Penn Treaty Underwriting Guide - NJLTC
40
PTA-UND(3/04)
Transcript of Penn Treaty Underwriting Guide - NJLTC
PTA-UND(3/04)
TABLE OF CONTENTS
General Information
Introduction .................................................................................. Page 1
Underwriting Considerations ........................................................ Page 1
Suitability Guidelines .................................................................... Page 2
Underwriting Tools/Protocol ........................................................ Page 4
Underwriting Classes (defined) ..................................................... Page 6
Underwriting Guidelines
Build tables (height/weight charts) ............................................... Page 7
Medical Conditions ....................................................................... Page 9
Medications
Unacceptable Medications ......................................................... Page 28
Common Medications and why typically prescribed .................. Page 28
Procedural Information
Replacements .............................................................................. Page 31
Counter Offers ............................................................................. Page 31
Spousal Discounts ...................................................................... Page 32
Reissues ...................................................................................... Page 32
Increasing Benefits ..................................................................... Page 33
Decreasing Benefits .................................................................... Page 33
Underwriting Appeals ................................................................. Page 33
Underwriting Class Upgrades ..................................................... Page 34
Reinstatements ............................................................................ Page 34
Effective Dates ............................................................................ Page 34
Saving Age .................................................................................. Page 34
IntroductionThe purpose of this guide is to assist our agency force with the Long-Term Careinsurance qualification process. Our unique Underwriting philosophy allows usto offer coverage to a very high percentage of potential applicants with the use offive different rate classes (including the Secured Risk Plan, available in mostStates). These rate classes and our diverse variety of products, including stand-alone Facility, stand-alone Home Care, comprehensive LTC, as well as both Tax-Qualified and Non-Tax qualified versions, are designed to fit the individual needsof your clients. (Please check the availability of products available within yourState on line at www.penntreaty.com or by contacting our Marketing Departmentat (800) 362-0700.)
By utilizing our risk stratification approach and charging the appropriatepremiums for a wide variety of risks, our goal is to properly classify the applicantssubmitted and issue as much of your business as possible. Those applicants whocan effectively live independently and do not exhibit signs of possible cognitiveimpairment are generally offered coverage, even if they may have had problemsobtaining ltci elsewhere.
Both you, our agents, and your clients are valued customers and we appreciateyour business. We work diligently to maintain and improve upon the best serviceavailable throughout the ltci industry. Our Underwriters are available for you tospeak with directly regarding questions of insurablility, rating, and to help you inany way. We encourage you to contact them directly at (800)222-3469 ext. #3516.
We also encourage you to use the Underwriting Wizard, available as software oron the Agent Resource Center at www.penntreaty.com. The Underwriting Wizardis the same tool utilized by our in-house Underwriting Staff and allows you toobtain a realistic quote based on your applicant’s health history. This tool can beparticularly helpful to you when attempting to correctly classify an applicant withmultiple medical conditions. The Agent Resource Center also allows you to reviewthe status of all your pending applications.
Underwriting ConsiderationsNaturally, an applicant must currently be capable of independently performing allActivities of Daily Living ( ADLs), including bathing, dressing, eating transferring,ambulating, continence and toileting. The applicant must also be capable ofperforming their Instrumental Activities of Daily Living (IADLs), including mealpreparation, light housekeeping, laundry, shopping/travel, telephoning,medication management, handling money/bill paying.
1

In addition to independence with the ADLs and IADLs, and in order to properlyevaluate the risk associated with needing Long Term Care in the future, we mustconsider several other factors which may affect the applicant’s ability to liveindependently. These factors include the following:
• Current health status, both mentally and physically, including heightand weight and all medications as well as the reasons they are beingtaken.
• Past health status including prior conditions, hospitalizations,surgeries, medications etc.
• Cognitive functioning.
• Activity Level with respect to both physical and social habits.
• Living Situation, including with whom applicant resides, wherethey reside, and the length of time they have resided in current home.
• Financial situation of applicant (see Suitability Guidelines below).
Suitability GuidelinesAlthough ltci is often an important tool that can be used to help protect individualsand their families from the potentially devastating and rising costs associated withthe risk of Long Term Care, it is important to remember that ltci is not for everyone.Prior to applying for insurance, agents must consider and discuss the client’s financialpicture and the appropriateness of purchasing ltci. Please verify requirements inyour State ( available on our website) as many States have adopted the NAIC suitabilitymodel and require the completion of Personal Worksheets designed to provide theInsurance Company insight into the applicant’s financial “picture”. (While applicantsdo have the option of not providing financial information, they must still sign theSuitability Form indicating that they do not wish to provide such information.) Whenthey choose not to provide financial information, the agent can greatly expedite theunderwriting process by having the applicant also sign and submit a Waiver Form.The following chart provides some guidelines with respect to the appropriateness ofpurchasing Long Term Care insurance.
Individual Assets(not incl. Primary residence) % of Income to be Applied to LTCi$30,000 or below Please reconsider applicants’ ltci needs$30,000 to $100,000 7 % of annual income$100,000 and above 10 % of annual income
2
The preceding figures are intended to be a practical rule of thumb, however it isimportant to remember that they are only guidelines. In certain cases, for example,those who may be eligible for Medicaid may find it appropriate for their family to payfor ltci premiums, giving the insured access to a higher quality of care in the settingof their choice.
In addition to having a reasonable expectation that premiums can be paid on aregular basis, several other factors should be taken into consideration, including thefollowing:
• The cost of care within the specific region where the applicant wouldreceive care.
• The applicant’s goals and needs with respect to the advantages and costof ltci to meet these goals and needs.
• The appropriateness of benefits in relation to the age of the applicant.
• If replacing, the appropriateness of replacement. A Comparison Formmust be competed and submitted with all replacements. All replacementsmust result in an improvement for the insured.
• The applicant should be made aware that our products are priced suchthat future rate increases are not anticipated, however, unforeseen factorsor adverse experience could affect rates and future rates may be increasedif required. The applicant should consider whether they could afford topay premiums if the rates were increased, for example, by 20%.
• The applicant should consider how their income as well as their assetsmay change in the future, including retirement, unforeseen life events, orany other factors which might affect their ability to pay premiums.
Suitability Procedures1. When required within your State (please verify if required and correct
forms needed by looking on our Website), the appropriate PersonalWorksheet must be completed and signed by your applicant and submittedwith the application for insurance. Please note that the applicant maychoose not to reveal their financial information by marking the appropriatebox, however, regardless of whether or not this information is provided,the form must be signed by the applicant and submitted to us.
2. If, upon receipt of the application and Personal Worksheet, the applicantmeets the criteria outlined in the above “Suitability Guidelines” section,we may proceed with the processing of the application.
3
3. If the Personal Worksheet indicates that the purchase of the proposedpolicy may not be suitable financially, we are required to forward theapplicant an Intent Confirmation Form, which they must complete andreturn to us in order for us to proceed.
4. If the applicant chooses not to provide their financial information bychecking the appropriate box, the agent will significantly expedite theUnderwriting process by also submitting a signed Suitability Waiver Form.Otherwise, we must again contact your applicant regarding theserequirements and receive confirmation that they wish to proceed.
Underwriting Tools and ProtocolThe application is the first and perhaps the most important tool an Underwriter utilizesduring the Underwriting process. We cannot over-emphasize the importance ofcompleting each application thoroughly and providing details regarding healthconditions, hospitalizations, accurate height and weight, as well as medications andthe reasons they are being taken. A properly completed application and good fieldUnderwriting, utilizing the proper rate classifications beginning on page 9 of thisguide and/or the Underwriting Wizard, will result in fewer declines, fewer counter-offers, and often times significantly expedites the Underwriting process. Any additionalinformation provided by the agent with respect to activity level, exercise, work orvolunteer status, living arrangements etc. can be very valuable and provide insightwhich may not be evident from the application alone. We welcome such informationand if additional space is needed, please submit an attachment, signed and dated bythe applicant which will be treated as part of the application.
All applications must be signed and dated on the actual date completed and shouldbe received in our office within 2 weeks of the date signed.
Following is a list of additional tools, a brief description of what these tools entail, aswell as an indication of when each of these tools are generally required:
Personal History Interview (PHI) - A telephonic interview designed to confirminformation on the application, as well as to obtain additional information regardingthe applicant’s physical health, cognitive status, and activity level.
Paramedical Interview - A face-to-face interview, conducted in the applicant’s homeby a health professional. A Paramedical interview does not include blood work,urinalysis, or other invasive testing, but is a series of questions to help us furtherevaluate the applicant’s medical history, physical condition, and cognitive status. Itis also valuable because it provides additional insight into the applicant’s activitylevel and living arrangements, which may not be as evident through the use of atelephonic interview.
4
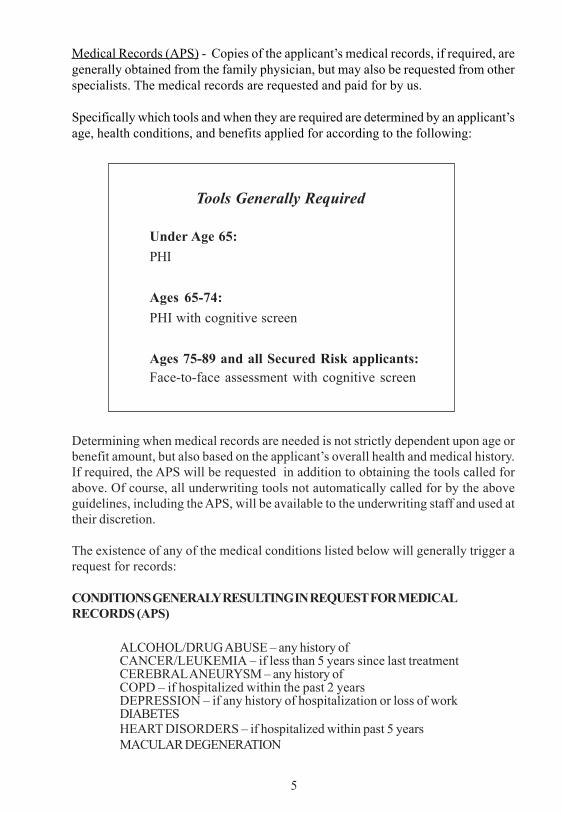
Medical Records (APS) - Copies of the applicant’s medical records, if required, aregenerally obtained from the family physician, but may also be requested from otherspecialists. The medical records are requested and paid for by us.
Specifically which tools and when they are required are determined by an applicant’sage, health conditions, and benefits applied for according to the following:
Tools Generally Required
Under Age 65:PHI
Ages 65-74:PHI with cognitive screen
Ages 75-89 and all Secured Risk applicants:Face-to-face assessment with cognitive screen
Determining when medical records are needed is not strictly dependent upon age orbenefit amount, but also based on the applicant’s overall health and medical history.If required, the APS will be requested in addition to obtaining the tools called forabove. Of course, all underwriting tools not automatically called for by the aboveguidelines, including the APS, will be available to the underwriting staff and used attheir discretion.
The existence of any of the medical conditions listed below will generally trigger arequest for records:
CONDITIONS GENERALY RESULTING IN REQUEST FOR MEDICALRECORDS (APS)
ALCOHOL/DRUG ABUSE – any history ofCANCER/LEUKEMIA – if less than 5 years since last treatmentCEREBRAL ANEURYSM – any history ofCOPD – if hospitalized within the past 2 yearsDEPRESSION – if any history of hospitalization or loss of workDIABETESHEART DISORDERS – if hospitalized within past 5 yearsMACULAR DEGENERATION
5
PERIPHERAL VASCULAR DISEASESARCOIDOSISSPINAL STENOSIS – if not surgically correctedSTROKE or TIA – any history ofSYNCOPE – if within past yearTRANSIENT GLOBAL AMNESIATREMOR
In addition to the above, an APS is likely to be requested whenever an applica-tion or applicant interview reveals any of the following:
• 3 or more conditions which are chronic (ongoing, long duration).• 4 or more current medications.• Chronic condition with lack of control, complications, or which does
not indicate regular care by a physician (indicating poorcompliance).
