
Pharmacokinetics and Pharmacodynamics of in Cystic …aac.asm.org/content/30/2/260.full.pdf · The...
7
ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, Aug. 1986, p. 260-266 0066-4804/86/080260-07$02.00/0 Copyright © 1986, American Society for Microbiology Vol. 30, No. 2 Pharmacokinetics and Pharmacodynamics of Ciprofloxacin in Cystic Fibrosis Patients MARC LEBEL,l 2* MICHEL G. BERGERON,' FRAN1;OIS VALLtE,' CELINE FISET 1,2 GIStLE CHASSt,' PIERRE BIGONESSE,3 AND GEORGES RIVARD3 Service d'Infectiologiel* and Departement de Pe'diatrie,3 Le Centre Hospitalier de l'Universite Laval, Quebec, Quebec GI V 4G2, and Ecole de Pharmacie, Universite Laval, Quebec, Quebec GIK 7P4,2 Canada Received 20 December 1985/Accepted 29 May 1986 The pharmacokinetics and blister fluid penetration of oral ciprofloxacin were compared in 11 cystic fibrosis (CF) patients who had sputum colonization but were asymptomatic and in 12 healthy volunteers after a single dose (500 mg) and at steady state (500 mg every 8 h). The antibacterial effect of ciprofloxacin therapy was also evaluated by bacterial counts of colonizing pathogens in the respiratory secretions of CF patients. The CF patients were 15.9% lighter in weight than the controls (P < 0.05). After a single dose, the elimination half-life of ciprofloxacin was decreased by a third in the CF patients as compared with the controls (2.62 versus 3.93 h, respectively; P < 0.01). This was the result of a diminished apparent volume of distribution in CF subjects. Interestingly, we observed no statistically significant difference in total apparent and renal clearances between the groups. Suction-induced blister fluid penetration was not different between CF patients and healthy volunteers. In CF patients, ciprofloxacin exhibited levels in respiratory secretions above the reported MIC for Pseudomonas aeruginosa: 1.36 and 1.86 ,ug/ml at 2 h after a single dose and at steady state, respectively. An important fall (mean, 3.9 loglo/ml) in the log titer in 10 patients with P. aeruginosa in their respiratory secretions was observed after 5 days of treatment. However, this improvement was short-lived; the secondary increase in bacterial counts observed in five patients and the development of five resistant strains were causes for concern. The pharmacokinetic results presented here showed that ciprofloxacin should be administered every 8 or even every 6 h in CF patients. Among the quinolones presently under investigation, ciprofloxacin has shown superior in vitro activity, especially against Pseudomonas aeruginosa (3, 22). This microorgan- ism, especially the mucoid strains, is extremely difficult to eliminate from the respiratory secretions of cystic fibrosis (CF) patients who are chronically colonized (19). Ciprofloxacin, which can be administered orally, may be- come a useful drug for the treatment of this infection. In fact, several clinical trials are presently being done to study the clinical efficacy of ciprofloxacin in the treatment of acute pulmonary exacerbations in patients with CF (S. W. Bender, H.-G. Posselt, R. Wonne, B. Stover, R. Strehl, and P. M. Shah, Ninth International Cystic Fibrosis Congress, Brighton, United Kingdom, June 1984; M. E. Hodson, M. J. Smith, and J. C. Batten, Proc. 14th Int. Congr. Chemother., p. 200, 1985). The pharmacokinetics of several antibiotics have been shown to be disturbed in CF patients. Increased clearance and altered volume of distribution for aminoglycosides and beta-lactam antibiotics have been described in patients with CF as compared with normal subjects or non-CF children (11, 12, 15, 25; L. Cliche, M. LeBel, and M. G. Bergeron, Can. J. Hosp. Pharm., in press). Conflicting results have been reported on impaired oral absorption of drugs in this population (6, 10, 17, 21). The purposes of this study were (i) to compare the single-dose and steady-state pharmacokinetics of ciprofloxacin in CF patients and in healthy volunteers (con- trols) and (ii) to determine the effect of ciprofloxacin therapy on bacterial counts (with special reference to P. aeruginosa) in the respiratory secretions of CF patients. * Corresponding author. MATERIALS AND METHODS Subjects. A total of 11 CF patients (7 males and 4 females; ages 19 to 25 years) and 12 healthy volunteers (6 males and 6 females; ages 19 to 25 years) gave their informed consent to participate in the study. Subject characteristics are de- scribed in Table 1. The protocol was approved by the Centre Hospitalier de l'Universitd Laval Human Research Review and Pharmacology-Therapeutics committees. The diagnosis of CF was based on a compatible family and clinical history, abnormal sweat test, and pancreatic insufficiency or chronic pulmonary disease. All patients met these criteria. All pa- tients except no. 11 had a good to excellent clinical evalua- tion score by the rating system of Shwachman and Kulczycki (23). All subjects were judged to be otherwise healthy on the basis of a history, physical examination, chemistry profile, complete blood count, and urinalysis. Volunteers were determined to be not pregnant after direct latex agglutination pregnancy tests. The patients were stud- ied during an infection-free period; they had stopped all prophylactic antimicrobial therapy (oral and inhalation) 5 days prior to the study. The CF patients were kept on pancreatic enzymes, multivitamins, and any other medica- tions required by their disease (Table 1). The subjects had to restrain from any strenuous or athletic activity during the study period but were allowed to circulate around the clinical pharmacokinetic research unit. Alcoholic beverages and caffeine were withheld 24 h prior to the study and on day 1, 6, or 9. Study design. On the morning of day 1 and following an overnight fast, each subject received a single 500-mg oral dose of ciprofloxacin (Miles Laboratories, Rexdale, Ontario, Canada) taken with 200 ml of drinking water. Starting on the morning of day 2 and continuing through day 5 for healthy 260 on June 3, 2018 by guest http://aac.asm.org/ Downloaded from
Transcript of Pharmacokinetics and Pharmacodynamics of in Cystic …aac.asm.org/content/30/2/260.full.pdf · The...
ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, Aug. 1986, p. 260-2660066-4804/86/080260-07$02.00/0Copyright © 1986, American Society for Microbiology
Vol. 30, No. 2
Pharmacokinetics and Pharmacodynamics of Ciprofloxacin inCystic Fibrosis Patients
MARC LEBEL,l 2* MICHEL G. BERGERON,' FRAN1;OIS VALLtE,' CELINE FISET 1,2 GIStLE CHASSt,'PIERRE BIGONESSE,3 AND GEORGES RIVARD3
Service d'Infectiologiel* and Departement de Pe'diatrie,3 Le Centre Hospitalier de l'Universite Laval, Quebec,Quebec GIV 4G2, and Ecole de Pharmacie, Universite Laval, Quebec, Quebec GIK 7P4,2 Canada
Received 20 December 1985/Accepted 29 May 1986
The pharmacokinetics and blister fluid penetration of oral ciprofloxacin were compared in 11 cystic fibrosis(CF) patients who had sputum colonization but were asymptomatic and in 12 healthy volunteers after a singledose (500 mg) and at steady state (500 mg every 8 h). The antibacterial effect of ciprofloxacin therapy was alsoevaluated by bacterial counts of colonizing pathogens in the respiratory secretions of CF patients. The CFpatients were 15.9% lighter in weight than the controls (P < 0.05). After a single dose, the elimination half-lifeof ciprofloxacin was decreased by a third in the CF patients as compared with the controls (2.62 versus 3.93h, respectively; P < 0.01). This was the result of a diminished apparent volume of distribution in CF subjects.Interestingly, we observed no statistically significant difference in total apparent and renal clearances betweenthe groups. Suction-induced blister fluid penetration was not different between CF patients and healthyvolunteers. In CF patients, ciprofloxacin exhibited levels in respiratory secretions above the reported MIC forPseudomonas aeruginosa: 1.36 and 1.86 ,ug/ml at 2 h after a single dose and at steady state, respectively. Animportant fall (mean, 3.9 loglo/ml) in the log titer in 10 patients with P. aeruginosa in their respiratorysecretions was observed after 5 days of treatment. However, this improvement was short-lived; the secondaryincrease in bacterial counts observed in five patients and the development of five resistant strains were causesfor concern. The pharmacokinetic results presented here showed that ciprofloxacin should be administeredevery 8 or even every 6 h in CF patients.
Among the quinolones presently under investigation,ciprofloxacin has shown superior in vitro activity, especiallyagainst Pseudomonas aeruginosa (3, 22). This microorgan-ism, especially the mucoid strains, is extremely difficult toeliminate from the respiratory secretions of cystic fibrosis(CF) patients who are chronically colonized (19).Ciprofloxacin, which can be administered orally, may be-come a useful drug for the treatment of this infection. In fact,several clinical trials are presently being done to study theclinical efficacy of ciprofloxacin in the treatment of acutepulmonary exacerbations in patients with CF (S. W. Bender,H.-G. Posselt, R. Wonne, B. Stover, R. Strehl, and P. M.Shah, Ninth International Cystic Fibrosis Congress,Brighton, United Kingdom, June 1984; M. E. Hodson, M. J.Smith, and J. C. Batten, Proc. 14th Int. Congr. Chemother.,p. 200, 1985).The pharmacokinetics of several antibiotics have been
shown to be disturbed in CF patients. Increased clearanceand altered volume of distribution for aminoglycosides andbeta-lactam antibiotics have been described in patients withCF as compared with normal subjects or non-CF children(11, 12, 15, 25; L. Cliche, M. LeBel, and M. G. Bergeron,Can. J. Hosp. Pharm., in press). Conflicting results havebeen reported on impaired oral absorption of drugs in thispopulation (6, 10, 17, 21).The purposes of this study were (i) to compare the
single-dose and steady-state pharmacokinetics ofciprofloxacin in CF patients and in healthy volunteers (con-trols) and (ii) to determine the effect of ciprofloxacin therapyon bacterial counts (with special reference to P. aeruginosa)in the respiratory secretions of CF patients.
* Corresponding author.
MATERIALS AND METHODS
Subjects. A total of 11 CF patients (7 males and 4 females;ages 19 to 25 years) and 12 healthy volunteers (6 males and6 females; ages 19 to 25 years) gave their informed consent toparticipate in the study. Subject characteristics are de-scribed in Table 1. The protocol was approved by the CentreHospitalier de l'Universitd Laval Human Research Reviewand Pharmacology-Therapeutics committees. The diagnosisofCF was based on a compatible family and clinical history,abnormal sweat test, and pancreatic insufficiency or chronicpulmonary disease. All patients met these criteria. All pa-tients except no. 11 had a good to excellent clinical evalua-tion score by the rating system of Shwachman andKulczycki (23). All subjects were judged to be otherwisehealthy on the basis of a history, physical examination,chemistry profile, complete blood count, and urinalysis.Volunteers were determined to be not pregnant after directlatex agglutination pregnancy tests. The patients were stud-ied during an infection-free period; they had stopped allprophylactic antimicrobial therapy (oral and inhalation) 5days prior to the study. The CF patients were kept onpancreatic enzymes, multivitamins, and any other medica-tions required by their disease (Table 1). The subjects had torestrain from any strenuous or athletic activity during thestudy period but were allowed to circulate around theclinical pharmacokinetic research unit. Alcoholic beveragesand caffeine were withheld 24 h prior to the study and on day1, 6, or 9.Study design. On the morning of day 1 and following an
