
Please switch your mobile device to silent during the session
77
Transcript of Please switch your mobile device to silent during the session

Please switch your mobile device to silent during the session
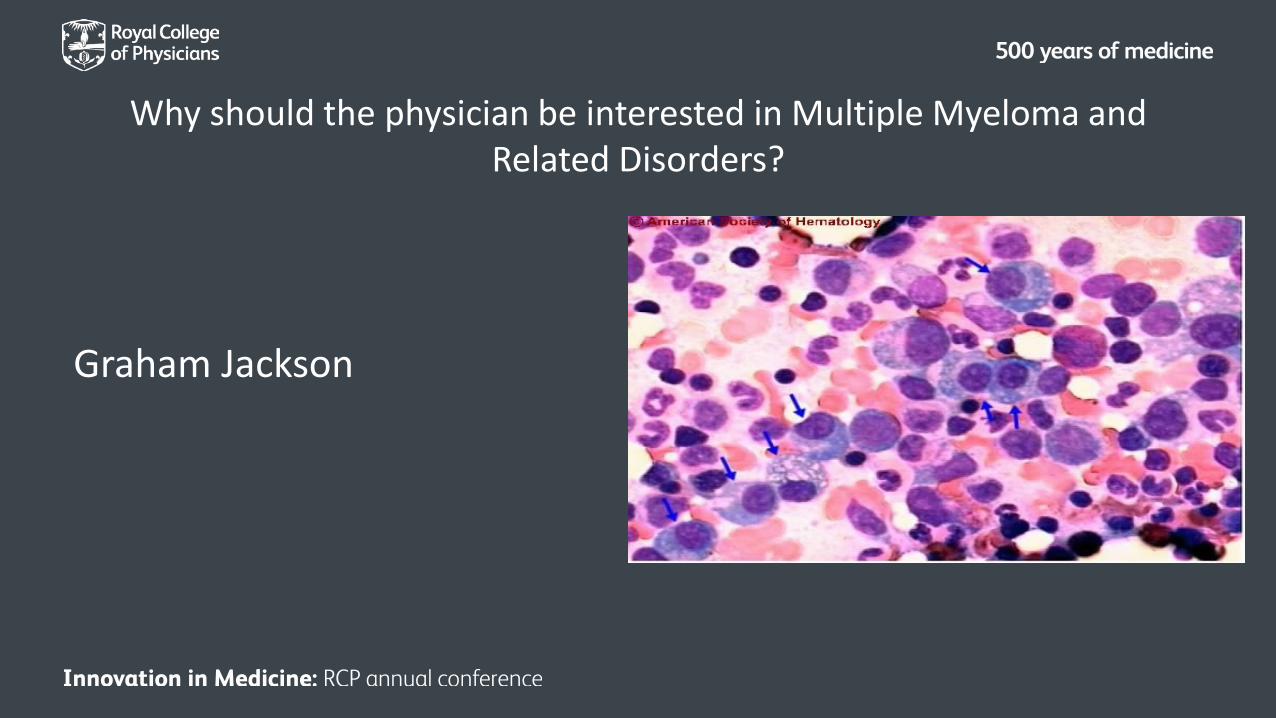
Why should the physician be interested in Multiple Myeloma and Related Disorders?
Graham Jackson
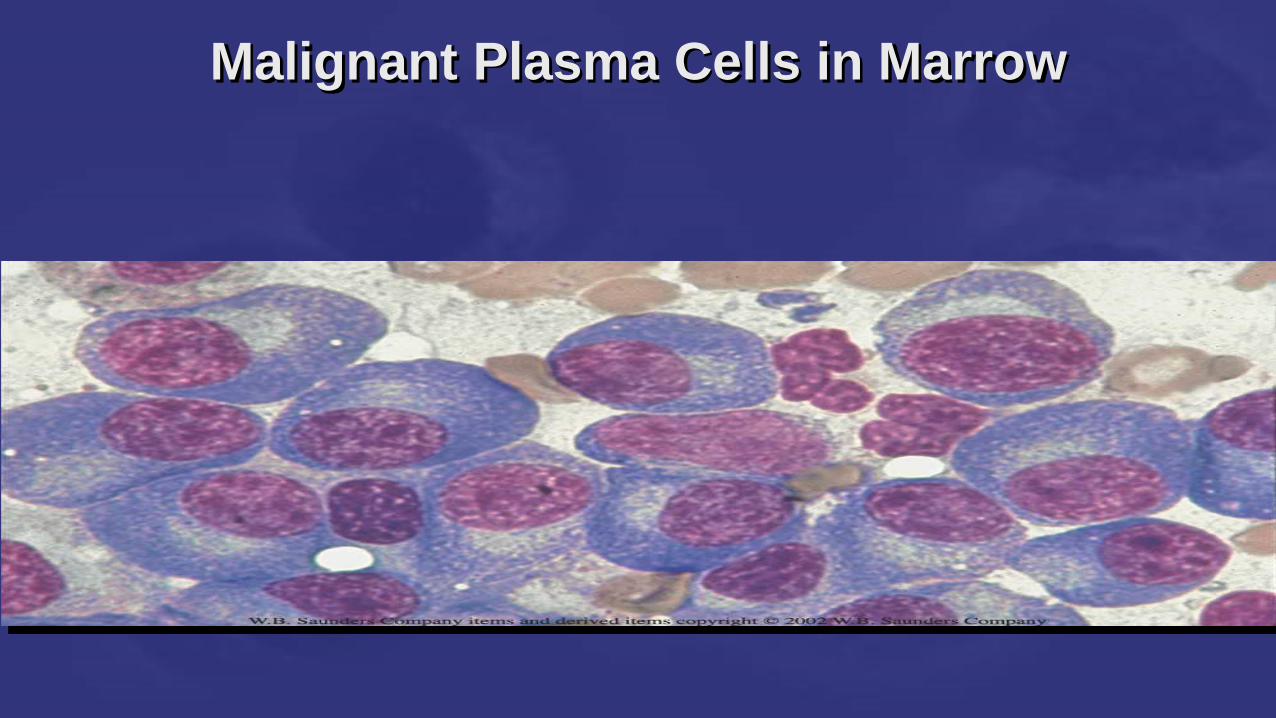
Malignant Plasma Cells in Marrow
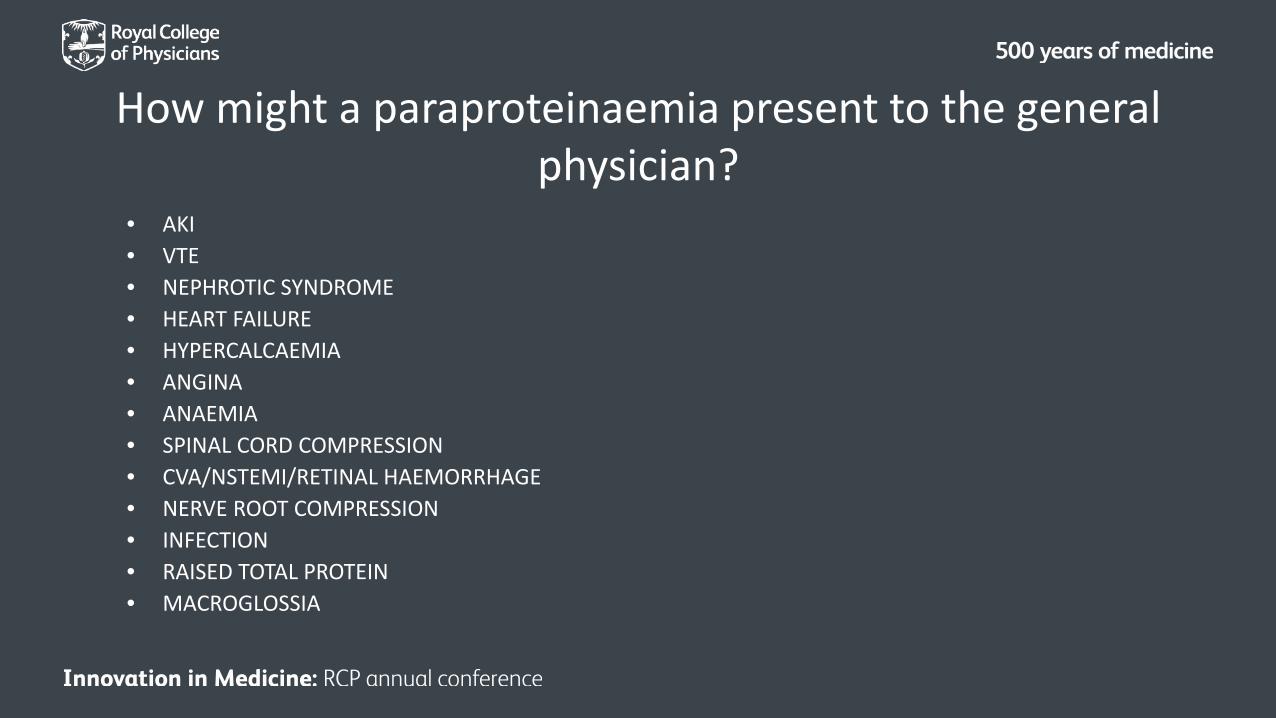
How might a paraproteinaemia present to the general physician?
• AKI• VTE• NEPHROTIC SYNDROME • HEART FAILURE• HYPERCALCAEMIA• ANGINA • ANAEMIA• SPINAL CORD COMPRESSION• CVA/NSTEMI/RETINAL HAEMORRHAGE • NERVE ROOT COMPRESSION• INFECTION • RAISED TOTAL PROTEIN • MACROGLOSSIA
Plasma cell disorders
• Multiple Myeloma • MGUS• Amyloidosis • Plasmacytomas• Poems syndrome • Cryoglobulinaemias
Plasma cell disorders
• Multiple Myeloma
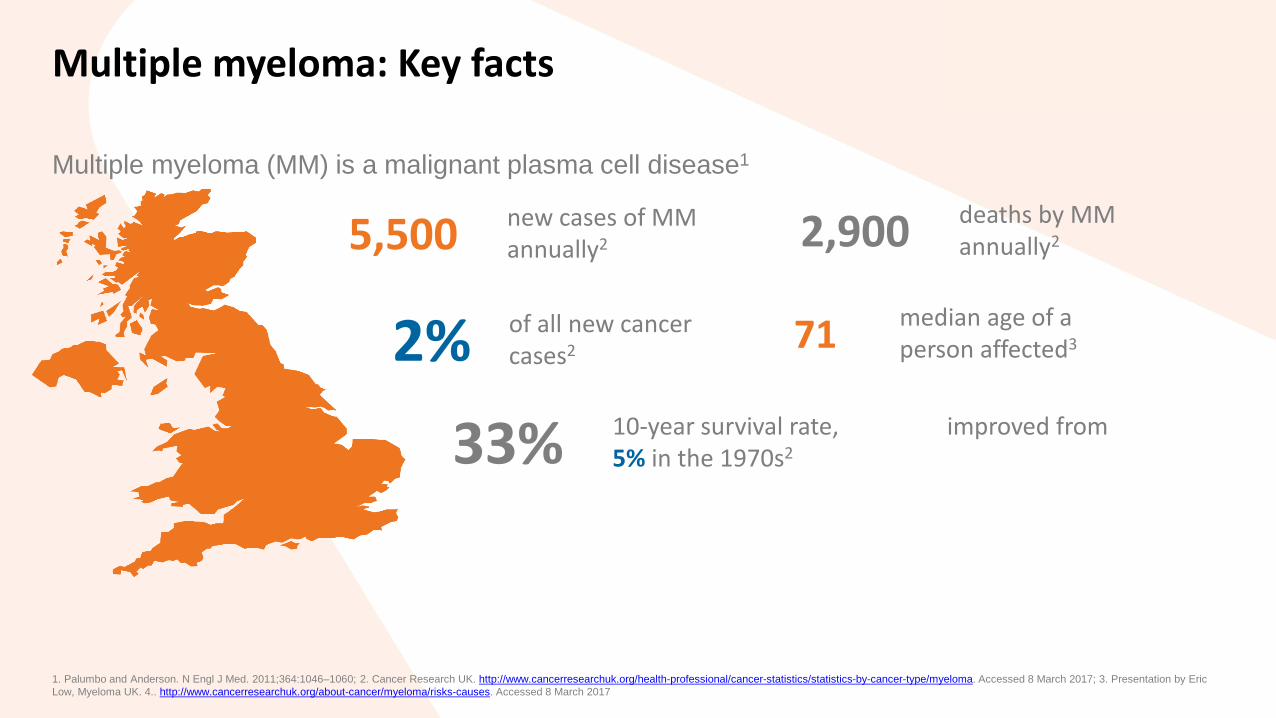
Multiple myeloma: Key facts
Multiple myeloma (MM) is a malignant plasma cell disease1
5,500 new cases of MM annually2 2,900 deaths by MM
annually2
2% of all new cancer cases2 71 median age of a
person affected3
33% 10-year survival rate, improved from 5% in the 1970s2
1. Palumbo and Anderson. N Engl J Med. 2011;364:1046–1060; 2. Cancer Research UK. http://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/myeloma. Accessed 8 March 2017; 3. Presentation by Eric Low, Myeloma UK. 4.. http://www.cancerresearchuk.org/about-cancer/myeloma/risks-causes. Accessed 8 March 2017
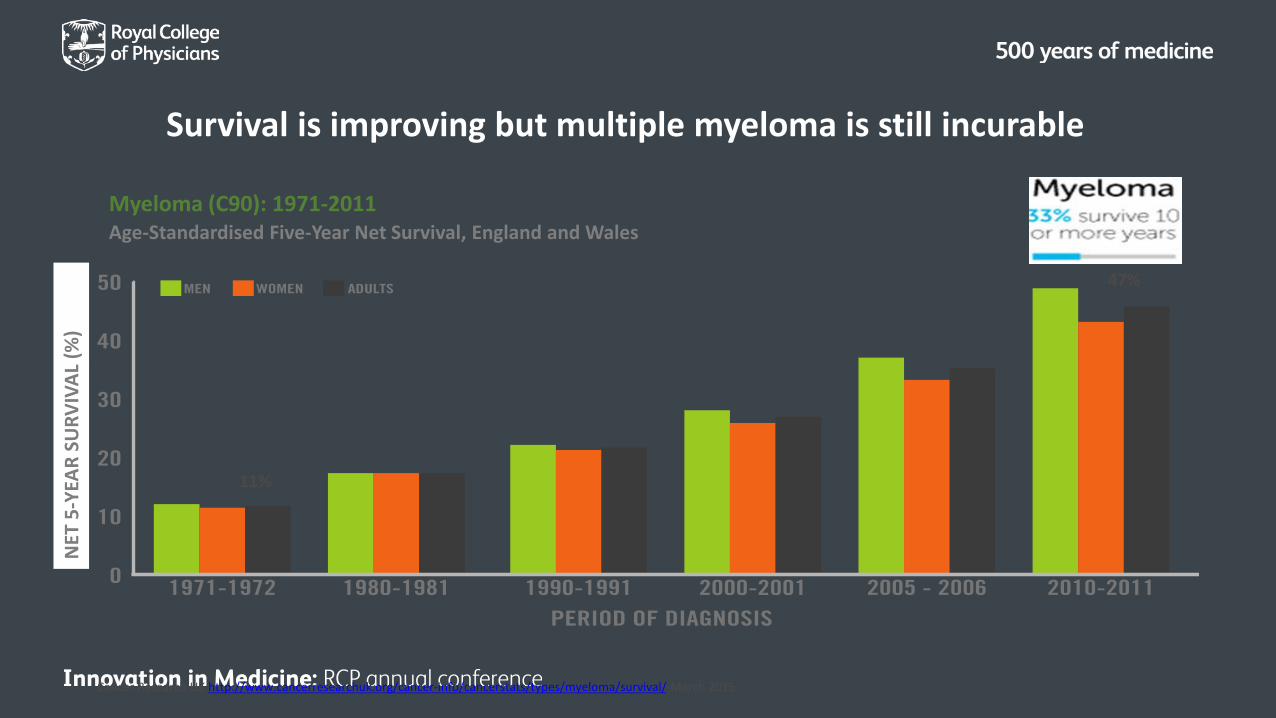
Survival is improving but multiple myeloma is still incurable
Cancer Research UK http://www.cancerresearchuk.org/cancer-info/cancerstats/types/myeloma/survival/ March 2015
Myeloma (C90): 1971-2011Age-Standardised Five-Year Net Survival, England and Wales
47%
11%
NET
5-Y
EAR
SURV
IVAL
(%)
Multiple MyelomaEpidemiology
Aetiology
• Causes remain uncertain
– Radiation, agriculture (farming), metals, rubber, chemicals, combustion fuel products.
