Peds lecture pt 2 (rev 5/12). PATH REVIEW (VOL3 pg 179) Congential: Club Foot & Hip Dysplasia...
59
Peds lecture pt 2 (rev 5/12)
-
Upload
ada-spencer -
Category
Documents
-
view
215 -
download
1
Transcript of Peds lecture pt 2 (rev 5/12). PATH REVIEW (VOL3 pg 179) Congential: Club Foot & Hip Dysplasia...
Peds lecture pt 2 (rev 5/12)
PATH REVIEW (VOL3 pg 179)
• Congential: Club Foot & Hip Dysplasia• Fractures: Greenstick, Torus or buckle• Hirschsprung’s (Megacolon)• INTUSSUSCEPTION• Hylaine Membrane Disease• CROUP• Osgood-Schlatters Disease• Pyloric Stenosis• Slipped Epiphysis • REFLUX• R/O FOREIGN BODY

IMAGING PEDS
• How does techniques• Differ from• ADULTS / CHILDREN• INFANTS
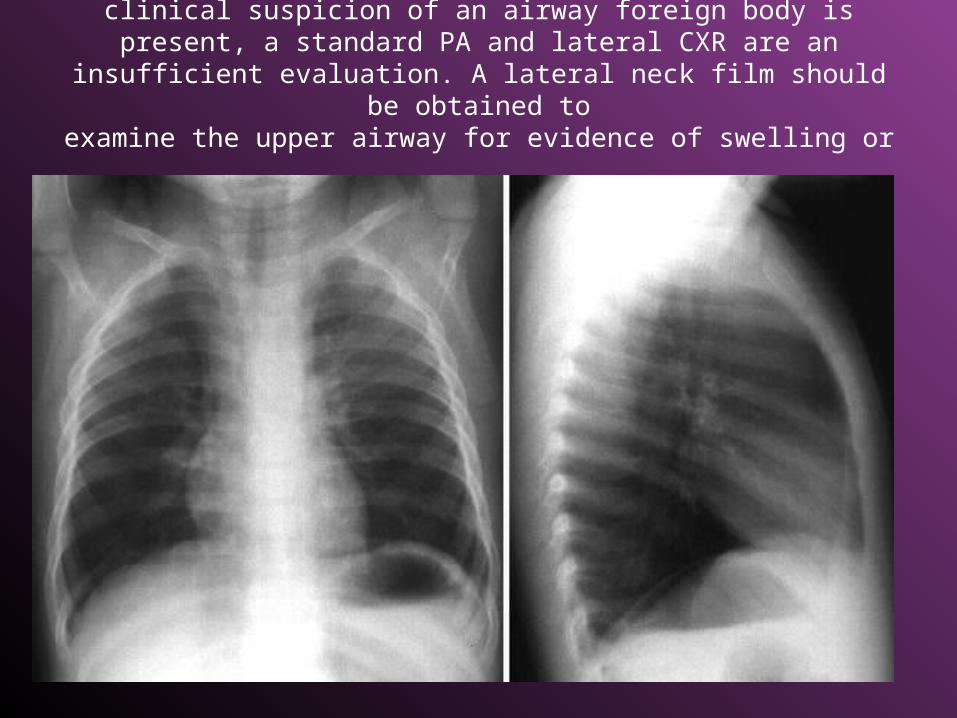
This CXR is within normal limits; however, when a clinical suspicion of an airway foreign body is present, a standard PA and lateral CXR are
an insufficient evaluation. A lateral neck film should be obtained to
examine the upper airway for evidence of swelling or foreign body.

RDS – Respiratory Distress

Hyaline Membrane Disease
• Acute pulmonary disorder of the newborn characterized by
• Generalized atelectasis
• Ventilation-perfusion abnormalities
• Reduced lung compliance
• M:F =1.8:1 – slightly more common in males

Hyaline Membrane Disease
• Cause • Immature surfactant
production • (usually begins at 18-20
weeks of gestational age) • CLINICAL SIGNS• Abnormal retraction of
chest wall • Cyanosis • Expiratory grunting • Increased respiratory rate

HyalineHyaline Membrane Disease Membrane Disease
• Predispositions • Premature infants • Cesarean section • Infants of diabetic mothers • Perinatal asphyxia • Onset
– Usually less than 2-5 hours after birth – Increases in severity from 24 to 48 hours – Then, gradual improvement after 48-72 hours

Hyaline Membrane Disease
Imaging findings • Typically, diffuse “ground-glass” opacification of both
lungs with air bronchograms and hypoaeration
• Hypoaeration from loss of lung volume (may be counteracted by respiratory therapy)
• Fine granular pattern • Prominent air bronchograms • Bilateral and symmetrical distribution • Prognosis • Spontaneous clearing within 7-10 days (mild course in
untreated survivors) • Death in 18%

