Stridor, Stertor and Snoring- Common Pediatric Airway Problems
Upload
corey-collins-do-faapCategory
view
191download
1
Monday, May 23, 2011
Basics of Pediatric Airway Management
Corey E. Collins, D.O., F.A.A.P Director, Pediatric Anesthesiology Massachusetts Eye and Ear Infirmary Boston, MA
1
Corey E Collins, D.O.Monday, May 23, 2011
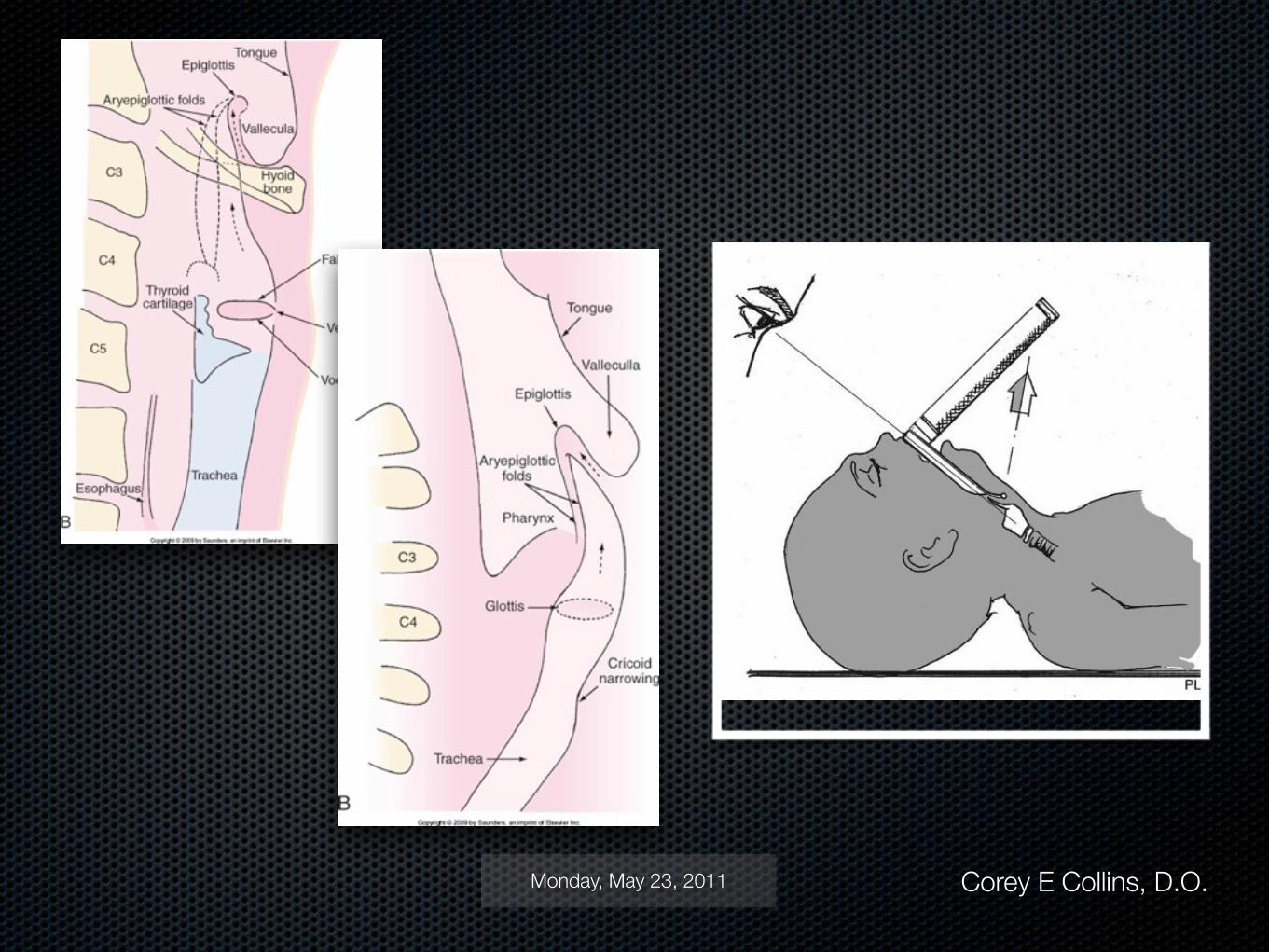
Pediatric Airway Anatomy
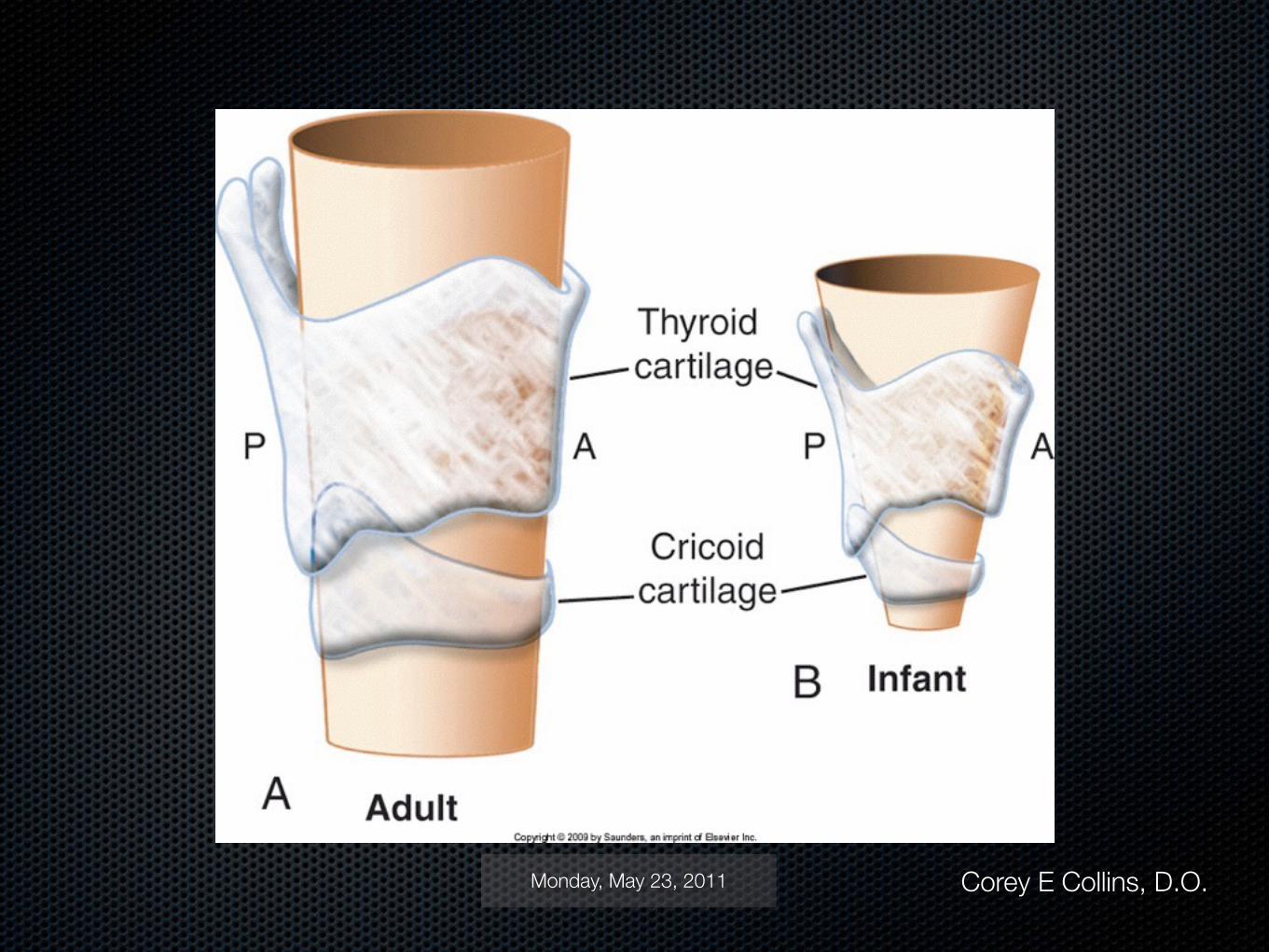
Narrowest part of airway is Cricoid Cartilage (vs V.C.)
Epiglottis and Tongue are relatively large
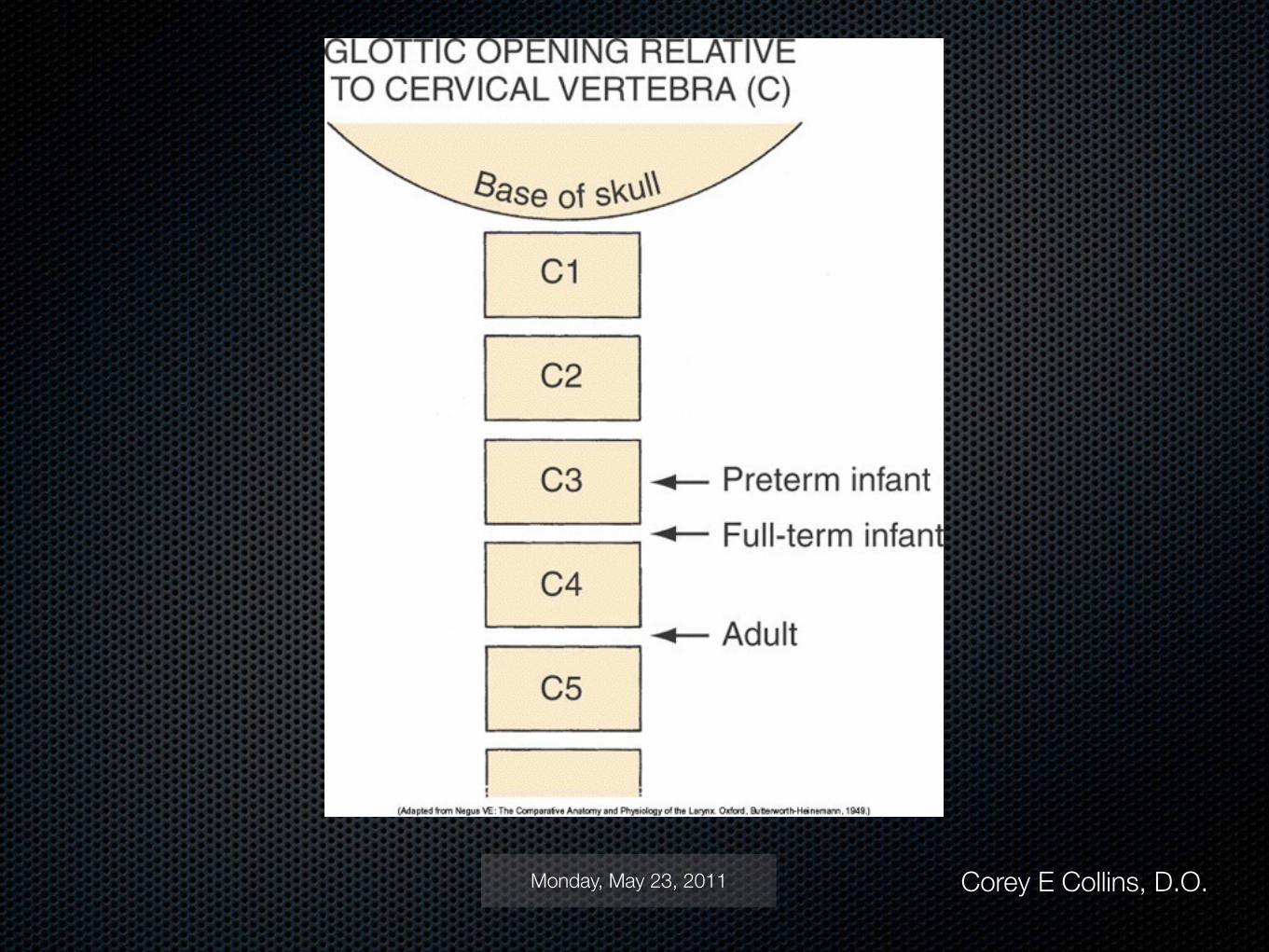
Larynx is Higher and Anteriorly tilted
Obligate Nasal Breathers until 6 mo
2
Corey E Collins, D.O.Monday, May 23, 2011
3
Corey E Collins, D.O.Monday, May 23, 2011
4
Corey E Collins, D.O.Monday, May 23, 2011
5
Corey E Collins, D.O.Monday, May 23, 2011
6
laryngeal view when introducing a tracheal tube orother instruments. When open the blade forms an85-degree angle with the handle. It is our experiencethat for trainees and other inexperienced intubatorsthis together with the ease of view encourages thegentle indirect lift of the epiglottis rather than thetemptation to use a levering and potentially moreforceful action as may be the case when using aconventional straight or curved blade. Figures 2, 3and 4.
