
Patterns of chronic inflammation in extensively treated ... · CLINICAL FOCUS: PAIN MANAGEMENT...
6
Full Terms & Conditions of access and use can be found at http://www.tandfonline.com/action/journalInformation?journalCode=ipgm20 Download by: [Fudan University] Date: 22 January 2017, At: 01:34 Postgraduate Medicine ISSN: 0032-5481 (Print) 1941-9260 (Online) Journal homepage: http://www.tandfonline.com/loi/ipgm20 Patterns of chronic inflammation in extensively treated patients with arachnoiditis and chronic intractable pain John A. Bilello & Forest S. Tennant To cite this article: John A. Bilello & Forest S. Tennant (2017) Patterns of chronic inflammation in extensively treated patients with arachnoiditis and chronic intractable pain, Postgraduate Medicine, 129:1, 87-91, DOI: 10.1080/00325481.2017.1270155 To link to this article: http://dx.doi.org/10.1080/00325481.2017.1270155 Accepted author version posted online: 08 Dec 2016. Published online: 17 Dec 2016. Submit your article to this journal Article views: 15 View related articles View Crossmark data
Transcript of Patterns of chronic inflammation in extensively treated ... · CLINICAL FOCUS: PAIN MANAGEMENT...

Full Terms & Conditions of access and use can be found athttp://www.tandfonline.com/action/journalInformation?journalCode=ipgm20
Download by: [Fudan University] Date: 22 January 2017, At: 01:34
Postgraduate Medicine
ISSN: 0032-5481 (Print) 1941-9260 (Online) Journal homepage: http://www.tandfonline.com/loi/ipgm20
Patterns of chronic inflammation in extensivelytreated patients with arachnoiditis and chronicintractable pain
John A. Bilello & Forest S. Tennant
To cite this article: John A. Bilello & Forest S. Tennant (2017) Patterns of chronic inflammationin extensively treated patients with arachnoiditis and chronic intractable pain, PostgraduateMedicine, 129:1, 87-91, DOI: 10.1080/00325481.2017.1270155
To link to this article: http://dx.doi.org/10.1080/00325481.2017.1270155
Accepted author version posted online: 08Dec 2016.Published online: 17 Dec 2016.
Submit your article to this journal
Article views: 15
View related articles
View Crossmark data
CLINICAL FOCUS: PAIN MANAGEMENTORIGINAL RESEARCH
Patterns of chronic inflammation in extensively treated patients with arachnoiditisand chronic intractable painJohn A. Bilelloa and Forest S. Tennantb
aAtlantic Diagnostic Laboratories, Bensalem, PA, USA; bVeract Intractable Pain Clinic, West Covina, CA, USA
ABSTRACTObjective: To use biomarkers to gain insight into and gauge the residual (post-treatment) level ofinflammation in two groups of intensively treated patients with severe chronic pain.Methods: Three study groups were analyzed, and included: (i) patients (n = 90) with chronic intractablepain (CIP), (ii) patients (n = 26) with chronic pain and MRI-documented arachnoiditis (ARC) and (iii)normal subjects without a diagnosis of chronic pain (n = 86). We determined and compared the serumconcentrations of Alpha-1 Antitrypsin (A1AT), Myeloperoxidase (MPO) and soluble Tumor NecrosisFactor receptor type 2 (sTNFR2) in each of the patient populations studied.Results: Patients treated for ARC or CIP had higher serum levels of A1AT and MPO than normaluntreated subjects without a diagnosis of chronic pain. ARC patients had an A1AT mean serumconcentration of 167.9 ± 41.9 mg/dL as compared to 148.9 ± 35.2 mg/dL for normal subjects(p = 0.023). CIP patients had the highest mean serum A1AT level 183.6 ± 39.2 mg/dL with p valuesof <0.0001 or 0.08 when compared to normal subjects or ARC patients respectively. ARC patients had anMPO mean serum concentration of 344.6 ± 227.9 ng/mL as compared to 188.2 ± 107.5 ng/mL fornormal subjects (p = < 0.0001). CIP patients had a similar mean serum MPO level of 352.3 ± 164 ng/mLwith p values of <0.0001 or 0.85 when compared to normal subjects or ARC patients respectively. Inaddition, we noted a difference in the pattern of MPO expression in patients with ARC in that 34% hadlevels of MPO at normal or below and 31% had levels 2-fold or greater than normal.Conclusion: This data supports the concept that in centralized pain, sites of neuroinflammationelaborate MPO and other inflammatory factors which may not be completely cleared from the systemdespite extensive and complex treatment regimens.
