosa and Saureus are the commonest organisms Nocardia andGram negatives should also be considered Atypicalpathogens (eg Legionella) are rare Response to appro-
priate antibiotics is usually good but may require pro-tracted courses of antibiotics because of high tendencyto relapse Patients with severe immunodeciency(CD4+ T lymphocyte count lt100983221L) and a history ofPseudomonas infection or bronchiectasis or neutropeniashould receive antibiotics that cover P aeruginosa aswell as other Gram negatives The possibility of concur-rent PCP or tuberculosis should be excluded
TUBERCULOSIS
TB may be the initial presentation of AIDS particularlyin sub-Saharan Africa The pattern of TB in HIV patients
coughs up material containing cysts and tropho-zoites The technique is time-consuming and requiresmeticulous technique and is less sensitive thanbronchoscopy but less invasive The possibility ofconcurrent tuberculosis should be consideredand steps taken to minimise the risk of spread ofinfection
3 Bronchoscopy with bronchoalveolar lavage leads to
the diagnosis in over 90 of cases Specimens shouldbe sent for cytology Transbronchial biopsy is notnecessary in most cases PCR using bronchial lavagespecimens may be useful in non-HIV patients withsuspected PCP
Antipneumocystis treatment should be started as soonas the diagnosis is suspected Treatment of choice istrimethoprim plus sulfamethoxazole (co-trimoxazole)20 mgkgday+ 100 mgkgday for 3 weeks plusprednisolone 40 mg orally twice daily for 5 days fol-lowed by 20 mg twice daily for 5 days and then 20 mgper day until the end of PCP treatment Side-effects of
co-trimoxazole are common in HIV patients (nauseavomiting skin rash myelotoxicity) The dose should bereduced by 25 if the WBC count falls Patients whoare intolerant of co-trimoxazole should be treated with
bull pentamidine 4 mgkgday iv or
bull primaquine with clindamycin or
bull trimetrexate with leucovorin (plusmnoral dapsone)
Response to treatment is usually excellent with aresponse time of 4ndash7 days If the patient deteriorates orfails to improve consider (re-)bronchoscopy (is thediagnosis correct) treat co-pathogens and considera short course of high-dose iv methylprednisolone
Table 365 Causes of CXR changes and empirical treatment of pneumonia in the immunocompromised
CHEST X-RAY
APPEARANCE CAUSES
EMPIRICAL TREATMENT FOR
SUSPECTED PNEUMONIA
Diffuse infiltrate CMV and other herpes virusesPneumocystis carinii Bacteria
Aspergillus (advanced)Cryptococcus (uncommon)Non-infectious causes eg drug reaction non-specific
interstitial pneumonitis radiation pneumonitis(uncommon) malignancy leucoagglutinin reaction
Broad-spectrum antibiotics for at least 48 h(eg 3rd-generation cephalosporin andaminoglycoside)
Co-trimoxazoleLung biopsy or lavage within 48 h or full2-week course of co-trimoxazole (dependson patient tolerance of invasive procedure)
Focal infiltrate Gram-negative rodsS aureusAspergillusCryptococcusNocardiaMucorP carinii (uncommon)Tuberculosis
LegionellaNon-infectious causes (eg malignancy non-specificinterstitial pneumonitis radiation pneumonitis)
Broad-spectrum antibioticsIf response seen continue treatment for
2 weeksIf disease progresses lung biopsyaspirate
within 48ndash72 hours or empirical trial ofantifungalplusmn macrolide
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1317
426 Pneumonia
reaction are the most useful tests for demonstratingCMV disease Using thresholds of 10300 000ndash50200 000 positive circulating peripheral WBC the posi-tive predictive value for CMV-pp65 ranges from64 to 82 and the negative predictive value from70 to 954344 Treatment consists of intravenous gan-ciclovir for at least 14 days Foscarnet can be used if
ganciclovir fails
FUNGAL PNEUMONIA
Fungi are rare but important causes of pneumoniaThey can be divided into two main groups based on theimmune response required to combat infection withthese organisms Histoplasma blastomycosis coccidi-oidomycosis paracoccidioidomycosis and Cryptococcus require specic cell-mediated immunity for their controland thus in contrast to infections that are controlled byphagocytic activity the diseases caused by these organ-isms can occur in otherwise healthy individuals
although they cause much more severe illness inpatients with impaired cell-mediated immunity (egpatients infected with HIV and organ transplant recipi-ents) With the exception of Cryptococcus these organ-isms are rarely seen outside North America Aspergillus and Mucor spores are killed by non-immune phago-cytes and as a result these fungi rarely result in clinicalillness in patients with normal neutrophil numbers andfunction
CANDIDIASIS This is effectively a combination of the two types offungal infection in which impaired cell-mediatedimmunity predisposes to mucosal overgrowth withCandida but impaired phagocytic function or numbersis usually required before deep invasion of tissuesoccurs Primary Candida pneumonia (ie isolated lunginfection) is uncommon4145 and more commonly pul-monary lesions are only one manifestation of dissemi-nated candidiasis Even more common is benigncolonisation of the airway with Candida In mostreported cases of primary Candida pneumonia ampho-tericin B has been used In disseminated candidiasistreatment should be directed to treatment of dissemi-nated disease rather than Candida pneumonia per se45
INVASIVE ASPERGILLOSIS 46
This is a highly lethal condition in the immunocom-promised despite treatment and therefore investiga-tion and treatment should be prompt and aggressiveIt is associated with exposure to construction workDenitive diagnosis requires both histological evidenceof acute-angle branching septated non-pigmentedhyphae measuring 2ndash4 983221m in width and cultures yield-ing Aspergillus species from biopsy specimens ofinvolved organs Recovery of Aspergillus species fromrespiratory secretions in immunocompromised butnot immunocompetent patients may indicate invasive
disease with a positive predictive value as high as
depends on the degree of immunosuppression Inpatients with CD4+ T lymphocytes gt350 cells983221L theclinical presentation is similar to TB in non-HIV-infectedpatients although extrapulmonary disease is morecommon In patients with CD4+ T lymphocytes lt350cells983221L extrapulmonary disease (pleuritis pericardi-tis meningitis) is common Severely immunocompro-
mised patients (CD4+
T lymphocytes lt100 cells983221L)may present with severe systemic disease with highfever rapid progression and systemic sepsis In thesepatients lower and middle lobe disease is more commonmiliary disease is common and cavitation is lesscommon Sputum smears and culture may be positiveeven with a normal CXR
Response to treatment is usually rapid Managementof TB in HIV is complex owing to numerous druginteractions consultation with an expert in treatment ofHIV-related TB should be strongly considered Complexinteractions occur between rifamycins (eg rifampicinand rifabutin) and protease inhibitors and non-
nucleoside reverse transcriptase inhibitors used to treatpatients infected with HIV The choice of rifampicin orrifabutin depends on a number of factors includingthe unique and synergistic adverse effects for each indi-vidual combination of rifampicin and anti-HIV drugsand consultation with a physician with experiencein treating both TB and HIV is advised40 IDSA-recommended dosage adjustment for patients receivingantiretrovirals and rifabutin37 can be obtained viathe lsquolink pagersquo (httpwwwaiccuhkeduhkweb8Pneumonia20guidelineshtm) The optimal time forinitiating antiretroviral therapy in patients with TB iscontroversial Early therapy may decrease HIV disease
progression but may be associated with a high inci-dence of adverse effects and an immune reconstitutionreaction37
CMV PNEUMONITIS4142
Risk of infection is highest following allogeneic stemcell transplantation followed by lung transplantationpancreas transplantation and then liver heart and renaltransplantation and advanced AIDS If both the recipi-ent and the donor are seronegative then the risk of bothinfection and disease are negligible If the recipient is
seropositive the risk of infection is approximately 70but the risk of disease is only 20 regardless of theserostatus of the donor However if the recipient isseronegative and the donor is seropositive the risk ofdisease is 70 If steroid pulses and antilymphocyteglobulin are given for treatment of acute rejection therisk of developing disease is markedly increased Infec-tion may be the result of primary infection or reactiva-tion of latent infection It is clinically important butoften difcult to distinguish between CMV infectionand CMV disease and a denitive diagnosis can bemade only histologically Detection of CMV-pp65antigen in peripheral WBC and detection of CMV DNA
or RNA in the blood by quantitative polymerase chain
