2 Pharmacology Pharmacodynamics
60
Pharmacology pharmacodynamics
-
Upload
laurence-hattersley -
Category
Health & Medicine
-
view
3.454 -
download
0
description
A historical viewpoint of discovery of: - Neurotransmitters via poisons - Receptors for neurotransmitters - Antibiotics
Transcript of 2 Pharmacology Pharmacodynamics

Pharmacology
pharmacodynamics
Pharmacology
• Pharmacology is the science of the action and use of drugs.
• A drug is a substance applied to a living system with the intent of bringing about a change; – this broad definition allows it to include such everyday
substances as coffee and sugar.
• It is underpinned by the basic science of pharmacology, • It is underpinned by the basic science of pharmacology, with added focus on the application of pharmacological principles and methods in the real world.
• It has a broad scope, from the discovery of new target molecules, to the effects of drug usage in whole populations
Pharmacology – a bit of history• Like anatomy and physiology, we tend to
regard all the knowledge we have now of pharmacology as ‘standard’; like it has always been there
• The process of discovery has been a learning curvecurve
• The discovery of some neurotransmitters has its origins in toxins and poisons that are found in nature.
• It begins in France in the 19th century
Pharmacology history
Neurotransmitters– the function of poisons
• Claude Bernard (1813 – 1878) carried out investigations on curare, a deadly plant toxin used by the South American Indians. – They used it on the tips of their darts that they blow
at animals.
• The curare quickly paralyses any animal hit by the • The curare quickly paralyses any animal hit by the dart and then the hunters can collect the beast at their leisure (i.e. not keep running after it until it is incapacitated or dead) for food later.
• Here, the key point is that curare is not absorbed orally, so the poisoned meat can be consumed without danger.

Neurotransmitters
• Bernard worked with the nerves that supply the skeletal system. He found that curare blocked the ability of skeletal muscle to respond to nervous stimulation. – Here, though, the muscles were not paralysed within
themselves and could still be stimulated directly. themselves and could still be stimulated directly.
• Bernard found that both nerves and muscleswould still respond to stimulation individually.
• This observation suggested the existence of a neuromuscular junction between the nerve and the muscle and it was at this site where curare acted.
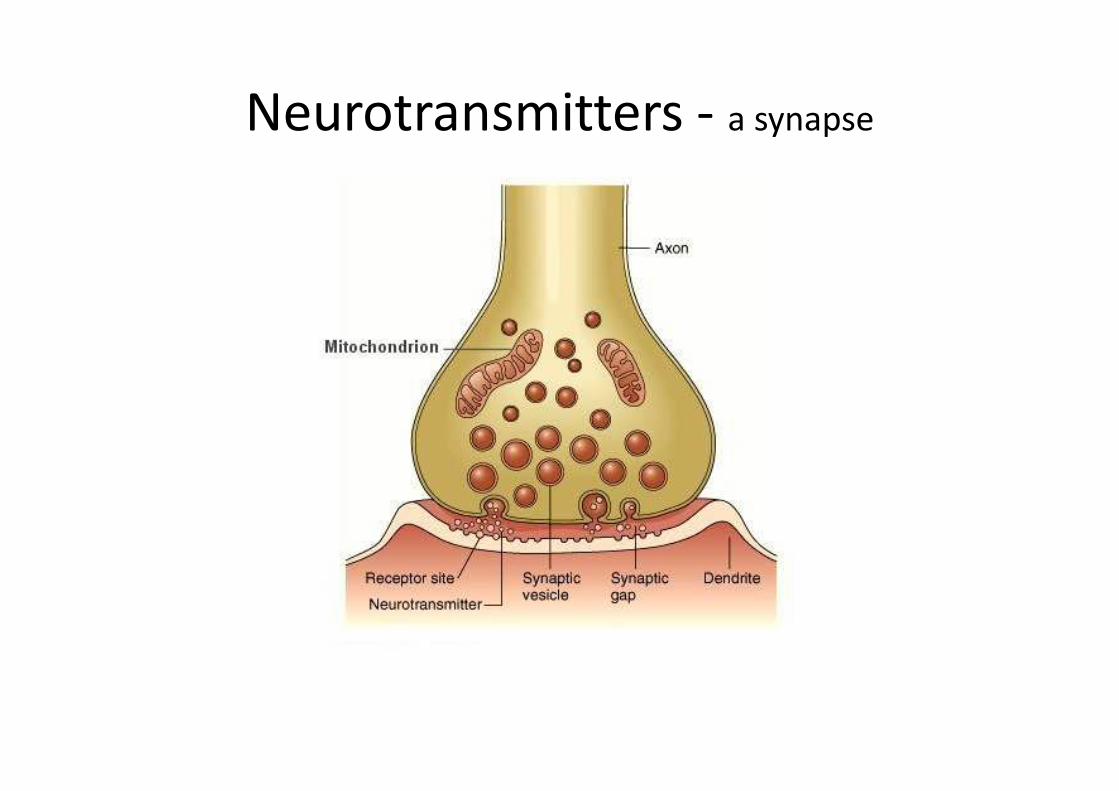
Neurotransmitters - a synapse

