Pediatric Community Acquired Pneumonia - · PDF file · 2017-05-04Pediatric...
56
Pediatric Community Acquired Pneumonia Newborn/Pediatric Critical Care Conference Russell J. OsguthorpeMD
Transcript of Pediatric Community Acquired Pneumonia - · PDF file · 2017-05-04Pediatric...

Pediatric Community Acquired Pneumonia
Newborn/Pediatric Critical Care Conference
Russell J. OsguthorpeMD

• Review pathophysiology
• Review common organisms
• Review recommended management
• Review common radiographic findings
• Review complications (effusion and abscess)
Outline

Pretest
• Which organisms are the most likely causes of pneumonia in a term 3 day old?
• What is the recommended duration of antibiotics for uncomplicated pediatric CAP?
• What organisms typically cause pleural effusions?

Acute Pneumonia
• Pneumonia = Greek for “lung inflammation”
• Inflammation of alveoli and interstitial tissue by an infectious organism
• Arises from aspiration, inhalation, or hematogenous seeding of infectious organism

• Leading infectious cause of mortality in children worldwide1
• Estimated to have killed 1.6 million children < 5 yo since 20001
• In U.S. CAP accounts for ~9% outpatient visits in <2 yo and ~5% in 3-6 yo2
Acute Pneumonia
1Black RE, Cousens S, Johnson HL et al. Global, regional, and national causes of child mortality in 2008: a systematic analysis.Lancet. 2010;375:1969-1975.2Grijalva et al. National impact of universal childhood immunizations with pneumococcal conjugate vaccine on outpatient medical care visits in the United States. Pediatrics 2006; 118:865-873.

Pneumonia Pathophysiology
• Physical and physiologic barriers of respiratory tract:
- Filtration and humidification
- Mucus production
- Epiglottis and cough
• B and T cells
• Alveolar phagocytes
• Failure of these barriers or a large inoculum leads to pneumonia

CAP: Difficulty in Diagnosis
• Primarily a clinical diagnosis
– No single pathognomonic sign (fever, abdominal pain, hypoxia, etc.)
• Bacterial vs. viral etiology
• Can see co-infections (bacterial-viral, viral-viral)1
1Thorburn K, Harigopal S, Reddy V, et al. High incidence of pulmonary bacterial co-infection in children with severe respiratory syncytial virus (RSV) bronchiolitis. Thorax 2006; 61:611–5.

• Acute onset
• Usually focal pulmonary findings
• Unvaccinated more at risk
• Alveolar rich blood supply can lead to bacteremia
• Gradual onset
• Usually diffuse pulmonary findings
• Disrupt alveolar macrophages secondary infection
• Greater appreciation in age of vaccination and improving molecular diagnostics
Viral CAPBacterial CAP

CAP: Difficulty in Diagnosis
• Bloodstream infection helps establish diagnosis but only occur in ≤ 10%1,2
• Pathogens vary by age, underlying immune function
1Hickey RW, Bowman MJ, Smith GA. Utility of blood cultures in pediatric patients found to have pneumonia in the emergency department. Ann Emerg Med 1996; 27:721–5.2Shah SS, Dugan MH, Bell LM, et al. Blood cultures in the emergency department evaluation of childhood pneumonia. Pediatr Infect Dis J 2011; 30:475–79.

• Review pathophysiology
• Review common organisms
• Review recommended management
• Review common radiographic findings
• Review complications (effusion and abscess)
Outline

CAP Organisms: 0-3 weeks
• Group B strep
• Gram negative enteric bacilli
• L.monocytogenes
• T.pallidum
• CMV
• HSV
• Genital Mycoplasma and Ureaplasma (LBW)
• Which organisms are the most likely causes of pneumonia in a term 3 day old?
• What is the recommended duration of antibiotics for uncomplicated pediatric CAP?
• What organisms typically cause pleural effusions?
McIntosh K: Community-acquired pneumonia in children. N Engl J Med 2002; 346:429-437.

CAP Organisms: 0-3 weeks
• Early vs. late onset
• Consider risk factors: preterm delivery, chorioamnionitis, PROM
• C.trachomatis tends to present by 2-3 weeks
McIntosh K: Community-acquired pneumonia in children. N Engl J Med 2002; 346:429-437.

CAP Organisms: 3 wk-3mo
• C.trachomatis
• RSV
• Rhinovirus
• Parainfluenza viruses
• S.pneumoniae
• B.pertussis
McIntosh K: Community-acquired pneumonia in children. N Engl J Med 2002; 346:429-437.