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1417
Parapneumonic effusion 427
needle aspiration or if there is debris within the uiddrainage using an intercostal drain The diagnosis isconrmed by aspiration of pus
TREATMENT The mainstay of treatment is drainage either by inter-costal drain or by surgical intervention Patients whopresent before the pus is loculated and a brinous peelhas formed on the lung can usually be treated bysimple drainage The combination with intrapleuralbrinolysis may be benecial Optimal surgical man-agement which consists of decortication (open or tho-racoscopic) is indicated if the empyema is moreadvanced or if simple drainage fails This is a majorprocedure and many patients with cardiac or chronicrespiratory disease will not tolerate it Alternatives forthese patients are instillation of thrombolytics into thepleural space or thoracostomy Antibiotics have onlyan adjunctive role Broad-spectrum antibiotic regimenswith anaerobic cover should be used until the resultsof microbiological analysis of the aspirated pus areavailable
AcknowledgementsAll tables and gures are reproduced from ICU web(wwwaiccuhkeduhkweb8) with permission of theauthors
80ndash90 in patients with leukaemia or bone marrowtransplant recipients Bronchoalveolar lavage withsmear culture and antigen detection has excellent spe-cicity and reasonably good positive predictive valuefor invasive aspergillosis in immunocompromisedpatients Although radiological features may give a clueto the diagnosis they are not sufciently specic to be
diagnosticIn acutely ill immunocompromised patients intrave-nous therapy should be initiated if there is suggestiveevidence of invasive aspergillosis while further investi-gations to conrm or refute the diagnosis are carriedout First-line therapy is voriconazole47 Echinocandinsand amphotericin are alternatives
PARAPNEUMONIC EFFUSION
This may be an uncomplicated effusion that resolveswith appropriate treatment of the underlying pneumo-nia or a complicated effusion that develops into an
empyema unless drained Complicated effusions tendto develop 7ndash14 days after initial uid formation Theyare characterised by increasing pleural uid volumecontinued fever and pleural uid of low pH (lt73) thatcontains a large number of neutrophils and may revealorganisms on Gram staining or culture An outline ofmanagement is given in Figure 365
EMPYEMA48
DEFINITION Collection of pus in the pleural space
AETIOLOGY Follows infection of the structures surrounding thepleural space including subdiaphragmatic structuresand chest trauma or may be associated with malig-nancy Anaerobic bacteria usually streptococci orGram-negative rods are responsible for 76 of cases
DIAGNOSIS The diagnosis is usually simple The patient is usuallyseptic and may have a productive cough and chest painThe chest X-ray may show features suggestive of apleural effusion and underlying consolidation but may
also show an abscess cavity with a uid level in whichcase CT scanning will be required to distinguishbetween an abscess and an empyema Ultrasound canbe useful to conrm the presence of uid in the pleuralspace and to determine whether it can be drained by
Figure 365 An approach to the management of
parapneumonic effusions
Parapneumonic effusion
gt 1 cm thick
on lateral decubitus
film
Pleural aspirate
turbid or purulent or
Gram stain +ve
Pleural aspirate
pH
Serial thoracocentesis Treat as empyemaObserve
No
gt72 lt70
70ndash72
No
Yes
Yes
httpwwwexpertconsultcomAccess the complete references list online at
1 American Thoracic Society and Infectious Diseases Society of America Guidelines for the manage-ment of adults with hospital-acquired ventilator-associated and healthcare associated pneumonia
Am J Respir Crit Care Med 2005171388ndash416
2 Mandell LA Wunderink RG Anzueto A et al Infec-tious Diseases Society of AmericaAmerican Tho-racic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin
Infect Dis 200744S27ndash72
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1517
428 Pneumonia
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1617
References 428e1
REFERENCES 1 American Thoracic Society and Infectious Diseases
Society of America Guidelines for the management of adults with hospital-acquired ventilator-associated and healthcare associated pneumonia Am J Respir Crit Care Med 2005171388ndash416
2 Mandell LA Wunderink RG Anzueto A et al Infec-tious Diseases Society of AmericaAmerican Tho-racic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744S27ndash72
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
4 Woodhead M Blasi F Ewig S et al Guidelines for the management of adult lower respiratory tract infections Eur Respir J 2005261138ndash80
5 Torres A Rello J Update in community-acquired and nosocomial pneumonia 2009 Am J Respir Crit
Care Med 2010181782ndash76 Van der Eerden MM Vlaspolder F de Graaff CS et
al Value of intensive diagnostic microbiological investigation in low- and high-risk patients with community-acquired pneumonia Eur J Clin Micro Infect Dis 200524241ndash9
7 Murdoch DR Nucleic acid amplication tests for the diagnosis of pneumonia Clin Infect Dis 2003361162ndash70
8 Blaschke AJ Interpreting assays for the detection of Streptococcus pneumonia Clin Infect Dis 201152(S4)S331ndash7
9 Rello J Lisboa T Lujan M Severity of pneumococcal
pneumonia associated with genomic bacterial load Chest 2009136832ndash4010 Azoulay E Bergeron A Polymerase chain reaction
for diagnosing pneumocystis pneumonia in non-HIV immunocompromised patients with pulmonary inl-trates Chest 2009135(3)655
11 Garcia-Vidal C Fernandez-Sabe N Carratala J Early mortality in patients with community-acquired pneumonia causes and risk factors Eur Respir J200832733ndash9
12 Dellinger RP Carlet JM Masur H et al Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock Intensive Care Med200430536ndash55
13 Metersky ML Ma A Houck PM et al Antibiotics for bacteremic pneumonia improved outcomes with macrolides but not uoroquinolones Chest 2007131466ndash73
14 Dunbar LM Wunderink RG Habib MP High-dose short-course levooxacin for community-acquired pneumonia a new treatment paradigm Clin Infect Dis 200337752ndash60
15 Matthaiou DK Ntani G An ESICM systematic review and meta-analysis of procalcitonin-guided antibiotic therapy algorithms in adult critically ill patients Intensive Care Med 201238940ndash9
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
17 Gruber PC Gomersall CD Joynt GM Avian inu-enza (H5N1) implications for intensive care Inten-sive Care Med 200632823ndash9
18 Belongia EA Irving SA Clinical characteristics and 30-day outcomes for inuenza A 2009 (H1N1) 2008ndash2009 (H1N1) and 2007ndash8 (H3N2) infections JAMA2010304(10)1091
19 Lee N Chan PKS Complications and outcomes of pandemic 2009 inuenza A (H1N1) virus infection in hospitalized adults how do they differ from those in seasonal inuenza J Infect Dis 20112031739ndash47
20 Kim SH Hong SB Corticosteroid treatment in critically ill patients with pandemic inuenza AH1N1 2009 infection analytic strategy using pro-pensity scores Am J Respir Crit Care Med 20111831207ndash14
21 Centers for Disease Control and Prevention (CDC) Bacterial coinfections in lung tissue specimens from
fatal cases of 2009 pandemic inuenza A (H1N1) ndash United States MayndashAugust 2009 MMWR 2009581071ndash4
22 Safdar N Dezfulian C Clinical and economic conse-quences of ventilator-associated pneumonia A sys-tematic review Crit Care Med 200533(10)2184ndash93
23 Shorr AF Sherner JH Invasive approaches to the diagnosis of ventilator-associated pneumonia A meta-analysis Crit Care Med 200533(1)46ndash53
24 Melsen WG Rovers MM Ventilator-associated pneumonia and mortality A systematic review of observational studies Crit Care Med 2009372709ndash18
25 Bekaert M Timsit JF Attributable mortality of ventilator-associated pneumonia A reappraisal using causal analysis Am J Respir Crit Care Med20111841133ndash9
26 CDC Healthcare Infection Control Practices AdvisoryCommittee Guidelines for preventing health-care-associated pneumonia 2003 Recommendations ofCDC and the Healthcare Infection Control PracticesAdvisory Committee Online Available httpwwwcdcgovmmwrpreviewmmwrhtmlrr5303a1htm
27 Cofn SE Klompas M SHEAIDSA practice recom-mendation strategies to prevent ventilator-associated pneumonia in acute care hospitals Infect Control
Hosp Epidemiol 200829S31ndash4028 Masterton RG Galloway A Guidelines for the man-
agement of hospital-acquired pneumonia in the UK Report of the Working Party on Hospital-Acquired Pneumonia of the British Society for Antimicrobial Chemotherapy J Antimicrob Chemother 2008625ndash34
29 VAP Guidelines Committee and the Canadian Critical Care Trials Group Comprehensive evidence-based clinical practice guidelines for ventilator-associated pneumonia prevention J Crit Care 200823126ndash37