When the applicant is informed by the agent at time of application which tools willmost likely be required, the applicant is much more likely to understand theunderwriting process and be more willing, when necessary, to provide and/orassist us in obtaining the above information.
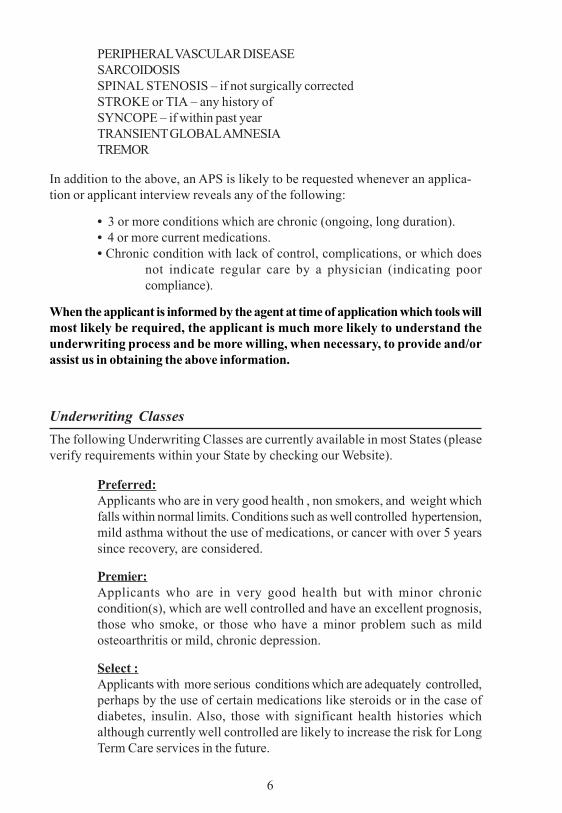
Underwriting ClassesThe following Underwriting Classes are currently available in most States (pleaseverify requirements within your State by checking our Website).
Preferred:Applicants who are in very good health , non smokers, and weight whichfalls within normal limits. Conditions such as well controlled hypertension,mild asthma without the use of medications, or cancer with over 5 yearssince recovery, are considered.
Premier:Applicants who are in very good health but with minor chroniccondition(s), which are well controlled and have an excellent prognosis,those who smoke, or those who have a minor problem such as mildosteoarthritis or mild, chronic depression.
Select :Applicants with more serious conditions which are adequately controlled,perhaps by the use of certain medications like steroids or in the case ofdiabetes, insulin. Also, those with significant health histories whichalthough currently well controlled are likely to increase the risk for LongTerm Care services in the future.
6
Standard (sub standard in FL):Applicants who have a very significant health condition, which althoughinsurable, greatly increases the risk for needing Long Term Care in thefuture, such as those currently being treated for cancer, severe heartconditions like cardiomyopathy, or those individuals who may have severalchronic Conditions which together, significantly increase the risk of needingLTC in the future.
Secured Risk Plan:Includes those individuals who have been diagnosed with a condition whichhistorically has been considered uninsurable. Those eligible are generallyin the beginning stages and/or exhibit little if any symptoms of the conditionand do not have an impending need for care. Examples are beginning stageParkinson’s or those who have been diagnosed with Multiple Sclerosisbut whose activities are not significantly limited. The Secured Risk Planalso allows us to offer coverage to those who, due to the significance ormultiplicity of conditions, such as diabetes with a heart condition and historyof a stroke, are not eligible for the other ltci products we offer. Those withany signs of cognitive impairment are not eligible for the Secured Risk Planor any ltci we offer.
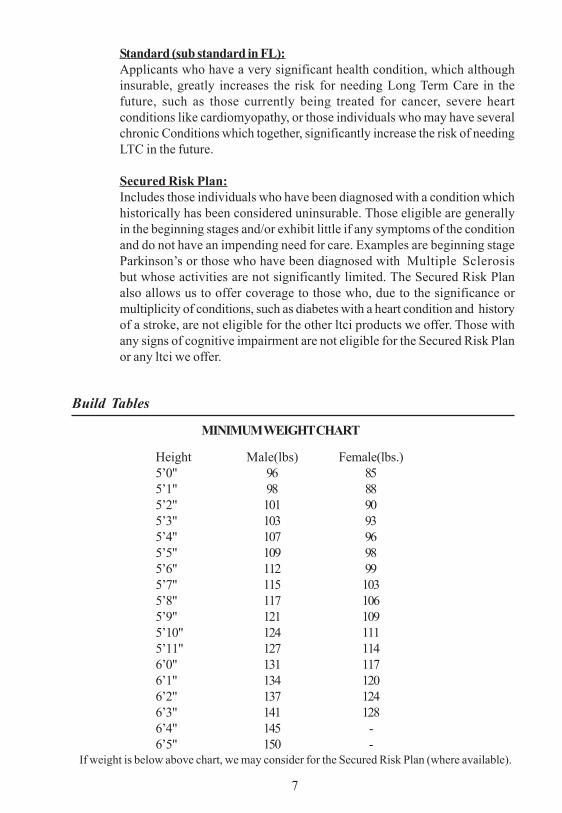
Build Tables
MINIMUM WEIGHT CHART
Height Male(lbs) Female(lbs.)5’0" 96 855’1" 98 885’2" 101 905’3" 103 935’4" 107 965’5" 109 985’6" 112 995’7" 115 1035’8" 117 1065’9" 121 1095’10" 124 1115’11" 127 1146’0" 131 1176’1" 134 1206’2" 137 1246’3" 141 1286’4" 145 -6’5" 150 -
If weight is below above chart, we may consider for the Secured Risk Plan (where available).
7
8
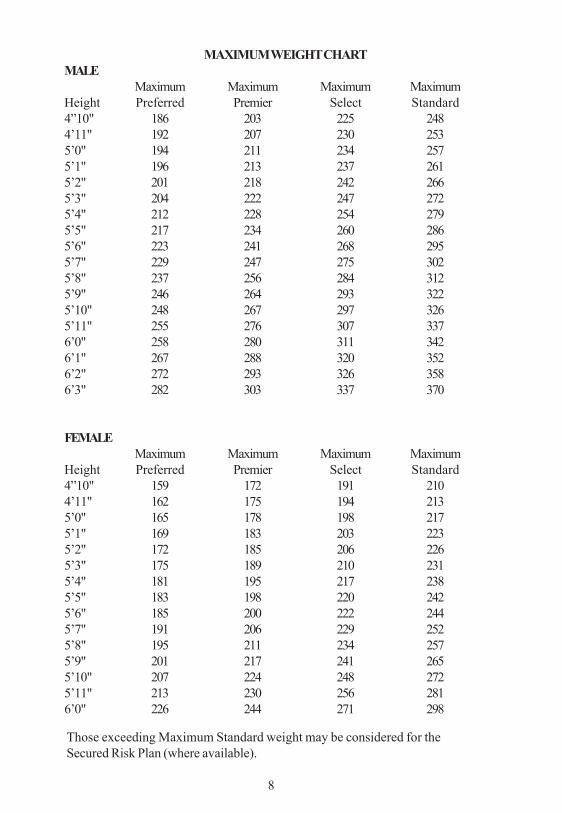
MAXIMUM WEIGHT CHARTMALE
Maximum Maximum Maximum MaximumHeight Preferred Premier Select Standard4”10" 186 203 225 2484’11" 192 207 230 2535’0" 194 211 234 2575’1" 196 213 237 2615’2" 201 218 242 2665’3" 204 222 247 2725’4" 212 228 254 2795’5" 217 234 260 2865’6" 223 241 268 2955’7" 229 247 275 3025’8" 237 256 284 3125’9" 246 264 293 3225’10" 248 267 297 3265’11" 255 276 307 3376’0" 258 280 311 3426’1" 267 288 320 3526’2" 272 293 326 3586’3" 282 303 337 370
Those exceeding Maximum Standard weight may be considered for theSecured Risk Plan (where available).
FEMALEMaximum Maximum Maximum Maximum
Height Preferred Premier Select Standard4”10" 159 172 191 2104’11" 162 175 194 2135’0" 165 178 198 2175’1" 169 183 203 2235’2" 172 185 206 2265’3" 175 189 210 2315’4" 181 195 217 2385’5" 183 198 220 2425’6" 185 200 222 2445’7" 191 206 229 2525’8" 195 211 234 2575’9" 201 217 241 2655’10" 207 224 248 2725’11" 213 230 256 2816’0" 226 244 271 298
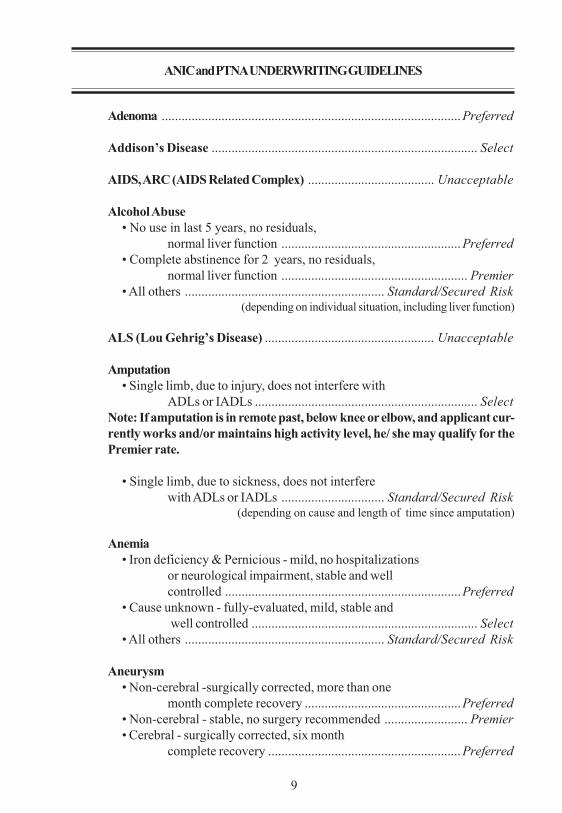
ANIC and PTNA UNDERWRITING GUIDELINES
Adenoma ..........................................................................................Preferred
Addison’s Disease ................................................................................ Select
AIDS, ARC (AIDS Related Complex) ...................................... Unacceptable
Alcohol Abuse• No use in last 5 years, no residuals,
normal liver function ......................................................Preferred• Complete abstinence for 2 years, no residuals,
normal liver function ........................................................ Premier• All others ............................................................ Standard/Secured Risk
(depending on individual situation, including liver function)
ALS (Lou Gehrig’s Disease) ................................................... Unacceptable
Amputation• Single limb, due to injury, does not interfere with
ADLs or IADLs ................................................................... SelectNote: If amputation is in remote past, below knee or elbow, and applicant cur-rently works and/or maintains high activity level, he/ she may qualify for thePremier rate.
