L coracoid , likely marrow island L paraspinal , likely residual tumor

Annals ofthe Rheumatic Diseases 1991; 50: 755-759
Paraspinal muscle fibrosis: a specific pathologicalcomponent in ankylosing spondylitis
R G Cooper, A J Freemont, R Fitzmaurice, S M Alani, M I V Jayson
AbstractThe histological appearance of percutaneoussuperficial paraspinal muscle biopsy speci-mens from eight patients with ankylosingspondylitis was compared with that of biopsyspecimens from 13 control patients withsimilar degrees of disability and spinal im-mobility due to severe, chronic mechanicalback pain. In both groups marked type Imuscle fibre atrophy was shown. Additionally,in patients with ankylosing spondylitis therewere obvious increases in perifibre connectivetissue in association with central migration ofcell nuclei but without evidence of inflam-mation. Qualitative electromyography failedto show denervation changes in either group.Paraspinal muscle fibrosis, occurring overand above atrophic changes due to disuse,seems to be a specific pathological com-ponent of ankylosing spondylitis which maybe of particular importance in early disease asit may contribute towards back stiffness andweakness.
Rheumatic DiseasesCentre, University ofManchester,Hope Hospital,Salford M6 8HD,United KingdomR G CooperA J FreemontR FitzmauriceM I V Jayson
Department ofNeurophysiology,Hope Hospital,Salford M6 8HD,United KingdomS M AlaniCorrespondence to:Dr R G Cooper,Rheumatic Diseases Centre,Hope Hospital,Salford M6 8HD,United Kingdom.Accepted for publication18 October 1990
Pathological changes of the vertebral columnare well documented in ankylosing spondylitis,but only limited studies have investigatedwhether the paraspinal muscles are affectedby the disease process. The main finding ofthese studies was selective type II muscle fibreatrophy,"1 but an excess of perifibre connectivetissue was occasionally shown.2 5 Clearly,pathological changes in paravertebral musclescould have a considerable impact in ankylosingspondylitis as back mobilising physiotherapyhas a major role in treatment regimens. Ourstudy investigated further the pathologicalchanges occurring in paraspinal muscles ofpatients with early and advanced ankylosingspondylitis and compared them with biopsyspecimens from controls with chronic mech-anical back pain to determine whether thesechanges were merely secondary to the spinaldisease or due to a specific pathological process.
Patients and methodsStudies were made on eight male patients whofulfilled the New York criteria for defmiiteankylosing spondylitis7 and who were HLA-B27 positive and rheumatoid factor negative.They were considered in two groups-four withearly disease and mobile spines and four withadvanced disease and immobile spines-toassess whether pathological changes were
dependent on disease severity. Lumbar spinalflexion was assessed quantitatively by a modi-
fied Schober's test, where the mean for men andwomen is 6-6-5 cm,8 and by measuring thefinger to floor distance. Lumbar spinal exten-sion was assessed semiquantitatively on a scaleout of 3 where 0/3=no extension, 1/3=exten-sion just possible, 2/3 extension obvious butlimited, 3/3=extension normal, 4/3=extensionexcessive, and 5/3=marked hyperextension. Allof the immobile patients with ankylosingspondylitis had flexion deformities of thelumbar spine, with no visible extension, but allmanaged some degree of lumbar flexion.These patients with ankylosing spondylitis
were compared with 13 patients (six male, sevenfemale) with severe chronic mechanical backpain despite previous laminectomy procedures.Both groups had severe functional impairmentwhen assessed by questionnaire to rate chronicdisability scores.9 The patients with back painalso had severe reduction of spinal mobility,hence their choice as 'controls' for comparisonwith the patients with ankylosing spondylitis.Any patients with spinal pain symptoms attri-butable to inflammatory, metabolic, or neo-plastic causes, with clinical or radiologicalevidence of significant scoliosis (>10°) or whohad ingested any agent capable of affectingskeletal muscle were excluded from the controlgroup.