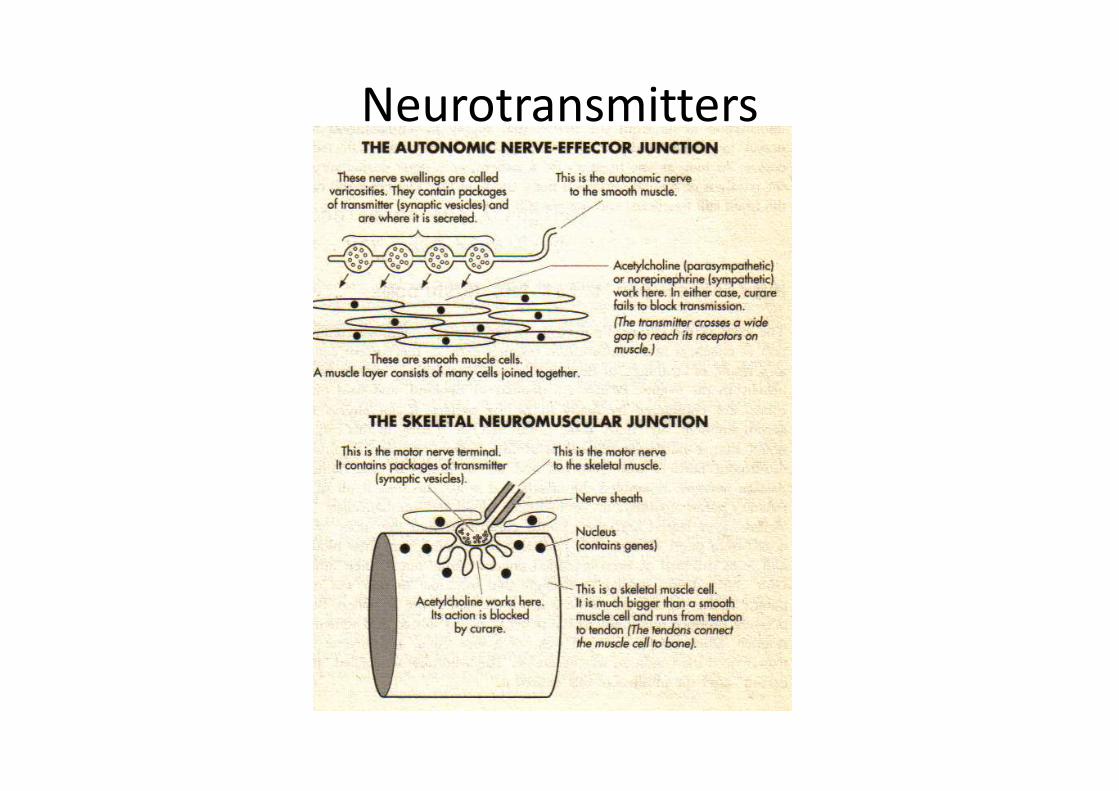
Neurotransmitters
• The equivalent region in the autonomic
nervous system where smooth muscle, or
cardiac muscle, or glands are innervated is
called the neuroeffector junction.
• The neuroeffector junction is unaffected by • The neuroeffector junction is unaffected by
curare, suggesting that there was a different
mechanism of action in the autonomic
neurotransmission than at the neuromuscular
junction
Neurotransmitters

Neurotransmitters• Modern surgery of today also uses curare for similar
reasons – to paralyse muscles. They drip it into veins for this effect
– so the patient needs to be artificially ventilated (as the respiratory muscles are paralysed) but they stay alive because the cardiac muscle is different to skeletal muscle
– Skeletal muscle is known as neurogenic – it must have a nerve supply for it to function and contract. nerve supply for it to function and contract.
– Cardiac muscle is different. It is myogenic, in that it has its own intrinsic rhythm and does not require a nerve supply for it to function
• With curare, as long as the patient can ‘breathe’ (via the ventilator) he will live; the heart still beats, the brains still functions and the gut still moves

Neurotransmitters• Muscarine – don’t eat the mushrooms
• Early in the 20th century, Sir Henry Dale (a
Don at Oxford University) observed that eating
some types of wild mushrooms (sought in the
environs at picnics etc) of the type Amanita
Muscaria produced an effect similar to that if
all the parasympathetic nerves had been
stimulated simultaneously.

Neurotransmitters - Muscarine• On eating Amanita Muscaria
– The victims’ eyes teared and their pupils constricted into little dots.
– Sweat oozed from all their pores
– Saliva drooled from their mouths
– Faeces dribbled or even exploded uncontrollably out of their anuses. their anuses.
– Guts churned and moved so strongly if was often painful and even visible under the skin of the abdomen.
– Blood pressure dropped ominously as the victims’ heart rate slowed and even sometimes, briefly, stopped.
– Survival of this was uncertain, and the condition was called ‘muscarism’ after the mushroom that caused it.