– Familial and genetic factors have been implicated– Twice as common in patients of Afro-Caribean descent– All have pre-existing MGUS
Multiple MyelomaKey facts
• Myeloma is the cancer with most rapidly improving prognosis of all major cancer types
• Patients with Myeloma have to wait the longest between the first visit to GP with symptoms and diagnosis in the UK
• Of all cancers myeloma is most likely to be diagnosed in A and E or by the acute physician
Multiple Myeloma• Multiple myeloma is a cancer of bone marrow plasma cells
• It is characterised by
– monoclonal protein in serum and / or urine
– lytic bone lesions
– excess plasma cells in the bone marrow

What problems does myeloma cause?
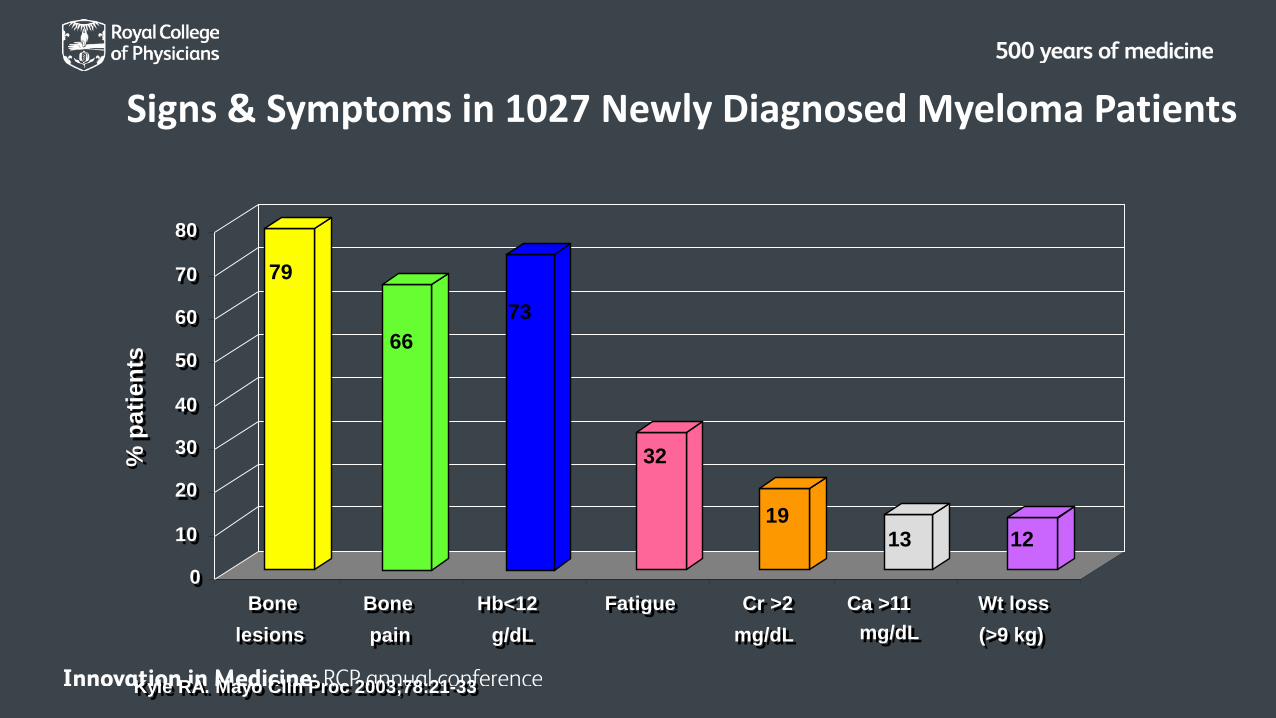
Signs & Symptoms in 1027 Newly Diagnosed Myeloma Patients
0
10
20
30
40
50
60
70
80
Bonelesions
Fatigue Cr >2mg/dL
Ca >11mg/dL
Wt loss(>9 kg)
% p
atie
nts
79
Hb<12g/dL
73
Bonepain
66
32
1319
12
Kyle RA. Mayo Clin Proc 2003;78:21-33
What problems does myeloma cause?
• Renal failure
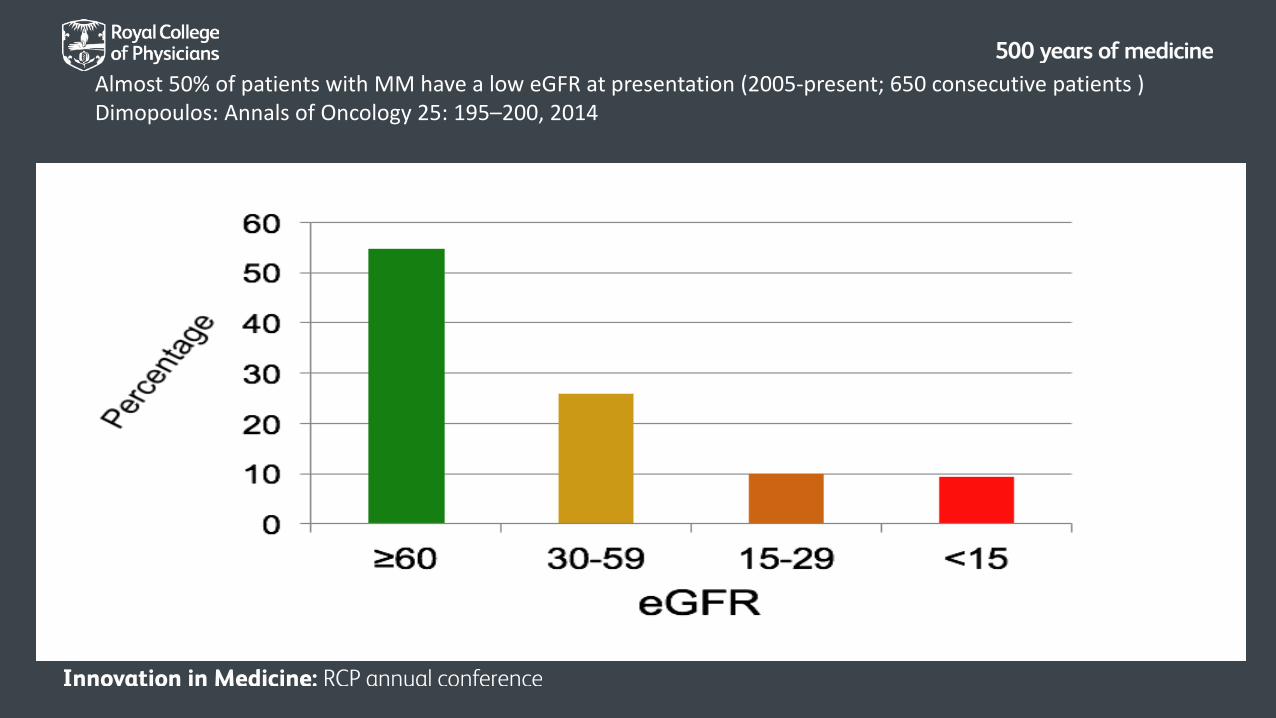
Almost 50% of patients with MM have a low eGFR at presentation (2005-present; 650 consecutive patients )Dimopoulos: Annals of Oncology 25: 195–200, 2014
Why do patients with myeloma getrenal damage?
• Light chain toxicity

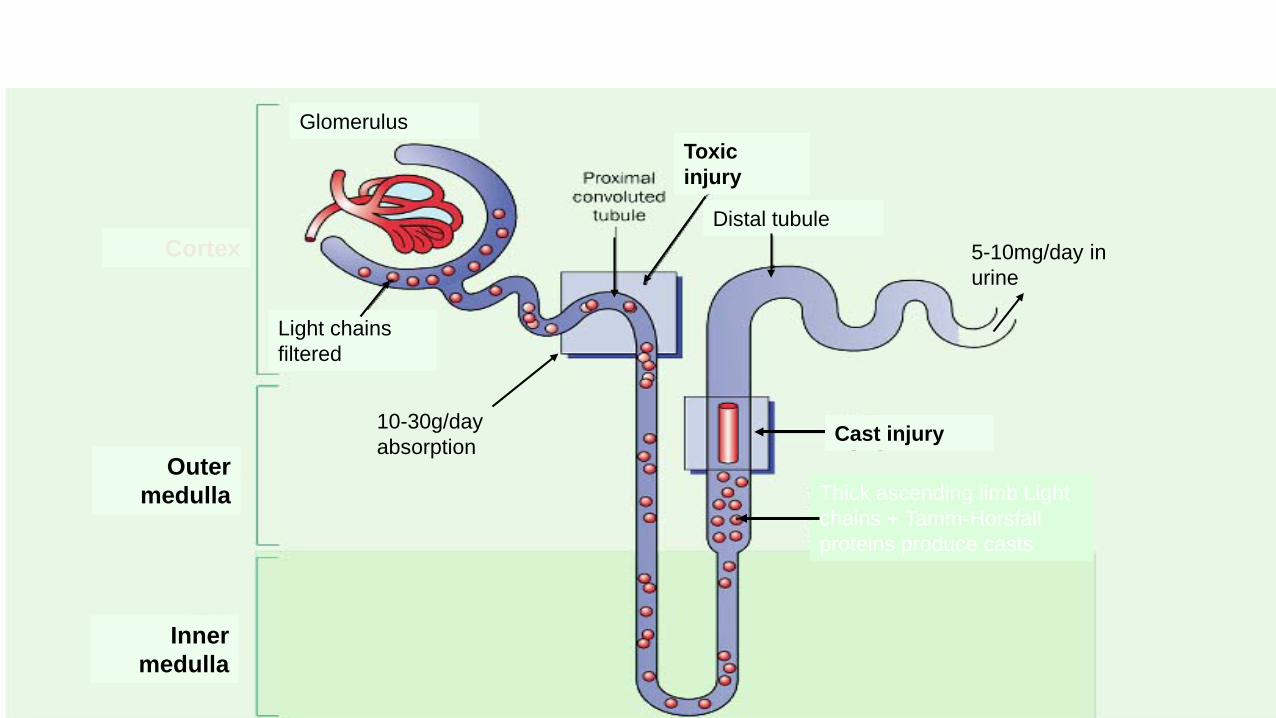
Cortex
Outer medulla
Inner medulla
Cast injury
Glomerulus
Light chains filtered
Distal tubule
10-30g/day absorption
Toxic injury
5-10mg/day in urine
Thick ascending limb Light chains + Tamm-Horsfall proteins produce casts
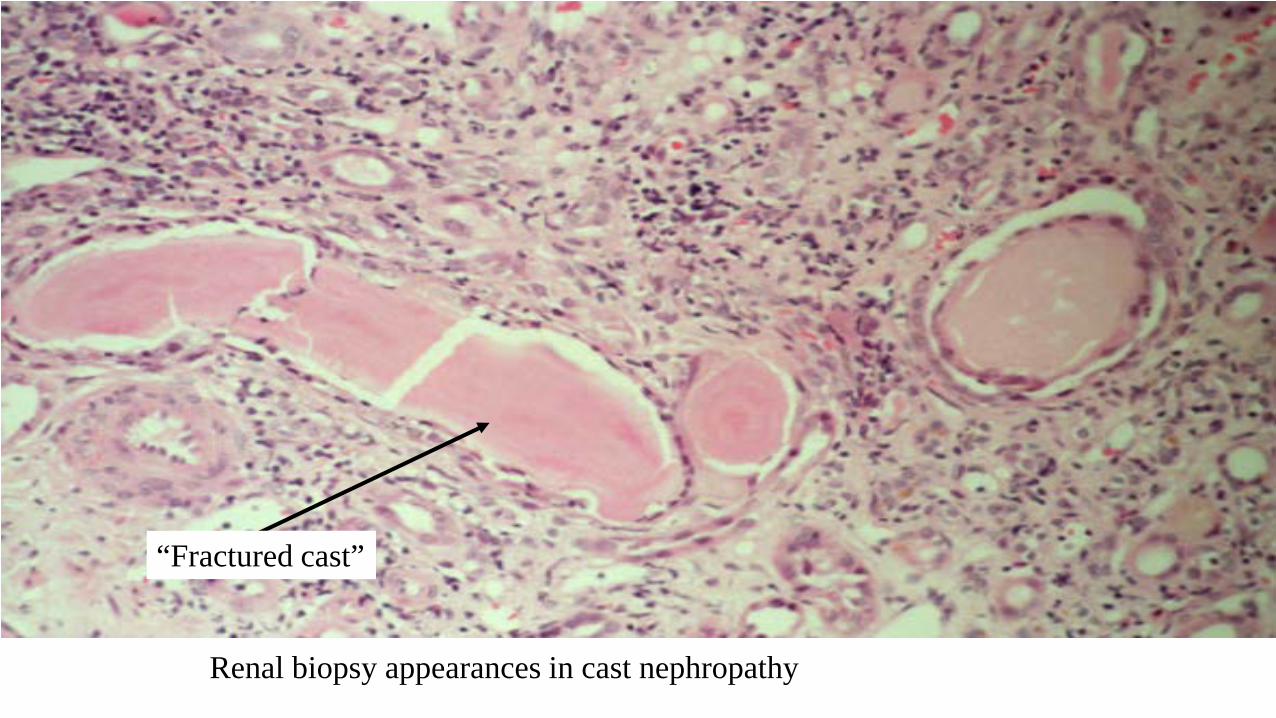
“Fractured cast”
Renal biopsy appearances in cast nephropathy

Why do patients with myeloma getrenal damage?
