Plasma cell dyscrasia with renal impairment including MGRS · Plasma cell dyscrasia with renal...
38
Plasma cell dyscrasia with renal impairment including MGRS ~ The importance of multi-departmental management ~ Dept. Nephrology, Japan Community Health Care Organization Sendai Hospital Shinichi Mizuno
-
Upload
nguyenphuc -
Category
Documents
-
view
218 -
download
0
Transcript of Plasma cell dyscrasia with renal impairment including MGRS · Plasma cell dyscrasia with renal...
Plasma cell dyscrasia with renal impairment including MGRS
~ The importance of multi-departmental management ~
Dept. Nephrology, Japan Community Health Care Organization Sendai Hospital
Shinichi Mizuno
Japanese Society of Myeloma COI Disclosure
Shinichi Mizuno
The author have no financial conflicts of interest to disclose concerning the presentation.
Looking from different angles
Myeloma
Nephrologists
Myeloma History
1844: mollities ossium fatigue, bone pain from fractures
(1845:abnormal urine protein)
1848: analysis of abnormal urine protein ‘hydrated deutoxide of albumen'
1873 : description of “multiple myeloma”
1875-95: description of plasma cell 1900 : plasma cell ⇒ Myeloma cell
Orthopaedic ?
Nephrology ?
1880:Bence Jones Protein(BJP)
Henry Bence Jones
Blood 2008; 111: 2962-72
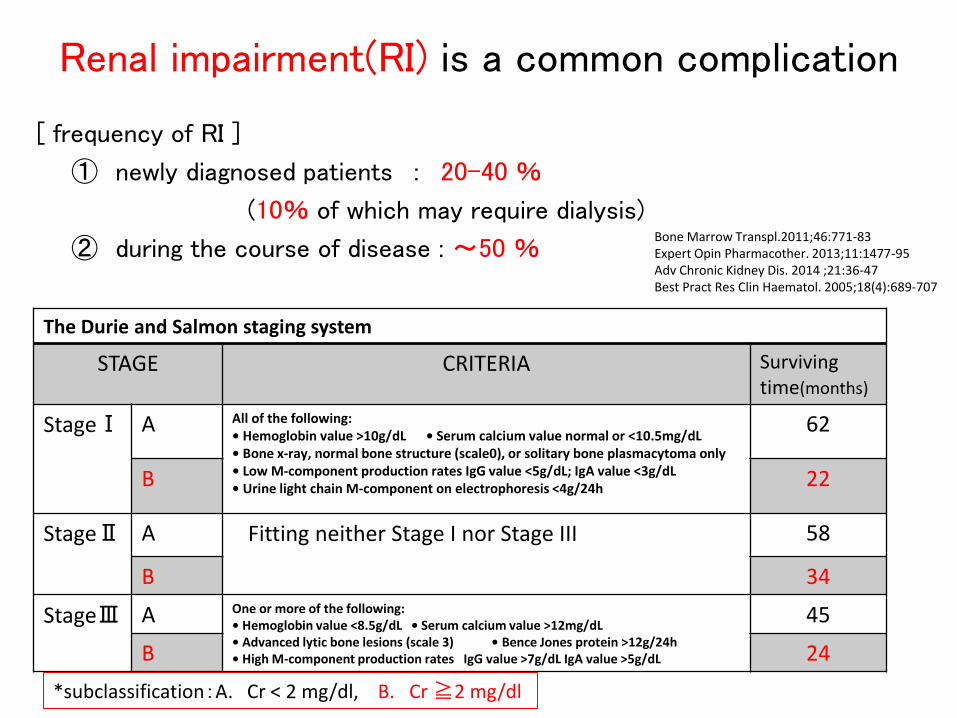
Renal impairment(RI) is a common complication
[ frequency of RI ]
① newly diagnosed patients : 20-40 %
(10% of which may require dialysis)
② during the course of disease : ~50 %
The Durie and Salmon staging system
STAGE CRITERIA Surviving time(months)
StageⅠ A All of the following: • Hemoglobin value >10g/dL • Serum calcium value normal or <10.5mg/dL • Bone x-ray, normal bone structure (scale0), or solitary bone plasmacytoma only • Low M-component production rates IgG value <5g/dL; IgA value <3g/dL • Urine light chain M-component on electrophoresis <4g/24h
62
B 22
StageⅡ A Fitting neither Stage I nor Stage III 58
B 34
StageⅢ A One or more of the following: • Hemoglobin value <8.5g/dL • Serum calcium value >12mg/dL • Advanced lytic bone lesions (scale 3) • Bence Jones protein >12g/24h • High M-component production rates IgG value >7g/dL IgA value >5g/dL
45
B 24
*subclassification:A. Cr < 2 mg/dl, B. Cr ≧2 mg/dl
Bone Marrow Transpl.2011;46:771-83 Expert Opin Pharmacother. 2013;11:1477-95 Adv Chronic Kidney Dis. 2014 ;21:36-47 Best Pract Res Clin Haematol. 2005;18(4):689-707
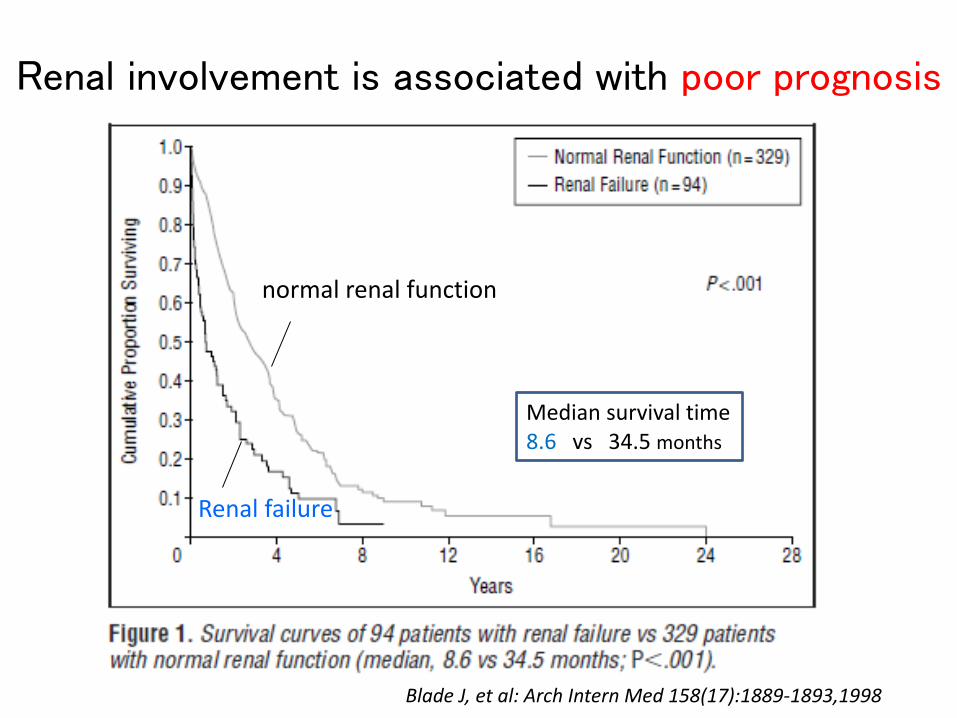
Renal involvement is associated with poor prognosis
Blade J, et al: Arch Intern Med 158(17):1889-1893,1998
Median survival time 8.6 vs 34.5 months
normal renal function
Renal failure
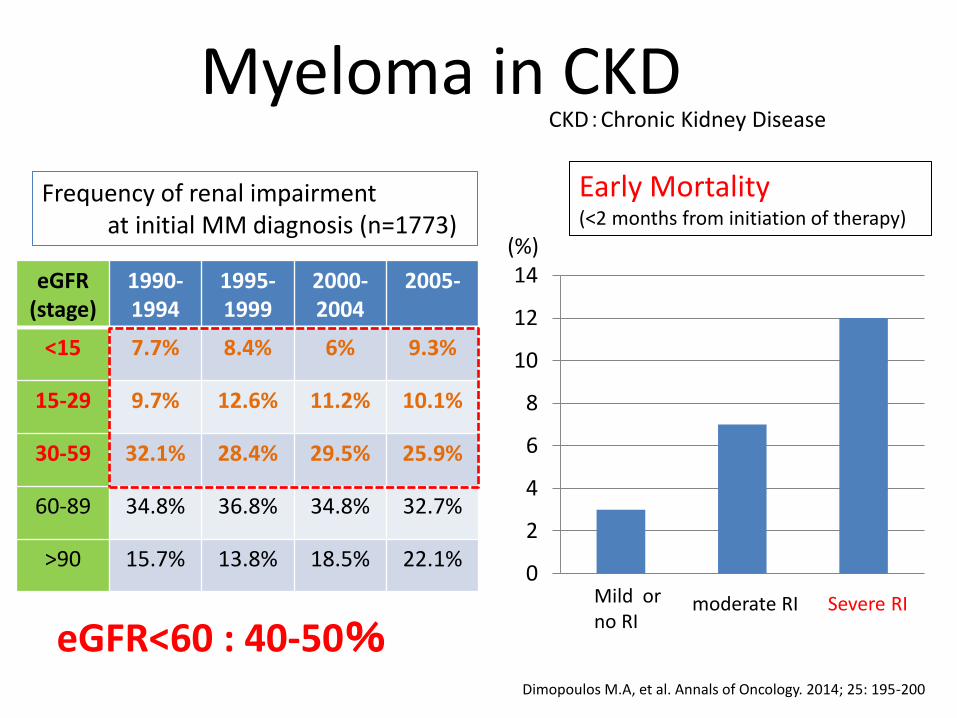
Myeloma in CKD
