
Hospital-Acquired Bacterial Pneumonia & Ventilator ... · Hospital-Acquired Bacterial Pneumonia &...
37
Hospital-Acquired Bacterial Pneumonia & Ventilator-Associated Bacterial Pneumonia October 12, 2012 Joseph G. Toerner, MD, MPH Associate Director for Medical Affairs Office of Antimicrobial Products CDER, FDA
Transcript of Hospital-Acquired Bacterial Pneumonia & Ventilator ... · Hospital-Acquired Bacterial Pneumonia &...
Hospital-Acquired Bacterial Pneumonia & Ventilator-Associated Bacterial Pneumonia
October 12, 2012
Joseph G. Toerner, MD, MPH Associate Director for Medical Affairs
Office of Antimicrobial Products CDER, FDA
∗ Collaborative efforts and public-private partnerships in antibacterial drug development ∗ CTTI’s “Accelerating Antibacterial Drug Development” ∗ Brookings Council on Antibacterial Drug Development ∗ Biomarkers Consortium of the FNIH for CABP & ABSSSI Bring together the thought-leaders in the field to move drug
development forward
∗ Potential for synergy with current ongoing efforts ∗ FNIH is currently in process for development of an endpoint
for pneumonia (CABP)
Issues in Clinical Trial Design for Drug Development to Treat Patients with HABP/VABP

∗ Background information ∗ Workshop/Draft Guidance/AIDAC Nov 2011
∗ Overview of outcome assessments ∗ Biomarkers, clinician-reported outcomes, clinical endpoints
∗ Management of patients with HABP/VABP ∗ Clinical care of patients
∗ Design strategies and operational efficiency for HABP/VABP ∗ Feasibility issues
∗ Successful approaches to endpoint development ∗ FNIH Biomarkers Consortium for CABP
Summary for Today’s Presentations HABP/VABP
Highlights of the Workshop Discussions ∗ Evaluating drugs for HABP/VABP challenging
∗ Efforts to minimize hospital-acquired infections: CMS, Joint Commission
∗ Multicenter trials: bacterial etiologies and ICU management strategies differs among centers
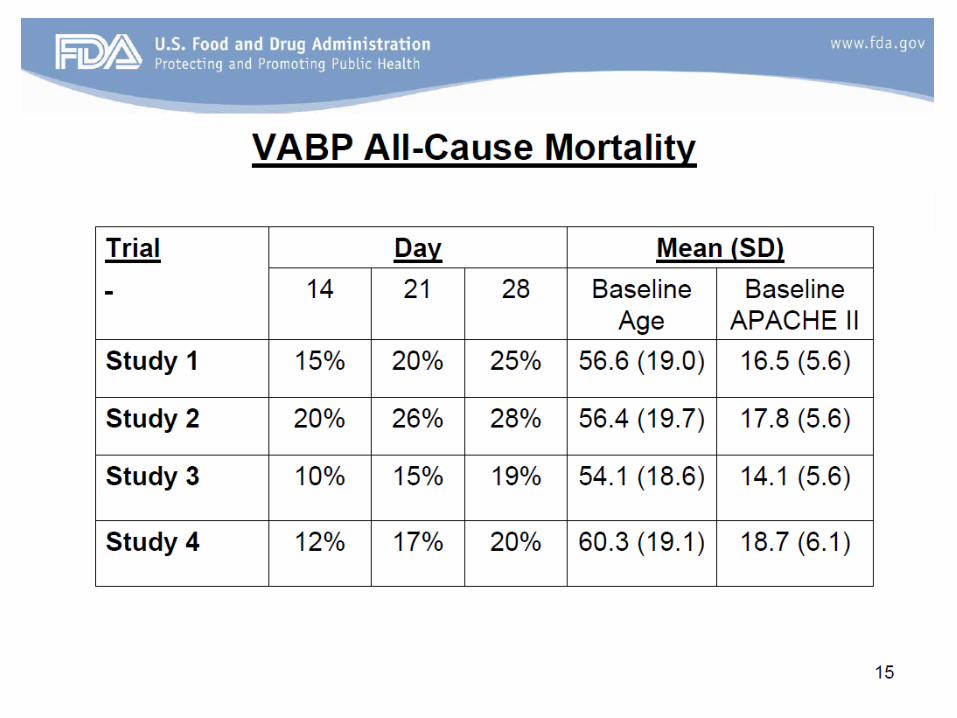
∗ All-cause mortality endpoint discussed ∗ Treatment effect from historical studies ∗ Concerns with evaluating mortality
∗ Non-respiratory events contributing to mortality ∗ Timing: 14 days – 28 days
FDA Co-Sponsored Workshop for HAPB/VABP
Spring 2009: Proceedings: CID Aug 2010 (51) Suppl 1