• Light chain toxicity• Hypercalcaemia• Dehydration• Nephrotoxic drugs – particularly NSAIDS• Infection• Hyperuricaemia
Why do patients with myeloma getrenal damage?
• Light chain toxicity –treat disease ASAP with novel therapies
• Hypercalcaemia – hydration, bisphosphonate• Dehydration - hydration• Nephrotoxic drugs – stop• Infection - treat• Hyperuricaemia – hydration, allopurinol
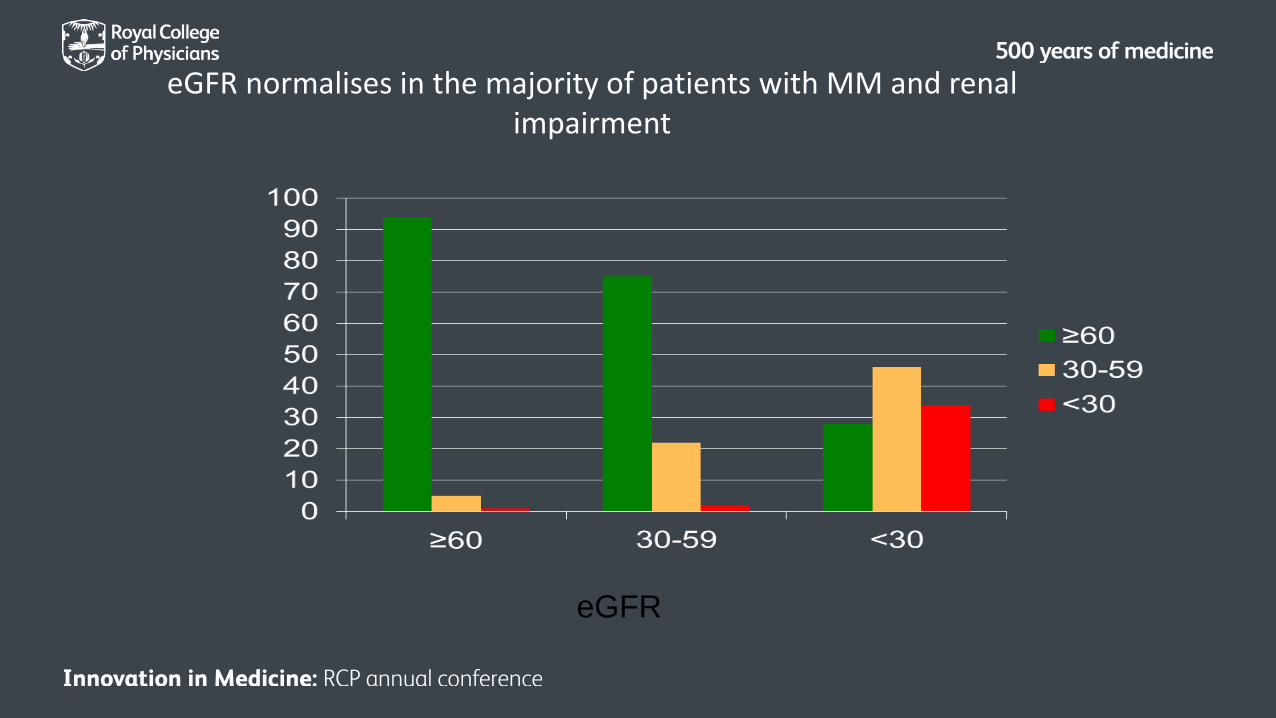
eGFR normalises in the majority of patients with MM and renal impairment
eGFR
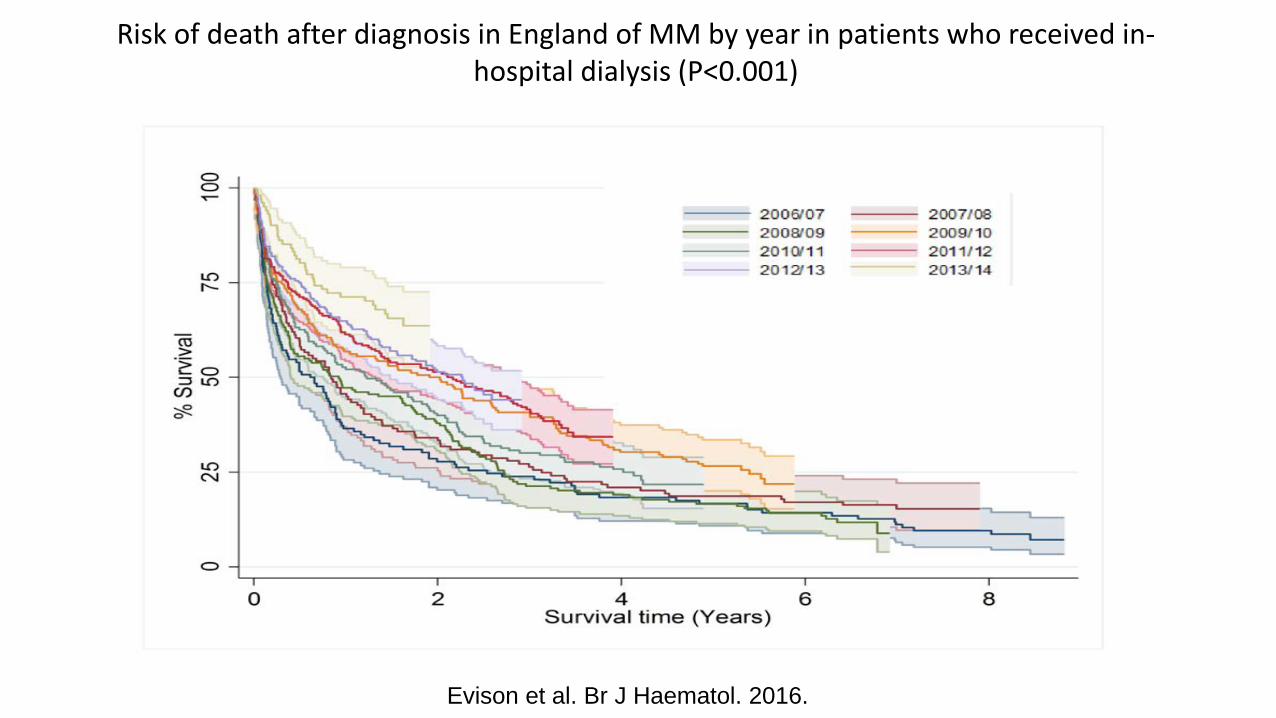
Risk of death after diagnosis in England of MM by year in patients who received in-hospital dialysis (P<0.001)
Evison et al. Br J Haematol. 2016.
What problems does myeloma cause?
• Renal failure• Amyloid
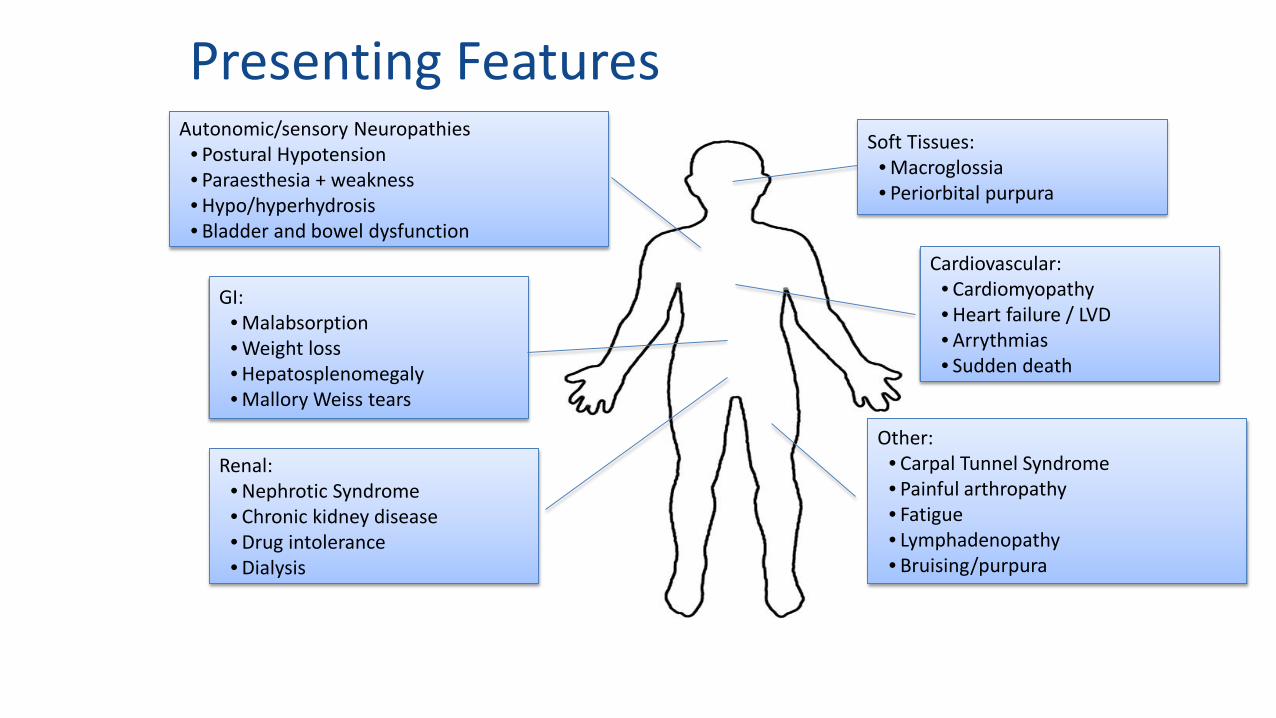
Presenting Features
Renal:• Nephrotic Syndrome• Chronic kidney disease• Drug intolerance• Dialysis
Other:• Carpal Tunnel Syndrome• Painful arthropathy• Fatigue• Lymphadenopathy• Bruising/purpura
GI:• Malabsorption• Weight loss• Hepatosplenomegaly• Mallory Weiss tears
Cardiovascular:• Cardiomyopathy• Heart failure / LVD• Arrythmias• Sudden death
Soft Tissues:• Macroglossia• Periorbital purpura
Autonomic/sensory Neuropathies• Postural Hypotension• Paraesthesia + weakness• Hypo/hyperhydrosis• Bladder and bowel dysfunction
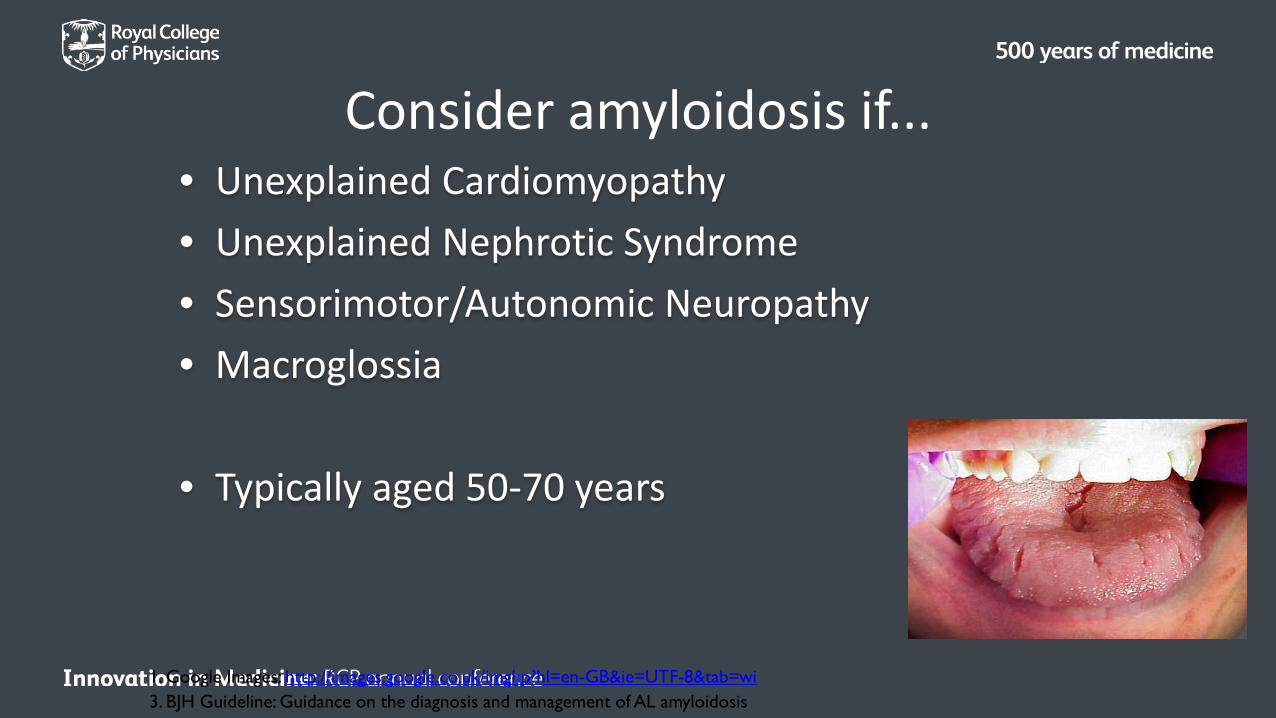
Consider amyloidosis if...• Unexplained Cardiomyopathy• Unexplained Nephrotic Syndrome• Sensorimotor/Autonomic Neuropathy• Macroglossia
• Typically aged 50-70 years
1. Google Images: http://images.google.co.uk/imghp?hl=en-GB&ie=UTF-8&tab=wi3. BJH Guideline: Guidance on the diagnosis and management of AL amyloidosis

• No blood test can be used to diagnose amyloidosis• Biopsy Rectum, gums, abdominal fat
• Congo Red StainApple green birefringance
• Biopsy!
If you suspect amyloid...
What problems does myeloma cause?