overnight fast, each subject received a single 500-mg oraldose of ciprofloxacin (Miles Laboratories, Rexdale, Ontario,Canada) taken with 200 ml of drinking water. Starting on themorning of day 2 and continuing through day 5 for healthy
260
on June 3, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
PHARMACOKINETICS OF CIPROFLOXACIN IN CF PATIENTS
TABLE 1. Demographic characteristics of subjects
Subject Sexa Age (yr) Ht (cm) Wt (kg) Body surface Lean body Current medications ShwachmanI
area (in) massb (kg) score (%
F 19 156
M 21 174.5
M 25 178
M 21 173F 19 158
F 19 159.5
F 21 161
M 21 170
M 20 170.5
M 20 157.5
M 19 172.5
46.6
65.5
54.4
5244.5
1.43
1.79
1.68
1.621.42
51 1.51
51.3 1.52
45. 1.50
69.1 1.80
35.6
57.9
1.28
1.69
36.7 Pancreatic enzymes,multivitamins, salbutamol(aerosol)
54.0 Pancreatic enzymes,multivitamins, salbutamol(aerosol)
47.9 Pancreatic enzymnes,multivitamins
45.6 Pancreatic enzymes, tolmetin35.9 Pancreatic enzymes,
lactulose, oralcontraceptives
39.4 Salbutamol (aerosol),multivitamins
39.9 Pancreatic enzymes,multivitamins
40.5 Pancreatic enzymes,multivitamins
55.0 Pancreatic enzymes,multivitamins,theophylline, salbutamol(aerosol)
32.6 Pancreatic enzymes,multivitamins, prednisone
49.3 Pancreatic enzymes,multivitamins, theophylline
20.5 + 1.8 166.4 ± 8.0 52.1 ± 9.6 1.57 ± 0.16 43.3 ± 7.5
Healthy volunteers1234S6789101112
F 25 170.0M 21 174.5F 23 155.0F 23 162.0M 19 168.0F 25 166.0M 22 176.7M 22 180.0F 22 176.0M 22 173.0M 19 175.5F 24 178.0
59.867.049.554.469.662.060.075.057.067.562.160.6
1.691.811.461.571.791.691.741.941.701.801.761.76
45.755.337.941.554.647.648.960.345.554.852.347.7
Oral contraceptives
Oral contraceptives
22.3 ± 2.0 164.6 ± 21.4 62.0 ± 7.0 1.73 ± 0.12 49.3 ± 6.4a F, Female; M, male.b Calculated by the following relationships: Lean body mass for men = 1.10 x weight - 128 x (weight2Aheight2); lean body mass for women = 1.07 x weight
- 148 x (weight2/height2).
volunteers or through day 8 for CF patients, a 500-mgciprofloxacin tablet was taken orally in a fasting state every8 h (a total of 12 and 21 doses, respectively). A final 500-mgdose was given on the morning of day 6 for healthy volun-teers and day 9 for CF patients.Serum and urine sampling. Blood samples were drawn via
an intravenous catheter from an antecubital vein accordingto the following sequence: 0, 0.25, 0.5, 0.75, 1, 1.5, 2, 2.5, 3,4, 5, 6, 8, and 10 h after the first single dose (day 1). After thelast dose (day 6 or 9), an additional sample was drawn at 24h. A dilute heparin solution (33 U/ml) was used to maintainthe patency of the needle, and at least 1 to 1.5 ml of bloodwas removed and discarded before the sample was drawn.Blood samples (10 ml for healthy volunteers, 5 ml for CFpatients to minimize blood loss) were collected intoVACUTAINER tubes (Becton Dickinson Vacutainer Sys-
tems, Rutherford, N.J.) with red stoppers and no anticoagu-lant. The serum was allowed to clot at room temperature for20 min and was then centrifuged within 20 min. The serumwas frozen at -80°C until assayed.
Urine was collected immediately before administrationand after the first (single) dose and the last dose at intervalsof 0 to 2, 2 to 4, 4 to 8, and 8 to 24 h after dosing. Aliquotsof each urine sample were stored at -80°C until assayed.
Saliva, blister fluid, and respiratory secretion sampling.Mixed saliva was obtained by having the subjects chew on apiece of paraffin wax (Parafilm; Amnerican Can Co., Green-wich, Conn.). After any food ingestion, the buccal mucosawas rinsed with water. Collection was performed immedi-ately before administration, at 0, 0.5, 1, 3, 5, and 8 h after thefirst dose, and at 0.5, 1, 3, 5, 8, and 24 h after the last dose.Each healthy volunteer had ten skin blisters produced on
CF patients1
2
3
45
7
8
9
10
11
12
65
80
85
6685
77
72
70
85
35
71
Mean ± SD 72 ± 14
Mean ± SD
VOL. 30, 1986 261
on June 3, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

ANTIMICROB. AGENTS CHEMOTHER.
the forearm after both the first and last doses. Only six CFpatients (two females, four males) had skin blisters producedon the forearm after the last dose. Suction-induced skinblisters were produced by the slightly modified method ofHellum et al. (7). In brief, a Plexiglas block with 10 bores(diameter, 8 mm) 'was strapped to the volar area of theforearm after the skin had been swabbed with 70%isopropanol. Controlled suction (-400 mm of Hg) wasapplied until semispherical blisters had been produced (1.5to 2 h). The blister fluid was samnpled by puncture with alow-dead-space syringe (Micro-fine III; Becton Dickinsonand Co., Rutherford, N.J.), and aspiration of 0. 10 to 0.15 mlof fluid was performed on one or two blisters, if needed.Each blister was sampled only once. The harvesting timesequence was 0.5, 1, 2, 2.5, 3, 4, 6, and 8 h after the first dosefor healthy volunteers. After multiple doses, the blisterswere punctured at '2, 3, 4, 6, 8, and 10 h for both groups.Additional sampling was performed in the healthy volunteersat 1 and 24 h after the last dose.
Respiratory secretions were obtained by expectoration inCF patients for ciprofloxacin concentration determinationsat 1, 2, and 4 h after the first and last doses. Respiratorysecretions were also collected for cultures and bacterialcounts before the first dose and 2 h after the doses on days5 and 9. On the last day, four patients had difficulty produc-ing sputum, and in one of these a deep pharyngeal swab(Culturette II; Marion Scientific, Div. Marion Laboratories,Inc., Kansas City, Mo.) had to be used to extract secretionsfrom her throat. Cultures and bacterial counts were repeatedon respiratory secretions obtained 60 days after treatment.
