Pediatric airway management
82
BY Deiaa El - Din M. Tamer P.I.C.U. Specialist
-
Upload
deiaa-tamer -
Category
Health & Medicine
-
view
207 -
download
2
Transcript of Pediatric airway management

BY
Deiaa El-Din M. Tamer
P.I.C.U. Specialist

Recognize signs and symptoms of unstable airway.
Recognize signs and symptoms of respiratory failure.
Identify anatomic and physiologic variables involvedin the management of the pediatric airway.
Describe how to open and maintain an airwaymanually and with the help of different airwaymaneuvers.
Explain how to support a patient with bag-maskventilation.
Describe the preparation for and the sequence ofintubating pediatric patient.
Recognize the potential for difficult intubation anddiscuss alternative methods of establishing a stableairway.
You are called to a 7 month old boy with respiratorysyncytial virus bronchiolitis, child is alert andinteractive, pink, but has retractions.
What signs and symptoms indicate airway instability?
Is there airway instability in this case?
What intervention?
Nose:
Nose provides nearly half of the total airway resistance
Nose is short soft and small with nearly circular nares.
Infants under 2 months are obligate nasal breather.
They can be easily occluded by edema , secretions , orexternal pressure.
Cleaning the nasal passages by suctioning cansignificantly improve an infant’s respiratory condition.

Larger in proportion to the oral cavity than in the adultTongue
Epiglottis
Larynx
Narrower, shorter at the level of the first vertebra and overlaps the soft palate
Higher in the neck C2 in neonates (C3-C4) in children than in the adult (C5-C6)The angel between the base of the tongue and the glotticopening is more acute
Cricoid More conically shaped in infants; narrowest portion is at the cricoid ring, whereas in the adult it is at the level of the vocal cords
Trachea Deviated posteriorly and downward (becomes anatomically similar to the adult between 8 and 10 years of age)
Head Occiput relatively large compared with the adults'Optimal intubating position is with shoulder roll to prevent neck flexion in the supine position


Musculoskeletal:
The chest wall of the infant is relatively weak andunstable .
The use of abdominal muscles leads to characteristicseesaw or abdominal breathing pattern.
Intercostal, subcostal and suprasternal retractionsbecome prominent as airway obstruction occur.
Fatigue of respiratory muscles may lead to decreaserespiratory effort as respiratory failure progresses.

General appearance of the child with careful attention :
Tone
Interactiveness
Consolability
Look/Gaze
Speech/Cry
Injury to the airway or other conditions that will affect theairway (cervical spine fracture facial burn).
Signs of airway obstruction due to decreased level ofconsciousness.

Assessment of respiratory rate
Work of breathing
Abnormal airway sounds
Abnormal positioning
Retractions
Nasal flaring
Head bobbing

Osculates over the mouth, nose and neck as well ascentral and peripheral chest listen for quality,pitch right to left symmetry and magnitude ofbreath sound:
Extrathoracic airway obstruction : high pitchedinspiratory stridor and retractions.
Intrathoracic airway obstruction : sings and symptomsthat occur predominantly during the expiration , highpitched expiratory sound (wheezing ).
Incomplete obstruction (foreign body) : snoring ,stridor gurgling or noisy breathing.
Complete airway obstruction : sever respiratory effortwith absent breath sounds.
Parenchymal lung diseases : Crackles and endinspiratory noises .
Asymmetry of breath sounds is an important clue.

Evaluate mental status: Agitation and irritability may indicate hypoxemia.
Lethargy in the presence of acceptable oxygensaturation may reflect high carbon dioxide level.
Presence and strength of protective airway reflexes.
If respiratory efforts are absent and an immediateremedy is not available proceed to manual support andassisted ventilation while preparing to establish anartificial airway

Longitudinal physical assessment Arterial blood gas
HypoventilationAlveolar hyperventilationMetabolic acidosisMetabolic alkalosis
Pulse oximetry Exhaled carbon dioxide: ETCO2 numerical values are
dependent on 3 variables:CO2 productionDelivery of blood to lungs & the lungs ability to exchange gasAlveolar ventilation
Normal = 35-45mmHgHyperventilation = < 35mmHg (Respiratory alkalosis)Hypoventilation = > 45mmHg (respiratory acidosis)