• Single limb, due to sickness, does not interferewith ADLs or IADLs ............................... Standard/Secured Risk
(depending on cause and length of time since amputation)
Anemia• Iron deficiency & Pernicious - mild, no hospitalizations
or neurological impairment, stable and wellcontrolled .......................................................................Preferred
• Cause unknown - fully-evaluated, mild, stable andwell controlled .................................................................... Select
• All others ............................................................ Standard/Secured Risk
Aneurysm• Non-cerebral -surgically corrected, more than one
month complete recovery ...............................................Preferred• Non-cerebral - stable, no surgery recommended ......................... Premier• Cerebral - surgically corrected, six month
complete recovery ..........................................................Preferred
9
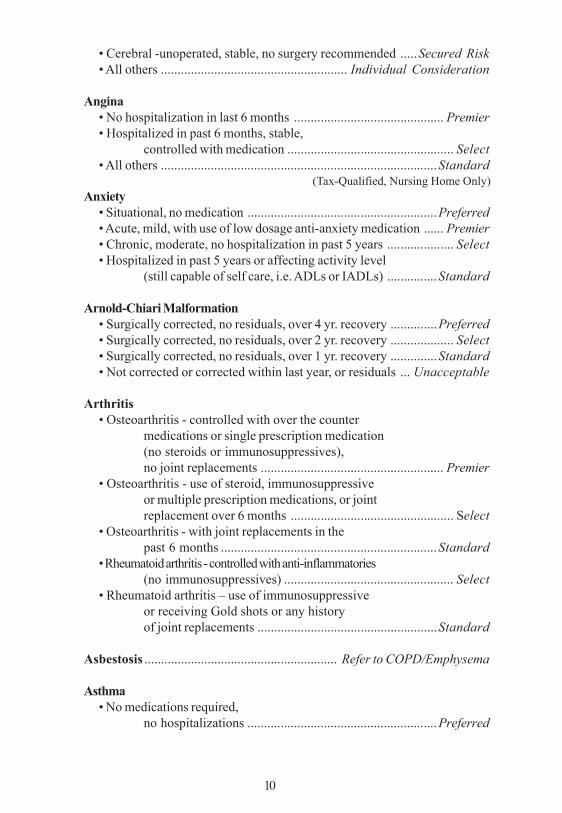
• Cerebral -unoperated, stable, no surgery recommended .....Secured Risk• All others ........................................................ Individual Consideration
Angina• No hospitalization in last 6 months ............................................. Premier• Hospitalized in past 6 months, stable,
controlled with medication .................................................. Select• All others ...................................................................................Standard
(Tax-Qualified, Nursing Home Only)Anxiety
• Situational, no medication .........................................................Preferred• Acute, mild, with use of low dosage anti-anxiety medication ...... Premier• Chronic, moderate, no hospitalization in past 5 years .................... Select• Hospitalized in past 5 years or affecting activity level
(still capable of self care, i.e. ADLs or IADLs) ...............Standard
Arnold-Chiari Malformation• Surgically corrected, no residuals, over 4 yr. recovery ..............Preferred• Surgically corrected, no residuals, over 2 yr. recovery ................... Select• Surgically corrected, no residuals, over 1 yr. recovery ..............Standard• Not corrected or corrected within last year, or residuals ... Unacceptable
Arthritis• Osteoarthritis - controlled with over the counter
medications or single prescription medication(no steroids or immunosuppressives),no joint replacements ....................................................... Premier
• Osteoarthritis - use of steroid, immunosuppressiveor multiple prescription medications, or jointreplacement over 6 months ................................................. Select
• Osteoarthritis - with joint replacements in thepast 6 months .................................................................Standard
• Rheumatoid arthritis - controlled with anti-inflammatories(no immunosuppressives) ................................................... Select
• Rheumatoid arthritis – use of immunosuppressiveor receiving Gold shots or any historyof joint replacements ......................................................Standard
Asbestosis .......................................................... Refer to COPD/Emphysema
Asthma• No medications required,
no hospitalizations .........................................................Preferred
10
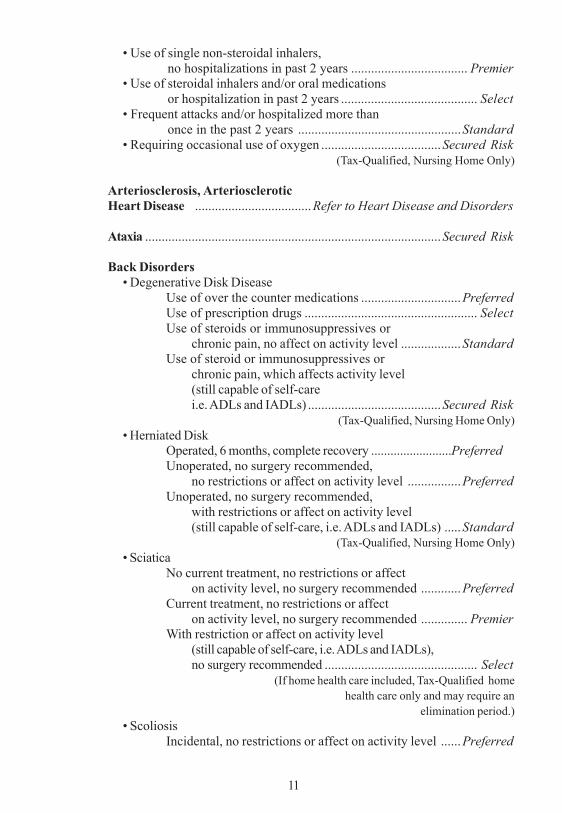
• Use of single non-steroidal inhalers,no hospitalizations in past 2 years ................................... Premier
• Use of steroidal inhalers and/or oral medicationsor hospitalization in past 2 years ......................................... Select
• Frequent attacks and/or hospitalized more thanonce in the past 2 years .................................................Standard
• Requiring occasional use of oxygen ....................................Secured Risk (Tax-Qualified, Nursing Home Only)
Arteriosclerosis, ArterioscleroticHeart Disease ...................................Refer to Heart Disease and Disorders
Ataxia .........................................................................................Secured Risk
Back Disorders• Degenerative Disk Disease
Use of over the counter medications ..............................PreferredUse of prescription drugs .................................................... SelectUse of steroids or immunosuppressives or
chronic pain, no affect on activity level ..................StandardUse of steroid or immunosuppressives or
chronic pain, which affects activity level(still capable of self-carei.e. ADLs and IADLs) ........................................Secured Risk
(Tax-Qualified, Nursing Home Only)• Herniated Disk
Operated, 6 months, complete recovery .........................PreferredUnoperated, no surgery recommended,
no restrictions or affect on activity level ................PreferredUnoperated, no surgery recommended,
with restrictions or affect on activity level(still capable of self-care, i.e. ADLs and IADLs) .....Standard
(Tax-Qualified, Nursing Home Only)• Sciatica
No current treatment, no restrictions or affecton activity level, no surgery recommended ............Preferred
Current treatment, no restrictions or affecton activity level, no surgery recommended .............. Premier
With restriction or affect on activity level(still capable of self-care, i.e. ADLs and IADLs),no surgery recommended .............................................. Select
(If home health care included, Tax-Qualified homehealth care only and may require an
elimination period.)• Scoliosis
Incidental, no restrictions or affect on activity level ......Preferred
11

• Spinal StenosisSurgically corrected, complete recovery .........................PreferredUnoperated, no surgery recommended, norestrictions or affect on activity level .................................. Select
• Chronic pain or numbness, no restrictionsor affect on activity level ................................................ Standard
(Tax-Qualified, Nursing Home Only)• Chronic pain or numbness, which affects
activity level (still capable of self-carei.e. ADLs and IADLs) ............................................... Secured Risk
(Tax-Qualified, Nursing Home Only)
Bell’s Palsy ..................................................................................... Preferred
Bronchiectasis• Mild to moderate, controlled, stable
pulmonary function tests .................................................... Select• Chronic with ongoing steroid usage or
poor pulmonary function tests .......................................StandardBronchitis
• Acute, mild, well controlled .......................................................Preferred• Chronic, well controlled with use of steroid,
stable pulmonary function tests .......................................... Select• Not well controlled or poor pulmonary
function tests .......................................... Standard/Secured Risk
Bursitis ........................................................................................... Preferred
Cancer - Prostate• Over 2 years since diagnosis and treatment initiated,
PSA under 1.5, not necessarily organ-confined,but no clinical evidence of metastasis ............................ Preferred
(no involvement of bone, lymph nodes or other organs)• Over 2 years since diagnosis and treatment initiated, PSA
1.5 or over, not necessarily organ-confined, but noclinical evidence of metastasis ............................................ Select
(no involvement of bone, lymph nodes or other organs)• Under 2 years since diagnosis and treatment initiated, PSA
under 1.5, organ confined ................................................ Premier• Under 2 years since diagnosis and treatment initiated,
PSA under 1.5, not organ confined, but noclinical evidence of metastasis ............................................ Select
(No involvement of bone, lymph nodes or other organs)• Under 2 years since diagnosis and treatment initiated,
PSA1.5 or over, organ confined .......................................... Select• Less than 2 years since diagnosis and treatment initiated,
PSA 1.5 or over, not organ confined ............................... Standard
12
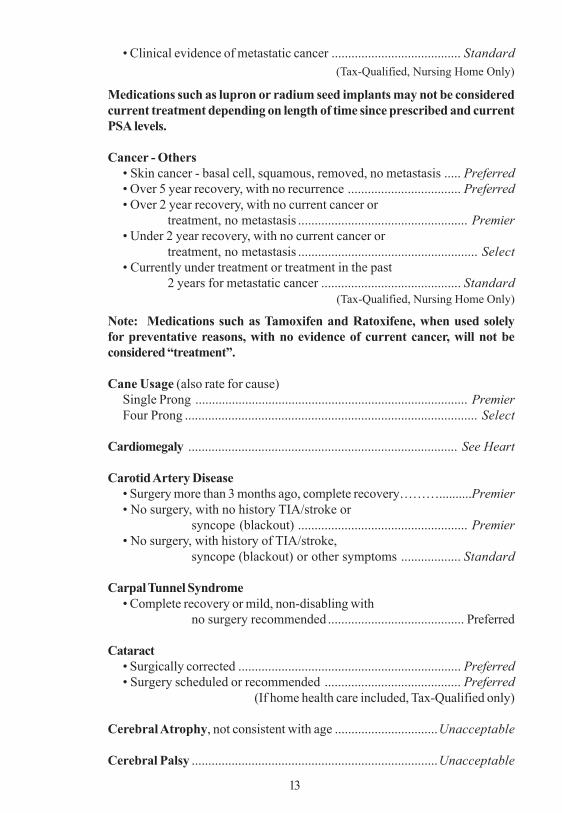
• Clinical evidence of metastatic cancer ....................................... Standard (Tax-Qualified, Nursing Home Only)
Medications such as lupron or radium seed implants may not be consideredcurrent treatment depending on length of time since prescribed and currentPSA levels.
Cancer - Others• Skin cancer - basal cell, squamous, removed, no metastasis ..... Preferred• Over 5 year recovery, with no recurrence .................................. Preferred• Over 2 year recovery, with no current cancer or
treatment, no metastasis ................................................... Premier• Under 2 year recovery, with no current cancer or
treatment, no metastasis ...................................................... Select• Currently under treatment or treatment in the past
2 years for metastatic cancer .......................................... Standard (Tax-Qualified, Nursing Home Only)
Note: Medications such as Tamoxifen and Ratoxifene, when used solelyfor preventative reasons, with no evidence of current cancer, will not beconsidered “treatment”.