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1717
428e2 Pneumonia
30 Torres A Ewig S Dening treating and preventing hospital acquired pneumonia European perspective Intensive Care Med 2009359ndash29
31 Frame RN Johnson MC Eichenhorn MS et al Active tuberculosis in the medical intensive care unit a 15-year retrospective analysis Crit Care Med 1987151012ndash14
32 National Collaborating Centre for Chronic Condi-tions Tuberculosis Clinical diagnosis and manage-ment of tuberculosis and measures for its prevention and control London Royal College of Physicians 2006
33 Small PM Fujiwara PI Management of tuberculosis in the United States N Engl J Med 2001345189ndash200
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
35 Centers for Disease Control and Prevention Guide-lines for preventing the transmission of Mycobacte-rium tuberculosis in health-care settings 2005 MMWR
2005541ndash11936 Hilbert G Gruson D Vargas F et al Noninvasive
ventilation in immunosuppressed patients with pul-monary inltrates fever and acute respiratory failure N Engl J Med 2001344481ndash7
37 Benson CA Kaplan JE Masur H Treating oppor-tunistic infections among HIV-infected adults and adolescents recommendations from CDC the National Institutes of Health and the HIV Medicine AssociationInfectious Diseases Society of America Clin Infect Dis 200540S131ndash235
38 Randall CJ Yarnold PR Schwartz DN et al Improve-ments in outcomes of acute respiratory failure for
patients with human immunodeciency virus-related Pneumocystis carinii pneumonia Am J Respir Crit Care Med 2000162393ndash8
39 Croda J Croda MG Neves A et al Benet of antiret-roviral therapy on survival of human immunode-ciency virus-infected patients admitted to an intensive care unit Crit Care Med 200937(5)1605
40 Centers for Disease Control Updated guidelines for the use of rifabutin or rifampicin for the treatment and prevention of tuberculosis among HIV-infected patients taking protease inhibitors or nonnucleoside reverse transcriptase inhibitors MMWR 200049185ndash9
41 Tamm M The lung in the immunocompromised patient Infectious complications part 2 Respiration199966199ndash207
42 Van der Bij W Speich R Management of cytomega-lovirus infection and disease after solid-organ trans-plantation Clin Infect Dis 200133(Suppl 1)S32ndash7
43 Schaumlfer P Tenschert W Cremaschi L et al Area under the viraemia curve versus absolute viral load utility for predicting symptomatic cytomegalovirus infections in kidney transplant patients J Med Virol20016585ndash9
44 Meyer-Koenig U Weidmann M Kirste G et al Cytomegalovirus infection in organ-transplant recip-ients diagnostic value of pp65 antigen test qualita-tive polymerase chain reaction (PCR) and quantitative
Taqman PCR Transplantation 2004771692ndash8
45 Pappas PG Rex JH Sobel JD Guidelines for treat-ment of candidiasis Clin Infect Dis 200438161ndash89
46 Stevens DA Kan VL Judson MA Practice guidelines for diseases caused by Aspergillus Clin Infect Dis200030696ndash709
47 Herbrecht R Denning DW Patterson TF Voricona-zole versus amphotericin B for primary therapy of invasive aspergillosis N Engl J Med 2002347408ndash15
48 Peek GJ Morcos S Cooper G The pleural cavity BMJ20003201318ndash21
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6

7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1317
426 Pneumonia
reaction are the most useful tests for demonstratingCMV disease Using thresholds of 10300 000ndash50200 000 positive circulating peripheral WBC the posi-tive predictive value for CMV-pp65 ranges from64 to 82 and the negative predictive value from70 to 954344 Treatment consists of intravenous gan-ciclovir for at least 14 days Foscarnet can be used if
ganciclovir fails
FUNGAL PNEUMONIA
Fungi are rare but important causes of pneumoniaThey can be divided into two main groups based on theimmune response required to combat infection withthese organisms Histoplasma blastomycosis coccidi-oidomycosis paracoccidioidomycosis and Cryptococcus require specic cell-mediated immunity for their controland thus in contrast to infections that are controlled byphagocytic activity the diseases caused by these organ-isms can occur in otherwise healthy individuals
although they cause much more severe illness inpatients with impaired cell-mediated immunity (egpatients infected with HIV and organ transplant recipi-ents) With the exception of Cryptococcus these organ-isms are rarely seen outside North America Aspergillus and Mucor spores are killed by non-immune phago-cytes and as a result these fungi rarely result in clinicalillness in patients with normal neutrophil numbers andfunction
CANDIDIASIS This is effectively a combination of the two types offungal infection in which impaired cell-mediatedimmunity predisposes to mucosal overgrowth withCandida but impaired phagocytic function or numbersis usually required before deep invasion of tissuesoccurs Primary Candida pneumonia (ie isolated lunginfection) is uncommon4145 and more commonly pul-monary lesions are only one manifestation of dissemi-nated candidiasis Even more common is benigncolonisation of the airway with Candida In mostreported cases of primary Candida pneumonia ampho-tericin B has been used In disseminated candidiasistreatment should be directed to treatment of dissemi-nated disease rather than Candida pneumonia per se45
INVASIVE ASPERGILLOSIS 46
This is a highly lethal condition in the immunocom-promised despite treatment and therefore investiga-tion and treatment should be prompt and aggressiveIt is associated with exposure to construction workDenitive diagnosis requires both histological evidenceof acute-angle branching septated non-pigmentedhyphae measuring 2ndash4 983221m in width and cultures yield-ing Aspergillus species from biopsy specimens ofinvolved organs Recovery of Aspergillus species fromrespiratory secretions in immunocompromised butnot immunocompetent patients may indicate invasive
disease with a positive predictive value as high as
depends on the degree of immunosuppression Inpatients with CD4+ T lymphocytes gt350 cells983221L theclinical presentation is similar to TB in non-HIV-infectedpatients although extrapulmonary disease is morecommon In patients with CD4+ T lymphocytes lt350cells983221L extrapulmonary disease (pleuritis pericardi-tis meningitis) is common Severely immunocompro-
mised patients (CD4+
T lymphocytes lt100 cells983221L)may present with severe systemic disease with highfever rapid progression and systemic sepsis In thesepatients lower and middle lobe disease is more commonmiliary disease is common and cavitation is lesscommon Sputum smears and culture may be positiveeven with a normal CXR
Response to treatment is usually rapid Managementof TB in HIV is complex owing to numerous druginteractions consultation with an expert in treatment ofHIV-related TB should be strongly considered Complexinteractions occur between rifamycins (eg rifampicinand rifabutin) and protease inhibitors and non-
nucleoside reverse transcriptase inhibitors used to treatpatients infected with HIV The choice of rifampicin orrifabutin depends on a number of factors includingthe unique and synergistic adverse effects for each indi-vidual combination of rifampicin and anti-HIV drugsand consultation with a physician with experiencein treating both TB and HIV is advised40 IDSA-recommended dosage adjustment for patients receivingantiretrovirals and rifabutin37 can be obtained viathe lsquolink pagersquo (httpwwwaiccuhkeduhkweb8Pneumonia20guidelineshtm) The optimal time forinitiating antiretroviral therapy in patients with TB iscontroversial Early therapy may decrease HIV disease
progression but may be associated with a high inci-dence of adverse effects and an immune reconstitutionreaction37
CMV PNEUMONITIS4142
Risk of infection is highest following allogeneic stemcell transplantation followed by lung transplantationpancreas transplantation and then liver heart and renaltransplantation and advanced AIDS If both the recipi-ent and the donor are seronegative then the risk of bothinfection and disease are negligible If the recipient is
seropositive the risk of infection is approximately 70but the risk of disease is only 20 regardless of theserostatus of the donor However if the recipient isseronegative and the donor is seropositive the risk ofdisease is 70 If steroid pulses and antilymphocyteglobulin are given for treatment of acute rejection therisk of developing disease is markedly increased Infec-tion may be the result of primary infection or reactiva-tion of latent infection It is clinically important butoften difcult to distinguish between CMV infectionand CMV disease and a denitive diagnosis can bemade only histologically Detection of CMV-pp65antigen in peripheral WBC and detection of CMV DNA
or RNA in the blood by quantitative polymerase chain