Microbiology and susceptibility testing. Respiratory secre-tions were liquefied with equal volumes of Sputolysin(Calbiochem-Behring, La Jolla, Calif.) and cultured on Mac-Conkey, Mannitol, blood, and chocolate agars. Microorgan-ism identification was performed by standard bacteriological
5.0-
E
z0
c
zwUz0Uz
U
0
crC-0
TABLE 2. Pharmacokinetic parameters after a single dose of 500mg of ciprofloxacin
Mean + SD for:Parametera
CF patients Controls P
AbsorptionCmax (,ug/ml) 2.84 + 0.63 2.26 ± 0.75Tmax (h) 1.55 ± 0.56 1.33 t 0.46Lag time (h) 0.36 ± 0.31 0.34 ± 0.16Ka (h-1) 1.060 t 0.496 2.792 t 1.304 <0.01
EliminationC8 (,g/ml) 0.39 ± 0.18 0.41 ± 0.13tj,2 (h) 2.62 ± 1.04 3.93 t 1.12 <0.01AUCO, (,ug. h/ml) 11.07 ± 3.43 10.00 ± 2.78CLapp (ml/min) 828.0 ± 287.5 908.0 ± 243.6CLR (ml/min) 474.1 ± 159.5 395.6 ± 139.0CLNR app (ml/min) 353.6 ± 190.4 512.4 ± 204.4Vss app (liters/kg) 2.12 ± 0.75 3.76 ± 0.90 <0.001
a Cmax, maximum concentration of drug in serum; T.ax, time to maximumconcentration of drug in serum; Ka, absorption constant; C8, concentration at8 h; t4/2, half-life.
techniques used routinely in our microbiology laboratory.Serial dilutions of liquefied respiratory secretions (from 101to 1010) were used for determinations in triplicate of bacterialcounts of primary pathogens. MIC determinations weredone on a total of 28 P. aeruginosa strains found in respira-tory secretions by the agar dilution procedure described bySteers and colleagues (18, 26). The final inoculum used was5 x 105 CFU/ml. The antibiotic powers were kindly providedby the following pharmaceutical companies: ciprofloxacin(Miles Laboratories), enoxacin (Parke-Davis Canada Inc.,Scarborough, Ontario, Canada), ceftazidime (Glaxo Labora-tories, Toronto, Ontario, Canada), cefsulodin (LaboratoiresAbbott Ltde, Montreal, Quebec, Canada), ticarcillin(Laboratoires Beecham Inc., Pointe-Claire, Quebec, Can-ada), tobramycin (Eli Lilly Canada Inc., Scarborough,Ontario, Canada), and netilmicin (Schering Canada Inc.,Pointe-Claire, Quebec, Canada). Calcium and magnesiumions were not added in the broth we used, since the Mueller-Hinton broth we used met the specifications of the NationalCommittee for Clinical Laboratory Standards (18).Sample analysis. Serum, urine, saliva, and blister fluid
E
0)
z
0
1.1zw
9z
0
U-0a.
TIME ( H)FIG. 1. Mean concentrations of oral ciprofloxacin in serum after
a single 500-mg dose. Symbols: 0, CF patients; *, healthyvolunteers.
TIME (H)
FIG. 2. Mean concentrations of oral ciprofloxacin in serum atsteady state. Symbols: 0, CF patients; *, healthy volunteers.
262 LEBEL ET AL.
on June 3, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

PHARMACOKINETICS OF CIPROFLOXACIN IN CF PATIENTS
TABLE 3. Pharmacokinetic parameters at ciprofloxacinsteady state
Mean + SD for:Parametera p
CF patients Controls
AbsorptionCmax (ig/ml) 3.78 ± 0.97 3.51 ± 1.33"Tmax (h) 1.72 ± 0.44 1.04 ± 0.42 <0.002ka (h-') 0.862 ± 0.662 2.301 ± 0.824 <0.001
EliminationC8 (p.g/ml) 0.82 ± 0.34c 0.82 ± 0.32bt112 (h) 3.90 ± 1.71 4.87 ± 1.30dAUCO, (,ug- h/ml) 14.61 ± 3.85c 13.93 ± 5.32dCLapp (ml/min) 601.3 ± 133.1b 690.6 ± 297.0dCLR (ml/min) 319.1 ± 156.9b 358.4 ± 135.8CLNR app (ml/min) 283.0 ± 124.74 316.6 ± 246.9dVss app (liters/kg) 2.29 ± 0.98 3.71 ± 0.96 <0.008a See Table 2, footnote a, for definitions.b p < 0.01 (paired t test; single dose versus steady state).c P < 0.001 (paired t test; single dose versus steady state).d p < 0.05 (paired t test; single dose versus steady state).
samples were analyzed for total ciprofloxacin by a reverse-phase, ion-pairing, high pressure liquid chromatographyprocedure we developed (26a). In brief, separation ofciprofloxacin and nalidixic acid (internal standard) wasachieved by using UV absorption at 313 nm and a C18Nova-Pak column (Waters Associates, Inc., Milford,Mass.). The mobile phase consisted of 35% phosphatebuffer, 65% methanol, and 5.5 mM hexadecyltrime thylam-monium (HDTA) and was adjusted to pH 7.4. Serum samplepreparation involved protein precipitation with acetonitrile(1:2), followed by methylene chloride-2-propanol (90:10)extraction. The sensitivity limit of the assay was 0.06 ,ug ofserum and blister fluid per ml. The coefficient of variationfrom day to day was <5.3%, and the serum and urinerecoveries were 55 and 108%, respectively. Linear regres-sion analysis of the standard calibration lines yielded acorrelation coefficient of >0.999, indicating excellent linear-ity of the assay between 0.125 and 10.0 ,ug/ml. Whencompared with a microbiological assay of serum, the corre-lation coefficient was 0.922 (n = 58).