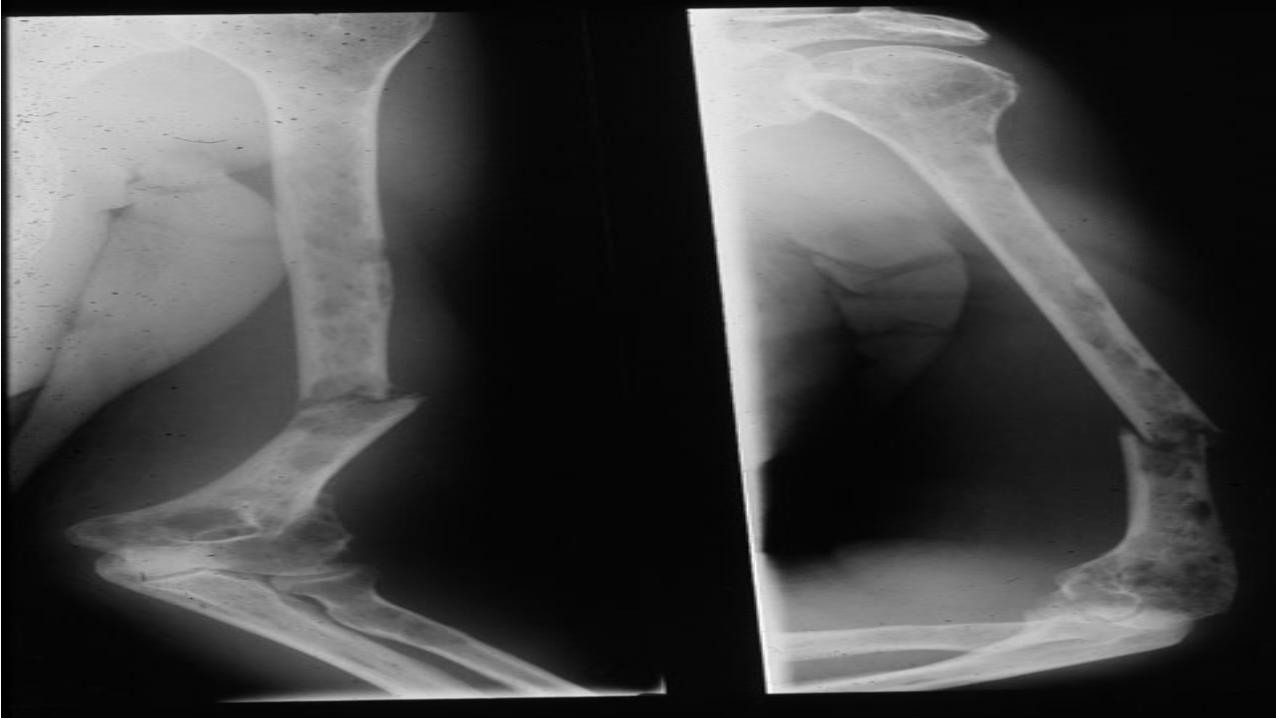
• Renal failure• Amyloid• Hypercalcaemia• Bone problems

Multiple ‘punched-out’ lytic lesions in the skull in myeloma

Wedgecompressionfracture of athoracicvertebra

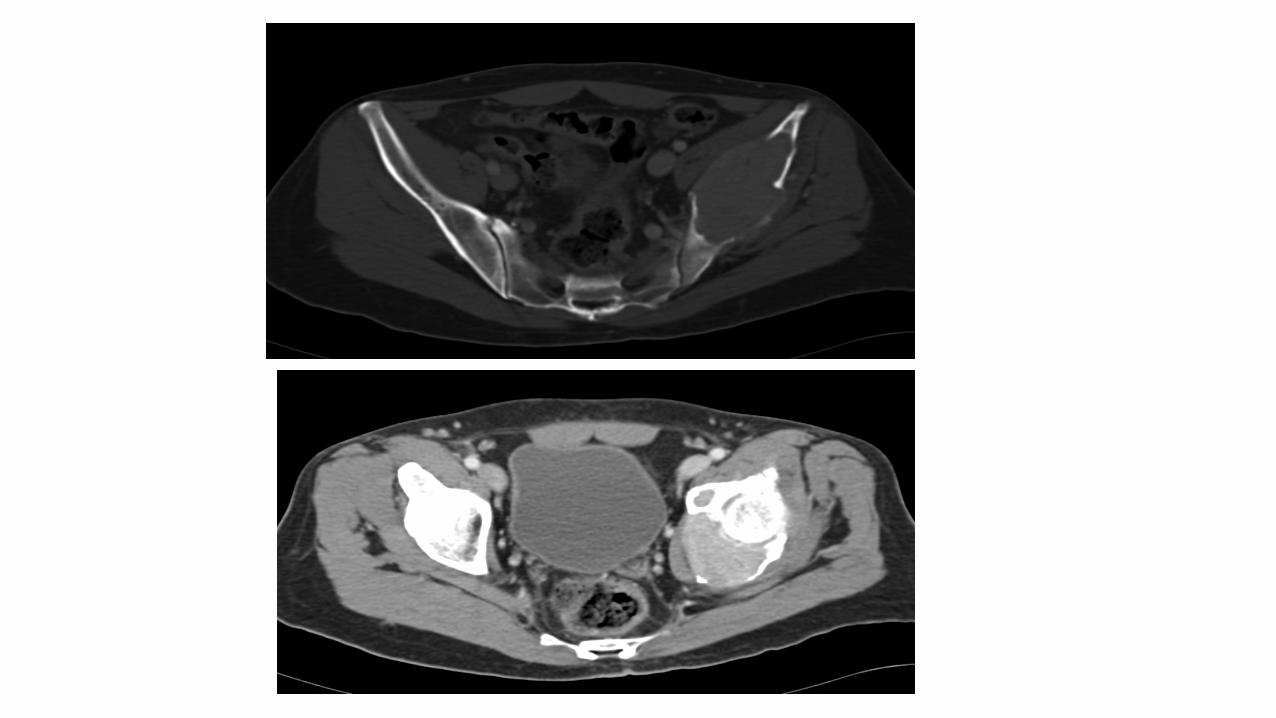
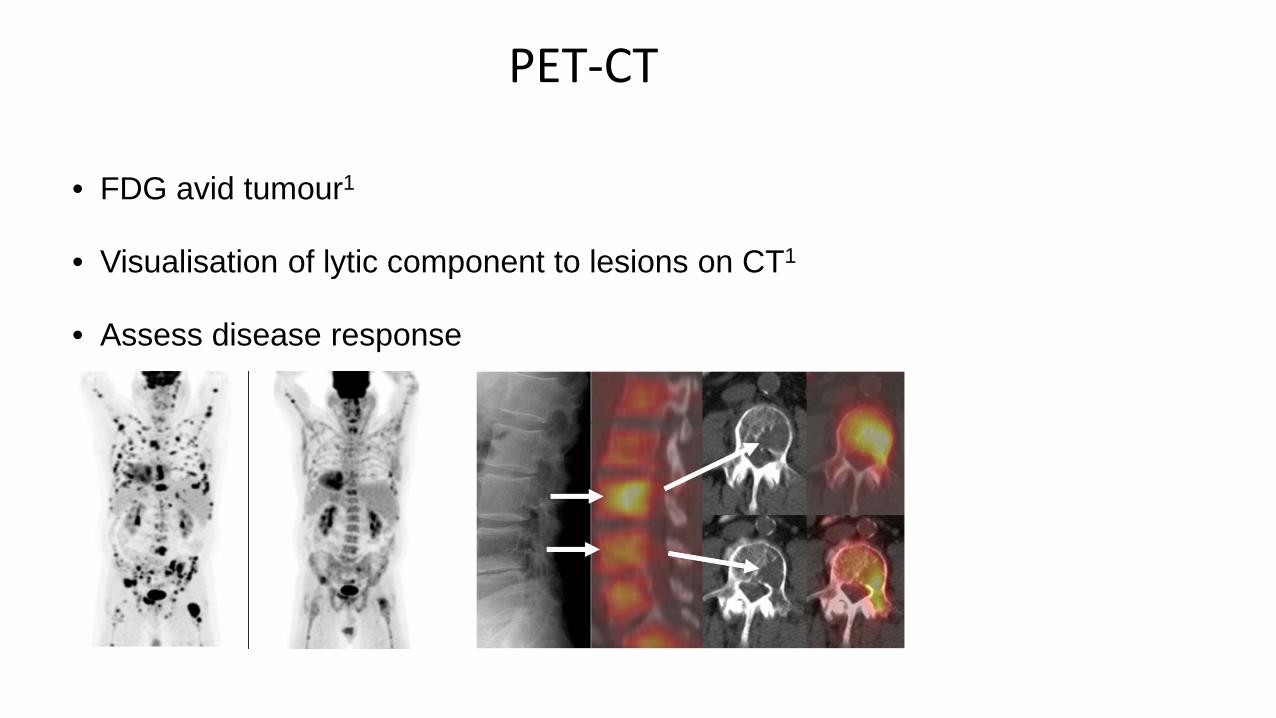
• FDG avid tumour1
• Visualisation of lytic component to lesions on CT1
• Assess disease response
PET-CT
Bisphosphonates
Treatment of Bone Disease
• Hypercalcaemia
– IV fluids
– Steroids
– Bisphosphonates – with care!!
Cochrane Review
• 11 trials, 2183 patients
• Prevent vertebral fractures OR 0.59 (0.45-0.78) p <0.00005• Amelioration of pain OR 0.59 (0.46-0.76) p <0.00005
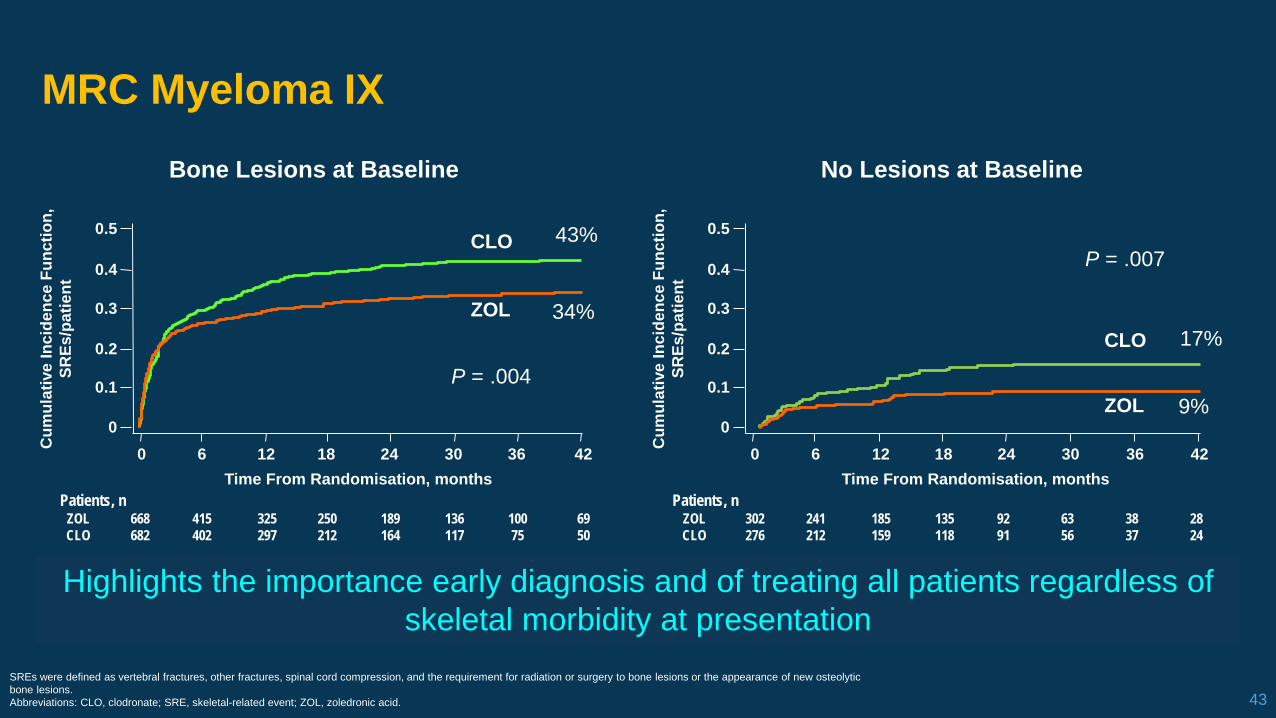
MRC Myeloma IX
43SREs were defined as vertebral fractures, other fractures, spinal cord compression, and the requirement for radiation or surgery to bone lesions or the appearance of new osteolytic bone lesions.Abbreviations: CLO, clodronate; SRE, skeletal-related event; ZOL, zoledronic acid.
Highlights the importance early diagnosis and of treating all patients regardless of skeletal morbidity at presentation
0 6 12 18 24 30 36 42
Bone Lesions at Baseline No Lesions at Baseline
0.5
0.4
0.3
0.2
0.1
0
Time From Randomisation, months
Cum
ulat
ive
Inci
denc
e Fu
nctio
n,SR
Es/p
atie
nt
668682
415402
325297
250212
189164
136117
10075
6950
ZOLCLO
Patients, n
0 6 12 18 24 30 36 42
0.5
0.4
0.3
0.2
0.1
0
Time From Randomisation, months
Cum
ulat
ive
Inci
denc
e Fu
nctio
n,SR
Es/p
atie
nt
302276
241212
185159
135118
9291
6356
3837
2824
ZOLCLO
Patients, n
CLO
ZOLCLO
ZOLP = .004
43%
34%17%
9%
P = .007
Zometa overview
• Overall survival 45.5mo clodronate v 51.6 mo for zometa
• Overall survival advantage for Zometa v clodronate = 6 months mainly seen in BD pts
What problems does myeloma cause?