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1417
Parapneumonic effusion 427
needle aspiration or if there is debris within the uiddrainage using an intercostal drain The diagnosis isconrmed by aspiration of pus
TREATMENT The mainstay of treatment is drainage either by inter-costal drain or by surgical intervention Patients whopresent before the pus is loculated and a brinous peelhas formed on the lung can usually be treated bysimple drainage The combination with intrapleuralbrinolysis may be benecial Optimal surgical man-agement which consists of decortication (open or tho-racoscopic) is indicated if the empyema is moreadvanced or if simple drainage fails This is a majorprocedure and many patients with cardiac or chronicrespiratory disease will not tolerate it Alternatives forthese patients are instillation of thrombolytics into thepleural space or thoracostomy Antibiotics have onlyan adjunctive role Broad-spectrum antibiotic regimenswith anaerobic cover should be used until the resultsof microbiological analysis of the aspirated pus areavailable
AcknowledgementsAll tables and gures are reproduced from ICU web(wwwaiccuhkeduhkweb8) with permission of theauthors
80ndash90 in patients with leukaemia or bone marrowtransplant recipients Bronchoalveolar lavage withsmear culture and antigen detection has excellent spe-cicity and reasonably good positive predictive valuefor invasive aspergillosis in immunocompromisedpatients Although radiological features may give a clueto the diagnosis they are not sufciently specic to be
diagnosticIn acutely ill immunocompromised patients intrave-nous therapy should be initiated if there is suggestiveevidence of invasive aspergillosis while further investi-gations to conrm or refute the diagnosis are carriedout First-line therapy is voriconazole47 Echinocandinsand amphotericin are alternatives
PARAPNEUMONIC EFFUSION
This may be an uncomplicated effusion that resolveswith appropriate treatment of the underlying pneumo-nia or a complicated effusion that develops into an
empyema unless drained Complicated effusions tendto develop 7ndash14 days after initial uid formation Theyare characterised by increasing pleural uid volumecontinued fever and pleural uid of low pH (lt73) thatcontains a large number of neutrophils and may revealorganisms on Gram staining or culture An outline ofmanagement is given in Figure 365
EMPYEMA48
DEFINITION Collection of pus in the pleural space
AETIOLOGY Follows infection of the structures surrounding thepleural space including subdiaphragmatic structuresand chest trauma or may be associated with malig-nancy Anaerobic bacteria usually streptococci orGram-negative rods are responsible for 76 of cases
DIAGNOSIS The diagnosis is usually simple The patient is usuallyseptic and may have a productive cough and chest painThe chest X-ray may show features suggestive of apleural effusion and underlying consolidation but may
also show an abscess cavity with a uid level in whichcase CT scanning will be required to distinguishbetween an abscess and an empyema Ultrasound canbe useful to conrm the presence of uid in the pleuralspace and to determine whether it can be drained by
Figure 365 An approach to the management of
parapneumonic effusions
Parapneumonic effusion
gt 1 cm thick
on lateral decubitus
film
Pleural aspirate
turbid or purulent or
Gram stain +ve
Pleural aspirate
pH
Serial thoracocentesis Treat as empyemaObserve
No
gt72 lt70
70ndash72
No
Yes
Yes
httpwwwexpertconsultcomAccess the complete references list online at
1 American Thoracic Society and Infectious Diseases Society of America Guidelines for the manage-ment of adults with hospital-acquired ventilator-associated and healthcare associated pneumonia
Am J Respir Crit Care Med 2005171388ndash416
2 Mandell LA Wunderink RG Anzueto A et al Infec-tious Diseases Society of AmericaAmerican Tho-racic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin
Infect Dis 200744S27ndash72
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1517
428 Pneumonia
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1617
References 428e1
REFERENCES 1 American Thoracic Society and Infectious Diseases
Society of America Guidelines for the management of adults with hospital-acquired ventilator-associated and healthcare associated pneumonia Am J Respir Crit Care Med 2005171388ndash416
2 Mandell LA Wunderink RG Anzueto A et al Infec-tious Diseases Society of AmericaAmerican Tho-racic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744S27ndash72
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
4 Woodhead M Blasi F Ewig S et al Guidelines for the management of adult lower respiratory tract infections Eur Respir J 2005261138ndash80
5 Torres A Rello J Update in community-acquired and nosocomial pneumonia 2009 Am J Respir Crit
Care Med 2010181782ndash76 Van der Eerden MM Vlaspolder F de Graaff CS et
al Value of intensive diagnostic microbiological investigation in low- and high-risk patients with community-acquired pneumonia Eur J Clin Micro Infect Dis 200524241ndash9
7 Murdoch DR Nucleic acid amplication tests for the diagnosis of pneumonia Clin Infect Dis 2003361162ndash70
8 Blaschke AJ Interpreting assays for the detection of Streptococcus pneumonia Clin Infect Dis 201152(S4)S331ndash7
9 Rello J Lisboa T Lujan M Severity of pneumococcal
pneumonia associated with genomic bacterial load Chest 2009136832ndash4010 Azoulay E Bergeron A Polymerase chain reaction
for diagnosing pneumocystis pneumonia in non-HIV immunocompromised patients with pulmonary inl-trates Chest 2009135(3)655
11 Garcia-Vidal C Fernandez-Sabe N Carratala J Early mortality in patients with community-acquired pneumonia causes and risk factors Eur Respir J200832733ndash9
12 Dellinger RP Carlet JM Masur H et al Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock Intensive Care Med200430536ndash55
13 Metersky ML Ma A Houck PM et al Antibiotics for bacteremic pneumonia improved outcomes with macrolides but not uoroquinolones Chest 2007131466ndash73
14 Dunbar LM Wunderink RG Habib MP High-dose short-course levooxacin for community-acquired pneumonia a new treatment paradigm Clin Infect Dis 200337752ndash60
15 Matthaiou DK Ntani G An ESICM systematic review and meta-analysis of procalcitonin-guided antibiotic therapy algorithms in adult critically ill patients Intensive Care Med 201238940ndash9
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
17 Gruber PC Gomersall CD Joynt GM Avian inu-enza (H5N1) implications for intensive care Inten-sive Care Med 200632823ndash9
18 Belongia EA Irving SA Clinical characteristics and 30-day outcomes for inuenza A 2009 (H1N1) 2008ndash2009 (H1N1) and 2007ndash8 (H3N2) infections JAMA2010304(10)1091
19 Lee N Chan PKS Complications and outcomes of pandemic 2009 inuenza A (H1N1) virus infection in hospitalized adults how do they differ from those in seasonal inuenza J Infect Dis 20112031739ndash47
20 Kim SH Hong SB Corticosteroid treatment in critically ill patients with pandemic inuenza AH1N1 2009 infection analytic strategy using pro-pensity scores Am J Respir Crit Care Med 20111831207ndash14
21 Centers for Disease Control and Prevention (CDC) Bacterial coinfections in lung tissue specimens from
fatal cases of 2009 pandemic inuenza A (H1N1) ndash United States MayndashAugust 2009 MMWR 2009581071ndash4
22 Safdar N Dezfulian C Clinical and economic conse-quences of ventilator-associated pneumonia A sys-tematic review Crit Care Med 200533(10)2184ndash93
23 Shorr AF Sherner JH Invasive approaches to the diagnosis of ventilator-associated pneumonia A meta-analysis Crit Care Med 200533(1)46ndash53
24 Melsen WG Rovers MM Ventilator-associated pneumonia and mortality A systematic review of observational studies Crit Care Med 2009372709ndash18
25 Bekaert M Timsit JF Attributable mortality of ventilator-associated pneumonia A reappraisal using causal analysis Am J Respir Crit Care Med20111841133ndash9
26 CDC Healthcare Infection Control Practices AdvisoryCommittee Guidelines for preventing health-care-associated pneumonia 2003 Recommendations ofCDC and the Healthcare Infection Control PracticesAdvisory Committee Online Available httpwwwcdcgovmmwrpreviewmmwrhtmlrr5303a1htm
27 Cofn SE Klompas M SHEAIDSA practice recom-mendation strategies to prevent ventilator-associated pneumonia in acute care hospitals Infect Control
Hosp Epidemiol 200829S31ndash4028 Masterton RG Galloway A Guidelines for the man-
agement of hospital-acquired pneumonia in the UK Report of the Working Party on Hospital-Acquired Pneumonia of the British Society for Antimicrobial Chemotherapy J Antimicrob Chemother 2008625ndash34
29 VAP Guidelines Committee and the Canadian Critical Care Trials Group Comprehensive evidence-based clinical practice guidelines for ventilator-associated pneumonia prevention J Crit Care 200823126ndash37
