Pain Final
30
Pain Assessment and Management Guideline for Practice, 2 nd Edition Marlene Walden, PhD RNC NNP CCNS Sharyn Gibbins, PhD RN NNP
-
Upload
sasha-hidayat-full -
Category
Documents
-
view
238 -
download
0
description
pain final
Transcript of Pain Final

Pain Assessment and Management
G u i d e l i n e f o r P r a c t i c e , 2 n d E d i t i o n
Marlene Walden, PhD RNC NNP CCNS
Sharyn Gibbins, PhD RN NNP

This guideline is an outline of the pain assessment and management practices that currently are accepted and documented by experts in the field of neonatal care. In addition, it summarizes and recommends pain assess-ment and management practices based on the best evidence for the nursing care of infants. This guideline does not preclude the use of manufacturers’ recommen-dations or other acceptable methods of assessing and managing pain in infants. The use of other practices known to improve the quality of neonatal care is encour-aged and not restricted by this document.
The National Association of Neonatal Nurses (NANN) developed this guideline in response to members’ requests. Broad in scope, it can provide a foundation for specific nursing protocols, policies, and procedures developed by individual institutions.
Development and AcknowledgmentsThis guideline was written by two NANN members with established expertise in pain assessment and management. It was modified based on thoughtful comments and edit-ing suggestions of volunteer reviewers.
NANN especially thanks Abbott Nutrition and Children’s Medical Ventures for providing educational grants for the publication of this guideline. Abbott Nutrition and Children’s Medical Ventures had no prior substantive review rights or input into the content of the guideline.
The following contributors and reviewers are recognized for their assistance.
AuthorsMarlene Walden, PhD RNC NNP CCNSSharyn Gibbins, PhD RN NNP
ReviewersDaniel Batton, MD, American Academy of Pediatrics Sandra Sundquist Beauman, MSN RNCJim Couto, MA, American Academy of PediatricsMary Ann Gibbons, BSN RNMelinda Porter, RNC CNS NNPAnn Stark, MD FAAP, Chair of AAP Committee on Fetus and NewbornCarol Wallman, RNC NNP MS, NANN/AWHONN Liaison to AAP Committee on Fetus and Newborn
Pain Assessment and ManagementGuideline for Practice, 2nd Edition
Copyright © 2001, 2008 National Association of Neonatal Nurses. All rights reserved. First edition 2001Second edition 2008Reproduction, distribution, or translation of this publication without the express written permission of NANN is strictly prohibited.ISBN 0-9787636-2-9.
4700 W. Lake AvenueGlenview, IL 60025-1485800/451-3795Fax 888/477-6266www.NANN.org
Publisher’s note: The product is provided on an as-is basis. National Association of Neonatal Nurses, the authors and editors neither represent nor guarantee that the content will, if followed, ensure safe and effective patient care. NANN, the authors and editors assume no liability or responsibility in connection with the content. The content reflects NANN’s judgment regarding the state of general knowledge and practice in this field as of the date of publication and is subject to change based on the availability of new scientific information. The content is not intended to be a substi-tute for professional medical judgment, diagnosis, or treatment.

Pain Assessment and Management 3
Newborn infants, particularly those born preterm, reg-ularly are subjected to a multitude of diagnostic and therapeutic procedures that are painful but medically nec-essary to their care (Gibbins et al., 2006; Stevens et al., 2007). Simons and colleagues (2003) found that infants born at 25–42 weeks gestation experienced an average of 14 painful procedures per day during the first 2 weeks of life. The most frequently performed procedures were nasal, endotracheal, and nasopharyngeal suctioning fol-lowed by heelstick and intravenous and nasogastric tube insertions. The number of procedures encountered by infants in the neonatal intensive care unit (NICU) is par-tially due to a substantial number of failed attempts. In the Simons et al. study, the failure rate for placement of central venous catheters, peripheral arterial catheters, and intravenous cannulae were 45.6%, 37.5%, and 30.9%, respectively. Although most of the procedures per-formed in this study were rated by physicians and nurses to be painful (>4 on a 10-point scale), very few infants received any pharmacologic or nonpharmacologic proce-dural pain management.
Evidence suggests that the cumulative effects of repeated painful medical procedures on the developing brain may be of significant biological and clinical impor-tance (Anand, 1998). Pain can place increased demands on the cardiorespiratory system (Craig, Whitfield, Grunau, Linton, & Hadjistavropoulos, 1993; McIn-tosh, Van Veen, & Brameyer, 1994; Stevens & Johnston, 1994; Stevens, Johnston, & Horton, 1993). In addition, pain can lead to an elevation in intracranial pressure, theoretically increasing the risk of intraventricular hem-orrhage (Stevens & Johnston; Stevens et al., 1993). Pain in infants contributes to adverse long-term developmen-tal outcomes, such as decreased sensitivity to common childhood pain, and a higher incidence of somatic com-plaints (i.e., physical complaints of unknown origin; Fitzgerald & Shortland, 1988; Grunau, Whitfield, & Petrie,1994; Grunau, Whitfield, Petrie, & Fryer, 1994).
This practice guideline, which presents the evidence for the assessment and management of pain in infants,
is based on scientific literature and clinical recommen-dations from professional and accrediting organizations such as the Agency for Health Care Policy and Research (AHCPR [now the Agency for Healthcare Research and Quality], 1992), National Association of Neonatal Nurs-es (NANN, 2001), Joint Commission on Accreditation of Healthcare Organizations (JCAHO [now The Joint Com-mission], 2001), American Academy of Pediatrics (AAP, 1999), American Academy of Pediatrics/Canadian Pae-diatric Society (AAP/CPS, 2000, 2006), the American Society for Pain Management Nursing (Herr et al., 2006), and the International Association for the Study of Pain (IASP, 2005).
Infant pain assessment and management is often in- adequate despite the availability of assessment instruments and safe, effective pharmacologic and nonpharmacolog-ic interventions to prevent or minimize pain and distress. Although the prevention of pain in neonates should be the goal of all caregivers, because repeated painful expo-sures have the potential for deleterious consequences, if painful procedures are required, careful consideration of safe and effective interventions should be provided (AAP/CPS, 2006). The goal of this guideline is to pro-vide the knowledge necessary to effectively assess and manage postoperative, procedural, and disease-related pain in hospitalized infants.
Definition of PainThe International Association for the Study of Pain (2004) defines pain as “an unpleasant sensory and emo-tional experience associated with actual or potential tissue damage, or described in terms of such damage.” The inability to communicate verbally does not negate the possibility that an individual is experiencing pain and is in need of appropriate pain-relieving treatment. Apply-ing this definition to infants, Anand & Craig (1996) suggest that newborns display physiologic and behavioral cues to signal tissue damage. Caregivers should use these response cues as objective and valid indicators of pain in infants.
Pain Assessment and Management: Guideline for Practice

Pain Assessment and Management 4
Guideline IEducation and competency validation in pain assessment and management shall be conducted during orientation and at regularly defined intervals throughout employment for all nurses delivering care to infants (AAP/CPS, 2000, 2006; IASP, 2005; JCAHO, 2001; NANN, 2001).
Key PointsA. Nurses shall demonstrate competency in neonatal
content areas including, but not limited to, the following:
1. Anatomy and physiology of pain transmission, modulation, and perception
2. Pain assessmenta. physiologic and behavioral indicatorsb. valid and reliable instruments to measure
painc. contextual factors such as gestational
age or behavioral state that modify pain expression in infants
3. Pain managementa. nonpharmacologic approaches (e.g.,
behavioral and environmental strategies)b. pharmacologic interventions (e.g., non-
steroidal antiinflammatory drugs, opioids, and adjuvant analgesics)(1) side effects(2) assessment and management of opioid
tolerance, dependence, and withdrawal(3) local anesthetics and analgesics (e.g.,
EMLA [eutectic mixture of local anes-thetics], lidocaine, Ametop creams)
c. special procedural techniques (e.g., veni-puncture versus heelstick, spring-loaded lancet versus straight lancet)
d. palliative and end-of-life care 4. Documentation of pain assessment, interven-
tions, and response to pharmacologic and nonpharmacologic interventions
5. Parental role in pain assessment and management
6. Institutional pain-related policies and procedures
B. Education to achieve competency shall be based on the following:
1. Sufficient scope and duration to ensure contin-ued competency
2. Current research findings related to pain assess-ment and management
3. Educational content identified by professional or accrediting organizations
4. Identified or stated learning needs of the health-care provider
5. Performance and findings from continuous quality improvement activities
6. Input and involvement of the multidisciplinary team and the support of unit nursing and medi-cal leaders
7. Appropriate documentation in the provider’s record or personnel file (i.e., the content and scope of the program and the provider’s suc-cessful completion of required competency activities)
C. Upon completion of educational activities, the nurse shall be able to do the following:
1. Identify physiologic and behavioral responses to pain
2. Consider gestational age and developmental stage in evaluating infant pain
3. Select an age-appropriate instrument with pub-lished reliability and validity to assess infant pain
4. Demonstrate the use of appropriate nonpharma-cologic interventions for the infant experiencing pain
5. Demonstrate knowledge of the mechanisms of actions, duration, excretion, and appropriate dosing of pain medications
6. Administer ordered medications safely 7. Recognize and report adverse side effects of
analgesics 8. List the equipment and personnel needed to
adequately monitor the infant after administer-ing pain medication
9. Demonstrate critical-thinking skills and appro-priate nursing interventions in the event of an adverse reaction to pharmacologic therapy
10. Educate parents and families on pain assess-ment and management approaches being used and enlist their assistance, as appropriate
11. Advocate for a well-rounded pain management plan
12. Appropriately documenta. assessment and reassessment of pain statusb. nonpharmacologic interventionsc. pharmacologic therapy, including
medication, dose, route, and time of administration
d. infant’s response to all interventionse. education and involvement of the parent or
caregiver13. Demonstrate appropriate interpersonal skills in
communicating with the physician and family members regarding the infant’s pain status