All subjects gave their informed consent forparticipation in this study, which was approvedby Salford Health Authority ethical committee.
After clinical assessment of lumbar spinemobility both patients and controls underwentpercutaneous superficial erector spine biopsyabout 5 cm from the midline at the level ofL3/4. The correct lumbar level was identifiedby palpation of the superior border of the iliaccrest. The conchotome biopsy technique withasepsis and under local anaesthetic was used.10Muscle samples were oriented immediatelyunder the dissecting microscope and snapfrozen in liquid nitrogen cooled isopentane.Cryostat sections were later prepared and stainedwith haematoxylin and eosin and histochemicalsections prepared using both myosine ATPaseat pH 9-4" and Mason's trichrome, the latterfor visualising collagen. Immediately beforebiopsy patients with ankylosing spondylitisunderwent venesection of serum for creatininekinase estimation. Qualitative needle electro-myography of superficial paraspinal muscleswas also undertaken in six patients with anky-losing spondylitis and in six with chronicmechanical back pain to assess the possibilitythat myopathic or denervation/renervationchanges were present. In addition, the para-spinal muscles and other spinal structures of
755

Cooper, Freemont, Fitzmaurice, Alani,Jayson
five patients with ankylosing spondylitis werevisualised radiographically in a single transaxialview obtained by computed tomography at thelevel of the upper vertebral end plate of L4.
ANALYSISQualitative and semiquantitative histologicalinterpretation of muscle biopsy specimens wasprovided by an experienced osteoarticularpathologist (AJF). Qualitative paraspinal elec-
Table I Group clinical details of mobile and immobile patients with ankylosing spondylitisand with chronic mechanical back pain. Results are given as means (SD)
Clinical Patient groups and numbersvariable
Ankylosing spondylitis Chronic mechanicalback pain
Mobile Immobile (6M, 7F)(4M) (4M)
Age (years) 41-3 (13-5) 54 3 (10-8) 44-2 (5-2)Disease duration (years) 12-5 (11-8) 20 5 (18 5) 7-3 (4 2)Schober's test (cm) 6-5 (2-6) 3-0 (1-6) 2-4 (0-9)Finger-floor distance (cm) 14 5 (8-2) 39-8 (13-9) 48-8 (9-2)Back extension (n/3)* 2-3 (1-0) 0-0 (0-0) 1-2 (0-93)Waddell disability index score (0-9) 2-0 (1-6) 6-0 (1-8) 7-3 (1-3)
*See 'Patients and methods'.
tromyography was performed and interpretedby an experienced neurophysiologist (SMA).Statistical analyses were performed with theMann-Whitney U test.
ResultsTables 1 and 2 show group clinical details ofpatients with ankylosing spondylitis and withback pain and table 2 gives the histologicalresults of paraspinal muscle biopsies. Thepatient groups were of roughly similar age butpatients with ankylosing spondylitis had alonger history of back symptoms. Lumbarmobility, except for extension in the immobilepatients with ankylosing spondylitis, was clearlymore restricted in the patients with chronicmechanical back pain, who also had more severechronic disability index scores. Both in patientswith ankylosing spondylitis and in those withback pain there was clear evidence of type IImuscle fibre atrophy (fig 1). The ratio of type Ito type II fibres was 2-10:1 in patients withankylosing spondylitis (mean 4:1) comparedwith 1-5:1 in patients with back pain (mean3:1). Histological evidence of fatty infiltration