Dimopoulos M.A, et al. Annals of Oncology. 2014; 25: 195-200
0
2
4
6
8
10
12
14
Mild or no RI
moderate RI Severe RI
Early Mortality (<2 months from initiation of therapy)
(%)
eGFR (stage)
1990-1994
1995-1999
2000-2004
2005-
<15 7.7% 8.4% 6% 9.3%
15-29 9.7% 12.6% 11.2% 10.1%
30-59 32.1% 28.4% 29.5% 25.9%
60-89 34.8% 36.8% 34.8% 32.7%
>90 15.7% 13.8% 18.5% 22.1%
Frequency of renal impairment at initial MM diagnosis (n=1773)
CKD:Chronic Kidney Disease
eGFR<60 : 40-50%
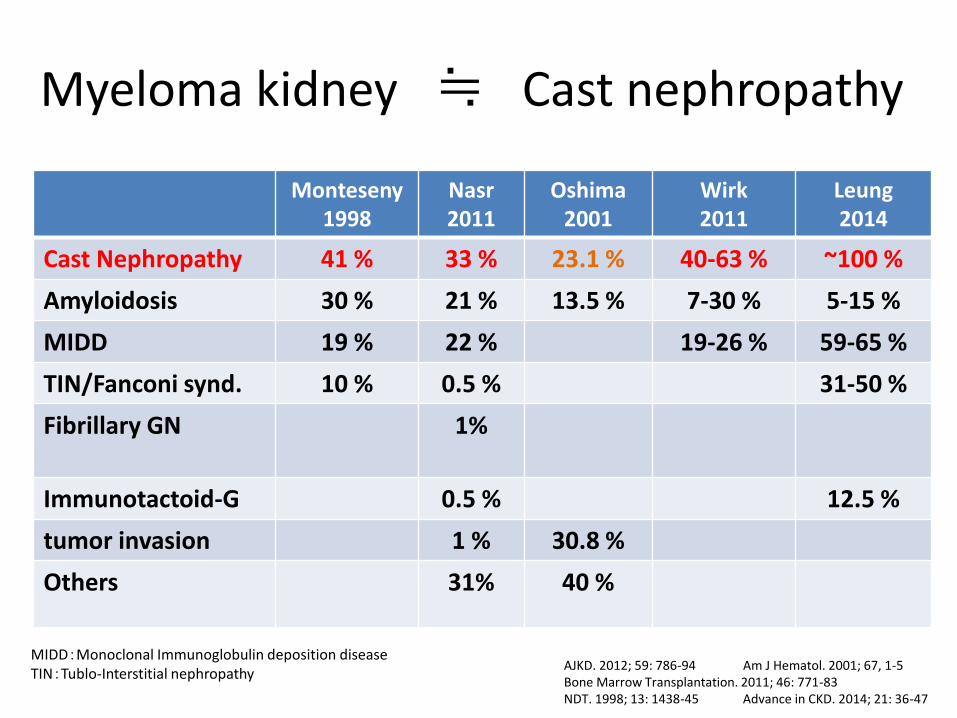
Myeloma kidney ≒ Cast nephropathy
Monteseny 1998
Nasr 2011
Oshima 2001
Wirk 2011
Leung 2014
Cast Nephropathy 41 % 33 % 23.1 % 40-63 % ~100 %
Amyloidosis 30 % 21 % 13.5 % 7-30 % 5-15 %
MIDD 19 % 22 % 19-26 % 59-65 %
TIN/Fanconi synd. 10 % 0.5 % 31-50 %
Fibrillary GN 1%
Immunotactoid-G 0.5 % 12.5 %
tumor invasion 1 % 30.8 %
Others
31% 40 %
AJKD. 2012; 59: 786-94 Am J Hematol. 2001; 67, 1-5 Bone Marrow Transplantation. 2011; 46: 771-83 NDT. 1998; 13: 1438-45 Advance in CKD. 2014; 21: 36-47
MIDD:Monoclonal Immunoglobulin deposition disease TIN:Tublo-Interstitial nephropathy
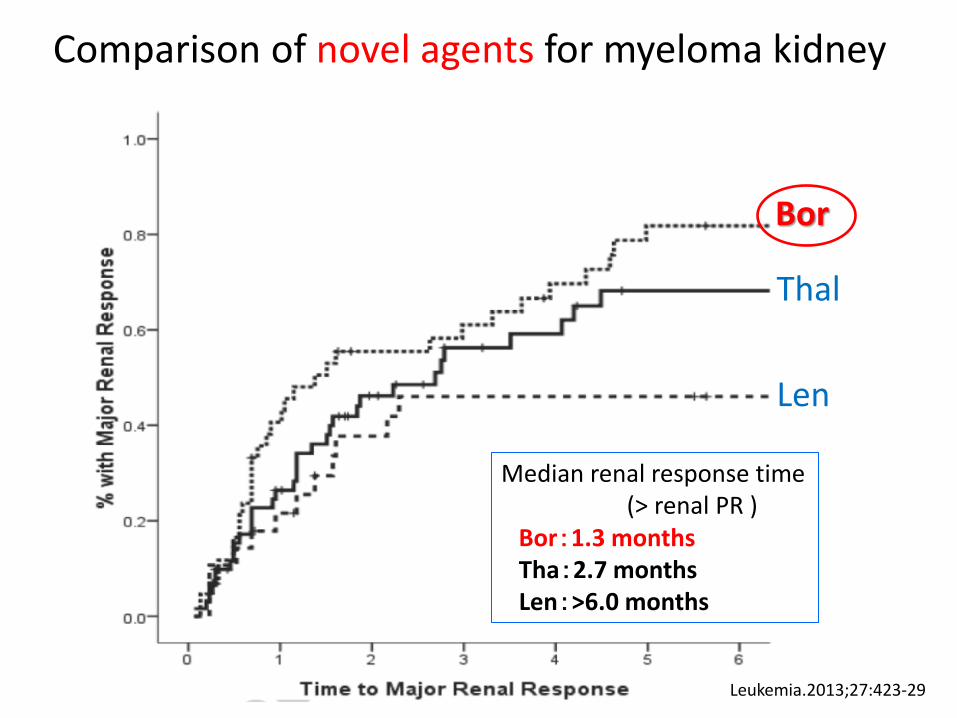
Comparison of novel agents for myeloma kidney
Bor
Thal
Len
Leukemia.2013;27:423-29
Median renal response time (> renal PR ) Bor:1.3 months Tha:2.7 months Len:>6.0 months
(thick ascending loop of Henle)
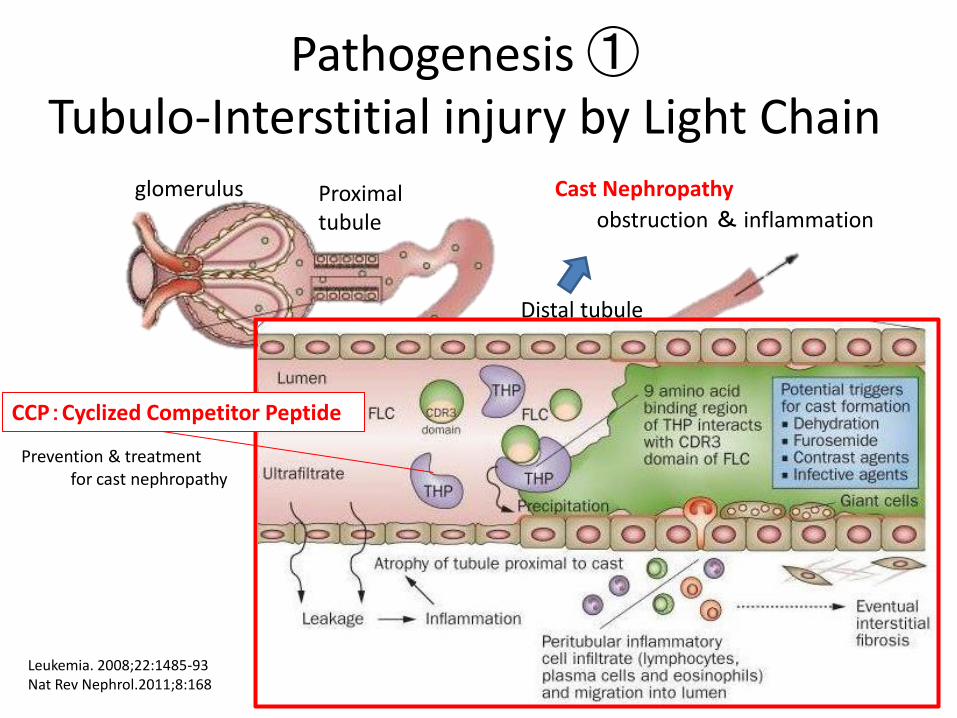
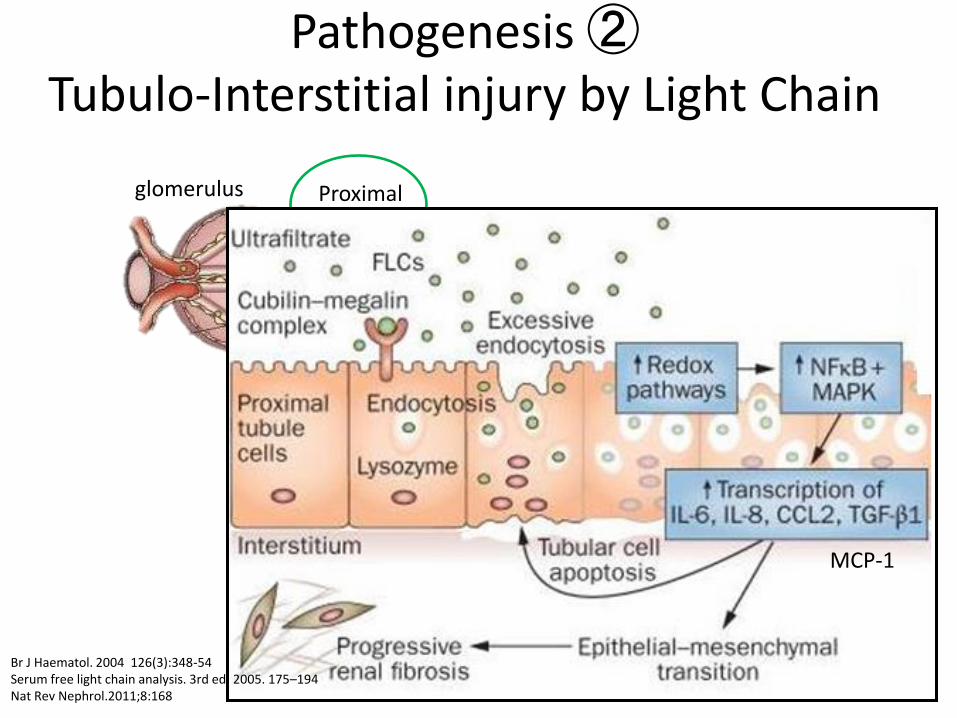
Pathogenesis ① Tubulo-Interstitial injury by Light Chain
glomerulus Proximal tubule obstruction & inflammation
Distal tubule
Leukemia. 2008;22:1485-93 Nat Rev Nephrol.2011;8:168
Cast Nephropathy
CCP:Cyclized Competitor Peptide
Prevention & treatment for cast nephropathy
Proximal tubule Cast-Nephropathy
Distal tubule
MCP-1
glomerulus
Br J Haematol. 2004 126(3):348-54 Serum free light chain analysis. 3rd ed; 2005. 175–194 Nat Rev Nephrol.2011;8:168
Pathogenesis ② Tubulo-Interstitial injury by Light Chain
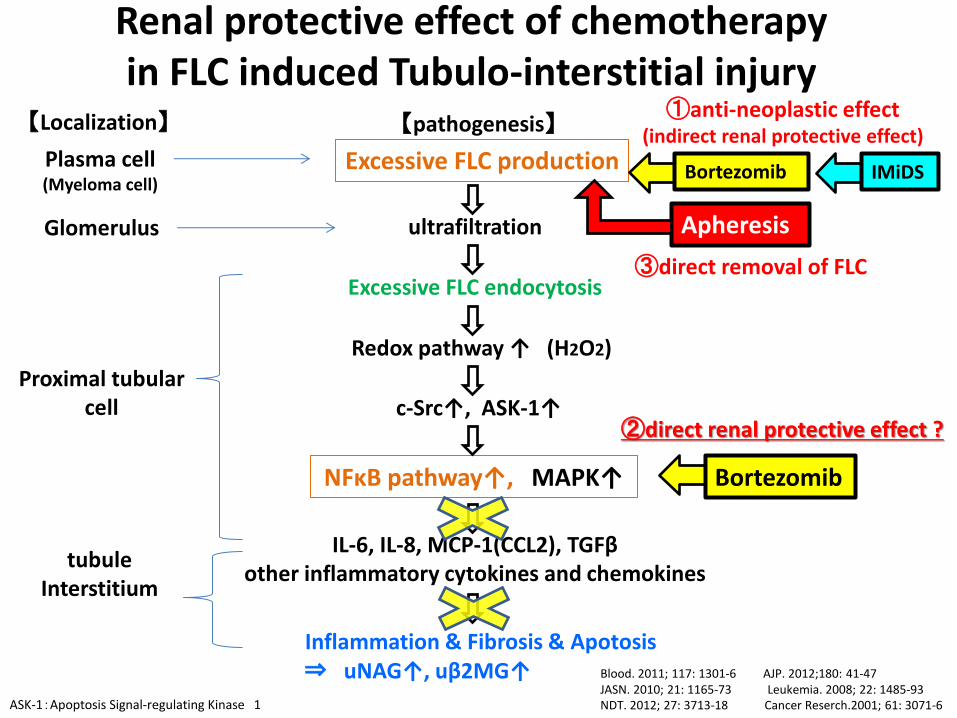
Renal protective effect of chemotherapy in FLC induced Tubulo-interstitial injury
Excessive FLC production
Redox pathway ↑ (H2O2)
NFκB pathway↑, MAPK↑
Inflammation & Fibrosis & Apotosis ⇒ uNAG↑, uβ2MG↑
IL-6, IL-8, MCP-1(CCL2), TGFβ other inflammatory cytokines and chemokines
Blood. 2011; 117: 1301-6 AJP. 2012;180: 41-47 JASN. 2010; 21: 1165-73 Leukemia. 2008; 22: 1485-93 NDT. 2012; 27: 3713-18 Cancer Reserch.2001; 61: 3071-6
c-Src↑, ASK-1↑
ultrafiltration
Excessive FLC endocytosis
Plasma cell (Myeloma cell)
Glomerulus
Proximal tubular cell
tubule Interstitium
【Localization】 【pathogenesis】
Bortezomib
①anti-neoplastic effect (indirect renal protective effect)
IMiDS
Bortezomib
②direct renal protective effect ?