Inadequate oxygenation
Low O2
Pneumonia
CHF
Inadequate ventilation
High CO2
Asthma/COPD
Inadequate protection
Airway Malformations
Airway trauma
Decrease level of conscious
Anticipated course
Hematomas
Long transports

Ventilation
Breathe In…Breathe Out…
This is the active, mechanicalprocess of breathing.
How we get rid of CO2
At the cellular level, O2 &glucose combine to produceenergy. CO2 is the wasteproduct.
CO2 is carried back throughthe blood & exhaled throughthe lungs via the aveoli.
Capnography measuresventilation.
OxygenationO2…Did you get it into the body?
How we get oxygen to the tissues.
Gas exchange occurs at thecapillary alveolar membrane.
O2 is transported to the tissuesthrough the bloodstream.
Pulse oximetry measures oxygenin the blood.

Cardiac and respiratory arrest
Hypoxaemia (Pao2 < 7.8 kPa, Sao2 < 90%)
Shock
Low cardiac output and metabolic acidosis (bicarbonate <18 mmol/l)
Respiratory distress
Ventilationperfusion mismatch (acute asthma, atelectaticlung zones)
Inadequate tissue perfusion
Low haemoglobin concentration
Abnormal oxygen dissociation curve(haemoglobinopathies, high carboxyhaemoglobin)
Histotoxic poisoning of intracellular enzymes(septicaemia)

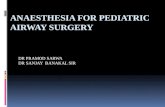
Simple oxygen mask (C)
Partial rebreathing mask (D)
Non-rebreathing mask (B)
Face tent
Nasal cannula (A)

A 15 years old female arrived to ED by ambulance afteringestion of 6 tablets of diazepam for committingsuicide after failure in the exam, she is not respondingto painful stimuli, RR 27 c/min but with retraction andnoisy breathing.
What is the emergency problem in this case?
What is the management?
What is the important points in the assessment?





INDICATIONS
■ Oropharyngeal airways provide a conduit for airflowthrough the mouth to the pharynx.
■ Oropharyngeal airways prevent mandibular tissuefrom obstructing the posterior pharynx.
■ Oropharyngeal airways may be used in theunconscious infant or child if procedures (ie, head tilt-chin lift or jaw thrust) to open the airway fail toprovide and maintain a clear, unobstructed airway.

CONTRAINDICATIONS
Absolute
■ Avoid inserting an oropharyngeal airway in consciousor semiconscious patients because it may stimulategagging and vomiting.
EQUIPMENT
■ Oropharyngeal airways come in various sizes rangingfrom 4 cm to 10 cm.
■ Oropharyngeal airways consist of a flange, a shortbiteblock segment, and a curved body usually made ofplastic and shaped to provide an air channel andsuction conduit through the mouth.

TIPS
■ Oropharyngeal airways do notprevent aspiration.
PATIENT PREPARATION
■ Measure the distance from thecentral incisors to the angle ofthe mandible to approximatethe correct size oral airway.
PATIENT POSITIONING
■ Head and airway must bepositioned properly tomaintain a patent airway evenafter insertion of anoropharyngeal airway.

PROCEDURE
■ The airway can be placed with a tongue blade holdingthe tongue on the floor of the mouth.
■ Depress the tongue and gently glide the airway withthe concave side downward, following the curvature ofthe tongue.
■ The airway can also be introduced upside down andgently rotated to the proper position, using rotation topull the base of the tongue forward.
• Do not exert pressure on the palate if using thistechnique.
• This technique is done without instrumentation.

MONITORING
■ Monitor for airway obstruction; the following clinical signsmay manifest:
•Agitation.
• Desaturation.
• Impaired air exchange when auscultated.
• Diminished chest rise.
■ Use pulse oximetry to measure oxygen saturation levels.
■ Measure heart rate.
■ Check blood pressure using a noninvasive device.

