Pneumonia
24
Pneumonia • Acute inflammation of lung parenchyma • Inflammatory infiltrate in alveoli ( = consolidation)
description
Community Acquired Pneumonia
Transcript of Pneumonia

Pneumonia• Acute inflammation of lung parenchyma
• Inflammatory infiltrate in alveoli
( = consolidation)

CLASSIFICATION:
Aetiology.
Morpological class. - Bronchopneumonia vs. lobar
pneumonia.
Community acquired vs hospital acquired
(nosocomial) infection.
The patient's immune status.

AETIOLOGY
• Bacteria, viruses, fungi, mycoplasma,chlamydia.
• Microbiological identification of organism often
not possible.

• Previously healthy individual:
→ S. pneumoniae
• Pre-existing viral infection
→ Staph. aureus or S. pneumoniae
• Chronic bronchitis
→ Haemophilus influenzae or S. pneumoniae
• AIDS
→ Pneumocystis carinii, cytomegalovirus, TB

Morphological classification
- Bronchopneumonia
- Lobar pneumonia


Bronchopneumonia:
• Infants + young children and the elderly.
• Usually secondary to other conditions associated with local and
general defence mechanisms:
- viral infections (influenza, measles)
- aspiration of food or vomitus
- obstruction of a bronchus (foreign body or neoplasm)
- inhalation of irritant gases
- major surgery
- chronic debilitating diseases, malnutrition

Lobar pneumonia:
S. pneumoniae.
Previously healthy individuals.
Abrupt onset.
Unilateral stabbing chest pain on inspiration (due to fibrinous pleurisy).

Pathology of lobar pneumonia:
4 phases:
Congestion
Lasts < 24 hours: Alveoli filled with
oedema fluid and bacteria.

Red hepatization
• Firm, 'meaty' and airless appearance of lung.
• Alveolar capillary dilatation.
• Strands of fibrin extending from one alveolus to
another via inter-alveolar pores of Kohn.
• Also neutrophils in alveoli.
• Pleura: Fibrinous exudate.

Grey hepatization
Less hyperaemia.
Macrophages, neutrophils + fibrin

Resolution
- Lysis and removal of fibrin via sputum +lymphatics.
- Begins after 8-9 days (without antibiotics).
- Sudden improvement of patient's condition.

Complications of lobar pneumonia
1. Abscess formation
2. Empyema
3. Failure of resolution ⇒ intra-alveolar scarring
('carnification') ⇒ permanent loss of ventilatory
function of affected parts of lung.
4. Bacteraemia:
- Infective endocarditis
- Cerebral abscess / meningitis
- Septic arthritis

Klebsiella pneumoniae
• Common inhabitant of oral cavity (poor
oral hygiene).
• Lobar pneumonia in the elderly, diabetics,
alcoholics (aspiration of saliva).

Community acquired vs. nosocomial infection
Nosocomial infection:
- Often patients in ICU
- ↓ Local resistance to infection in lungs
- Intubation of respiratory tract
- Altered normal flora due to antibiotics
- E.coli, Klebsiella, Proteus, Pseudomonas,
Staph. aureus.

Immune status
Infection by usually non-pathogenic organisms
('opportunistic infection')
- Pneumocystis carinii
- Other fungi
- Cytomegalovirus (CMV)

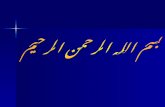
Fig. A viral pneumonia with interstitial lymphocyticinfiltrates. Note that there is no alveolar exudate. Thus, the patient with this type of pneumonia will probably not have a productive cough.

The most common causes for viral pneumonia are:
• Influenza
• Parainfluenza
• Adenovirus
• Respiratory syncytial virus (RSV)
- appears mostly in children
• Cytomegalovirus
- in immunocompromised hosts.

Fig. RSV accounts for many cases of pneumonia in children under 2 years, and can be a cause for death in infants 1 to 6 months of age or older.

DEFINITION:
Localised area of suppuration and tissue necrosis.
Lung abscess

Fig. Chest X-ray. Abscess. Note air-fluid level

Aetiopathogenesis
• Aspiration of infected oropharyngeal
contents / vomitus.
NB: Poor oral hygiene and sepsis.
Risk of aspiration:
- Loss of consciousness (alcoholic stupor,
anaesthesia, epilepsy).
- Oesophageal pathology (carcinoma, congenital
atresia / fistula).

• Obstruction of bronchus
- carcinoma, foreign body.
• Complication of pneumonia
- virulent organisms esp. Klebsiella, Staph.
• Bronchiectasis.
• Septic embolism (infective endocarditis on
right-sided heart valves) or septisaemia.
• Penetrating trauma e.g. stab wound.
• Direct spread of sepsis from other organs
(e.g. amoebic liver abscess).

Complications
• Rupture into pleural space ⇒ empyema or
broncho-pleural fistula (⇒ pyopneumothorax).
• Rupture into pericardium ⇒ pericarditis.
• Septisaemia ⇒ sepsis in other organs e.g.
osteomyelitis, brain abscess.
• Erosion of blood vessels ⇒ haemoptysis.
• Organisation ⇒ fibrosis.