Pain Assessment and Management 5
Guideline IIPain is assessed and reassessed at regular intervals throughout the infant’s hospitalization (AHCPR, 1992; AAP/CPS, 2000, 2006; IASP, 2005; JCAHO, 2001; NANN, 2001).
Key PointsA. Pain assessment is an essential component of pain
management (AHCPR, 1992; AAP/CPS, 2000, 2006; IASP, 2005; JCAHO, 2001; NANN, 2001).
B. Infants are unable to self-report pain; therefore, other measures must be used to detect pain and evaluate interventions. No single objective assessment strategy, such as interpretation of behaviors, pathology, or estimates of pain by others, is sufficient by itself.
C. Use the hierarchy of Pain Assessment Techniques (Herr et al., 2006; McCaffery & Pasero, 1999).
1. Verbal self-report (not possible in infants) 2. Search for potential causes of pain 3. Observe patient behaviors, which are not
always accurate reflections of pain intensity, and in some cases, indicate another source of distress, such as physiologic or emotional distress
4. Surrogate reporting of parents and caregivers 5. Attempt an analgesic trial if there are pathologic
conditions or procedures likely to cause pain or if pain behaviors continue after attention to basic needs and comfort measures
D. Frequency of pain assessments for postoperative, procedural, and disease-related pain in hospitalized infants should be based upon the expected intensity and duration of the pain (AHCPR, 1992; IASP, 2005; NANN, 2001).
E. Pain should be assessed upon admission and at reg-ularly defined intervals throughout the infant’s hospitalization (AAP/CPS, 2000; IASP, 2005; JCAHO, 2001; NANN, 2001). For example, a pol-icy may state that pain is assessed upon admission and once every 8 hours, unless ongoing or recurrent pain caused by surgery, disease, or therapy dictates more frequent assessment. Some institutions adopt pain assessment as the fifth vital sign (i.e., pain is assessed with every vital sign assessment).
F. Institutions should develop policies for the assessment of procedure-related, postoperative, and disease- related pain common among patients in the NICU.
G. A high index of suspicion should be utilized when assessing infants for the presence, absence, or inten-sity of pain (AHCPR, 1992; NANN, 2001).
1. Developmental maturity, health status, and envi-ronmental factors contribute to an inconsistent, less robust pattern of pain response among preterm and term infants, even in the same
infant over a period of time and in different situ-ations (Craig et al., 1993; Gibbins & Stevens, 2003; Grunau, Linhares, Holsti, Oberlander, & Whitfield, 2004; Johnston, Stevens, Craig, & Grunau, 1993; Shapiro, 1993).
2. The presence of pain should be presumed in all situations considered to cause pain in adults and children, even in the absence of behavioral or physiologic signs (Franck, 1998).
H. A multidimensional approach that incorporates both physiologic and behavioral indicators should be used to assess pain (AHCPR, 1992; NANN, 2001).
1. Heart rate appears to be the most reliable physi-ological measure of pain (Sweet & McGrath, 1998). Three other frequently used physiological measures of pain include oxygen saturation, blood pressure, and breathing patterns. Other physiological indicators such as intracranial pressure and heart rate variability, although reli-able, are clinically difficult to evaluate.a. Research exploring brief, acute noxious
stimuli suggests that heart rate and blood pressure generally increase during pain while oxygen saturation decreases. Respi-ratory rate may either increase or decrease during pain, but typically becomes more rapid, shallow, or irregular (Hummel & van Dijk, 2006; Sweet & McGrath, 1998).
b. Physiologic measures may be the sole method of assessing pain in infants who are pharmacologically paralyzed for mechanical ventilation or who are severely neuro-logically impaired (Hummel & van Dijk, 2006). Observe for vital sign changes dur-ing handling; increases in heart rate and blood pressure generally indicate the need for more analgesia, sedation, or both in the paralyzed infant. Variability in heart rate and blood pressure decreases in a sedated infant.
c. When pain is prolonged, physiologic mea-sures may not be valid indicators, as vital sign changes cannot be maintained (Hummel & van Dijk, 2006).
d. Physiologic measures reflect the body’s nonspecific response to stress and may not be specific to pain (Barr, 1992; Gunnar, Connors, Isensee, & Wall, 1988). There-fore, physiologic measures should be used along with behavioral measures that have been demonstrated to be more consistent and specific to pain in infants (Duhn & Medves, 2004; NANN, 2001; Stevens, Johnston, & Horton, 1994).

Pain Assessment and Management 6
2. The most frequently studied behavioral responses to pain in the neonate are facial activity, crying, and body movements.a. Facial activity (i.e., brow bulge, eye
squeeze, nasolabial furrow, and open mouth) is the most specific indicator of acute procedural pain (Gibbins & Stevens, 2003; Grunau & Craig, 1987; Grunau, Johnston, & Craig, 1990; Hummel & van Dijk, 2006; Stevens et al., 1993).
b. Acoustical and temporal characteristics of pain cries have been demonstrated to be dif-ferent from those of other types of cries, in both preterm and full-term infants, but dif-ficult to discriminate in the clinical setting (Fuller, 1991; Grunau & Craig, 1987). (1) Types of cries differ along a contin-
uum of intensity according to graded levels of noxious stimuli that corre-spond to adults’ judgments about the urgency or severity of the infant’s dis-tress (Fuller, 1991; Porter, Porges, & Marshall, 1988).
(2) Although the presence of crying can pro-vide valuable information about pain, its absence should not be equated with absence of pain (Johnston et al., 1999; Johnston, Stevens, Yang, & Horton, 1995; Stevens et al., 1993; Stevens et al., 1994). The absence of a response may indicate the depletion of the infant’s response capability, not a lack of pain perception (Franck, 1998).
c. Franck (1986) demonstrated that healthy, full-term newborns make swiping motions toward a lanced foot with the unaffected leg, as if trying to push away the noxious stimulus.
d. Preterm infants may uniquely respond to acute pain by increased flexion and exten-sion of arms and toe and finger splay (Grunau, Holsti, Whitfield, & Ling, 2000; Holsti, Grunau, Oberlander, & Whitfield, 2004; Morison et al., 2003).
e. Extremely low-birthweight (ELBW) infants have limited capacity to respond to pain. ELBW infants have inadequate muscle strength, posture, tone, and movement compared to term infants; interpretation of their pain responses is difficult (Gibbins & Stevens, 2003). Responses to pain in this high-risk population are currently under investigation.
f. Cognitively impaired infants show similar physiological and behavioral responses to pain compared to healthy term infants, but with decreased magnitude (Stevens et al., 2007).
3. Expression of pain is altered by the contextual factors surrounding the painful event (Johnston & Stevens, 1996; Johnston et al., 1999; Stevens et al., 1994).a. Behavioral state has been shown to act as a
moderator of behavioral pain responses in both full-term and preterm infants (Grunau & Craig; 1987; Johnston et al., 1999; Ste-vens & Johnston, 1994; Stevens, Johnston, Petryshen, & Taddio, 1996). Awake or alert infants demonstrate a more robust reaction to painful stimuli than sleeping infants.
b. Research examining both facial and body activity has demonstrated that the more premature the infant, the less vigorous and robust the response (Craig et al., 1993; Johnston et al., 1999; Johnston et al., 1995). Craig and colleagues suggest that the less vigorous response demonstrated by preterm infants “should be interpreted in the context of the energy resources avail-able to respond and the relative immaturity of the musculoskeletal system” (p. 296).
c. Evidence suggests that preterm infants in the NICU with a history of painful experiences have a diminished or less mature behavioral response to subsequent painful procedures (Johnston & Stevens, 1996).
d. Johnston and colleagues (1999) found that preterm infants’ lack of response to a heel-stick procedure was predicted by lower gestational age at birth, postnatal age at the time of the study, length of time since the last painful procedure, and behavioral state.
e. Other contextual factors that alter infants’ pain expression include severity of illness, technician expertise, gender, environmental stress, procedural modifiers, and initial threshold and sensitization after repeated stimulation (Craig et al., 1993; Grunau & Craig, 1987; Johnston & Stevens, 1996; Johnston et al., 1993; Johnston et al., 1995; McIntosh et al., 1994; Stevens & Johnston, 1994; Stevens et al., 1993; Stevens et al., 1994).
I. Reliable and valid multidimensional instruments should be used to assess pain in infants (AHCPR, 1992; AAP/CPS, 2000, 2006; Anand & International Evidence-Based Group for Neonatal Pain (IEBGNP),

Pain Assessment and Management 7
2001; Duhn & Medves, 2004; IASP, 2005; NANN, 2001).
1. In choosing an instrument to use in assessing pain in infants, caregivers should take into consideration all published psychometric data, including the aspects of validity, reliability, and clinical utility. Caregivers should also consider infant population, setting, and type of pain experienced when choosing a pain instrument (Duhn & Medves, 2004).
2. Total pain scores obtained by utilizing a behav-ioral pain assessment tool should be interpreted cautiously, taking into consideration the pres-ence of risk factors for pain and the infant’s ability to exhibit pain behaviors (Hummel & van Dijk, 2006). Numeric pain assessment scores do not measure the infant’s actual pain; instead, the infant’s response to pain is measured.
3. Few multidimensional pain measures have established adequate psychometric properties and clinical utility for use with infants. The most commonly used published instruments that demonstrate acceptable psychometric and clini-cal utility properties are the Premature Infant Pain Profile (PIPP) developed by Stevens and colleagues (1996), the CRIES tool (Bildner & Krechel, 1996), and the Neonatal Infant Pain Scale (NIPS) developed by Lawrence and col-leagues (1993).a. PIPP (see Figure 1)
(1) was tested in infants of 28–40 weeks gestational age with procedural pain
(2) incorporates contextual factors that may modify the pain response
(3) includes two physiologic indicators of pain (i.e., heart rate and oxygen sat-uration); three behavioral indicators (i.e., brow bulge, eye squeeze, and nasolabial furrow); and two contex-tual factors (i.e., gestational age and behavioral state)
(4) uses a 4-point scale (0–3); scores on the seven indicators are added for a total pain score
(5) maximum attainable score depends on the infant’s gestational age (younger preterm infants can reach a maximum PIPP score of 21, older infants can attain a maximum score of 18)
(6) for all age groups, has a total pain score that is interpreted as follows:
(a) ≤6 = minimal or no pain (b) 7–12 = mild to moderate pain
(requires nonpharmacologic comfort measures)
(c) >12 = moderate to severe pain (most likely requires pharmaco-logic intervention in conjunction with comfort measures)
b. CRIES (see Figure 2)(1) assesses postoperative pain in preterm
and full-term infants(2) was tested in infants of 32–36 weeks
gestational age(3) acronym is named for the five indicators
it measures, each of which is scored on a 3-point scale (0–2): Crying, Requires oxygen to maintain satura-tion greater than 95%, Increased vital signs, Expression, and Sleepless
(4) has a total score that ranges from 0 to 10
(5) has a total pain score that is interpreted as follows:
(a) ≤4 = mild pain (requires non- pharmacologic comfort measures) (b) ≥5 = moderate to severe pain
(most likely requires pharmaco- logic intervention in conjunction with comfort measures)
c. NIPS (see Figure 3) (1) was tested for validity and reliability
in preterm and full-term infants with procedural pain
(2) was tested in infants of 28–38 weeks gestational age
(3) has a six-item scale; five items are behavioral (i.e., facial expression, cry-ing, arms, legs, and state of arousal) and one is physiologic (i.e., breathing pattern)
(4) each behavior other than crying has descriptors for the two possible scores (i.e., 0 and 1); crying is scored on a 3-point scale (0–2)
(5) has a total score that ranges from 0 to 7d. Emerging pain assessment instruments
include the Pain Assessment Tool (PAT; Hodgkinson, Bear, Thorn, & Van Blaricum, 1994) that was developed for postopera-tive pain, the Scale for Use in Newborns (SUN; Blauer & Gerstmann, 1998) that was developed for procedural pain, the Bernese Pain Scale for Neonates (BPSN; Cignacco, Mueller, Hamers, & Gessler, 2004) that was specifically developed to assess the responses of preterm neonates or

Pain Assessment and Management 8
those who require mechanical ventilation to procedural pain, and the Neonatal Pain Agitation and Sedation Scale (N-PASS; Hummel, Puchalski, Weiss, & Creech, 2003) that was developed to measure ongoing
and acute pain and sedation in preterm and term neonates. More research to establish reliability and validity of these measures is needed.