ASK-1:Apoptosis Signal-regulating Kinase 1
Apheresis
③direct removal of FLC
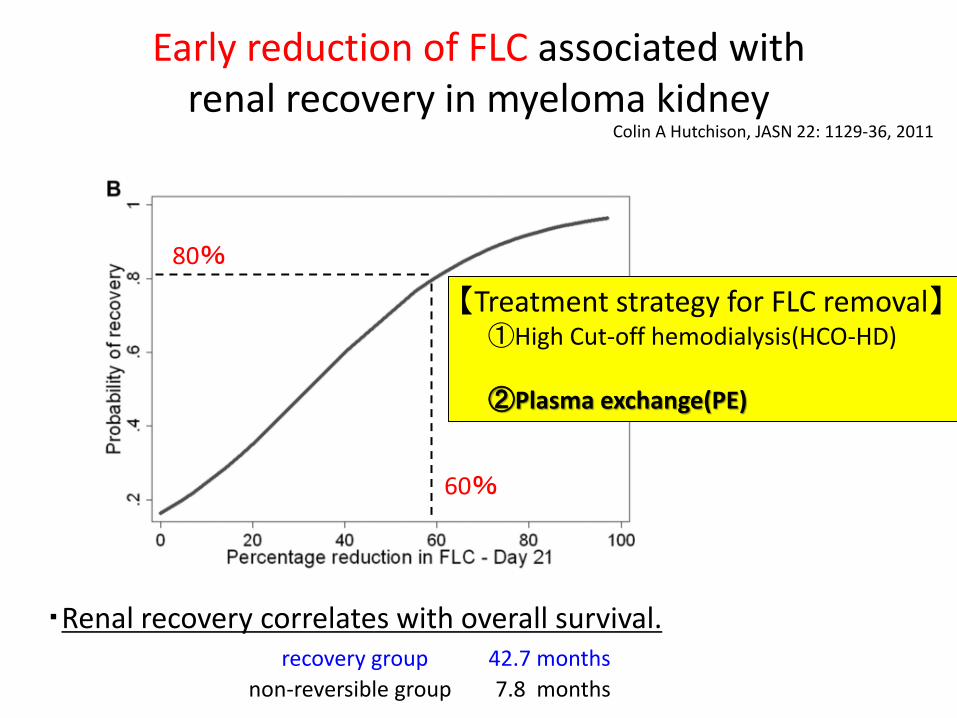
Early reduction of FLC associated with renal recovery in myeloma kidney
Colin A Hutchison, JASN 22: 1129-36, 2011
60%
80%
・Renal recovery correlates with overall survival. recovery group 42.7 months
non-reversible group 7.8 months
【Treatment strategy for FLC removal】 ①High Cut-off hemodialysis(HCO-HD) ②Plasma exchange(PE)
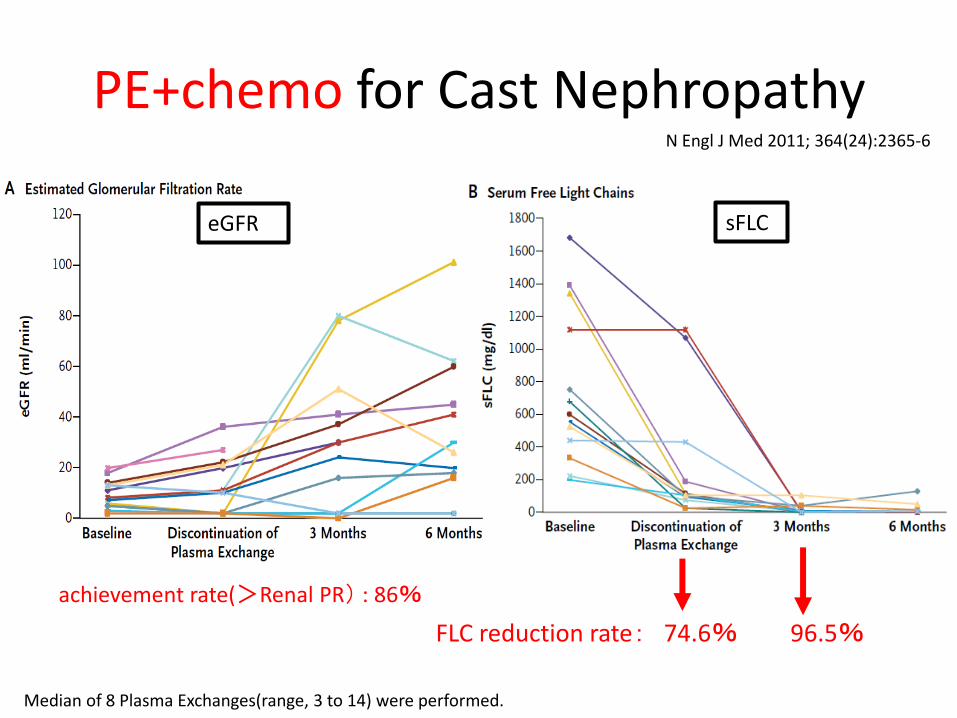
PE+chemo for Cast Nephropathy
achievement rate(>Renal PR) : 86%
FLC reduction rate: 74.6% 96.5%
N Engl J Med 2011; 364(24):2365-6
sFLC eGFR
Median of 8 Plasma Exchanges(range, 3 to 14) were performed.
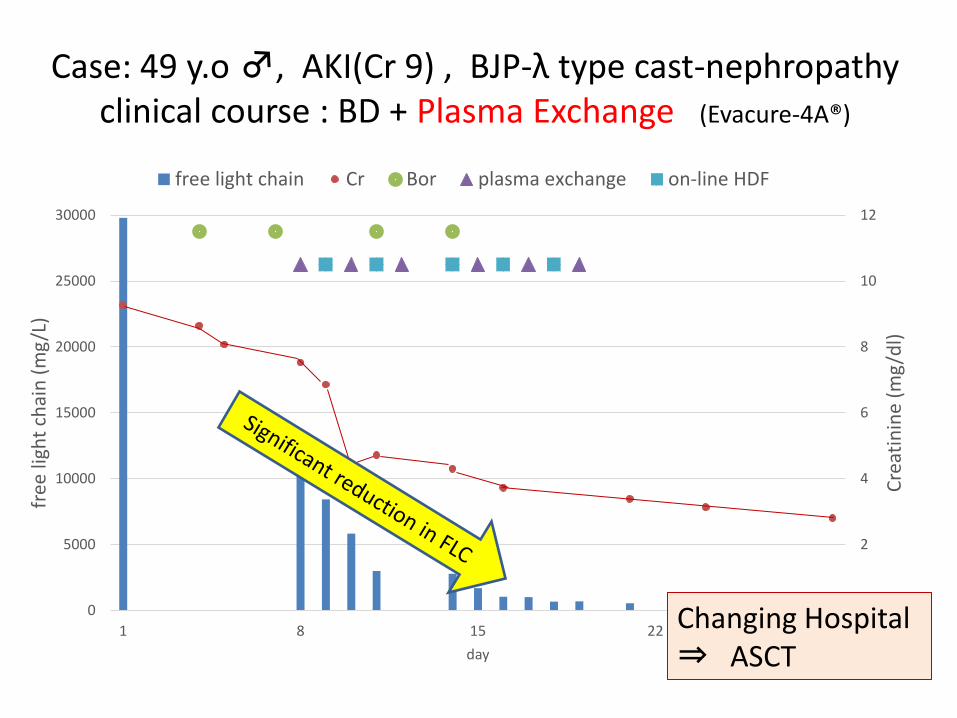
Case: 49 y.o ♂, AKI(Cr 9) , BJP-λ type cast-nephropathy clinical course : BD + Plasma Exchange (Evacure-4A®)
0
2
4
6
8
10
12
0
5000
10000
15000
20000
25000
30000
1 8 15 22 29
Cre
atin
ine
(mg
/dl)
free
ligh
t ch
ain
(m
g/L
)
day
free light chain Cr Bor plasma exchange on-line HDF
Changing Hospital ⇒ ASCT
Non-Cast nephropathy
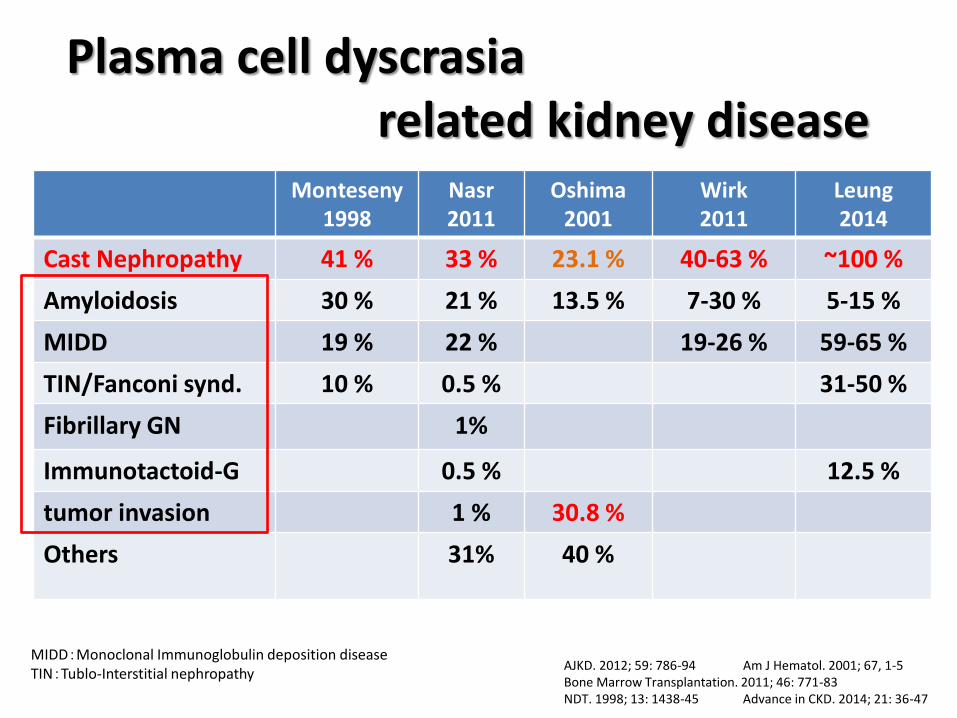
Monteseny 1998
Nasr 2011
Oshima 2001
Wirk 2011
Leung 2014
Cast Nephropathy 41 % 33 % 23.1 % 40-63 % ~100 %
Amyloidosis 30 % 21 % 13.5 % 7-30 % 5-15 %
MIDD 19 % 22 % 19-26 % 59-65 %
TIN/Fanconi synd. 10 % 0.5 % 31-50 %
Fibrillary GN 1%
Immunotactoid-G 0.5 % 12.5 %
tumor invasion 1 % 30.8 %
Others
31% 40 %
AJKD. 2012; 59: 786-94 Am J Hematol. 2001; 67, 1-5 Bone Marrow Transplantation. 2011; 46: 771-83 NDT. 1998; 13: 1438-45 Advance in CKD. 2014; 21: 36-47
MIDD:Monoclonal Immunoglobulin deposition disease TIN:Tublo-Interstitial nephropathy
Plasma cell dyscrasia related kidney disease
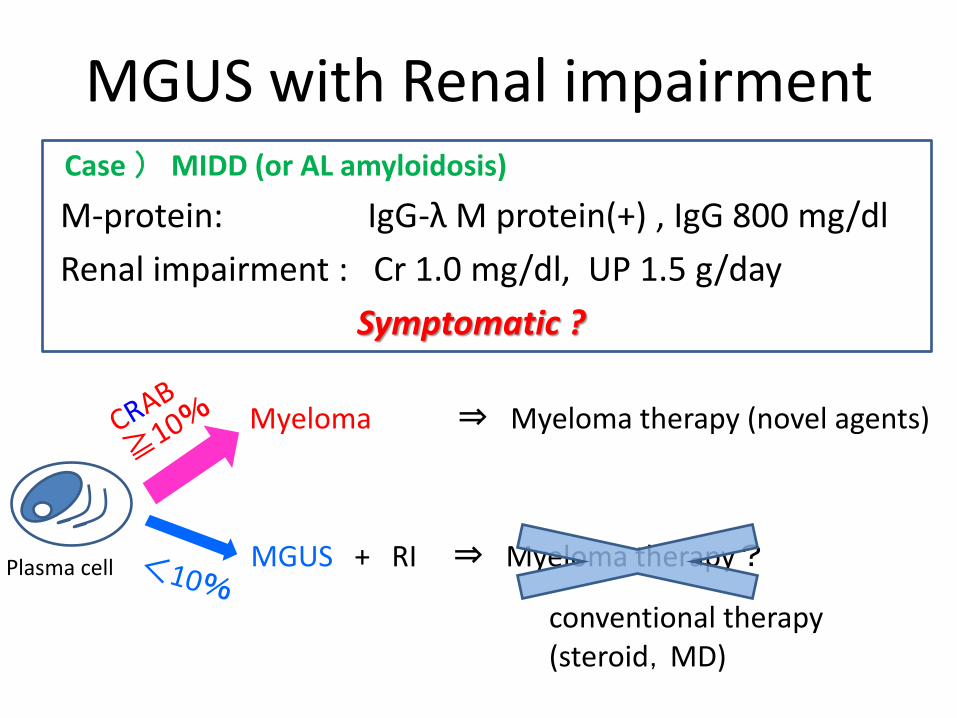
MGUS with Renal impairment Case ) MIDD (or AL amyloidosis)