Cane Usage (also rate for cause)Single Prong .................................................................................. PremierFour Prong ........................................................................................ Select
Cardiomegaly ................................................................................. See Heart
Carotid Artery Disease• Surgery more than 3 months ago, complete recovery………..........Premier• No surgery, with no history TIA/stroke or
syncope (blackout) ................................................... Premier• No surgery, with history of TIA/stroke,
syncope (blackout) or other symptoms .................. Standard
Carpal Tunnel Syndrome• Complete recovery or mild, non-disabling with
no surgery recommended ......................................... Preferred
Cataract• Surgically corrected ................................................................... Preferred• Surgery scheduled or recommended ......................................... Preferred
(If home health care included, Tax-Qualified only)
Cerebral Atrophy, not consistent with age ...............................Unacceptable
Cerebral Palsy ..........................................................................Unacceptable
13
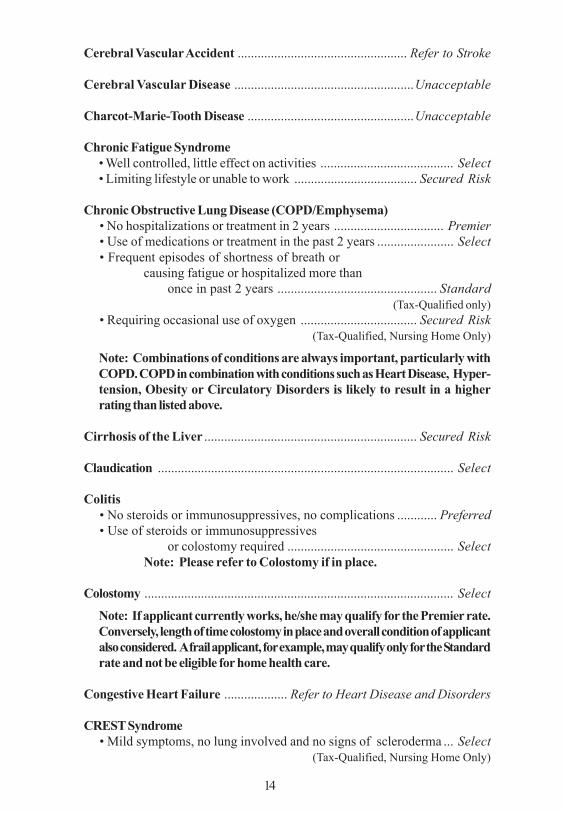
Cerebral Vascular Accident ................................................... Refer to Stroke
Cerebral Vascular Disease ......................................................Unacceptable
Charcot-Marie-Tooth Disease ..................................................Unacceptable
Chronic Fatigue Syndrome• Well controlled, little effect on activities ........................................ Select• Limiting lifestyle or unable to work ..................................... Secured Risk
Chronic Obstructive Lung Disease (COPD/Emphysema)• No hospitalizations or treatment in 2 years ................................. Premier• Use of medications or treatment in the past 2 years ....................... Select• Frequent episodes of shortness of breath or
causing fatigue or hospitalized more thanonce in past 2 years ................................................ Standard
(Tax-Qualified only)• Requiring occasional use of oxygen ................................... Secured Risk
(Tax-Qualified, Nursing Home Only)
Note: Combinations of conditions are always important, particularly withCOPD. COPD in combination with conditions such as Heart Disease, Hyper-tension, Obesity or Circulatory Disorders is likely to result in a higherrating than listed above.
Cirrhosis of the Liver ................................................................ Secured Risk
Claudication ......................................................................................... Select
Colitis• No steroids or immunosuppressives, no complications ............ Preferred• Use of steroids or immunosuppressives
or colostomy required .................................................. SelectNote: Please refer to Colostomy if in place.
Colostomy ............................................................................................. Select
Note: If applicant currently works, he/she may qualify for the Premier rate.Conversely, length of time colostomy in place and overall condition of applicantalso considered. A frail applicant, for example, may qualify only for the Standardrate and not be eligible for home health care.
Congestive Heart Failure ................... Refer to Heart Disease and Disorders
CREST Syndrome• Mild symptoms, no lung involved and no signs of scleroderma ... Select
(Tax-Qualified, Nursing Home Only)
14
15
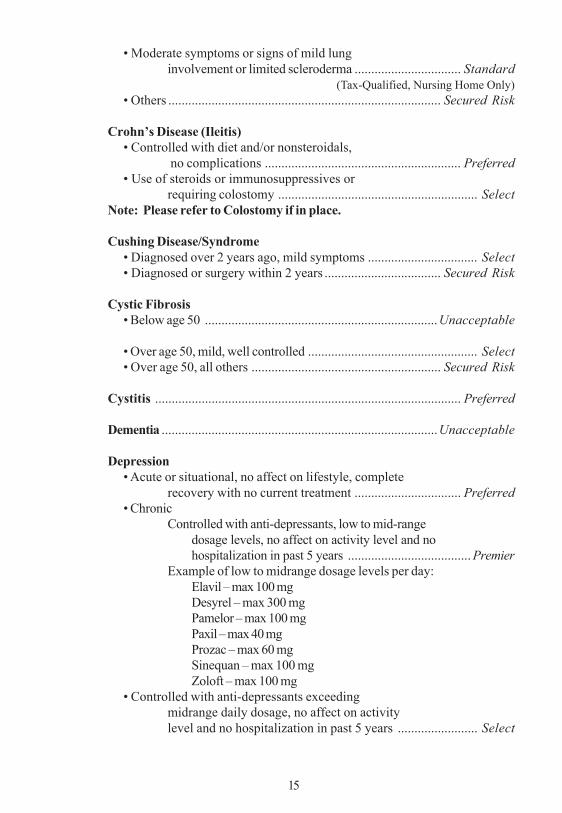
• Moderate symptoms or signs of mild lunginvolvement or limited scleroderma ................................ Standard
(Tax-Qualified, Nursing Home Only)• Others .................................................................................. Secured Risk
Crohn’s Disease (Ileitis)• Controlled with diet and/or nonsteroidals,
no complications ........................................................... Preferred• Use of steroids or immunosuppressives or
requiring colostomy ............................................................ SelectNote: Please refer to Colostomy if in place.
Cushing Disease/Syndrome• Diagnosed over 2 years ago, mild symptoms ................................. Select• Diagnosed or surgery within 2 years ................................... Secured Risk
Cystic Fibrosis• Below age 50 ......................................................................Unacceptable
• Over age 50, mild, well controlled ................................................... Select• Over age 50, all others ......................................................... Secured Risk
Cystitis ............................................................................................ Preferred
Dementia ...................................................................................Unacceptable
Depression• Acute or situational, no affect on lifestyle, complete
recovery with no current treatment ................................ Preferred• Chronic
Controlled with anti-depressants, low to mid-rangedosage levels, no affect on activity level and nohospitalization in past 5 years ..................................... Premier
Example of low to midrange dosage levels per day:Elavil – max 100 mgDesyrel – max 300 mgPamelor – max 100 mgPaxil – max 40 mgProzac – max 60 mgSinequan – max 100 mgZoloft – max 100 mg
• Controlled with anti-depressants exceedingmidrange daily dosage, no affect on activitylevel and no hospitalization in past 5 years ........................ Select
16
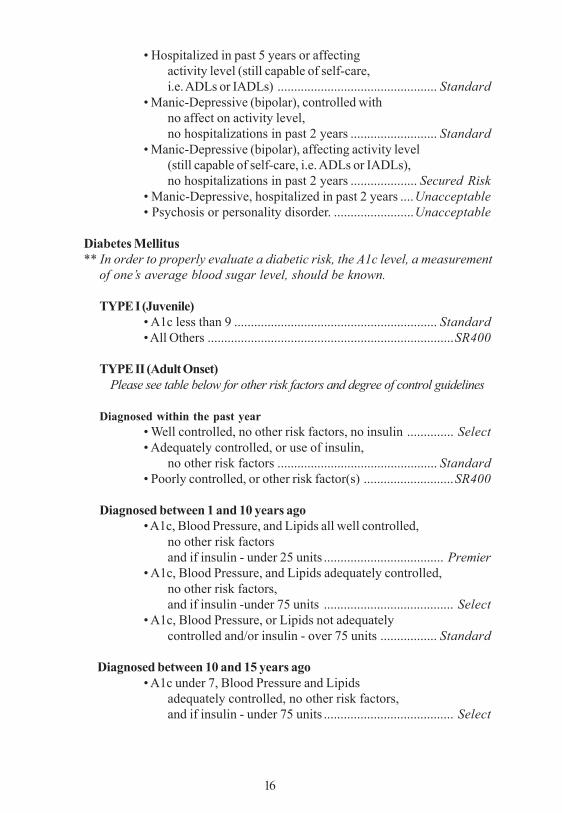
• Hospitalized in past 5 years or affectingactivity level (still capable of self-care,i.e. ADLs or IADLs) ................................................ Standard
• Manic-Depressive (bipolar), controlled withno affect on activity level,no hospitalizations in past 2 years .......................... Standard
• Manic-Depressive (bipolar), affecting activity level(still capable of self-care, i.e. ADLs or IADLs),no hospitalizations in past 2 years .................... Secured Risk
• Manic-Depressive, hospitalized in past 2 years ....Unacceptable• Psychosis or personality disorder. ........................Unacceptable
Diabetes Mellitus** In order to properly evaluate a diabetic risk, the A1c level, a measurement
of one’s average blood sugar level, should be known.
TYPE I (Juvenile)• A1c less than 9 ............................................................. Standard• All Others ..........................................................................SR400
TYPE II (Adult Onset) Please see table below for other risk factors and degree of control guidelines
Diagnosed within the past year• Well controlled, no other risk factors, no insulin .............. Select• Adequately controlled, or use of insulin,
no other risk factors ................................................ Standard• Poorly controlled, or other risk factor(s) ...........................SR400
Diagnosed between 1 and 10 years ago• A1c, Blood Pressure, and Lipids all well controlled,
no other risk factorsand if insulin - under 25 units .................................... Premier
• A1c, Blood Pressure, and Lipids adequately controlled,no other risk factors,and if insulin -under 75 units ....................................... Select
• A1c, Blood Pressure, or Lipids not adequatelycontrolled and/or insulin - over 75 units ................. Standard
Diagnosed between 10 and 15 years ago• A1c under 7, Blood Pressure and Lipids
adequately controlled, no other risk factors,and if insulin - under 75 units ....................................... Select
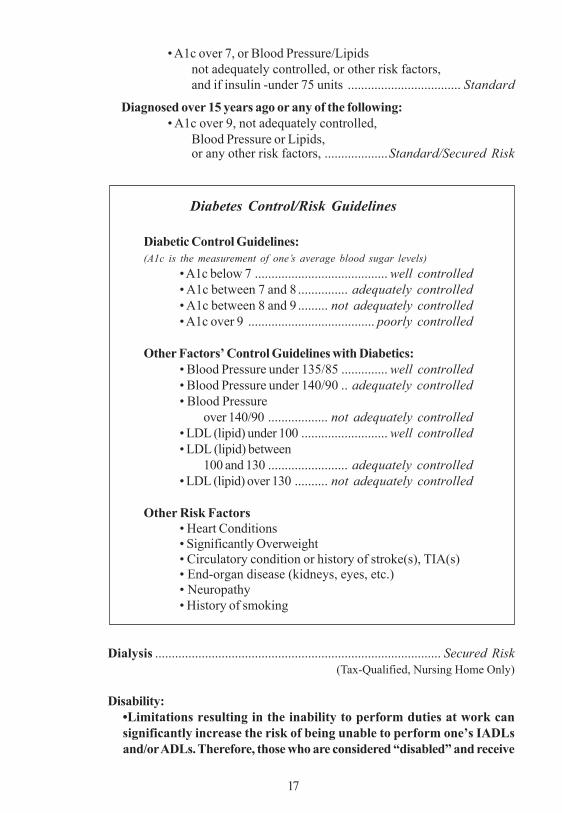
• A1c over 7, or Blood Pressure/Lipidsnot adequately controlled, or other risk factors,and if insulin -under 75 units .................................. Standard
Diagnosed over 15 years ago or any of the following:• A1c over 9, not adequately controlled,
Blood Pressure or Lipids,or any other risk factors, ...................Standard/Secured Risk
Diabetes Control/Risk Guidelines
Diabetic Control Guidelines:(A1c is the measurement of one’s average blood sugar levels)
• A1c below 7 ........................................ well controlled• A1c between 7 and 8 ............... adequately controlled• A1c between 8 and 9 ......... not adequately controlled• A1c over 9 ...................................... poorly controlled
Other Factors’ Control Guidelines with Diabetics:• Blood Pressure under 135/85 .............. well controlled• Blood Pressure under 140/90 .. adequately controlled• Blood Pressure
over 140/90 .................. not adequately controlled• LDL (lipid) under 100 .......................... well controlled• LDL (lipid) between
100 and 130 ........................ adequately controlled• LDL (lipid) over 130 .......... not adequately controlled
Other Risk Factors• Heart Conditions• Significantly Overweight• Circulatory condition or history of stroke(s), TIA(s)• End-organ disease (kidneys, eyes, etc.)• Neuropathy• History of smoking
Dialysis ...................................................................................... Secured Risk (Tax-Qualified, Nursing Home Only)
Disability:•Limitations resulting in the inability to perform duties at work cansignificantly increase the risk of being unable to perform one’s IADLsand/or ADLs. Therefore, those who are considered “disabled” and receive
17
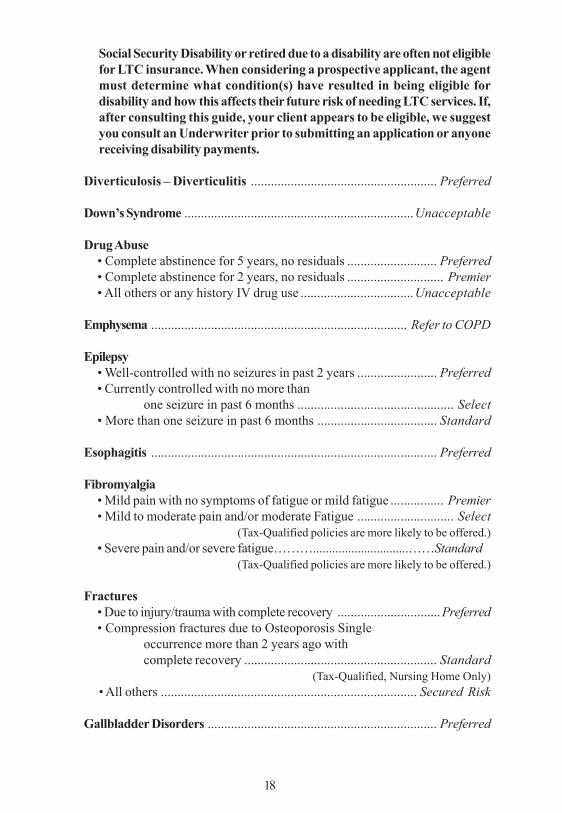
Social Security Disability or retired due to a disability are often not eligiblefor LTC insurance. When considering a prospective applicant, the agentmust determine what condition(s) have resulted in being eligible fordisability and how this affects their future risk of needing LTC services. If,after consulting this guide, your client appears to be eligible, we suggestyou consult an Underwriter prior to submitting an application or anyonereceiving disability payments.