• Renal failure• Amyloidosis• Hypercalcaemia• Bone problems • Anaemia• Infection• Thrombosis
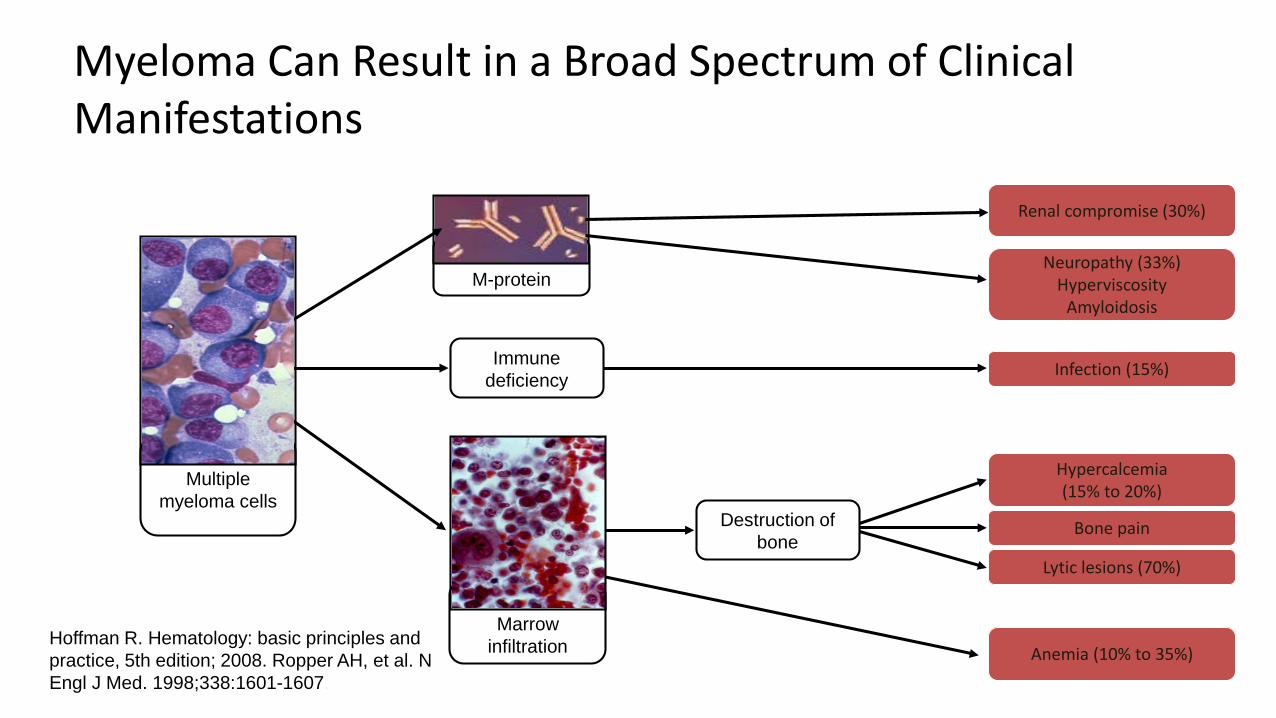
Myeloma Can Result in a Broad Spectrum of Clinical Manifestations
Hoffman R. Hematology: basic principles and practice, 5th edition; 2008. Ropper AH, et al. N Engl J Med. 1998;338:1601-1607.
M-protein
Bone pain
Neuropathy (33%)Hyperviscosity
Amyloidosis
Hypercalcemia (15% to 20%)
Immunedeficiency
Anemia (10% to 35%)
Lytic lesions (70%)
Infection (15%)
Marrow infiltration
Multiple myeloma cells
Destruction of bone
Renal compromise (30%)

MGUS
Monoclonal Gammopathy of Undetermined Significance
• Bone marrow plasma cells <10%
• Paraprotein less than 30g
• No CRAB (hyperCalcaemia, Renal impairment, Anaemia and Bone disease)
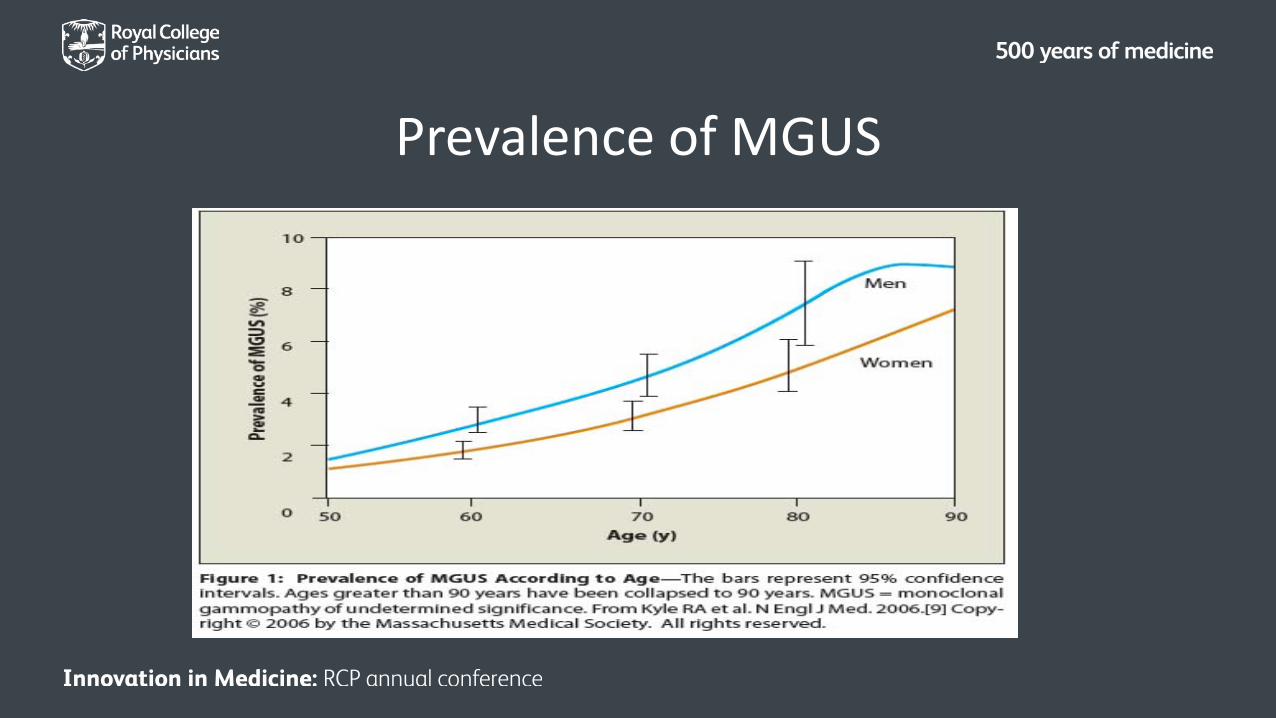
Prevalence of MGUS
MGUS
All myeloma patients have a pre-existing MGUSOver 20 years • 25% will progress to myeloma
– RISK FACTORS
• IgA paraprotein• PP > 15g• Abnormal SFLC
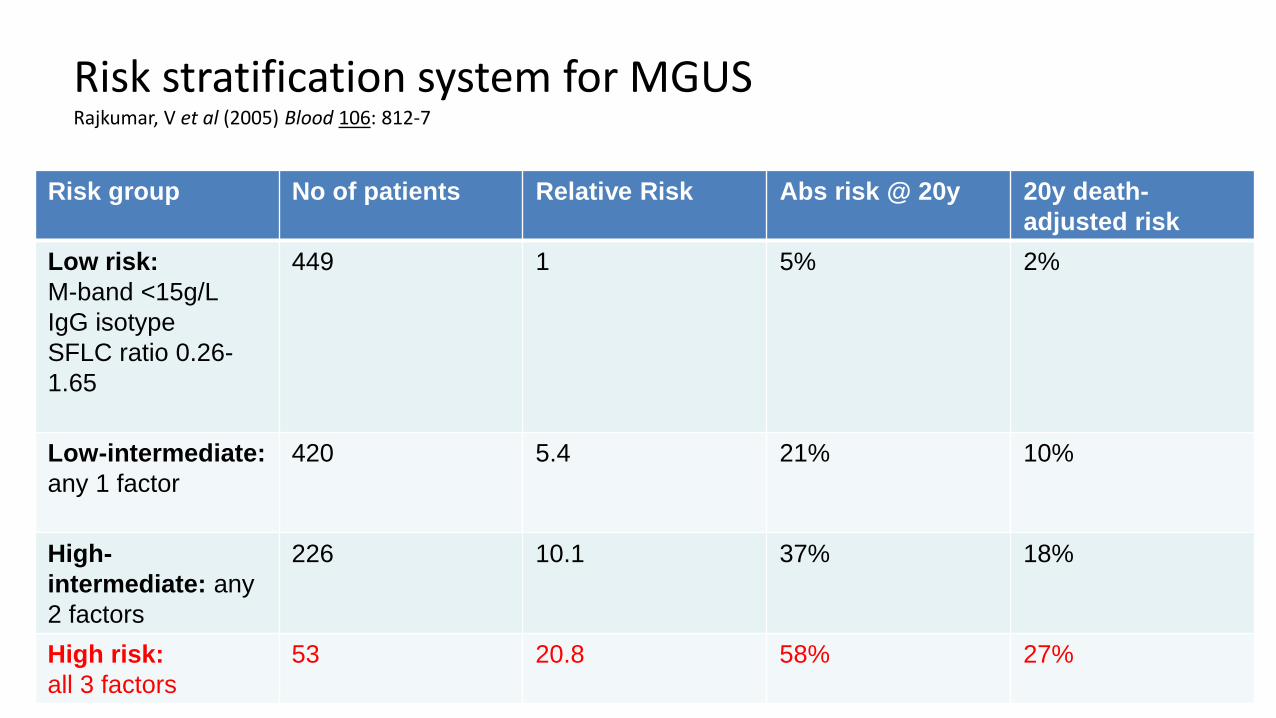
Risk stratification system for MGUS Rajkumar, V et al (2005) Blood 106: 812-7
Risk group No of patients Relative Risk Abs risk @ 20y 20y death-adjusted risk
Low risk:M-band <15g/LIgG isotypeSFLC ratio 0.26-1.65
449 1 5% 2%
Low-intermediate: any 1 factor
420 5.4 21% 10%
High-intermediate: any 2 factors
226 10.1 37% 18%
High risk: all 3 factors
53 20.8 58% 27%
Asymptomatic Myeloma
Asymptomatic/smouldering myeloma
• Higher risk of progression than MGUS:– 50% at 5 years– 65% at 10 years
