Physiology of Plasma Proteins
21
Blood Plasma Blood Plasma Anti-coagulated Anti-coagulated blood is blood is Centrifuged: Centrifuged: • clear plasma at top clear plasma at top (55%) (55%) • Plasma : 92% water Plasma : 92% water 7% 7% proteins proteins 1% 1% solutes solutes Plasma - 92% water 7% proteins 1% solutes
-
Upload
drakgupta6924 -
Category
Documents
-
view
1.109 -
download
8
description
For first year MBBS students
Transcript of Physiology of Plasma Proteins

Blood PlasmaBlood PlasmaAnti-coagulated blood Anti-coagulated blood is Centrifuged:is Centrifuged:•clear plasma at top clear plasma at top (55%)(55%)•Plasma : 92% waterPlasma : 92% water 7% proteins7% proteins 1% solutes1% solutes
Plasma -92% water7% proteins1% solutes

Separation of Plasma ProteinsSeparation of Plasma ProteinsHundreds of different proteins are present in Hundreds of different proteins are present in plasma.plasma.
The Most Important Plasma Proteins are :The Most Important Plasma Proteins are : Albumin – 60% Globulins – 35% Clotting proteins – 4% Enzymes– 1%
Normal A/G Ratio Normal A/G Ratio - - 1.7:11.7:1
ElectrophoresisElectrophoresis: separates plasma proteins into 5 : separates plasma proteins into 5 bands: Albumin, alpha 1globulin, alpha 2 globulin, Beta bands: Albumin, alpha 1globulin, alpha 2 globulin, Beta globulin and gamma globulin. globulin and gamma globulin.
Ultracentrifugation Method- Ultracentrifugation Method- Different plasma proteins Different plasma proteins have diff densities is the basis of this technique. This also have diff densities is the basis of this technique. This also determines molecular weight of plasma proteins: determines molecular weight of plasma proteins: Albumin- 69,000, Globulin-1,56,000, Fibrinogen-4,00,000Albumin- 69,000, Globulin-1,56,000, Fibrinogen-4,00,000

Protein Normal value
Examples
Albumin 55.8-60% Prealbumin, Albumin
Alpha 1 2.2 -4.6% α1-Antitrypsin, Thyroxin Binding Globulin etc
Alpha 2 8.2-12.5% Haptoglobulin, Ceruloplasmin, α2- macroglobulin
Beta (1+2)
7.2-14.5% Transferin, Low density lipoprotein, Complement.
Gamma 11.5-18.5% IgG, IgA. IgM, IgD, IgE

Characteristics of Plasma Characteristics of Plasma ProteinsProteins
Most of plasma proteins are synthesized in the Liver cells & move into blood
The exception is of the Immunoglobulins which are synthesized by B Lymphocytes and some complement proteins which are synthesized by macrophages.
Plasma Proteins > 60,000 m.wt .are not filtered and excreted while those < 60,000 m.wt. pass through glomerulus into urine

AlbuminAlbumin Normal plasma level: 3.5 - 5.0 g/dl, Molecular Wt.= 65,000 Half Life of plasma clearance-19 days, Acts as a binding protein for
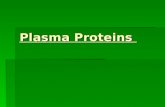
many substances in plasma. CappilaryHydrostatic PressureHydrostatic Pressure exerted by extracellular fluid exerted by extracellular fluid
present inside cappilaries on cappilary wall cause leakage of present inside cappilaries on cappilary wall cause leakage of fluid out of cappilaries at arteriolar end. The fluid leaked out is fluid out of cappilaries at arteriolar end. The fluid leaked out is reabsorbed due to the Oncotic Pressure in cappilaries created reabsorbed due to the Oncotic Pressure in cappilaries created by Albumin.by Albumin.
Colloid(Oncotic)osmotic pressure Colloid(Oncotic)osmotic pressure created by albumin in created by albumin in the bloo capillaries as they are not permeable to albumin& it the bloo capillaries as they are not permeable to albumin& it pulls tissue fluid back into capillaries. This is important to pulls tissue fluid back into capillaries. This is important to maintain normal blood volume and blood pressure.maintain normal blood volume and blood pressure.
Starling Hypothesis –Starling Hypothesis –Net Filtration through capillary Net Filtration through capillary membrane is proportional to the hydrostatic pressure membrane is proportional to the hydrostatic pressure difference across the membrane (Pc-Pi) minus the difference across the membrane (Pc-Pi) minus the oncotic pressure difference (Pic-Pii),oncotic pressure difference (Pic-Pii),where Pc &Pi are where Pc &Pi are hydrostatic pressures in cappilary wall & interstitial fluid hydrostatic pressures in cappilary wall & interstitial fluid respectively and Pic & Pii are Oncotic Pressures inside respectively and Pic & Pii are Oncotic Pressures inside cappilaries & tissue fluid respectively.cappilaries & tissue fluid respectively.