Pain Assessment and Management 9
Guideline IIIUse both nonpharmacologic and pharmacologic therapies to control or prevent pain (AHCPR, 1992; AAP/CPS, 2000, 2006; Anand & IEBGNP, 2001; IASP, 2005; NANN, 2001).
Key PointsA. Nonpharmacologic strategies to promote comfort
and stability are vitally important during all minor to moderately painful procedures. Nonpharmaco-logical interventions minimize the infant’s pain and distress while maximizing the infant’s regulatory and coping abilities. Pharmacologic therapies should always be accompanied by nonpharmacologic com-fort measures as these strategies provide additive or synergistic benefits (Franck & Lawhon, 2000).
1. It is important, when possible, to reduce the number of painful procedures performed on infants (Franck & Lawhon, 2000; Leslie & Marlow, 2006). This can be accomplished by using noninvasive monitoring techniques such as oxygen saturation monitors as well as critically evaluating the need for all caregiving practices, such as the number and grouping of laboratory and diagnostic procedures, and by scheduling clinical procedures on the basis of medical necessity rather than routine.
2. Painful procedures should not be performed at the same time as other, nonemergency routine care (e.g., taking vital signs, changing a diaper). Evidence suggests that after exposure to a pain-ful stimulus, a preterm infant’s pain sensitivity is accentuated by an increased excitability of noci-ceptive neurons in the dorsal horn of the spinal cord (Fitzgerald, Millard, & McIntosh, 1989; Fitzgerald, Shaw, & McIntosh, 1988; Holsti, Grunau, Oberlander, & Whitfield, 2005). This sensory hypersensitivity, referred to as the wind-up phenomenon, may exist for prolonged periods after a painful stimulus. It can cause other, nonnoxious stimuli (e.g., handling, physical examination, nursing procedures) to be perceived as painful because of heightened activity in noci-ceptive pathways. Stress cues must be the guide for determining the timing of painful and other, nonemergency clinical care activities.
3. Containment and positioning strategies can be used to maintain midline flexion and facilitate hand-to-mouth opportunities, thus helping infants achieve self-regulation.a. Handling and immobilization in preparation
for painful procedures can heighten activity in nociceptive pathways and accentuate infants’ pain responses (AAP, 1999; Porter, Miller, Cole, & Marshall, 1991; Porter,
Wolf, & Miller, 1998). Every attempt should be made to minimize handling before a painful procedure.
b. Swaddling during and after a heelstick reduces the physiological and behavioral pain indicators in preterm neonates (Cignacco et al., 2007; Fearon, Kisilevsky, Hains, Muir, & Tranmer, 1997).
c. A hand-swaddling technique, known as facilitated tucking (i.e., holding the infant’s extremities flexed and contained close to the trunk), during a painful procedure may sig-nificantly reduce pain responses in preterm infants (Cignacco et al., 2007; Corff, Seide-man, Venkataraman, Lutes, & Yates, 1995; Ward-Larson, Horn, & Gosnell, 2004).
4. Excessive and unpredictable sound levels and bright or continuous lighting levels in the NICU have been associated with increased physiologic and behavioral stress responses in preterm infants (Long, Lucey, & Philips, 1980; Shiroiwa, Kami-ya, & Uchiboi, 1986). Although research has not systematically documented the effects of sound and lighting levels on pain responses in preterm infants, clinical experience suggests that light and sound levels should be as low as possible during painful procedures (Franck & Lawhon, 2000). A consensus group on NICU design suggests that light levels should not exceed 60 footcandles, which is equivalent to soft room lighting. Task lights and phototherapy lights can exceed 300 footcandles, and therefore caution should be taken to protect infants’ eyes during the use of these light sources.
5. Nonnutritive sucking (NNS) is the most widely studied nonpharmacological approach to pain management. The mechanisms of action are thought to be related to the activation of non-opioid pathways as the infant sucks on the pacifier. Pain-relieving effects of NNS cease after the pacifier is removed from the mouth (Boyle et al., 2006; Campos, 1989; Carbajal, Chauvet, Couderc, & Olivier-Martin, 1999; Field & Gold-son, 1984; Gibbins, Stevens, & Hodnett, 2002; Marchette, Main, Redick, Bagg, & Leatherland, 1991; Miller & Anderson, 1993; Shiao, Chang, Lannon, Yarandi, 1997; Stevens et al., 1999).
6. The safety and efficacy of sucrose for preterm and term infants has been reported in many studies. A systematic review of 21 randomized controlled trials found that sucrose decreased crying time, heart rate, facial action, and compos-ite pain scores during heel lance and venipuncture (Stevens, Yamada, & Ohlsson, 2004).

Pain Assessment and Management 10
a. The most effective dose of sucrose remains unclear, but ranges between 0.05 and 2 ml of a 24% solution have been reported. Sucrose is most effective when it is administered approximately 2 minutes before the pain-ful stimulus (Stevens, Taddio, Ohlsson, & Einarson, 1997). This 2-minute time interval is thought to coincide with the endogenous opioid release triggered by the sweet taste of sucrose (Stevens et al., 1999). Sucrose is optimally administered to the tip of the tongue where sweet receptors lie. No effect is obtained when given by nasogastric (NG) tube and may not be effective via bottle or nipple when given to an infant with an efficient suck, bypassing the tip of the tongue.
b. There is less evidence for the safety and efficacy of sucrose for infants less than 27 weeks gestation; therefore, its use must be considered on an individual basis. A study by Willis, Chabot, Radde, and Chance (1977) suggests that the hyperosmolality of a 20% sucrose solution (0.5–1 ml mixed with calcium lactate) given 20 minutes before feedings by NG may have contrib-uted to a higher-than-normal incidence of necrotizing enterocolitis (NEC) in very-low-birthweight infants. The study failed to consider other risk factors such as immaturity, presence of umbilical lines, administration via NG tube, or the hyper-osmolar calcium solution administered with the sucrose as causative factors for NEC. Johnston and colleagues (2002) compared motor development, alertness and neurobehavioral outcomes in preterm infants less than 31 weeks gestation who received either sucrose or water for every painful procedure during the first 7 days of life. The study found a dose-related response, with infants who received more doses of sucrose having lower scores on motor development tests at 36 and 40 weeks postconceptional age. A more recent study by Stevens and colleagues (2005) did not demonstrate any adverse events, clinical outcomes, or neurobiological risk status in infants greater than 26 weeks gestation who received 24% sucrose plus pacifier prior to all painful procedures in the NICU during the first 28 days of life.
c. The long-term safety of repeated doses of sucrose in neonates, particulary ELBW
infants, has not been established and further research is needed (Stevens et al., 2004).
7. Breastfeeding or breast milk for procedural pain in neonates has been well researched. A review of the research recommends that, if available, breastfeeding or breast milk should be used to alleviate procedural pain in neonates undergoing a single painful procedure, as compared to placebo, positioning, or no intervention. Administration of glucose or sucrose had similar effective-ness as breastfeeding for reducing pain. The effectiveness of breast milk for repeated painful procedures is not established and further research is needed (Shah, Aliwalas, & Shah, 2006).
B. Opioid analgesics and local anesthetics are the most com-mon pharmacologic interventions used with neonates.
1. The first goal of pharmacologic management is to distinguish between the need for pain relief and the need for sedation. Opioids are generally used in clinical situations when severe pain is assessed or anticipated (AHCPR, 1992; Simons & Anand, 2006). Sedatives blunt behavioral responses to noxious stimuli without providing pain relief. Therefore, sedatives should not be used unless pain has been ruled out (Hartley, Franck, & Lundergan, 1989).
2. Intravenous opioids, particularly morphine and fentanyl, remain the most common analgesics administered in the NICU (Simons & Anand, 2006). There is little scientific evidence dem-onstrating the pharmacodynamics of opioid usage in the neonatal population (Franck & Miaskowski, 1998; Simons & Anand). However, published dosing guidelines exist to guide the safe administration of opioids in monitored infants (see Table 1).
3. Most studies measure the pharmacokinetics of opioids after a single intravenous dose or dur-ing a continuous intravenous infusion. Limited data suggest that there is no substantial benefit to administering a continuous infusion of opioids over intermittent dosing in neonates (Bouwmeester et al., 2001; Bouwmeester, van den Anker, Hop, Anand, & Tibboel, 2003).
4. Infants less than 1 month old have been found to have longer elimination half-lives and delayed clearance of opioids compared with adults or children older than 1 year (Franck & Miaskowski, 1998). As a result, longer dosing intervals are often indicated for neonates, com-pared with those for older infants and children.
5. Enterohepatic recirculation may contribute to prolonged clearance and elimination in infants (Franck & Miaskowski, 1998). As a result, higher

Pain Assessment and Management 11
plasma concentrations of opioids for longer periods of time have been demonstrated in both preterm and full-term infants as compared with older children. Therefore, monitoring should be continued for several hours after opioids have been discontinued (Franck & Miaskowski).
6. Variations in response to opioids between infants and older children or adults may be due to differences in the number and type of mu receptors in the brain and spinal cord. Younger infants may require significantly higher opioid concentrations to achieve adequate analge-sia than older children do (Dahlstrom, Bolme, Feychting, Noack, & Paalzow, 1979; Lynn, Opheim, & Tyler, 1984; Olkkola, Maunuksela, Korpela, & Rosenberg, 1988).
7. Regular assessments are needed, using a valid and reliable neonatal pain instrument, to ensure the adequacy of opioid therapy.
8. Regular assessments also are needed to identify the side effects associated with opioid therapy (Franck & Miaskowski, 1998). Although opioids are often withheld because of a fear of opioid-induced cardiorespiratory side effects, few data are available to support this concern (Farrington, McGuinness, Johnson, Erenberg, & Leff, 1993; Franck & Miaskowski; Koren et al., 1985; Pur-cell-Jones, Dormon, & Sumner, 1987). Side effects often can be minimized by administering boluses slowly (Franck & Miaskowski; Gregory, 1994a, 1994b; Yaster & Deshpande, 1988).
9. Sedation level should also be assessed regularly, monitoring for the attainment of desired seda-tion level or inadvertent over-sedation.
10. Recent research highlights the potential for increased adverse neurologic outcomes in ven-tilated infants with morphine administration, particularly in hypotensive infants (Anand et al., 2004; Aranda et al., 2005; Hall, Kronsberg, Barton, Kaiser, & Anand, 2005). Closely monitor the infant for hypotension.
11. Neonates who require opioid therapy for more than several days may develop physical depen-dence and then exhibit withdrawal symptoms if the opioid is stopped abruptly or weaned too rapidly. Withdrawal symptoms include neuro-logic excitability, gastrointestinal dysfunction, and other signs such as poor weight gain. The prevalence of opioid withdrawal is greater in infants who have received fentanyl as opposed to morphine. Similarly, infants who receive higher total doses or longer duration of infusion are significantly more likely to experience withdrawal (Dominguez, Lomako, Katz, &
Kelly, 2003). Data are insufficient to determine the optimal weaning rate of opioids to prevent withdrawal symptoms in neonates on opioid therapy. Ducharme, Carnevale, Clermont, and Shea (2005) reported that adverse withdrawal symptoms in children who received continuous infusions of opioids or benzodiazepines could be prevented when the daily rate of weaning did not exceed 20% for children who received opioids or benzodiazepines for 1–3 days; 13%–20% for 4–7 days; 8%–13% for 8–14 days; 8% for 15–21 days; and 2%–4% for more than 21 days, respectively. An opioid-weaning protocol and behavioral withdrawal scale should be used for infants weaning from prolonged opioid therapy. The Neonatal Abstinence Syndrome scale (Finnegan, Kron, Connoughton, & Emich, 1975) or other valid measures can be used to guide rate of opioid weaning and monitor for withdrawal symptoms.
12. Prolonged use of opioids may lead to analgesic tolerance, requiring increased dosing to attain pain relief. An infant who becomes tolerant to the cur-rent dosage may exhibit pain behaviors, increased wakefulness, and increased sympathetic responses such as high-pitched crying and tremors when handled or disturbed (Suresh & Anand, 1998). Tolerance to opioids is managed by increasing the dosage, although the use of adjunctive analgesics can be clinically beneficial (Anand & Ingraham, 1996; Franck & Vilardi, 1995).
C. Nonopioid analgesics Acetaminophen is a nonopioid analgesic useful for
short-term management of mild to moderate pain in neonates. Although acetaminophen has been shown to significantly reduce pain response dur-ing skin excision and reduce comfort scores at 6 hours following the circumcision procedure (How-ard, Howard, & Weitzman, 1994), other studies have failed to demonstrate efficacy resulting from acute-tissue injury of heelstick and postoperative pain relief after cadiac surgery (Shah, Taddio, & Ohls-son, 1998; van Lingen et al., 1999). The results from these studies suggest that acetaminophen may be more appropriate for mild-to-moderate dull, continuous pain that results from inflammatory conditions (Anand, Menon, Narsinghani, & McIntosh, 2000).
D. Topical anesthetics 1. Eutectic Mixture of Local Anesthetics (EMLA)
cream, a eutectic mixture of lidocaine and prilocaine, is approved for use in infants who have a gestational age of 37 weeks or more (AstraZeneca, 1999). EMLA cream requires 1 hour of skin contact for efficacy. A systematic