COMPLICATIONS
■ If the oropharyngeal airway is too large, it may obstruct thelarynx, make a tight mask fit difficult, and traumatizelaryngeal structures.
■ If the oropharyngeal airway is too small or is insertedimproperly, it pushes the tongue posteriorly, obstructingthe airway.
■ If the oral airway is placed in the awake patient, it mayinduce vomiting, aspiration, and laryngospasm.
■ If the airway is too long, it may induce vomiting andaspiration.
CAVEAT
■ The oropharyngeal airway may not be sufficient to relieveupper airway obstruction, and the patient maysubsequently require intubation.

INDICATIONS
■ Nasopharyngeal airways provide a conduit for airflowbetween the nares and the pharynx.
■ Nasopharyngeal airways prevent mandibular tissuefrom obstructing the posterior pharynx.
■ Nasopharyngeal airways may be used in consciouspatients (unlike oropharyngeal airways).
■ Nasopharyngeal airways may be used in children withimpaired consciousness or in neurologically impairedpatients with poor pharyngeal tone leading to upperairway obstruction.
■ Nasopharyngeal airways can be used to suctionsecretions.

CONTRAINDICATIONS Absolute■ Nasal airway occlusions.■ Nasal fractures.■ Coagulopathy (because of the risk of epistaxis).■ Cerebrospinal fluid leak.■ Basilar skull fracture.■ Adenoidal hypertrophy.
EQUIPMENT■ A nasopharyngeal airway is a soft rubber or plastic tube.■ Nasopharyngeal airways come in various sizes ranging from
12F to 36F.■ A shortened tracheal tube may be used as a nasopharyngeal
airway.■ Lubrication jelly.

RISKS■ Nasal bleeding.■ When using a shortened tracheal tube instead of a soft
nasopharyngeal airway, injury to the soft tissues of thenasal passages may occur because of the rigid stiff plastic.
TIPS■ Nasopharyngeal airways do not prevent aspiration.
PATIENT PREPARATION■ Measure the distance from the nares to the tragus of the ear
to approximate the appropriate size and length of tube.
PATIENT POSITIONING■ Head and airway must be positioned properly to maintain a
patent airway even after insertion of a nasopharyngealairway.

PROCEDURE
■ The tube is lubricated and inserted into the nostriland positioned into the posterior pharynx.
■ Advance the tube gently, following the naturalcurvature of the nasal passage to direct the tube in aposterior inferior position.
■ After measuring as above, use the largest diametertube that can fit into the nose without causingblanching of the nares.
■ If passage does not occur easily, attempt the othernostril because patients may have different size nasalpassages.



MONITORING
■ Because the nasopharyngeal airway has a smallinternal diameter, it can be obstructed with mucus,blood, vomit, or the soft tissues of the pharynx.
■ When necessary, suction the airway frequently toensure patency.
■ Use pulse oximetry to measure oxygen saturationlevels.
■ Measure heart rate.
■ Check blood pressure using a noninvasive device.

COMPLICATIONS
■ If the nasopharyngeal airway is too long, it may causebradycardia through vagal stimulation or it may injure theepiglottis or vocal cords.
■ Physical irritation of the larynx or lower pharynx maystimulate coughing, vomiting, or laryngospasm (if the tubeis too long).
■ Nasopharyngeal airways can cause a pressor response withincreased blood pressure.
■ Failure of insertion.
■ Epistaxis (due to mucosal tears or avulsion of turbinates).
■ Submucosal tunneling and pressure sores.
■ Perforation of cartilage into the sinuses.
■ Stimulation of nasal secretions with obstruction of thetube.
■ Prolonged placement of a tight fitting tube may lead tonasal necrosis.

CAVEAT
■ The nasopharyngeal airway may not be sufficient torelieve upper airway obstruction, and the patient maysubsequently require intubation.

A 15 years old female arrived to ED by ambulance afteringestion of 6 tablets of diazepam for committingsuicide after failure in the exam, she is not respondingto painful stimuli, RR 27 c/min but with retraction andnoisy breathing.
What is the emergency problem in this case?
What is the management?
What is the important points in the assessment?