Pharmacokinetic analysis. Pharmacokinetic analysis wasperformed by using model-independent methods. The elim-ination rate constant (kel) was calculated from the terminalexponential phase of semilogarithmic plots (4).The area under the serum concentration-time curve
(AUC) from time zero to time t (AUC,},) was calculated withconventional linear trapezoidal and extrapolation methods.The apparent serum clearance (CLapp) of ciprofloxacin wasestimated from the model-independent pharmacokineticsequation CLapp = dose/AUC> ,, where 0-t is 0 to infinityafter a single dose and 0 to T after the last dose (here, T = 8h). Although we previously used an absolute bioavailabilityvalue (f) of 70% to better estimate total clearance (14), wecould not assume identical bioavailability in healthy volun-teers and CF patients.The renal clearance (CLR) of ciprofloxacin was calculated
from the relationship CLR = Ae(ti -- t2)/AUC(t1 -* t2), whereAe is the amount of ciprofloxacin found unchanged in urinefrom time t1 to time t2. The apparent nonrenal clearance(CLNR app) was estimated from substraction of CLR from theapparent total clearance. The apparent volume of distribu-tion (Vapp) after a single dose was calculated from therelationship Vapp = (dose [area under the first moment
of the concentration-time curve {AUMC}/AUC2]) -(dose ka[AUC]) (20). The Vapp at steady state (Vss app) wasdetermined by the equation, derived from the work of Smithand Schentag (24), V,s app = (dose[AUMC/AUC2]) -(dose/ka [AUC]), where AUC = AUCSS o and AUMC =AUMCSS o - (AUCss t_/ka) + TAUCss (David Nix,personal communication).We did not calculate separately the pharmacokinetic pa-
rameters for men and women because of data from Hoffier etal., who showed that the disposition of ciprofloxacin isindependent of sex (9).
Statistical analysis. Comparisons of pharmacokinetic databetween both groups were made with a one-way analysis ofvariance. The paired t test was used to determine thestatistical significance between single-dose and steady-statedata. A P value of <0.05 was considered statistically signif-icant.
RESULTSStudy groups. The demographic characteristics of both
controls and CF patients are shown in Table 1. On themorning of day 1, patient 6 chose not to participate in thestudy; we were unable to replace her. Although an attemptwas made to select healthy volunteers with less-than-idealbody weight to match underweight CF patients, CF patientswere 15.9% lighter in weight than controls (P < 0.05).
Pharmacokinetics. Mean levels of ciprofloxacin in serumfollowing the first (single) dose in CF patients and controlsare shown in Fig. 1, and the corresponding pharmacokineticdata are shown in Table 2. Mean peak ciprofloxacin concen-trations in serum were slightly higher in CF patients than incontrols (2.84 + 0.63 versus 2.26 + 0.75 ,ug/ml, respectively)but did not reach the level of statistical significance. Al-though not visually apparent, the absorption phase wasslower in CF patients, as shown by absorption constantvalues of 1.06 + 0.50 versus 2.79 ± 1.30 h-1 in CF andhealthy subjects, respectively.
5.0,
E20)-
z0UJ
zw
0za0
0cc
0-0~
1.0
0 2 4 6 8 10
TIME (H)FIG. 3. Mean concentrations of ciprofloxacin in blister fluid at
steady state. Symbols: 0, CF patients; *, healthy volunteers.
VOL. 30, 1986 263
on June 3, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
ANTIMICROB. AGENTS CHEMOTHER.
The elimination half-life of ciprofloxacin was decreased bya third in CF patients as compared with controls (2.62 ± 1.04versus 3.93 ± 1.12 h, respectively; P < 0.01). This differencein mean half-life values cannot be visually observed in Fig. 1,since representation of mean concentrations in serum vanishthis difference (16). Interestingly, we observed no statisti-cally significant difference in apparent total clearance andbetween CF and healthy subjects. Furthermore, we normal-ized the apparent total clearance to lean body mass for eachsubject (Table 1). Both apparent total clearances were fairlysimilar (945.3 versus 918.5 ml/min per 50 kg of lean bodymass for CF and healthy subjects, respectively). The de-creased half-life was the result of a diminished apparentvolume of distribution (2.12 ± 0.75 versus 3.76 ± 0.90liters/kg in CF patients and healthy volunteers, respectively;P < 0.001).Although not completely comparable, steady-state
ciprofloxacin levels in serum after the last dose for CF andcontrol subjects (doses 22 and 13, respectively) are shown inFig. 2. As anticipated from pharmacokinetic theory, peakconcentrations in serum for both CF and healthy subjectswere higher (3.78 versus 2.84 and 3.51 versus 2.26 ,ug/ml,respectively) after the last dose than after the first dose(Table 3). As observed in healthy volunteers, the apparenttotal clearance of ciprofloxacin in CF patients showed asignificant decrease after multiple doses. In contrast tohealthy volunteers, no increase in half-life could be demon-strated in this patient population when single-dose andsteady-state data were compared.We performed an analysis of covariance with weight, body
surface area, and lean body mass as covariables; thesecovariables were not statistically significant for any of thepharmacokinetic parameters, either for a single dose or forsteady state, except for weight, which was a covariable (P <0.02) for the time to maximum concentration of drug inserum after a single dose.Mean peak concentrations of ciprofloxacin after a single
dose in saliva were higher in controls than in CF patients(1.32 versus 1.01 ,ug/ml, respectively), but the difference wasnot statistically significant. At steady state, these peak levelsin saliva were similar (1.57 jig/ml for normal volunteers and1.51 pug/ml for CF patients). No statistically significantdifference could be observed in peak levels in saliva betweenboth groups. The ratios of the peak concentration in saliva tothe simultaneous concentration in serum yielded remarkablyconstant values, except for controls after a single dose (0.78+ 0.36). The ratio after a single dose in CF patients was 0.49,and those at steady state were 0.55 and 0.53 in CF andhealthy subjects, respectively.