The McCoy laryngoscope was developed in theearly 1990s to help with difficult intubation in adult
patients (28). Lately a pediatric version of the McCoylaryngoscope, based on the Seward straight blade,has become available. It has been designed to conferthe advantages of the straight blade in aligning thevarious axes in the infant airway whilst allowingthe epiglottis to be lifted with the blade tip in thevallecula. It is suggested that that this should allow aview comparable to that of a straight blade (25).
The two more commonly used intubation aids arethe gum-elastic bougie and the malleable stylet. Thebougie has been used for difficult intubation via theorotracheal and nasotracheal route (29,30). The useof such intubation aids is not free of complicationboth with respect to the equipment used and thepotential for trauma (31,32). Latto et al. found thatalthough the gum-elastic bougie is commonly used,
Figure 2Laryngoscopists view with Cardiff blade (above) and Macintosh(below) to show relative positions of the respective blades whenplaced in the valeculla and the epiglottis is elevated to expose theglottis. The arrow illustrates the direction of lift required to obtainthis view with the Cardiff blade.
Figure 3Miller 1 (above) and Cardiff Blade (below). Two views todemonstrate the difference in blade configuration.
Figure 4Macintosh (above) and Cardiff Blade (below). Two views todemonstrate the difference in blade configuration.
PEDIATRIC LARYNGOSCOPES AND INTUBATION AIDS 33
! 2009 The AuthorsJournal compilation ! 2009 Blackwell Publishing Ltd, Pediatric Anesthesia, 19 (Suppl. 1), 30–37
Corey E Collins, D.O.Monday, May 23, 2011
7
Corey E Collins, D.O.Monday, May 23, 2011
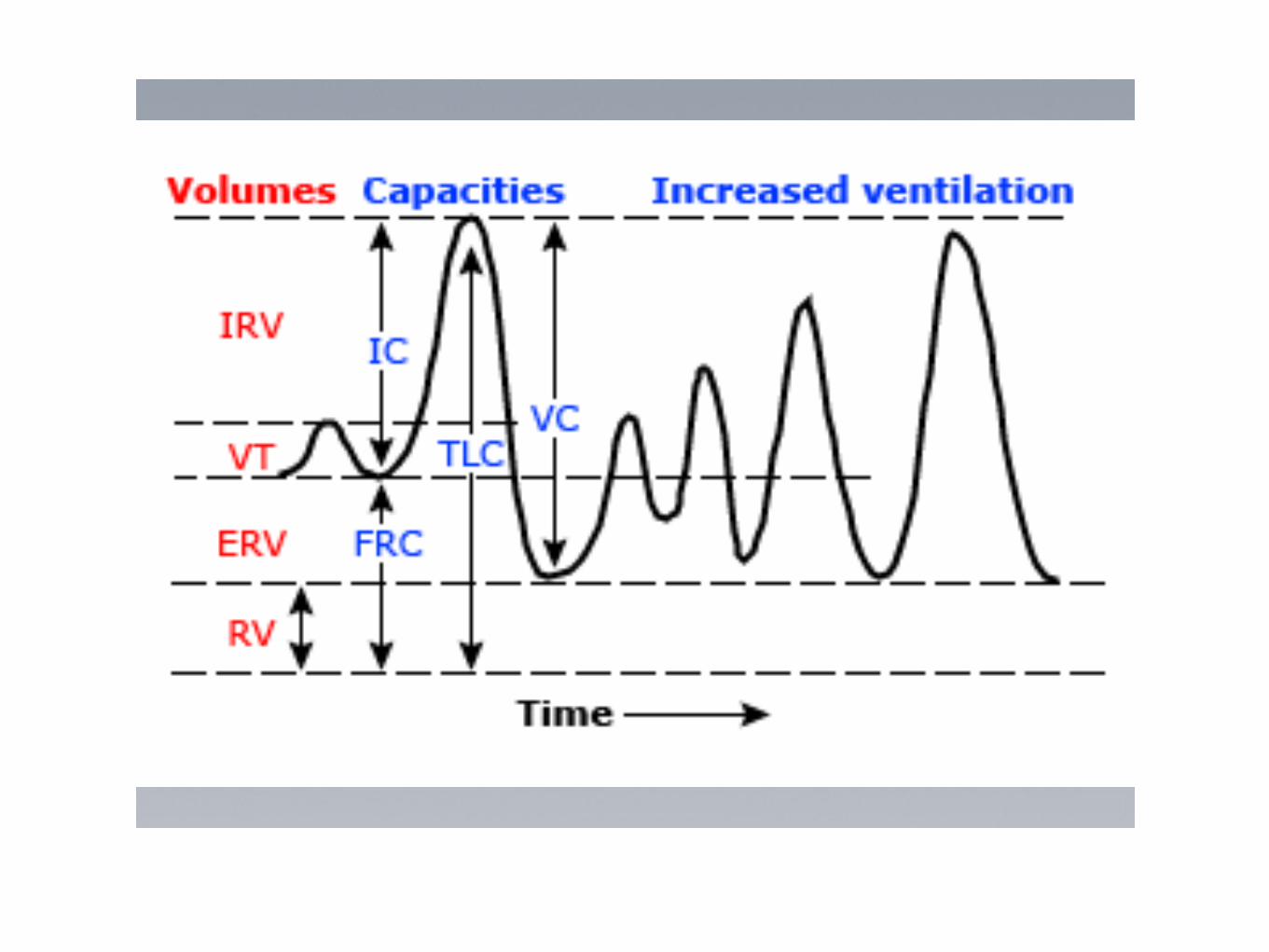
Respiratory Physiology
Vt = 6-8 ml/kg same as adults
Increased VO2: 6-8 mL/kg/min vs 4-6
Increased Minute Ventilation via RR
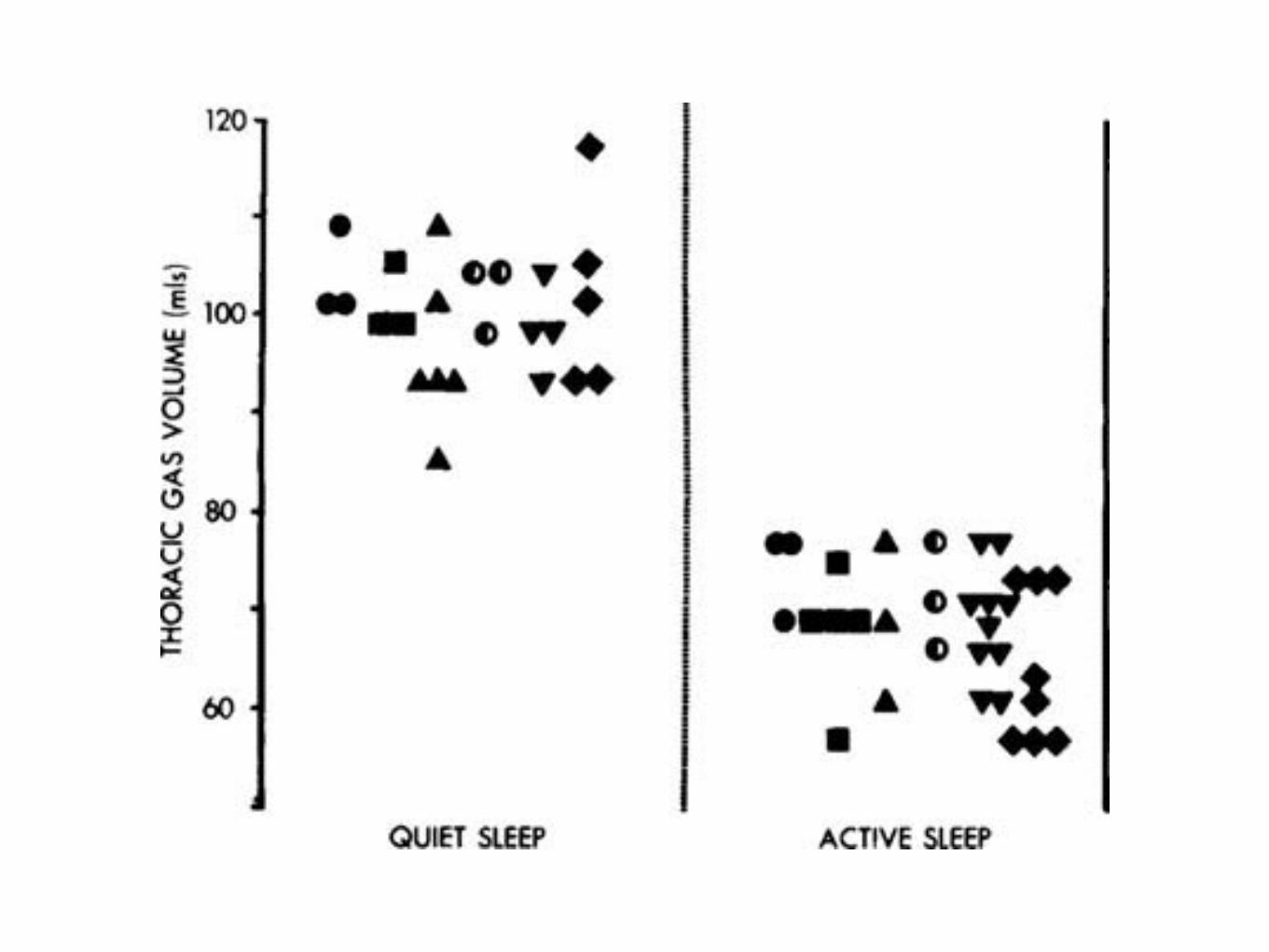
FRC :: adults but the higher MV/ FRC results in faster desaturation
8
Corey E Collins, D.O.Monday, May 23, 2011
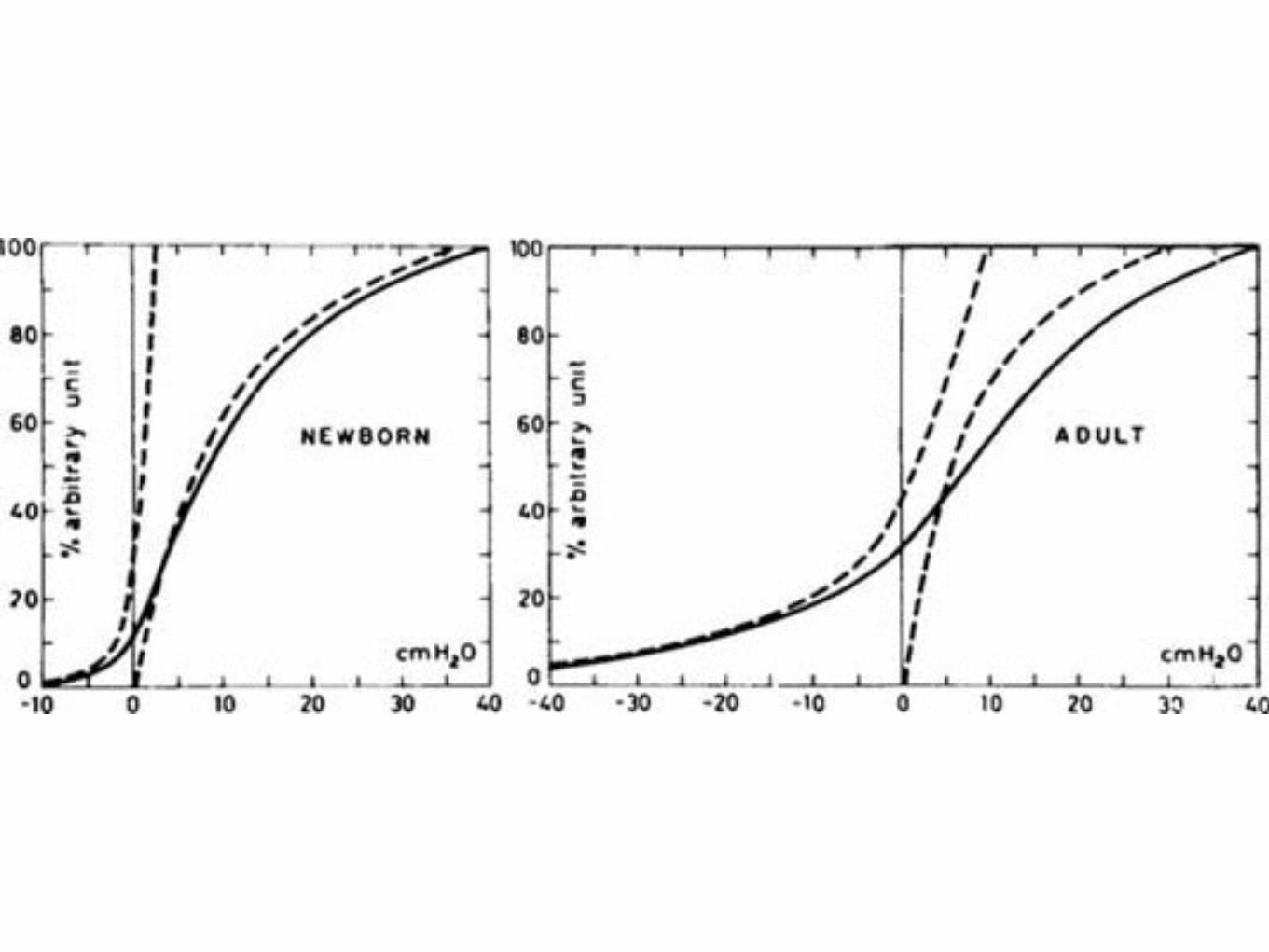
Respiratory Physiology 2
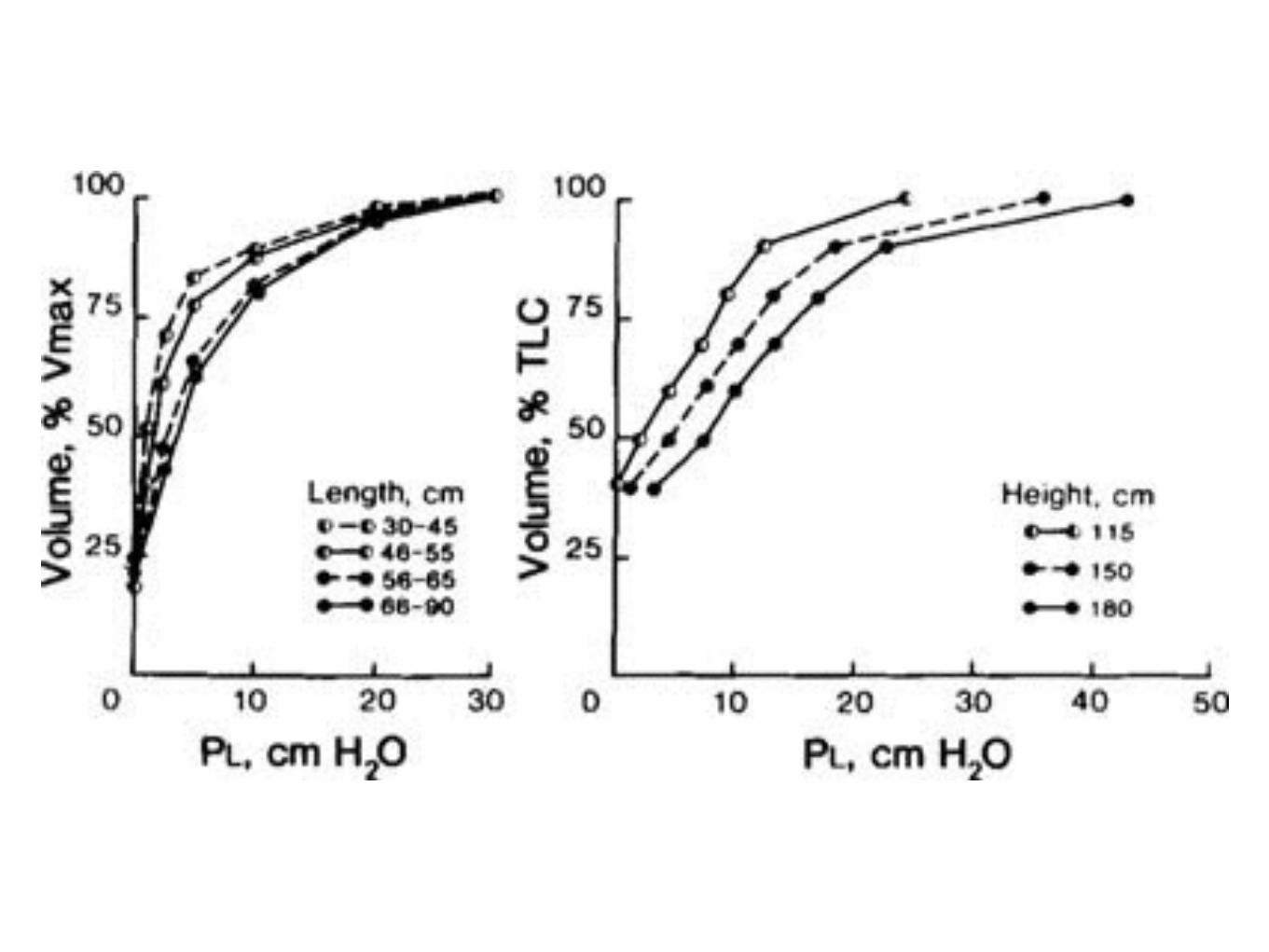
Increased Chest wall compliance = less recoil
Higher Closing Capacity = desat if FRC falls
Decreased TLC: flat diaphragm, horizontal ribs (<5y)