Highlights of the Workshop Discussions ∗ Non-mortality endpoints discussed
∗ “days in ICU”; “days on ventilator”, “PaO2/FiO2 ratio” ∗ Lack of consistent evaluation of clinical endpoints in trials:
treatment effects unknown ∗ Definition of HABP and VABP for enrollment
∗ Enrich for bacterial disease (CPIS scores for VABP) ∗ Analysis population: micro-ITT (easier for VABP) ∗ Role of quantitative cultures in mechanical ventilation
∗ Consortia or cooperative groups could enhance protocol development and implementation
FDA Co-Sponsored Workshop for HAPB/VABP
∗ Draft Guidance issued November 29, 2010 ∗ Enrollment criteria
∗ Sufficiently ill trial population, mortality ~ 20% ∗ Adequate period of hospitalization/ventilation (e.g. > 48 hours) ∗ New radiographic findings ∗ Clinical criteria (e.g. fever, cough, dyspnea, hypoxemia) ∗ Microbiologic criteria
Draft Guidance for HAPB/VABP

∗ Efficacy Considerations ∗ All-cause mortality primary endpoint
∗ 28-days after randomization ∗ Active-control NI trial design: M1 20% ∗ Appendix justification NI margin: NI margin 10% ∗ Sample size: 481 per arm (AIDAC background)
∗ Recommend only VABP or only HABP trials ∗ Efficacy/safety demonstrated in VABP support indication for
both HABP and VABP ∗ Efficacy/safety demonstrated in HABP support indication for
HABP
Draft Guidance for HAPB/VABP

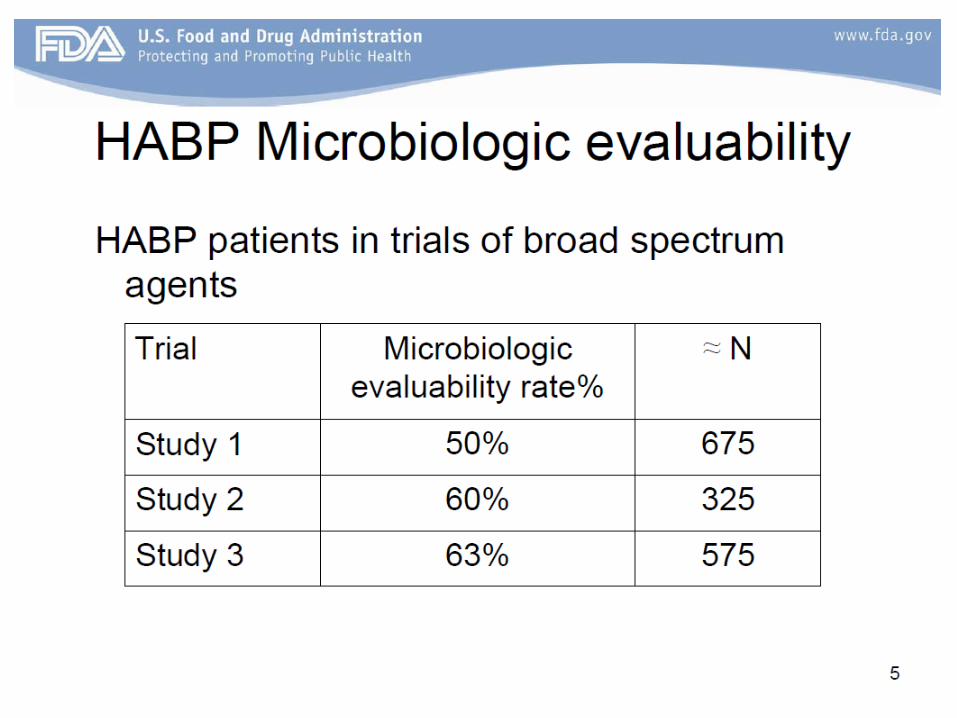
∗ Efficacy Considerations, cont. ∗ Micro-ITT analysis population (70% micro-evaluable VABP) ∗ Historical trials offered no data on clinical signs/symptoms
∗ Other Considerations ∗ Exclude patients with receipt of prior antibacterial drugs ∗ Acknowledged empirical use of concomitant antibacterial
drugs ∗ Avoid concomitant antibacterial drugs with overlapping activity
∗ Trials in patients with unmet need
Draft Guidance for HAPB/VABP