Neurotransmitters - Muscarine• Muscarine , the poison extracted from Amanita
Muscaria, were all found to be identical to those elicited by the parasympathetic neurotransmitter
• However, in contrast to curare, Muscarine isabsorbed on ingestion (hence the symptoms)
• Muscarine does not occur naturally in the body, so it couldn’t be the neurotransmitter itself. so it couldn’t be the neurotransmitter itself.
• Dale found that all of the effectors that would respond to muscarine respond identically to acetylcholine (Ach), which does occur naturally. This suggested to Dale and others that ACh might be the neurotransmitter of parasympathetic nerves

Autonomic nervous system

Scopolamine and Atropine – hot, dry and wide
eyed
• Another set of plants poisons that helped to confirm that ACh is the parasympathetic neurotransmitter
• Responses of effectors to muscarine, acetylcholine, and parasympathetic nerves are all specifically blocked by toxins in an extract of belladonna (atropine) and other plants
• If ACh could cause stimulation of parasympathetic • If ACh could cause stimulation of parasympathetic neuroeffector junctions, it would be called an agonist.
• The chemical that would block this activity would be called an antagonist. With parasympathetic responses, such antagonists were found in toxins like hyoscine (called scopolamine in the USA)

Parasympathetic blocker - atropine• Atropine is used extensively by
ophthalmologists to dilate pupils for eye
exams
• These compounds are toxic because they can
block the actions of acetylcholine
– see this as a compound binding with the receptors
at the neuroeffector junction, but not having a
stimulatory effect.

Parasympathetic blocker - atropine– If atropine occupies the neurotransmitter receptor
sites, without stimulating them, it results in less available sites for stimulation by acetylcholine.
– Victims become
• blind (as their lens’ cannot accommodate),
• hot as Hades (they cannot sweat),
• red as beet (the skin blood vessels dilate),
• mad as a hatter (the drugs enter the brain and have the same effect as in the periphery);
• their mouths dry up (they cannot spit)
• their pupils open wide (hence use by ophthalmologists)
• their hearts race.

Parasympathetic blocker - atropine
• Both hyoscine and atropine thus abolished the effects of parasympathetic nerve stimulation, but leave the effects of sympathetic
stimulation intact.
• From this it seems to Dale that must be the final parasympathetic neurotransmitter and that the sympathetic neurotransmitter Achmust be something else. Dale won the Nobel Prize for his discoveries