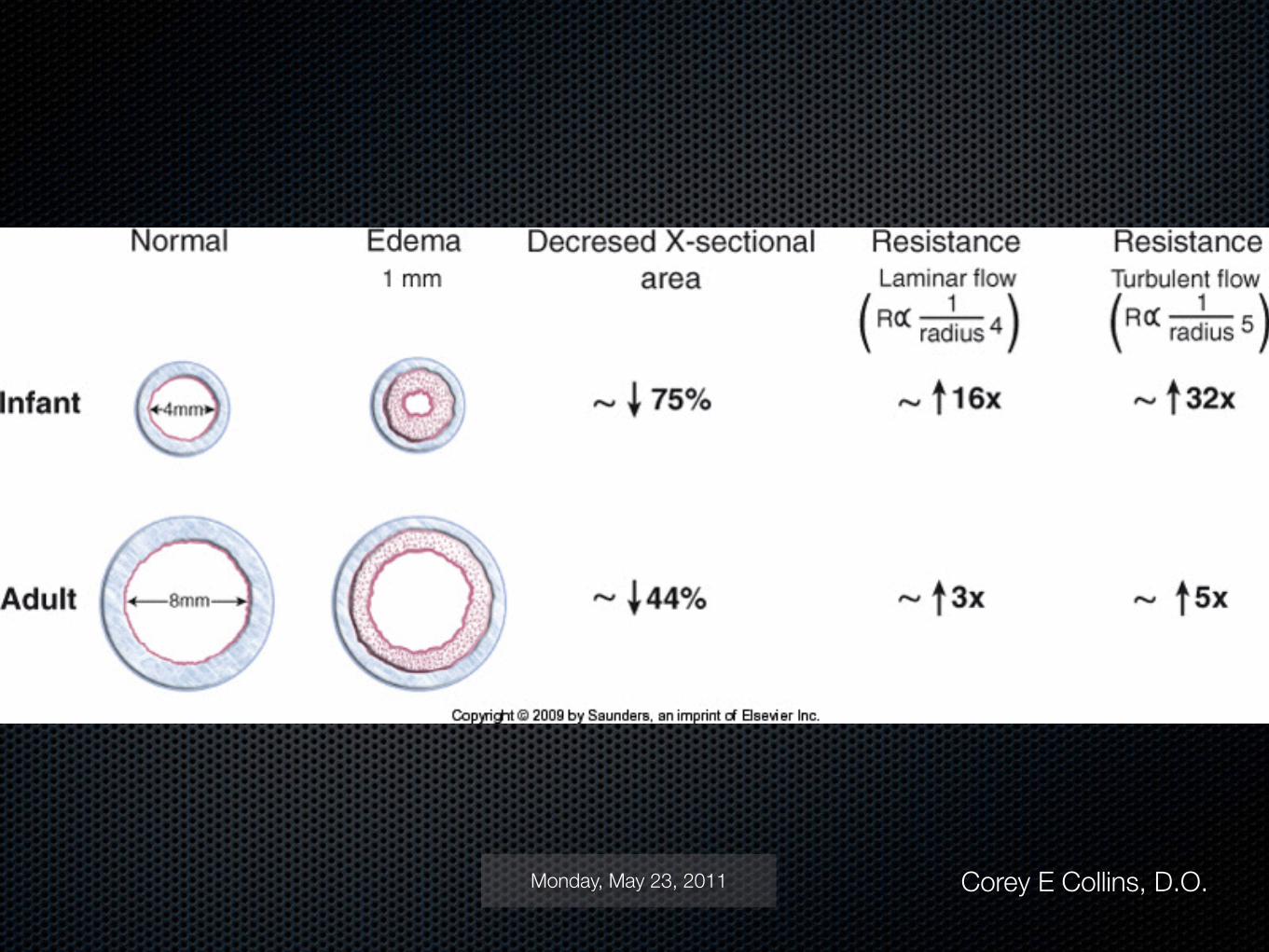
Airway resistance ˆ4th power. Actual diameters are larger :: adults but any decrease will have more effect
“Economy of Breathing”
9
Corey E Collins, D.O.Monday, May 23, 2011
Respiratory Physiology
14
Corey E Collins, D.O.Monday, May 23, 2011
15
Corey E Collins, D.O.Monday, May 23, 2011
Airway Management
Consider need for intervention and risks
Indications
Impaired CNS
Obstruction
Increased Work of Breathing
Hypoxia
16

Corey E Collins, D.O.Monday, May 23, 2011
Face MasksAlways keep a variety of sizes available
17
Corey E Collins, D.O.Monday, May 23, 2011
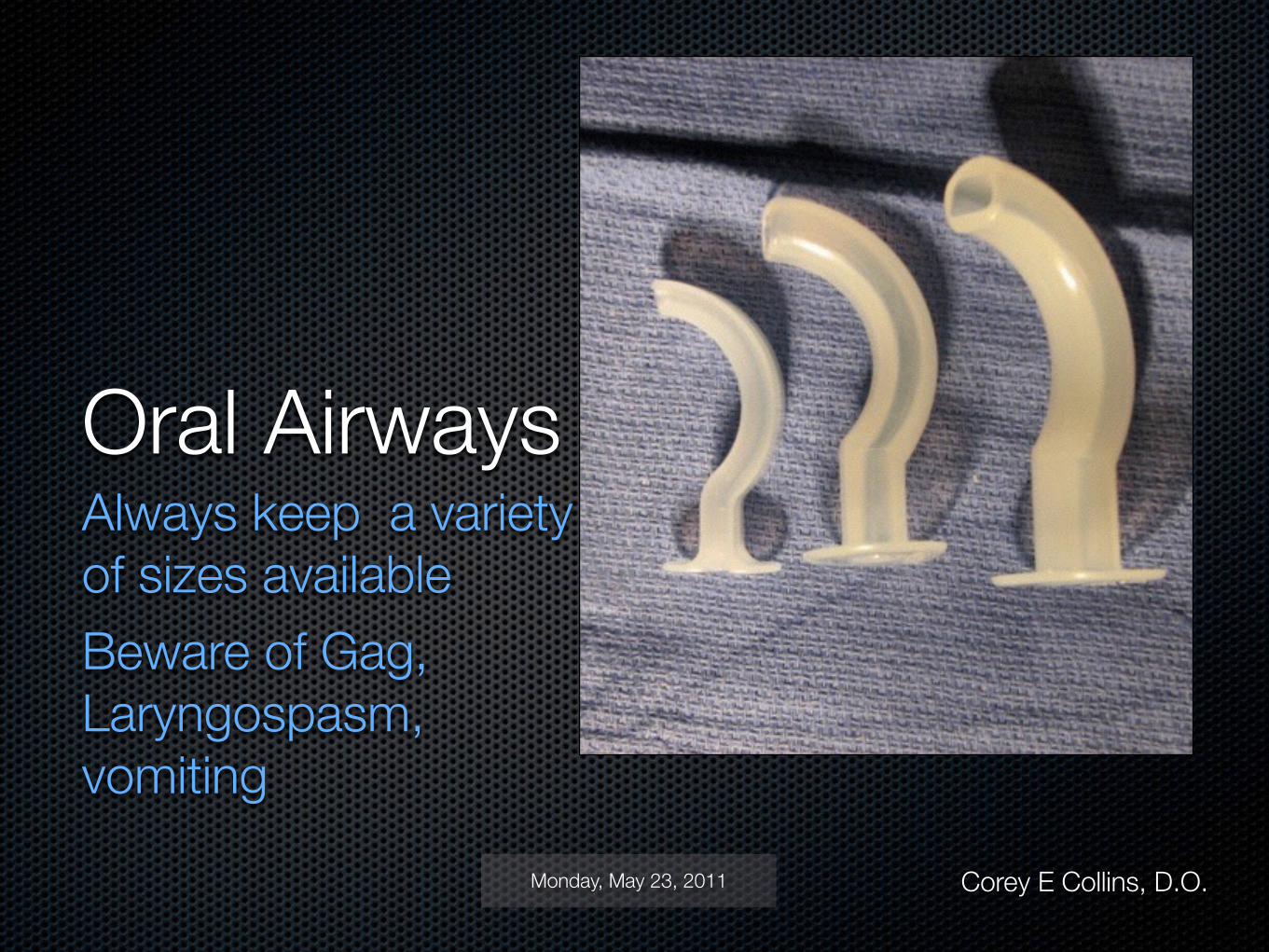
Oral AirwaysAlways keep a variety of sizes available Beware of Gag, Laryngospasm, vomiting
18
Corey E Collins, D.O.Monday, May 23, 2011
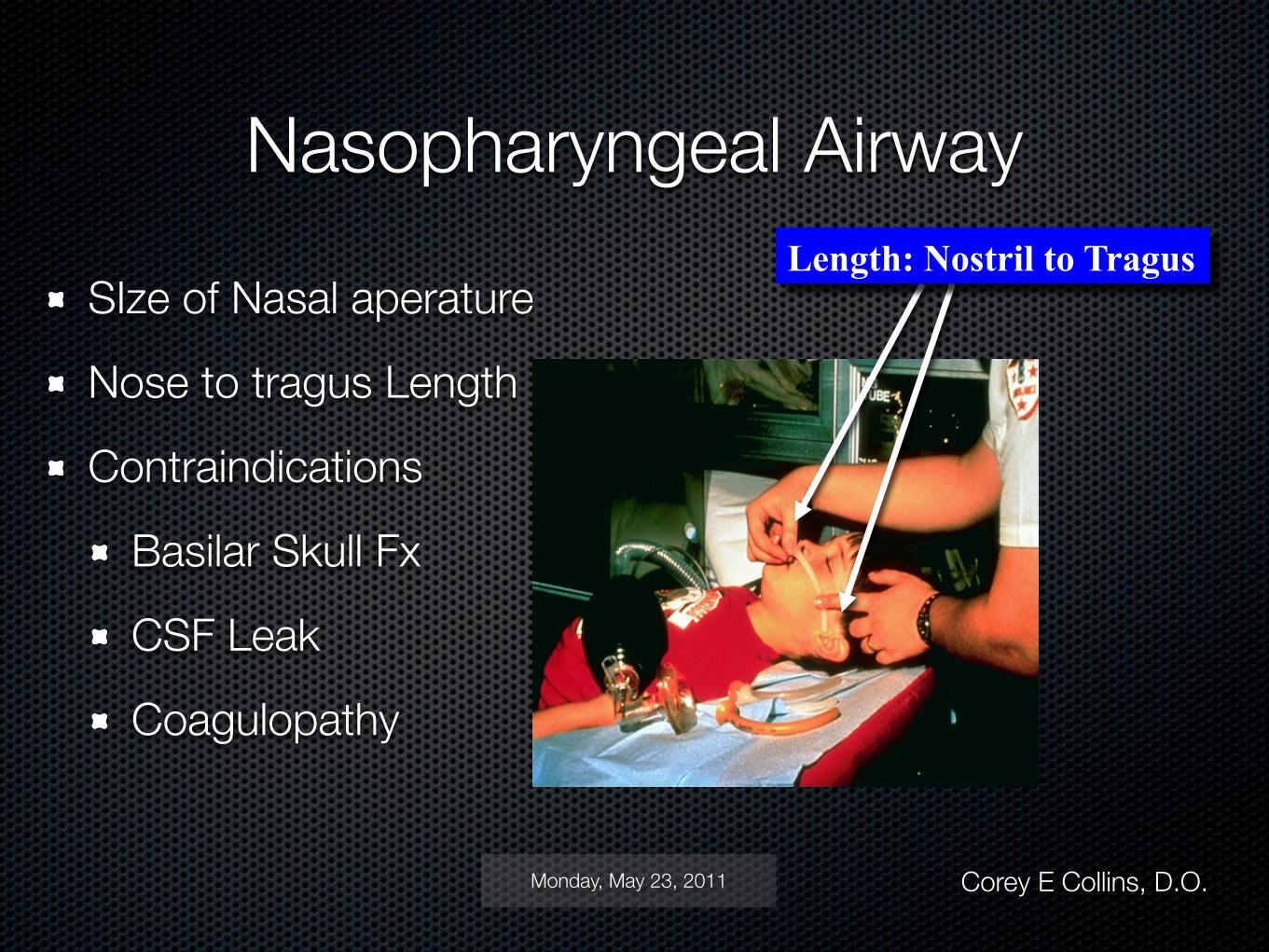
Length: Nostril to Tragus SIze of Nasal aperature
Nose to tragus Length
Contraindications
Basilar Skull Fx
CSF Leak
Coagulopathy
Nasopharyngeal Airway
19
Corey E Collins, D.O.Monday, May 23, 2011
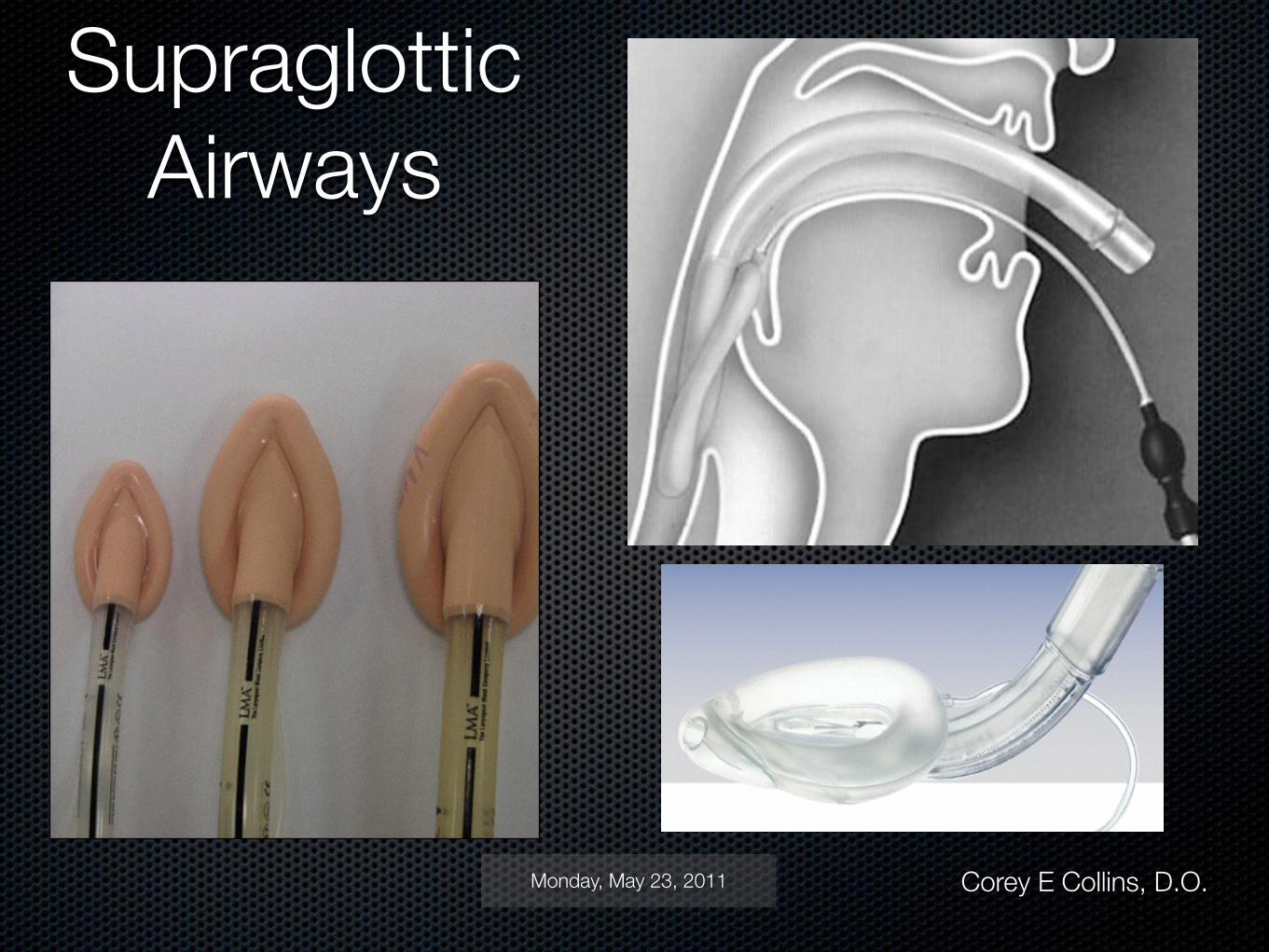
Supraglottic Airways
20
Corey E Collins, D.O.Monday, May 23, 2011