∗ 14 responses submitted to the docket ∗ Most from industry, several from individuals
∗ 9 areas of criticism ∗ In general, guidance is not practical ∗ Efficacy endpoint: concern with all-cause mortality ∗ Statistical considerations: too conservative ∗ Comparator antibacterial drugs ∗ Issue of prior antibacterial drugs ∗ Trial population considerations ∗ Clinical microbiology considerations ∗ Entry criteria concerns ∗ Trials in patients with unmet need
Comment to the Draft Guidance for HAPB/VABP

∗ 14 responses submitted to the docket ∗ Most from industry, several from individuals
∗ Nov 4, 2011 AIDAC addressed 5 areas of criticism ∗ In general, guidance is not practical ∗ Efficacy endpoint: concern with all-cause mortality ∗ Statistical considerations: too conservative ∗ Comparator antibacterial drugs ∗ Issue of prior antibacterial drugs ∗ Trial population considerations ∗ Clinical microbiology considerations ∗ Entry criteria concerns ∗ Trials in patients with unmet need
Comment to the Draft Guidance for HAPB/VABP
∗ In general, guidance is not practical ∗ Efficacy endpoint: all-cause mortality
∗ Advances in ICU care, mortality < 20% ∗ Requirement for micro-ITT analysis population: trials too large ∗ Uncertainty about the timing of day 28 all-cause mortality
Comment to the Draft Guidance for HAPB/VABP

∗ Statistical considerations
∗ Extensive discounting to arrive at NI margin ∗ 12.5% NI margin supportable
∗ (sample size = approx. 320 per arm) ∗ Questions about choice of OR metric of 1.67 ∗ Sample size estimates: trials too large
Comment to the Draft Guidance for HAPB/VABP

∗ Issue of prior antibacterial drugs ∗ Excluding prior use unjustified and impractical ∗ Perioperative antibacterial drugs commonly used in
trauma/surgical patients
Comment to the Draft Guidance for HAPB/VABP

∗ Discussion about these topics: ∗ Limitations and merits of a single trial plus supportive
evidence ∗ Discuss NI margin of 10% and use of the odds ratio ∗ Preferred timing of the all-cause mortality endpoint ∗ Prior antibacterial drug administration
November 4, 2011 AIDAC on HAPB/VABP
∗ Limitations and merits of a single trial plus supportive evidence
In general, the committee agreed that a single trial can be used to support efficacy and safety in the evaluation of a new antibacterial drug for the treatment of HABP/VABP
Types of supportive data: ∗ Another trial in another indication (cIAI, CABP. ABSSSI) ∗ Nonclinical data (animal models, PK/PD)
November 4, 2011 AIDAC on HAPB/VABP
∗ Discuss NI margin of 10% and use of the odds ratio
∗ An approach without having absolute certainty with a >20% mortality in the control group ∗ Addresses the “moving target” of mortality
∗ Some concern about higher sample sizes
November 4, 2011 AIDAC on HAPB/VABP