Parasympathetic blocker• He introduced new adjectives to describe these
receptors– the effectors to acetylcholine that mimic
parasympathetic nerve stimulation are called muscarinic
– the receptors upon hyoscine and atropine, which blocks the activity of acetylcholine, are called blocks the activity of acetylcholine, are called muscarinic antagonists.
– They were called this, not just in memory of the toxins producing their effects, but that the actions of acetylcholine were not all muscarinic and names had to be invented to distinguish between different effects.
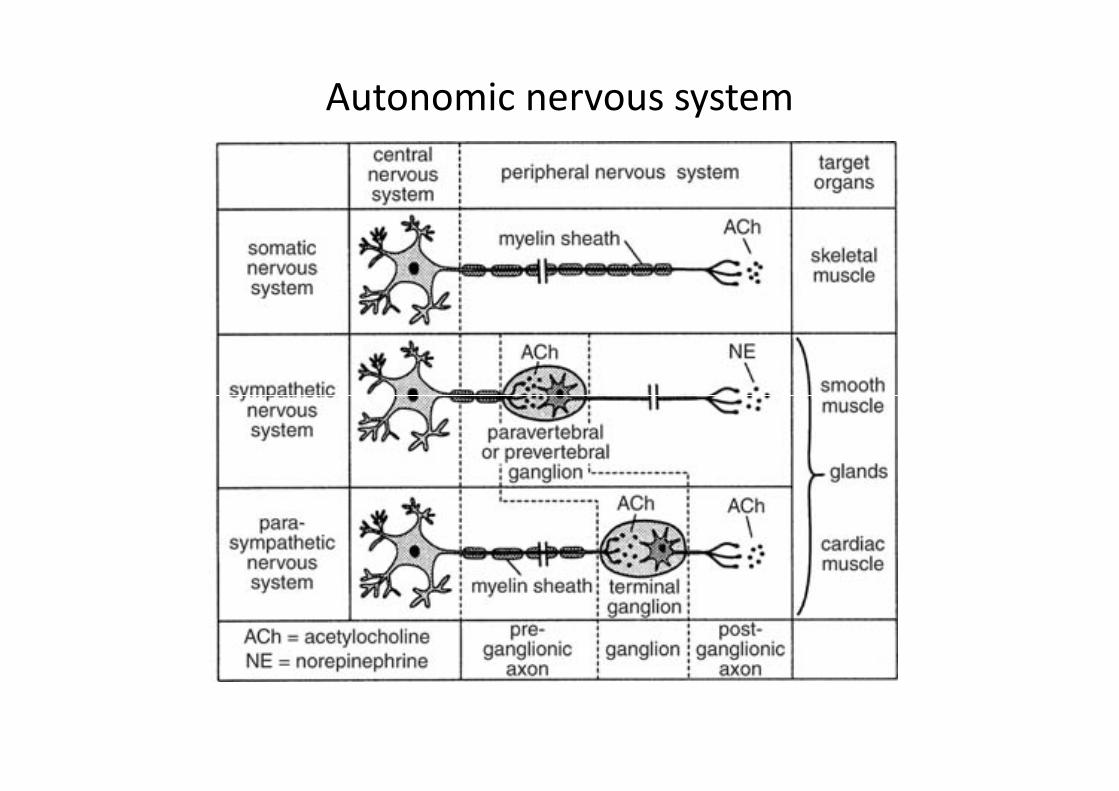
Autonomic nervous system
• Please note here that the junction between the
postganglionic nerve cell and a smooth muscle,
cardiac muscle or gland is only the final link in a
chain.
• Nerve pathways in the autonomic nervous system
involve at least two nerves cells. involve at least two nerves cells.
– Between the two sets of cells is a ganglia (a collection
of nerve cell bodies outside the brain and spinal cord).
– Those of the parasympathetic are all very close to, or
on, their target tissue, whereas those of the
sympathetic are far from their target tissue
Autonomic nervous system
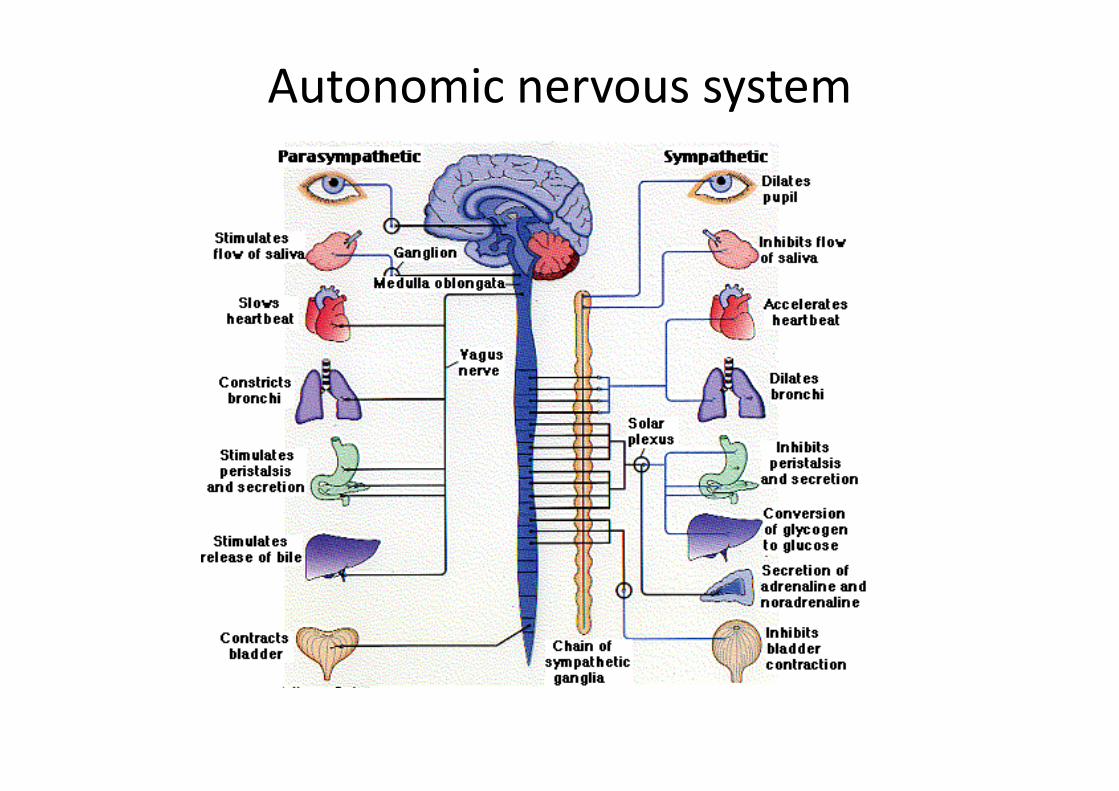
Autonomic nervous system

Autonomic nervous system

Nicotine – another reason not to smoke
• Their common factor is that Ach is the
neurotransmitter secreted at both of
autonomic ganglia
• However, at the neuroeffector junction
– acetylcholine is secreted at parasympathetic– acetylcholine is secreted at parasympathetic
neuroeffector junctions,
– nor-adrenaline is secreted at sympathetic ones

Nicotine – another reason not to smoke
• Muscarine
– mimics the effect of ACh at the neuroeffector
junction
– has no effect on the transmission at the ganglionic
junction between the two
• The ganglia of both sympathetic and • The ganglia of both sympathetic and
parasympathetic nervous systems respond to
nicotine (as in cigarettes)
• Nicotine potently stimulates both sympathetic
and parasympathetic ganglionic nerve cells.