M-protein: IgG-λ M protein(+) , IgG 800 mg/dl
Renal impairment : Cr 1.0 mg/dl, UP 1.5 g/day
Symptomatic ?
Myeloma ⇒ Myeloma therapy (novel agents)
MGUS + RI ⇒ Myeloma therapy?
conventional therapy (steroid,MD)
Plasma cell
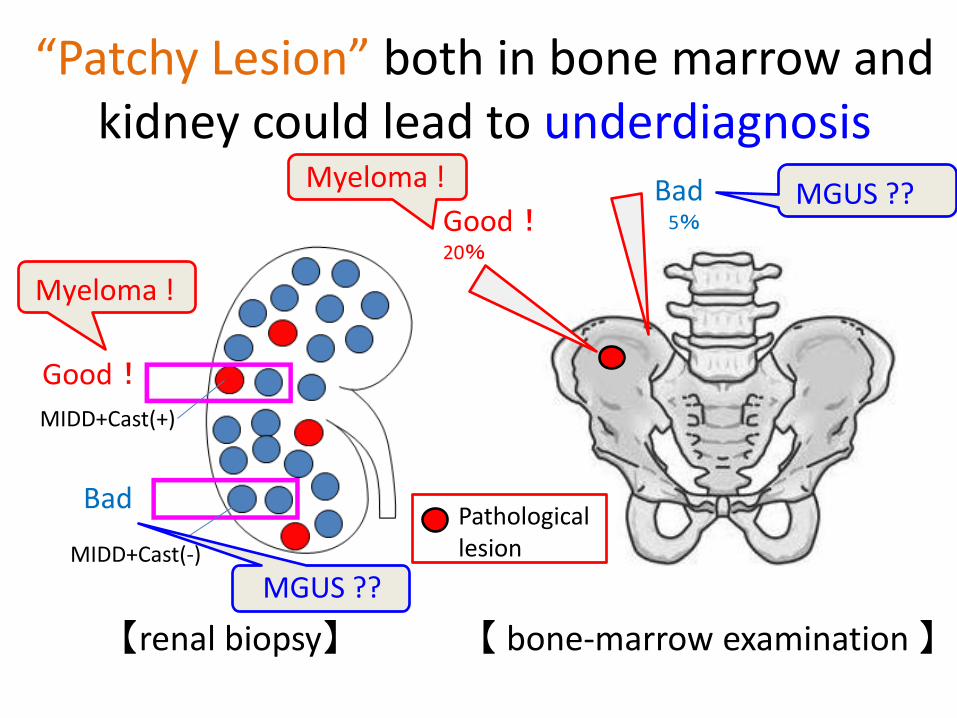
“Patchy Lesion” both in bone marrow and kidney could lead to underdiagnosis
Good! 20%
Bad 5%
【 bone-marrow examination 】
Pathological lesion
【renal biopsy】
MIDD+Cast(-)
MIDD+Cast(+)
Good!
Bad
Myeloma !
Myeloma ! MGUS ??
MGUS ??
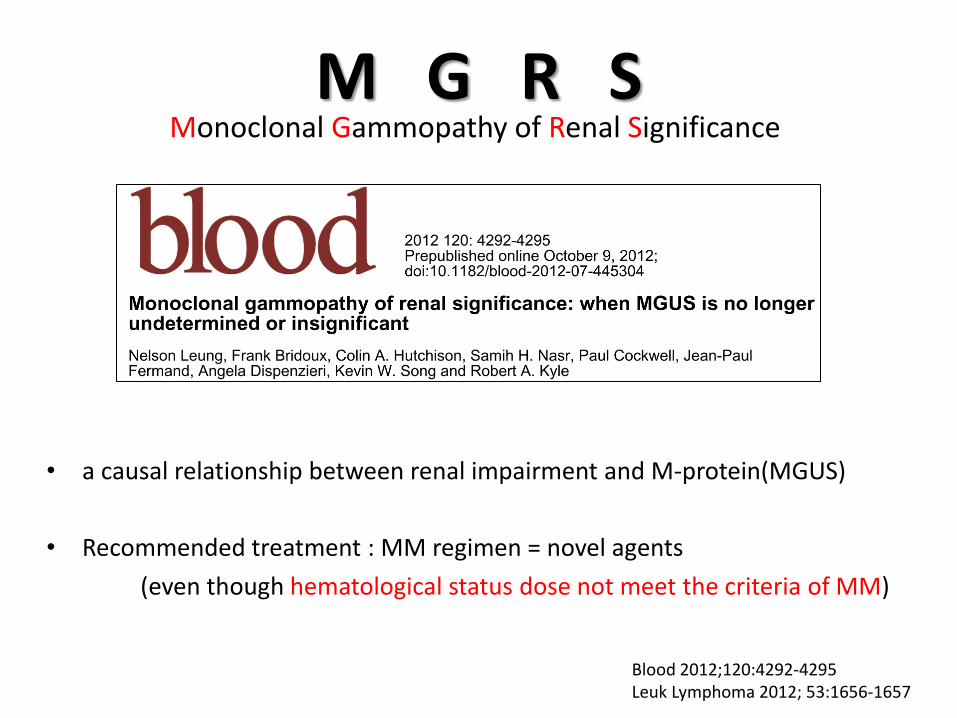
M G R S
• a causal relationship between renal impairment and M-protein(MGUS)
• Recommended treatment : MM regimen = novel agents
(even though hematological status dose not meet the criteria of MM)
Monoclonal Gammopathy of Renal Significance
Blood 2012;120:4292-4295 Leuk Lymphoma 2012; 53:1656-1657
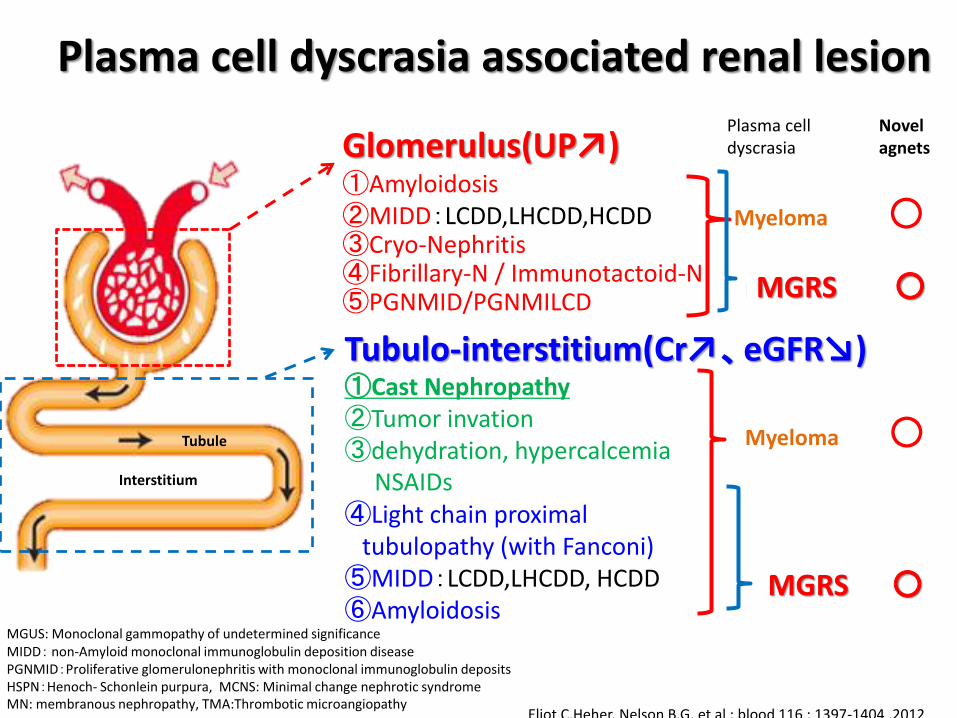
Plasma cell dyscrasia associated renal lesion
Eliot C.Heher, Nelson B.G, et al : blood 116 ; 1397-1404 ,2012
Glomerulus(UP↗) ①Amyloidosis ②MIDD:LCDD,LHCDD,HCDD ③Cryo-Nephritis ④Fibrillary-N / Immunotactoid-N ⑤PGNMID/PGNMILCD Tubulo-interstitium(Cr↗、eGFR↘) ①Cast Nephropathy ②Tumor invation ③dehydration, hypercalcemia NSAIDs ④Light chain proximal tubulopathy (with Fanconi) ⑤MIDD:LCDD,LHCDD, HCDD ⑥Amyloidosis MGUS: Monoclonal gammopathy of undetermined significance
MIDD: non-Amyloid monoclonal immunoglobulin deposition disease PGNMID:Proliferative glomerulonephritis with monoclonal immunoglobulin deposits HSPN:Henoch- Schonlein purpura, MCNS: Minimal change nephrotic syndrome MN: membranous nephropathy, TMA:Thrombotic microangiopathy
Interstitium
Myeloma
Myeloma
Novel agnets
Plasma cell dyscrasia
○
○
×
×
MGUS
MGUS MGRS ○
MGRS ○
Tubule
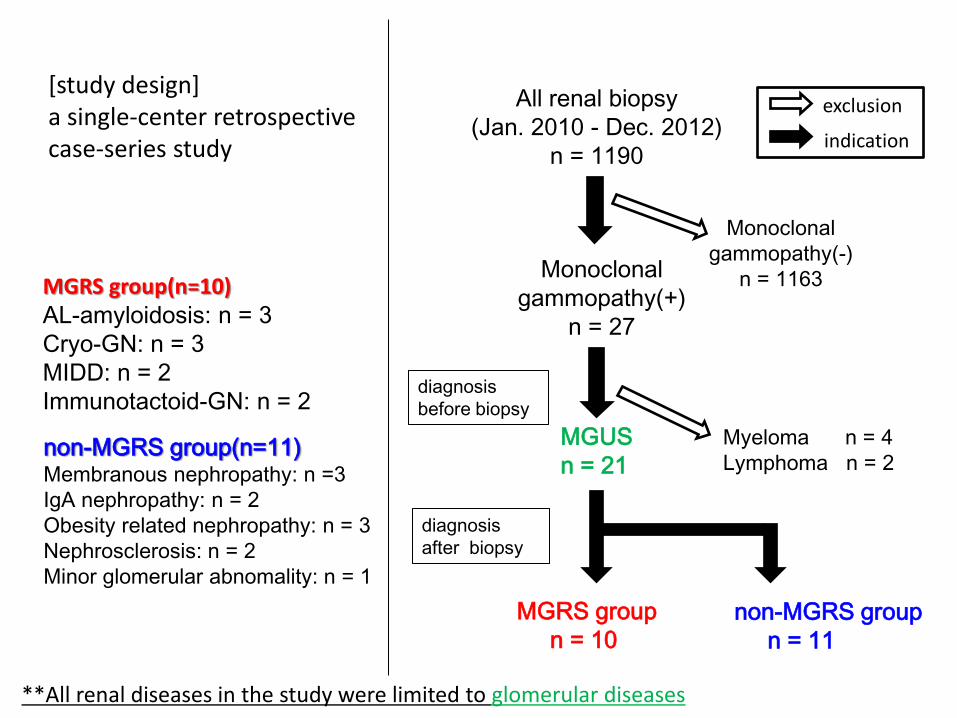