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1717
428e2 Pneumonia
30 Torres A Ewig S Dening treating and preventing hospital acquired pneumonia European perspective Intensive Care Med 2009359ndash29
31 Frame RN Johnson MC Eichenhorn MS et al Active tuberculosis in the medical intensive care unit a 15-year retrospective analysis Crit Care Med 1987151012ndash14
32 National Collaborating Centre for Chronic Condi-tions Tuberculosis Clinical diagnosis and manage-ment of tuberculosis and measures for its prevention and control London Royal College of Physicians 2006
33 Small PM Fujiwara PI Management of tuberculosis in the United States N Engl J Med 2001345189ndash200
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
35 Centers for Disease Control and Prevention Guide-lines for preventing the transmission of Mycobacte-rium tuberculosis in health-care settings 2005 MMWR
2005541ndash11936 Hilbert G Gruson D Vargas F et al Noninvasive
ventilation in immunosuppressed patients with pul-monary inltrates fever and acute respiratory failure N Engl J Med 2001344481ndash7
37 Benson CA Kaplan JE Masur H Treating oppor-tunistic infections among HIV-infected adults and adolescents recommendations from CDC the National Institutes of Health and the HIV Medicine AssociationInfectious Diseases Society of America Clin Infect Dis 200540S131ndash235
38 Randall CJ Yarnold PR Schwartz DN et al Improve-ments in outcomes of acute respiratory failure for
patients with human immunodeciency virus-related Pneumocystis carinii pneumonia Am J Respir Crit Care Med 2000162393ndash8
39 Croda J Croda MG Neves A et al Benet of antiret-roviral therapy on survival of human immunode-ciency virus-infected patients admitted to an intensive care unit Crit Care Med 200937(5)1605
40 Centers for Disease Control Updated guidelines for the use of rifabutin or rifampicin for the treatment and prevention of tuberculosis among HIV-infected patients taking protease inhibitors or nonnucleoside reverse transcriptase inhibitors MMWR 200049185ndash9
41 Tamm M The lung in the immunocompromised patient Infectious complications part 2 Respiration199966199ndash207
42 Van der Bij W Speich R Management of cytomega-lovirus infection and disease after solid-organ trans-plantation Clin Infect Dis 200133(Suppl 1)S32ndash7
43 Schaumlfer P Tenschert W Cremaschi L et al Area under the viraemia curve versus absolute viral load utility for predicting symptomatic cytomegalovirus infections in kidney transplant patients J Med Virol20016585ndash9
44 Meyer-Koenig U Weidmann M Kirste G et al Cytomegalovirus infection in organ-transplant recip-ients diagnostic value of pp65 antigen test qualita-tive polymerase chain reaction (PCR) and quantitative
Taqman PCR Transplantation 2004771692ndash8
45 Pappas PG Rex JH Sobel JD Guidelines for treat-ment of candidiasis Clin Infect Dis 200438161ndash89
46 Stevens DA Kan VL Judson MA Practice guidelines for diseases caused by Aspergillus Clin Infect Dis200030696ndash709
47 Herbrecht R Denning DW Patterson TF Voricona-zole versus amphotericin B for primary therapy of invasive aspergillosis N Engl J Med 2002347408ndash15
48 Peek GJ Morcos S Cooper G The pleural cavity BMJ20003201318ndash21
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6

7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1417
Parapneumonic effusion 427
needle aspiration or if there is debris within the uiddrainage using an intercostal drain The diagnosis isconrmed by aspiration of pus
TREATMENT The mainstay of treatment is drainage either by inter-costal drain or by surgical intervention Patients whopresent before the pus is loculated and a brinous peelhas formed on the lung can usually be treated bysimple drainage The combination with intrapleuralbrinolysis may be benecial Optimal surgical man-agement which consists of decortication (open or tho-racoscopic) is indicated if the empyema is moreadvanced or if simple drainage fails This is a majorprocedure and many patients with cardiac or chronicrespiratory disease will not tolerate it Alternatives forthese patients are instillation of thrombolytics into thepleural space or thoracostomy Antibiotics have onlyan adjunctive role Broad-spectrum antibiotic regimenswith anaerobic cover should be used until the resultsof microbiological analysis of the aspirated pus areavailable
AcknowledgementsAll tables and gures are reproduced from ICU web(wwwaiccuhkeduhkweb8) with permission of theauthors
80ndash90 in patients with leukaemia or bone marrowtransplant recipients Bronchoalveolar lavage withsmear culture and antigen detection has excellent spe-cicity and reasonably good positive predictive valuefor invasive aspergillosis in immunocompromisedpatients Although radiological features may give a clueto the diagnosis they are not sufciently specic to be
diagnosticIn acutely ill immunocompromised patients intrave-nous therapy should be initiated if there is suggestiveevidence of invasive aspergillosis while further investi-gations to conrm or refute the diagnosis are carriedout First-line therapy is voriconazole47 Echinocandinsand amphotericin are alternatives
PARAPNEUMONIC EFFUSION
This may be an uncomplicated effusion that resolveswith appropriate treatment of the underlying pneumo-nia or a complicated effusion that develops into an
empyema unless drained Complicated effusions tendto develop 7ndash14 days after initial uid formation Theyare characterised by increasing pleural uid volumecontinued fever and pleural uid of low pH (lt73) thatcontains a large number of neutrophils and may revealorganisms on Gram staining or culture An outline ofmanagement is given in Figure 365
EMPYEMA48
DEFINITION Collection of pus in the pleural space
AETIOLOGY Follows infection of the structures surrounding thepleural space including subdiaphragmatic structuresand chest trauma or may be associated with malig-nancy Anaerobic bacteria usually streptococci orGram-negative rods are responsible for 76 of cases
DIAGNOSIS The diagnosis is usually simple The patient is usuallyseptic and may have a productive cough and chest painThe chest X-ray may show features suggestive of apleural effusion and underlying consolidation but may
also show an abscess cavity with a uid level in whichcase CT scanning will be required to distinguishbetween an abscess and an empyema Ultrasound canbe useful to conrm the presence of uid in the pleuralspace and to determine whether it can be drained by
Figure 365 An approach to the management of
parapneumonic effusions
Parapneumonic effusion
gt 1 cm thick
on lateral decubitus
film
Pleural aspirate
turbid or purulent or
Gram stain +ve
Pleural aspirate
pH
Serial thoracocentesis Treat as empyemaObserve
No
gt72 lt70
70ndash72
No
Yes
Yes
httpwwwexpertconsultcomAccess the complete references list online at
1 American Thoracic Society and Infectious Diseases Society of America Guidelines for the manage-ment of adults with hospital-acquired ventilator-associated and healthcare associated pneumonia
Am J Respir Crit Care Med 2005171388ndash416
2 Mandell LA Wunderink RG Anzueto A et al Infec-tious Diseases Society of AmericaAmerican Tho-racic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin
Infect Dis 200744S27ndash72
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1517
428 Pneumonia
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1617
References 428e1
REFERENCES 1 American Thoracic Society and Infectious Diseases
Society of America Guidelines for the management of adults with hospital-acquired ventilator-associated and healthcare associated pneumonia Am J Respir Crit Care Med 2005171388ndash416
2 Mandell LA Wunderink RG Anzueto A et al Infec-tious Diseases Society of AmericaAmerican Tho-racic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744S27ndash72
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
4 Woodhead M Blasi F Ewig S et al Guidelines for the management of adult lower respiratory tract infections Eur Respir J 2005261138ndash80
5 Torres A Rello J Update in community-acquired and nosocomial pneumonia 2009 Am J Respir Crit
Care Med 2010181782ndash76 Van der Eerden MM Vlaspolder F de Graaff CS et
al Value of intensive diagnostic microbiological investigation in low- and high-risk patients with community-acquired pneumonia Eur J Clin Micro Infect Dis 200524241ndash9
7 Murdoch DR Nucleic acid amplication tests for the diagnosis of pneumonia Clin Infect Dis 2003361162ndash70
8 Blaschke AJ Interpreting assays for the detection of Streptococcus pneumonia Clin Infect Dis 201152(S4)S331ndash7
9 Rello J Lisboa T Lujan M Severity of pneumococcal
pneumonia associated with genomic bacterial load Chest 2009136832ndash4010 Azoulay E Bergeron A Polymerase chain reaction
for diagnosing pneumocystis pneumonia in non-HIV immunocompromised patients with pulmonary inl-trates Chest 2009135(3)655