Clinical Significance of Albumin Clinical Significance of Albumin Hypoalbuminaemia: Causes
a.. Protein loss- 1. Nephrotic Syndrome: Defect in glomerular
basement membrane leads to proteinuria (albuminuria), hypoalbumnemia, Hyperlipidaemia& generlaized edema
2. Burns: Loss of albumin due to plasma leakage from damaged blood vessels from burnt tissues
b. Decreased synthesis- Liver diseasec. Inadequate dietary intake –Malnutrition Consequence of hypoalbuminaemia:
Swelling of body → oedema

1-Antitrypsin
Role: 1-antitrypsin inhibits Trypsin, Elastase, and Collegenase & other proteolytic Enzymes released during inflammation
Clinical Significance: 1-antitrypsin Deficiency : Hereditary disorder Lack of 1-antitrypsin →→ uninhibited tissue
breakdown during inflammation Causes pulmonary emphysema (decreased area
of gas exchange due to loss of alveoli) in adults and cirrhosis in children.

Thyroxine Binding GlobulinThyroxine Binding GlobulinIt is the major transport protein for thyroid It is the major transport protein for thyroid hormone.hormone.
99.7% of thyroxine is bound to TBG and 99.7% of thyroxine is bound to TBG and only 0.3% is free and active at cellular only 0.3% is free and active at cellular level.level.
Clinical SignificanceClinical Significance: A complete : A complete deficiency in causes Thyrotoxicosis as it deficiency in causes Thyrotoxicosis as it increases level of free thyroxine in blood increases level of free thyroxine in blood and symptoms of Graves’ disease.and symptoms of Graves’ disease.

Haptoglobin It binds with ‘free’ hemoglobin & prevents
loss of hemoglobin in urine as this complex can not pass through renal glomeruli
Haptoglobin + hemoglobin complex is removed from circulation by reticuloendothelial system. In liver components are recycled- Haptoglobin is destroyed
Hemoglobin is broken down to globin and heme and then further to iron and bilirubin
Clinical Significance: Haptoglobin level falls in hemolytic states.

Ceruloplasmin Cu transport protein, Clinical Significance: Wilson’s Disease: an
autosomal recessive disorder. (a) Cu is deposited in the liver due to reduced biliary excretion- result- Liver enlargement, jaundice, Liver failure(b) Deficiency of ceruloplasmin results in deposition of Cu in
tissues and low plasma copper concentrations- CNS dysfunction, arthritis, Kaysher Fleischer Ring Around cornea in eyes.
(c) Cu filtered through glomeruli urinary copper excretion Treatment: D-penicillamine -a copper-chelating agent → reduce tissue
copper concentrations

Alpha -2 MacroglobulinAlpha -2 Macroglobulin
A major plasma proteinase A major plasma proteinase inhibitor.inhibitor.
Clinical Significance- Its level is Clinical Significance- Its level is increased in increased in Nephrotic Syndrome Nephrotic Syndrome

TransferinTransferin An Iron transport protein. Free iron is toxic so all iron is protein-bound:
transferrin, ferritin, haemosiderin, hemoglobin Only 0.1% of total body iron circulates in plasma:
as Fe3+ bound to transferrin Clinical significance of transferin:
in iron deficiency in iron overload in nephrotic syndrome because low mwt
transferrin is lost in urine.