All renal biopsy
(Jan. 2010 - Dec. 2012)
n = 1190
Monoclonal
gammopathy(-)
n = 1163 Monoclonal
gammopathy(+)
n = 27
Myeloma n = 4
Lymphoma n = 2
MGRS group
n = 10
non-MGRS group
n = 11
diagnosis
after biopsy
diagnosis
before biopsy
exclusion
MGUS
n = 21
indication
[study design] a single-center retrospective case-series study
MGRS group(n=10) AL-amyloidosis: n = 3
Cryo-GN: n = 3
MIDD: n = 2
Immunotactoid-GN: n = 2
non-MGRS group(n=11) Membranous nephropathy: n =3
IgA nephropathy: n = 2
Obesity related nephropathy: n = 3
Nephrosclerosis: n = 2
Minor glomerular abnomality: n = 1
**All renal diseases in the study were limited to glomerular diseases
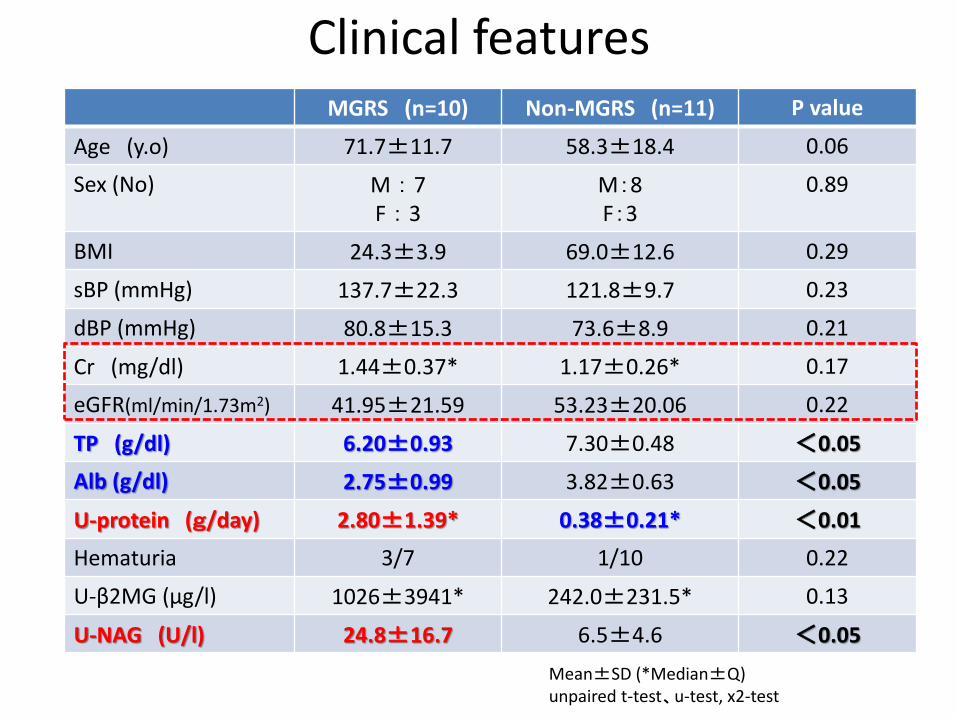
Clinical features MGRS (n=10) Non-MGRS (n=11) P value
Age (y.o) 71.7±11.7 58.3±18.4 0.06
Sex (No) M : 7 F : 3
M:8 F:3
0.89
BMI 24.3±3.9 69.0±12.6 0.29
sBP (mmHg) 137.7±22.3 121.8±9.7 0.23
dBP (mmHg) 80.8±15.3 73.6±8.9 0.21
Cr (mg/dl) 1.44±0.37* 1.17±0.26* 0.17
eGFR(ml/min/1.73m2) 41.95±21.59 53.23±20.06 0.22
TP (g/dl) 6.20±0.93 7.30±0.48 <0.05
Alb (g/dl) 2.75±0.99 3.82±0.63 <0.05
U-protein (g/day) 2.80±1.39* 0.38±0.21* <0.01
Hematuria 3/7 1/10 0.22
U-β2MG (μg/l) 1026±3941* 242.0±231.5* 0.13
U-NAG (U/l) 24.8±16.7 6.5±4.6 <0.05
Mean±SD (*Median±Q) unpaired t-test、u-test, x2-test
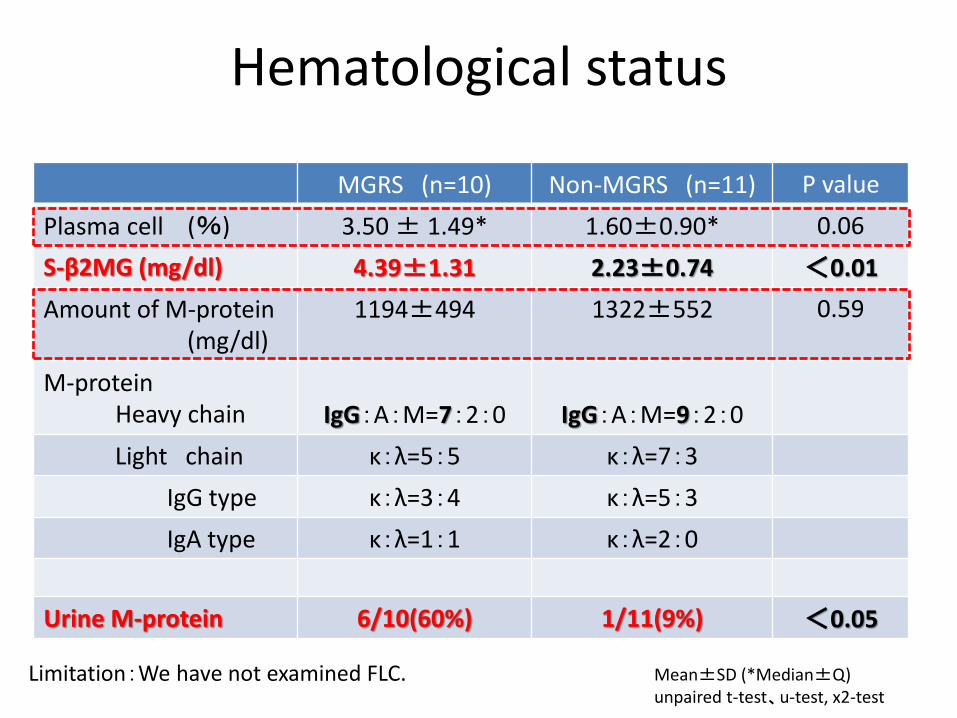
Hematological status
MGRS (n=10) Non-MGRS (n=11) P value
Plasma cell (%) 3.50 ± 1.49* 1.60±0.90* 0.06
S-β2MG (mg/dl) 4.39±1.31 2.23±0.74 <0.01
Amount of M-protein (mg/dl)
1194±494 1322±552 0.59
M-protein Heavy chain
IgG:A:M=7:2:0
IgG:A:M=9:2:0
Light chain κ:λ=5:5 κ:λ=7:3
IgG type κ:λ=3:4 κ:λ=5:3
IgA type κ:λ=1:1 κ:λ=2:0
Urine M-protein 6/10(60%) 1/11(9%) <0.05
Mean±SD (*Median±Q) unpaired t-test、u-test, x2-test
Limitation:We have not examined FLC.