Diverticulosis – Diverticulitis ........................................................ Preferred
Down’s Syndrome .....................................................................Unacceptable
Drug Abuse• Complete abstinence for 5 years, no residuals ........................... Preferred• Complete abstinence for 2 years, no residuals ............................. Premier• All others or any history IV drug use ..................................Unacceptable
Emphysema ............................................................................. Refer to COPD
Epilepsy• Well-controlled with no seizures in past 2 years ........................ Preferred• Currently controlled with no more than
one seizure in past 6 months ............................................... Select• More than one seizure in past 6 months .................................... Standard
Esophagitis ...................................................................................... Preferred
Fibromyalgia• Mild pain with no symptoms of fatigue or mild fatigue ................ Premier• Mild to moderate pain and/or moderate Fatigue ............................. Select
(Tax-Qualified policies are more likely to be offered.)• Severe pain and/or severe fatigue………..............................……Standard
(Tax-Qualified policies are more likely to be offered.)
Fractures• Due to injury/trauma with complete recovery ...............................Preferred• Compression fractures due to Osteoporosis Single
occurrence more than 2 years ago withcomplete recovery .......................................................... Standard
(Tax-Qualified, Nursing Home Only)• All others ............................................................................. Secured Risk
Gallbladder Disorders ..................................................................... Preferred
18

Gastritis ........................................................................................... Preferred
Gaucher’s Disease .................................................................... Secured Risk
Glaucoma• Well controlled, stable with minimal vision loss ....................... Preferred• Poorly controlled or unstable with minimal vision loss .................. Select• Vision loss causing functional impairment .........................Unacceptable
Gout ................................................................................................. Preferred
Graves Disease ................................................................................ Preferred
Guillain-Barre Syndrome• Full recovery, no residual weakness .......................................... Preferred• Post syndrome, with residual weakness ........ Select/Standard (TQ only)• Currently afflicted ...............................................................Unacceptable
Heart Disease and Disorders• No hospitalization or Single hospitalization
over 1 year ago, stable ..................................................... Premier• Single hospitalization in last 1 year, stable ..................................... Select• More than one hospitalization in past 1 year ............................ Standard
(Tax-Qualified, Nursing Home Only)Unless:• Cardiomyopathy
Without CHF (Congestive Heart Failure) or singleepisode of CHF in the past 2 years ......................... Standard
(Tax-Qualified, Nursing Home Only)All others ................................................................. Secured Risk
(Tax-Qualified, Nursing Home Only)• Congestive Heart Failure
Single episode, surgically corrected, no treatmentin past 1 year (no Cardiomyopathy) .......................... Premier
Single episode, hospitalized within past 1 year,currently stable, controlled with medications(no Cardiomyopathy) ................................................... Select
Single episode with Cardiomyopathy ............................ StandardAll others ................................................................. Secured Risk
• Atrial FibrillationSingle episode, more than 1 year ago ............................... PremierMore than one episode or episode in past 1 year ago ........ Select
Note: Combinations of conditions are always important, particularly with HeartConditions. Heart Conditions in combination with conditions such as diabetes,Hypertension, Obesity or Circulatory Disorders is likely to result in a higherrating than listed above.
19
20
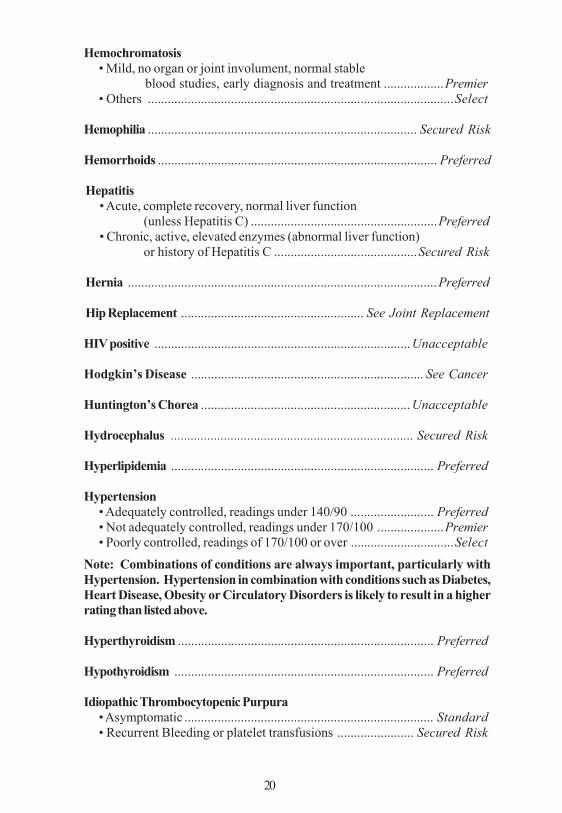
Hemochromatosis• Mild, no organ or joint involument, normal stable
blood studies, early diagnosis and treatment ..................Premier• Others ............................................................................................Select
Hemophilia ................................................................................. Secured Risk
Hemorrhoids .................................................................................... Preferred
Hepatitis• Acute, complete recovery, normal liver function
(unless Hepatitis C) ........................................................Preferred• Chronic, active, elevated enzymes (abnormal liver function)
or history of Hepatitis C ...........................................Secured Risk
Hernia .............................................................................................Preferred
Hip Replacement ....................................................... See Joint Replacement
HIV positive .............................................................................Unacceptable
Hodgkin’s Disease ...................................................................... See Cancer
Huntington’s Chorea ............................................................... Unacceptable
Hydrocephalus ......................................................................... Secured Risk
Hyperlipidemia ............................................................................... Preferred
Hypertension• Adequately controlled, readings under 140/90 ......................... Preferred• Not adequately controlled, readings under 170/100 ....................Premier• Poorly controlled, readings of 170/100 or over ...............................Select
Note: Combinations of conditions are always important, particularly withHypertension. Hypertension in combination with conditions such as Diabetes,Heart Disease, Obesity or Circulatory Disorders is likely to result in a higherrating than listed above.
Hyperthyroidism ............................................................................. Preferred
Hypothyroidism .............................................................................. Preferred
Idiopathic Thrombocytopenic Purpura• Asymptomatic ........................................................................... Standard• Recurrent Bleeding or platelet transfusions ....................... Secured Risk
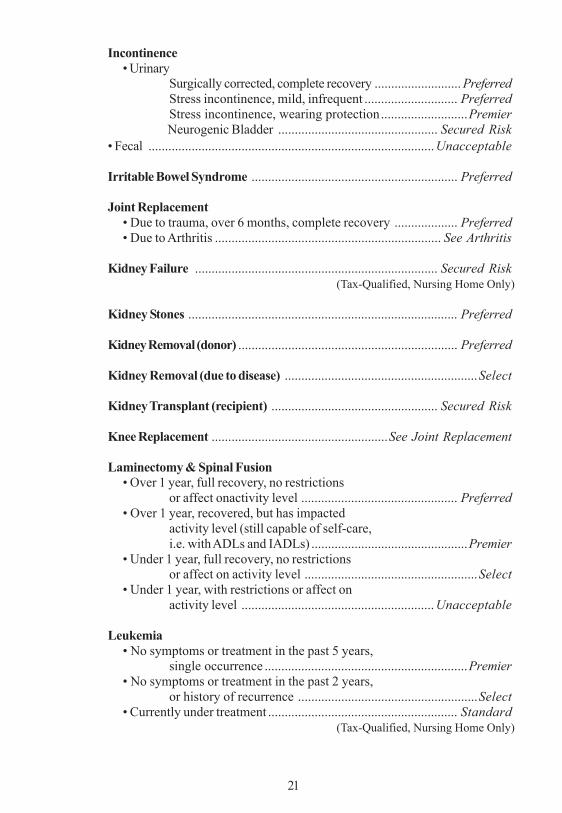
Incontinence• Urinary
Surgically corrected, complete recovery .......................... PreferredStress incontinence, mild, infrequent ............................ PreferredStress incontinence, wearing protection..........................PremierNeurogenic Bladder ................................................ Secured Risk
• Fecal ......................................................................................Unacceptable
Irritable Bowel Syndrome .............................................................. Preferred
Joint Replacement• Due to trauma, over 6 months, complete recovery ................... Preferred• Due to Arthritis .................................................................... See Arthritis
Kidney Failure ......................................................................... Secured Risk (Tax-Qualified, Nursing Home Only)
Kidney Stones ................................................................................. Preferred
Kidney Removal (donor) .................................................................. Preferred
Kidney Removal (due to disease) ..........................................................Select
Kidney Transplant (recipient) .................................................. Secured Risk
Knee Replacement .....................................................See Joint Replacement
Laminectomy & Spinal Fusion• Over 1 year, full recovery, no restrictions
or affect onactivity level ............................................... Preferred• Over 1 year, recovered, but has impacted
activity level (still capable of self-care,i.e. with ADLs and IADLs) ...............................................Premier
• Under 1 year, full recovery, no restrictionsor affect on activity level ....................................................Select
• Under 1 year, with restrictions or affect onactivity level .......................................................... Unacceptable
Leukemia• No symptoms or treatment in the past 5 years,
single occurrence .............................................................Premier• No symptoms or treatment in the past 2 years,
or history of recurrence ......................................................Select• Currently under treatment ......................................................... Standard
(Tax-Qualified, Nursing Home Only)
21
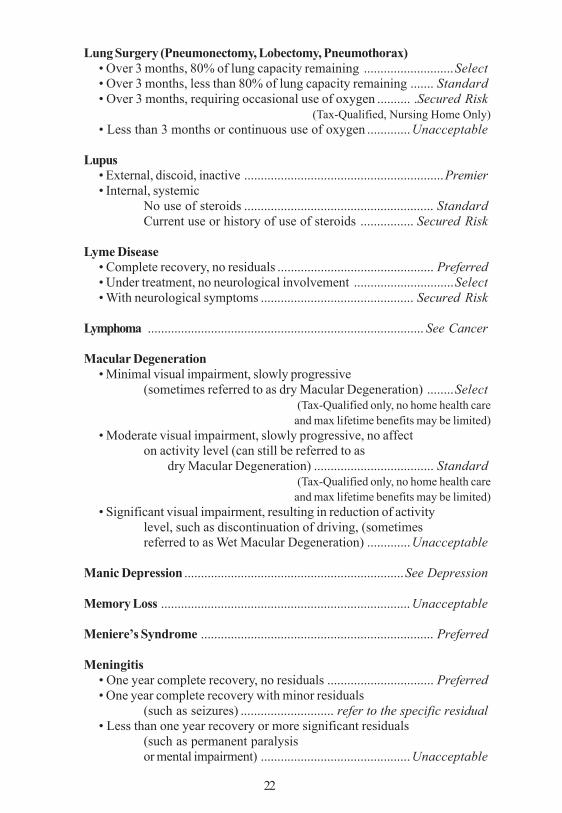
Lung Surgery (Pneumonectomy, Lobectomy, Pneumothorax)• Over 3 months, 80% of lung capacity remaining ...........................Select• Over 3 months, less than 80% of lung capacity remaining ....... Standard• Over 3 months, requiring occasional use of oxygen .......... .Secured Risk
(Tax-Qualified, Nursing Home Only)• Less than 3 months or continuous use of oxygen .............Unacceptable
Lupus• External, discoid, inactive ............................................................Premier• Internal, systemic
No use of steroids ......................................................... StandardCurrent use or history of use of steroids ................ Secured Risk
Lyme Disease• Complete recovery, no residuals ............................................... Preferred• Under treatment, no neurological involvement ..............................Select• With neurological symptoms .............................................. Secured Risk
Lymphoma ................................................................................... See Cancer
Macular Degeneration• Minimal visual impairment, slowly progressive