Table 2 Individual clinical and histological details of mobile and immobile patients with ankylosing spondylitis andwith chronic mechanical back pain
Patient Age Disease Schober's Finger-floor Back Waddell Histologygroup and (years) duration test distance extension disabilitysex (years) (cm) (cm) (n/3) index score
(0-9)AS * (mobile)M 23 4 8 21 3 2 Type II atrophy. Minimal fibrosisM 52 25 9 9 1 0 Minimal fibrosisM 51 20 6 6 3 4 Type II atrophy. Fatty infiltrationM 39 1 3 22 2 2 Gross fatty infiltration
AS (immobile)M 66 46 3 52 0 4 Gross type II atrophy with fat and fibrosisM 49 4 3 41 0 8 Gross type II atrophy with severe fibrosisM 60 10 1 46 0 5 Gross type II atrophy with severe fibrosisM 42 22 5 20 0 7 Gross type II atrophy with fat and fibrosis
CMBP*M 49 9 3 50 0 8 Type II atrophyM 36 2 3-5 32 3 5 Type II atrophyM 43 7 2 50 2 8 NormalM 44 15 2 62 1 7 Type II atrophyM 49 4 1-5 59 1 7 NormalM 46 3 4-5 43 3 7 Type II atrophyF 52 4 2 43 1 6 Type II atrophyF 46 8 2 55 1 6 Type I atrophy. Neuropathic (?) (EMG* not done)F 44 14 2-5 44 1 7 Marked fatty infiltrationF 39 3 1-5 60 1 9 Type II atrophyF 49 8 2 56 1 9 Marked type II atrophyF 43 7 2 42 0 9 Type II atrophy with fatty infiltrationF 35 11 3 39 1 7 Type II atrophy with fatty infiltration
*AS=ankylosing spondylitis; CMBP=chronic mechanical back pain; EMG=electromyography.
Figure) Transverse sections ofparaspinal musclefrom patients with ankylosing spondylitis showing (A) a biopsy specimenstained with ATPase atpH 9-4; type II (darkly stained)fibres are clearly atrophic in early ankylosingspondylitis, as also seenin patients with chronic mechanical back pain and (B) biopsy specimen stained with haematoxylin and eosin, exuberantfibrosis with central migration ofnuclei in advanced ankylosing spondylitis.
756

Paraspinal musclefibrosis in ankylosing spondylitis
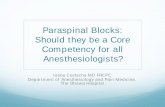
Figure 2 Computed tomographic scans through the upper table ofL4 in patients with ankylosing spondylitis with (1) mobileand (B) rigid spines. Gross, bilateral paraspinal muscle atrophy with fatty replacement is shown in the patient with the rigidspine, whereas the appearance is relatively normal in the patient with the mobile spine.
was present in both patient groups but was
more marked and sometimes dramatic in anky-losing spondylitis, as confirmed by computedtomography (fig 2). In addition, in most patientswith ankylosing spondylitis there was clearhistological evidence of perifibre and periseptalinfiltration with fibrous connective tissue (fig1). The degree of fibrosis varied according tothe severity of spinal disease, being greatest inthe patients with the most rigid spines, thoughfibrosis was present even in patients with fullymobile spines (table 2). In those biopsy speci-mens where fibrosis was most marked there wasalso evidence of internalisation of muscle cellnuclei (fig 1). There was no evidence ofincreased fibrosis in any of the muscle biopsyspecimens from patients with chronic mechani-cal back pain. The histological abnormalities inankylosing spondylitis were not associated withinflammatory cell infiltration or with skeletalmuscle enzyme abnormalities, serum creatinekinase being less than 190 IU/l in all subjects.Qualitative electromyography showed no abnor-mality in either group of patients.