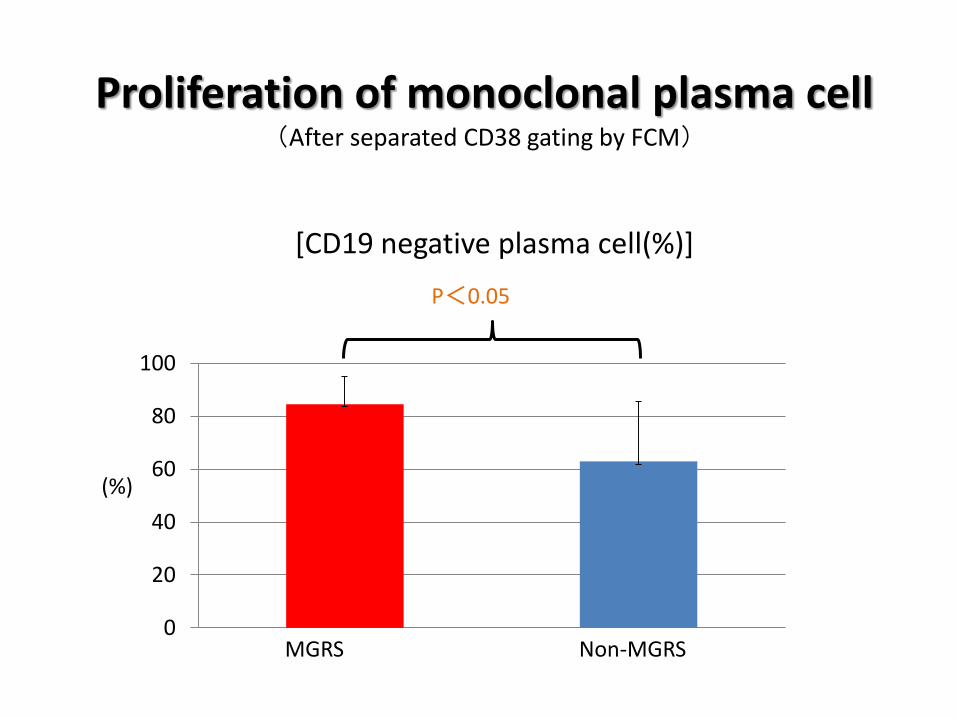
Proliferation of monoclonal plasma cell (After separated CD38 gating by FCM)
MGRS Non-MGRS
P<0.05
(%)
0
20
40
60
80
100
[CD19 negative plasma cell(%)]
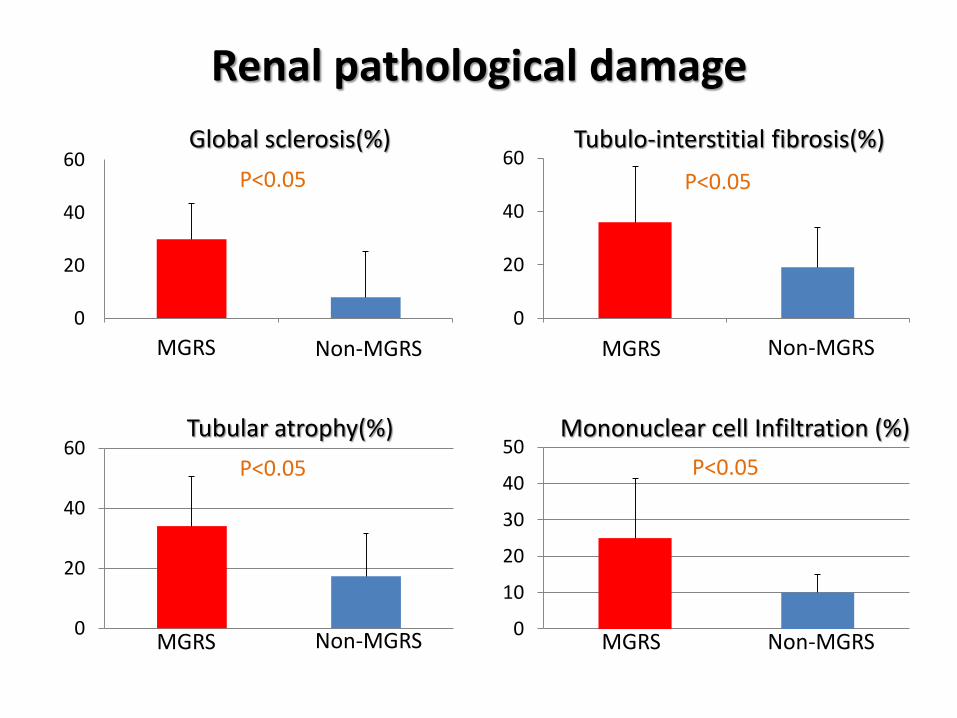
Renal pathological damage
0
20
40
60
1 2
Global sclerosis(%)
P<0.05
0
20
40
60
1 2
Tubulo-interstitial fibrosis(%)
P<0.05
0
20
40
60Tubular atrophy(%)
MGRS
MGRS
MGRS Non-MGRS
Non-MGRS
Non-MGRS
0
10
20
30
40
50
Non-MGRS MGRS
P<0.05 P<0.05
Mononuclear cell Infiltration (%)
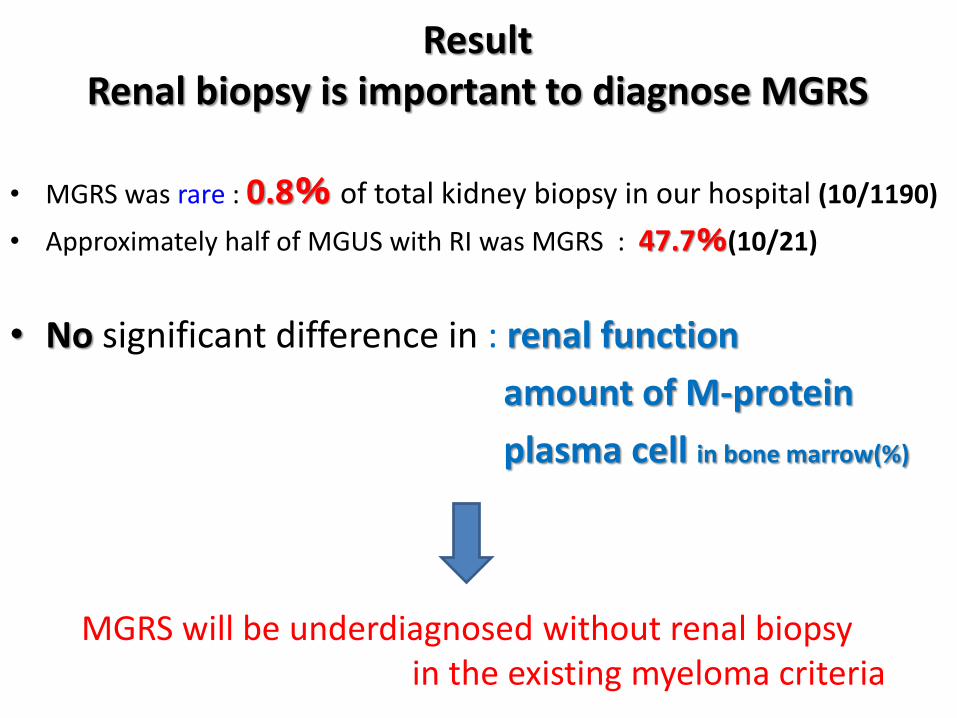
• MGRS was rare : 0.8% of total kidney biopsy in our hospital (10/1190)
• Approximately half of MGUS with RI was MGRS : 47.7%(10/21)
• No significant difference in : renal function
amount of M-protein
plasma cell in bone marrow(%)
Result Renal biopsy is important to diagnose MGRS
MGRS will be underdiagnosed without renal biopsy in the existing myeloma criteria
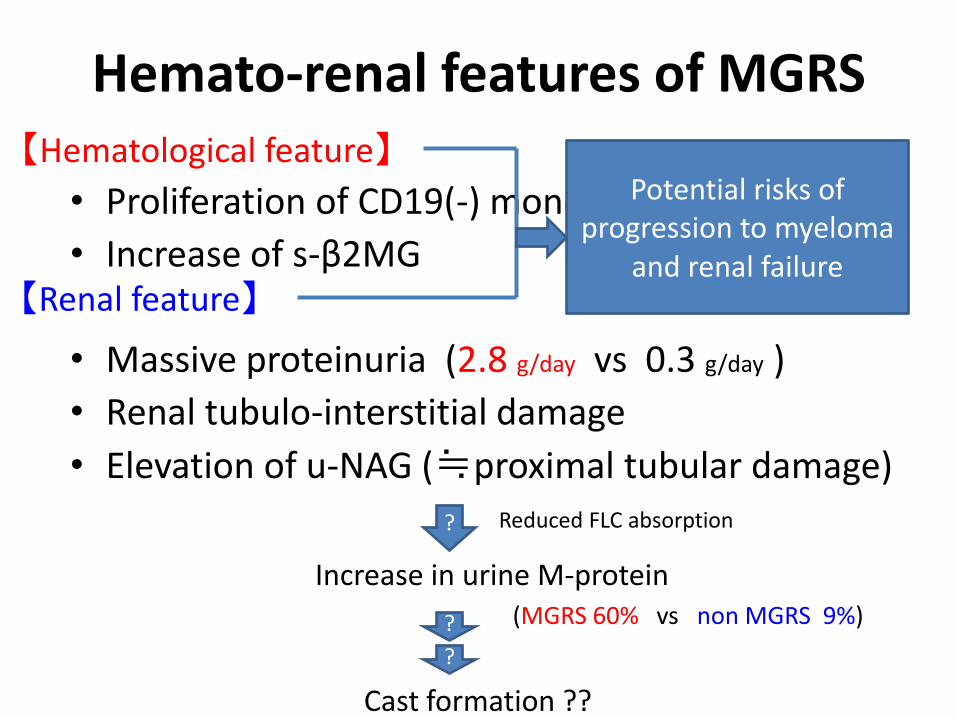
Hemato-renal features of MGRS
• Proliferation of CD19(-) monoclonal plasma cell
• Increase of s-β2MG
• Massive proteinuria (2.8 g/day vs 0.3 g/day )
• Renal tubulo-interstitial damage
• Elevation of u-NAG (≒proximal tubular damage)
【Hematological feature】
【Renal feature】
? Reduced FLC absorption
Increase in urine M-protein (MGRS 60% vs non MGRS 9%) ?
Cast formation ??
?