Hyaline Membrane Disease
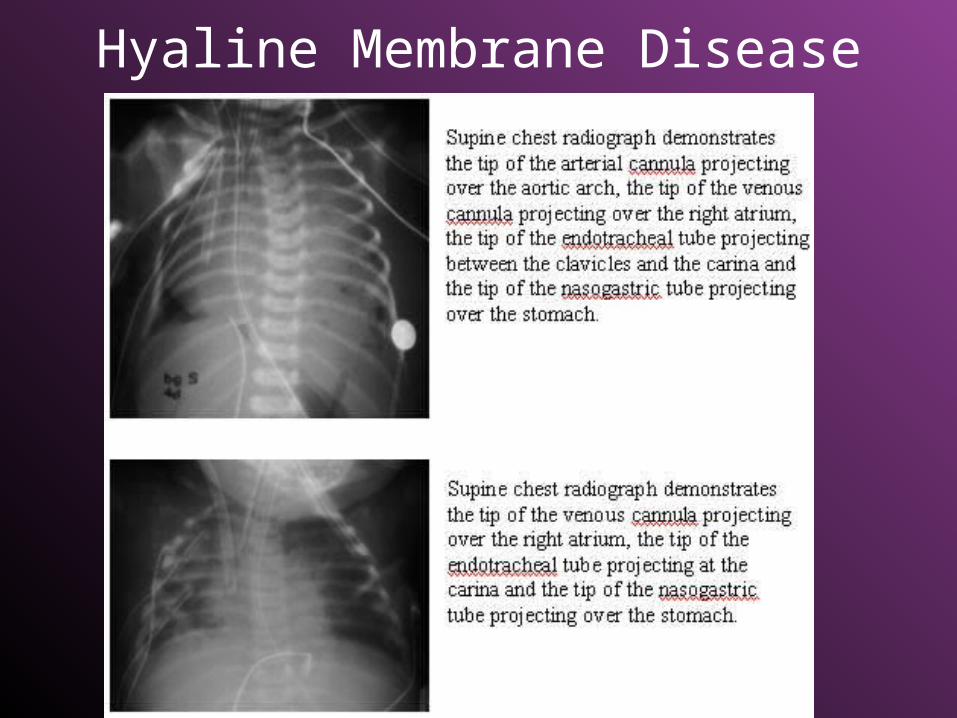
Hyaline Membrane Disease
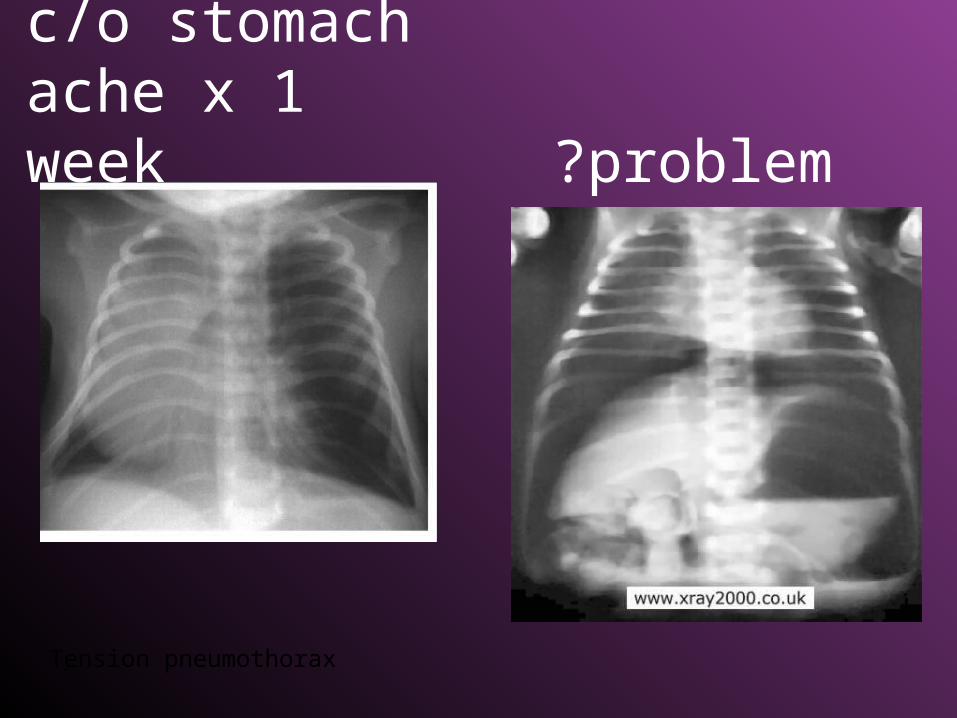
c/o stomach ache x 1 week ?problem
Tension pneumothorax