Pain Assessment and Management 12
review of 11 studies of EMLA cream as a treat-ment for acute pain in infants was conducted by Taddio, Ohlsson, Einarson, Stevens, and Koren (1998). Data suggest that EMLA cream reduces pain during circumcision, venipuncture, arterial puncture, and percutaneous venous catheter placement. The data, however, failed to support the efficacy of EMLA cream in managing pain from heelstick. The potential increased risk of methemoglobinemia can be minimized if its use is limited to no more than once daily on intact skin only, and it should not be used with other drugs known to cause methemoglobinemia such as acetaminophen, phenytoin, phenobarbital, or nitroprusside (Brisman, Ljung, Otterbom, Larsson, & Andreasson, 1998).
2. Tetracaine 4% gel (Ametop) has also been rela-tively well investigated in neonates. Tetracaine produces local anesthesia within 30–45 minutes. Ametop has been shown to be beneficial for venipuncture, vaccination, and IV insertion (O’Brien, Taddio, Lyszkiewicz, & Koren, 2005), but it is ineffective for heelsticks and peripherally inserted central catheters.
3. Liposomal lidocaine cream (LMX 4%) is a relatively new topical anesthetic for use in new-borns. Several studies in older children have evaluated the efficacy of LMX and EMLA dur-ing peripheral intravenous catheter insertion and found a 30-minute application of LMX to be as effective as a 60-minute application of EMLA for producing topical anesthesia for peripheral intravenous access (Eichenfield, Funk, Fallon-Friedlander, & Cunningham, 2005; Kleiber, Sorenson, Whiteside, Gronstal, & Tannous, 2002; Koh et al., 2004). Similar results were found in a recent study in neonates in reducing circumcision pain in term newborns (Lehr et al., 2005). LMX may be a better choice than EMLA because of its faster onset of action and no risk of methemoglobinemia. Further studies in neonates are needed to establish the safety and efficacy of LMX for management of proce-dural pain in neonates.
E. Procedural pain is common in the NICU and should be managed with a combination of nonpharmacologic and pharmacologic interventions (AAP/CPS, 2006; Anand & IEBGNP, 2001; Anand et al., 2005). Anand and IEBGNP provide guidelines for preventing and treating pain associated with commonly per-formed procedures in the NICU (Table 2).
1. Heelsticka. The significant pain response to heelstick
can be explained by the painful nature of
the lancing procedure in combination with the squeezing of the heel to obtain the blood sample.
b. Although data are sparse, it appears reason-able to recommend that only spring-loaded mechanical lancets be used for heelstick procedures. The use of mechanical lancets results in less bruising, less need for repeat punctures, and fewer behavioral and physi-ologic distress responses (Harpin & Rutter, 1983; McIntosh et al., 1994). McIntosh and colleagues reported that use of a mechani-cal lancet was more effective than EMLA cream or tactile and vocal stimulation in reducing infants’ pain response to the heel-stick procedure.
c. Barker, Willetts, Cappendijk, and Rutter (1996) found that heel warming had no effect on infant responses to pain during a heelstick procedure.
d. Evidence-based interventions to reduce pain associated with heelsticks include pacifier with sucrose, swaddling, contain-ment, facilitated tucking, breastfeeding, and skin-to-skin contact with the mother (Anand & IEBGNP, 2001).
2. Circumcisiona. Although the procedure is not medically
necessary, some parents or caregivers choose to have their infants circumcised. Procedural analgesia should be provided during circumcision (AAP, 1999).
b. Subcutaneous ring block appears to pro-vide superior analgesia; however, the AAP policy statement also endorses the use of dorsal penile nerve blocks and EMLA cream for pain associated with circumcision (AAP, 1999).
c. Containment, facilitated tucking, hand-to-mouth opportunities, and flexed positioning should be used to decrease the infant’s dis-tress from the procedure (AAP, 1999).
d. The use of a sucrose-dipped pacifier during the procedure and acetaminophen adminis-tered before or immediately following can supplement the above analgesic approaches (AAP, 1999).
3. Venipuncture may be preferable to heelstick in minimizing procedure-related pain in full-term infants (Anand & IEBGNP, 2001). A systematic review of four randomized, controlled trials of full-term infants found that pain scores were significantly lower with venipuncture as com-pared to heelstick (Shah & Ohlsson, 2004).

Pain Assessment and Management 13
Another study by Ogawa and colleagues (2005) demonstrated that pain scores during venipunc-ture were lower than scores during heelstick. The researchers also reported that venipuncture scores without sucrose were significantly lower than the heelstick group with sucrose. However, frequent venipuncture for blood sampling is not feasible for most infants in the NICU, neces-sitating the continued use of heelsticks. Support during venipuncture includes swaddling, facilitated tucking, sucrose water, and topical anesthetic cream in infants ≥37 weeks gestation.
4. Technician expertise, such as the skill of the oper-ator, influences pain responses in infants (Grunau & Craig, 1987). Ensuring staff competence to perform required procedures may reduce the number of painful procedures to which an infant is exposed by reducing the number of failed attempts (Simons et al., 2003). Competence levels of the personnel performing procedures on hos-pitalized infants should be monitored.
F. Mechanical ventilation Mechanical ventilation via an endotracheal tube is
described as painful and distressful by adults and children, requiring analgesia and sedation. Histor-ically, infants in the NICU, particularly preterm infants, have received little or no treatment of pain and distress while ventilated, with wide variations in beliefs and practice. A recent, large, multicenter trial of morphine drip versus placebo in ventilated infants found no improvement in short-term neurologic out-comes and worse outcomes in some subgroups (Anand et al., 2004; Aranda et al., 2005). A secondary analysis by Hall and colleagues (2005) found that open-label bolus morphine in preterm neonates with preexisting hypotension who were receiving preemptive analgesia was associated with severe intraventricular hemorrhage and death. A systematic review of 13 randomized, con-trolled trials found that opioids reduced pain scores but did not alter the risk of poor neurologic outcome, with the conclusion that there is insufficient evidence available to recommend the routine use of opioids in mechanically ventilated neonates (Bellu, de Waal, & Zanini, 2005).
G. Perioperative pain management 1. Operative anesthesia should be provided to all
infants by a competent professional. 2. Postoperative pain management
a. Opioids should be administered around the clock or via continuous infusion. The dura-tion of this administration is dependent upon the type and invasiveness of the surgical procedure, the infant’s status postopera-tively, and pain assessment scoring.
b. Data are inconsistent on whether non-steroidal antiinflammatory drugs and acetaminophen provide clinically important postoperative analgesia after minor or major surgery in neonates. Data are also unclear on whether these agents provide clinically important opioid-sparing effects after sur-gery (Berde et al., 2005).
H. Pain management at end of life 1. Although it is common practice to administer
opioid agents to dying adults, opioids are not routinely administered to critically ill or dying infants when life support is being withdrawn or withheld (Partridge & Wall, 1997).
2. Given the difficulty of accurate pain assessment in neonates at the end of life (EOL), caregivers should consider risk factors for pain and use physiologic measures to guide pain management decisions (Walden, Sudia-Robinson, & Carrier, 2001).
3. Continuous infusions of opioids are often required to manage pain at EOL and should be titrated to desired clinical response (analgesia; Anand et al., 2000). Opioid doses well beyond those described for standard analgesia are often required for infants who are in severe pain or who have developed tolerance after the prolonged use of opioids (Partridge & Wall, 1997).
4. Physiologic comfort measures may palliate pain and distress in infants at EOL and include reduction of noxious stimuli, organization of caregiving, and positioning and containment strategies (Walden et al., 2001).
I. Long-term effects of pain The long-term effects of pain in animals are clear, with
changes observed in pain thresholds, social behaviors, stress responses, and pain responses to nonpainful stim-uli (Fitzgerald & Anand, 1993; Plotsky, Bradley, & Anand, 2000; Reynolds, Alvares, Middleton, & Fitzgerald, 1997; Ruda, Ling, Hohmann, Peng, & Tachibana, 2000). Preliminary human data suggest early pain experiences may alter future pain responses. Johnston and Stevens (1996) compared pain responses of neonates who were born at 28 weeks of gesta-tion and were hospitalized in a NICU for 4 weeks (32 weeks postconceptional age) to neonates who were born at 32 weeks of gestation. Heart rate, oxy-gen saturation, and three facial actions (brow bulge, nasolabial furrow, and eye squeeze) were used as individual pain indicators. Neonates were observed during a routine heel lance. Neonates who had spent 4 weeks in the NICU (less mature) had decreased behavioral response and significantly higher heart and lower oxygen saturation at the time of the heel lance than neonates born at 32 weeks. Taddio,

Pain Assessment and Management 14
Goldbach, Ipp, Stevens, and Koren (1995) examined the effectiveness of EMLA for relieving procedur-al pain associated with immunization in 4- and 6-month-old infants. Males circumcised with-in 2 days of birth had significantly longer crying bouts (53 seconds versus 19 seconds, p = .02) and
higher pain intensity scores, as measured on the Visu-al Analogue Scale (VAS; 8 versus 6, p = .01), at immunization at 4 or 6 months of age than males who were not circumcised. This finding was con-firmed in subsequent research (Taddio, Katz, Ilersich, & Koren, 1997).

Pain Assessment and Management 15
Guideline IVA collaborative, interdisciplinary approach to pain con-trol, including all members of the healthcare team and infant’s family, should be used to develop a pain man-agement plan. Include the input of all members of the healthcare team as well as that of the infant’s family when-ever possible (AHCPR, 1992; AAP, 1999; IASP, 2005; JCAHO, 2001; NANN, 2001).
Key PointsA. Parents play a key role in assessing and managing
their infant’s pain. 1. Parents have many concerns and fears about
their infant’s pain and about the medications used in the treatment of pain (Franck, Allen, Cox, & Winter, 2005; Gale, Franck, Kools, & Lynch, 2004). Parents may fear the effects of pain on their child’s development. They may also fear that their infant may become “addicted” to the analgesics (Franck et al., 2000).
2. According to Harrison (1993), a key principle of family-centered neonatal care is that “parents and professionals must work together to acknowledge and alleviate the pain of infants in intensive care” (p. 646). To accomplish this, parents and healthcare professionals must talk openly and honestly about acute and chronic pain associated with medical diseases as well as about pain associated with operative, diagnostic, and thera-peutic procedures.
3. Parents should be informed that effective pain relief is an important part of their infant’s care in the NICU (AHCPR, 1992).
4. Healthcare providers are obligated to ensure that parents receive accurate and unbiased information about the risks and benefits of (as well as alternatives to) analgesia and anesthesia, so that they can make informed treatment choices (Harrison, 1993).
5. Healthcare providers should explore parents’ cultural and religious beliefs about pain. These beliefs should be taken into account when determining a pain-management plan.
6. Parents have the right to seek another medical opinion or to refuse a burdensome course of therapy (Harrison, 1993).
7. Parents should be taught to observe how their infant expresses pain through physiologic and behavioral cues.
8. Parents, in addition to making decisions about analgesia and anesthesia options, often are ready, willing, and able to help caregivers provide nonpharmacologic pain relief during minor painful procedures. Parents should be taught individualized techniques that are comforting to their infant.
9. Institutions are responsible for documenting the degree of parents’ satisfaction with the pain management their child is receiving in the hospital (AHCPR, 1992; IASP, 2005; JCAHO, 2001; NANN, 2001).