ARTICLE HISTORYReceived 27 October 2016Accepted 6 December 2016
KEYWORDSInflammation; arachnoiditis;biomarkers; intractable; pain
1. Introduction
Severe chronic pain is one of the most intractable and difficultsyndromes to treat successfully. Chronic pain is usuallydefined as any persistent or intermittent pain that lasts morethan 3 months [1,2]. Inflammation and pain usually go hand-in-hand, since tissue injury initiates the inflammatory processresulting in a cascade of biochemical reactions that prime thenervous system for pain sensing [3–6]. Moreover, long-terminflammation reinforces adaptive changes in the nervous sys-tem that can cause the sensation of pain to become exagger-ated, chronic, and can affect a specific part of the body orencompass multiple regions [7–9]. In particular, there is asubgroup of patients that has a chronic intractable pain (CIP)syndrome or disease, all have incurable, extremely painfulconditions, as evidenced by failure of various interventionsto control their pain, including surgery, nerve blocks, physicalrehabilitation, and some opioids. These patients may be non-functional, bedridden, or housebound and often suffer fromfatigue, insomnia, depression, and anxiety. Objective assess-ment invariably reveals intermittently elevated blood pressureand pulse rate and abnormal concentrations of serum cortisoland other adrenal hormones, indicating the presence of a
severe and extended stress state [9–11]. In clinical practice,CIP patients are often considered to have a central pain syn-drome when affected individuals have multifocal pain com-bined with other somatic symptoms indicated earlier.Arachnoiditis (ARC) is a chronic pain condition caused by aninflammation of the arachnoid lining—one of the three liningsthat surrounds the brain and spinal cord [12]. While somewhatrare, the most severe cases of ARC are associated with intenselumbar pain. Physiologically, ARC is a nonspecific inflamma-tory process usually caused by an invasion into the dural sac—whether by bacteria, blood, or injections of various irritantsubstances that produce a spectrum of pathological changesoriginating on the arachnoid membrane. The resulting inflam-matory response eventually proliferates to other intrathecalneural elements leading to fibrosis and adhesions that involvethe nerve roots, the arachnoid, the spinal cord, and the duramater. This progression culminates in permanent disabilitycharacterized by severe intractable pain, neurological deficit,and other related symptoms.
While the pathophysiology of ARC and CIP are very differ-ent, nonetheless, both ARC and CIP are highly debilitatingconditions which require extensive and complex treatment.The goal of such treatment is to improve a patient’s function
CONTACT John A. Bilello [email protected] Atlantic Diagnostic Laboratories, 3510 Progress Drive, Bensalem, PA 19020, USA
POSTGRADUATE MEDICINE, 2017VOL. 129, NO. 1, 87–91http://dx.doi.org/10.1080/00325481.2017.1270155
© 2016 Informa UK Limited, trading as Taylor & Francis Group

and quality of life by reducing inflammation and alleviatingsymptoms, especially pain.
The primary objective of this studywas to determine if we cangain insight into and gauge the residual (post-treatment) level ofinflammation in chronic pain states. While biomarker measure-ments of inflammatory biomarkers in cerebral spinal fluidmay bean interesting investigative tool for neuroinflammation, they aredifficult to use in routine patient monitoring—particularly whenmultiple tests on severely compromised patients are proposed.We have focused our study on inflammatory mediators in theserum of patients, since the eventual application of such mea-surements to the clinical monitoring of patients with severe painwould be less invasive.