• Cumulative probability: 70% at 15 years• Median time to progression: ≈5 years
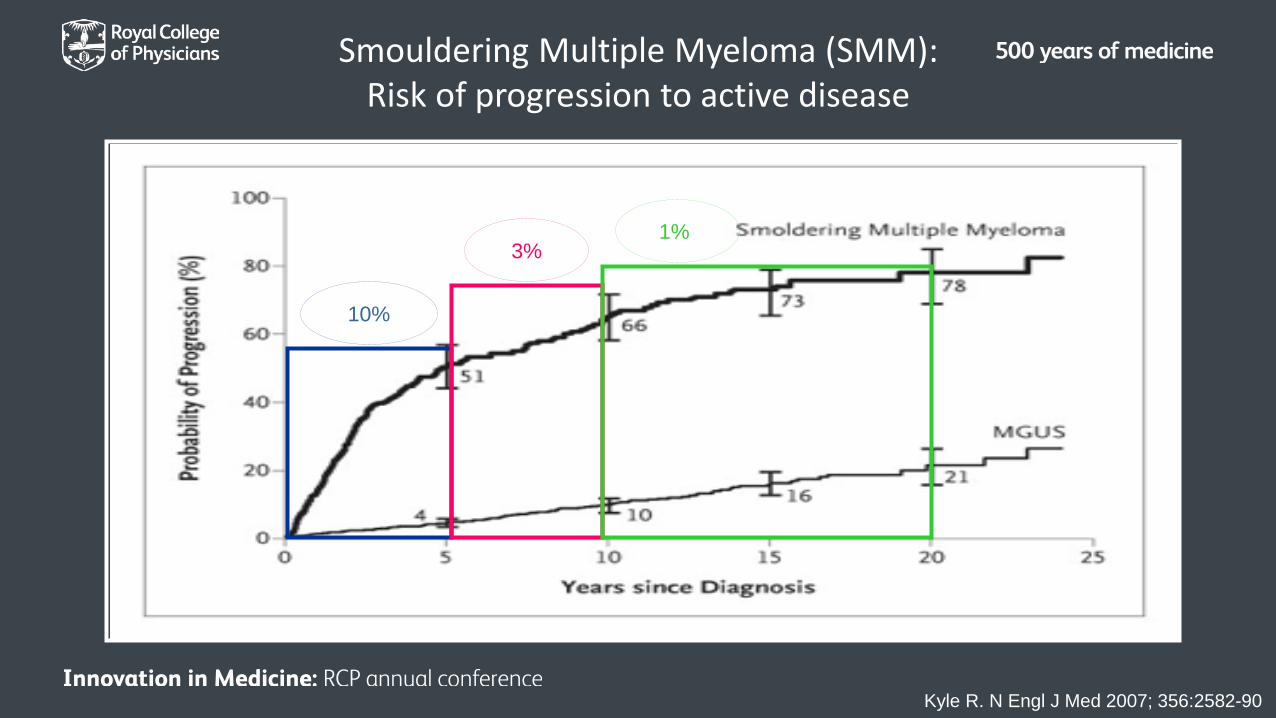
Kyle R. N Engl J Med 2007; 356:2582-90
10%
3%1%
Smouldering Multiple Myeloma (SMM): Risk of progression to active disease
Symptomatic Myeloma
Myeloma Prognostic Factors
• Serum β2 microglobulin• Cytogenetics • Albumen • Age• LDH • Peripheral blood plasma cells
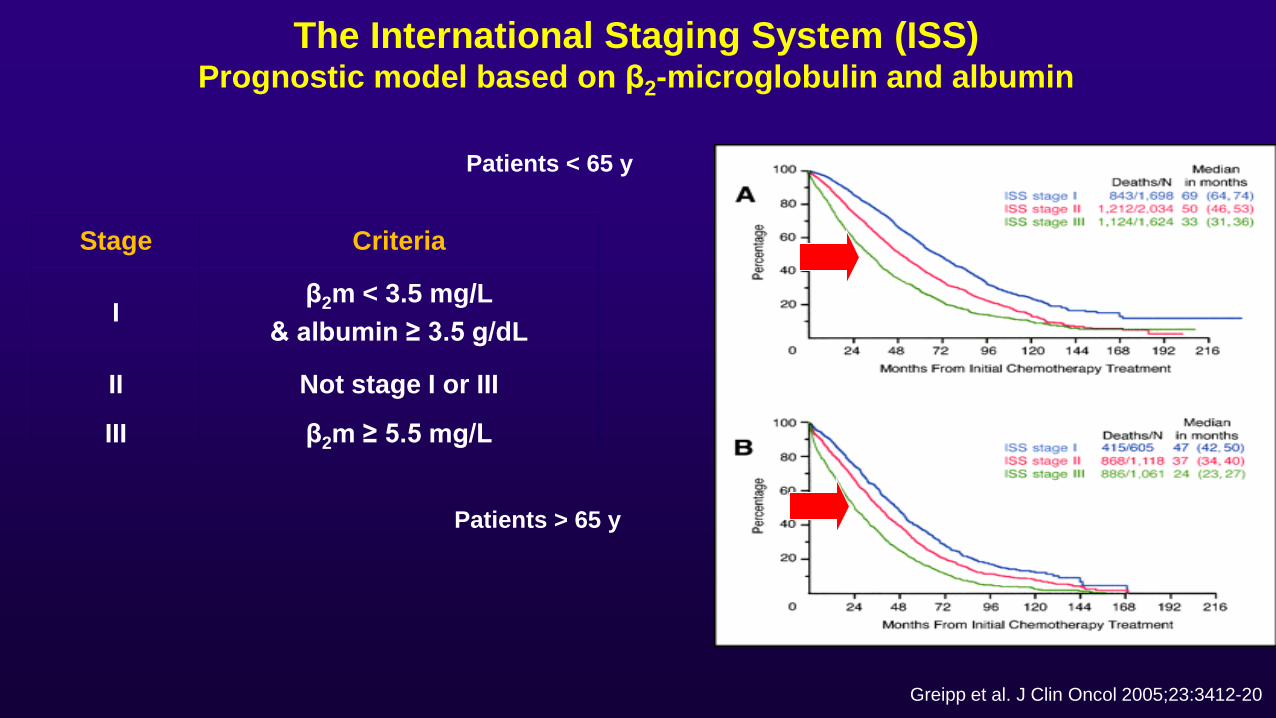
The International Staging System (ISS)Prognostic model based on β2-microglobulin and albumin
Patients < 65 y
Patients > 65 y
Stage Criteria
Iβ2m < 3.5 mg/L
& albumin ≥ 3.5 g/dL
II Not stage I or III
III β2m ≥ 5.5 mg/L
Greipp et al. J Clin Oncol 2005;23:3412-20
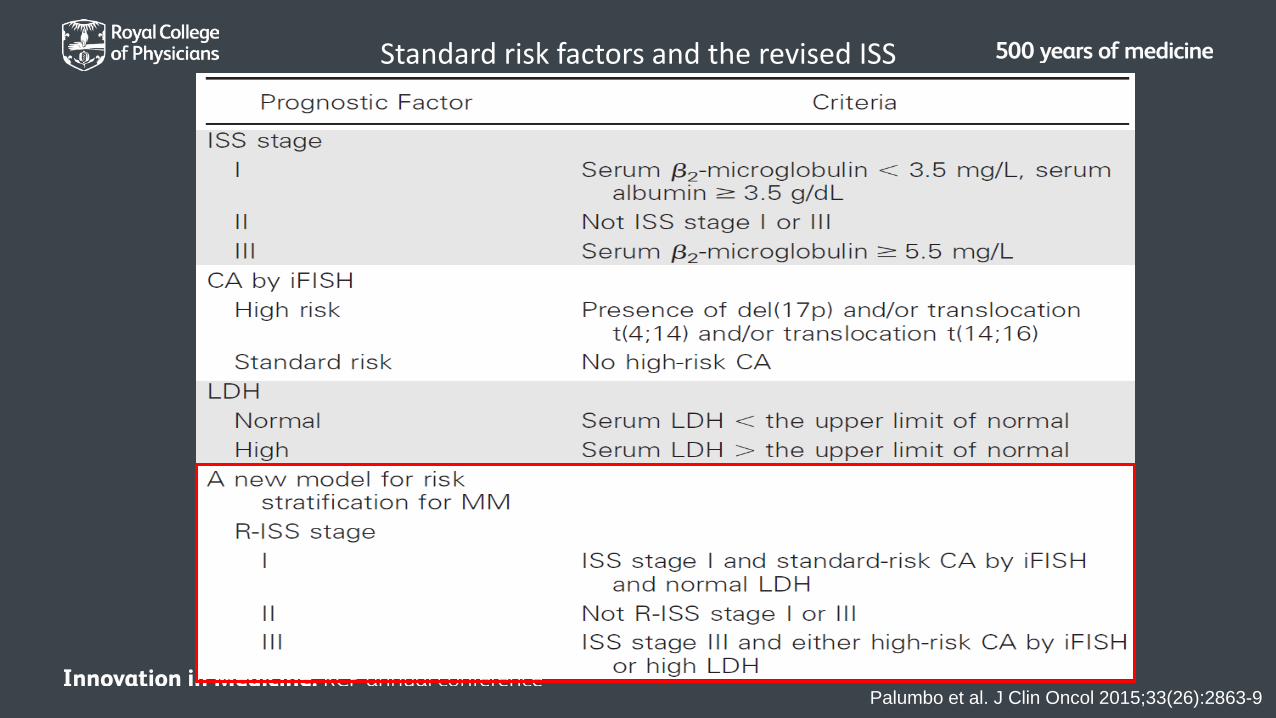
Standard risk factors and the revised ISS
Palumbo et al. J Clin Oncol 2015;33(26):2863-9
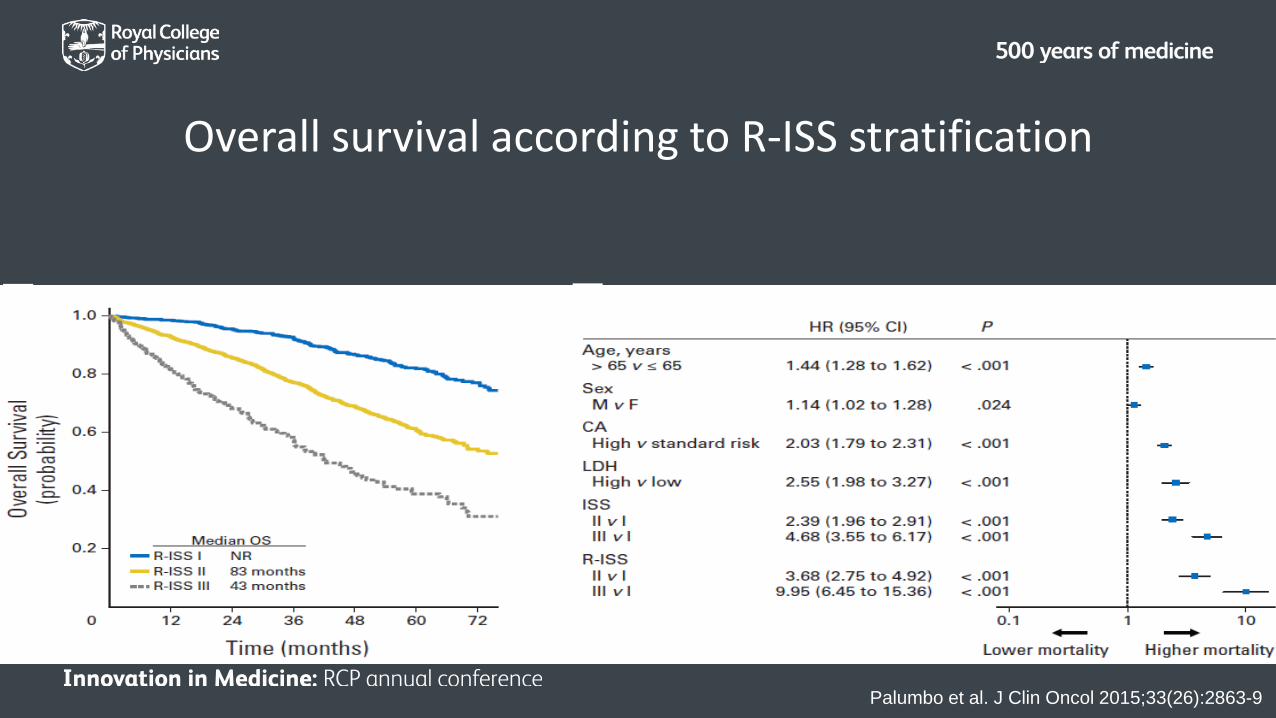
Overall survival according to R-ISS stratification
Palumbo et al. J Clin Oncol 2015;33(26):2863-9
Improving outcomes
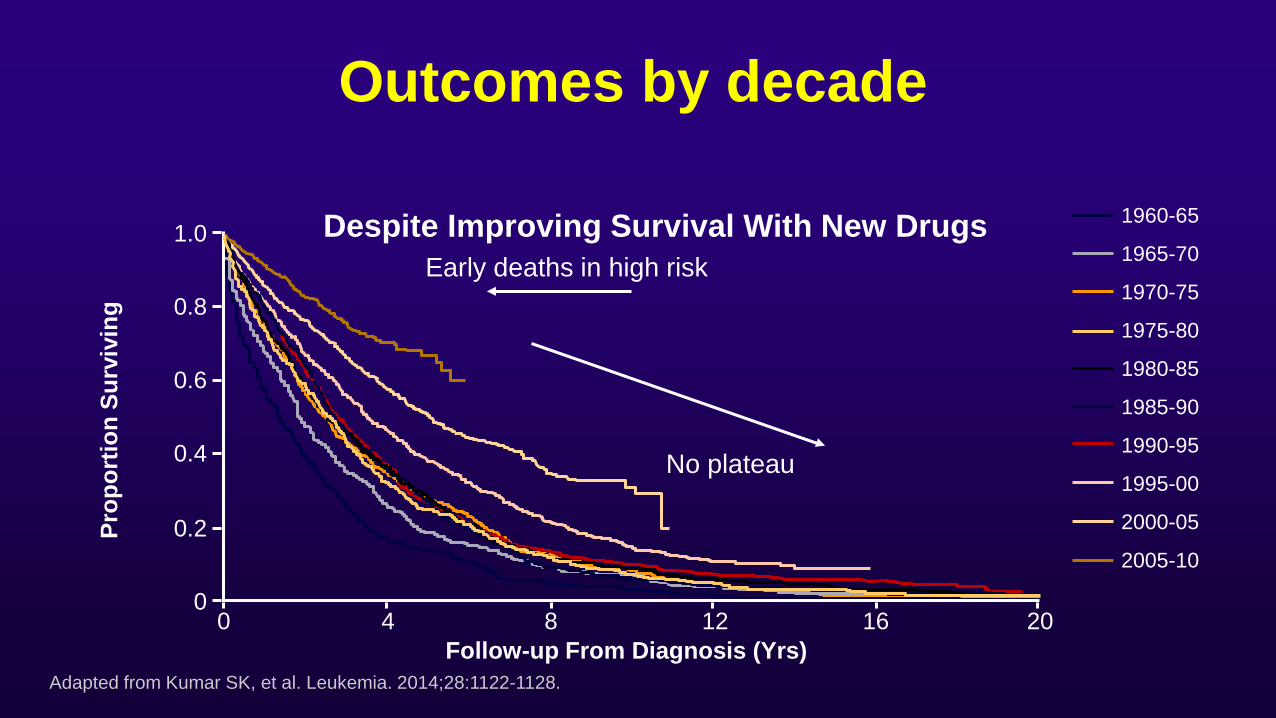
1960-65
1965-70
1970-75
1975-80
1980-85
1985-90
1990-95
1995-00
2000-05
2005-10
Early deaths in high risk
No plateau
Adapted from Kumar SK, et al. Leukemia. 2014;28:1122-1128.
Despite Improving Survival With New Drugs 1.0
0.8
0.6
0.4
0.2
00 4 8 12 16 20
Follow-up From Diagnosis (Yrs)
Prop
ortio
n Su
rviv
ing
Outcomes by decade
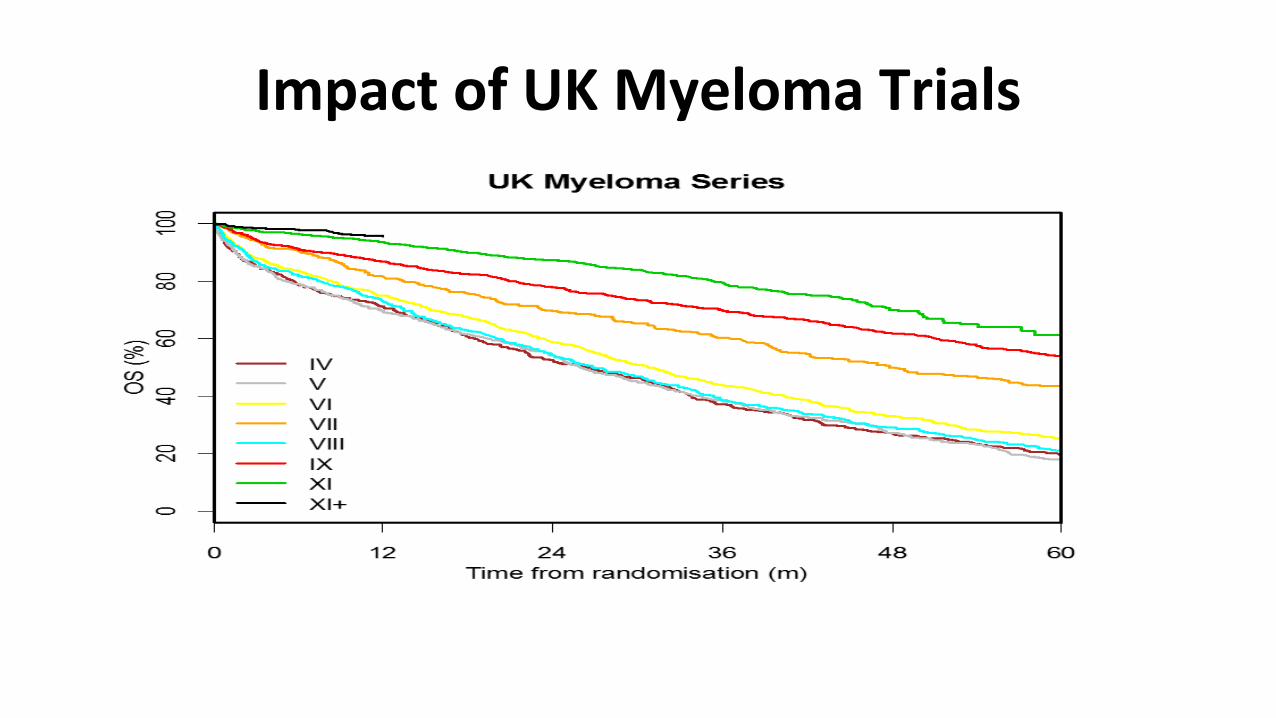
Impact of UK Myeloma Trials
Why are things changing?