Pain Assessment and Management 16
Guideline VPain assessment and management practices should be documented in a manner that facilitates regular reassess-ment and follow-up intervention (IASP, 2005; JCAHO, 2001).
Key PointsA. Pain has been termed “the fifth vital sign” (American
Pain Society [APS], 1995). An infant’s pain should be assessed upon admission and at regularly defined intervals throughout the hospitalization (AAP/CPS, 2000; APS; IASP, 2005; JCAHO, 2001).
B. Pain scores, interventions, and responses should be documented in a way that facilitates high visibility and regular review by members of the healthcare team. Figure 4 shows a tool designed to accomplish this objective.
C. Pain scores should be recorded on the nursing prog-ress record, using a valid and reliable pain instrument at time intervals defined in hospital policy.
D. Environmental factors that appear to reduce or exac-erbate the infant’s pain should be documented.
E. Nonpharmacologic strategies used alone or in con-junction with pharmacologic therapy should be documented.
F. Pharmacologic interventions—including the medica-tion administered, as well as the time, dosage, route, and side effects—should be recorded on the nursing progress or medication record, as dictated by hospital policy.
G. Patient response to interventions, both pharmacologic and nonpharmacologic, should be documented, using valid and reliable assessment methods.
H. The level of parental involvement with and knowledge of their infant’s pain cues and current pain manage-ment should be recorded.

Pain Assessment and Management 17
Guideline VIPolicies and procedures that support and promote opti-mal pain assessment and management practices should be established by institutions caring for infants (AHCPR, 1992; AAP/CPS, 2000; JCAHO, 2001).
Key PointsA. Policies and procedures related to pain assessment
and management should: 1. Define each multidisciplinary team member’s
responsibilities and scope of practice in assess-ing and managing pain
2. Outline an education and competency assess-ment program
3. List indications for baseline monitoring as well as frequency of assessment for infants expe-riencing ongoing or recurrent pain caused by surgery, disease, or diagnostic or therapeutic procedures
4. List pain instruments approved for use with infants. Although consistency of instrument use is encouraged across hospital units, the needs of the patient population should be the determining factor in the selection of pain instruments. Spe-cific instruments may be needed to assess pain in special populations (e.g., extremely preterm infants or infants who undergo prolonged hospi-talization and experience chronic pain)
5. Detail approved nonpharmacologic pain relief measures
6. Outline an approach to pharmacologic pain management
7. Discuss the role of parents in pain assessment and management
8. Describe documentation requirements

Pain Assessment and Management 18
Guideline VIIInstitutions caring for infants should collect data to mon-itor the appropriateness and effectiveness of their pain management practices (AHCPR, 1992; IASP, 2005; JCAHO, 2001).
Key PointsA. In addition to reviewing the current pain standards
of professional and accrediting organizations, insti-tutions should perform an extensive review of the literature to determine the evidence base on pain assessment and management in infants. Based on this review, institutional barriers to optimal pain assess-ment and management practices should be identified.
B. The creation of a multidisciplinary pain team should be considered to address the identified barriers and facilitate improvements in pain management practices for infants. The team’s objectives might include the following:
1. Choose a pain assessment tool 2. Develop standardized documentation, including
pain score, interventions, and infant responses to interventions
3. Develop policies or a protocol to assess and manage pain in newborns
4. Create parent-education materials about pain assessment and management
5. Identify outcome measures relating to pain assessment and management
6. Educate nursing staff on the use of tools, documentation, pain reporting, pain policies or protocol, and appropriate intervention strategies
C. Outcome measures should be defined and baseline data collected before and after recommended practice changes are implemented so as to evaluate the effect of these changes on patient outcomes. Outcome mea-sures that might be monitored include:
1. Intervals of pain assessment 2. Types and appropriateness of pain medications
ordered 3. Congruence between medications ordered and
medications administered 4. Length of time between identification of pain
and intervention 5. Number and types of nonpharmacologic
interventions 6. Patient responses to interventions, including
side effects 7. Parent education about infant pain cues and
ways to provide comfort 8. Extent of parental involvement in comforting
their infant 9. Parental satisfaction with pain management for
their infant
ConclusionNurses play an essential role in optimizing pain assess-ment and management in the NICU. Nurses are in a key position to observe infant response to painful pro-cedures or clinical conditions, using valid and reliable pain instruments. The nurse, in conjunction with the healthcare team and the parents, uses assessment data to effectively implement nonpharmacologic and pharma-cologic pain management strategies. The nurse is an advocate for the infant, minimizing pain and distress throughout the infant’s hospital stay. Nurses also play a role in measuring patient outcomes and participating in interdisciplinary initiatives regarding pain assessment and management. Finally, the nurse plays a role in on-going research and education of the profession regarding best practices on pain assessment and management in neonates.

Pain Assessment and Management 19
ReferencesAgency for Health Care Policy and Research. (1992). Acute
pain management in infants, children, and adolescents: Operative and medical procedures: Quick reference guide for clinicians. Rockville, MD: U.S. Department of Health and Human Services.
American Academy of Pediatrics/Canadian Paediatric Society. (2000). Prevention and management of pain and stress in the neonate. Pediatrics, 105, 454–461.
American Academy of Pediatrics/Canadian Paediatric Society. (2006). Prevention and management of pain and stress in the neonate: An update. Pediatrics, 118, 2231–2241.
American Academy of Pediatrics, Task Force on Circumcision. (1999). Circumcision policy statement. Pediatrics, 103, 686–693.
American Pain Society (1995). Pain: The fifth vital sign. Retrieved September 9, 2000, from www.ampainsoc.org.
Anand, K. (1998). Clinical importance of pain and stress in preterm infants. Biology of the Neonate, 73, 1–9.
Anand, K., & Craig, K. (1996). New perspectives on the defi-nition of pain. Pain, 67, 3–6.
Anand, K., & Ingraham, J. (1996). Tolerance, dependence, and strategies for compassionate withdrawal of analge-sics and anxiolytics in the Pediatric ICU. Critical Care Nurse, 16(6), 87–93.
Anand, K. J., Hall, R. W., Desai, N., Shephard, B., Bergqvist, L. L., Young, T. E., et al. (2004). Effects of morphine analgesia in ventilated preterm neonates: Primary out-comes from the NEOPAIN randomised trial. Lancet, 363(9422), 1673–1682.
Anand K. J. S., & International Evidence-Based Group for Neonatal Pain. (2001). Consensus statement for the prevention and management of pain in the newborn. Archives of Pediatric Adolescent Medicine, 155, 173–180.
Anand K. J. S., Johnston, C. C., Oberlander, T. F., Taddio, A., Tutag Lehr, V., & Walco, G. A. (2005). Analgesia and local anesthesia during invasive procedures in the neo-nate. Clinical Therapeutics, 27(6), 844–876.
Anand K. J. S., Menon, G., Narsinghani, U., & McIntosh, N. (2000). Systemic analgesic therapy. In K. J. S. Anand, B. J. Stevens, & P. J. McGrath (Eds.), Pain in infants (2nd ed., pp. 159–188). Amsterdam: Elsevier.
Aranda, J. V., Carlo, W., Hummel, P., Thomas, R., Lehr, V. T., & Anand, K. J. S. (2005). Analgesia and seda-tion during mechanical ventilation in neonates. Clinical Therapeutics, 27(6), 877–899.
AstraZeneca (1999, May 21). FDA approves EMLA cream for use in full-term neonates, supporting its use in new-born circumcision. Retrieved September 12, 2000, from www.emla-usa.com/news/pr52199.htm.
Barker, D. P., Willetts, B., Cappendijk, V. C., & Rutter, N. (1996). Capillary blood sampling: Should the heel be warmed? Archives of Disease in Childhood. Fetal and Neonatal Edition, 74(2), F139–F140.
Barr, R. (1992). Is this infant in pain? Caveats from the clini-cal setting. APS Journal, 1, 187–190.
Bellu, R., de Waal, K. A., & Zanini, R. (2005). Opioids for neonates receiving mechanical ventilation. Cochrane Database of Systematic Reviews, 1, CD004212.
Berde, B. B., Jaksic, T., Lynn, A. M., Maxwell, L. G., Soriano, S. G., & Tibboel, D. (2005). Anesthesia and analgesia during and after surgery in neonates. Clinical Therapeutics, 27(6), 900–921.
Bildner, J., & Krechel, S. (1996). Increasing staff nurse awareness of postoperative pain management in the NICU. Neonatal Network, 15(1), 11–16.
Blauer, T., & Gerstmann, D. (1998). A simultaneous compari-son of three neonatal pain scales during common NICU procedures. Clinical Journal of Pain, 1, 39–47.
Bouwmeester, N. J., Anand, K. J., van Dijk, M., Hop, W. C., Boomsma, F., & Tibboel, D. (2001). Hormonal and metabolic stress responses after major surgery in children aged 0–3 years: A double-blind, randomized trial com-paring the effects of continuous versus intermittent mor-phine. British Journal of Anaesthesia 87(3), 390–399.
Bouwmeester, N. J., van den Anker, J. N., Hop, W. C., Anand, K. J., & Tibboel, D. (2003). Age- and therapy-related effects on morphine requirements and plasma concentra-tions of morphine and its metabolites in postoperative infants. British Journal of Anesthesia, 90(5), 642–652.
Boyle, E. M., Freer, Y., Khan-Orakzai, Z., Watkinson, M., Wright, E., Ainsworth, J. R., et al. (2006). Sucrose and non-nutritive sucking for the relief of pain in screening for retinopathy of prematurity: A randomised controlled trial. Archives of Disease in Childhood. Fetal and Neonatal Edition, 91(3), F166–F168.
Brisman, M., Ljung, B. M., Otterbom, I., Larsson, L. E., & Andreasson, S. E. (1998). Methemoglobin formation after the use of EMLA cream in term neonates. Acta Paediatrica, 7(11), 1191–1194.
Campos, R. (1989). Soothing pain-elicited distress in infants with swaddling and pacifiers. Child Development, 60, 781–792.
Carbajal, R., Chauvet, X., Couderc, S., & Olivier-Martin, M. (1999). Randomised trial of analgesic effects of sucrose, glucose, and pacifiers in term neonates. British Medical Journal, 319, 1393–1397.
Carrier, C., & Walden, M. (2001). Integrating research and standards to improve pain management practices for new-borns and infants. Newborn and Infant Nursing Reviews, 1(2), 122–131.
Cignacco, E., Hamers, J. P., Stoffel, L., van Lingen, R. A., Gessler, P., McDougall, J., et al. (2007). The efficacy of non-pharmacological interventions in the management of procedural pain in preterm and term neonates: A systematic literature review. European Journal of Pain, 11, 139–152.
Cignacco, E., Mueller, R., Hamers, J. P., & Gessler, P. (2004). Pain assessment in the neonate using the Bernese Pain Scale for Neonates. Early Human Development, 78(2), 125–131.
Corff, K., Seideman, R., Venkataraman, P., Lutes, L., & Yates, B. (1995). Facilitated tucking: A nonpharmacologic comfort measure for pain in preterm infants. Journal of Obstetric, Gynecologic, and Neonatal Nursing, 24, 143–147.