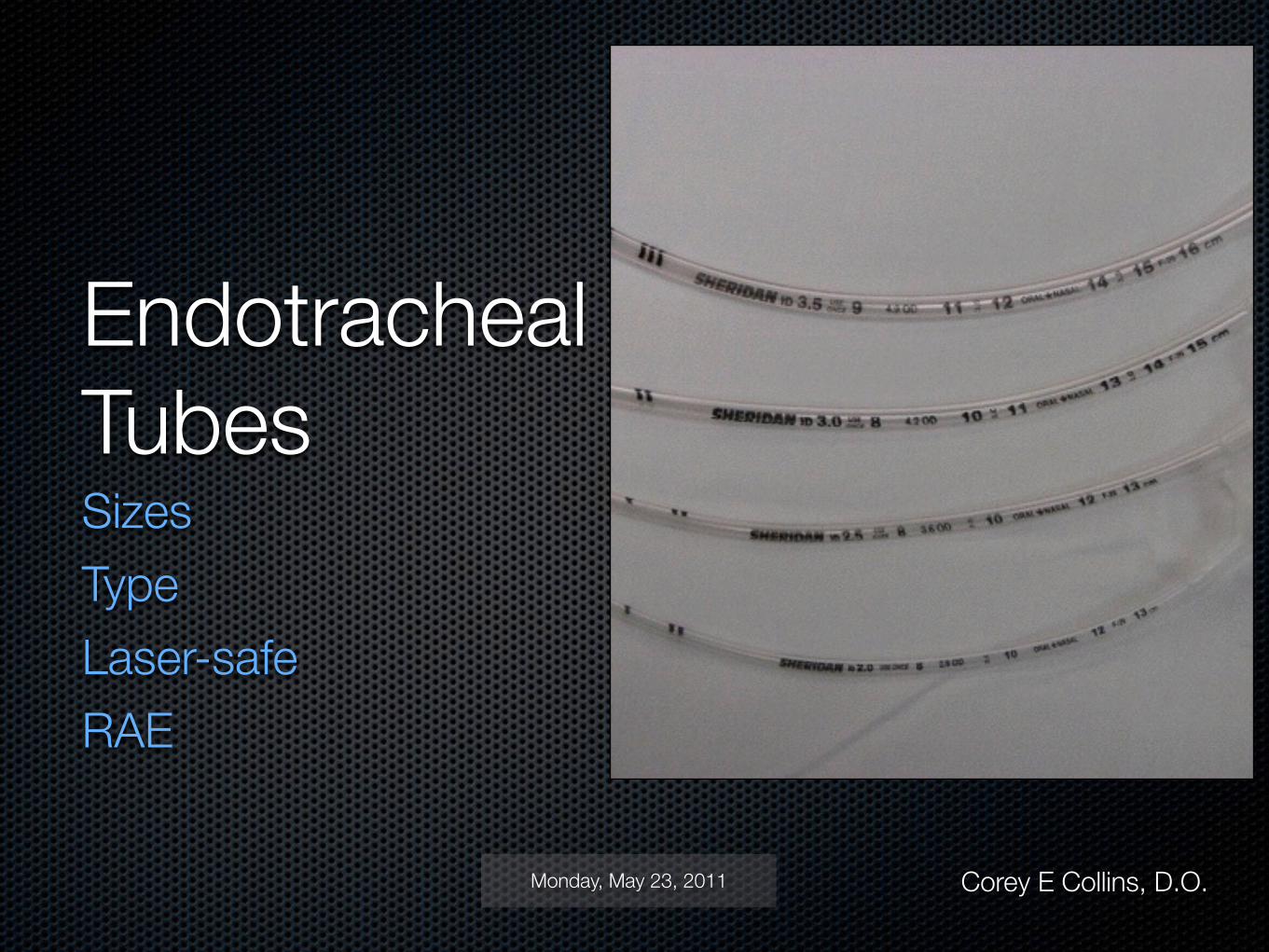
Endotracheal TubesSizes Type Laser-safe RAE
21
Corey E Collins, D.O.Monday, May 23, 2011
Endotracheal Tubes: SizePasses easily through V.C. Into subglottis
Leak < 20 cm H2O
16 + age/ 4
Have 0.5 mm larger and smaller
22
Corey E Collins, D.O.Monday, May 23, 2011
Endotracheal Tubes: Cuff?Reintubation 23% vs 1.2%
Cuff Pressure?
Mucosal Injury?
Aspiration?
Bottom line: safe, smaller, low pressure
23
Corey E Collins, D.O.Monday, May 23, 2011
Endotracheal Tubes: DepthMid tracheal Position
Age/2 +12
3x ETT Size
Withdrawal from Mainstem Bronchus
Concerns: Extubation, Cervical motion, injury, response
24
Corey E Collins, D.O.Monday, May 23, 2011
Adjuncts neededAnticipate problems Have back-up plans for airway issues
25

Corey E Collins, D.O.Monday, May 23, 2011
LaryngoscopesVariety of Sizes Choice of blade: age, personal preference, Anatomy
26
Corey E Collins, D.O.Monday, May 23, 2011
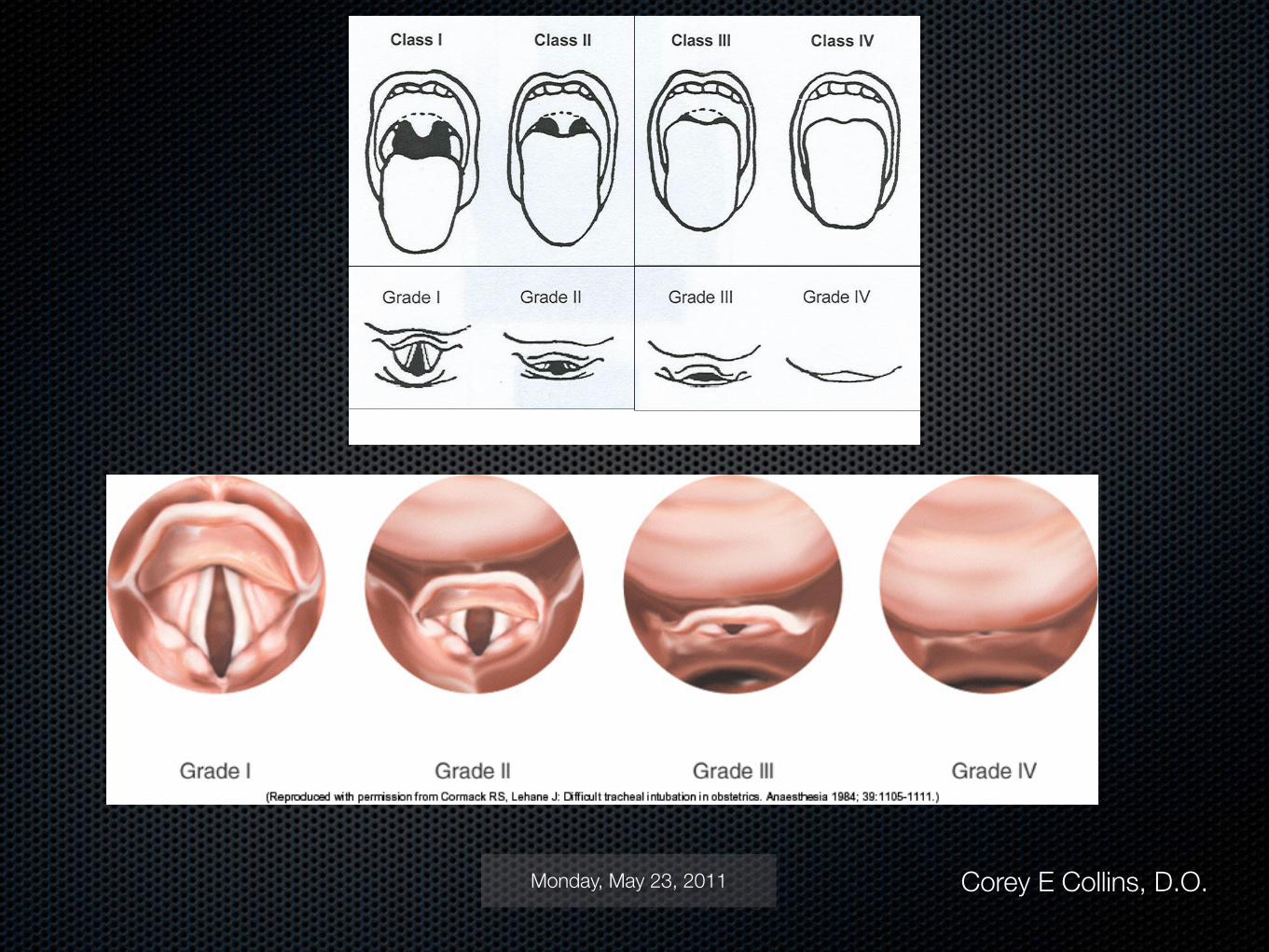
Predictors of Difficult Intubations in Children
Syndromes
Decreased Mobility of Cervical Spine/ TMJ
Small mouth, receding jaw/ large overbite
Trauma
History of Difficult Intubation
27