Potential risks of progression to myeloma
and renal failure
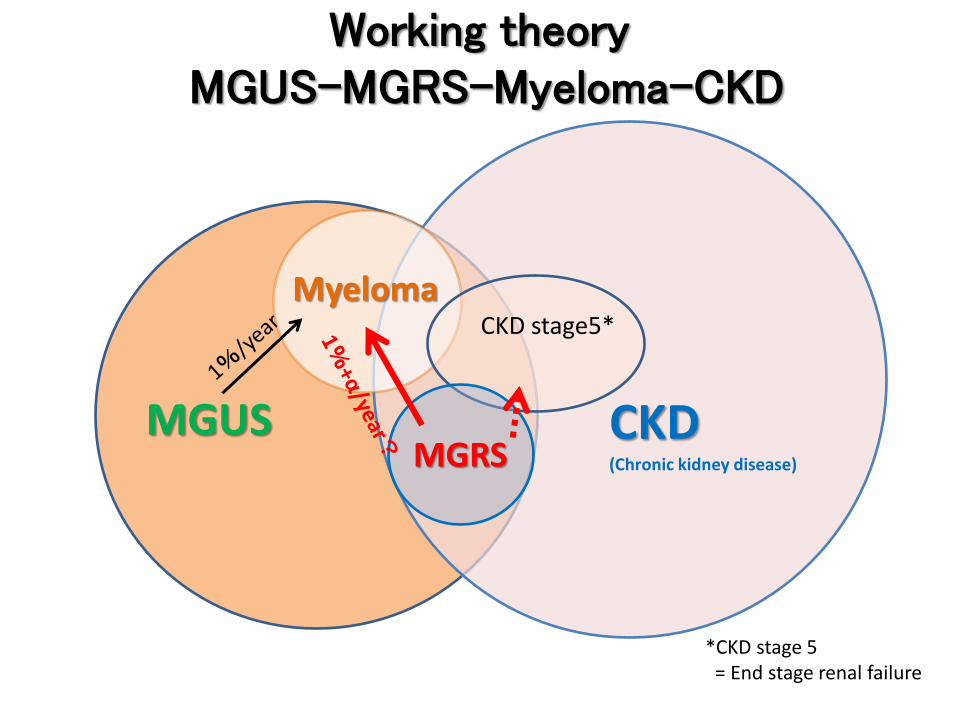
MGUS
Working theory MGUS-MGRS-Myeloma-CKD
CKD (Chronic kidney disease)
Myeloma CKD stage5*
*CKD stage 5 = End stage renal failure
MGRS
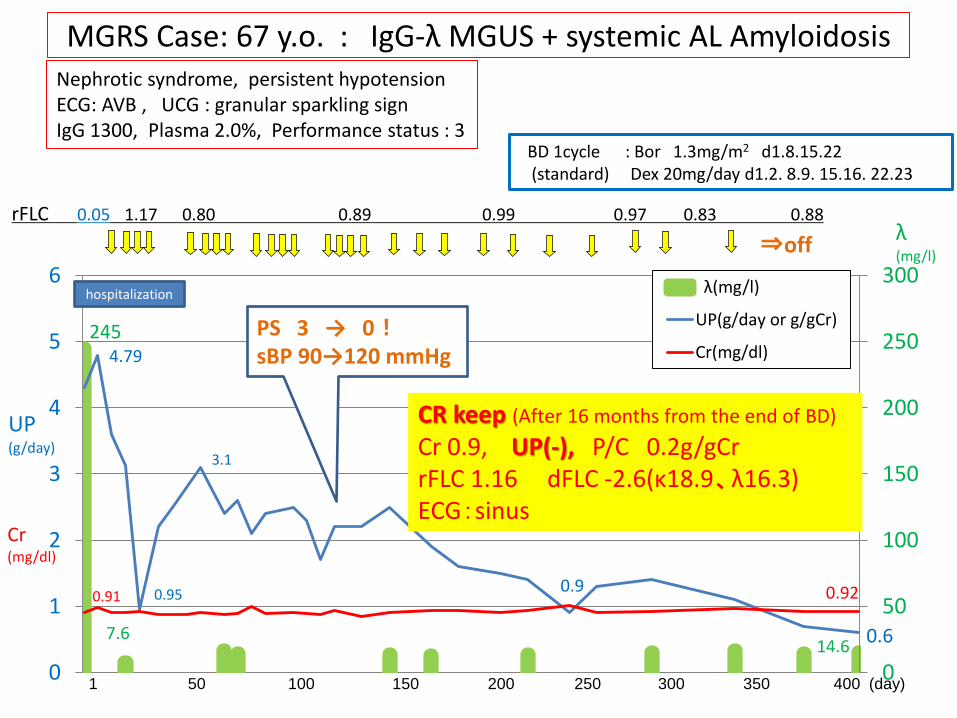
MGRS Case: 67 y.o. : IgG-λ MGUS + systemic AL Amyloidosis
rFLC 0.05 1.17 0.80 0.89 0.99 0.97 0.83 0.88
245
7.6 14.6
4.79
0.95
3.1
0.9
0.6
0.91 0.92
0
50
100
150
200
250
300
0
1
2
3
4
5
6 λ(mg/l)
UP(g/day or g/gCr)
Cr(mg/dl)
1 50 100 150 200 250 300 350 400 (day)
BD 1cycle : Bor 1.3mg/m2 d1.8.15.22 (standard) Dex 20mg/day d1.2. 8.9. 15.16. 22.23
UP (g/day)
Cr (mg/dl)
λ (mg/l)
hospitalization
PS 3 → 0! sBP 90→120 mmHg
⇒off
CR keep (After 16 months from the end of BD)
Cr 0.9, UP(-), P/C 0.2g/gCr rFLC 1.16 dFLC -2.6(κ18.9、λ16.3) ECG:sinus
Nephrotic syndrome, persistent hypotension ECG: AVB , UCG : granular sparkling sign IgG 1300, Plasma 2.0%, Performance status : 3
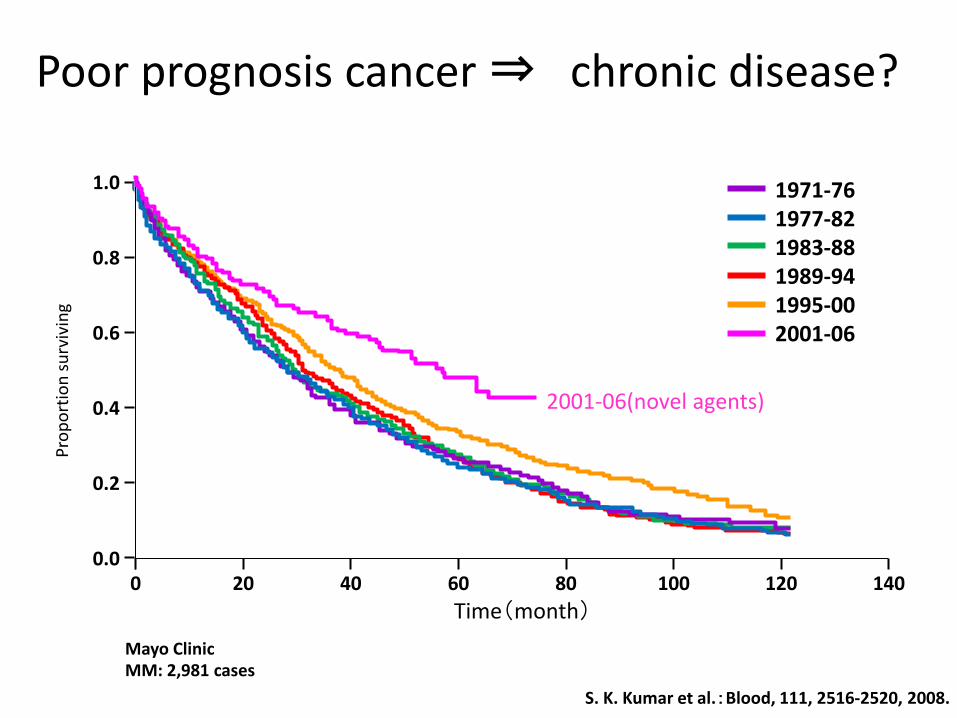
Poor prognosis cancer ⇒ chronic disease?
0 0.0
20 40 60 80 120
1.0
0.8
0.4
Time(month)
0.6
0.2
140 100
Pro
po
rtio
n s
urv
ivin
g
1971-76 1977-82 1983-88 1989-94 1995-00 2001-06
S. K. Kumar et al.:Blood, 111, 2516-2520, 2008.
Mayo Clinic MM: 2,981 cases
2001-06(novel agents)