LipoproteinsLipoproteinsLow Density Lipoproteins (LDL)Low Density Lipoproteins (LDL) transports transports cholesterol from the from the liver to the tissues of the to the tissues of the body. LDL cholesterol is therefore considered the body. LDL cholesterol is therefore considered the "bad" cholesterol as high levels of LDL cholesterol "bad" cholesterol as high levels of LDL cholesterol is associated with high risk of is associated with high risk of cardiovascular disease
High-density lipoproteinHigh-density lipoprotein ( (HDLHDL) removes ) removes cholesterol from cholesterol from atheroma within within arteries and and transport it back to the liver for excretion or re-transport it back to the liver for excretion or re-utilization—so HDL is called utilization—so HDL is called good cholesterol“good cholesterol“. .
A high level of HDL protect against A high level of HDL protect against cardiovascular diseases, and low HDL cholesterol , and low HDL cholesterol levels (less than 40 mg/dL) increase the risk for levels (less than 40 mg/dL) increase the risk for heart diseaseheart disease

Complement SystemComplement SystemThe complement system consists of a number of small The complement system consists of a number of small proteins found in the circulating blood .proteins found in the circulating blood .
Over 20 proteins and protein fragments make up the Over 20 proteins and protein fragments make up the complement system,.complement system,.
The following are the basic functions of the complementThe following are the basic functions of the complement1. 1. Lysis of cells, bacteria and virusesLysis of cells, bacteria and viruses..2. 2. Opsonization for phagocytosis of foreign antigens. for phagocytosis of foreign antigens.3. 3. Immune Clearance, which removes immune complexes , which removes immune complexes from immune system.from immune system.
Clinical SignificanceClinical Significance: Deficiency in complement system : Deficiency in complement system plasma proteins- AutoImuune Disorers, Infectionsplasma proteins- AutoImuune Disorers, Infections

Acute Phase Reactant –C Acute Phase Reactant –C Reactive ProteinsReactive Proteins
C-Reactive Proteins (CRP): The C-Reactive Proteins (CRP): The proteins react with the C-proteins react with the C-polysaccahrides of pneumoccocci polysaccahrides of pneumoccocci thus its name thus its name
Plasma concentration of CRP rises Plasma concentration of CRP rises rapidly in response to acute rapidly in response to acute inflammation & bacterial infections. It inflammation & bacterial infections. It is normal in Viral infections.is normal in Viral infections.

Fibrinogen
It is an acute phase reactant Most abundant of the coagulation factors Forms the fibrin clot Helps in platelet aggregation

Proteins of immune systemProteins of immune system Immunoglobulins
Synthesized by B lymphocytes, Differentiation of B lymphocytes plasma cells
secreting immunoglobulins Two Identical Heavy Chains 2 Idenical Light -Chains linked by dilsuphide bonds 5 Types
IgG IgM IgA IgE IgD

Plasma immunoglobulinsPlasma immunoglobulinsIgG Major (75%), crosses placenta, complement fixation
IgM First line of defence; produced in acute stage of infection , largest Immunoglobulin, Fix complementcan be synthesized by fetus
IgA Present in secretions like saliva, tears, sweat, & colostrum, tears., Prevents attachment of bacteria & viruses to mucus membranes
IgD Found surface of many B Lymphocytes, role is uncertain
IgE Allergic response, Lysis of Worms
Raised in: eczema, Hay fever, Asthma, Anaphylactic shock

Immunoglobulin deficienciesImmunoglobulin deficiencies
IgM deficiency – predisposes to septicaemia
IgG deficiency – recurrent pyogenic infections of tissues (lung, skin) by toxin-producing organisms, e.g. staphylocci, streptococci
IgE – symptomless or recurrent, mild respiratory tract infections

MULTIPLEMYELOMAMULTIPLEMYELOMAMultiple myeloma is a cancer of plasma cells Multiple myeloma is a cancer of plasma cells that that produce produce monoclonal immunoglobulin (Protein M) monoclonal immunoglobulin (Protein M) and invade and destroy adjacent bone tissue. and invade and destroy adjacent bone tissue.

Oncotic & hydrostatic pressures