Corey E Collins, D.O.Monday, May 23, 2011
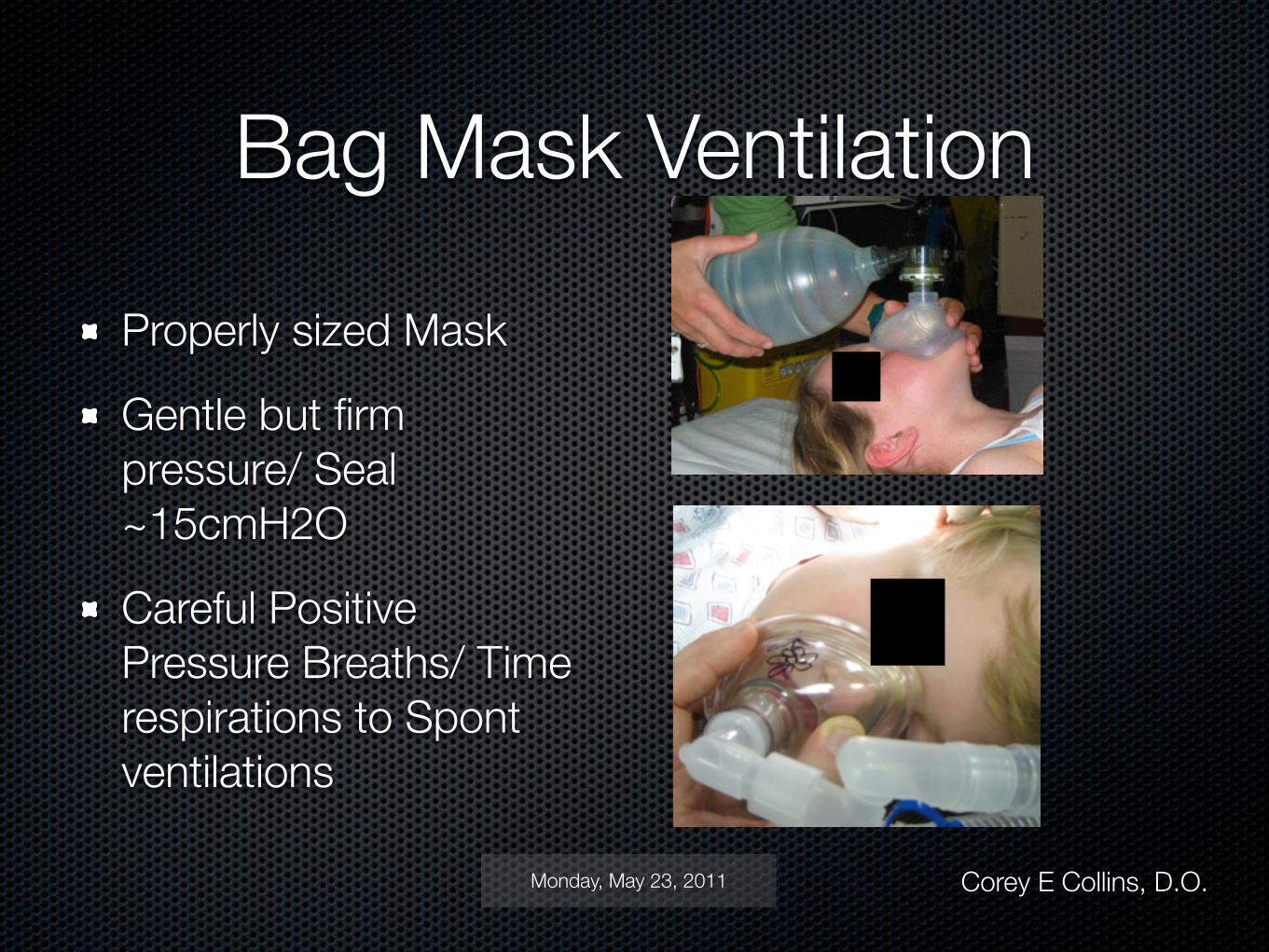
Bag Mask Ventilation
Properly sized Mask
Gentle but firm pressure/ Seal ~15cmH2O
Careful Positive Pressure Breaths/ Time respirations to Spont ventilations
28
Corey E Collins, D.O.Monday, May 23, 2011
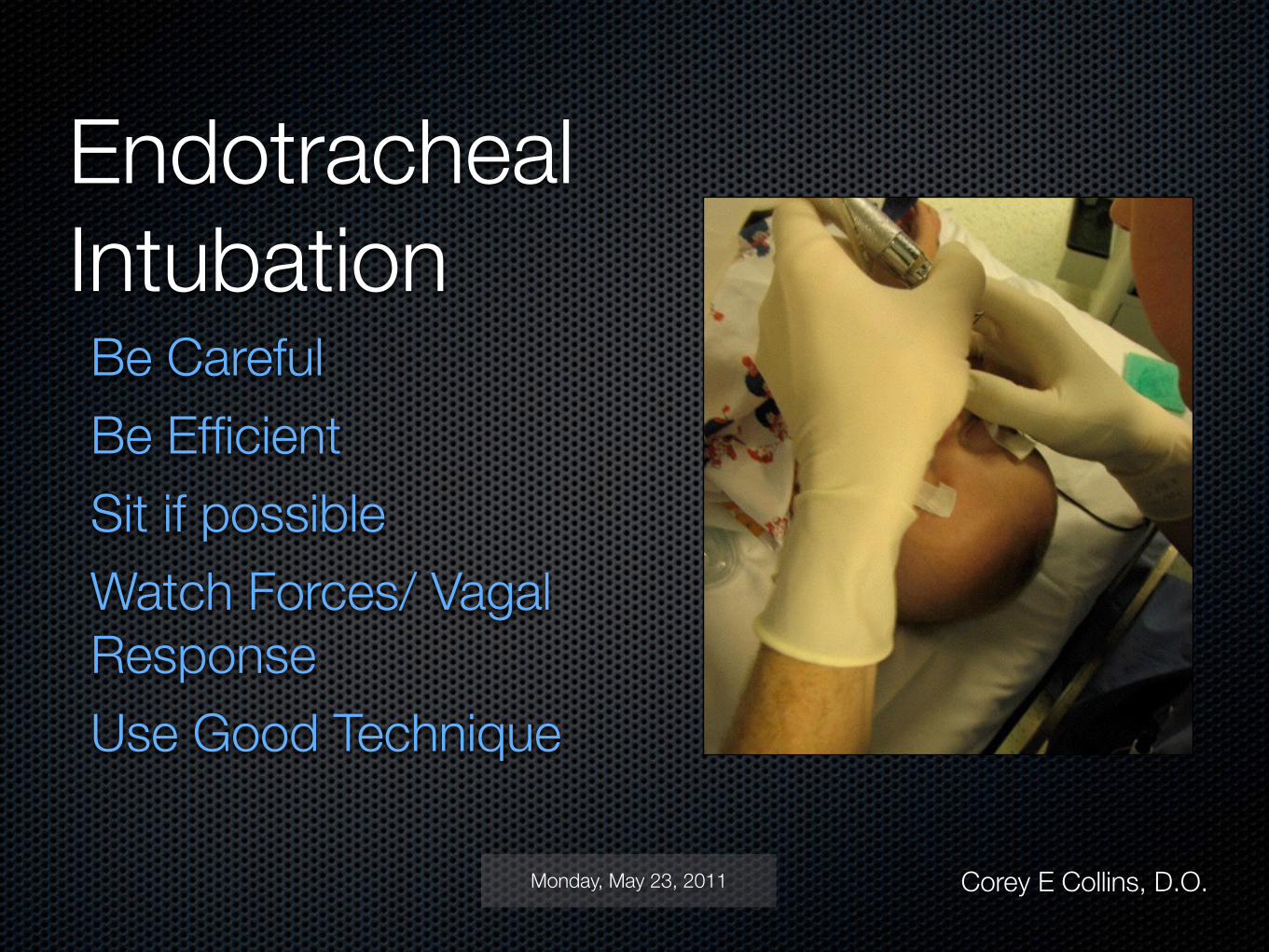
Endotracheal IntubationBe Careful Be Efficient Sit if possible Watch Forces/ Vagal Response Use Good Technique
29
Corey E Collins, D.O.Monday, May 23, 2011
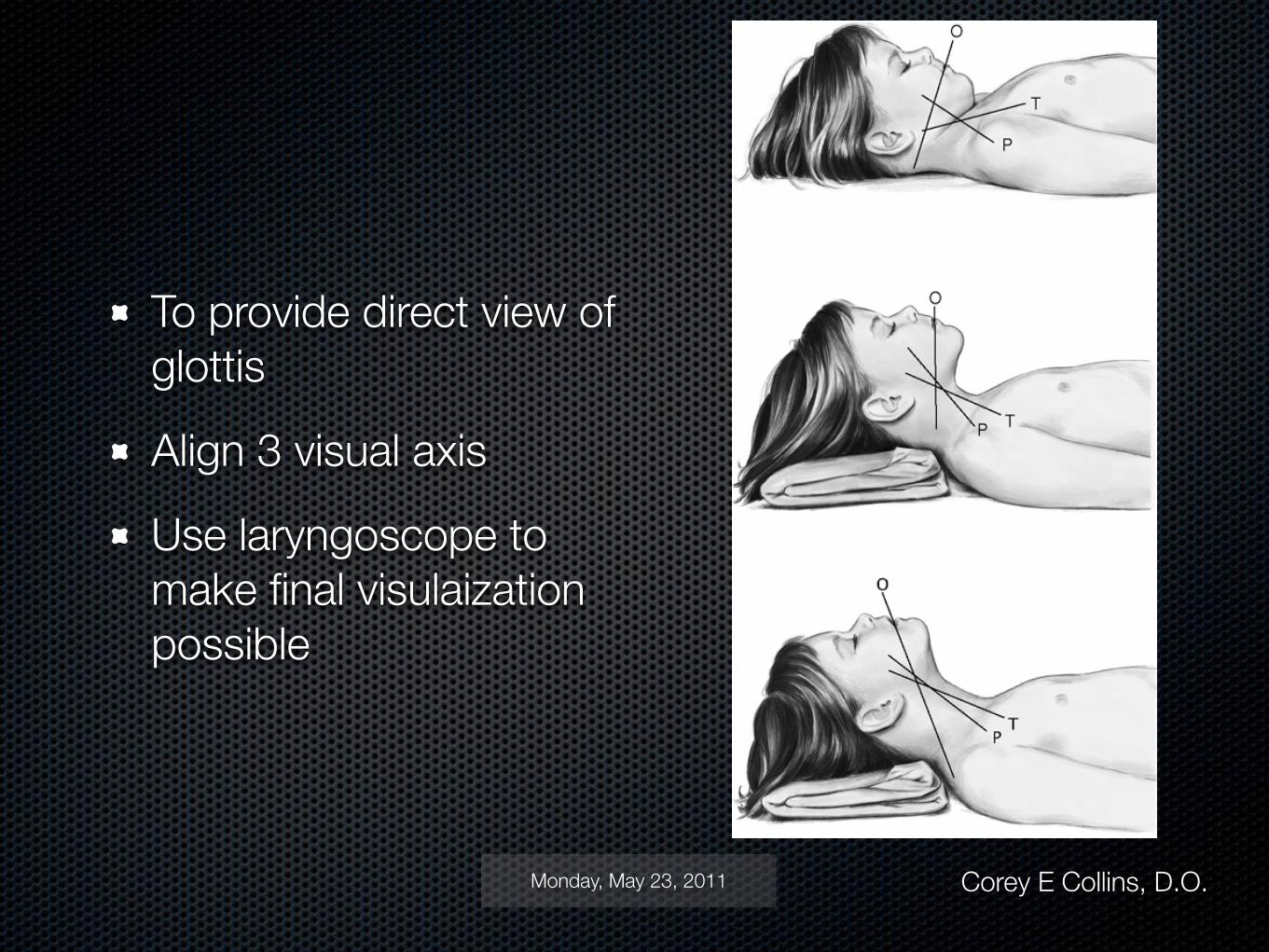
To provide direct view of glottis
Align 3 visual axis
Use laryngoscope to make final visulaization possible
30
Corey E Collins, D.O.Monday, May 23, 2011
laryngeal view when introducing a tracheal tube orother instruments. When open the blade forms an85-degree angle with the handle. It is our experiencethat for trainees and other inexperienced intubatorsthis together with the ease of view encourages thegentle indirect lift of the epiglottis rather than thetemptation to use a levering and potentially moreforceful action as may be the case when using aconventional straight or curved blade. Figures 2, 3and 4.