CAP Organisms: 3mo-5yo
• RSV, parainfluenza, HMPV, influenza, adenovirus, rhinovirus
• S.pneumoniae
• H.influenzae (non-typeable)
• S.aureus
• M.pneumoniae
• Other viruses: Enterovirus, parechovirus
McIntosh K: Community-acquired pneumonia in children. N Engl J Med 2002; 346:429-437.

CAP Organisms: 5yo-15yo
• S. pneumoniae
• S. aureus
• Influenza virus
• HMPV*
• M. pneumoniae
• C. pneumoniae
McIntosh K: Community-acquired pneumonia in children. N Engl J Med 2002; 346:429-437.


Pathogens Detection in Relation to Age among Hospitalized Children with CAP in EPIC Study--January 1, 2010 to June 30,
2011
Bacterial Pathogen Detected
< 5 yon=964
5-9 yon=211
10-17 yon=145
All agesn=1320
S.pneumoniae 3% 1% 2% 3%
M.pneumoniae 2% 9% 19% 5%
S.pyogenes 1% 0% 2% 1%
C.pneumoniae <1% 1% 1% <1%
S.aureus <1% <1% 0% <1%

• Review pathophysiology
• Review common organisms
• Review recommended management
• Review common radiographic findings
• Review complications (effusion and abscess)
Outline

Clinical Scenario
You are seeing a previously healthy, fully vaccinated, 4 yo child in clinic. She presents with 2 days of fever and worsening cough.
What are the next steps to work her up for pneumonia?

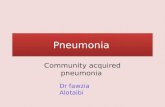
IDSA Pediatric CAP Guidelines
• Obtain pulse oximetry and examine
– Exam consistent with pneumonia?
• Decide on inpatient vs. outpatient
– Hypoxemia? ↑ WOB? Shock? AMS?
• Hospitalization recommended:
– moderate-to-severe CAP
– patients 3-6 mo old
– Concern for virulent pathogen, e.g. MRSA
– Concern for poor follow-up/compliance

IDSA Pediatric CAP Guidelines
• Recommended inpatient management:
– Does the child require ICU care?
– CBC with diff, ESR, CRP, test for influenza and start treatment if high suspicion
– 2 view CXR (repeat not routinely needed)
– Blood culture for complicated pneumonia or for moderate-to-severe pneumonia
– Tracheal aspirate culture (if intubated) and pleural fluid (if significant) for culture and/or PCR testing
– Reassess in 24-48 hours

IDSA Pediatric CAP Guidelines
• Recommended outpatient management:
– Little evidence to support extensive testing
– Test for influenza and treat if high suspicion
– Do not necessarily need CXR or labs
– Routine blood culture not routinely needed for fully immunized, non-toxic child
– Consider blood culture for child who does not show clinical improvement or who has worsening symptoms
– Reassess in 24-48 hours

Bacterial CAP Treatment (IDSA)
• Inpatient: Ampicillin or PCN G recommended empiric therapy (target S.pneumoniae)
– PCN allergy: Ceftriaxone, clindamycin, vancomycin
– If suspect MRSA, add clindamycin or vancomycin
– Incomplete immunizations, high rate of PCN-resistant S.pneumoniae, or empyema: give 3G cephalosporin
– Discharge: step down to oral therapy preferred over outpatient parenteral therapy

Bacterial CAP Treatment (IDSA)
• Outpatient: amoxicillin recommended empiric therapy (target S.pneumoniae)
– PCN allergy or PCN-resistant S.pneumoniae: Ceftriaxone, clindamycin, levofloxacin*
– If suspect atypical organism, use macrolide

• Which organisms are the most likely causes of pneumonia in a term 3 day old?
• What is the recommended duration of antibiotics for uncomplicated pediatric CAP?
• What organisms typically cause pleural effusions?

Bacterial CAP Treatment
• Lack of prospective RCT evaluating duration of therapy in U.S.
– Various international studies have looked at 3-10 days of treatment
• IDSA recommends 10 days for uncomplicated pneumonia
– 2-4 weeks for complicated pneumonia

Viral CAP Treatment (IDSA)
• Antibiotics not routinely required for preschool aged children (viral most likely)
• If suspect influenza, promptly initiate neuraminidase inhibitor (Tamiflu)
• Supportive care

Recommended Tamiflu dosing
• <12 mo old: 3 mg/kg BID
– Emerging data may change dosing1
• >12 mo old: weight-dependent dosing
– ≤15kg: 30 mg BID
– 15-23kg: 45 mg BID
– 23-40kg: 60mg BID
– > 40 kg: 75 mg BID
1Kimberlin DW, Acosta EP, Prichard MN et al. Oseltamivir Pharmacokinetics, Dosing, Resistance Among Children Aged < 2 Years withInfluenza. JID 2013;207: 709-20.
Pediatric CAP: algorithm steps 1-3
…with notes