∗ Prior antibacterial drug administration The use of antibacterial drugs for the current episode of
HABP/VABP in the 24 hours prior to enrollment appears to be acceptable along with efforts to minimize patients that receive prior effective antibacterial drugs.
November 4, 2011 AIDAC on HAPB/VABP
18
∗ Preferred timing of the all-cause mortality endpoint The timing of the all-cause mortality endpoint should be
between 14 and 28 days
Other comments during discussion about mortality endpoint ∗ Patients can be maintained in ICU setting “artificially” ∗ Should look at other clinical endpoints ∗ Primary endpoint should be clinically-based ∗ PK/PD can help define clinical endpoint ∗ Look at endpoints earlier in therapy (e.g., CABP)
November 4, 2011 AIDAC on HAPB/VABP

∗ All-cause mortality endpoint ∗ Always evaluate mortality in trials ∗ Difficulty in planning for trials based on an anticipated rate of
mortality in the control group ∗ Deaths may be due to other co-morbid conditions
∗ Clinical endpoint ∗ Work done in other areas have established new efficacy
endpoint: CABP and ABSSSI ∗ Efforts to identify a new clinical endpoint or biomarker in
HABP/VABP may be valuable
HAPB/VABP Current Thinking
∗ Prior antibacterial drug therapy ∗ A rationale to permit use of prior therapy for the current
episode of HABP/VABP for up to 24 hours prior to enrollment ∗ AIDAC discussion in the context of a 28-day all-cause mortality
endpoint ∗ Are anticipatory informed consent procedures upon hospital or
ICU admission possible? ∗ Alleviate the concerns about an effect of prior effective therapy
HAPB/VABP Current Thinking
21
The document outlines a format to approach the FDA with new endpoint or biomarker development
22
∗ Endpoints ∗ All-cause mortality: feasibility ∗ Clinical endpoints
∗ Ways to identify a clinical endpoint ∗ FNIH approach successful for CABP and work continues
∗ May be possible to use a similar approach for HABP/VABP
∗ Clinical Trial Design ∗ Operational efficiencies ∗ HABP & VABP patients together in one trial or separate
evaluation ∗ Potential role of clinical trial networks
HAPB/VABP Summary for Today’s Discussion
Back Up
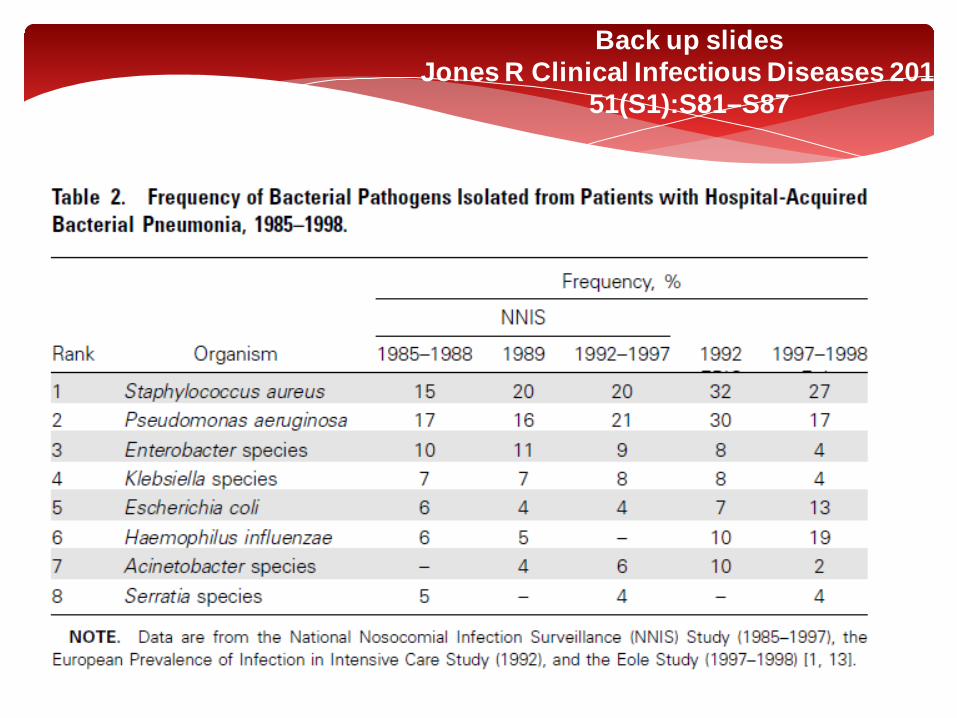
Back up slides Jones R Clinical Infectious Diseases 2010;
51(S1):S81–S87
25
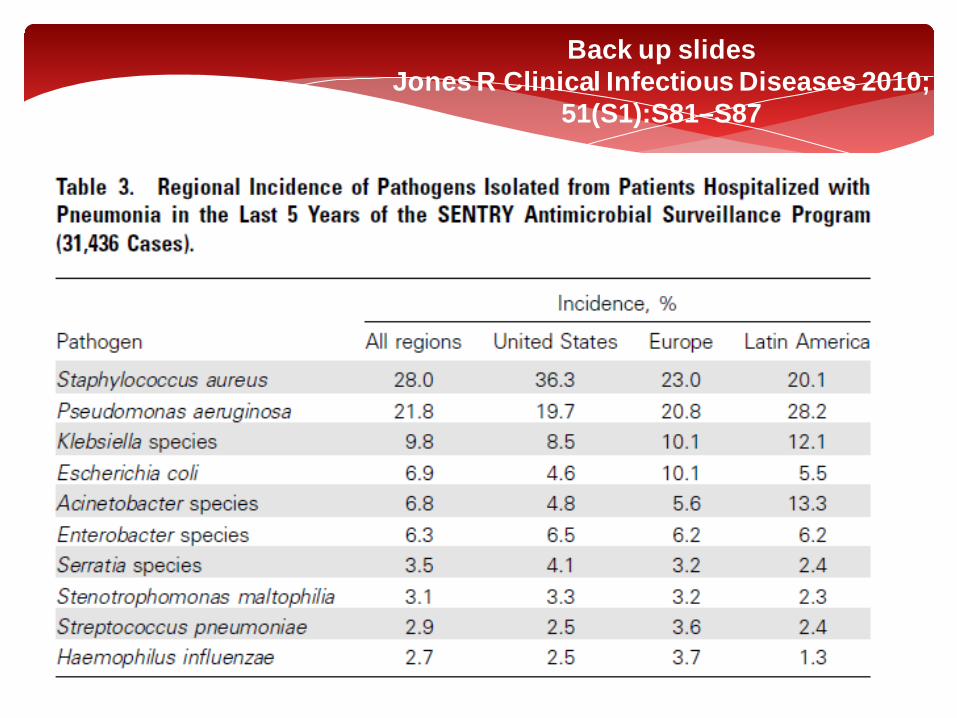
Back up slides Jones R Clinical Infectious Diseases 2010;
51(S1):S81–S87