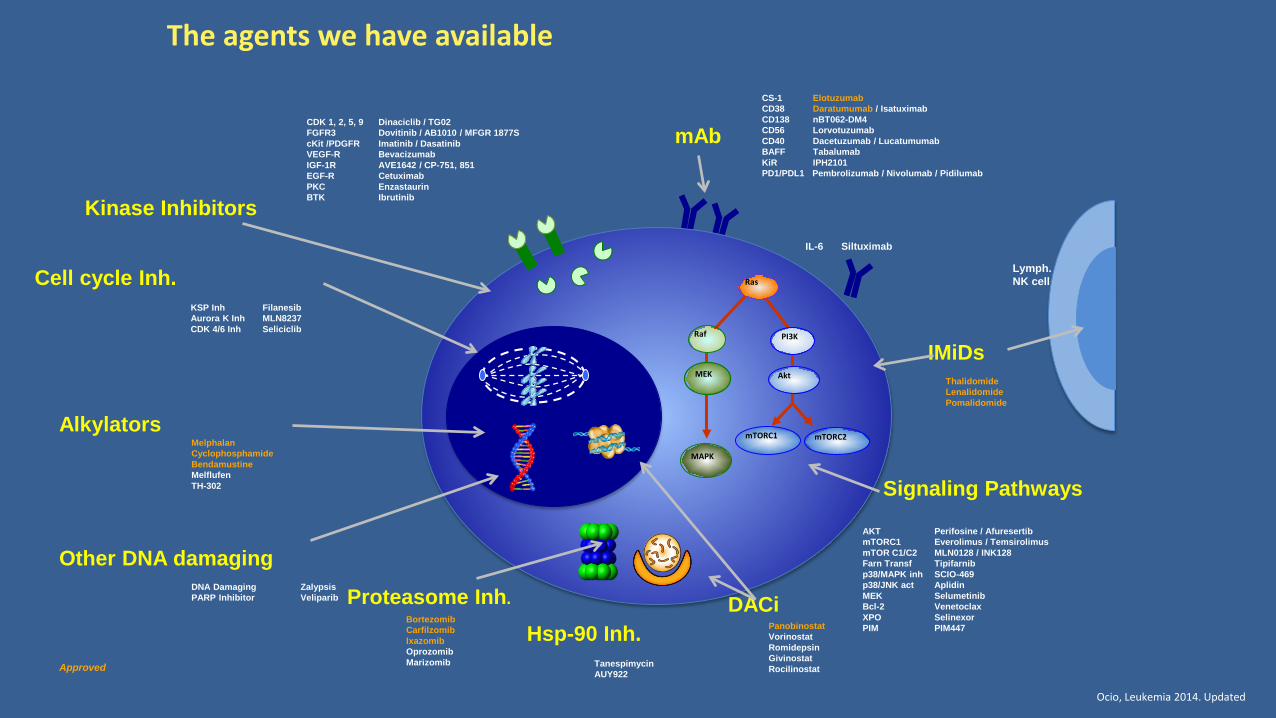
Ocio, Leukemia 2014. Updated
The agents we have available
Raf
MEK
MAPK
PI3K
Akt
Ras
mTORC1 mTORC2
Lymph.NK cell
Approved
ThalidomideLenalidomidePomalidomide
IMiDs
PanobinostatVorinostatRomidepsinGivinostatRocilinostat
DACi
CS-1 ElotuzumabCD38 Daratumumab / IsatuximabCD138 nBT062-DM4CD56 LorvotuzumabCD40 Dacetuzumab / LucatumumabBAFF TabalumabKiR IPH2101PD1/PDL1 Pembrolizumab / Nivolumab / Pidilumab
IL-6 Siltuximab
mAb
BortezomibCarfilzomibIxazomibOprozomibMarizomib
Proteasome Inh.
MelphalanCyclophosphamideBendamustineMelflufenTH-302
Alkylators
TanespimycinAUY922
Hsp-90 Inh.
DNA Damaging ZalypsisPARP Inhibitor Veliparib
Other DNA damaging
KSP Inh FilanesibAurora K Inh MLN8237CDK 4/6 Inh Seliciclib
Cell cycle Inh.
AKT Perifosine / AfuresertibmTORC1 Everolimus / TemsirolimusmTOR C1/C2 MLN0128 / INK128Farn Transf Tipifarnibp38/MAPK inh SCIO-469p38/JNK act AplidinMEK SelumetinibBcl-2 VenetoclaxXPO SelinexorPIM PIM447
Signaling Pathways
CDK 1, 2, 5, 9 Dinaciclib / TG02FGFR3 Dovitinib / AB1010 / MFGR 1877ScKit /PDGFR Imatinib / DasatinibVEGF-R BevacizumabIGF-1R AVE1642 / CP-751, 851EGF-R CetuximabPKC EnzastaurinBTK IbrutinibKinase Inhibitors
Thalidomide
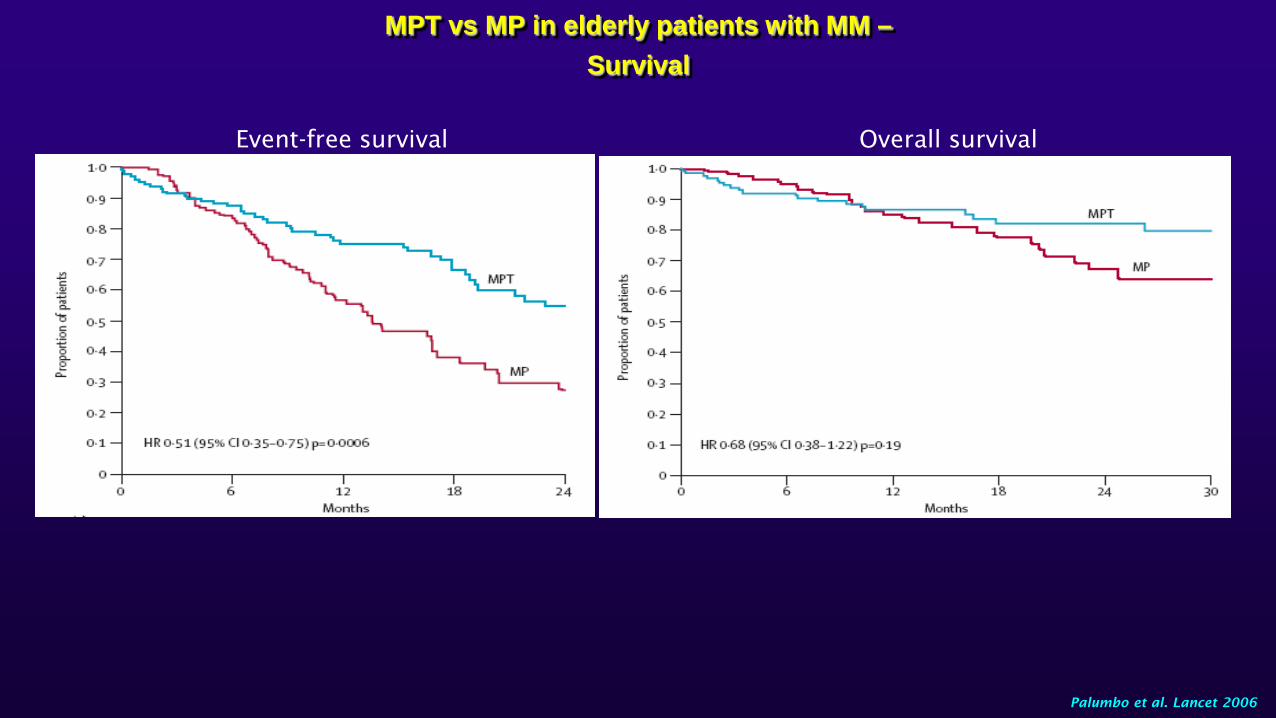
Event-free survival Overall survival
Palumbo et al. Lancet 2006
MPT vs MP in elderly patients with MM –Survival
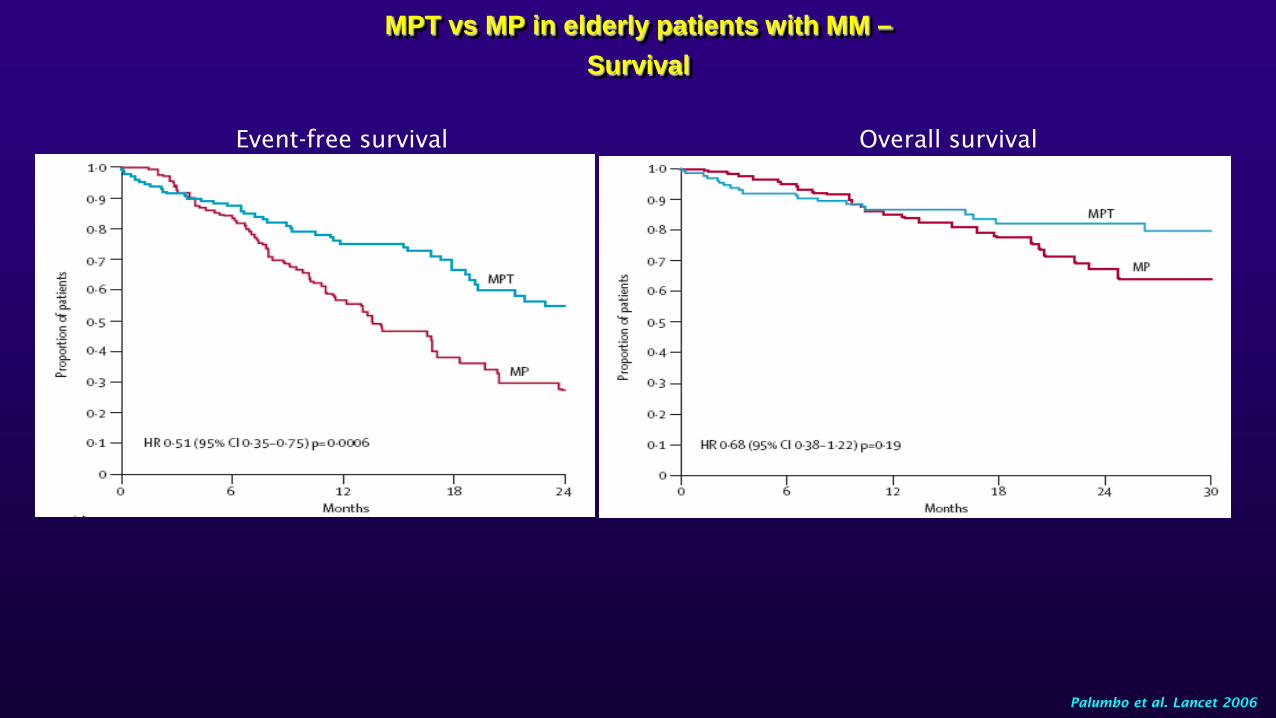
Event-free survival Overall survival
Palumbo et al. Lancet 2006
MPT vs MP in elderly patients with MM –Survival
Velcade
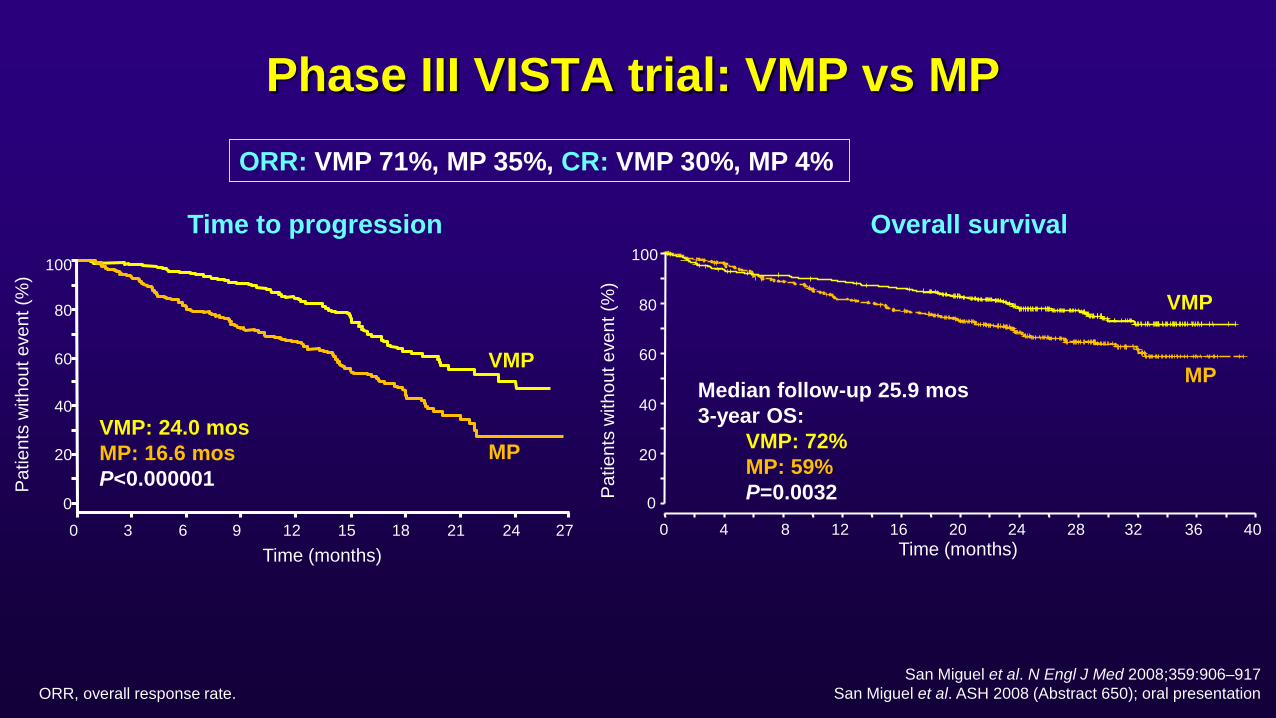
Phase III VISTA trial: VMP vs MP
0 3 6 9 12Time (months)
15 18 21 24 270
20
40
60
80
100
VMP
Patie
nts
with
out e
vent
(%)
Time (months)0 4 8 12 16 20 24 28 32 36 40
0
20
40
60
80
100
Patie
nts
with
out e
vent
(%)
Time to progression Overall survival
San Miguel et al. N Engl J Med 2008;359:906–917San Miguel et al. ASH 2008 (Abstract 650); oral presentation
ORR: VMP 71%, MP 35%, CR: VMP 30%, MP 4%
Median follow-up 25.9 mos3-year OS:
VMP: 72%MP: 59%P=0.0032
VMP: 24.0 mosMP: 16.6 mosP<0.000001
MP
VMP
MP
ORR, overall response rate.