DiscussionInflammation or effusion within a joint, even inthe absence of pain, can cause reflex inhibitionof the muscles controlling that joint. 12-14 Theresulting weakness may render the joint lessstable and therefore liable to further damage.'4This is most obvious in the knee, when synovitismay lead to quadriceps weakness and wastingand joint instability. Whether the spinal painand inflammation which occur in ankylosingspondylitis might impair paraspinal muscleactivation by similar reflex inhibition is un-known. The findings of type II paraspinalmuscle fibre atrophy in patients with ankylosingspondylitis and in those with chronic mechanicalback pain provides indirect evidence that inboth groups motor activation has been reduced.It was not possible, however, to determinewhether this resulted from simple disuse due topain on movement, or from reflex inhibition.The histological appearance of normal para-
spinal muscles is poorly recorded in limited
cadaveric studies.'5 16 These indicate that type Iand II fibres are of roughly equal size but with adistribution that favours type I fibres slightly,type I:type II fibre ratios being 1-2-1-4:1. Thepresent finding of mean ratios of 3:1 and 4:1 forpatients with back pain and ankylosing spondy-litis respectively, together with minor to markedtype II fibre atrophy, presumably indicatestype II fibre loss as a consequence of thereduced motor activation. Previous histologicalinvestigations of paraspinal muscles in ankylos-ing spondylitis' showed, in addition to theselective type II fibre atrophy, type I fibrechanges in the form of 'moth-eaten' and'targetoid' fibres on NADH-diaphorase histo-chemical preparations.' As these type I fibrechanges are not specific for ankylosing spondy-litis the NADH-diaphorase staining techniquewas not used in this study. Electron microscopystudies of paraspinal muscle in ankylosingspondylitis have shown marked structural dis-ruption with Z band streaming, loss of myo-filamentous alignment, loss or absence of mito-chondria, abnormalities of the basementmembrane, and the presence of abnormal lipidand nemeline inclusion bodies.' Such abnor-malities also occur in congenital structuralmyopathies, where renervation follows denerva-tion and where muscles are under reducedtension-for example, because of tenotomy. 7 Itis believed that a necessary stimulus for accurateexpression of synthetic muscle enzymes istension, without which muscle disorganisationcan occur.' Loss of spinal movement, as inadvanced ankylosing spondylitis or severechronic mechanical back pain might, perhaps,lead to this. The early interpretations of thehistological abnormalities in ankylosing spondy-litis were of simple disuse atrophy, but neuro-genic mechanisms were subsequently proposed,with damage to the posterior branches of thespinal nerves arising owing to bony encroach-ment by pathological apophysial joints in exitforamina.5 Only one previous study undertookparaspinal electromyography, the results show-ing only minor evidence of denervation.3 Thelack of any electromyographic evidence fordenervation or renervation in the current study
757

Cooper, Freemont, Fitzmaurice, Alani, Jayson
seems to exclude significant nerve root com-pression as a cause of the noted histologicalchanges. Furthermore, if neurological damagehad been occurring then, by chance, it shouldpresumably have resulted in type I and II fibrechanges of roughly similar degree. This was notthe case in this or previous studies. Neurologicaldamage to motor nerves causes muscle fibrewasting and angulation with evidence of fibrerenervation, including fibre-type grouping. 17The marked predilection for type II fibreatrophic changes in ankylosing spondylitis andchronic mechanical back pain, without evidenceof fibre-type grouping, therefore suggestsreduced activation and not denervation.
In previous histological studies where para-spinal muscle fibrosis in ankylosing spondylitiswas occasionally shown2 5 it was suggested thatsuch an abnormality was non-specific andsecondary to disuse or denervation. Patientswith ankylosing spondylitis were not comparedwith 'control' subjects, however, to validatesuch claims, hence our use of patients withchronic mechanical back pain who actually hada greater degree of immobility and functionalimpairment than that seen in the patients withankylosing spondylitis. Such a comparisonshowed striking differences in the pathologicalappearance of paraspinal muscle in the twogroups-namely, the presence of excessive peri-fibre and periseptal fibrosis in patients withankylosing spondylitis. This was not seen inpatients with back pain. These findings cannotbe explained by differences in spinal mobility orthe severity of histological changes alone as thetype II fibre atrophy and fatty infitration wereof a similar extent in both groups of patients.Furthermore, the fibrosis in ankylosing spondy-litis occurred even in patients with almost fullymobile lumbar spines, who had only minor typeII fibre atrophy. Disease duration, and there-fore potential duration of spinal immobility,was in general greater in patients with ankylos-ing spondylitis, but it was apparent that para-spinal fibrosis occurred even where diseaseduration was obviously less than the meanduration of 7-2 years in patients with chronicmechanical back pain. These results stronglysuggest that paraspinal muscle fibrosis in anky-losing spondylitis is a specific pathologicalprocess.