26
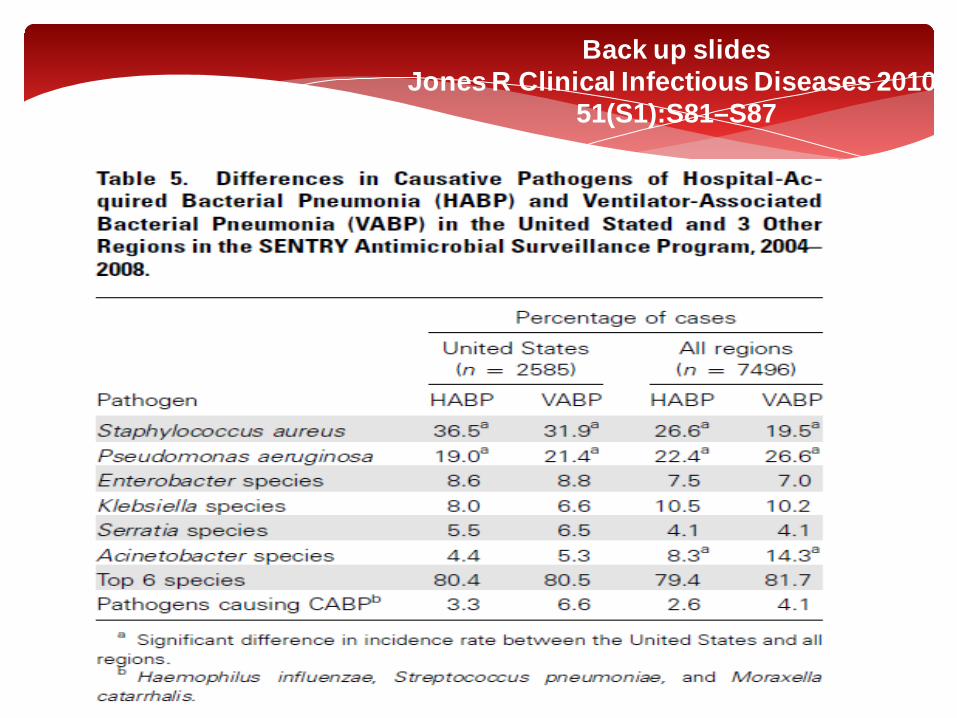
Back up slides Jones R Clinical Infectious Diseases 2010;
51(S1):S81–S87
Back up slides Jones R Clinical Infectious Diseases 2010;
51(S1):S81–S87