John Langley• John Langley (1852 – 1925) wrote the original description
of the autonomic nervous system in 1921.
• In this book Langley included the sympathetic, parasympathetic and enteric (inherent within the gut) nervous systems.
• Langley used nicotine to map the ANS.
• He did this by painting nicotine on autonomic ganglia and watching sympathetic and parasympathetic responses. watching sympathetic and parasympathetic responses.
• He elicited a different effect as per the different ganglion he painted and by doing so he established to which division each ganglion belonged.
• He found nicotine had no effect at the neuroeffectorjunction; it did nothing when applied directly to sympathetic of parasympathetic nerve endings.

John Langley• He painted:
• Nicotine on ganglion cells that supplied a gland:
– The gland they supplied secreted
• Nicotine painted directly onto the gland
– Had no effect – Had no effect
• Muscarine painted on the ganglion cells
– Nothing happened
• Muscarine painted directly onto the gland
– The gland secreted
• So why did this happen?
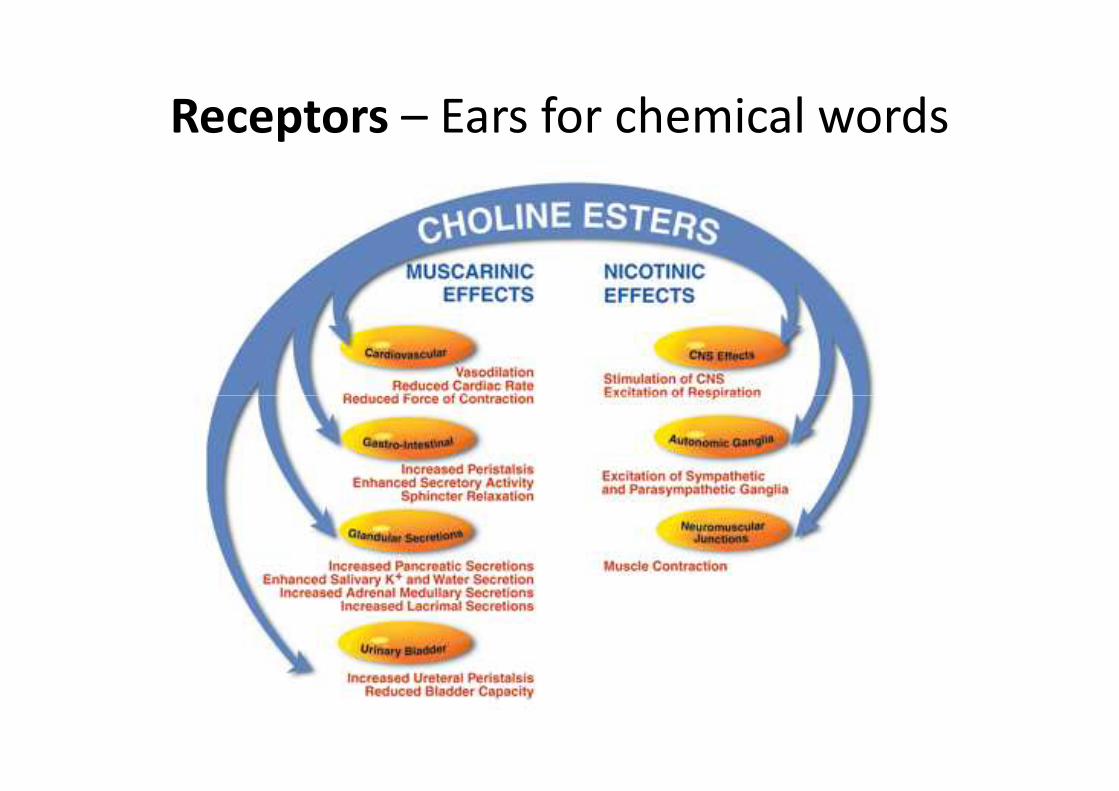
Receptors – Ears for chemical words• The answer to these observed phenomena lies in
the receptors.
• Neurotransmitters are the chemical that are released at nerve endings
• Receptors are the sites on the target tissue that respond to the neurotransmitters; these enable the target tissue to respond to the the target tissue to respond to the neurotransmitter
• Drugs and toxins, like muscarine and nicotine, have an effect on these molecular switches that activate cells by mimicking natural signalling molecules and binding to receptors.
Receptors – Ears for chemical words• The acetylcholine receptor can bind with
many molecules (some completely different to
ACh) and the end result of stimulation
depends upon which receptors are present on
the target tissue

Receptors – Ears for chemical words
• Cholinergic receptors are those receptors to which ACh bind
• Nicotinic receptors are those which nicotine-binding type of ACh receptors (at NMJ and autonomic ganglia)
• Muscarinic receptors are those which bind • Muscarinic receptors are those which bind muscarine-binding type receptors of ACh receptors
• Curare blocks nicotinic receptors (i.e. is an antagonist to nicotine)
• Atropine blocks muscarinic receptors (NEJ)
Receptors – Ears for chemical words

Receptors – Ears for chemical wordsNeuromuscular
junction
Autonomic
ganglion receptors
Postganglionic
receptors
Receptors nicotinic nicotinic Muscarinic
Agonist Acetylcholine; nicotine Acetylcholine; nicotine Acetylcholine. muscarine
Antagonist Curare Curare Atropine

Receptors – Ears for chemical words
• Present day science has deciphered the genes and the messages that encode the actual receptors
– It has shown that the muscular and ganglionic nicotinic receptors are several individual molecules that are similar, but not identical, to one another.
– This suggests that it is possible to design drugs to match these differences.
– This selective potency has enabled the advent of a group of drugs called ganglion blocking agents to be produced and (unlike curare) can produce ganglion block without producing neuromuscular paralysis.