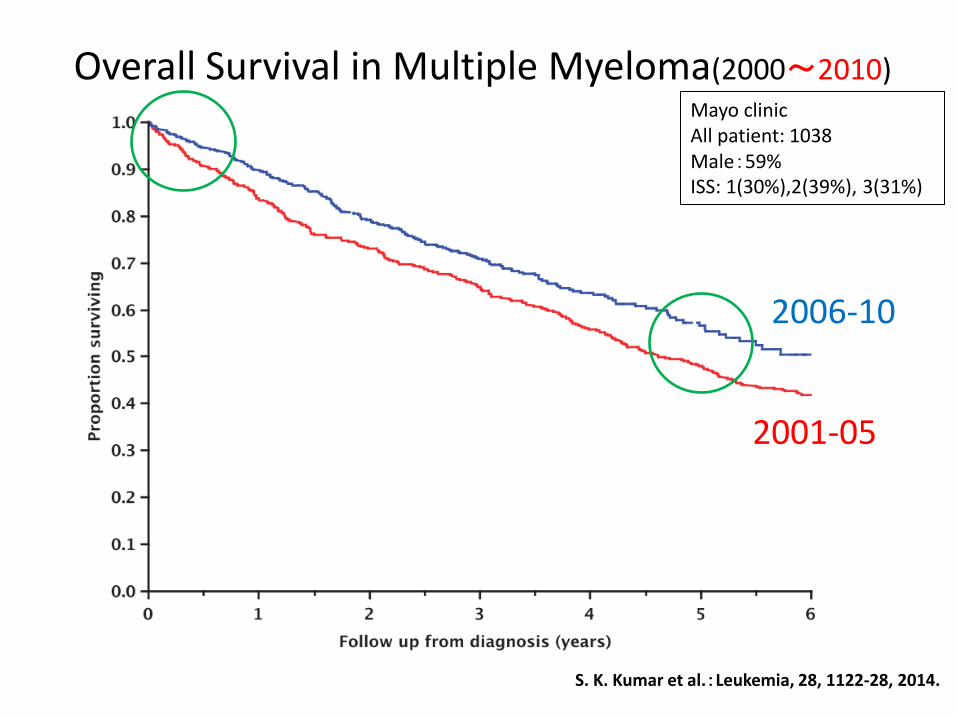
S. K. Kumar et al.:Leukemia, 28, 1122-28, 2014.
2006-10
2001-05
Overall Survival in Multiple Myeloma(2000~2010) Mayo clinic All patient: 1038 Male:59% ISS: 1(30%),2(39%), 3(31%)
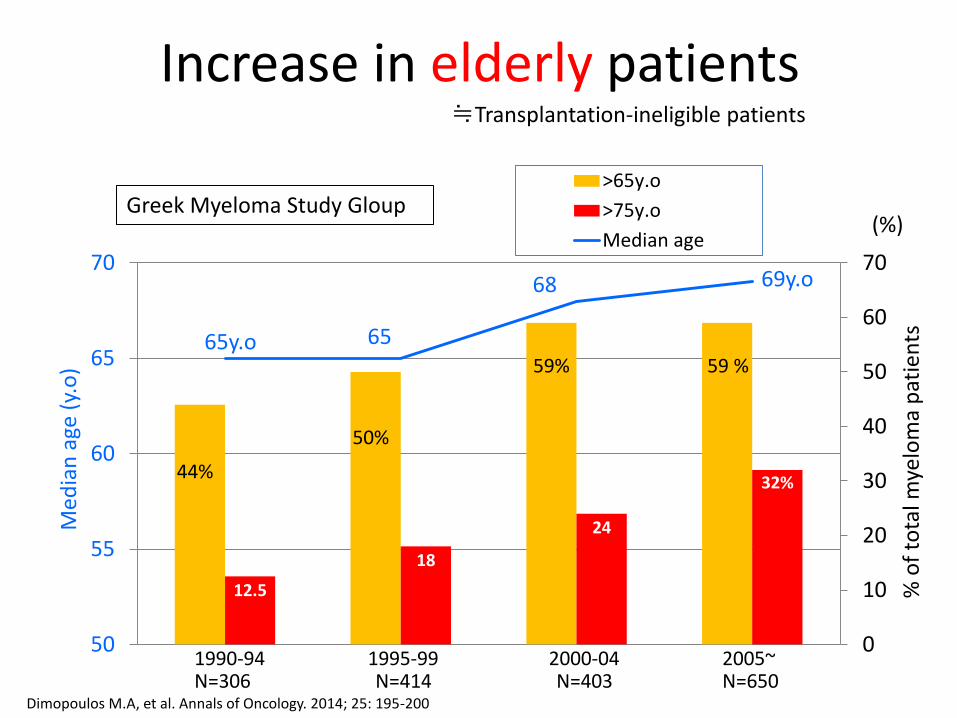
Increase in elderly patients
44%
50%
59% 59 %
12.5
18
24
32%
65y.o 65
68 69y.o
0
10
20
30
40
50
60
70
50
55
60
65
70
>65y.o
>75y.o
Median age(%)
Med
ian
age
(y.
o)
1990-94 1995-99 2000-04 2005~ N=306 N=414 N=403 N=650
Dimopoulos M.A, et al. Annals of Oncology. 2014; 25: 195-200
Greek Myeloma Study Gloup
≒Transplantation-ineligible patients
% o
f to
tal m
yelo
ma
pat
ien
ts
a variety of problems in elderly patients and chronicity
■Comorbidities in multiple organs
• Metabolic syndrome (HT, DM, Obesity, Dyslipidemia) • Cardiovascular events(AMI, angina, CHF, stroke , etc) • Dementia / ADL ↓ • Chronic Kidney Disease (CKD) ■sequela after hematological response ■drug: difficulty dose adjustment (cancer drug, antibiotic) ■diet: salt restriction (sometimes adverse result??)
■Background : personal and social
• Increase in elderly single population • Increase in patients living in remote areas • Demand of Homecare medicine (national project)
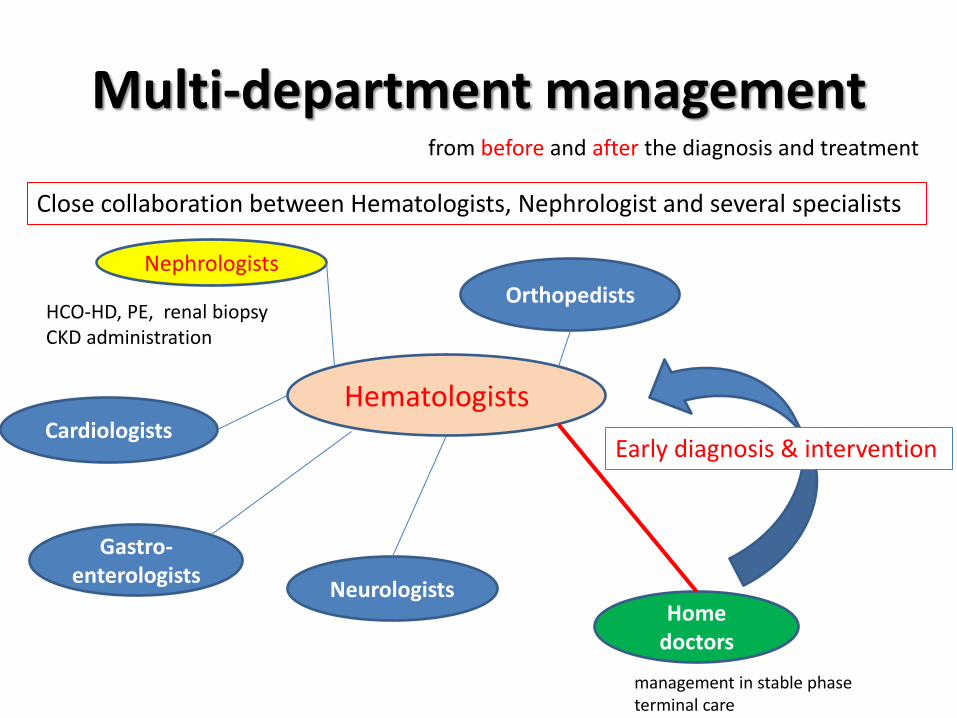
Multi-department management from before and after the diagnosis and treatment
Close collaboration between Hematologists, Nephrologist and several specialists
Early diagnosis & intervention
HCO-HD, PE, renal biopsy CKD administration
Nephrologists
Home doctors
Cardiologists
Neurologists
Orthopedists
Hematologists
Gastro-enterologists
management in stable phase terminal care
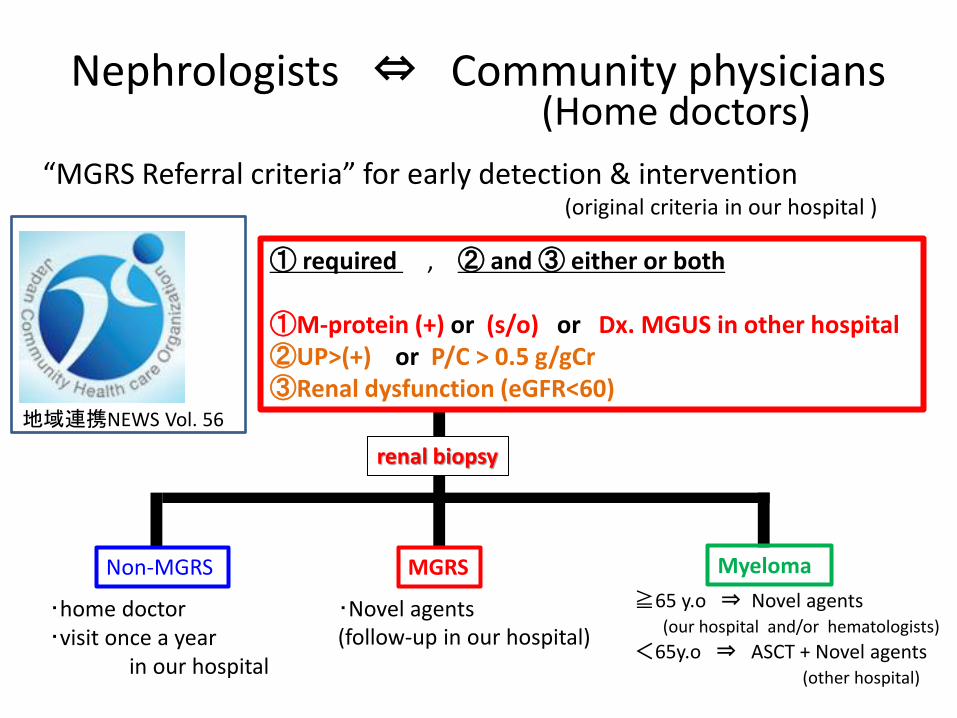
Nephrologists ⇔ Community physicians
“MGRS Referral criteria” for early detection & intervention
(original criteria in our hospital )
① required , ② and ③ either or both ①M-protein (+) or (s/o) or Dx. MGUS in other hospital ②UP>(+) or P/C > 0.5 g/gCr ③Renal dysfunction (eGFR<60)
地域連携NEWS Vol. 56
(Home doctors)
renal biopsy
Non-MGRS
・home doctor ・visit once a year in our hospital
MGRS
・Novel agents (follow-up in our hospital)
Myeloma
≧65 y.o ⇒ Novel agents (our hospital and/or hematologists) <65y.o ⇒ ASCT + Novel agents (other hospital)
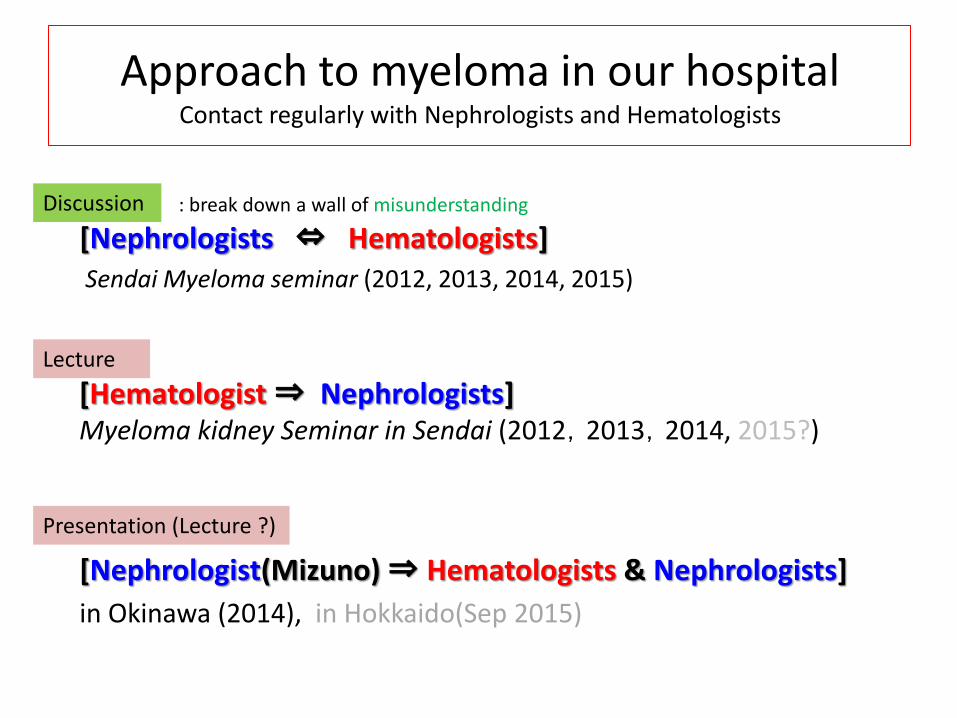
Approach to myeloma in our hospital Contact regularly with Nephrologists and Hematologists
[Nephrologists ⇔ Hematologists] Sendai Myeloma seminar (2012, 2013, 2014, 2015)
[Nephrologist(Mizuno) ⇒ Hematologists & Nephrologists]
in Okinawa (2014), in Hokkaido(Sep 2015)
[Hematologist ⇒ Nephrologists] Myeloma kidney Seminar in Sendai (2012,2013,2014, 2015?)
Discussion
Lecture
Presentation (Lecture ?)
: break down a wall of misunderstanding
Thank you for your kind attention