IniencephalyHistory:Newborn girl with short neck and head tilted up toward the sky. She died approximately 24 hours after birth due to multiple anomalies
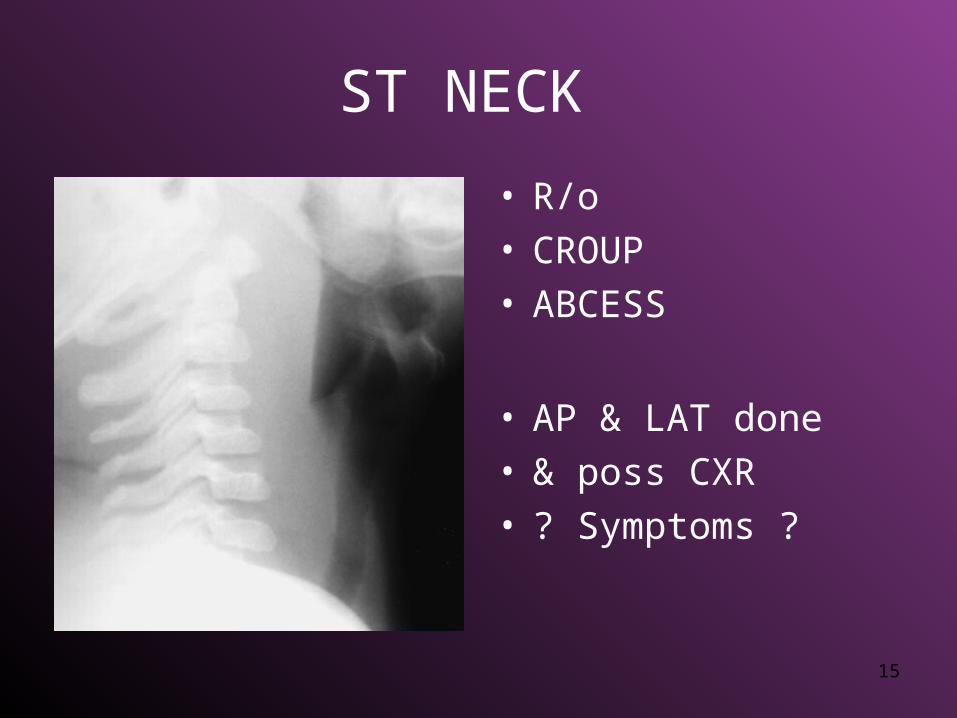
ST NECK
• R/o• CROUP• ABCESS
• AP & LAT done• & poss CXR• ? Symptoms ?
15

“BABYGRAM” FOR FB
From Mouth to Anus - AP & possible Lateral

• BLOCKER PLACEMENT
• GRID OR NO • GRID?


INTUSSUSCEPTION
A barium enema demonstrated an intussusception at the hepatic flexure which was successfully reduced

Intussuception Volvulus
20
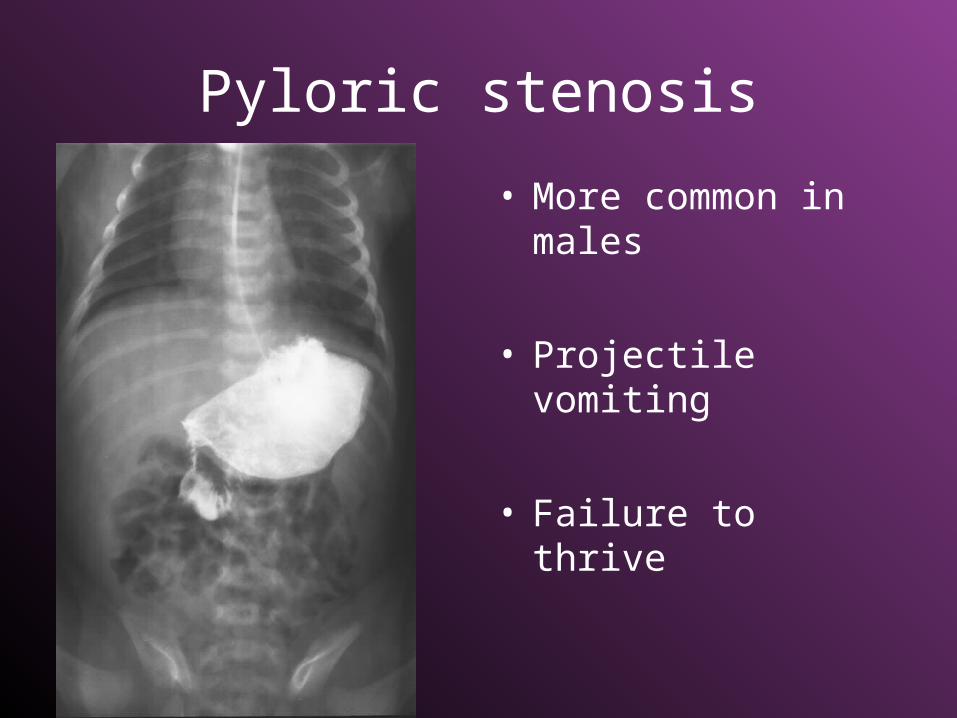
Pyloric stenosis
• More common in males
• Projectile vomiting
• Failure to thrive