Steady-state blister production was more erratic in CFpatients; fewer blisters were obtained than in controls. Meanlevels of ciprofloxacin in blister fluid for CF patients andcontrols are shown in Fig. 3. The mean peak ciprofloxacin
TABLE 4. MIC90 against 28 P. aeruginosa isolates
MIC90 (,ug/ml) on day:Antibiotic
0 (n = 22) 5 (n = 10) 9 (n = 15) 60 (n =18)
Ciprofloxacin 1 1 4 1Enoxacin 4 2 16 4Ceftazidime 4 4 4 4Cefsulodin 8 4 4 4Ticarcillin 32 32 64 32Tobramycin 16 16 8 8Netilmicin >128 >128 128 64
PATIENT
FIG. 4. P. aeruginosa counts in the 11 CF patients before thefirst dose (0) and on days 5 (5), 9 (9), and 60 (60) after treatment.
concentrations observed after the last dose in CF patientsand controls were similar (1.79 + 0.51 versus 1.87 + 0.66pug/ml, respectively). From the elimination portion of indi-vidual curves, a half-life of 4.40 ± 1.78 h was obtained in CFpatients, a value which was not significantly different fromthe value obtained in controls (3.32 ± 2.40 h).
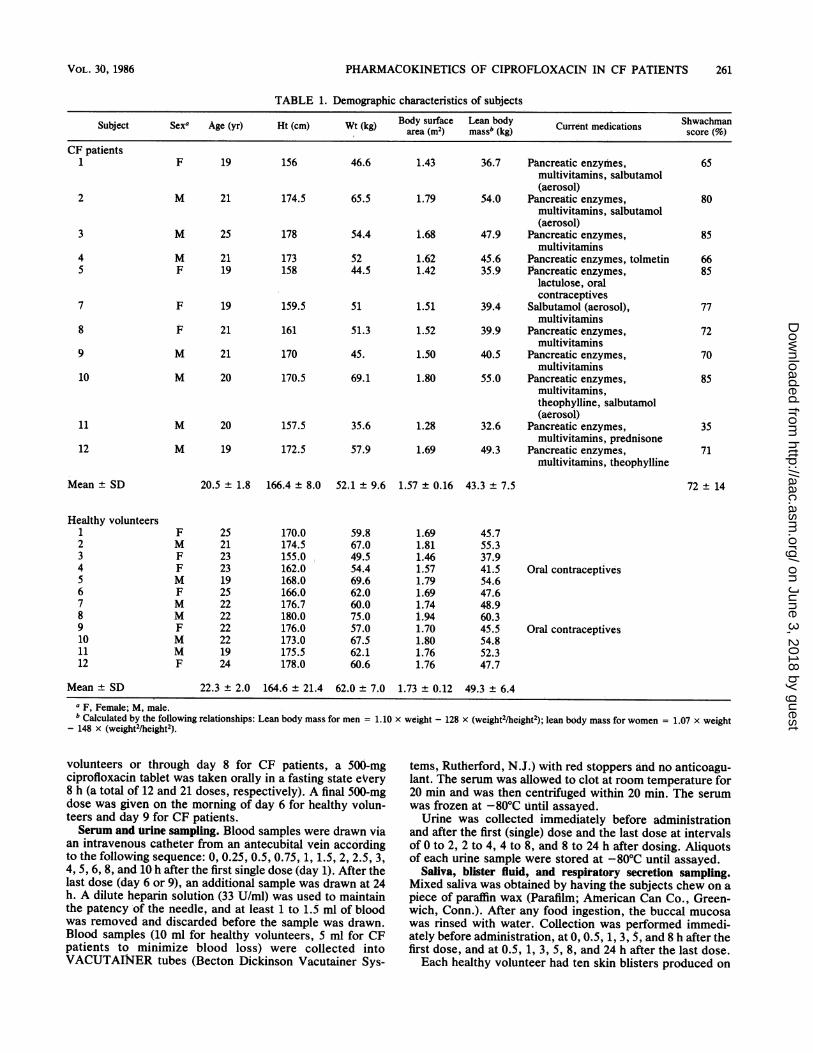
Respiratory secretions. Peak concentrations in respiratorysecretions observed at 2 h were 1.36 and 1.86 ,ug/ml after asingle dose and at steady state, respectively. Before therapy,seven CF patients harbored P. aeruginosa in respiratorysecretions, one had Staphylococcus aureus, two had boththese bacteria, and one had P. maltophilia, P. cepacia, andS. aureus. The MICs of ciprofloxacin and other antibacterialagents for 90% (MIC%0) of a total of 28 P. aeruginosa isolatesare shown in Table 4. Ciprofloxacin had lower MIC90s thanthe other six antibiotics tested. Five ciprofloxacin-resistantstrains (MICgo, >4) of P. aeruginosa appeared in threedifferent patients during therapy. Also of interest was theincreased MIC90 observed with enoxacin (Table 4); ninestrains of P. aeruginosa developed resistance to enoxacin(MIC90, >4) under ciprofloxacin treatment.The bacterial counts ofP. aeruginosa in the 11 CF patients
is shown in Fig. 4. An important fall (mean, 3.9 log1l/ml) inthe log titer in 10 patients with P. aeruginosa in theirrespiratory secretions can be observed after 5 days oftreatment; five patients had increases in bacterial countsfrom days 5 to nine. Five still had lower bacterial counts 60days after treatment; the other six had the same level or ahigher level of colonization by P. aeruginosa than beforetreatment.
Subjective clinical improvement was noted in at least fivepatients; four of them had difficulty in producing respiratorysecretions on the last day and also had a significant decreasein colony counts.
DISCUSSION
Ciprofloxacin is eliminated by a combination of hepaticbiotransformation and renal excretion. Four metabolites ofciprofloxacin in urine are currently known, and their renalexcretion amounts to 13.5% (H. J. Zeiler, U. Peterson, andW. Gau, Program Abstr. 24th Intersci. Conf. Antimicrob.Agents Chemother., abstr. no. 983, 1984). Ciprofloxacinexhibits a large apparent volume of distribution and low
264 LEBEL ET AL.
on June 3, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

PHARMACOKINETICS OF CIPROFLOXACIN IN CF PATIENTS
protein binding (20 to 43%). Renal excretion is the mainelimination pathway, with tubular secretion being somewhatmore important than glomerular filtration (2, 8, 27, 28).