11 Garcia-Vidal C Fernandez-Sabe N Carratala J Early mortality in patients with community-acquired pneumonia causes and risk factors Eur Respir J200832733ndash9
12 Dellinger RP Carlet JM Masur H et al Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock Intensive Care Med200430536ndash55
13 Metersky ML Ma A Houck PM et al Antibiotics for bacteremic pneumonia improved outcomes with macrolides but not uoroquinolones Chest 2007131466ndash73
14 Dunbar LM Wunderink RG Habib MP High-dose short-course levooxacin for community-acquired pneumonia a new treatment paradigm Clin Infect Dis 200337752ndash60
15 Matthaiou DK Ntani G An ESICM systematic review and meta-analysis of procalcitonin-guided antibiotic therapy algorithms in adult critically ill patients Intensive Care Med 201238940ndash9
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
17 Gruber PC Gomersall CD Joynt GM Avian inu-enza (H5N1) implications for intensive care Inten-sive Care Med 200632823ndash9
18 Belongia EA Irving SA Clinical characteristics and 30-day outcomes for inuenza A 2009 (H1N1) 2008ndash2009 (H1N1) and 2007ndash8 (H3N2) infections JAMA2010304(10)1091
19 Lee N Chan PKS Complications and outcomes of pandemic 2009 inuenza A (H1N1) virus infection in hospitalized adults how do they differ from those in seasonal inuenza J Infect Dis 20112031739ndash47
20 Kim SH Hong SB Corticosteroid treatment in critically ill patients with pandemic inuenza AH1N1 2009 infection analytic strategy using pro-pensity scores Am J Respir Crit Care Med 20111831207ndash14
21 Centers for Disease Control and Prevention (CDC) Bacterial coinfections in lung tissue specimens from
fatal cases of 2009 pandemic inuenza A (H1N1) ndash United States MayndashAugust 2009 MMWR 2009581071ndash4
22 Safdar N Dezfulian C Clinical and economic conse-quences of ventilator-associated pneumonia A sys-tematic review Crit Care Med 200533(10)2184ndash93
23 Shorr AF Sherner JH Invasive approaches to the diagnosis of ventilator-associated pneumonia A meta-analysis Crit Care Med 200533(1)46ndash53
24 Melsen WG Rovers MM Ventilator-associated pneumonia and mortality A systematic review of observational studies Crit Care Med 2009372709ndash18
25 Bekaert M Timsit JF Attributable mortality of ventilator-associated pneumonia A reappraisal using causal analysis Am J Respir Crit Care Med20111841133ndash9
26 CDC Healthcare Infection Control Practices AdvisoryCommittee Guidelines for preventing health-care-associated pneumonia 2003 Recommendations ofCDC and the Healthcare Infection Control PracticesAdvisory Committee Online Available httpwwwcdcgovmmwrpreviewmmwrhtmlrr5303a1htm
27 Cofn SE Klompas M SHEAIDSA practice recom-mendation strategies to prevent ventilator-associated pneumonia in acute care hospitals Infect Control
Hosp Epidemiol 200829S31ndash4028 Masterton RG Galloway A Guidelines for the man-
agement of hospital-acquired pneumonia in the UK Report of the Working Party on Hospital-Acquired Pneumonia of the British Society for Antimicrobial Chemotherapy J Antimicrob Chemother 2008625ndash34
29 VAP Guidelines Committee and the Canadian Critical Care Trials Group Comprehensive evidence-based clinical practice guidelines for ventilator-associated pneumonia prevention J Crit Care 200823126ndash37
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1717
428e2 Pneumonia
30 Torres A Ewig S Dening treating and preventing hospital acquired pneumonia European perspective Intensive Care Med 2009359ndash29
31 Frame RN Johnson MC Eichenhorn MS et al Active tuberculosis in the medical intensive care unit a 15-year retrospective analysis Crit Care Med 1987151012ndash14
32 National Collaborating Centre for Chronic Condi-tions Tuberculosis Clinical diagnosis and manage-ment of tuberculosis and measures for its prevention and control London Royal College of Physicians 2006
33 Small PM Fujiwara PI Management of tuberculosis in the United States N Engl J Med 2001345189ndash200
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
35 Centers for Disease Control and Prevention Guide-lines for preventing the transmission of Mycobacte-rium tuberculosis in health-care settings 2005 MMWR
2005541ndash11936 Hilbert G Gruson D Vargas F et al Noninvasive
ventilation in immunosuppressed patients with pul-monary inltrates fever and acute respiratory failure N Engl J Med 2001344481ndash7
37 Benson CA Kaplan JE Masur H Treating oppor-tunistic infections among HIV-infected adults and adolescents recommendations from CDC the National Institutes of Health and the HIV Medicine AssociationInfectious Diseases Society of America Clin Infect Dis 200540S131ndash235
38 Randall CJ Yarnold PR Schwartz DN et al Improve-ments in outcomes of acute respiratory failure for
patients with human immunodeciency virus-related Pneumocystis carinii pneumonia Am J Respir Crit Care Med 2000162393ndash8
39 Croda J Croda MG Neves A et al Benet of antiret-roviral therapy on survival of human immunode-ciency virus-infected patients admitted to an intensive care unit Crit Care Med 200937(5)1605
40 Centers for Disease Control Updated guidelines for the use of rifabutin or rifampicin for the treatment and prevention of tuberculosis among HIV-infected patients taking protease inhibitors or nonnucleoside reverse transcriptase inhibitors MMWR 200049185ndash9
41 Tamm M The lung in the immunocompromised patient Infectious complications part 2 Respiration199966199ndash207
42 Van der Bij W Speich R Management of cytomega-lovirus infection and disease after solid-organ trans-plantation Clin Infect Dis 200133(Suppl 1)S32ndash7
43 Schaumlfer P Tenschert W Cremaschi L et al Area under the viraemia curve versus absolute viral load utility for predicting symptomatic cytomegalovirus infections in kidney transplant patients J Med Virol20016585ndash9
44 Meyer-Koenig U Weidmann M Kirste G et al Cytomegalovirus infection in organ-transplant recip-ients diagnostic value of pp65 antigen test qualita-tive polymerase chain reaction (PCR) and quantitative
Taqman PCR Transplantation 2004771692ndash8
45 Pappas PG Rex JH Sobel JD Guidelines for treat-ment of candidiasis Clin Infect Dis 200438161ndash89
46 Stevens DA Kan VL Judson MA Practice guidelines for diseases caused by Aspergillus Clin Infect Dis200030696ndash709
47 Herbrecht R Denning DW Patterson TF Voricona-zole versus amphotericin B for primary therapy of invasive aspergillosis N Engl J Med 2002347408ndash15
48 Peek GJ Morcos S Cooper G The pleural cavity BMJ20003201318ndash21
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6

7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1517
428 Pneumonia
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1617
References 428e1
REFERENCES 1 American Thoracic Society and Infectious Diseases
Society of America Guidelines for the management of adults with hospital-acquired ventilator-associated and healthcare associated pneumonia Am J Respir Crit Care Med 2005171388ndash416
2 Mandell LA Wunderink RG Anzueto A et al Infec-tious Diseases Society of AmericaAmerican Tho-racic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744S27ndash72
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
4 Woodhead M Blasi F Ewig S et al Guidelines for the management of adult lower respiratory tract infections Eur Respir J 2005261138ndash80
5 Torres A Rello J Update in community-acquired and nosocomial pneumonia 2009 Am J Respir Crit
Care Med 2010181782ndash76 Van der Eerden MM Vlaspolder F de Graaff CS et
al Value of intensive diagnostic microbiological investigation in low- and high-risk patients with community-acquired pneumonia Eur J Clin Micro Infect Dis 200524241ndash9
7 Murdoch DR Nucleic acid amplication tests for the diagnosis of pneumonia Clin Infect Dis 2003361162ndash70
8 Blaschke AJ Interpreting assays for the detection of Streptococcus pneumonia Clin Infect Dis 201152(S4)S331ndash7
9 Rello J Lisboa T Lujan M Severity of pneumococcal
pneumonia associated with genomic bacterial load Chest 2009136832ndash4010 Azoulay E Bergeron A Polymerase chain reaction
for diagnosing pneumocystis pneumonia in non-HIV immunocompromised patients with pulmonary inl-trates Chest 2009135(3)655
11 Garcia-Vidal C Fernandez-Sabe N Carratala J Early mortality in patients with community-acquired pneumonia causes and risk factors Eur Respir J200832733ndash9
12 Dellinger RP Carlet JM Masur H et al Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock Intensive Care Med200430536ndash55
13 Metersky ML Ma A Houck PM et al Antibiotics for bacteremic pneumonia improved outcomes with macrolides but not uoroquinolones Chest 2007131466ndash73
14 Dunbar LM Wunderink RG Habib MP High-dose short-course levooxacin for community-acquired pneumonia a new treatment paradigm Clin Infect Dis 200337752ndash60
15 Matthaiou DK Ntani G An ESICM systematic review and meta-analysis of procalcitonin-guided antibiotic therapy algorithms in adult critically ill patients Intensive Care Med 201238940ndash9