2. Materials and methods
2.1. Pain patient populations and normal subjects
The three study groups analyzed include (a) patients withchronic intractable pain (CIP) from the Veract Intractable PainClinic (n = 90), (b) patients with a diagnosis of ARC (n = 26),and (c) a series of prospectively collected sera from subjectswithout chronic pain. Samples were collected from patientsduring the years 2012–2016 and were stored at a temperaturelower than −80°C prior to assay.
Gender and age distribution of the subjects are given inTable 1. The ARC group was a prospective collection ofpatients who presented with severe pain and whose MRIconfirmed the diagnosis. Twenty ARC patients (77%) werefemale and six (23%) were male. The average body massindex (BMI) for ARC females was 27.0 ± 4.1 (range 19.0–31.8).ARC males had an average BMI of 26.6 ± 2.7 (range 21.6–2.7)
The CIP study group consisted of 56 (62%) females and 34(38%) males. The average BMI for females was 26.5 ± 7.8(range: 13.3–48.7). Males had an average BMI of 27.9 ± 4.8(range: 19.6–40.9).
There were no specific exclusion criteria for pain patientsbased upon gender or other comorbidities; patients 18 yearsand younger were excluded. All medications were allowed;while they represent potential confounders, they were sub-stantially diverse and often used in combination and essentialfor the patient’s well-being.
Samples from healthy normal subjects (non-pain) wereobtained from the Brain Institute of the University of Utah(n = 9) Caritas St. Elisabeth Medical Center (Boston, MA)(n = 3). These 12 patients were selected based upon clinicalinterviews at both academic sites. A series of serum samplesfrom normal subjects (n = 31) with no history of neurologicdisease, mood disorders, or chronic pain were obtained from acommercial source (PrecisionMed, San Diego, CA). In addition,we procured serum samples prospectively from healthy volun-teers in both San Diego, CA (n = 9), and Durham, NC (n = 35).Non-pain subjects from local sources were excluded if they
were taking drugs for chronic pain (e.g. opioids, NSAIDS, anti-depressants). The quality of life in the normal volunteer popu-lation was assessed using the PHQ-9 [13]; subjects with PHQ-9scores >5 were excluded. Female subjects without chronicpain (n = 40) had an average BMI of 25.0 ± 6.4 as comparedto males (n = 46) who had an average BMI of 27.7 ± 4.8.
2.2. Sample collection and handling
Each study subject provided a blood sample, which was pro-cessed to collect serum. The sites prepared serum under stan-dardized conditions. Briefly, blood was allowed to clot for30 min, centrifuged 10 min at 1300 × g (relative centrifugalforce) to collect serum that was aliquoted within 30 min ofcentrifugation. Serum samples were promptly shipped at 4°C(or frozen at −80°C until ready for shipment on dry ice) to theRidge Diagnostics CLIA Laboratory (Research Triangle Park, NC).The date and time of the blood draw was recorded by the studysite for each sample, along with subject gender, height, andweight. All samples were identified by a sequentially appliedaccession number which blinded the technician doing testing tothe source of the sample and patient identifiers.
2.3. Serum biomarker assays
Serum levels of alpha-1 antitrypsin (A1AT), myeloperoxidase(MPO), and soluble tumor necrosis factor alpha receptor type II(sTNFR2) were measured by validated individual quantitativeimmunoassays. Standard curves for calibrating the quantity ofeach biomarker were generated by non-serial dilution of eachpurified protein. Normal reference ranges (mean ± 2SD) for eachbiomarker were previously determined from a large healthycontrol group; gender-specific differences in normal referenceranges were observed for some analytes. A1AT serum concen-trations were measured by an analytically validated immunotur-bidimetric assay developed at the Ridge Laboratory. sTNFR2levels in serum were quantified using ELISA kits (Quantikine,R&D Systems/BioTechne, Minneapolis, MN). MPO was quantifiedusing an ELISA kit (ALPCO, Salem, NH).
2.4. Calculations
Age, gender, height, and weight of each subject were recordedand BMI was calculated using the formula BMI = (weight in lbs.× 703)/(height in inches)2 and an online calculator [http://www.mayoclinic.com/health/bmi-calculator/NU00597]. Probability (pvalues) was calculated using the Student’s t-test to assess thestatistical significance of differences in mean serum concentra-tion of each biomarker between the chronic pain populationsand healthy subjects without chronic pain.