Pain Assessment and Management 20
Craig, K., Whitfield, M., Grunau, R., Linton, J., & Hadjistavropoulos, H. (1993). Pain in the preterm neo-nate: Behavioral and physiological indices. Pain, 52, 287–299.
Dahlstrom, B., Bolme, P., Feychting, H., Noack, G., & Paalzow, L. (1979). Morphine kinetics in children. Clinical Pharmacology and Therapeutics, 26, 354–365.
Dominguez, K. D., Lomako, D. M., Katz, R. W., & Kelly, H. W. (2003). Opioid withdrawal in critically ill neonates. Annals of Pharmacotherapy, 37(4), 473–477.
Ducharme, C., Carnevale, F. A., Clermont, M. S., & Shea, S. (2005). A prospective study of adverse reactions to the weaning of opioids and benzodiazepines among critically ill children. Intensive and Critical Care Nursing, 21(3), 179–186.
Duhn, L., & Medves, J. (2004). A systematic integrative review of infant pain assessment tools. Advances in Neonatal Care: Official Journal of the National Association of Neonatal Nurses, 4(3), 126–140.
Eichenfield, L. F., Funk, A., Fallon-Friedlander, S., & Cunningham, B. B. (2005). A clinical study to evaluate the efficacy of ELA-Max as compared with eutectic mix-ture of local anesthetics cream for pain reduction of veni-puncture in children. Pediatrics, 109(6), 1092–1099.
Farrington, E., McGuinness, G., Johnson, G., Erenberg, A., & Leff, R. D. (1993). Continuous intravenous morphine infusion in postoperative newborn infants. American Journal of Perinatology, 10(1), 84–87.
Fearon, I., Kisilevsky, B. S., Hains, S. M., Muir D. W., & Tranmer, J. (1997). Swaddling after heel lance: Age- specific effects on behavioral recovery in preterm infants. Journal of Developmental and Behavioral Pediatrics, 18, 222–232.
Field, T., & Goldson, E. (1984). Pacifying effects of nonnutri-tive sucking on term and preterm infants during heelstick procedures. Pediatrics, 74, 1012–1015.
Finnegan, L. P., Kron, R. E., Connoughton, J. F., & Emich, J. P. (1975). A scoring system for evaluation and treatment of the neonatal abstinence syndrome: A new clinical and research tool. In P. I. Morselli, S. Garatani, & F. Sereni (Eds.), Basic and therapeutic aspects of perinatal phar-macology (pp. 139–153). New York: Raven Press.
Fitzgerald, M., & Anand, K. J. S. (1993). Developmental neu-roanatomy and neurophysiology of pain. In N. Schechter & D. B. Berde (Eds.), Pain in infants, children and ado-lescents (pp. 11–32). Baltimore: Wilkins.
Fitzgerald, M., Millard, C., & McIntosh, N. (1989). Cutaneous hypersensitivity following peripheral tissue damage in newborn infants and its reversal with topical anaesthesia. Pain, 39, 31–36.
Fitzgerald, M., Shaw, A., & McIntosh, N. (1988). The post-natal development of the cutaneous flexor reflex: A com-parative study in premature infants and newborn rat pups. Developmental Medicine and Child Neurology, 30, 520–526.
Fitzgerald, M., & Shortland, P. (1988). The effect of neo-natal peripheral nerve section on the somadendritic growth of sensory projection cells in the rat spinal cord. Developmental Brain Research, 42, 129–136.
Franck, L. (1986). A new method to quantitatively describe pain behavior in infants. Nursing Research, 35(1), 28–31.
Franck, L. (1998). Identification, management, and preven-tion of pain in the neonate. In C. Kenner, J. Lott, & A. Flandermeyer (Eds.), Comprehensive neonatal nurs-ing: A physiologic perspective (2nd ed., pp. 778–803). Philadelphia: W. B. Saunders.
Franck, L., & Lawhon, G. (2000). Environmental and behav-ioral strategies to prevent and manage neonatal pain. In K. J. S. Anand, B. J. Stevens, & P. J. McGrath (Eds.), Pain in infants (2nd ed., pp. 203–216). Amsterdam: Elsevier.
Franck, L., & Miaskowski, C. (1998). The use of intravenous opioids to provide analgesia in critically ill, prema-ture infants: A research critique. Journal of Pain and Symptom Management, 15(1), 41–69.
Franck, L., & Vilardi, J. (1995). Assessment and management of opioid withdrawal in ill infants. Neonatal Network, 14(2), 39–48.
Franck, L. S., Allen, A., Cox, S., & Winter, I. (2005). Parents' views about infant pain in neonatal intensive care. Clinical Journal of Pain, 21(2), 133–139.
Franck, L. S., Boyce, W. T., Gregory, G. A., Jemerin, J., Levine, J, & Miaskowski, C. (2000). Plasma norepineph-rine levels, vagal tone index, and flexor reflex threshold in premature neonates receiving intravenous morphine during the postoperative period: A pilot study. Clinical Journal of Pain, 16(2), 95–104.
Fuller, B. (1991). Acoustic discrimination of three types of infant cries. Nursing Research, 40, 156–160.
Gale, G., Franck, L. S., Kools, S., & Lynch, M. (2004). Parents’ perceptions of their infant’s pain experience in the NICU. International Journal of Nursing Studies, 41(1), 51–58.
Gibbins, S., Maddalena, P., Moulsdale, W., Garrard, F., jan Mohamed, T., Nichols, A., et al. (2006). Pain assessment and pharmacologic management for infants with NEC: A retrospective chart audit. Neonatal Network, 25(5), 339–345.
Gibbins, S., & Stevens, B. (2003). The influence of ges-tational age on the efficacy and short-term safety of sucrose for procedural pain relief. Advances in Neonatal Care: Official Journal of the National Association of Neonatal Nurses, 3(5), 241–249.
Gibbins, S., Stevens, B., & Hodnett, E. (2002). Efficacy and safety of sucrose for procedural pain relief in preterm and term neonates. Nursing Research, 51(6), 375–382.
Gregory, G. (1994a). Anesthesia for premature infants. In G.A. Gregory (Ed.), Pediatric anesthesia (3rd ed., pp. 351–373). New York: Churchill Livingstone.
Gregory, G. (1994b). Pharmacology. In G. A. Gregory (Ed.), Pediatric anesthesia (3rd ed., pp. 13–45). New York: Churchill Livingstone.
Grunau, R., & Craig, K. (1987). Pain expression in infants: Facial action and cry. Pain, 28, 395–410.
Grunau, R., Johnston, C., & Craig, K. (1990). Neonatal facial and cry responses to invasive and non-invasive proce-dures. Pain, 42, 295–305.

Pain Assessment and Management 21
Grunau, R., Linhares, M. B., Holsti, L., Oberlander, T. F., & Whitfield, M. F. (2004). Does prone or supine position influence pain responses in preterm infants at 32 weeks gestational age? Clinical Journal of Pain, 20(2), 76–82.
Grunau, R., Whitfield, M., & Petrie, J. (1994). Pain sensitivity and temperament in extremely low-birth-weight premature tod-dlers and preterm and full-term controls. Pain, 58, 341–346.
Grunau, R., Whitfield, M., Petrie, J., & Fryer, E. (1994). Early pain experience, child and family factors, as pre-cursors of somatization: A prospective study of extremely premature and fullterm children. Pain, 56, 353–359.
Grunau, R. E., Holsti, L., Whitfield, M. F., & Ling, E. (2000). Are twitches, startles, and body movements pain indi-cators in extremely low birth weight infants? Clinical Journal of Pain, 16(1), 37–45.
Gunnar, M., Connors, J., Isensee, J., & Wall, L. (1988). Adrenocortical activity and behavioral distress in human newborns. Developmental Psychobiology, 21, 297–310.
Hall, R. W., Kronsberg, S. S., Barton, B. A., Kaiser, J. R., & Anand, K. J. (2005). Morphine, hypotension, and adverse outcomes among preterm neonates: Who’s to blame? Secondary results from the NEOPAIN trial. Pediatrics, 115(5), 1351–1359.
Harpin, V., & Rutter, N. (1983). Making heel pricks less pain-ful. Archives of Disease in Childhood, 58, 226–228.
Harrison, H. (1993). The principles for family-centered neo-natal care. Pediatrics, 92, 643–650.
Hartley, S., Franck, L., & Lundergan, R. (1989). Maintenance sedation of agitated infants in the NICU with chloral hydrate: New concerns. Journal of Perinatology, 9, 162–164.
Herr, K., Coyne, P. J., Key, T., Manworren, R., McCaffery, M., Merkel, S., et al. (2006). Pain assessment in the nonverbal patient: Position statement with clinical practice recom-mendations. Pain Management Nursing, 7(2), 44–52.
Hodgkinson, K., Bear, M., Thorn, J., & Van Blaricum, S. (1994). Measuring pain in neonates: Evaluating an instru-ment and developing a common language. Australian Journal of Advance Nursing, 12(1), 17–22.
Holsti, L., Grunau, R. E., Oberlander, T. F., & Whitfield, M. F. (2004). Specific Newborn Individualized Developmental Care and Assessment Program move-ments are associated with acute pain in preterm infants in the neonatal intensive care unit. Pediatrics, 114(1), 65–72.
Holsti, L., Grunau, R. E., Oberlander, T. F., & Whitfield, M. F. (2005). Prior pain induces heightened motor responses during clustered care in preterm infants in the NICU. Early Human Development, 81(3), 293–302.
Howard, C. R., Howard, F. M., & Weitzman, M. L. (1994). Acetaminophen analgesia in neonatal circumcision: The effect on pain. Pediatrics, 93, 641–646.
Hummel, P., Puchalski, M., Weiss, M., & Creech, S. (2003, May). N-PASS: Neonatal pain agitation and sedation scale—Reliability & validity. Poster presentation at the Pediatric Academic Societies Annual Meeting, Seattle, WA.
Hummel, P., & van Dijk, M. (2006). Pain assessment: Current status and challenges. Seminars in Fetal and Neonatal Medicine, 11, 237–245.
International Association for the Study of Pain. (2004). IASP Pain Terminology. Retrieved August 31, 2007, from www.iasp-pain.org/AM/Template.cfm?Section=Home&template=/CM/HTMLDisplay.cfm&ContentID=3088.
International Association for the Study of Pain. (2005). Core curriculum for professional education in pain [online]. Retrieved August 31, 2007, from www.iasp-pain.org/AM/Template.cfm?Section=Home&template=/CM/HTMLDisplay.cfm&ContentID=4223#TOC.
Johnston, C., Filion, R., Snider, L., Majnemer, A., Limperopoulos, C., Walker, C., et al. (2002). Routine sucrose analgesia during the first week of life in neonates younger than 31 weeks’ postconceptional age. Pediatrics, 110(3), 523–528.
Johnston, C., & Stevens, B. (1996). Experience in a neonatal intensive care unit affects pain response. Pediatrics, 98, 925–930.
Johnston, C., Stevens, B., Craig, K., & Grunau, R. (1993). Developmental changes in pain expression in premature, full-term, two- and four-month-old infants. Pain, 52, 201–208.
Johnston, C., Stevens, B., Franck, L., Jack, A., Stremler, R., & Platt, R. (1999). Factors explaining lack of response to heel stick in preterm newborns. Journal of Obstetric, Gynecologic, and Neonatal Nursing, 28, 587–594.
Johnston, C., Stevens, B., Yang, F., & Horton, L. (1995). Differential response to pain by very premature infants. Pain, 61, 471–479.
Joint Commission on Accreditation of Healthcare Organizations. (2001). Pain management standards for 2001. Retrieved September 9, 2000, from www.jcaho.org/standard/pm.html.
Kleiber, C., Sorenson, M., Whiteside, K., Gronstal, B. A., & Tannous, R. (2002). Topical anesthetics for intravenous insertion in children: A randomized equivalency study. Pediatrics, 110(4), 758–761.
Koh, J. L., Harrison, D., Myers, R., Dembinski, R., Turner, H., & McGraw, T. (2004). A randomized, double-blind comparison study of EMLA and ELA-Max for topical anesthesia in children undergoing intravenous insertion. Paediatric Anaesthesia, 14(12), 977–982.
Koren, G., Butt, W., Chinyanga, H., Soldin, S., Tan, Y. K., & Pape, K. (1985). Post-operative morphine infusion in newborn infants: Assessment of disposition characteris-tics and safety. Journal of Pediatrics, 107, 963–967.
Lawrence, J., Alcock, D., McGrath, P., Kay, J., MacMurray, S., & Dulberg, C. (1993). The development of a tool to assess neonatal pain. Neonatal Network, 12(6), 59–66.
Lehr, V. T., Cepeda, E., Frattarelli, D. A., Thomas, R., LaMothe, J., & Aranda, J. V. (2005). Lidocaine 4% cream compared with lidocaine 2.5% and prilocaine 2.5% or dorsal penile block for circumcision. American Journal of Perinatology, 22(5), 231–237.
Leslie, A., & Marlow, N. (2006). Non-pharmacological pain relief. Seminars in Fetal and Neonatal Medicine, 11, 246–250.
Long, J., Lucey, J., & Philips, A. (1980). Noise and hypoxemia in the intensive care nursery. Pediatrics, 65, 143–145.