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
17 Gruber PC Gomersall CD Joynt GM Avian inu-enza (H5N1) implications for intensive care Inten-sive Care Med 200632823ndash9
18 Belongia EA Irving SA Clinical characteristics and 30-day outcomes for inuenza A 2009 (H1N1) 2008ndash2009 (H1N1) and 2007ndash8 (H3N2) infections JAMA2010304(10)1091
19 Lee N Chan PKS Complications and outcomes of pandemic 2009 inuenza A (H1N1) virus infection in hospitalized adults how do they differ from those in seasonal inuenza J Infect Dis 20112031739ndash47
20 Kim SH Hong SB Corticosteroid treatment in critically ill patients with pandemic inuenza AH1N1 2009 infection analytic strategy using pro-pensity scores Am J Respir Crit Care Med 20111831207ndash14
21 Centers for Disease Control and Prevention (CDC) Bacterial coinfections in lung tissue specimens from
fatal cases of 2009 pandemic inuenza A (H1N1) ndash United States MayndashAugust 2009 MMWR 2009581071ndash4
22 Safdar N Dezfulian C Clinical and economic conse-quences of ventilator-associated pneumonia A sys-tematic review Crit Care Med 200533(10)2184ndash93
23 Shorr AF Sherner JH Invasive approaches to the diagnosis of ventilator-associated pneumonia A meta-analysis Crit Care Med 200533(1)46ndash53
24 Melsen WG Rovers MM Ventilator-associated pneumonia and mortality A systematic review of observational studies Crit Care Med 2009372709ndash18
25 Bekaert M Timsit JF Attributable mortality of ventilator-associated pneumonia A reappraisal using causal analysis Am J Respir Crit Care Med20111841133ndash9
26 CDC Healthcare Infection Control Practices AdvisoryCommittee Guidelines for preventing health-care-associated pneumonia 2003 Recommendations ofCDC and the Healthcare Infection Control PracticesAdvisory Committee Online Available httpwwwcdcgovmmwrpreviewmmwrhtmlrr5303a1htm
27 Cofn SE Klompas M SHEAIDSA practice recom-mendation strategies to prevent ventilator-associated pneumonia in acute care hospitals Infect Control
Hosp Epidemiol 200829S31ndash4028 Masterton RG Galloway A Guidelines for the man-
agement of hospital-acquired pneumonia in the UK Report of the Working Party on Hospital-Acquired Pneumonia of the British Society for Antimicrobial Chemotherapy J Antimicrob Chemother 2008625ndash34
29 VAP Guidelines Committee and the Canadian Critical Care Trials Group Comprehensive evidence-based clinical practice guidelines for ventilator-associated pneumonia prevention J Crit Care 200823126ndash37
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1717
428e2 Pneumonia
30 Torres A Ewig S Dening treating and preventing hospital acquired pneumonia European perspective Intensive Care Med 2009359ndash29
31 Frame RN Johnson MC Eichenhorn MS et al Active tuberculosis in the medical intensive care unit a 15-year retrospective analysis Crit Care Med 1987151012ndash14
32 National Collaborating Centre for Chronic Condi-tions Tuberculosis Clinical diagnosis and manage-ment of tuberculosis and measures for its prevention and control London Royal College of Physicians 2006
33 Small PM Fujiwara PI Management of tuberculosis in the United States N Engl J Med 2001345189ndash200
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
35 Centers for Disease Control and Prevention Guide-lines for preventing the transmission of Mycobacte-rium tuberculosis in health-care settings 2005 MMWR
2005541ndash11936 Hilbert G Gruson D Vargas F et al Noninvasive
ventilation in immunosuppressed patients with pul-monary inltrates fever and acute respiratory failure N Engl J Med 2001344481ndash7
37 Benson CA Kaplan JE Masur H Treating oppor-tunistic infections among HIV-infected adults and adolescents recommendations from CDC the National Institutes of Health and the HIV Medicine AssociationInfectious Diseases Society of America Clin Infect Dis 200540S131ndash235
38 Randall CJ Yarnold PR Schwartz DN et al Improve-ments in outcomes of acute respiratory failure for
patients with human immunodeciency virus-related Pneumocystis carinii pneumonia Am J Respir Crit Care Med 2000162393ndash8
39 Croda J Croda MG Neves A et al Benet of antiret-roviral therapy on survival of human immunode-ciency virus-infected patients admitted to an intensive care unit Crit Care Med 200937(5)1605
40 Centers for Disease Control Updated guidelines for the use of rifabutin or rifampicin for the treatment and prevention of tuberculosis among HIV-infected patients taking protease inhibitors or nonnucleoside reverse transcriptase inhibitors MMWR 200049185ndash9
41 Tamm M The lung in the immunocompromised patient Infectious complications part 2 Respiration199966199ndash207
42 Van der Bij W Speich R Management of cytomega-lovirus infection and disease after solid-organ trans-plantation Clin Infect Dis 200133(Suppl 1)S32ndash7
43 Schaumlfer P Tenschert W Cremaschi L et al Area under the viraemia curve versus absolute viral load utility for predicting symptomatic cytomegalovirus infections in kidney transplant patients J Med Virol20016585ndash9
44 Meyer-Koenig U Weidmann M Kirste G et al Cytomegalovirus infection in organ-transplant recip-ients diagnostic value of pp65 antigen test qualita-tive polymerase chain reaction (PCR) and quantitative
Taqman PCR Transplantation 2004771692ndash8
45 Pappas PG Rex JH Sobel JD Guidelines for treat-ment of candidiasis Clin Infect Dis 200438161ndash89
46 Stevens DA Kan VL Judson MA Practice guidelines for diseases caused by Aspergillus Clin Infect Dis200030696ndash709
47 Herbrecht R Denning DW Patterson TF Voricona-zole versus amphotericin B for primary therapy of invasive aspergillosis N Engl J Med 2002347408ndash15
48 Peek GJ Morcos S Cooper G The pleural cavity BMJ20003201318ndash21
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6

7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1617
References 428e1
REFERENCES 1 American Thoracic Society and Infectious Diseases
Society of America Guidelines for the management of adults with hospital-acquired ventilator-associated and healthcare associated pneumonia Am J Respir Crit Care Med 2005171388ndash416
2 Mandell LA Wunderink RG Anzueto A et al Infec-tious Diseases Society of AmericaAmerican Tho-racic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744S27ndash72
3 Pneumonia Guidelines Committee of the BTS Stand-ards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in adults update 2009 Thorax200964(Suppl III)iii1ndash55
4 Woodhead M Blasi F Ewig S et al Guidelines for the management of adult lower respiratory tract infections Eur Respir J 2005261138ndash80
5 Torres A Rello J Update in community-acquired and nosocomial pneumonia 2009 Am J Respir Crit
Care Med 2010181782ndash76 Van der Eerden MM Vlaspolder F de Graaff CS et
al Value of intensive diagnostic microbiological investigation in low- and high-risk patients with community-acquired pneumonia Eur J Clin Micro Infect Dis 200524241ndash9
7 Murdoch DR Nucleic acid amplication tests for the diagnosis of pneumonia Clin Infect Dis 2003361162ndash70
8 Blaschke AJ Interpreting assays for the detection of Streptococcus pneumonia Clin Infect Dis 201152(S4)S331ndash7
9 Rello J Lisboa T Lujan M Severity of pneumococcal
pneumonia associated with genomic bacterial load Chest 2009136832ndash4010 Azoulay E Bergeron A Polymerase chain reaction
for diagnosing pneumocystis pneumonia in non-HIV immunocompromised patients with pulmonary inl-trates Chest 2009135(3)655
11 Garcia-Vidal C Fernandez-Sabe N Carratala J Early mortality in patients with community-acquired pneumonia causes and risk factors Eur Respir J200832733ndash9
12 Dellinger RP Carlet JM Masur H et al Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock Intensive Care Med200430536ndash55
13 Metersky ML Ma A Houck PM et al Antibiotics for bacteremic pneumonia improved outcomes with macrolides but not uoroquinolones Chest 2007131466ndash73
14 Dunbar LM Wunderink RG Habib MP High-dose short-course levooxacin for community-acquired pneumonia a new treatment paradigm Clin Infect Dis 200337752ndash60
15 Matthaiou DK Ntani G An ESICM systematic review and meta-analysis of procalcitonin-guided antibiotic therapy algorithms in adult critically ill patients Intensive Care Med 201238940ndash9
16 Waterer GW Rello J Management of community-acquired pneumonia in adults Am J Respir Crit Care Med 2011183157ndash64
17 Gruber PC Gomersall CD Joynt GM Avian inu-enza (H5N1) implications for intensive care Inten-sive Care Med 200632823ndash9
18 Belongia EA Irving SA Clinical characteristics and 30-day outcomes for inuenza A 2009 (H1N1) 2008ndash2009 (H1N1) and 2007ndash8 (H3N2) infections JAMA2010304(10)1091
19 Lee N Chan PKS Complications and outcomes of pandemic 2009 inuenza A (H1N1) virus infection in hospitalized adults how do they differ from those in seasonal inuenza J Infect Dis 20112031739ndash47