3. Results
3.1. Chronic inflammatory biomarkers in patients withchronic pain
We measured the serum concentrations of three biomarkers ofchronic inflammation: A1AT, MPO, and sTNFR2. Box Whiskerplots (Figure 1) show significant variation in serum levels of
Table 1. Patient demographics.
Group Females Males Age Range
Arachnoiditis 20 6 47.9 ± 10.2 20–72CIP 56 34 48.5 ± 10.4 24–72Non-pain 40 46 42.7 ± 13.9 20–72
88 J. A. BILELLO AND F. S. TENNANT

the inflammatory biomarker A1AT in chronic pain patients andnormal subjects. ARC patients had an A1AT mean serum con-centration of 167.9 ± 41.9 mg/dL (range 87–263 mg/dL) ascompared to 148.9 ± 35.2 mg/dL (range 55–260) for normalsubjects (p = 0.023). CIP patients had a mean level of183.6 ± 39.2 mg/dL (range 105–281) with p-values of<0.0001 or 0.08 when compared to normal subjects or ARCpatients, respectively.
ARC patients had a mean serum MPO level of344.6 ± 227.9 ng/mL (range 94–1245 ng/mL) which was higherthan the mean concentration for normal subjects,188.2 ± 107.5 ng/mL (range 38–567) (p = < 0.0001). CIP patientshad a mean serum MPO level of 352.3 ± 164 ng/mL (range105–928) with p-values of <0.0001 or 0.85 when compared tonormal subjects or ARC patients, respectively (Figure 2).