ABSENCE OF DIAPHRAM
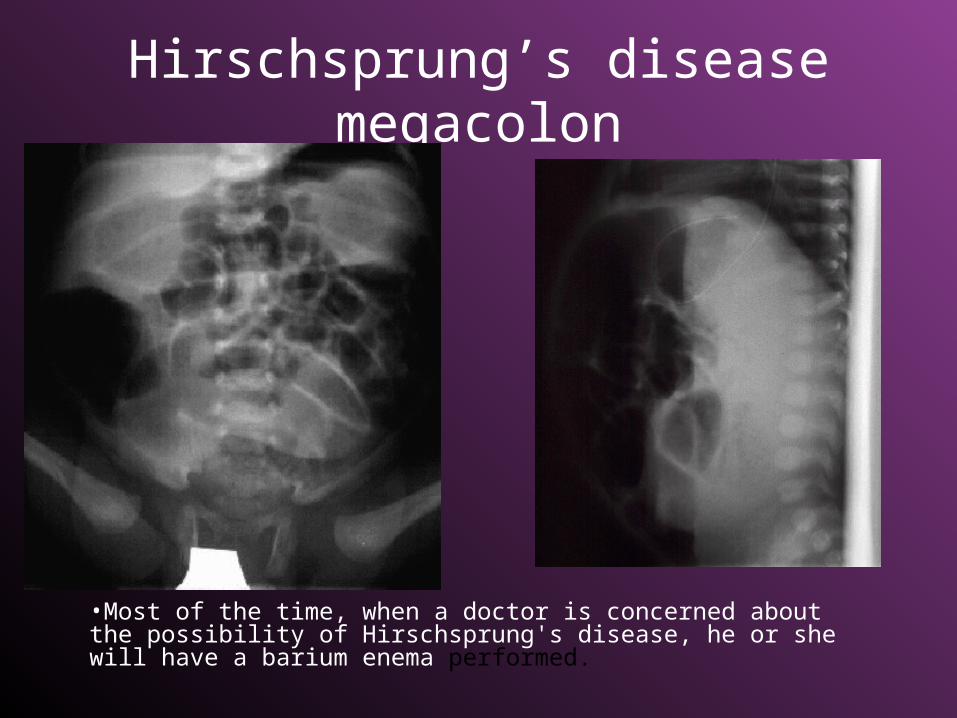
Hirschsprung’s diseasemegacolon
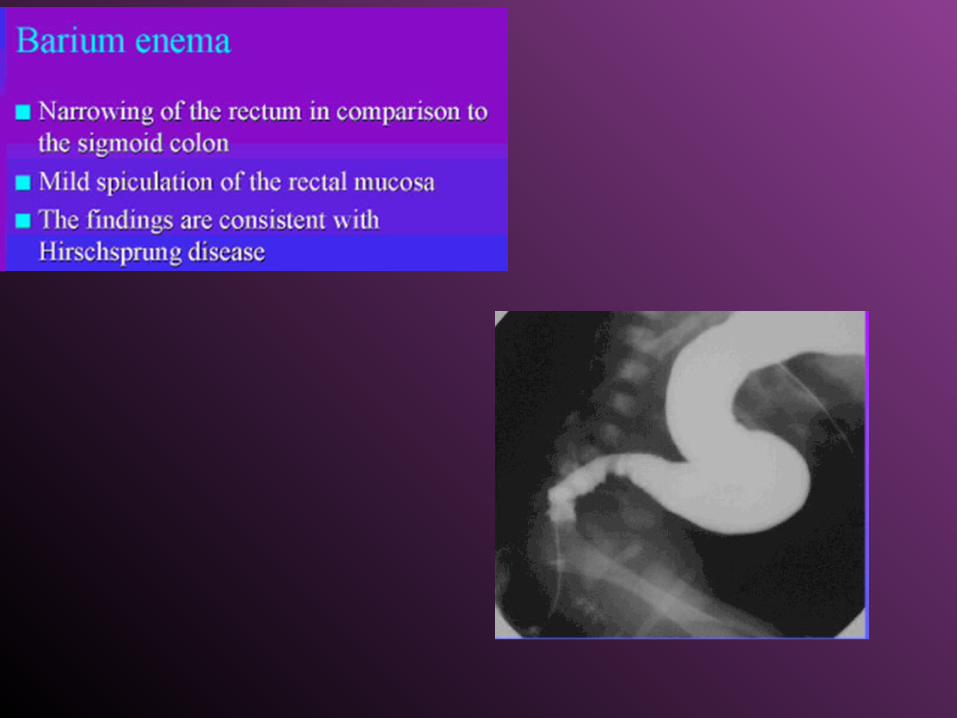
•Most of the time, when a doctor is concerned about the possibility of Hirschsprung's disease, he or she will have a barium enema performed.