Back up slides Jones R Clinical Infectious Diseases 2010;
51(S1):S81–S87

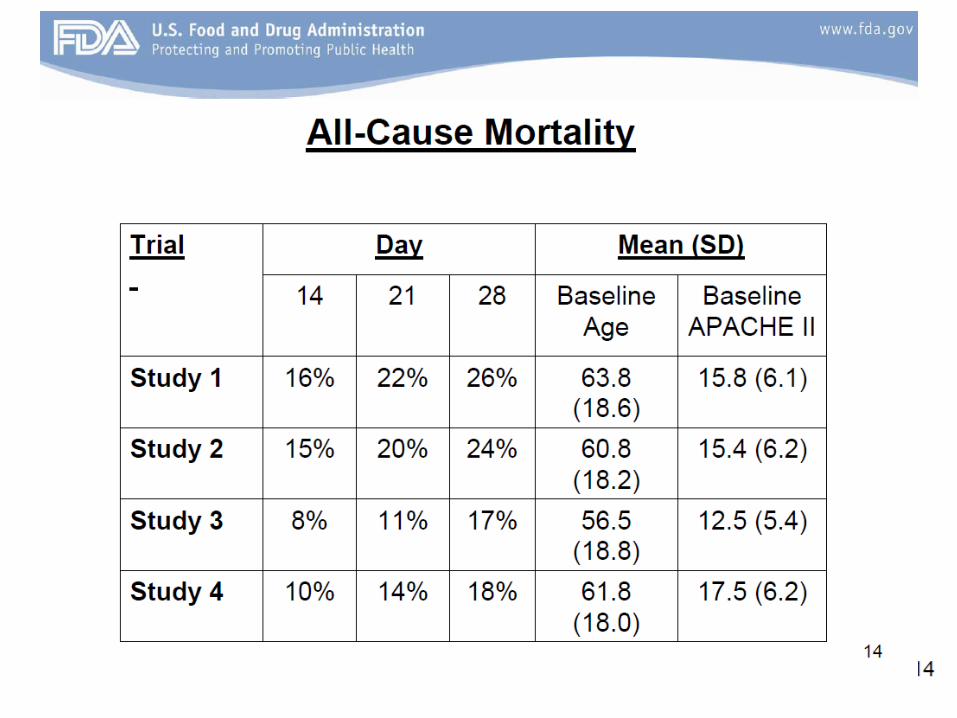
Back up slides HABP/VABP AIDAC Backgrounder

Back up slides HABP/VABP AIDAC Backgrounder
31
Back up slides HABP/VABP AIDAC Backgrounder




















![Ventilator Associated Pneumonia Treatment[1]](https://static.fdocuments.us/doc/165x107/577d23921a28ab4e1e9a2bfc/ventilator-associated-pneumonia-treatment1.jpg)