You use the maneuver of head tilt chin lift but thebreathing still noisy with retraction.
What will you do?

After about an hour the patient develop apnea.
What will you do?
What about the oropharyngeal airway?


INDICATIONS
■ To ventilate and oxygenate a patient.
■ A ventilation face mask may be used with anoropharyngeal or nasopharyngeal airway duringspontaneous, assisted, or controlled ventilation.
CONTRAINDICATIONS
Relative
■ In patients with full stomach, cricoid pressure must bemaintained to avoid vomiting and aspiration.

EQUIPMENT
■ Ventilation bags (manual resuscitator) come in 2 types:
self-inflating bag
flow-inflating (“anesthesia”) bag.
■ Ventilation bags used for resuscitation should be self inflating.
■ Ventilation bags come in different sizes: infant, child, and adult.
■ Face masks come in many sizes.
■ A ventilation mask consists of a rubber or plastic body, a standardconnecting port, and a rim or face seal.
■ Supplemental oxygen can be attached to ventilation bags toprovide oxygen to the patient.
RISKS
■ Vomiting and aspiration.

TIPS
■ Bag-mask ventilation gives the clinician time toprepare for more definitive airway management.
■ Good technique involves preserving good mask-faceseal, inflating the chest with minimal requiredpressure, and maintaining the optimal patency of theupper airway through manipulation of the mandibleand cervical spine.
■ The clinician should only use the force and tidalvolume necessary to cause the chest to rise visibly.

■ The mask should extend from the bridge of the nose tothe cleft of the chin, enveloping the nose and mouthbut avoiding compression of the eyes.
■ The mask should provide an airtight seal.
■ The goal of ventilation with a bag and mask should beto approximate normal ventilation.
PATIENT PREPARATION
■ Sedation may be required before beginning.

PATIENT POSITIONING
■ A neutral “sniffing” position without hyperextensionof the neck is usually appropriate for infants andtoddlers.
■ Avoid extreme hyperextension in infants because itmay produce airway obstruction.
■ In patients with head or neck injuries, the neck mustbe maintained in a neutral position.
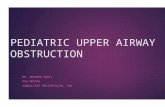
Head Tilt-Chin Lift Jaw Thrust

PROCEDURE
Sequence■ Open the airway via chin lift/jaw thrust maneuver.■ Seal the mask to the face.■ Deliver a tidal volume that makes the chest rise.
E-C Clamp Technique■ Tilt the head back and place a towel beneath the head.■ If head or neck injury is suspected, open the airway with
the jaw thrust technique without tilting the head.• If a second person is present, have that person immobilize
the spine.■ Apply the mask to the face.• Lift the jaw using the third, fourth, and fifth fingers from
the left hand under the angle of the mandible; this formsthe “E”


When lifting the jaw, the tongue is also lifted away from theposterior pharynx.
• Do not put pressure on the soft tissues under the jawbecause this may compress the airway.
■ Place the thumb and forefinger of the left hand in a “C”shape over the mask and exert downward pressure •Createa tight seal between the mask and the patient’s face usingthe left hand and lifting the jaw.
•Compress the ventilation bag with the right hand.
• Be sure the chest rises visibly with each breath.
■ If 2 people are present, then 1 person can hold the mask to
the face while the other person ventilates with the bag.
• One person uses both hands to open the airway andmaintain a tight mask-to-face seal.
• The second person compresses the ventilation bag.


■ If 2 or 3 people are present, someone can applypressure to the cricoid cartilage (termed “Sellickmaneuver”) to limit gastric distention in unconsciouspatients.
• The Sellick maneuver may also prevent regurgitationand aspiration of gastric contents.
•Avoid excessive cricoid pressure because it may produce
tracheal compression and obstruction or distortion ofthe upper airway anatomy.
■ To relieve gastric distention, a nasogastric tube can beplaced (if not contraindicated).


MONITORING
■ Use pulse oximetry to measure oxygen saturationlevels continuously.
■ Measure heart rate continuously.
■ Check blood pressure using a noninvasive device.
■ Ensure the chest rises visibly.