Pain Assessment and Management 22
Lynn, A. M., Opheim, K. E., & Tyler, D. C. (1984). Morphine infusion after pediatric cardiac surgery. Critical Care Medicine, 12(10), 863–866.
Marchette, L., Main, R., Redick, E., Bagg, A., & Leatherland, J. (1991). Pain reduction interventions during neonatal circumcision. Nursing Research, 40, 241–244.
McCaffery, M., & Pasero, C. (1999). Assessment: Underlying complexities, misconceptions, and practical tools. In M. McCaffery & C. Pasero (Eds.), Pain: Clinical manual (2nd ed., pp. 35–102). St. Louis: Mosby.
McIntosh, N., Van Veen, L., & Brameyer, H. (1994). Alleviation of the pain of heel prick in preterm infants. Archives of Disease in Childhood, 70, F177–F181.
Miller, H., & Anderson, G. (1993). Nonnutritive sucking: Effects on crying and heart rate in intubated infants requiring assisted mechanical ventilation. Nursing Research, 42, 305–307.
Morison, S. J., Holsti, L., Grunau, R. E., Whitfield, M. F., Oberlander, T. F., Chan, H. W., et al. (2003). Are there developmentally distinct motor indicators of pain in pre-term infants? Early Human Development, 72(2), 131–146.
National Association of Neonatal Nurses. (2001). Pain assess-ment and management: Guideline for practice. Des Plaines, IL: Author.
O’Brien, L., Taddio, A., Lyszkiewicz, D. A., & Koren, G. (2005). A critical review of the topical local anesthetic amethocaine (Ametop) for pediatric pain. Paediatric Drugs, 7(1), 41–54.
Ogawa, S., Ogihara, T., Fujiwara, E., Ito, K., Nakano, M., Nakayama, S., et al. (2005). Venepuncture is prefer-able to heel lance for blood sampling in term neonates. Archives of Disease in Childhood. Fetal and Neonatal Edition, 90(5), F432–F436.
Olkkola, K. T., Maunuksela, E. L., Korpela, R., & Rosenberg, P. H. (1988). Kinetics and dynamics of postop-erative intravenous morphine in children. Clinical Pharmacology and Therapeutics, 44(2), 128–136.
Partridge, J. C., & Wall, S. N. (1997). Analgesia for dying infants whose life support is withdrawn or withheld. Pediatrics, 99(1), 76–79.
Plotsky, P., Bradley, C., & Anand, K. (2000). Behavioral and neuroendocrine consequences of neonatal stress. In K. J. S. Anand, B. J. Stevens, & P. J. McGrath (Eds.), Pain in neonates (2nd rev. ed., pp. 77–101). Amsterdam: Elsevier Science B.V.
Porter, F., Miller, J., Cole, F., & Marshall, R. (1991). A con-trolled clinical trial of local anesthesia for lumbar punc-ture in newborns. Pediatrics, 88, 663–669.
Porter, F., Porges, S., & Marshall, R. (1988). Newborn cries and vagal tone: Parallel changes in response to circumci-sion. Child Development, 59, 495–505.
Porter, F., Wolf, C., & Miller, J. (1998). The effect of han-dling and immobilization on the response to acute pain in newborn infants. Pediatrics, 102, 1383–1389.
Purcell-Jones, G., Dormon, F., & Sumner, E. (1987). The use of opioids in infants: A retrospective study of 933 cases. Anaesthesia, 42, 1316–1320.
Reynolds, M., Alvares, D., Middleton, J., & Fitzgerald, M. (1997). Neonatally wounded skin induces NGF-independent sensory neurite outgrowth in vitro. Developmental Brain Research, 102, 275–283.
Ruda, M. A., Ling, Q. D., Hohmann, A. G., Peng, Y. B., & Tachibana, T. (2000). Altered nociceptive neuronal cir-cuits after neonatal peripheral inflammation. Science, 289, 628–630.
Shah, P. S., Aliwalas, L. I., & Shah, V. (2006) Breastfeeding or breast milk for procedural pain in neonates. Cochrane Database of Systematic Reviews, 3, CD004950.
Shah, V., & Ohlsson, A. (2004). Venepuncture versus heel lance for blood sampling in term neonates. Cochrane Database of Systematic Reviews, 4, CD001452.
Shah, V., Taddio, A., & Ohlsson, A. (1998). Randomized controlled trial of paracetamol for heel prick pain in neonates. Archives of Disease in Childhood. Fetal and Neonatal Edition, 79, F209–F211.
Shapiro, C. (1993). Nurses’ judgments of pain in term and preterm newborns. Journal of Obstetric, Gynecologic, and Neonatal Nursing, 22(1), 41–47.
Shiao, S., Chang, Y., Lannon, H., & Yarandi, H. (1997). Meta-analysis of the effects of nonnutritive sucking on heart rate and peripheral oxygenation: Research from the past 30 years. Issues in Comprehensive Pediatric Nursing, 20, 11–24.
Shiroiwa, Y., Kamiya, Y., & Uchiboi, S. (1986). Activity, cardiac and respiratory responses of blindfold preterm infants in a neonatal intensive care unit. Early Human Development, 14, 259–265.
Simons, S. H., & Anand, K. J. S. (2006). Pain control: Opioid dosing, population kinetics and side-effects. Seminars in Fetal and Neonatal Medicine, 11, 260–267.
Simons, S. H., van Dijk, M., Anand, K. S., Roofthooft, D., van Lingen, R. A., & Tibboel, D. (2003). Do we still hurt newborn babies? A prospective study of procedural pain and analgesia in neonates. Archives of Pediatric Adolescent Medicine, 157, 1058–1064.
Stevens, B., & Johnston, C. (1994). Physiological responses of premature infants to a painful stimulus. Nursing Research, 43, 226–231.
Stevens, B., Johnston, C., Franck, L., Petryshen, P., Jack, A., & Foster, G. (1999). The efficacy of developmentally sensitive interventions and sucrose for relieving pro-cedural pain in very low birth weight infants. Nursing Research, 48(1), 35–43.
Stevens, B., Johnston, C., & Horton, L. (1993). Multidimensional pain assessment in premature infants: A pilot study. Journal of Obstetric, Gynecologic, and Neonatal Nursing, 22, 531–541.
Stevens, B., Johnston, C., Petryshen, P., & Taddio, A. (1996). Premature infant pain profile: Development and initial validation. Clinical Journal of Pain, 12, 13–22.
Stevens, B., McGrath, P., Gibbins, S., Beyene, J., Breau, L., Camfield, C., et al. (2007). Determining behavioural and physiological responses to pain in infants at risk for neu-rological impairment. Pain, 127(1–2), 94–102.

Pain Assessment and Management 23
Stevens, B., Taddio, A., Ohlsson, A., & Einarson, T. (1997). The efficacy of sucrose for relieving procedural pain in infants: A systematic review and meta-analysis. Acta Paediatrica, 86, 837–842.
Stevens, B., Yamada, J., Beyene, J., Gibbins, S., Petryshen, P., Stinson, J., et al. (2005). Consistent management of repeated procedural pain with sucrose in preterm neo-nates: Is it effective and safe for repeated use over time? Clinical Journal of Pain, 21(6), 543–548.
Stevens, B., Yamada, J., & Ohlsson, A. (2004). Sucrose for analgesia in newborn infants undergoing painful proce-dures. Cochrane Database of Systematic Reviews, 3, CD001069.
Stevens, B. J., Johnston, C. C., & Horton, L. (1994). Factors that influence the behavioral pain responses of premature infants. Pain, 59(1), 101–109.
Suresh, S., & Anand, K. (1998). Opioid tolerance in infants: Mechanisms, diagnosis, assessment, and management. Seminars in Perinatology, 22, 425–433.
Sweet, S., & McGrath, P. (1998). Relative importance of mothers’ versus medical staffs’ behavior in the predic-tion of infant immunization pain behavior. Journal of Pediatric Psychology, 23(4), 249–256.
Taddio, A., Goldbach, M., Ipp, M., Stevens, B., & Koren, G. (1995). Effect of neonatal circumcision on pain responses during vaccination in boys. Lancet, 345(1), 291–292.
Taddio, A., Katz, J., Ilersich, A. L., & Koren, G. (1997) Effect of neonatal circumcision on pain response during subse-quent routine vaccination. Lancet, 349(9052), 599–603.
Taddio, A., Ohlsson, A., Einarson, T., Stevens, B., & Koren, G. (1998). A systematic review of lidocaine-prilocaine cream (EMLA) in the treatment of acute pain in infants. Pediatrics, 101(2), 299.
van Lingen, R. A., Deinum, J. T., Quak, J. M., Kuizenga, A. J., van Dam, J. G., Anand, K. J., et al. (1999). Pharmacokinetics and metabolism of rectally administered paracetamol in preterm neonates. Archives of Disease in Childhood. Fetal and Neonatal Edition, 80, F59–F63.
Walden, M., Sudia-Robinson, T., & Carrier, C. (2001). Comfort care for infants in the neonatal intensive care unit at end of life. Newborn and Infant Nursing Reviews, 1, 97–105.
Ward-Larson, C., Horn, R. A., & Gosnell, F. (2004). The efficacy of facilitated tucking for relieving procedural pain of endotracheal suctioning in very low birthweight infants. MCN: The American Journal of Maternal Child Nursing, 29(3), 151–156.
Willis, D. M., Chabot, J., Radde, I. C., & Chance, G. W. (1977). Unsuspected hyperosmolarity of oral solution contributing to necrotizing enterocolitis in very low birth weight infants. Pediatrics, 60, 535–538.
Yaster, M., & Deshpande, J. (1988). Management of pediatric pain with opioid analgesics. Journal of Pediatrics, 113, 421–429.
Young, T., & Mangum, O. B. (2006). NeoFax (19th ed.). Raleigh, NC: Acorn Publishing.

National Association of Neonatal Nurses 24
Process Indicator 0 1 2 3 Score
Chart Gestational age ≥ 36 weeks 32 weeks–35 weeks 6 days
28 weeks–31 weeks 6 days
≤ 28 weeks ____________
Score 15 seconds before event
Behavioral state
Active/awake Eyes open Facial movements
Quiet/awake Eyes openNo facial movements
Active/sleep Eyes closedFacial movements
Quiet/sleepEyes closedNo facial
movements ____________
Record baseline heart rate (___); Observe infant 30 seconds after event
Maximum heart rate
0–4 beats/ minute increase
5–14 beats/ minute increase
15–24 beats/ minute increase
25 or more beats/minute increase
____________
Observe infant 30 seconds after event
Brow bulge None (0%–9% of time)
Minimum (10%–39% of time)
Moderate (40%–69% of time)
Maximum (70% or more of time) ____________
Observe infant 30 seconds after event
Eye squeeze None (0%–9% of time)
Minimum (10%–39% of time)
Moderate (40%–69% of time)
Maximum (70% or more of time) ____________
Observe infant 30 seconds after event
Nasolabial furrow
None (0%–9% of time)
Minimum (10%–39% of time)
Moderate (40%–69% of time)
Maximum (70% or more of time) ____________
Total score ____________
Figure 1.
Premature Infant Pain Profile (PIPP)
PIPP Scoring Guidelines
1. Score the correct gestational age before beginning. 2. Assess baseline heart rate and oxygen saturation. a. For procedural pain, assess before the event. b. If pain is already present, review the chart for earlier baseline. 3. Score behavioral state by observing the infant for 15 seconds immediately before the event. 4. Observe the infant for 30 seconds immediately after the event.
Note. From “Premature Infant Pain Profile: Development and Initial Validation,” by B. Stevens, C. Johnston, P. Petryshen, and A. Taddio, 1996, Clinical Journal of Pain, 12, p. 22. Copyright 1996 by Lippincott Williams & Wilkins. Adapted with permission.
Description of Score
Record baseline oxygen saturation (___);
Minimum oxygen saturation
0–2.4% decrease
2.5%–4.9% decrease
5%–7.4% decrease
7.5% or more decrease
Observe infant 30 seconds after event ____________