In contrast to A1AT and MPO, ARC patients had serumlevels of sTNFR2 which were not statistically different fromthat of normal subjects. The mean serum level for ARCpatients was 2636 ± 719 pg/mL (range 1686–4221 pg/mL) as
compared to normal subjects 2548 ± 667 pg/mL (range1633–5798), p = 0.56. CIP patients had a mean sTNFR2 serumconcentration of 3128 ± 1203 pg/mL (range 1154–7727), withp-values of <0.0001 or 0.05 when compared to normal sub-jects or ARC patients, respectively (Figure 3).
3.2. Patterns of chronic inflammatory biomarkerexpression in patients with ARC
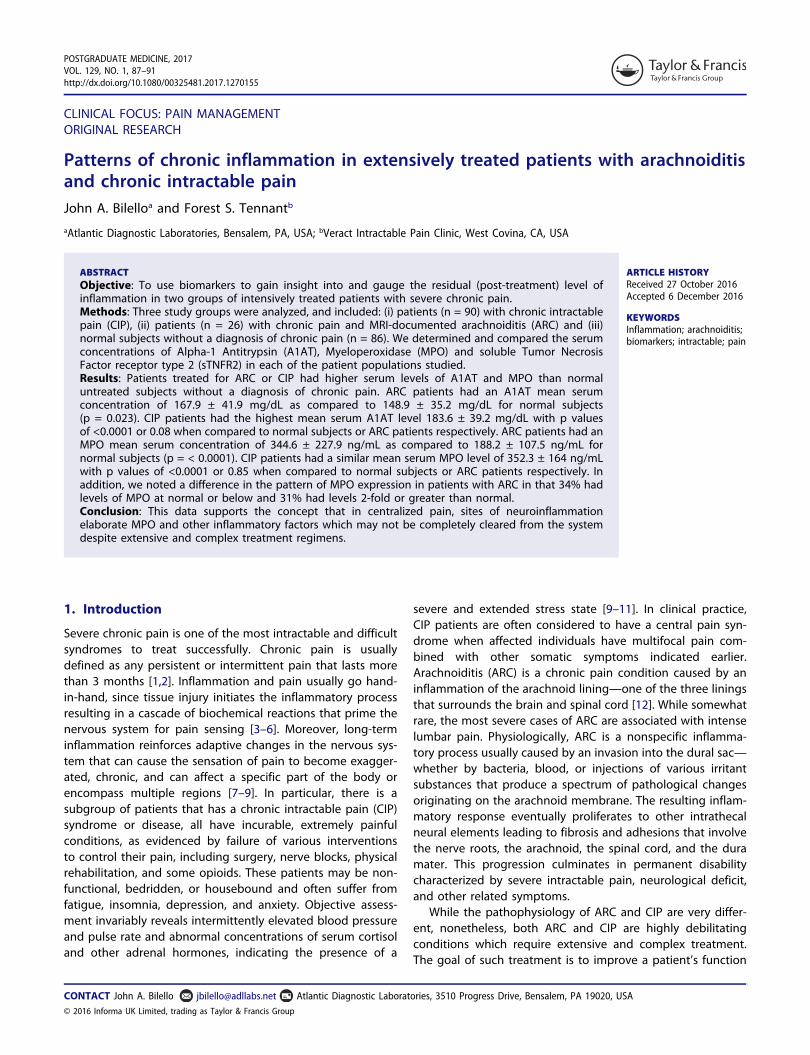
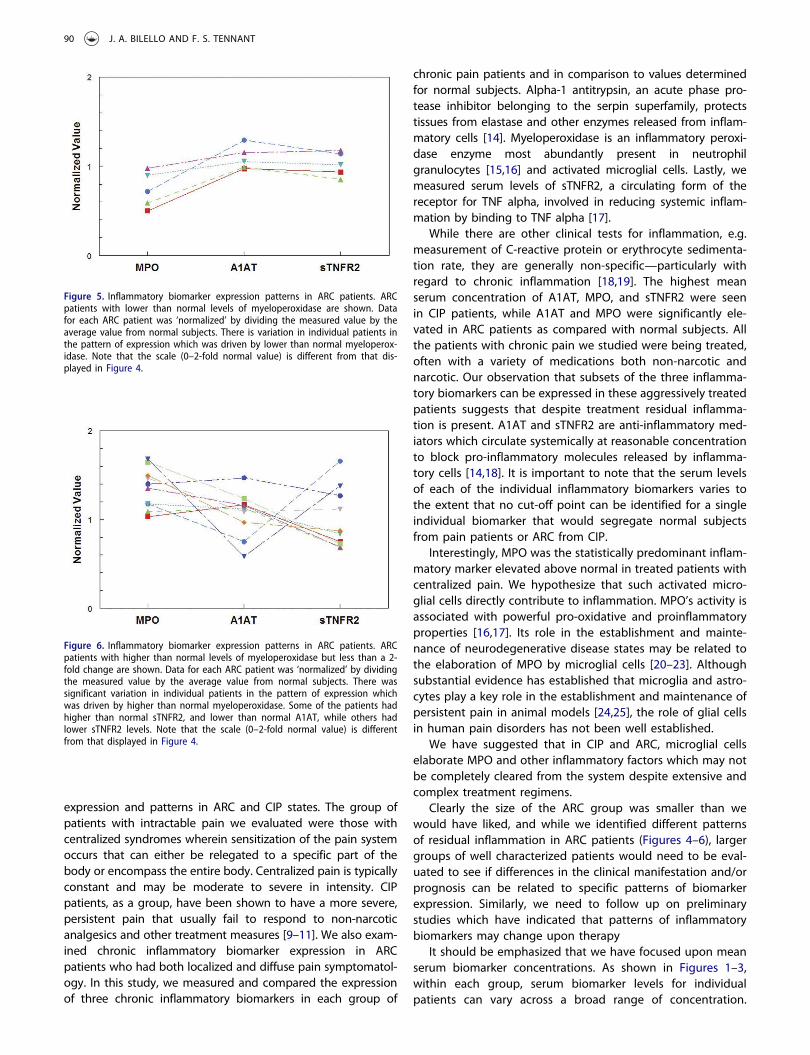
We noted significant variation in the pattern of MPO expres-sion in patients with ARC in that 38% had MPO serum levels 2-fold or greater than normal (Figure 4) and 19.2% had levels ofMPO at normal or below (Figure 5). There were also a signifi-cant number of ARC patients with intermediate serum levelsof MPO shown in Figure 6.