The McCoy laryngoscope was developed in theearly 1990s to help with difficult intubation in adult
patients (28). Lately a pediatric version of the McCoylaryngoscope, based on the Seward straight blade,has become available. It has been designed to conferthe advantages of the straight blade in aligning thevarious axes in the infant airway whilst allowingthe epiglottis to be lifted with the blade tip in thevallecula. It is suggested that that this should allow aview comparable to that of a straight blade (25).
The two more commonly used intubation aids arethe gum-elastic bougie and the malleable stylet. Thebougie has been used for difficult intubation via theorotracheal and nasotracheal route (29,30). The useof such intubation aids is not free of complicationboth with respect to the equipment used and thepotential for trauma (31,32). Latto et al. found thatalthough the gum-elastic bougie is commonly used,
Figure 2Laryngoscopists view with Cardiff blade (above) and Macintosh(below) to show relative positions of the respective blades whenplaced in the valeculla and the epiglottis is elevated to expose theglottis. The arrow illustrates the direction of lift required to obtainthis view with the Cardiff blade.
Figure 3Miller 1 (above) and Cardiff Blade (below). Two views todemonstrate the difference in blade configuration.
Figure 4Macintosh (above) and Cardiff Blade (below). Two views todemonstrate the difference in blade configuration.
PEDIATRIC LARYNGOSCOPES AND INTUBATION AIDS 33
! 2009 The AuthorsJournal compilation ! 2009 Blackwell Publishing Ltd, Pediatric Anesthesia, 19 (Suppl. 1), 30–37
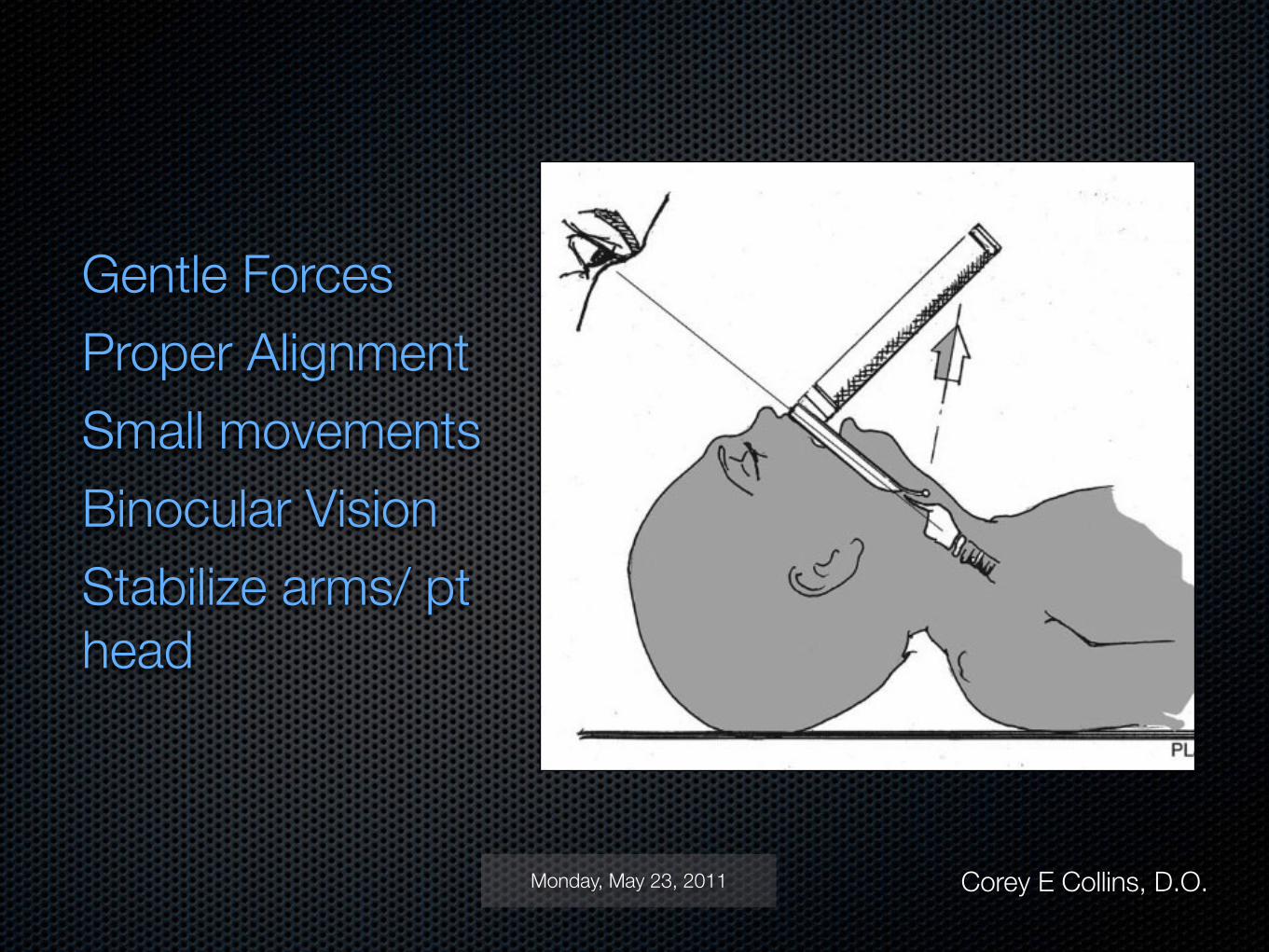
Gentle Forces Proper Alignment Small movements Binocular Vision Stabilize arms/ pt head
31
Corey E Collins, D.O.Monday, May 23, 2011
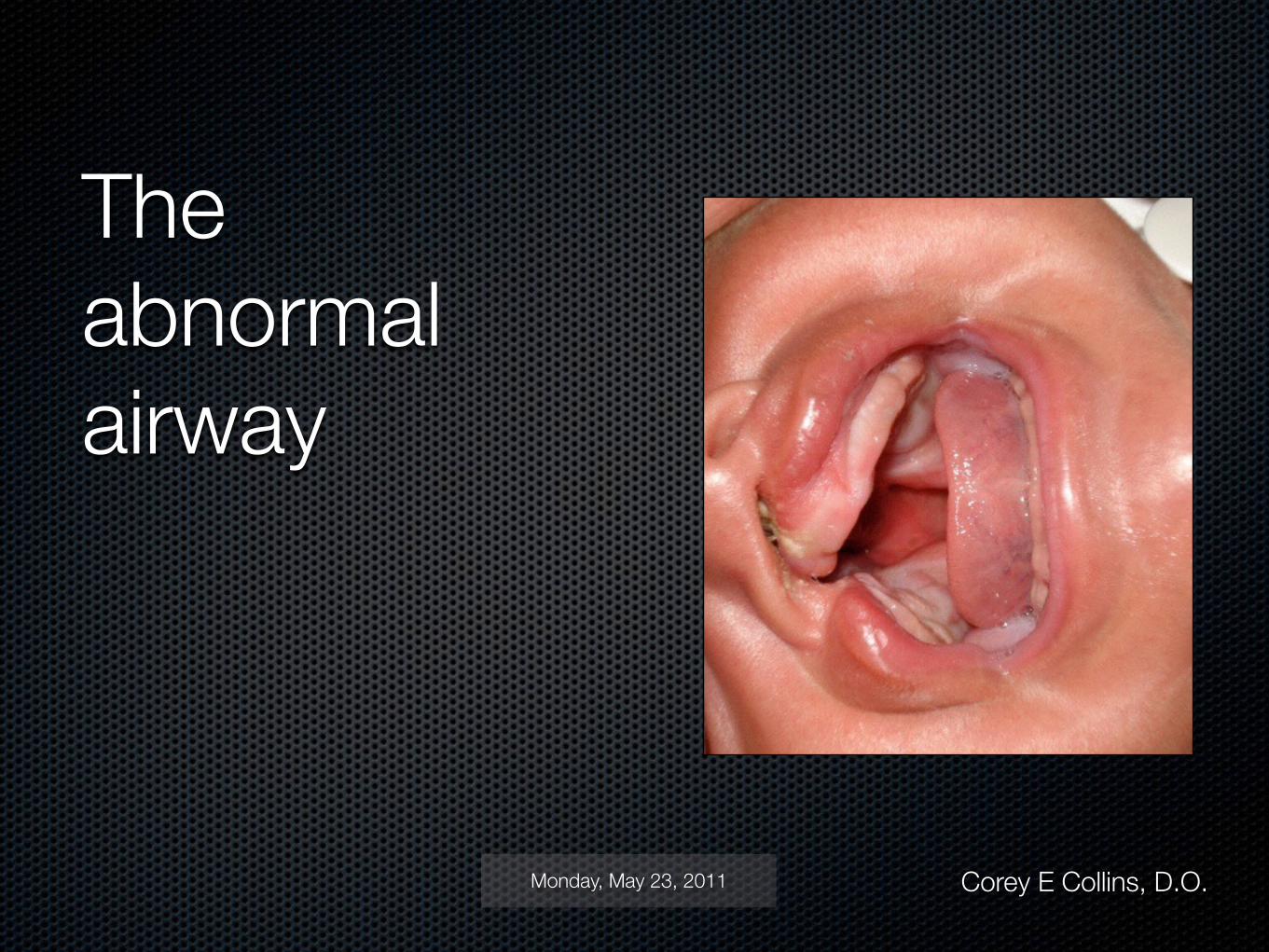
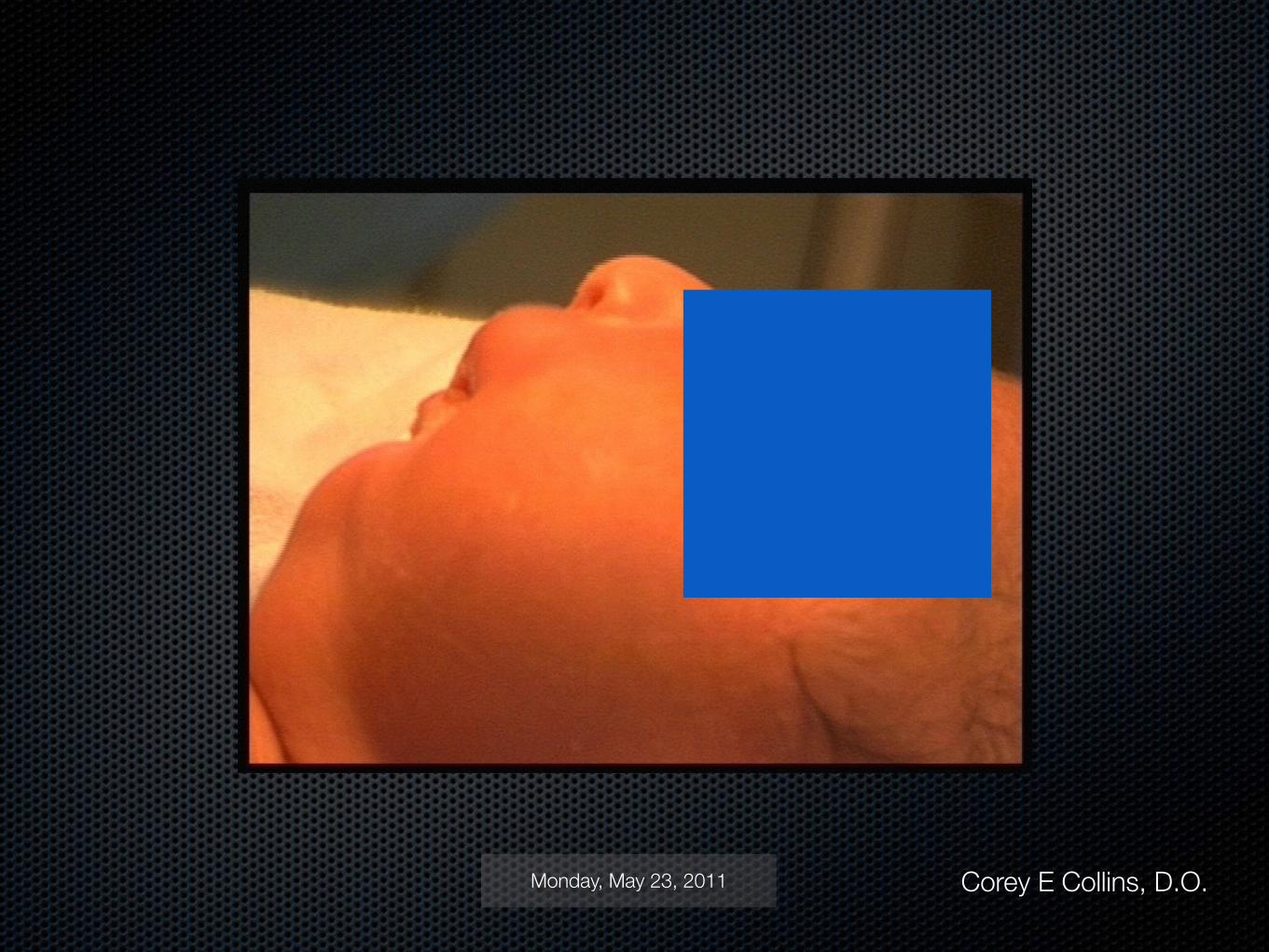
The abnormal airway
32
Corey E Collins, D.O.Monday, May 23, 2011
33
Corey E Collins, D.O.Monday, May 23, 2011
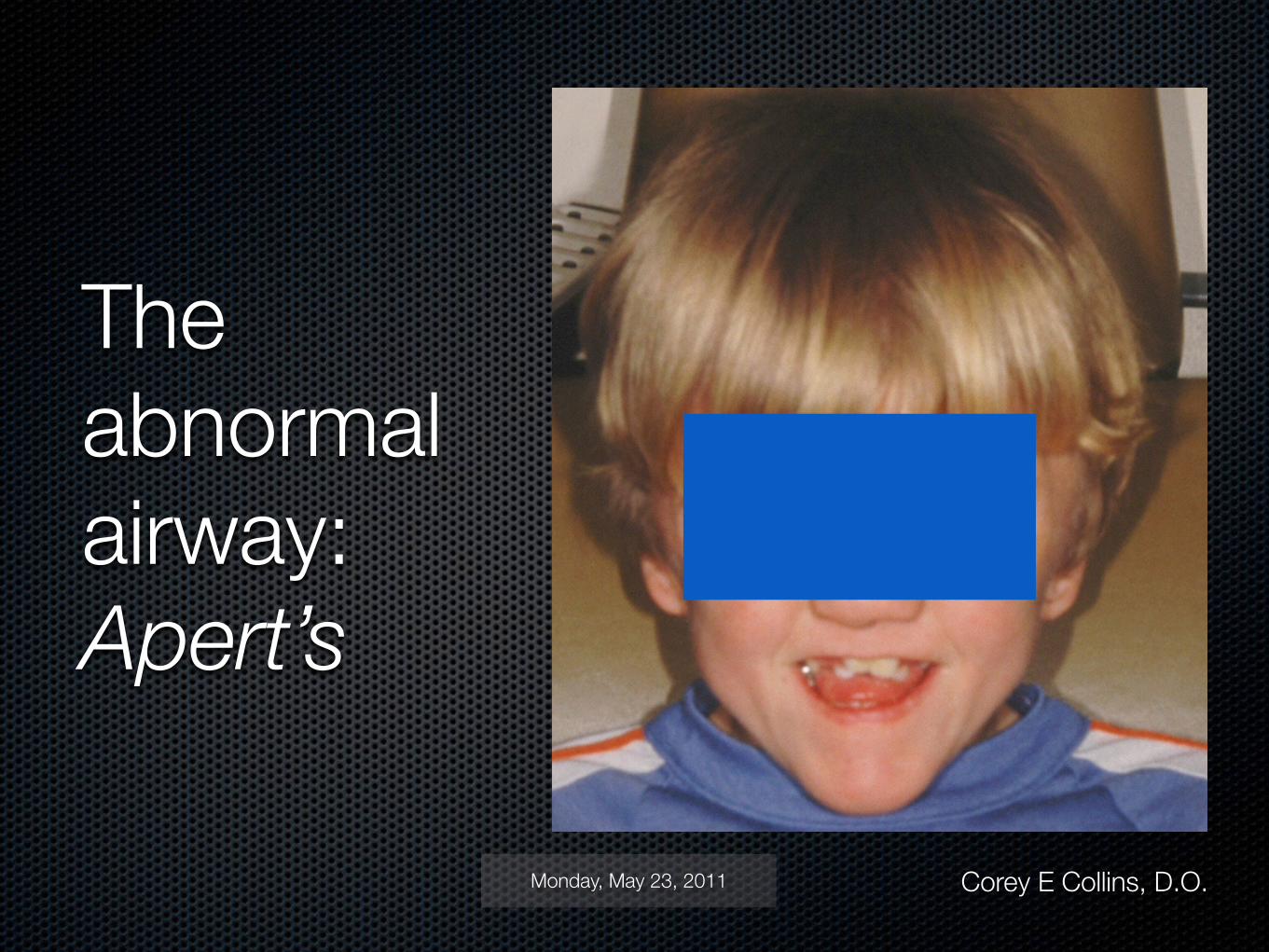
The abnormal airway: Apert’s
34
Corey E Collins, D.O.Monday, May 23, 2011
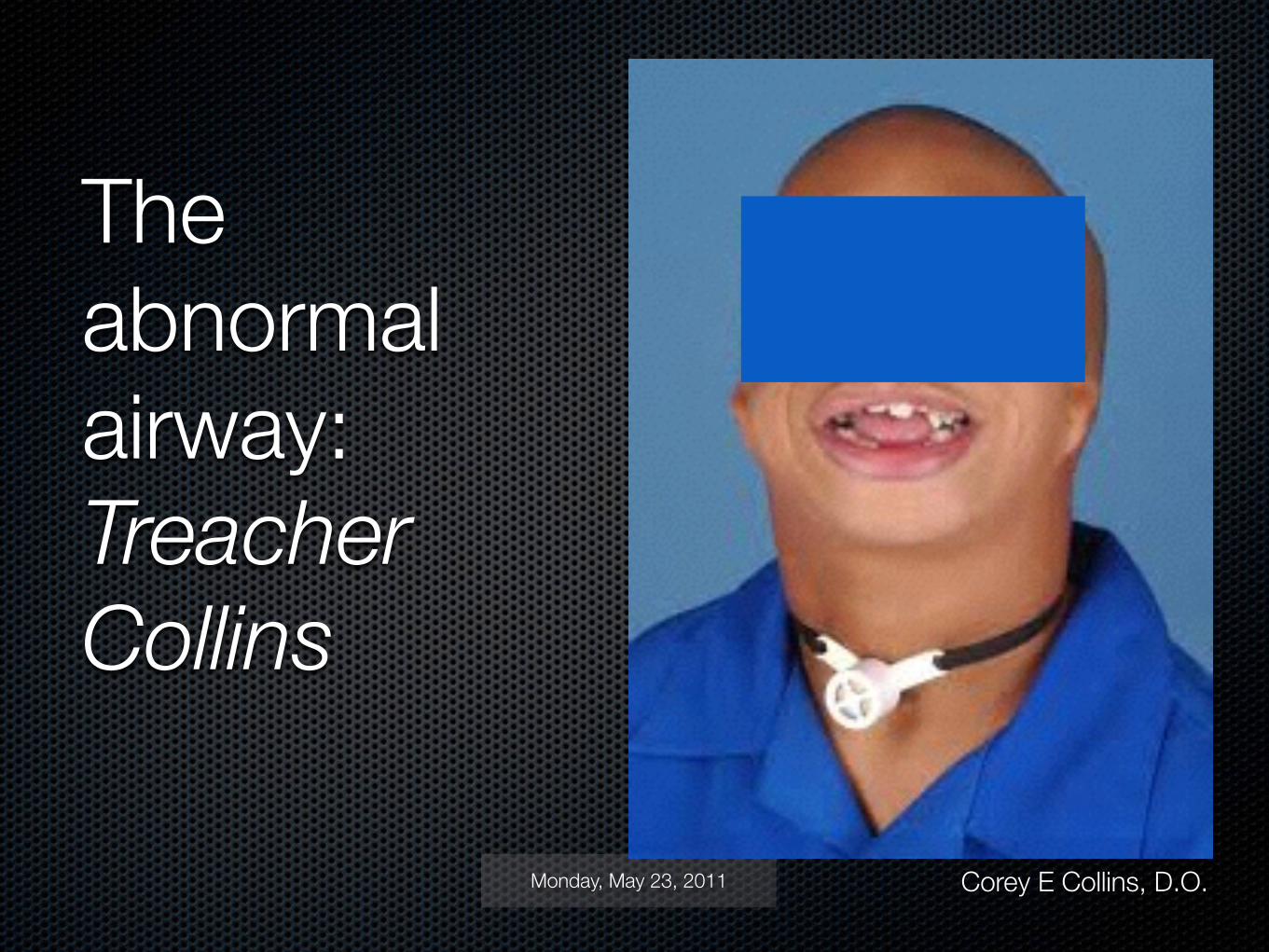
The abnormal airway: Treacher Collins
35
Corey E Collins, D.O.Monday, May 23, 2011
36