In normal muscle a few isolated collagenfibrils can be seen by electron microscopybetween fibres-in the endomysium. Minorincreases in endomysial collagen and connectivetissue occur with advancing age'8 and immobi-lisation,'9 but marked increases usually occuronly in certain circumstances-notably, afterprolonged denervation with advanced atrophy20and after myofibre destruction in musculardystrophy and inflammatory myositis.2' 22Extensive fibrosis can occur where muscle fibredamage is minimal-for instance, in the rare'rigid spine' syndrome. This affects malechildren causing marked limitation of the dorso-lumbar spine. Paraspinal electromyographyshows a myopathic pattern, whereas histologyshows excess cellularity, marked perimysial andendomysial fibrosis, replacement of muscle byconnective tissue, and central migration of
nuclei."3 These histological abnormalities seemremarkably similar to those presently describedin ankylosing spondylitis. As collagen, the chiefcomponent of fibrous connective tissue, has alow compliance even small increases could causeconsiderable muscle stiffness.'8A further histological difference between the
patient groups in the current study was thepresence of internalised nuclei in the paraspinalmuscle of patients with ankylosing spondylitis.Central migration of nuclei is a well recognised,but non-specific, feature of various myopathicprocesses. These could cause muscle celldamage or death, with characteristic electro-myography and serum creatine kinase changes,and previous studies showed raised enzymeconcentrations in some patients with ankylosingspondylitis,24 but neither of these abnormalitieswas recorded in the present study. Possibleexplanations for these apparent discrepanciesare that any myopathic process in ankylosingspondylitis is patchy, and hence liable to elec-tromyography sampling error, or of either lowor variable intensity, such that enzyme activitycould be normal. It was previously suggestedthat muscle fibrosis in ankylosing spondylitismight represent the end point ofan inflammatorymyopathic process.25 Although this may be thecase, this study and others have consistentlyshown that histological paraspinal muscleabnormalities in ankylosing spondylitis occurwithout obvious inflammation. The cause ofmuscle abnormalities is therefore unknown,but a process similar to enthesitis has beenproposed.5Muscle abnormalities are not limited to the
paraspinal muscle in ankylosing spondylitis astype II fibre wasting and central migration ofnuclei have been shown in quadriceps femoris,which have also been shown to be weak.25Furthermore, a mild diffuse increase of inter-stitial connective tissue has been demonstratedin myocardial tissue obtained from patients withankylosing spondylitis at necropsy.26 It thusseems that ankylosing spondylitis is associatedwith a generalised muscle problem. Paraspinalmuscle atrophy with fibrosis is likely to contri-bute towards the spinal weakness and stiffnessexperienced by patients with ankylosingspondylitis, adding to that resulting from patho-logical changes occurring in the spine. Byreducing the strength of the paraspinal muscles,such abnormalities may severely hampermobilising physiotherapy and may well hastenthe process of vertebral ankylosis.
1 Aufdermaur M. Anatomic pathologique de la spondyliteankylosante. Acta Rheumatologica 1954; (2): 60.
2 Pohl V W, Sievers B U. Veranderungen der musculatur beispondylitis ankylopoetica. Z Rheumatol 1974; 33: 249-53.
3 Roux H, Serratrice G, Maestracci D, et al. Les atteintesmusculaires au cours de la pelvispondylite rheumatismale.Rev Rheum Mal Osteoartic 1975; 42: 231-8.
4 Berman L, Isaacs H, Pickering A. Structural abnormalities ofmuscle tissue in ankylosing spondylitis. S Afr Med Jf 1976;50: 1238-40.