In this study, CF patients had a shorter ciprofloxacinelimination half-life in serum than did controls (2.62 versus3,93 h after a single dose, respectively); this observation isconsistent with other reports of increased drug elimination inpatients with CF (11, 12, 15; F. Sorgel, U. Stephan, H. G.Wiesemann, I. Bruning, H. C. Dominick, and C. Hesseling,Proc. 14th Int. Congr. Chemother. p. 178, 1985). Since theapparent total clearance of ciprofloxacin did not appear to bemodified by CF, this shorter half-life was mainly due to asmaller apparent volume of distribution (2.12 versus 3.76liters/kg; P < 0.001). It has been speculated that the in-creased volume of distribution of hydrosoluble drug in CFpatients is secondary to the reduced adipose tissue in thesepatients (13). The same hypothesis may apply in the oppositeway to explain a decreased volume of distribution ofciprofloxacin, a slightly liposoluble drug. In contrast totheophylline, the protein binding of ciprofloxacin is too lowto significantly affect its apparent volume of distribution inCF patients (10). Moreover, ciprofloxacin concentrations insaliva, grossly representative of the free fraction, were notdifferent between the groups.
Since we initiated this study, the results of four studies onthe pharmacokinetics of ciprofloxacin in CF patients havebeen presented or published (1, 5; J. F. Blumer, R. C. Stern,C. M. Myers, J. D. Klinger, and M. D. Reed, Proc. 14th Int.Congr. Chemother., p. 178, 1985; Sorgel et al., Proc. 14thInt. Congr. Chemother.). They reported a meanciprofloxacin half-life in CF patients of 3.6 to 5.15 h. In thetwo studies comparing CF and healthy subjects, neitherreported accelerated elimination of ciprofloxacin in CF pa-tients (Blumer et al., Proc. 14th Int. Congr. Chemother.;Sorgel et al., Proc. 14th Int. Congr. Chemother.). In fact, adecreased total clearance was observed by Blumer andco-workers (Blumer et al., Proc. 14th Int. Congr. Chemo-ther.). Potential discrepancies between our data and those ofothers are unclear. Differences between our observationsand those of other authors may be the result of the clinicalheterogeneity of CF. Strict adherence to severity scores anddetermination of blood volume, extracellular volume, andtrue lean body mass and surface area might allow directcomparisons between studies. Possible explanations wouldalso include a shorter blood-drawing period, since it hasbeen shown that a longer half-life could be obtained forciprofloxacin if blood levels are followed for longer than 10 h(single dose) (W. Wingender, personal communication).We also found in this study higher peak levels in serum for
CF patients than for controls, although this difference wasnot significant. Sorgel and co-workers made similar obser-vations when they speculated that the decreased bicarbonatesecretion in CF patients, which could influence the ioniza-tion of ciprofloxacin in the gastrointestinal tract, makesciprofloxacin more absorbable (Sorgel et al., Proc. 14th Int.Congr. Chemother.). Surprisingly, high ciprofloxacin con-centrations in serum in CF patients may be the result of acombination of slower and more complete absorption and asmaller apparent volume of distribution than in controls.Blumer and co-workers showed that pancreatic enzymes hadno effect on absorption, distribution, and elimination ofciprofloxacin (Blumer et al., Proc. 14th Int. Congr. Chemo-ther.). According to blister fluid data, the distribution ofciprofloxacin in extracellular fluid did not seem to be affectedin CF patients, as compared with normal volunteers.The pharmacokinetic results presented here showed that
ciprofloxacin should be administered every 8 or even every6 h in CF patients.
Ciprofloxacin induced a significant reduction in counts ofP. aeruginosa, but this improvement was short-lived. Weacknowledge the limitations of quantitative bacteriology inrespiratory secretions obtained by expectoration, but webelieve that this information is valuable in studies of thepharmacodynamic effects of antibacterial agents in clinicalsituations such as sputum colonization of CF patients. Thesecondary increase in bacterial counts observed in fivepatients and the development of five resistant strains arecauses for concern. Others have recently observed bacterialresistance to ciprofloxacin after long-term oral administra-tion (S. T. Chapman, D. C. E. Speller, and D. S. Reeves,Letter, Lancet ii:39, 1985; S. M. Crook, J. B. Selkon, andP. D. McLardy Smith, Letter, Lancet i:1275, 1985; C. M.Roberts, J. Batten, and M. E. Hodson, Letter, Lanceti:1442, 1985). One of these reports concerns CF patients.Caution against the use of ciprofloxacin in this populationshould prevail before clinical and microbiological studiesevaluate the in vivo importance of these observed in vitroresistance patterns.
ACKNOWLEDGMENTS
This study was supported by a grant from Miles Laboratories.We are grateful to Louise Cliche, Daniel Croteau, and the
personnel of the Centre Hospitalier de l'Universite Laval CysticFibrosis Clinic for their collaboration. We also thank Michael Spinofor his helpful comments.
LITERATURE CITED1. Bender, S. W., A. Dalhoff, P. M. Shah, R. Strehl, and H. G.
Possett. 1986. Ciprofloxacin pharmacokinetics in patients withcystic fibrosis. Infection 14:23-27.
2. Davis, R. L., J. R. Koup, J. Williams-Warren, A. Weber, andA. R. Smith. 1985. Pharmacokinetics of three oral formulationsof ciprofloxacin. Antimicrob. Agents Chemother. 28:74-77.
3. Eliopoulos G. M., A. Gardella, and R. C. Moellering, Jr. 1984.In vitro activity of ciprofloxacin, a new carboxyquinoline anti-microbial agent. Antimicrob. Agents Chemother. 25:331-335.
4. Gibaldi, M., and D. Perrier. 1982. Pharmacokinetics, 2nd ed.Marcel Dekker, Inc., New York.
5. Goldfarb, J., G. P. Wormser, M. A. Inchiosa, G. Guideri, M.Diaz, R. Gandhi, C. Goldzman, and A. V. Mascia. 1986. Singledose pharmacokinetic study of oral ciprofloxacin in youngadults with cystic fibrosis. J. Clin. Pharmacol. 26:222-226.