COMPLICATIONS
■ Reduction in cardiac output.
• Excessive ventilation volume and airway pressure maylower cardiac output by raising intrathoracic pressureand distending alveoli, increasing afterload of the rightheart, and decreasing venous return.
■ Vomiting and aspiration.
■ Air trapping, barotrauma, air leak, and reducedcardiac output can be caused by excessive tidal volumeand rate in patients with small airway obstruction (eg,asthma and bronchiolitis).

CAVEATS
■ It is important to coordinate bag-mask ventilationwith the patient’s spontaneous breaths in a patientwho is spontaneously breathing. Dyssynchrony canpredispose patients to barotrauma and air leak.
■ While performing bag-mask ventilation, it isimportant for someone with more advanced airwayskills to be preparing for intubation, or for someone tobe arranging for the patient’s transport to a facilitywhere definitive airway management can beperformed.
■ No muscle relaxant should be given unless a persontrained in advanced airway skills is present.


INDICATIONS
Respiratory
■ Apnea.
■ Acute respiratory failure (PaO2 < 50 mm Hg in patient with fraction of inspiredoxygen [FIO2] > 0.5 and PaCO2 > 55 mm Hg).
■ Need to control oxygen delivery (e.g. institution of positive end-expiratorypressure [PEEP], accurate delivery of FIO2 > 0.5)
■ Need to control ventilation (e.g. to decrease work of breathing, to controlPaCO2, to provide muscle relaxation).
Neurologic
■ Inadequate chest wall function (e.g. in patient with Guillain- Barré syndrome,poliomyelitis).
■ Absence of protective airway reflexes (e.g. cough, gag).
■ Glasgow Coma Score ≤ 8.
Airway
■ Upper airway obstruction.
■ Infectious processes (e.g. epiglottis, croup).
■ Trauma to the airway.
■ Burns (concern for airway edema).

CONTRAINDICATIONS
Absolute
■ Nasotracheal intubation is contraindicated in patientswith nasal fractures or basilar skull fractures.
RISKS
■ Desaturation.
■ Bradycardia.
■ Inability to intubate.
■ Tracheal tear or rupture.

EQUIPMENT■ Suction.• Should have a tonsil-tipped suction device or a largebore suction
catheter as well as a suction catheter of appropriate size that fitsinto the endotracheal tube.
■ Oxygen.■ Resuscitation bags.■ Masks (appropriate sizes for ventilation).■ Laryngoscope (blade, handle, bulb, battery).■ Endotracheal tubes (appropriate sizes, cuffed, uncuffed).■ Forceps.■ Oropharyngeal airway.■ Tongue blade.■ Bite block.■ Tape (to secure tube).■ Stylet (appropriate sizes).■ CO2 detector device.■ Syringe to inflate the endotracheal tube balloon on cuffed tubes.

Suction equipment: catheters, regulator/canister/tubing.
Oxygen: O2 flowmeter, preoxygenate 2-3 min, manualresuscitator bag with mask
Airway equipment: ETT, stylet, syringe (cuffed ETT),laryngoscope and blade, lubricating gel, OPA
Position, pharmacy, personnel: supine, rolls for positioning,bed height up
Monitors
ETCO2 detector

TIPS
■ The suggested sizes for endotracheal tubes.
■ Uncuffed tubes are generally recommended inchildren younger than 8 years, except in cases of severelung disease. Age Internal Diameter (mm)
Premature infant 2.5–3.0Newborn 3.0Newborn–6 months 3.56 months–12 months 3.5–4.012 months–2 years 4.0–4.53–4 years 4.5–5.05–6 years 5.0–5.57–8 years 5.5–6.09–10 years 6.0–6.511–12 years 6.5–7.013–14 years 7.0–7.5
Useful formula:(Age+16)/4(Age/4)+4

■ Laryngoscopes.
•Handle with battery and blade with light source. Adultand pediatric handles fit all blades, and differ only inhandle diameter.
• A straight blade provides greater displacement of thetongue into the floor of the mouth and visualization ofa pharynx and anterior larynx .

• A curved blade may be used in the older child; thebroader base and flange allow easier displacement ofthe tongue.