(sometimes referred to as dry Macular Degeneration) ........Select(Tax-Qualified only, no home health care
and max lifetime benefits may be limited)• Moderate visual impairment, slowly progressive, no affect
on activity level (can still be referred to asdry Macular Degeneration) .................................... Standard
(Tax-Qualified only, no home health careand max lifetime benefits may be limited)
• Significant visual impairment, resulting in reduction of activitylevel, such as discontinuation of driving, (sometimesreferred to as Wet Macular Degeneration) .............Unacceptable
Manic Depression ..................................................................See Depression
Memory Loss ........................................................................... Unacceptable
Meniere’s Syndrome ...................................................................... Preferred
Meningitis• One year complete recovery, no residuals ................................ Preferred• One year complete recovery with minor residuals
(such as seizures) ............................ refer to the specific residual• Less than one year recovery or more significant residuals
(such as permanent paralysisor mental impairment) ............................................. Unacceptable
22

Multiple Sclerosis ..................................................................... Secured Risk
Muscular Dystrophy ................................................................ Unacceptable
Myasthenia Gravis ..................................................................... Secured Risk
Nephrectomy ......................................... See Kidney Removal/Kidney Donor
Nephritis• Acute, no renal failure ................................................................ Preferred• Chronic .......................................... rate according to cause of condition
Neuralgia• Acute, mild ................................................................................ Preferred• Chronic (such as Diabetic, Peripheral, Alcoholic), but mild ............ Select• Chronic and severe or affecting activity level ........................... Standard
Neurofibromatosis ........................................................................... Standard (Tax-Qualified, Nursing Home Only)
Neurogenic Bladder ........................................................... See Incontinence
Obsessive Compulsive Disorder• No medications, does not affect activity level ........................... Preferred• Controlled with medications, does not affect
with activity level ......................................................... Select• All others ........................................................................... Unacceptable
Obesity ................................................................................ See Weight Chart
Organ Transplants• One year, complete recovery, no complications,
condition stable ....................................................... Secured Risk
Organic Brain Syndrome ........................................................ Unacceptable
Osteomyelitis• One year, complete recovery ..................................................... Preferred• Within last year, no longer being treated and no residuals ......... Premier• Currently being treated ........................................................ Secured Risk
Osteoporosis• Minor loss of bone density, has not contributed to
any fractures,may be being treated withmedications such as Fosamax or Didronelor with Calcium supplements ........................................... Premier
23
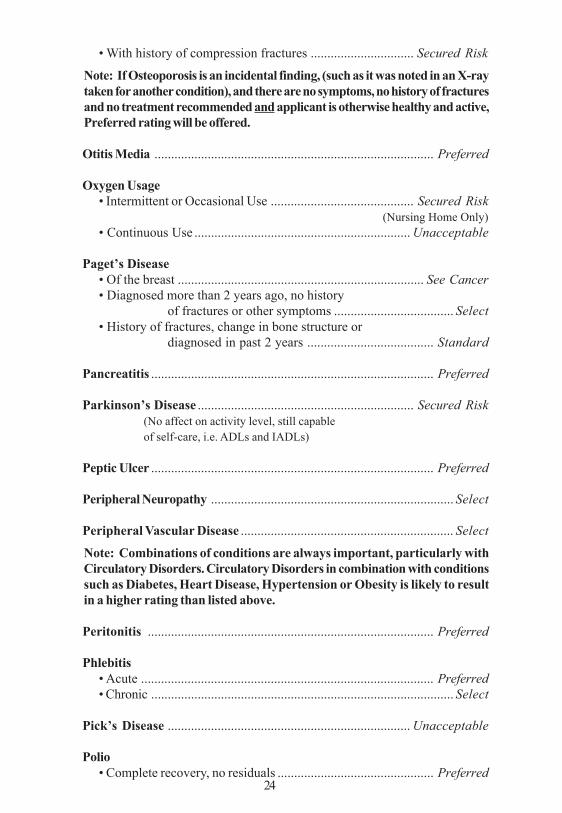
• With history of compression fractures ............................... Secured Risk
Note: If Osteoporosis is an incidental finding, (such as it was noted in an X-raytaken for another condition), and there are no symptoms, no history of fracturesand no treatment recommended and applicant is otherwise healthy and active,Preferred rating will be offered.
Otitis Media .................................................................................... Preferred
Oxygen Usage• Intermittent or Occasional Use ........................................... Secured Risk
(Nursing Home Only)• Continuous Use ................................................................. Unacceptable
Paget’s Disease• Of the breast .......................................................................... See Cancer• Diagnosed more than 2 years ago, no history
of fractures or other symptoms .................................... Select• History of fractures, change in bone structure or
diagnosed in past 2 years ...................................... Standard
Pancreatitis ..................................................................................... Preferred
Parkinson’s Disease ................................................................. Secured Risk(No affect on activity level, still capableof self-care, i.e. ADLs and IADLs)
Peptic Ulcer ..................................................................................... Preferred
Peripheral Neuropathy ......................................................................... Select
Peripheral Vascular Disease ................................................................ Select
Note: Combinations of conditions are always important, particularly withCirculatory Disorders. Circulatory Disorders in combination with conditionssuch as Diabetes, Heart Disease, Hypertension or Obesity is likely to resultin a higher rating than listed above.
Peritonitis ...................................................................................... Preferred
Phlebitis• Acute ........................................................................................ Preferred• Chronic ........................................................................................... Select
Pick’s Disease ......................................................................... Unacceptable
Polio• Complete recovery, no residuals ............................................... Preferred
24
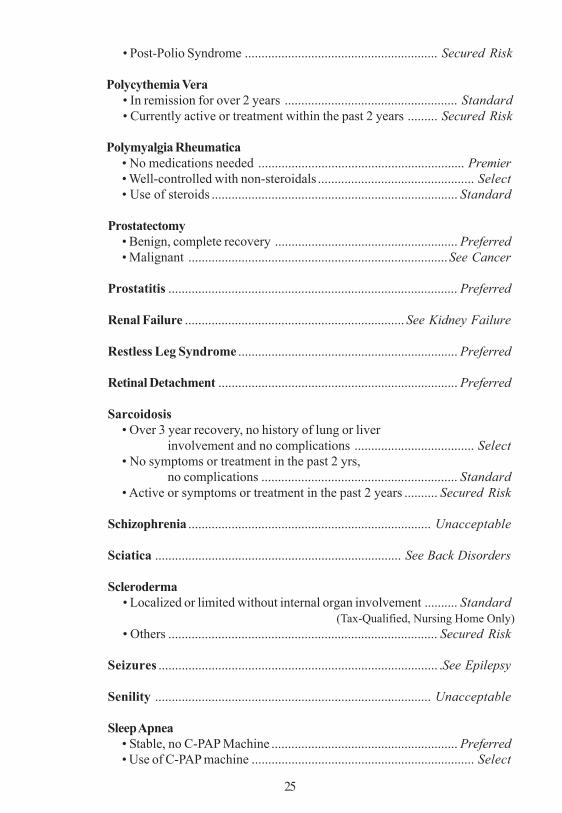
• Post-Polio Syndrome .......................................................... Secured Risk
Polycythemia Vera• In remission for over 2 years .................................................... Standard• Currently active or treatment within the past 2 years ......... Secured Risk
Polymyalgia Rheumatica• No medications needed .............................................................. Premier• Well-controlled with non-steroidals ............................................... Select• Use of steroids .......................................................................... Standard
Prostatectomy• Benign, complete recovery ....................................................... Preferred• Malignant ..............................................................................See Cancer
Prostatitis ....................................................................................... Preferred
Renal Failure .................................................................. See Kidney Failure
Restless Leg Syndrome .................................................................. Preferred
Retinal Detachment ........................................................................ Preferred
Sarcoidosis• Over 3 year recovery, no history of lung or liver
involvement and no complications .................................... Select• No symptoms or treatment in the past 2 yrs,
no complications ........................................................... Standard• Active or symptoms or treatment in the past 2 years .......... Secured Risk
Schizophrenia ......................................................................... Unacceptable
Sciatica .......................................................................... See Back Disorders
Scleroderma• Localized or limited without internal organ involvement .......... Standard
(Tax-Qualified, Nursing Home Only)• Others ................................................................................. Secured Risk
Seizures .................................................................................... .See Epilepsy
Senility ................................................................................... Unacceptable
Sleep Apnea• Stable, no C-PAP Machine ........................................................ Preferred• Use of C-PAP machine ................................................................... Select
25
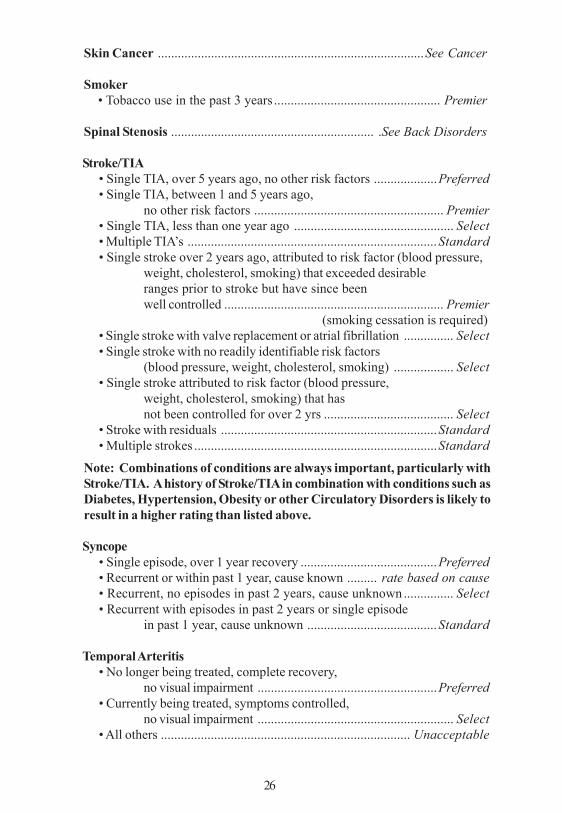
Skin Cancer ................................................................................See Cancer
Smoker• Tobacco use in the past 3 years .................................................. Premier
Spinal Stenosis ............................................................. .See Back Disorders
Stroke/TIA• Single TIA, over 5 years ago, no other risk factors ...................Preferred• Single TIA, between 1 and 5 years ago,
no other risk factors ......................................................... Premier• Single TIA, less than one year ago ................................................ Select• Multiple TIA’s ...........................................................................Standard• Single stroke over 2 years ago, attributed to risk factor (blood pressure,
weight, cholesterol, smoking) that exceeded desirableranges prior to stroke but have since beenwell controlled .................................................................. Premier
(smoking cessation is required)• Single stroke with valve replacement or atrial fibrillation ............... Select• Single stroke with no readily identifiable risk factors
(blood pressure, weight, cholesterol, smoking) .................. Select• Single stroke attributed to risk factor (blood pressure,
weight, cholesterol, smoking) that hasnot been controlled for over 2 yrs ....................................... Select
• Stroke with residuals .................................................................Standard• Multiple strokes .........................................................................Standard
Note: Combinations of conditions are always important, particularly withStroke/TIA. A history of Stroke/TIA in combination with conditions such asDiabetes, Hypertension, Obesity or other Circulatory Disorders is likely toresult in a higher rating than listed above.