Pediatric CAP: algorithm step 4
…with notes

Pediatric CAP: algorithm step 5
…with notes

Pediatric CAP: algorithm steps 6 and 7
…with notes

• Review pathophysiology
• Review common organisms
• Review recommended management
• Review common radiographic findings
• Review complications (effusion and abscess)
Outline

Classic Radiographic Findings
• Can be falsely normal and lag behind clinical exam
http://fitsweb.uchc.edu/ctanatomy/chest/review/lobes-anterior.html
RUL
RML
RLL
LUL
LLL

Viral Pneumonia

Viral Pneumonia

S.pneumoniae Focal Infiltrate

S.pneumoniae Focal Infiltrate

S.pneumoniae Focal Infiltrate

Nodular infiltrates

Nodular Infiltrates

Nodular Infiltrates

• Review pathophysiology
• Review common organisms
• Review recommended management
• Review common radiographic findings
• Review complications (effusion and abscess)
Outline

PPE and Empyema
• Pleural effusion: any fluid between visceral and parietal pleurae (exudate vs. transudate)
• Parapneumonic effusion (PPE): inflammatory fluid around a pneumonic process
• Empyema: purulent PPE
PPE Empyema

• Which organisms are the most likely causes of pneumonia in a term 3 day old?
• What is the recommended duration of antibiotics for uncomplicated pediatric CAP?
• What organisms typically cause pleural effusions?

PPE and Empyema
• Culture is often negative
• Common bacteria include: S.pneumoniae, S.aureus, S.pyogenes, M.pneumoniae1
• Rare complications include bronchopleural fistula
1Buckingham SC, King MD, Miller ML: Incidence and etiologies of complicated parapneumonic effusions in children, 1996 to 2001. Pediatr Infect Dis J2003; 22:499-504.

PPE and Empyema
• Radiographs are relatively sensitive and better predictors than physical exam
• Consider US or CT chest to distinguish fluid from parenchymal disease1
1Donnelly LF, Klosterman LA: CT appearance of parapneumonic effusions in children: findings are not specific for empyema. AJR Am J Roentgenol 1997; 169:179-182

Long 2012

PPE and Empyema Treatment
• Small-to-moderate rarely require drainage1
• Large (>1/2 thorax) usually require continuous drainage1
• PPE with loculations benefits from chest tube placement, fibrinolysis, or VATS2,3
• Consider VATS for persistent moderate-to-large effusions causing ongoing respiratory compromise
1Carter E, Walhausen J, Zhang W, et al: Management of children with empyema: pleural drainage is not always necessary. Pediatr Pulmonol 2010; 45:475-480.2Shah SS, DiCristina CM, Bell LM, et al: Primary early thoracoscopy and reduction in the length of hospital stay and additional procedures among children with complicated pneumonia: results of a multicenter retrospective cohort study. Arch Pediatr Adolesc Med 2008; 162:675-6813Sonnappa S, Cohen G, Owens CM, et al: Comparison of urokinase and video-assisted thoracoscopic surgery for treatment of childhood empyema. Am J Respir Crit Care Med 2006; 174:221-227

PPE and Empyema Treatment
• Empiric antibiotics target most likely organisms (ceftriaxone, vancomycin, clindamycin, azithromycin)
• Treat for 2-4 weeks

Necrotizing Pneumonia/Pulmonary Abscess
• Necrotizing pneumonia: insidious necrosis of lung parenchyma
– Suspect when no improvement despite appropriate antibiotics
– Often complicated by PPE
– Can lead to pulmonary abscess, pneumatocele, bronchopleural fistula
• Usually due to virulent, toxin-producing bacteria (S.pneumoniae, S.aureus, S.pyogenes)

Necrotizing Pneumonia/Pulmonary Abscess Treatment
• Percutaneous drainage of abscess can create bronchopulmonary fistula
– Consider drainage if no improvement after 5-7 days, abscess > 4 cm, causes mediastinal shift, or results in mechanical ventilation1
1Hoffer FA, Bloom DA, Colin AA, Fishman SJ: Lung abscess versus necrotizing pneumonia: implications for interventional therapy. Pediatr Radiol 1999; 29:87-91.

Necrotizing Pneumonia/Pulmonary Abscess Treatment
• Most cases respond to antibiotics without surgery
– Empiric choices depend on suspected source (clindamycin, zosyn)
• Treat for 4 weeks

Preventing CAP
• Immunize, immunize, immunize!

Summary
• Etiology of CAP varies with age
• Extensive testing and CXRs not routinely needed for outpatient
• Be wary of co-infections
• Recommended duration of treatment for uncomplicated CAP is 10 days
• PPE, empyema, necrotic lung, lung abscess require longer duration of antibiotics

Questions?