Monoclonal antibodies
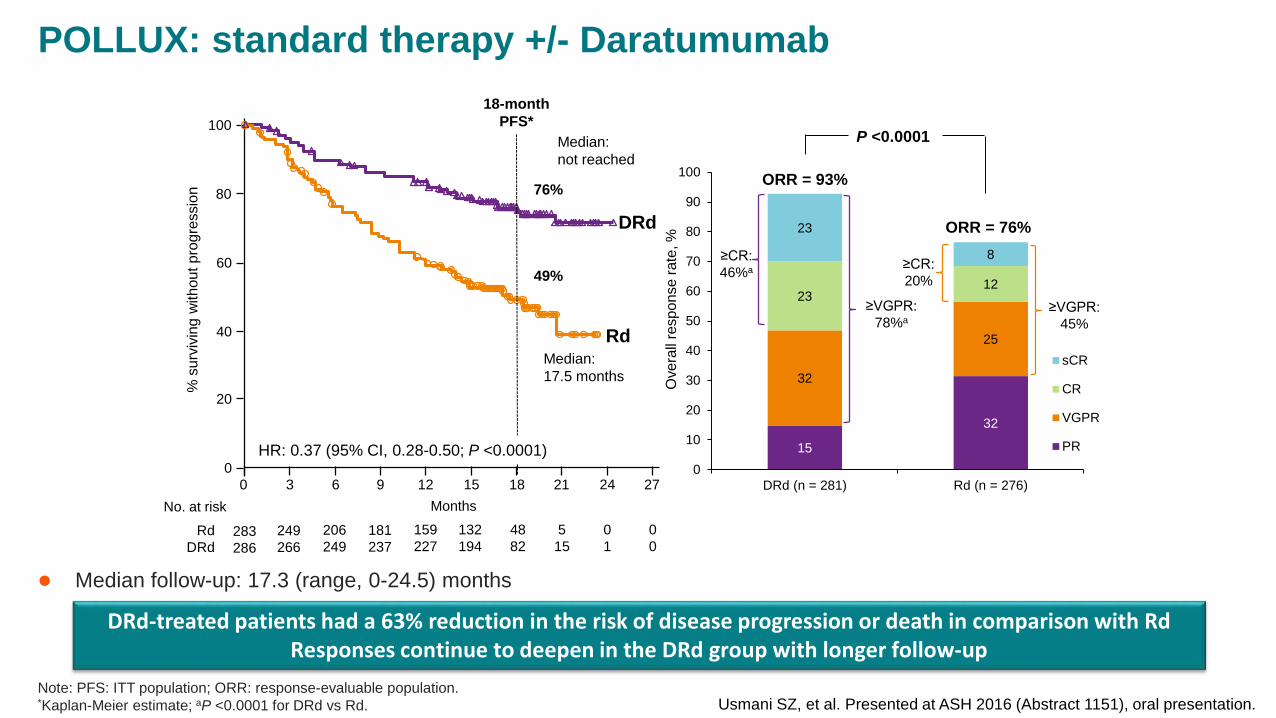
POLLUX: standard therapy +/- Daratumumab
Usmani SZ, et al. Presented at ASH 2016 (Abstract 1151), oral presentation.
% s
urvi
ving
with
out p
rogr
essi
on
0
20
40
60
80
100
0 3 6 9 12 18 21 27
283286
249266
206249
181237
159227
132194
515
01
RdDRd
No. at risk Months24
00
15
4882
76%
49%
18-month PFS*
Rd
DRd
Median: 17.5 months
HR: 0.37 (95% CI, 0.28-0.50; P <0.0001)
Ove
rall
resp
onse
rate
, %
15
32
32
25
2312
23
8
0
10
20
30
40
50
60
70
80
90
100
DRd (n = 281) Rd (n = 276)
sCR
CR
VGPR
PR
ORR = 93%
ORR = 76%
P <0.0001
≥VGPR: 78%a
≥CR: 46%a
≥VGPR: 45%
≥CR: 20%
Median: not reached
Note: PFS: ITT population; ORR: response-evaluable population.*Kaplan-Meier estimate; aP <0.0001 for DRd vs Rd.
Median follow-up: 17.3 (range, 0-24.5) months
DRd-treated patients had a 63% reduction in the risk of disease progression or death in comparison with Rd Responses continue to deepen in the DRd group with longer follow-up
Age and frailty
Prob
abilit
y of
sur
viva
l (%
)
Age < 75 yearsAge ≥ 75 years
0.00
0.25
0.50
0.75
1.00
0 0.5 1 1.5 2 2.5 3
Time since diagnosis
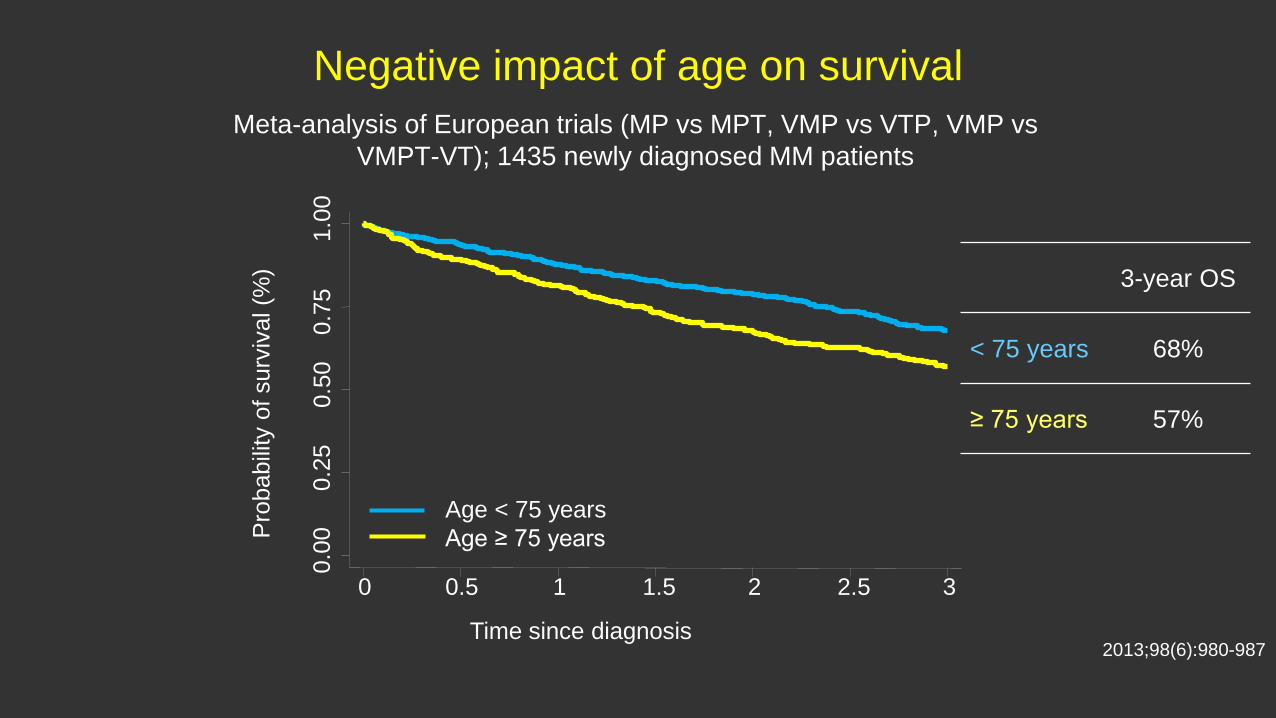
Negative impact of age on survivalMeta-analysis of European trials (MP vs MPT, VMP vs VTP, VMP vs
VMPT-VT); 1435 newly diagnosed MM patients
3-year OS
< 75 years 68%
≥ 75 years 57%
2013;98(6):980-987
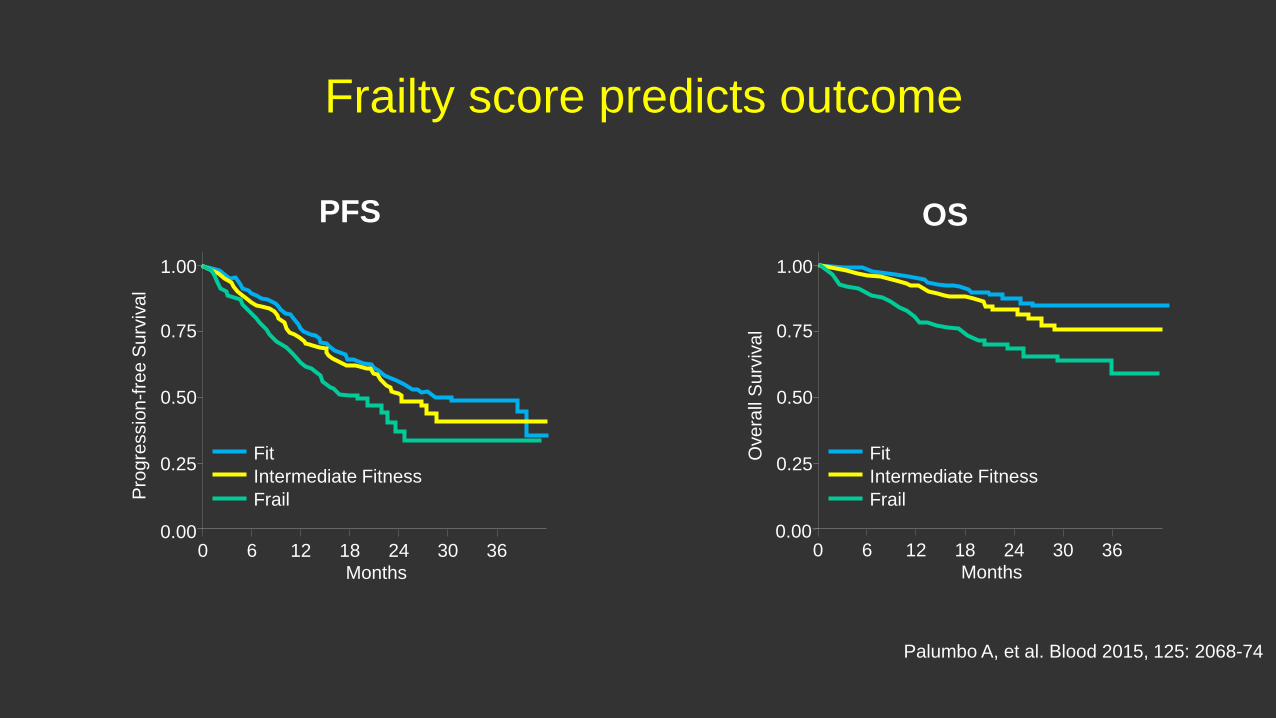
Frailty score predicts outcome
PFS OS
Prog
ress
ion-
free
Surv
ival
0.00
0.25
0.50
0.75
1.00
0 12 18 24 30 36Months
FitIntermediate FitnessFrail
6
Ove
rall
Surv
ival
0.25
0.50
0.75
1.00
FitIntermediate FitnessFrail
0.000 12 18 24 30 36
Months6
Palumbo A, et al. Blood 2015, 125: 2068-74
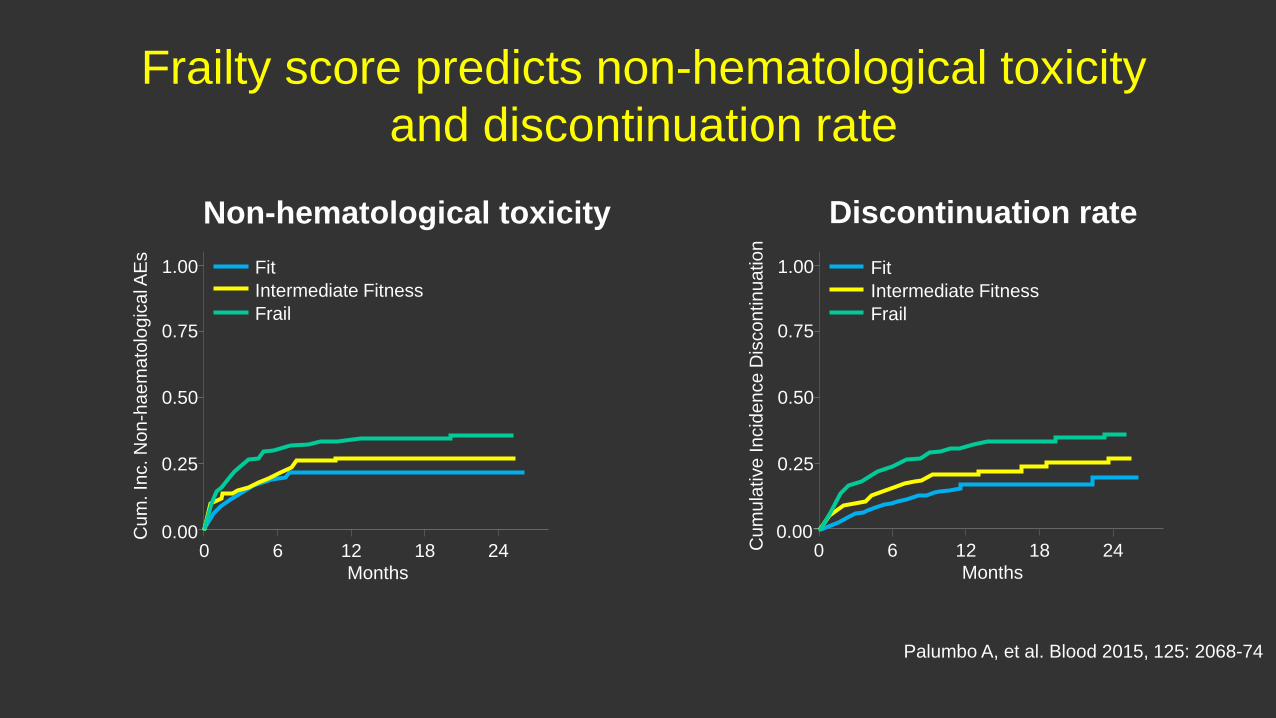
Frailty score predicts non-hematological toxicity and discontinuation rate
Discontinuation rate
Cum
. Inc
. Non
-hae
mat
olog
ical
AEs
0.00
0.25
0.50
0.75
1.00
0 12 18 24Months
FitIntermediate FitnessFrail
6 Cum
ulat
ive
Inci
denc
e D
isco
ntin
uatio
n
0.25
0.50
0.75
1.00 FitIntermediate FitnessFrail
0.000 12 18 24
Months6
Palumbo A, et al. Blood 2015, 125: 2068-74
Non-hematological toxicity
Conclusions• Plasma cell disorders are very relevant to the physician.
– VTE– Renal failure/AKI/nephrotic syndrome– Bone pain/SCC– Hypercalcaemia– Cardiomyopathy– Neuropathy – Infection/sepsis– Unexplained anaemia/raised ESR– Raised TP
Conclusions
• Plasma cell disorders are very relevant to the physician. • Myeloma can cause devastating problems that are largely
avoidable or reversible with prompt diagnosis.• The prognosis for all plasma cell disorders is improving rapidly
with multiple new therapies







![MP-100 MIDI foot switch...1. Switch on the device. 2. Press [Auto]. ð Automatic operation is started. 3. Switch off the device. 1.1.3 Symbols and signal words In this section you](https://static.fdocuments.us/doc/165x107/60b19542cbc740788b303441/mp-100-midi-foot-switch-1-switch-on-the-device-2-press-auto-automatic.jpg)