Syncope• Single episode, over 1 year recovery .........................................Preferred• Recurrent or within past 1 year, cause known ......... rate based on cause• Recurrent, no episodes in past 2 years, cause unknown............... Select• Recurrent with episodes in past 2 years or single episode
in past 1 year, cause unknown .......................................Standard
Temporal Arteritis• No longer being treated, complete recovery,
no visual impairment ......................................................Preferred• Currently being treated, symptoms controlled,
no visual impairment ........................................................... Select• All others ........................................................................... Unacceptable
26
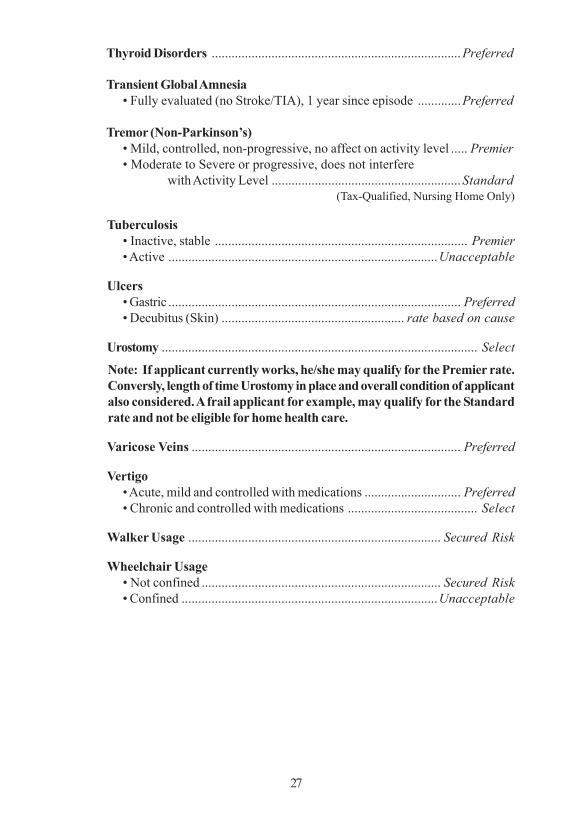
Thyroid Disorders ...........................................................................Preferred
Transient Global Amnesia• Fully evaluated (no Stroke/TIA), 1 year since episode .............Preferred
Tremor (Non-Parkinson’s)• Mild, controlled, non-progressive, no affect on activity level ..... Premier• Moderate to Severe or progressive, does not interfere
with Activity Level .........................................................Standard (Tax-Qualified, Nursing Home Only)
Tuberculosis• Inactive, stable ............................................................................ Premier• Active .................................................................................Unacceptable
Ulcers• Gastric ........................................................................................ Preferred• Decubitus (Skin) ....................................................... rate based on cause
Urostomy ............................................................................................... Select
Note: If applicant currently works, he/she may qualify for the Premier rate.Conversly, length of time Urostomy in place and overall condition of applicantalso considered. A frail applicant for example, may qualify for the Standardrate and not be eligible for home health care.
Varicose Veins ................................................................................. Preferred
Vertigo• Acute, mild and controlled with medications ............................. Preferred• Chronic and controlled with medications ....................................... Select
Walker Usage ............................................................................ Secured Risk
Wheelchair Usage• Not confined ........................................................................ Secured Risk• Confined .............................................................................Unacceptable
27
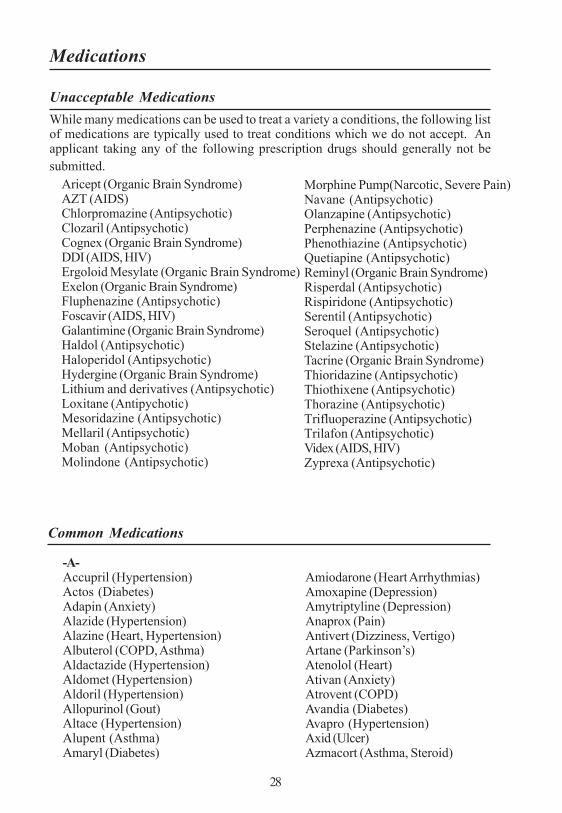
Medications
Unacceptable MedicationsWhile many medications can be used to treat a variety a conditions, the following listof medications are typically used to treat conditions which we do not accept. Anapplicant taking any of the following prescription drugs should generally not besubmitted.
-A-Accupril (Hypertension)Actos (Diabetes)Adapin (Anxiety)Alazide (Hypertension)Alazine (Heart, Hypertension)Albuterol (COPD, Asthma)Aldactazide (Hypertension)Aldomet (Hypertension)Aldoril (Hypertension)Allopurinol (Gout)Altace (Hypertension)Alupent (Asthma)Amaryl (Diabetes)
Common Medications
Amiodarone (Heart Arrhythmias)Amoxapine (Depression)Amytriptyline (Depression)Anaprox (Pain)Antivert (Dizziness, Vertigo)Artane (Parkinson’s)Atenolol (Heart)Ativan (Anxiety)Atrovent (COPD)Avandia (Diabetes)Avapro (Hypertension)Axid (Ulcer)Azmacort (Asthma, Steroid)
28
Morphine Pump(Narcotic, Severe Pain)Navane (Antipsychotic)Olanzapine (Antipsychotic)Perphenazine (Antipsychotic)Phenothiazine (Antipsychotic)Quetiapine (Antipsychotic)Reminyl (Organic Brain Syndrome)Risperdal (Antipsychotic)Rispiridone (Antipsychotic)Serentil (Antipsychotic)Seroquel (Antipsychotic)Stelazine (Antipsychotic)Tacrine (Organic Brain Syndrome)Thioridazine (Antipsychotic)Thiothixene (Antipsychotic)Thorazine (Antipsychotic)Trifluoperazine (Antipsychotic)Trilafon (Antipsychotic)Videx (AIDS, HIV)Zyprexa (Antipsychotic)
Aricept (Organic Brain Syndrome)AZT (AIDS)Chlorpromazine (Antipsychotic)Clozaril (Antipsychotic)Cognex (Organic Brain Syndrome)DDI (AIDS, HIV)Ergoloid Mesylate (Organic Brain Syndrome)Exelon (Organic Brain Syndrome)Fluphenazine (Antipsychotic)Foscavir (AIDS, HIV)Galantimine (Organic Brain Syndrome)Haldol (Antipsychotic)Haloperidol (Antipsychotic)Hydergine (Organic Brain Syndrome)Lithium and derivatives (Antipsychotic)Loxitane (Antipychotic)Mesoridazine (Antipsychotic)Mellaril (Antipsychotic)Moban (Antipsychotic)Molindone (Antipsychotic)

-B-Baclofen (Spasm, Multiple Sclerosis)Beclovent (Asthma, Steroid)Beconase (Asthma, Steroid)Brethine (Asthma, COPD)Bumex (Hypertension, Edema)Buspar (Anxiety)
C-Calan (Heart)Calcimar (Osteoporosis)Capoten (Hypertension)Capozide (Hypertension)Captopril (Hypertension)Carbidopa (Parkinson’s)Cardizem (Heart, Hypertension)Cardura (Hypertension)Casodex (Cancer/Prostate)Catapres (Hypertension)Celebrex (Arthritis)Centrax (Anxiety)Clinoril (Arthritis)Clonazepam (Seizures)Corgord (Heart, Hypertension)Coumadin (Blood Thinner)Cozaar (Hypertension)
-D-Darvocet (Pain)DepoProvera (Cancer)Desyrel (Depression)Diabenese (Diabetes)Diabeta (Diabetes)Didronel (Osteoporosis, Pagets
Disease)Digoxin (Heart Rhythym)Dilantin (Epilepsy)Diltiazem (Heart, Hypertension)Ditropan (Incontinence)Dypyridamole (Circulation, Stroke)Diuril (Hypertension)Dyazide (Hypertension, Edema)
-E-Effexor (Depression)Elavil (Depression)
29
Eldepryl (Parkinson’s)Eulexin (Cancer/Prostate)
-F-Feldene (Arthritis)Flomax (Prostate)Flonase (Asthma, Steroid)Flovent (Asthma, Steroid)Fosomax (Osteoporosis)
-G-Glipizide (Diabetes)Glucophage (Diabetes)Glyburide (Diabetes)Gold (Rheumatoid Arthritis)
-H-HCTZ (Hypertension)Heparin (Blood Thinner)Hytrin (Hypertension)
-I-Imuran (Cancer)Imipramine (Anxiety)Inderal (Heart, Hypertension)Indocin (Arthritis)Insulin (Diabetes)Isoptin (Heart)Isordil (Angina, Heart)
-K-K-lor (Hypertension)Kaochlor (Hypertension)Kaon (Hypertension)Klonopin (Seizures)
-L-Lanoxin (Heart)Lasix (Edema, Hypertension)Laquenil (Arthritis)Levodopa (Parkinson’s)Librax (Anxiety)Librium (Anxiety)Lipitor (Cholesterol)Lopressor (Hypertension)Lorazepam (Anxiety)
Common Medications (contiued)
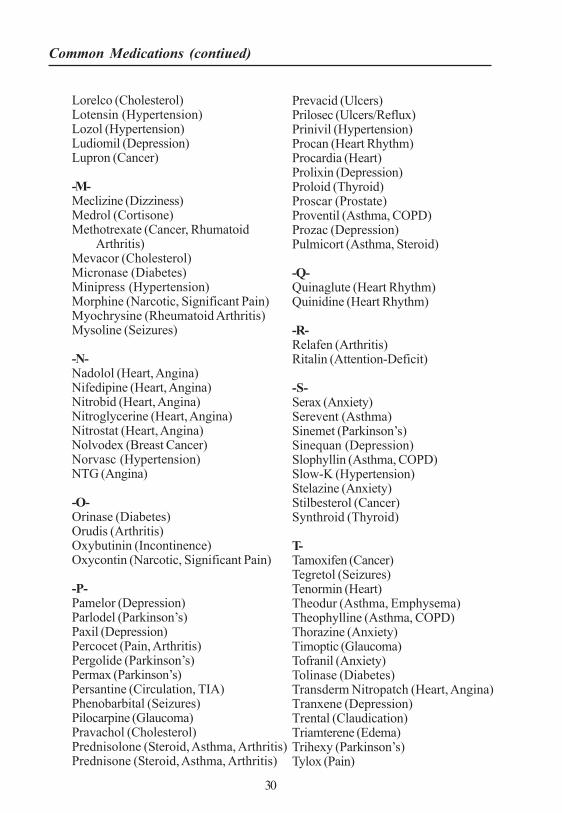
Lorelco (Cholesterol)Lotensin (Hypertension)Lozol (Hypertension)Ludiomil (Depression)Lupron (Cancer)
-M-Meclizine (Dizziness)Medrol (Cortisone)Methotrexate (Cancer, Rhumatoid
Arthritis)Mevacor (Cholesterol)Micronase (Diabetes)Minipress (Hypertension)Morphine (Narcotic, Significant Pain)Myochrysine (Rheumatoid Arthritis)Mysoline (Seizures)
-N-Nadolol (Heart, Angina)Nifedipine (Heart, Angina)Nitrobid (Heart, Angina)Nitroglycerine (Heart, Angina)Nitrostat (Heart, Angina)Nolvodex (Breast Cancer)Norvasc (Hypertension)NTG (Angina)
-O-Orinase (Diabetes)Orudis (Arthritis)Oxybutinin (Incontinence)Oxycontin (Narcotic, Significant Pain)
-P-Pamelor (Depression)Parlodel (Parkinson’s)Paxil (Depression)Percocet (Pain, Arthritis)Pergolide (Parkinson’s)Permax (Parkinson’s)Persantine (Circulation, TIA)Phenobarbital (Seizures)Pilocarpine (Glaucoma)Pravachol (Cholesterol)Prednisolone (Steroid, Asthma, Arthritis)Prednisone (Steroid, Asthma, Arthritis)
Prevacid (Ulcers)Prilosec (Ulcers/Reflux)Prinivil (Hypertension)Procan (Heart Rhythm)Procardia (Heart)Prolixin (Depression)Proloid (Thyroid)Proscar (Prostate)Proventil (Asthma, COPD)Prozac (Depression)Pulmicort (Asthma, Steroid)
-Q-Quinaglute (Heart Rhythm)Quinidine (Heart Rhythm)
-R-Relafen (Arthritis)Ritalin (Attention-Deficit)
-S-Serax (Anxiety)Serevent (Asthma)Sinemet (Parkinson’s)Sinequan (Depression)Slophyllin (Asthma, COPD)Slow-K (Hypertension)Stelazine (Anxiety)Stilbesterol (Cancer)Synthroid (Thyroid)
T-Tamoxifen (Cancer)Tegretol (Seizures)Tenormin (Heart)Theodur (Asthma, Emphysema)Theophylline (Asthma, COPD)Thorazine (Anxiety)Timoptic (Glaucoma)Tofranil (Anxiety)Tolinase (Diabetes)Transderm Nitropatch (Heart, Angina)Tranxene (Depression)Trental (Claudication)Triamterene (Edema)Trihexy (Parkinson’s)Tylox (Pain)
30
Common Medications (contiued)
31
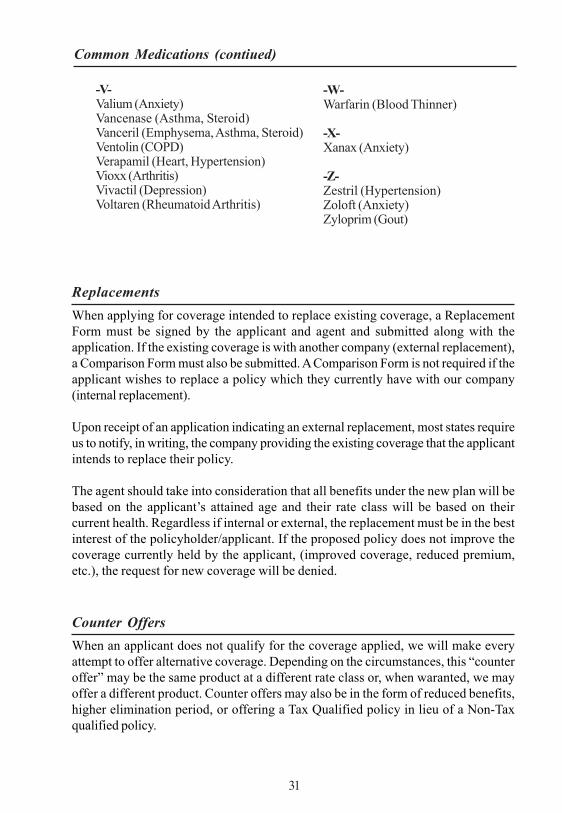
ReplacementsWhen applying for coverage intended to replace existing coverage, a ReplacementForm must be signed by the applicant and agent and submitted along with theapplication. If the existing coverage is with another company (external replacement),a Comparison Form must also be submitted. A Comparison Form is not required if theapplicant wishes to replace a policy which they currently have with our company(internal replacement).
Upon receipt of an application indicating an external replacement, most states requireus to notify, in writing, the company providing the existing coverage that the applicantintends to replace their policy.
The agent should take into consideration that all benefits under the new plan will bebased on the applicant’s attained age and their rate class will be based on theircurrent health. Regardless if internal or external, the replacement must be in the bestinterest of the policyholder/applicant. If the proposed policy does not improve thecoverage currently held by the applicant, (improved coverage, reduced premium,etc.), the request for new coverage will be denied.