20 Kim SH Hong SB Corticosteroid treatment in critically ill patients with pandemic inuenza AH1N1 2009 infection analytic strategy using pro-pensity scores Am J Respir Crit Care Med 20111831207ndash14
21 Centers for Disease Control and Prevention (CDC) Bacterial coinfections in lung tissue specimens from
fatal cases of 2009 pandemic inuenza A (H1N1) ndash United States MayndashAugust 2009 MMWR 2009581071ndash4
22 Safdar N Dezfulian C Clinical and economic conse-quences of ventilator-associated pneumonia A sys-tematic review Crit Care Med 200533(10)2184ndash93
23 Shorr AF Sherner JH Invasive approaches to the diagnosis of ventilator-associated pneumonia A meta-analysis Crit Care Med 200533(1)46ndash53
24 Melsen WG Rovers MM Ventilator-associated pneumonia and mortality A systematic review of observational studies Crit Care Med 2009372709ndash18
25 Bekaert M Timsit JF Attributable mortality of ventilator-associated pneumonia A reappraisal using causal analysis Am J Respir Crit Care Med20111841133ndash9
26 CDC Healthcare Infection Control Practices AdvisoryCommittee Guidelines for preventing health-care-associated pneumonia 2003 Recommendations ofCDC and the Healthcare Infection Control PracticesAdvisory Committee Online Available httpwwwcdcgovmmwrpreviewmmwrhtmlrr5303a1htm
27 Cofn SE Klompas M SHEAIDSA practice recom-mendation strategies to prevent ventilator-associated pneumonia in acute care hospitals Infect Control
Hosp Epidemiol 200829S31ndash4028 Masterton RG Galloway A Guidelines for the man-
agement of hospital-acquired pneumonia in the UK Report of the Working Party on Hospital-Acquired Pneumonia of the British Society for Antimicrobial Chemotherapy J Antimicrob Chemother 2008625ndash34
29 VAP Guidelines Committee and the Canadian Critical Care Trials Group Comprehensive evidence-based clinical practice guidelines for ventilator-associated pneumonia prevention J Crit Care 200823126ndash37
7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1717
428e2 Pneumonia
30 Torres A Ewig S Dening treating and preventing hospital acquired pneumonia European perspective Intensive Care Med 2009359ndash29
31 Frame RN Johnson MC Eichenhorn MS et al Active tuberculosis in the medical intensive care unit a 15-year retrospective analysis Crit Care Med 1987151012ndash14
32 National Collaborating Centre for Chronic Condi-tions Tuberculosis Clinical diagnosis and manage-ment of tuberculosis and measures for its prevention and control London Royal College of Physicians 2006
33 Small PM Fujiwara PI Management of tuberculosis in the United States N Engl J Med 2001345189ndash200
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
35 Centers for Disease Control and Prevention Guide-lines for preventing the transmission of Mycobacte-rium tuberculosis in health-care settings 2005 MMWR
2005541ndash11936 Hilbert G Gruson D Vargas F et al Noninvasive
ventilation in immunosuppressed patients with pul-monary inltrates fever and acute respiratory failure N Engl J Med 2001344481ndash7
37 Benson CA Kaplan JE Masur H Treating oppor-tunistic infections among HIV-infected adults and adolescents recommendations from CDC the National Institutes of Health and the HIV Medicine AssociationInfectious Diseases Society of America Clin Infect Dis 200540S131ndash235
38 Randall CJ Yarnold PR Schwartz DN et al Improve-ments in outcomes of acute respiratory failure for
patients with human immunodeciency virus-related Pneumocystis carinii pneumonia Am J Respir Crit Care Med 2000162393ndash8
39 Croda J Croda MG Neves A et al Benet of antiret-roviral therapy on survival of human immunode-ciency virus-infected patients admitted to an intensive care unit Crit Care Med 200937(5)1605
40 Centers for Disease Control Updated guidelines for the use of rifabutin or rifampicin for the treatment and prevention of tuberculosis among HIV-infected patients taking protease inhibitors or nonnucleoside reverse transcriptase inhibitors MMWR 200049185ndash9
41 Tamm M The lung in the immunocompromised patient Infectious complications part 2 Respiration199966199ndash207
42 Van der Bij W Speich R Management of cytomega-lovirus infection and disease after solid-organ trans-plantation Clin Infect Dis 200133(Suppl 1)S32ndash7
43 Schaumlfer P Tenschert W Cremaschi L et al Area under the viraemia curve versus absolute viral load utility for predicting symptomatic cytomegalovirus infections in kidney transplant patients J Med Virol20016585ndash9
44 Meyer-Koenig U Weidmann M Kirste G et al Cytomegalovirus infection in organ-transplant recip-ients diagnostic value of pp65 antigen test qualita-tive polymerase chain reaction (PCR) and quantitative
Taqman PCR Transplantation 2004771692ndash8
45 Pappas PG Rex JH Sobel JD Guidelines for treat-ment of candidiasis Clin Infect Dis 200438161ndash89
46 Stevens DA Kan VL Judson MA Practice guidelines for diseases caused by Aspergillus Clin Infect Dis200030696ndash709
47 Herbrecht R Denning DW Patterson TF Voricona-zole versus amphotericin B for primary therapy of invasive aspergillosis N Engl J Med 2002347408ndash15
48 Peek GJ Morcos S Cooper G The pleural cavity BMJ20003201318ndash21
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6

7172019 Pneumonia
httpslidepdfcomreaderfullpneumonia-568f5d4002e1c 1717
428e2 Pneumonia
30 Torres A Ewig S Dening treating and preventing hospital acquired pneumonia European perspective Intensive Care Med 2009359ndash29
31 Frame RN Johnson MC Eichenhorn MS et al Active tuberculosis in the medical intensive care unit a 15-year retrospective analysis Crit Care Med 1987151012ndash14
32 National Collaborating Centre for Chronic Condi-tions Tuberculosis Clinical diagnosis and manage-ment of tuberculosis and measures for its prevention and control London Royal College of Physicians 2006
33 Small PM Fujiwara PI Management of tuberculosis in the United States N Engl J Med 2001345189ndash200
34 American Thoracic Society CDC and Infectious Dis-eases Society of America Treatment of tuberculosis Am J Respir Crit Care Med 2003167603ndash62
35 Centers for Disease Control and Prevention Guide-lines for preventing the transmission of Mycobacte-rium tuberculosis in health-care settings 2005 MMWR
2005541ndash11936 Hilbert G Gruson D Vargas F et al Noninvasive
ventilation in immunosuppressed patients with pul-monary inltrates fever and acute respiratory failure N Engl J Med 2001344481ndash7
37 Benson CA Kaplan JE Masur H Treating oppor-tunistic infections among HIV-infected adults and adolescents recommendations from CDC the National Institutes of Health and the HIV Medicine AssociationInfectious Diseases Society of America Clin Infect Dis 200540S131ndash235
38 Randall CJ Yarnold PR Schwartz DN et al Improve-ments in outcomes of acute respiratory failure for
patients with human immunodeciency virus-related Pneumocystis carinii pneumonia Am J Respir Crit Care Med 2000162393ndash8
39 Croda J Croda MG Neves A et al Benet of antiret-roviral therapy on survival of human immunode-ciency virus-infected patients admitted to an intensive care unit Crit Care Med 200937(5)1605
40 Centers for Disease Control Updated guidelines for the use of rifabutin or rifampicin for the treatment and prevention of tuberculosis among HIV-infected patients taking protease inhibitors or nonnucleoside reverse transcriptase inhibitors MMWR 200049185ndash9
41 Tamm M The lung in the immunocompromised patient Infectious complications part 2 Respiration199966199ndash207
42 Van der Bij W Speich R Management of cytomega-lovirus infection and disease after solid-organ trans-plantation Clin Infect Dis 200133(Suppl 1)S32ndash7
43 Schaumlfer P Tenschert W Cremaschi L et al Area under the viraemia curve versus absolute viral load utility for predicting symptomatic cytomegalovirus infections in kidney transplant patients J Med Virol20016585ndash9
44 Meyer-Koenig U Weidmann M Kirste G et al Cytomegalovirus infection in organ-transplant recip-ients diagnostic value of pp65 antigen test qualita-tive polymerase chain reaction (PCR) and quantitative
Taqman PCR Transplantation 2004771692ndash8
45 Pappas PG Rex JH Sobel JD Guidelines for treat-ment of candidiasis Clin Infect Dis 200438161ndash89
46 Stevens DA Kan VL Judson MA Practice guidelines for diseases caused by Aspergillus Clin Infect Dis200030696ndash709
47 Herbrecht R Denning DW Patterson TF Voricona-zole versus amphotericin B for primary therapy of invasive aspergillosis N Engl J Med 2002347408ndash15
48 Peek GJ Morcos S Cooper G The pleural cavity BMJ20003201318ndash21
49 Meduri GU Chastre J The standardization of bron-choscopic techniques for ventilator-associated pneu-monia Chest 1992102557Sndash64S
50 Lorente L Blot S New issues and controversies in the prevention of ventilator-associated pneumonia Am
J Respir Crit Care Med 2010182870ndash6