Botulinum Toxin – the wonder of home cooking
• There was one more poison used in figuring that acetylcholine was the transmitter at the three major peripheral synapses:
– The parasympathetic neuroeffector junction
– The nerve-nerve junction in sympathetic and parasympathetic ganglia
– The musculoskeletal junction– The musculoskeletal junction
• Like Amanita Muscaria it can frequent picnics, but, unlike muscarine, this poison is not an intrinsic constituent of food that is consumed by mistake. This poison is added by the chef, though not deliberately or by lethal intent.
Botulinum Toxin – the wonder of home cooking
• Botulinum Toxin. It is made by a bacterium, Clostridium Botulinum
• It can cause an often fatal syndrome called botulism.
• Clostridium Botulinum is an obligate anaerobe– it cannot live in the presence of oxygen
• Oxygen in our bodies creates an environment where it is threat to it. However, it can make spores, which helps it survive conditions where growing conditions are not right. survive conditions where growing conditions are not right.
• These spores are remarkably resistant and long-lasting and when they do reach a good growing environment, they germinate.
• As they grow, they secrete their toxin and produce gas. These spores can contaminate food
• When food is canned or put up as preserves, the spores had better been killed by the canning or preserving process
Botulinum Toxin• There is no oxygen in a sealed can, any (aerobic)
organisms that depend upon oxygen will die
• Clostridium Botulinum loves it and will flourish. If the preserves are not sufficiently sterilized before canning, it is possibility that Clostridium Botulinum will form spores.
• If this can is opened, it will disgorge a burst of gas • If this can is opened, it will disgorge a burst of gas (probably unnoticed by the cook) and a dish containing Botulinum toxin will be served. Tinned tuna or salmon is an example of this and if you found any tin that bulges, it will possibly contain gas and is a tin that should not be consumed; such a bulge may be the mark of the presence of Clostridium Botulinum.
Botulinum Toxin• Botulinum toxin kills because, like curare, it abolishes
transmission at neuromuscular junctions. – The poisoned victim becomes gradually, but inexorably, weaker
as nerves lose their ability to stimulate muscle contraction. Those muscles used most are those to go first
– The more the victim struggles, the faster he becomes paralysed.
– The eyelids droop, the head sags, the wrinkles disappear from his face along with the activity of the facial muscles that caused them. them.
– As the muscular partition that separates the mouth and nose ceases to function, speech becomes more nasal.
– Weakness of the tongue causes words to slur. The legs lose their ability to support the body and the arms can no longer reach out for help.
– Then breathing stops; this is why botulism kills
– Salvation lies solely in an artificial respirator, but as botulism is not as reversible as curare, it will be needed be many months.

Botulinum Toxin
• Botulinum toxin is the most lethal of poisons; – weight for weight, nothing is as deadly.
– Cyanide is trivial in comparison.
• Its mechanism of action is different from curare
• Recall: – Curare blocks that action of acetylcholine at nicotinic – Curare blocks that action of acetylcholine at nicotinic
receptors.
• Botulinum does not.
• However, everything works as well as ever: the nerves will conduct, the receptors are active, and all the target organs (muscle, blood vessels, glands) work well
Botulinum Toxin
• Botulinum toxin gets into the nerve endings and digests critical proteins that enable the little packets of neurotransmitter to fuse with the cell membrane to release the acetylcholine transmitter.
• The Botulinum poisoned nerve is unable to • The Botulinum poisoned nerve is unable to secrete its neurotransmitter
– The nerve impulse passes down the nerve, reaches the terminal, which stands mute, unable to respond
– All the junctions that use acetylcholine as a transmitter thus cease to function.

Botulinum Toxin
• Unlike curare only blocks those junctions that have nicotinic receptors
• Botulinum toxin inactivates every nerve that uses acetylcholine as a neurotransmitter
– skeletal muscles fail
– the pupils no longer contract
– sweat cease to form
– saliva stops flowing.
• Botulinum toxin thus provided the ultimate proof that acetylcholine is a transmitter.

Botulinum Toxin – therapeutically?
• Botulinum toxin has proved useful though, if only in the cosmetic industry.
• Facial wrinkles are caused by repetitive contractions of the facial muscles and those wrinkles can be banished by paralysing the facial muscles. All hail the advent of ‘Botox’!
• Therapeutically, it has been used in cases of • Therapeutically, it has been used in cases of belepharospasm – the spontaneous and uncontrollable contraction of the eyelids.
• It has also been used in cases of cardiac sphincter spasm (at the entrance to the stomach). In all these cases the effects will eventually wear off, but it can be administered again and again.