4. Discussion
In this study of two pain populations and one normal controlgroup, we gained physiological information on biomarker
Figure 2. Box Whisker plots of MPO levels in serum. Data for ARC and CIPpatients is plotted as indicated in Figure 1 above. The p-value indicated is forthe comparison of ARC patients to control non-pain subjects and CIP patients.The p-value for MPO levels in CIP patients to control subjects was p = <0.0001.
Figure 4. Inflammatory biomarker expression patterns in ARC patients. ARCpatients with 2-fold or higher than normal levels of myeloperoxidase areshown. Data for each ARC patient was ‘normalized’ by dividing the measuredvalue by the average value from normal subjects. Despite variation in individualpatients, we observed a pattern of expression which was driven by myeloper-oxidase. MPO is an enzyme expressed in activated microglial cells whose activityhas been associated with neuroinflammation.
Figure 1. Box Whisker plots of A1AT levels in serum. Data for ARC patients (n =26), CIP patients (n = 90) and non-pain control subjects (n = 86) were plotted asboth box-whisker and mean and standard deviation from the mean (scaled line).The box encompasses 50% of the data points and the line across the box is themedian value. The ‘whiskers’ above and below the box are drawn down to the10th percentile and up to the 90th. Each dot represents the data for anindividual patient. The p-value indicated is for the comparison of the ARCdata set to control non-pain subjects and CIP patients. The p-value for CIPpatients to control (nonpain) subjects was: p = <0.0001 for A1AT.
Figure 3. Box Whisker plots of sTNFR2 levels in serum. Data for ARC and CIPpatients is plotted as indicated in Figure 1. The p-value indicated is for thecomparison of ARC patients to control non-pain subjects and CIP patients. Thep-value for sTNFR2 levels in CIP patients to control subjects was p = 0.00011.
POSTGRADUATE MEDICINE 89
expression and patterns in ARC and CIP states. The group ofpatients with intractable pain we evaluated were those withcentralized syndromes wherein sensitization of the pain systemoccurs that can either be relegated to a specific part of thebody or encompass the entire body. Centralized pain is typicallyconstant and may be moderate to severe in intensity. CIPpatients, as a group, have been shown to have a more severe,persistent pain that usually fail to respond to non-narcoticanalgesics and other treatment measures [9–11]. We also exam-ined chronic inflammatory biomarker expression in ARCpatients who had both localized and diffuse pain symptomatol-ogy. In this study, we measured and compared the expressionof three chronic inflammatory biomarkers in each group of
chronic pain patients and in comparison to values determinedfor normal subjects. Alpha-1 antitrypsin, an acute phase pro-tease inhibitor belonging to the serpin superfamily, protectstissues from elastase and other enzymes released from inflam-matory cells [14]. Myeloperoxidase is an inflammatory peroxi-dase enzyme most abundantly present in neutrophilgranulocytes [15,16] and activated microglial cells. Lastly, wemeasured serum levels of sTNFR2, a circulating form of thereceptor for TNF alpha, involved in reducing systemic inflam-mation by binding to TNF alpha [17].
While there are other clinical tests for inflammation, e.g.measurement of C-reactive protein or erythrocyte sedimenta-tion rate, they are generally non-specific—particularly withregard to chronic inflammation [18,19]. The highest meanserum concentration of A1AT, MPO, and sTNFR2 were seenin CIP patients, while A1AT and MPO were significantly ele-vated in ARC patients as compared with normal subjects. Allthe patients with chronic pain we studied were being treated,often with a variety of medications both non-narcotic andnarcotic. Our observation that subsets of the three inflamma-tory biomarkers can be expressed in these aggressively treatedpatients suggests that despite treatment residual inflamma-tion is present. A1AT and sTNFR2 are anti-inflammatory med-iators which circulate systemically at reasonable concentrationto block pro-inflammatory molecules released by inflamma-tory cells [14,18]. It is important to note that the serum levelsof each of the individual inflammatory biomarkers varies tothe extent that no cut-off point can be identified for a singleindividual biomarker that would segregate normal subjectsfrom pain patients or ARC from CIP.