• Hirschsprung's disease is a rare disorder occurring in about
• 1 out of every 5,000 to 10,000 newborn babies
• constipation occurs in as many as 1 out of every 5 to 10 children).
• This disease is much more common in boys than girls.
Hirschsprung’s diseasemegacolon
• Hirschsprung's disease is a blockage of the large intestine due to improper muscle movement in the bowel.
• It is a congenital condition, which means it is present from birth

• The intestine is constantly squeezed tight, preventing stool from passing.
• Almost all children with Hirschsprung's disease have problems with constipation from the day they are born; as many as half of babies with Hirschsprung's disease will not pass their first bowel movement during the first 36 hours of life
• There is currently no evidence to indicate that Hirschsprung's disease is caused by any medications or exposures to toxins during pregnancy.
• If a child has Hirschsprung's disease, some form of surgery is usually required to eliminate the problems with constipation.
Hirschsprung’s diseasemegacolon

Megacolon can also occur in adults
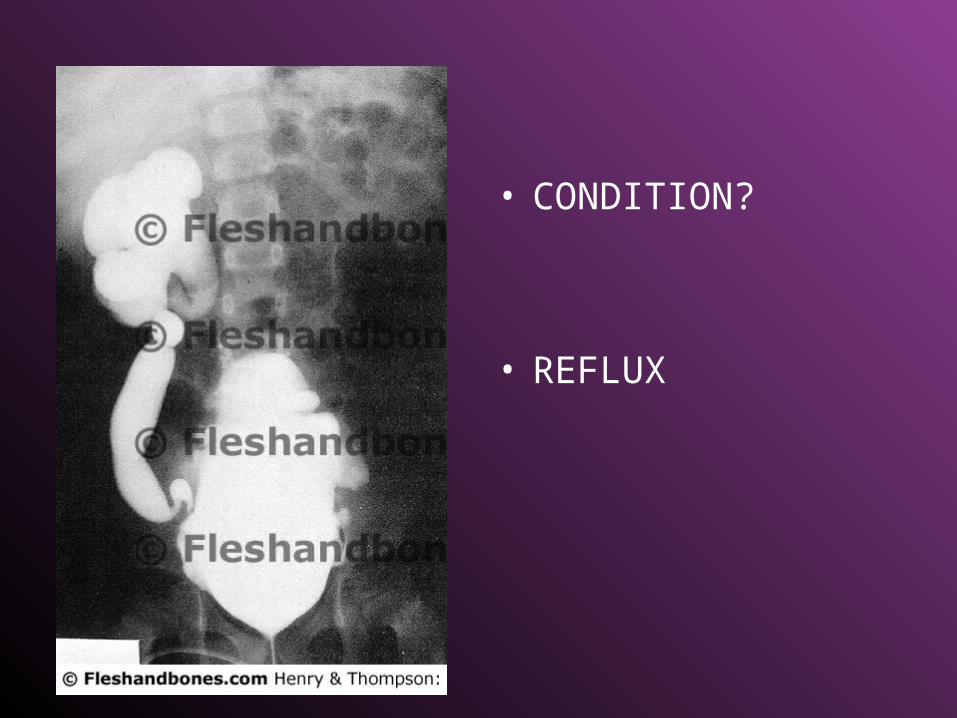
• CONDITION?
• REFLUX