■ The suggested sizes of blades.
■ If a difficult intubation is anticipated due to alteredsupraglottic anatomy, absolutely no irreversibleanesthetics or muscle relaxants should beadministered.
• Such patients should generally be intubated awake orin the operating room with halothane.
• For difficult intubations, other techniques, such asfiberoptic intubation, may be used.
Age Laryngoscope Blade SizeNewborn–6 months Miller 0-1, Wis Hipple 11 year Miller 1, Wis Hipple 1.5Child Miller 28–12 years Miller 2, Macintosh 2Adolescent Miller 3, Macintosh 3

PATIENT PREPARATION
■ Preoxygenate with 100% FIO2.
■ In an older child, explain each step as it is done.
PATIENT POSITIONING
■ A neutral “sniffing” position without hyperextensionof the neck is usually appropriate for infants andtoddlers.
•Avoid extreme hyperextension in infants because it mayproduce airway obstruction.
■ It is sometimes helpful to place a towel under thepatient’s shoulders.
■ In patients with head or neck injuries, the neck mustbe maintained in a neutral position.

PROCEDURE
Prior to Intubation
■ Check the intubation equipment before beginning.
■ Attach the blade to the handle and be sure that thebulb illuminates.
■ Attach suction to a suction machine and be sure thatsuction is turned on.
■ If using a stylet, insert stylet into endotracheal tube.
• The tip of the stylet should be 1–2 cm proximal to thedistal end of the endotracheal tube, ensuring that thestylet does not go through the Murphy eye.
■ Prepare to monitor the patient’s heart rate, oxygensaturation levels, and blood pressure.

Sequence■ Preoxygenate with 100% oxygen.■ Administer 0.01–0.02 mg/kg IV of atropine (minimum dose, 0.1
mg). Atropine may not be indicated in cases of significanttachycardia.
■ Administer IV sedation (e.g. fentanyl, morphine, midazolam,etomidate, thiopental, ketamine).
■ Apply cricoid pressure .■ Perform bag-mask ventilation with 100% oxygen.■ Give an IV muscle relaxant.■ Open the mouth and insert the laryngoscope.■ Avoid positioning the blade against the teeth, gums, or lips.■ Visualize the glottic opening.■ Suction any secretions that may obscure visualization.■ Insert endotracheal tube; observe the tube to pass through the
glottic opening.■ Remove the stylet while holding the tube securely in place, and
ventilate the patient.■ Secure the tube to the face.


Confirm Correct Position of Tube
■ Auscultation for symmetric breath sounds.
■ Good chest excursion.
■ Effective oxygenation.
■ Disposable colorimetric capnometer (color should changefrom purple to yellow if patient has a perfusing rhythm) orcapnograph.
■ Obtain chest radiograph.
■ Absence of breath sounds over the upper abdomen.
■ If unilateral breath sounds are heard on the right, pull backthe tube slowly while ventilating and listen for breathsounds on the left (probable intubation of right mainbronchus).
■ ETT depth (lip):
ETT size x 3
Age/2+12

MONITORING
■ Use pulse oximetry to measure oxygen saturation levelscontinuously.
■ Measure heart rate continuously.
■ Check blood pressure frequently using a noninvasivedevice.
COMPLICATIONS
■ Esophageal intubation.
■ Perforation of trachea.
■ Intubation of right main bronchus.
■ Aspiration.
■ Dental damage.
■ Laceration of lips or gums.

Acute deterioration post-intubation: (DOPE)
Displaced ETT
Obstruction of ETT
Pneumothorax
Equipment failure
FOLLOW-UP
■ The importance of follow-up is to make sure that theendotracheal tube remains in the correct position andis not obstructed.
■ Monitor end tidal CO2 using capnography.
■ Monitor oxygen saturation levels.
■ Check heart rate.


Advantages:
Used in any age
Easy to place
Few complications
Contraindications:
Gag reflex
FBs
Airway obstruction
High ventilation pressure
Does not secure airway


Difficult Airway







Nothing valuable can be lost by taking time
Thank You