Pain Assessment and Management 25
Figure 2.
CRIES: Neonatal Postoperative Pain Assessment Score
Indicator 0 1 2
Crying No High pitched Inconsolable
Requires oxygen for saturation > 95%
No < 30% > 30%
Increased vital signs Heart rate and blood pressure within 10% of preoperative value
Heart rate and blood pressure 11%–20% higher than preoperative value
Heart rate and blood pressure 21% or more above preop-erative value
Expression None Grimace Grimace/grunt
Sleeplessness No Wakes at frequent intervals
Constantly awake
CryingScore 0: No cry or cry not high pitchedScore 1: Cry high pitched, but consolableScore 2: High-pitched cry, inconsolable
Requires oxygen for saturation > 95%Score 0: No oxygen required from baselineScore 1: Oxygen requirement < 30% from baselineScore 2: Oxygen requirement > 30% from baseline
Increased vital signsScore 0: Heart rate and blood pressure are both unchanged or
at less than baselineScore 1: Heart rate or blood pressure is increased by < 20%Score 2: Heart rate or blood pressure is increased by > 20% Note: Measure blood pressure last so as not to wake the infant.
ExpressionScore 0: No grimaceScore 1: Grimace only is presentScore 2: Grimace and nonaudible grunt presentNote: Grimace consists of lowered brow, eyes squeezed shut, deepening nasolabial furrow, and open lips and mouth
SleeplessnessScore 0: Continuously asleepScore 1: Awakens at frequent intervalsScore 2: Awake constantlyNote: Based on infant’s state during preceding hour.
CRIES Scoring Guidelines
Scoring Criteria
Note. From “Increasing Staff Nurse Awareness of Postoperative Pain Management in the NICU,” by J. Bildner and S. Krechel, 1996, Neonatal Network, 15(1), p. 16. Copyright 1996 by S. Krechel & J. Bildner. Developed at University of Missouri–Columbia. Reprinted with permission.

National Association of Neonatal Nurses 26
Facial expressionScore 0: Relaxed muscles = Restful face, neutral expressionScore 1: Grimace = Tight facial muscles; furrowed brow, chin, jaw; negative facial expression (nose, mouth, brow)CryScore 0: No cry = Quiet, not cryingScore 1: Whimper = Mild moaning, intermittentScore 2: Vigorous cry = Loud scream, rising, shrill, continuousNote: Silent cry, as evidenced by obvious mouth and other facial movement, may be scored if baby is intubated.Breathing patternsScore 0: Relaxed = Usual pattern for this babyScore 1: Change in breathing = Indrawing, irregular, faster than usual, gagging, breath holding
ArmsScore 0: Relaxed/restrained = No muscular rigidity, occasional random movements of arms Score 1: Flexed/extended = Tense, straight arms, rigid or rapid extension, flexion LegsScore 0: Relaxed/restrained = No muscular rigidity, occasional random movements of legs Score 1: Flexed/extended = Tense, straight legs, rigid and/or rapid extension, flexion State of arousalScore 0: Sleeping/awake = Quiet, peaceful, sleeping or alert and settled Score 1: Fussy: Alert, restless, thrashing
Note. From “The Development of a Tool to Assess Neonatal Pain,” by J. Lawrence, D. Alcock, D. P. McGrath, J. Kay, S. MacMurray, and C. Dulberg, 1993, Neonatal Network, 12(6), p. 60. Copyright 1993 by the Children’s Hospital of Eastern Ontario, Ottawa, ON, Canada. Reprinted with permission.
NIPS Scoring Guidelines
Figure 3.
Neonatal Infant Pain Scale (NIPS) Before During After 1 2 1 2 3 4 5 1 2 3 minute minutes minute minutes minutes minutes minutes minute minutes minutesFacial expression0: Relaxed muscles1: GrimaceCry0: No cry1: Whimper2: Vigorous cry Breathing patterns0: Relaxed1: Change in breathingArms0: Relaxed/restrained1: Flexed/extendedLegs0: Relaxed/restrained1: Flexed/extendedState of arousal0: Sleeping/awake1: Fussy
Totalt
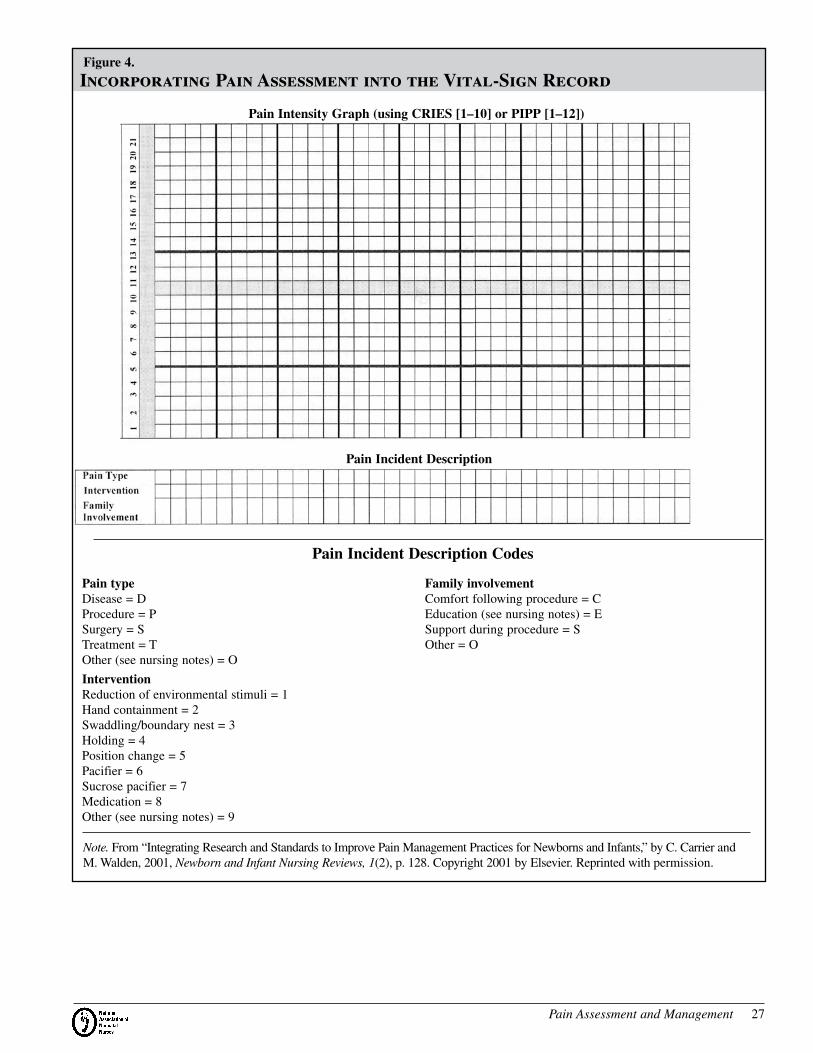
Pain Assessment and Management 27
Figure 4.
Incorporating Pain Assessment into the Vital-Sign Record
Pain typeDisease = DProcedure = PSurgery = STreatment = TOther (see nursing notes) = O
Intervention Reduction of environmental stimuli = 1Hand containment = 2Swaddling/boundary nest = 3Holding = 4Position change = 5Pacifier = 6Sucrose pacifier = 7Medication = 8Other (see nursing notes) = 9
Family involvementComfort following procedure = CEducation (see nursing notes) = ESupport during procedure = SOther = O
Pain Incident Description Codes
Pain Intensity Graph (using CRIES [1–10] or PIPP [1–12])
Pain Incident Description
Note. From “Integrating Research and Standards to Improve Pain Management Practices for Newborns and Infants,” by C. Carrier and M. Walden, 2001, Newborn and Infant Nursing Reviews, 1(2), p. 128. Copyright 2001 by Elsevier. Reprinted with permission.

National Association of Neonatal Nurses 28
Table 1. Analgesic Medications, Routes of Administration, and Recommended Dosages for Neonates
Drug Routes Dose Administration Notes
Opioid Analgesics
Morphine Intermittent intravenous (IV), intramuscular, subcutaneous
Continuous infusion
Oral/parenteral ratio
0.05–0.2 mg/kg
0.01–0.02 mg/kg/h
Give over at least 5 minutes.
Repeat as required (usually every 4 hours).
Give loading dose of 0.1–0.15 mg/kg over 1 hour. Oral dose
is 3–5 times IV dose.
Fentanyl Intermittent IV
Continuous infusion
1–4 mcg/kg
1–5 mcg/kg/h
Repeat as required (usually every 2–4 hours).
Tolerance may develop rapidly after constant infusion. Adjust
weaning schedule based on withdrawal symptoms.
Methadone By mouth (PO) 0.05–0.2 mg/kg Long-acting narcotic analgesic. Most commonly used for
weaning.
Give oral dose every 12–24 hours.
Adjust weaning schedule based on withdrawal symptoms.
Nonsteroidal Antiinflammatory Drugs
Acetaminophen PO
Rectal
12–15 mg/kg
12–18 mg/kg
Give loading dose of 20–25 mg/kg.
Give loading dose of 30 mg/kg.
Maintenance intervals:
Term infants: Give every 6 hours.
Preterm infants ≥32 weeks postconceptional age: Give
every 8 hours.
Preterm infants <32 weeks postconceptional age: Give every
12 hours.
Note. From NeoFax (19th ed., pp.150, 152–153, 161, 166–167), by T. E. Young and B. Mangum, 2006, Raleigh, NC: Acorn Publishing. Copyright 2006 by author. Adapted with permission.

Pain Assessment and Management 29
Table 2. Suggested Management of Painful Procedures Commonly Performed in the Neonatal Intensive Care Unit
Procedures
Pacifier with Sucrose
Swaddling, Containment, or Facilitated Tucking
EMLA Cream
Subcutaneous Infiltration of Lidocaine Opioids Other
Diagnostic ProceduresArterial puncture √ √ √ √Heel lancing √ √ Consider venipuncture, skin-
to-skin contact with mother; mechanical spring-loaded lance
Lumbar puncture √ √ √ Use careful physical handling
Venipuncture √ √ √Eye examination √ √ Consider topical anesthetic
Therapeutic ProceduresCentral venous line placement
√ √ √ √ √ Consider general anesthesia
Chest tube insertion
√ √ √ Anticipate need for intubation and ventilation in neonates spontaneously breathing, consider short-acting anes- thetic agents, avoid midazolam
Gavage tube insertion
√ √ Gentle technique and appro- priate lubrication
Intramuscular injection
√ √ √ Give drugs intravenously, whenever it is possible
Peripherally inserted central catheter placement
√ √ √ √
Endotracheal intubation
√ Various combinations of atropine, ketamine, thiopental sodium, succinylcholine chlo- ride, morphine, fentanyl, non- depolarizing muscle relaxant; consider topical lidocaine spray
Endotracheal suction
Sucrose optional
√ √
Surgical ProceduresCircumcision √ √ Mogen clamp preferred over
Gomco clamp; dorsal penile nerve block, ring block, or cau- dal block using plain or buffered lidocaine; consider acetamino- phen for postoperative pain
Note. From “Identification, Management, and Prevention of Newborn/Infant Pain,” by M. Walden and L. S. Franck in Comprehensive Neonatal Nursing: A Physiologic Perspective (3rd ed., p. 853), C. Kenner and J. W. Lott (Eds.), 2002, Philadelphia: W.B. Saunders. Copyright 2002 by W.B. Saunders. Reprinted with permission. This table was originally adapted from “Consensus Statement for the Prevention and Management of Pain in the Newborn,” by K. J. Anand and International Evidence-Based Group for Neonatal Pain, 2001, Archives of Pediatric Adolescent Medicine, 155, pp. 173–180. Copyright 2001 by the American Medical Association. Adapted with permission.

4700 W. Lake AvenueGlenview, IL 60025-1485800/451-3795Fax 888/477-6266www.NANN.org