Counter OffersWhen an applicant does not qualify for the coverage applied, we will make everyattempt to offer alternative coverage. Depending on the circumstances, this “counteroffer” may be the same product at a different rate class or, when waranted, we mayoffer a different product. Counter offers may also be in the form of reduced benefits,higher elimination period, or offering a Tax Qualified policy in lieu of a Non-Taxqualified policy.
-V-Valium (Anxiety)Vancenase (Asthma, Steroid)Vanceril (Emphysema, Asthma, Steroid)Ventolin (COPD)Verapamil (Heart, Hypertension)Vioxx (Arthritis)Vivactil (Depression)Voltaren (Rheumatoid Arthritis)
-W-Warfarin (Blood Thinner)
-X-Xanax (Anxiety)
-Z-Zestril (Hypertension)Zoloft (Anxiety)Zyloprim (Gout)
Common Medications (contiued)

Once we determine that a counter offer is necessary, the agent is informed of theoffer. Often times there are several options in terms of which benefits best fit theclients needs and we therefore await the agent’s reply and instructions on specificallyhow the policy should be issued.
Although our ability to counter offer utilizing our variety of products and rate classesallows many policies to be placed which would otherwise be rejected, we realize thatplacing a count-offer is often times difficult. Many counter offers may be avoided bygood field underwriting and utilizing the Underwriting Guidelines in this book at timeof application. We also welcome pre-qualification calls, where the agent can speakdirectly to an Underwriter who will offer suggestions on how the application shouldbe submitted based on the information provided. As mentioned in the Introduction,the Underwriting Wizard can also assist you in rating an applicant appropriately.
Spousal DiscountThe States of Michigan, New Jersey, and South Dakota require the spousal discountto be applied to any policy where the applicant has a spouse, regardless of whetherthe spouse applies for or is issued coverage. In all other States, the spousal discountis applied to each policy when, together, both spouses apply for and are issuedcoverage.We also will apply the spousal discount to a policy if the applicant’s spouse is anexisting policyholder of ours. If the second spouse’s policy is issued within one yearof the first spouse’s policy, we will also apply the spousal discount to the firstspouse’s policy upon the next renewal date.
Please note that if one spouse cancels their coverage within the 30 day free examinationperiod, the spousal discount will be removed from the remaining spouse’s policy. Inthe event of death, however, the spousal discount will remain in effect on the survivingspouse’s policy.
Those eligible for the spousal discount include all legally married couples, includingsame sex marriages or common law marriages, according to the laws within the Stateof issuance. Those legal spouses who do not have the same last name should submitevidence, such as a notarized document or copy of a jointly filed tax return, provingtheir marital status.
ReissuesAll requests to change coverage received in our office within 30 days of policydelivery to the applicant, will be considered for Reissue. The request must clearlyindicate what changes are desired and must be signed by the policyholder. Thesechanges may be additional benefits, reduction of benefits, or change in policy form.Aside from reductions, none of these changes are guaranteed and therefore must bereviewed and approved by an Underwriter. Any such change, if approved, will be
32

made effective as of the effective date of the policy, and a new schedule page reflectingthe changes will be forwarded to the agent or policyholder.
Requests for changes to an existing policy which the policyholder has had more than30 days will not be processed as a reissue, but instead will be processed as an“Increase in Coverage” or “Decrease in Coverage” (please see below).
Increasing BenefitsThere are three ways a policyholder can add coverage to an existing policy with ourcompany:
1. Replace the existing policy with a new policy. The agent should take intoconsideration that all benefits under the new plan will be based on theapplicant’s attained age and must ensure that replacement is in thepolicyholder’s best interest. (Please see “Replacements” on page 31.)
2. Purchase a second policy to supplement the existing plan. Please notethat the total daily benefit allowed under all policies cumulatively maynot exceed the maximum daily benefit allowed under the policy beingpurchased.
3. Add benefits to the existing policy. “Add-ons” to daily benefit or maximumbenefit periods or amounts can only be made to those plans which arecurrently being marketed. These add-ons, if approved, will be based onthe policyholder’s attained age.
Regardless of which method is used to add coverage, the additional benefits will beUnderwritten and, in order to be considered, a completed application must besubmitted.
Decreasing BenefitsUnless required otherwise by your state, requests to reduce benefits will be honoredas of the policy’s next renewal date and must be submitted, in writing, and signed bythe policyholder. We cannot reduce benefits below our normal policy minimums. Norcan a policyholder delete the benefits provided by the base policy while maintainingbenefits provided by attached riders.
Underwriting AppealsAlthough it is in our interest to offer the best rate class available for each applicantbased on their individual circumstances, we understand that you, as the agent, andyour clients may not always agree with the Underwriting decision. We encourageyou to contact us and we will be happy to review such cases and wherever possible,
33

while maintaining the applicant’s privacy, discuss the reason(s) for our decision. Weare also happy to review any additional medical information including letters fromphysicians which may give us additional insight into an applicant’s health statusand/or risk factors.
Underwriting Class UpgradesWith certain acute conditions, the “time since recovery”, as indicated in the enclosedguidelines, is an important factor in determining the correct rate class. If, accordingto the Underwriting guidelines, an existing policyholder appears to qualify for abetter rating than originally issued, we will be happy to review a new application anddetermine if we can upgrade the policyholder to a better rating. If approved, anupgrade is generally not made prior to the policy being in force for one year and ismade effective on the policy’s next renewal date. Upgrades on existing benefits willbe based on the policyholder’s original issue age, while any increases in benefits(add-ons) are based on the policyholder’s attained age. We encourage agents tocontact the Underwriting Department prior to completing an application for Upgradein order to determine whether the policyholder may be eligible.
ReinstatementsReinstatements are processed in accordance with the Reinstatement provisionsdescribed within each policy. In general, we will consider reinstatement for a periodof six months following the policy’s renewal date. Upon receipt of a completedapplication (please use current new business application) and at least a quarterlypremium, we will review to determine if reinstatement is possible and notify theclient. If eligible, the premium will be applied and billing will resume accordingly. Ifnot eligible, the premium check will be returned directly to the client.
Effective DatesIn all States but New York, where the effective date of the policy is the date written (ifissued), the effective date of policies is the date issued, unless requested otherwiseby the agent/applicant. If requested, we will generally make the policy effective up tothirty days subsequent to issuance. If a later effective date is desired, we will considermaking effective up to sixty days after issuance if requested during Underwritingand upon receipt of a valid reason, such as replacement of an existing policy.
Saving AgeIn all states but New York, where the effective date of the policy is the date ofapplication, the issue age will generally correspond to the applicant’s age at time ofapplication, regardless of whether or not the applicant has a birthday following date
34
of application. If specifically requested by the applicant, we can “save age” of anapplicant who has had a birthday within 30 days prior to signing the application. Ifthe application is approved and when specifically requested, the effective date willprecede the applicant’s birthday by one day and the rates will be based on thisyounger age. We cannot save age of any applicant if their birthday preceded thesigning of the application by more than 30 days. All applications must be signed anddated on the actual date completed and should be received in our office within 2weeks of the date signed.
35
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
Agent Notes
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
Agent Notes