• NOTE OPEN
JOINT SPACES
• DO NOT NEED ALL
PROJECTIONS AS DONE WITH ADULTS!
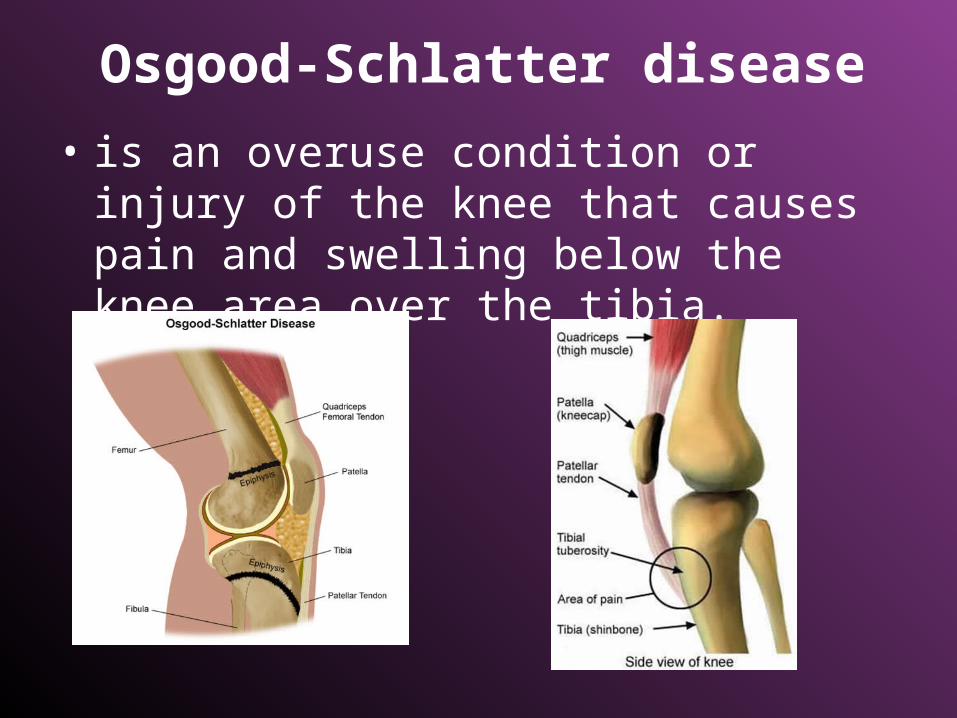
Osgood-Schlatter disease
• is an overuse condition or injury of the knee that causes pain and swelling below the knee area over the tibia.
Osgood-Schlatter disease
• Growth spurts can begin any time between the ages of 8-13 for girls and 10-15 for boys.
• OSD is most common in 11 to 14 y/o• OSD is more likely in teens who participate in
sports that involve running, twisting, and jumping, such as basketball, football, volleyball, soccer, tennis, figure skating, and gymnastics.
• With exercise, the muscles place increased stress on the growth plate

Osgood-Schlatter disease

FRACTURES IN CHILDREN
• GREENSTICK- • Incomplete fracture
• TORUS OR BUCKLE-• Impacted

POSITIONING FAT PADS

• 10 yo –• Pain no trauma
• Problem?
• These radiographs demonstrate a pathologic fracture through a bone cyst of the proximal humerus.



FRACTURES IN CHILDREN
• GREENSTICK• TORUS OR BUCKLE

FRACTURES IN CHILDREN
• GREENSTICK- /Incomplete• TORUS OR BUCKLE

Slipped Epiphysis• The head of femur dislocates into the
epiphysis
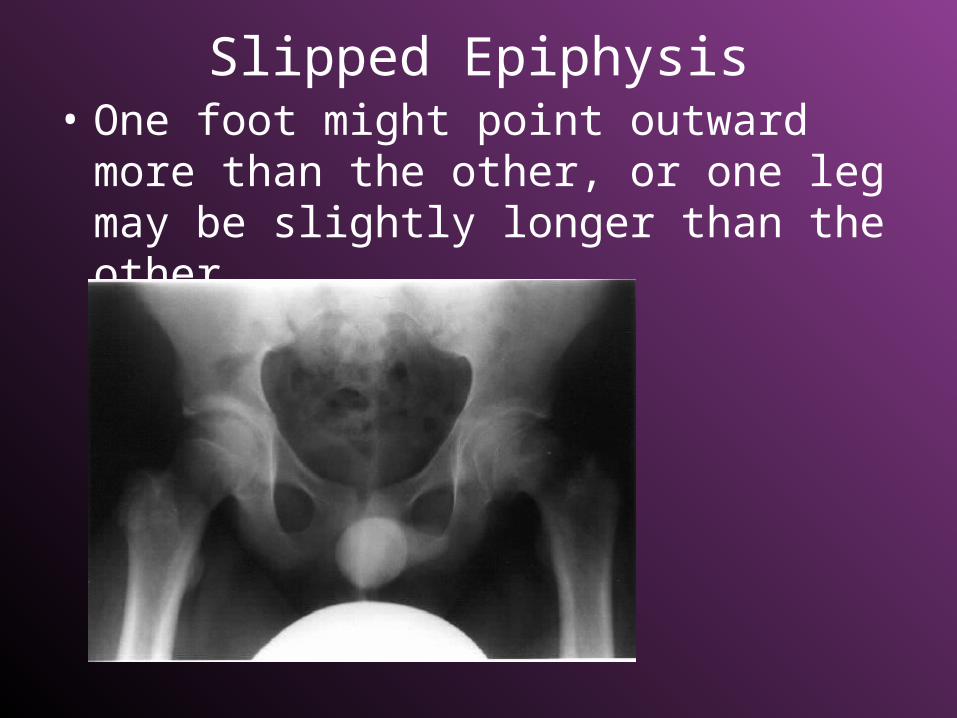
Slipped Epiphysis• One foot might point outward more than
the other, or one leg may be slightly longer than the other.