The sympathetic transmitter –
acetylcholine’s elusive partner• The sympathetic nervous system has been more resistant
than the parasympathetic to scientific analysis. – The neurotransmitter at the sympathetic neuroeffector junction
was not acetylcholine.
• In 1904, T R Elliot, in England, has shown that an extract of the adrenal gland – adrenaline- had effects that closely resembled those of stimulating sympathetic nerves. resembled those of stimulating sympathetic nerves.
• From this it was thought that adrenaline was the neurotransmitter
• This was incorrect as years later it was found to be its biosynthetic precursor, noradrenalin (or nor-epinephrine, as they say in America)
The sympathetic transmitter
• Nor-adrenalin was finally discovered by a Swedish scientist, Ulf S von Euler, after World War II, who worked as a post-doctoral student for a while in Dale’s laboratory.
• The receptors that respond to adrenaline and noradrenaline are called adrenoceptors and noradrenaline are called adrenoceptors and respond differently to the two chemicals.
• The structures of the two are very similar and it was found to be difficult to establish differences between their actions.

The sympathetic transmitter• The neurotransmitter at synapses at the
neuroeffector junction of sympathetic nerves is noradrenaline.
• This is concentrated in vesicles in granules collected in little varicosities along the length of the nervethe nerve
• Similar granules are found in large numbers in the cells of the adrenal medulla, but here the transmitter is mainly adrenaline.
• Noradrenaline and adrenaline are made from an amino acid substrate, tyrosine:

Adrenaline synthesis

Adrenaline synthesis
• Here you can see from the diagram, from
Tyrosine:
– Tyrosine – DOPA – Dopamine – Noradrenaline –
Adrenaline. Adrenaline.
• Of these, the last three are all themselves
neurotransmitters, though for different nerves
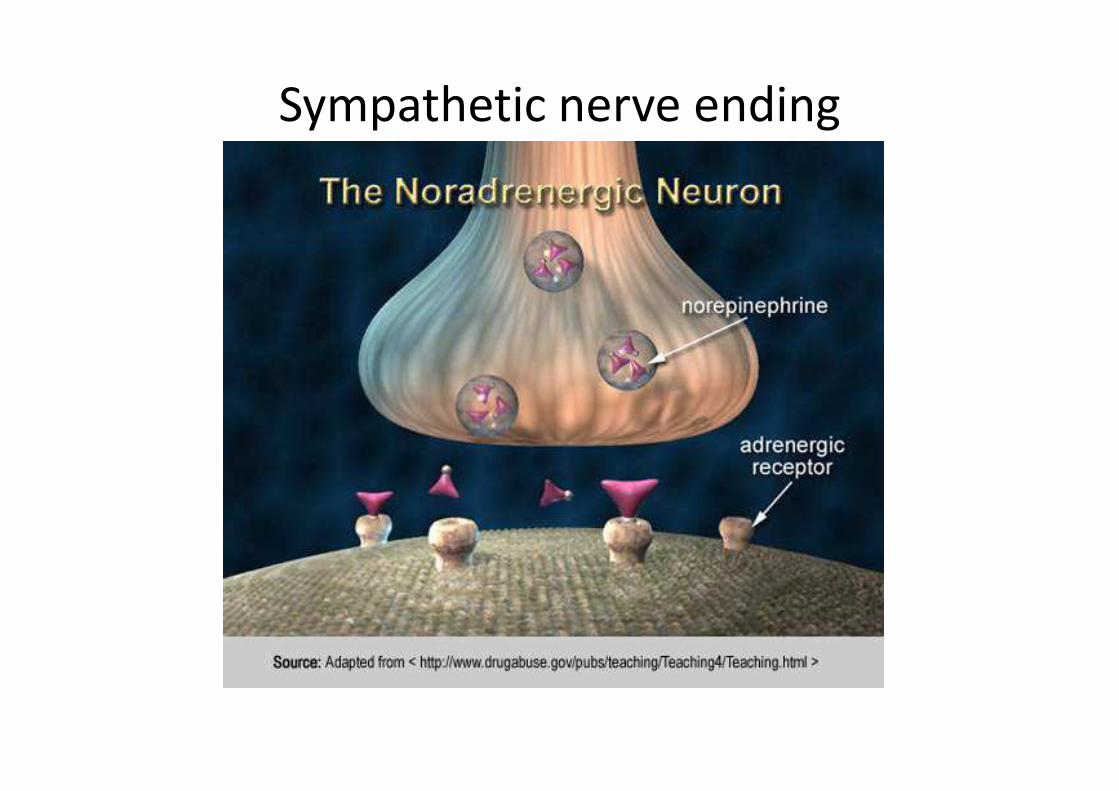
Sympathetic nerve ending

The sympathetic transmitter
• The effects of noradrenaline and adrenaline are very similar in action
– however their respective actions are dependent upon the receptors on which they act.
In the adrenal system there are• In the adrenal system there are
– α and β receptors
– these are subdivided into α1 and α2, and β1and β2.
• Confusing? Yes.