6. Harrison, C. J., M. I. Marks, D. F. Welch, B. B. Sharma, D.Baker, J. Dice, and the Collaborative CF Antibiotic Study Group.1985. A multicenter comparison of related pharmacologic fea-tures of cephalexin and dicloxacillin given for two months toyoung children with cystic fibrosis. Pediatr. Pharmacol. 5:7-16.
7. Hellum, K. B., A. Schreiner, A. Digranes, and I. Bergman. 1978.Skin blisters produced by suction: a new model for studies ofpenetration of antibiotics in humans. p. 620-622. In W.Siegenthaler and R. Luthy (ed.), Current chemotherapy, vol. 1.American Society for Microbiology, Washington, D.C.
8. Hoffken, G., H. Lode, C. Prinzing, K. Borner, and P. Koeppe.1985. Pharmacokinetics of ciprofloxacin after oral and paren-teral administration. Antimicrob. Agents Chemother.27:375-379.
9. Hoffler, D., A. Dalhoff, W. Gau, D. Beermann, and A. Michl.1984. Dose and sex-independent disposition of ciprofloxacin.Eur. J. Clin. Microbiol. 3:363-366.
10. Isles, A., M. Spino, E. Tabachnik, H. Levison, J. J. Thiessen,and S. M. MacLeod. 1983. Theophyline disposition in cysticfibrosis. Am. Rev. Respir. Dis. 127:417-421.
11. Jusko, W. J., L. L. Mosovich, M. S. Gerbracht, M. E. Mattar,and S. J. Yafse. 1975. Enchanced renal excretion of dicloxacillinin patients with cystic fibrosis. Pediatrics 56:1038-1044.
12. Kearns, G. L., B. C. Hilman, and J. T. Wilson. 1982. Dosing
VOL. 30, 1986 265
on June 3, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

ANTIMICROB. AGENTS CHEMOTHER.
implications of altered gentamicin disposition in patients withcystic fibrosis. J. Pediatr. 100:312-318.
13. Larsen, G. L., R. J. Barron, R. A. Landay, E. K. Cottom, M. A.Gonzalez, and J. G. Brooks. 1980. Intravenous aminophylline inpatients with cystic fibrosis. Am. J. Dis. Child. 134:1143-1148.
14. LeBel, M., F. Vallte, and M. G. Bergeron. 1986. Tissue pene-
tration of ciprofloxacin after single and multiple doses. Antimi-crob. Agents Chemother. 29:501-505.
15. Leeder, J. S., M. Spino, A. F. Isles, A. Tesoro, R. Gold, andS. M. MacLeod. 1984. Ceftazidime disposition in acute andstable cystic fibrosis. Clin. Pharmacol. Ther. 36:355-362.
16. Martin, E., W. Moll, P. Schmid, and L. Dettli. 1984. Problemsand pitfalls in estimating average pharmacokinetic parameters.Eur. J. Clin. Pharmacol. 26:595-602.
17. Nahata, M. C., A. H. Lubin, and J. A. Visconti. 1984.Cephalexin pharmacokinetics in patients with cystic fibrosis.Dev. Pharmacol. Ther. 7:221-222.
18. National Committee for Clinical Laboratory Standards. 1983.Tentative standard: methods for dilution antimicrobial suscep-tibility tests for bacteria that grow aerobically. M 7-T. NationalCommittee for Clinical Laboratory Standards, Villanova, Pa.
19. Nelson, J. D. 1985. Management of acute pulmonary exacerba-tions in cystic fibrosis: a critical appraisal. J. Pediatr.106:1030-1034.
20. Perrier, D., and M. Mayersohn. 1982. Noncompartmental de-termination of the steady state volume of distribution for anymode of administration. J. Pharm. Sci. 71:372-373.
21. Reed, M. D., R. C. Stern, J. S. Bertino, C. N. Myers, T. S.Yamashita, and J. L. Blumer. 1984. Dosing implications of rapid
elimination of trimethoprim-sulfamethoxazole in patients withcystic fibrosis. J. Pediatr. 104:303-307.
22. Roy, C., A. Foz, C. Segura, M. Tiraclo, M. Teixeil, and D.Teruel. 1983. Activity of ciprofloxacin (BAY o 9867) againstPseudomonas aeruginosa and ampicillin-resistant Enterobacte-riaceae. Infection 2:326-328.
23. Shwachman, H., and L. L. Kulczycki. 1958. Long-term study of105 patients with cystic fibrosis. Am. J. Dis. Child. 96:6-15.
24. Smith, I. L., and J. J. Schentag. 1984. Noncompartmentaldetermination of the steady-state volume of distribution duringmultiple dosing. J. Pharm. Sci. 73:281-282.
25. Spino, M., R. P. Chai. A. F. Isles, J. J. Thiessen, A. Tesoro, R.Gold, and S. M. MacLeod. 1984. Cloxacillin absorption anddisposition in cystic fibrosis. J. Pediatr. 105:829-835.
26. Steers, E., E. L. Foltz, B. S. Graves, and J. Riden. 1959. Aninocula replicating apparatus for routine testing of bacterialsusceptibility to antibiotics. Antibiot. Chemother. (Basel)9:307-311.
26a.Vallee, F., M. LeBel, and M. G. Bergeron. 1986. Determinationof ciprofloxacin in biological samples by reversed-phase highperformance liquid chromatography. Ther. Drug Monit.8:340-345.
27. Wingender, W., K. H. Graefe, W. Gau, D. Forster, D.Beermann, and P. Schacht. 1984. Pharmacokinetics ofciprofloxacin after oral and intravenous administration inhealthy volunteers. Eur. J. Clin. Microbiol. 3:355-359.
28. Wise, R., R. M. Lockley, M. Webberly, and J. Dent. 1984.Pharmacokinetics of intravenously administered ciprofloxacin.Antimicrob. Agents Chemother. 26:208-210.
266 LEBEL ET AL.
on June 3, 2018 by guesthttp://aac.asm
.org/D
ownloaded from


