Slipped Epiphysis
11 yo with a limp
Bilateral with worse on the right side


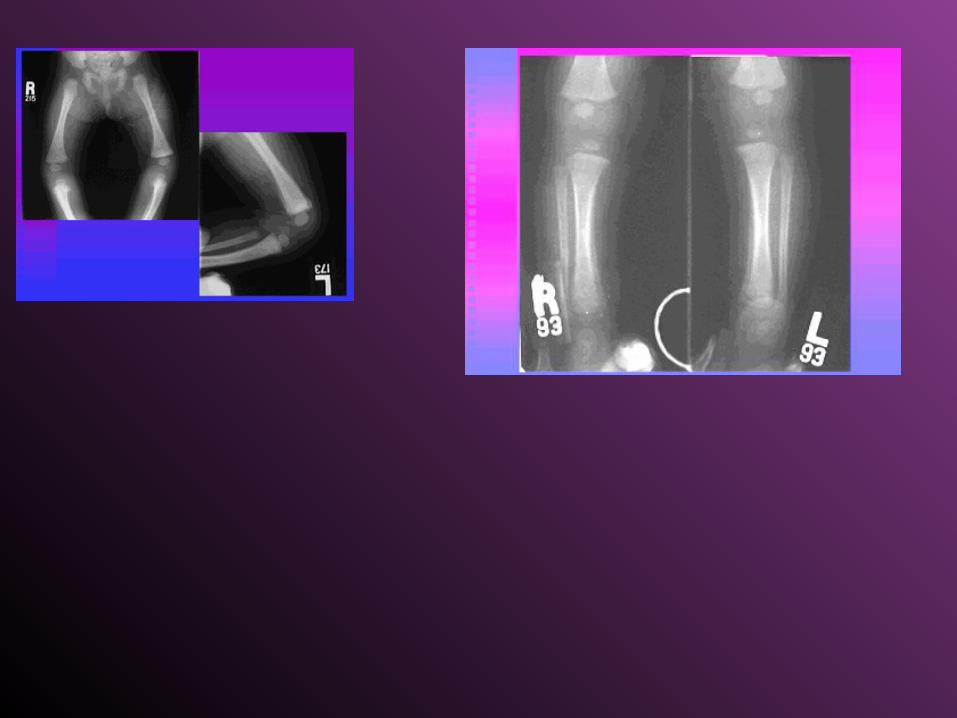
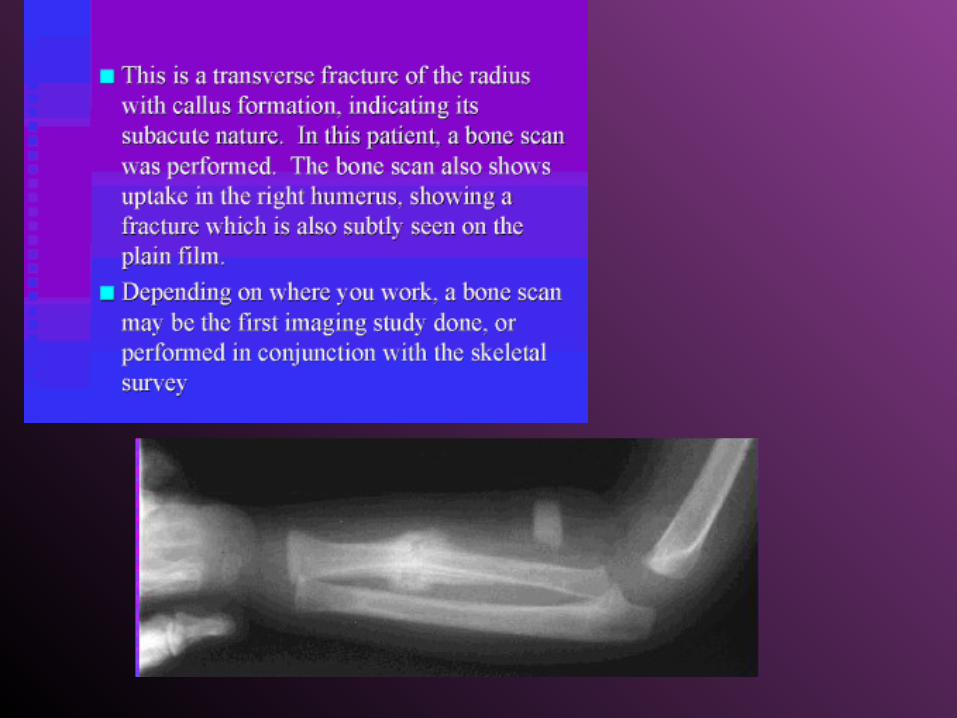
R/O Child Abuse
• Skeletal Survey• Bone Scan


Buckle or Corner Fx’s

• Moderate distention of several loops of bowel
• (lg or small?? )