Interestingly, MPO was the statistically predominant inflam-matory marker elevated above normal in treated patients withcentralized pain. We hypothesize that such activated micro-glial cells directly contribute to inflammation. MPO’s activity isassociated with powerful pro-oxidative and proinflammatoryproperties [16,17]. Its role in the establishment and mainte-nance of neurodegenerative disease states may be related tothe elaboration of MPO by microglial cells [20–23]. Althoughsubstantial evidence has established that microglia and astro-cytes play a key role in the establishment and maintenance ofpersistent pain in animal models [24,25], the role of glial cellsin human pain disorders has not been well established.
We have suggested that in CIP and ARC, microglial cellselaborate MPO and other inflammatory factors which may notbe completely cleared from the system despite extensive andcomplex treatment regimens.
Clearly the size of the ARC group was smaller than wewould have liked, and while we identified different patternsof residual inflammation in ARC patients (Figures 4–6), largergroups of well characterized patients would need to be eval-uated to see if differences in the clinical manifestation and/orprognosis can be related to specific patterns of biomarkerexpression. Similarly, we need to follow up on preliminarystudies which have indicated that patterns of inflammatorybiomarkers may change upon therapy
It should be emphasized that we have focused upon meanserum biomarker concentrations. As shown in Figures 1–3,within each group, serum biomarker levels for individualpatients can vary across a broad range of concentration.
Figure 5. Inflammatory biomarker expression patterns in ARC patients. ARCpatients with lower than normal levels of myeloperoxidase are shown. Datafor each ARC patient was ‘normalized’ by dividing the measured value by theaverage value from normal subjects. There is variation in individual patients inthe pattern of expression which was driven by lower than normal myeloperox-idase. Note that the scale (0–2-fold normal value) is different from that dis-played in Figure 4.
Figure 6. Inflammatory biomarker expression patterns in ARC patients. ARCpatients with higher than normal levels of myeloperoxidase but less than a 2-fold change are shown. Data for each ARC patient was ‘normalized’ by dividingthe measured value by the average value from normal subjects. There wassignificant variation in individual patients in the pattern of expression whichwas driven by higher than normal myeloperoxidase. Some of the patients hadhigher than normal sTNFR2, and lower than normal A1AT, while others hadlower sTNFR2 levels. Note that the scale (0–2-fold normal value) is differentfrom that displayed in Figure 4.
90 J. A. BILELLO AND F. S. TENNANT

Given the inter-patient variation, it is difficult to segregate CIPpatients from patients with ARC or other types of chronic painbased upon fixed cut-off points.
5. Conclusion
The use of biomarkers of chronic inflammatory processes canprovide better clinical evidence for continued inflammation andtissue damage. In conclusion, we suggest that monitoring thepre- and post-treatment levels of inflammatory biomarkers andalleviating the source of residual inflammationmay be of greaterimportance than palliative care in treating chronic pain patients.
Acknowledgments
We would like to acknowledge the support of Ridge Diagnostics whoprovided partial funding for this study. In addition, we thank Dr. LindaThurmond a former colleague at Ridge Diagnostics, who provided valu-able discussions and critique. We also acknowledge the excellent labora-tory assistance of Ms. Laurie Rotchford MLS who performed most of theassays reported in this study
Funding
This paper was funded in part by Ridge Diagnostics Inc.
Declaration of interest
JA Bilello is a former employee of Ridge Diagnostics Inc. The authors haveno other relevant affiliations or financial involvement with any organizationor entity with a financial interest in or financial conflict with thesubject matter or materials discussed in the manuscript apart from thosedisclosed.
References
1. American Chronic Pain Association. ACPA Resource Guide. 2016.Available from: www.theacpa.org
2. Simon LS. Relieving pain in America: a blueprint for transformingprevention, care, education, and research. Journal of Pain &Palliative Care Pharmacotherapy. 2012;26(2):197–198.