Organ Receptor type Response
Heart β1 Increase in heart rate,
contractility, and excitability
Coronary arteries α1
β2
Vasoconstriction
Vasodilatation
(predominant)
Skeletal muscles α1 Vasoconstriction
Skeletal arterioles β2 Vasodilatation
(predominant)
Bronchi β2 Bronchodilation
Iris α1 Contraction (pupil dilates)
Smooth muscle of gut α,β2 Relaxation
Sweat glands α1 Localised secretion
Salivary glands α1 Secretion (watery)
Bladder muscle β Relaxation
Bladder sphincter α1 Constriction
Metabolic effects β1
β2
Lipolysis
glycogenolysis

Organ Sympathetic Stimulation Parasympathetic Stimulation
Heart
↑ Rate (β1 & β2) ↓ Rate
↑ Contractile force (β1 & β2) ↓ Contractile force
↑ Conduction velocity ↓ Conduction velocity
ArteryConstriction (α1)
DilationDilation (β2)
VeinConstriction (α1)
Dilation (β2)
LungBronchial muscle:Relaxation (β2)
Bronchial muscle contraction
↑ Bronchial gland secretion
Gastrointestinal tract↓ Motility (β2) ↑ Motility
Sphincter: Contraction (α) Sphincter: Relaxation
Glycogenolysis (β2 & α)
Liver
Glycogenolysis (β2 & α)
Glycogen synthesisGluconeogenesis (β2 & α)
Lipolysis (β2 & α)
Kidney Renin secretion (β2)
BladderDetrusor: Relaxation (β2) Detrusor: Contraction
Sphincter: Contraction (α) Sphincter: Relaxation
Uterus
Contraction: Pregnant uterus (α)
Relaxation: Pregnant &non-pregnant uterus (β2)
Eye Pupil: Dilate (α)Pupil: Constrict
↑ Lacrimal gland secretions
Salivary glandsSubmandibularParotid
Viscous secretions (α) Watery secretions

Antibiotics • Term antibiotic coined in 1942 by Selman
Waksman to describe any substance produced
by a microorganism that is antagonist to the
growth of other microorganisms at high
dilution
• This definition excludes synthetic drugs – but
the didn’t know how then
• Now some are semi-synthetic, in that the
original compound was identified and it can
be ‘modified’

Antibiotics
• 1880’s – Paul Ehrlich noted that dyes would bind
to, and colour, cells
• He postulated that it might be possible to make
dyes/chemical that could target cells (e.g.
Bacteria) and kill them; but not harm the host
• He screened 100’s of dyes against organisms; • He screened 100’s of dyes against organisms;
through this (with Sahachiro Hata) discovered
Arsphenamine (Salvarsan)in 1908 (also called 606
• Found to be effective against syphilis (Hg prior to
this) but had nasty side-effects as As based
Antibiotics
• Blue mould on bread had been used since middle ages to treat suppurating wounds; was claims to this, but first published in 1875 by Royal Society
• In 1928, Alexander Fleming was growing staphylococcal bacteria in petri dishes and left staphylococcal bacteria in petri dishes and left one uncovered.
• In it he found areas where the bacteria wouldn’t grow; suggested a contaminant
• Noted the fungus (Penicillium Notatum) was effective against Gram positive bacteria

Antibiotics• He found that the mould was producing a
compound that inhibited the spread of
bacteria; called it penicillin.
• Found it to be very potent with minimal
toxicity
• But he believed, for a while, that penicillin
couldn’t last long enough inside the body to
kill pathological bacteria – stopped studying it
until 1931
• Began again in 1934
Antibiotics
• The chemical structure of penicillin was established in the 1940’s
• Mass production was established and 2.3 million doses were prepared ready for the Normandy invasion of 1944
• Following the discovery of its structure, it has • Following the discovery of its structure, it has been developed:
– Ampicillin – effective against a broad range of bacteria
– Beta-lactams –flucloxicillin, dicloxicillin, meticillin
– Many more
Antibiotics
• Mechanics of antibiotics:
1. Inhibition of peptidoglycan cross-links in the
cell wall
2. Inhibits DNA synthesis
3. Inhibits protein synthesis3. Inhibits protein synthesis

Cancer
• A ‘Cancer’ is descriptive of a group of cells
that display ‘malignant behaviour’:
– Invasion
– Metastases – Metastases
Cancer treatment
• Essentially three types of treatment:
– Surgery
– Chemotherapy
– Radiotherapy– Radiotherapy

Chemotherapy
• Chemotherapy is cytotoxic; effectively a
poison and can cause ‘apoptosis’
• All cells undergo mitosis
• Chemotherapy targets rapidly dividing cells
– Because of this, it will target all rapidly dividing – Because of this, it will target all rapidly dividing
cells:
• Hair
• Intestinal cells
• Bone marrow
Chemotherapy
• Even with tumour growth, the cells ‘adhere’ to
cell function and the regulation of cell growth
• It effective against ‘younger’ tumour cells
• With older cells, at the centre of the tumour,
there are less rapidly dividing cellsthere are less rapidly dividing cells
• Chemo less active against these cells
• Also, with solid tumours, the chemo may not
reach the centre of the tumour, therefore:
– Radiotherapy, surgery