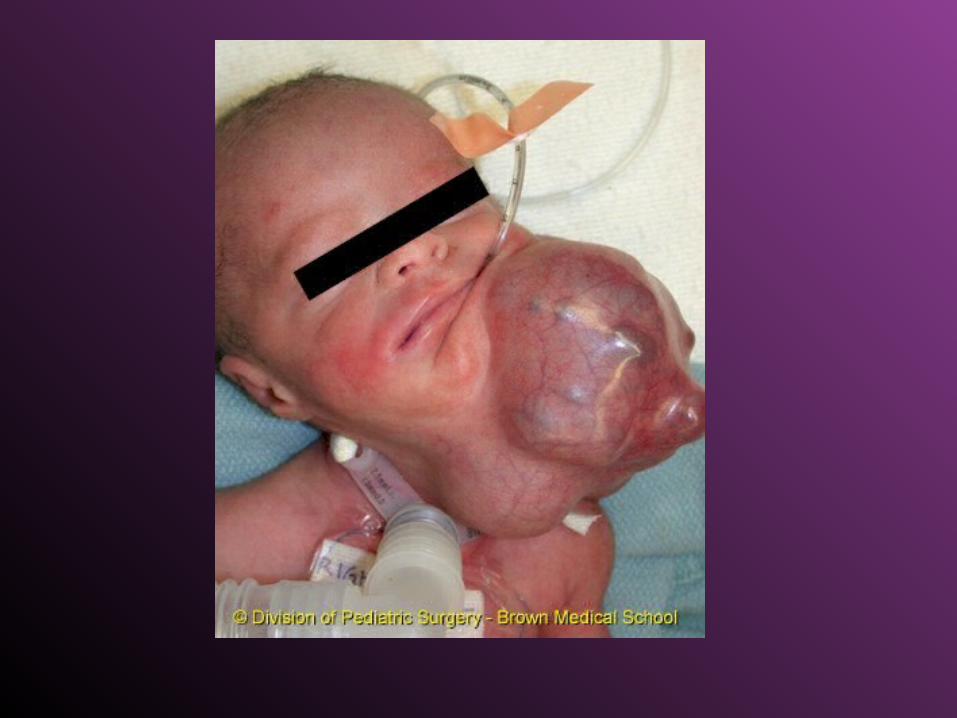
FETAL DEMISE +CONGENITAL ABNORMALITIES
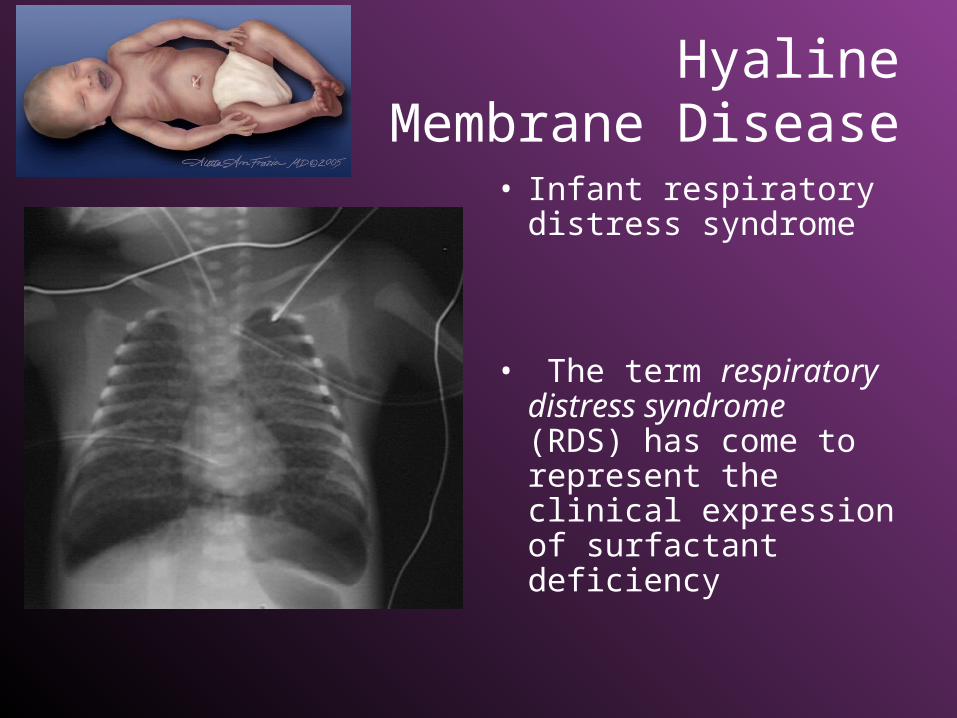
Hyaline Membrane Disease
• Infant respiratory distress syndrome
• The term respiratory distress syndrome (RDS) has come to represent the clinical expression of surfactant deficiency












![Intestinal pseudo-obstruction: adult Hirschsprung’s ...radiologyupdate.org/f/2018/06/Intestinal pseudo...ious causes [4]. One of them is Hirschsprung’s disease (HD), which is considered](https://static.fdocuments.us/doc/165x107/5e4e08035522ee140639de6b/intestinal-pseudo-obstruction-adult-hirschsprungas-pseudo-ious-causes.jpg)