3. Medzhitov R. Origin and physiological roles of inflammation.Nature. 2008;454(7203):428–435.
4. Tal M. A role for inflammation in chronic pain. Curr Rev Pain. 1999;3(6):440–446.
5. Marchand F, Perretti M, McMahon SB. Role of the immune systemin chronic pain. Nat Rev Neurosci. 2005;6(7):521–532.
6. Watkins LR, Maier SF, Goehler LE. Immune activation: the role ofpro-inflammatory cytokines in inflammation, illness responses andpathological pain states. Pain. 1995;63(3):289–302.
7. Clark AK, Old EA, Malcangio M. Neuropathic pain and cytokines:current perspectives. J Pain Res. 2013;6:803–814.
8. Woolf CJ. Central sensitization: implications for the diagnosis andtreatment of pain. Pain. 2011;152(3Suppl):S2–S15.
9. Tennant F. Hormone abnormalities in patients with severe andchronic pain who fail standard treatments. Postgrad Med.2015;127:1–4.
10. Tennant FS, Robinson D, Sagherian A, et al. Chronic opioid treatment ofintractable non-malignant pain. NIDA Res Monogr. 1988;81:174–180.
11. Tennant F. The physiologic effects of pain on the endocrine system.Pain Ther. 2013;2(2):75–86.
12. Dolan RA. Spinal adhesive arachnoiditis. Surg Neurol. 1993;39(6):479–484.
13. Kroenke K, Spitzer RL, Williams JBW. The PHQ-9: validity of a briefdepression severity measure. J Gen Internal Med. 2001;16:606–613.
14. Gettins PG. Serpin structure, mechanism, and function. Chem Rev.2002;102(12):4751–4804.
15. Arnhold J. Properties, functions, and secretion of human myeloper-oxidase. Biochemistry. 2004;69(1):4–9.
16. van der Veen BS, de winther MP, Heeringa P. Myeloperoxidase:molecular mechanisms of action and their relevance to humanhealth and disease. Antioxid Redox Signal. 2009;11(11):2899–2937.
17. Van Zee KJ, Kohno T, Fischer E, et al. Tumor necrosis factorsoluble receptors circulate during experimental and clinicalinflammation and can protect against excessive tumor necrosisfactor alpha in vitro and in vivo. Proc Natl Acad Sci. 1992;89(11):4845–4849.
18. Tennant F, Hermann L. Using biologic markers to identify legiti-mate chronic pain. Am Clin Lab. 2002;21(5):14.
19. Tennant F. Erythrocyte sedimentation rate and C-reactive protein:old but useful biomarkers for pain treatment. Pract Pain Manage.2013 [cited 2013 Mar 1]. Available from: http://www.practicalpainmanagement.com
20. Lefkowitz DL, Lefkowitz SS. Microglia and myeloperoxidase: adeadly partnership in neurodegenerative disease. Free Radic BiolMed. 2008;45(5):726–731.
21. Dublin P, Hanani M. Satellite glial cells in sensory ganglia: theirpossible contribution to inflammatory pain. Brain Behav Immun.2007;21(5):592–598.
22. Gray E, Thomas TL, Betmouni S, et al. Elevated activity and micro-glial expression of myeloperoxidase in demyelinated cerebral cor-tex in multiple sclerosis. Brain Pathol. 2008;18(1):86–95.
23. Choi DK, Pennathur S, Perier C, et al. Ablation of the inflammatoryenzyme myeloperoxidase mitigates features of Parkinson’s diseasein mice. J Neurosci. 2005;25(28):6594–6600.
24. Ellis A, Bennett DL. Neuroinflammation and the generation ofneuropathic pain. Br J Anaesth. 2013;111(1):26–37.
25. Chang L, Munsaka SM, Kraft-Terry S, et al. Magnetic resonancespectroscopy to assess neuroinflammation and neuropathic pain.J Neuroimmune Pharmacol. 2013;8(3):576–593.
POSTGRADUATE MEDICINE 91


