5 Carraba M, Chevallard M, Colombo B, Dworzak F, Mora M,Cornelio F. Muscle pathology in ankylosing spondylitis.Clin Expi Rheumatol 1984; 2: 139-44.
6 Kukulas B A, Morrison I, Owen E T, Kitridou R. Unusualparaspinal muscle lesions in ankylosing spondylitis. ClinExp Rheumatol 1987; 23: 23-9.
7 Bennett P H, Wood P H N, eds. Population studies of therheumatic diseases. Amsterdam: Excerpta Medica, 1968:456-8. (International congress series.)
758

Paraspinal musclefibrosis in ankylosing spondylitis
8 Moll J M H, Wright V. Normal range of spinal mobility. Anobjective clinical study. Ann Rheum Dis 1971; 30: 381-6.
9 Waddell G, Main C J. Assessment of severity of low-backdisorders. Spine 1984; 9: 204-8.
10 Dietrichson P, Coakley J, Smith P E M, Griffiths R D,Helliwell T, Edwards R H T. Conchotome and needlepercutaneous biopsy of skeletal muscle. Neurol NeurosurgPsychiatiy 1987; 50: 1461-7.
11 Round J M, Matthews Y, Jone D A. A quick, simple andreliable histochemical method for ATP-ase in humanmuscle preparation. Histochem 1980; 12: 707-10.
12 De Andradre J R, Grant C, Dixon A St J. Joint distensionand reflex muscle inhibition in the knee. BonegJoint Surg[Ami 1%5; 47: 313-22.
13 Baxendale R H, Ferrell W R, Wood L. Knee joint distensionand quadriceps maximal voluntary contraction in man.Physiol 1985; 367: lOOP.
14 Stokes M, Young A. The contribution of reflex inhibition toarthrogenous muscle weakness. Clin Sci 1984; 67: 7-14.
15 Johnson M A, Polgar J, Weightman D, Appleton D. Data ondistribution of fibre types in thirty-six human muscles. Anautopsy study. Neurol Sci 1973; 18: 111-29.
16 Polgar J, Johnson M A, Weightman D, Appleton D. Data onfibre size in thirty-six human muscles. An autopsy study.Neurol Sci 1973; 19: 307-18.
17 Cancilla P A. General reaction of muscle to injury. In:Heffner R R, ed. Contemporary issues in surgical pathology.
vol 3. Muscle pathology. New York: Churchill Livingstone,1984: 15-30.
18 Alnaqeeb M A, Al Zaid N S, Goldspink G. Connective tissuechanges and physical properties of developing and ageingskeletal muscle. Anat 1984; 139: 677-89.
19 Williams P E, Goldspink G. Connective tissue changes inimmobilised muscle. Anat 1984; 138: 343-50.
20 Tomanek R J, Lund D D. Degeneration of different types ofskeletal muscle fibres. I. Denervation. Anat 1973; 116:395-407.
21 Duance V C, Stephens H R, Dunn M, Bailey A J, DubowitzV. A role for collagen in the pathogenesis of musculardystrophy? Nature 1980; 284: 470-2.
22 Duance V C, Black C M, Dubowitz V, et al. Polymyositis-an immunofluorescence study on the distribution ofcollagen types. Muscle Nerve 1980; 30: 487-90.
23 Dubowitz V. Muscle disorders in childhood. Philadelphia:Saunders, 1978: 239-43.
24 Calin A. Raised serum creatine kinase activity in ankylosingspondylitis. Ann Rheum Dis 1975; 34: 244-7.
25 Hopkins G 0, McDougall J, Mills K R, Isenberg D A,Ebringer A. Muscle changes in ankylosing spondylitis. BrJRhewnatol 1983; 22: 151-7.
26 Brewerton D A, Gibson D G, Goddard D H, et al. Themyocardium in ankylosing spondylitis. A clinical, echo-cardiographic and histopathological study. Lancet 1987; i:995-8.
759